 Tao Luo
Tao Luo Xiao Jiang
Xiao Jiang Ning Xu
Ning Xu Xinyu Zhao
Xinyu Zhao Xingjie Xie
Xingjie Xie Xiuwen Xia
Xiuwen Xia XiaoLong Bian
XiaoLong Bian Haixia Liu
Haixia Liu
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Mol. Biosci., 18 April 2024
Sec. Cellular Biochemistry
Volume 11 - 2024 | https://doi.org/10.3389/fmolb.2024.1341290
This article is part of the Research TopicThe Role of Glucose, Lipid, and Amino Acid Homeostasis in Metabolic DiseaseView all 5 articles
Objective: This study aimed to explore the risk factors, metabolic characteristics, and potential biomarkers of mild cognitive impairment in type 2 diabetes mellitus (T2DM-MCI) and to provide potential evidence for the diagnosis, prevention, and treatment of mild cognitive impairment (MCI) in patients with type 2 diabetes mellitus (T2DM).
Methods: A total of 103 patients with T2DM were recruited from the Endocrinology Department of The Second Affiliated Hospital of Dalian Medical University for inclusion in the study. The Montreal Cognitive Assessment (MoCA) was utilized to evaluate the cognitive functioning of all patients. Among them, 50 patients were categorized into the T2DM-MCI group (MoCA score < 26 points), while 53 subjects were classified into the T2DM without cognitive impairment (T2DM-NCI) group (MoCA score ≥ 26 points). Serum samples were collected from the subjects, and metabolomics profiling data were generated by Ultra-high performance liquid chromatography-mass spectrometry (UHPLC-MS). These groups were analyzed to investigate the differences in expression of small molecule metabolites, metabolic pathways, and potential specific biomarkers.
Results: Comparison between the T2DM-MCI group and T2DM-NCI group revealed significant differences in years of education, history of insulin application, insulin resistance index, insulin-like growth factor-binding protein-3 (IGFBP-3), and creatinine levels. Further binary logistic regression analysis of the variables indicated that low educational level and low serum IGFBP-3 were independent risk factor for T2DM-MCI. Metabolomics analysis revealed that differential expression of 10 metabolites between the T2DM-MCI group and T2DM-NCI group (p < 0.05 and FDR<0.05, VIP>1.5). Kyoto Encyclopedia of Genes and Genomes (KEGG) enrichment pathway analysis revealed that fatty acid degradation was the most significant pathway. Receiver operating characteristic (ROC) analysis shows that lysophosphatidylcholine (LPC) 18:0 exhibited greater diagnostic efficiency.
Conclusion: This study revealed that a shorter duration of education and lower serum IGFBP-3 levels are independent risk factors for T2DM-MCI. Serum metabolites were found to be altered in both T2DM-MCI and T2DM-NCI groups. T2DM patients with or without MCI can be distinguished by LPC 18:0. Abnormal lipid metabolism plays a significant role in the development of MCI in T2DM patients.
Type 2 Diabetes Mellitus (T2DM) is a prevalent subtype of diabetes mellitus (Srikanth et al., 2020) characterized by chronic hyperglycemia resulting from reduced insulin sensitivity in individuals. The International Diabetes Federation (IDF) estimated that 537 million adults aged 20–79 years had diabetes in 2021 (Sun et al., 2022). T2DM induces damage and dysfunction in a majority of tissues and organs (Harding et al., 2019), leading to severe complications such as diabetic ketoacidosis (DKA), hyperosmolar hyperglycaemic state (HHS), and MCI (Umpierrez and Korytkowski, 2016).
Cognitive function refers to the brain’s ability to receive, process, and transform external information. T2DM is a risk factor for cognitive dysfunction, which is now acknowledged as a complication of T2DM (Simó et al., 2017). Patients suffering from T2DM combined with cognitive impairment are less capable of managing their diabetes, leading to a vicious cycle between T2DM and cognitive dysfunction. This cycle substantially increases the health and financial burden on patients with T2DM who also experience cognitive impairment. However, the risk factors and specific mechanisms underlying cognitive impairment in T2DM patients have not yet been fully elucidated, and there is no uniform standard for the diagnosis and treatment of cognitive impairment in this population. Therefore, it is imperative to identify the controllable risk factors and pathogenesis of cognitive impairment in T2DM patients and to explore the therapeutic targets for the prevention and treatment of cognitive impairment in T2DM patients population in the future.
Metabolomics, characterized by its high sensitivity, throughput, and accuracy, is a research technique finding extensive applications in the medical field, particularly in the study of metabolic diseases. In clinical research, metabolomic changes are assessed, and biomarkers of disease are explored through metabolomics. Several studies based on metabolomic analysis techniques, utilizing various samples of small molecule metabolites from diabetic patients or animal models, have revealed metabolic abnormalities in individuals or animals with cognitive impairment compared to those with normal cognition (Song et al., 2017; Zhao et al., 2018; Sun et al., 2020; Chen et al., 2021). However, research involving non-targeted metabolomics of T2DM-MCI remains relatively scarce. Ultra-high performance liquid chromatography-mass spectrometry (UHPLC-MS), a commonly employed metabolomics technique known for its high sensitivity and coverage of the metabolome, is widely utilized in the analysis of non-targeted metabolomics biomarkers of disease.
In our research, we analyzed the risk factors for T2DM-MCI and identified metabolomic indicators using UHPLC-MS. We compared the differences in metabolic components between T2DM-NCI and T2DM-MCI, analyzed the abnormal metabolic pathways in T2DM-MCI, identified characteristic biomarkers of T2DM-MCI, and provided new insights for effective interventional treatment of cognitive impairment in T2DM patients in the future.
The research received approved from the Ethics Committee of The Second Affiliated Hospital of Dalian Medical University (Approval Number: 2021 NO. 121). A total of 113 patients with T2DM admitted to the department of Endocrinology at The Second Affiliated Hospital of Dalian Medical University were enrolled in the T2DM group. The cognitive function of all subjects was assessed using the MoCA scale (Supplementary Figure S1). Among them, 50 patients with MoCA scores < 26 were categorized into the T2DM-MCI group, while 53 patients with MoCA scores ≥ 26 were classified into the T2DM-NCI group.
According to the 2022 diagnostic criteria of the American Diabetes Association (ADA) (American Diabetes Association Professional Practice Committee, 2022), diabetes is diagnosed in individuals presenting typical hyperglycemic symptoms and meeting one of the following conditions: (a) Fasting Plasma Glucose (FPG) ≥ 7.0 mmol/L; (b) Oral Glucose Tolerance Test (OGTT) ≥ 11.1 mmol/L; (c) Glycosylated Hemoglobin (HbA1c) ≥ 6.5%; (d) Random blood glucose ≥11.1 mmol/L in patients exhibiting typical symptoms of hyperglycemia or hyperglycaemic crisis.
Meeting the aforementioned diagnosis and the criteria indicates the presence of T2DM, characterized by: (a) Adult-onset, insidious onset, and chronic course; (b) Absence of tendency to ketosis in a non-stressed state; (c) Efficacy of hypoglycemic drugs; (d) Negative insulin-related antibodies, low insulin secretion curve, and C-peptide (C-P) release curve or delayed peak.
The criteria for diagnosing MCI follow the guidelines established by the National Institute on Aging-Alzheimer’s Association (NIA-AA) (Albert et al., 2011), including: (a) Cognitive deficits reported by the patient, family member, or physician; (b) Objective evidence of impairment in one or more cognitive domains. In this study, cognitive function was assessed using the MoCA scale, with a MoCA score of ≥26 considered as NCI and a score of <26 indicating MCI. If the individual has 12 years of education or less, 1 point will be added to their MoCA score. (c) Maintaining independent living ability; (d) Absence of dementia.
Hypoglycemia is a common complication in individuals with diabetes. The workgroup of the ADA proposed diabetic hypoglycaemia for clinical trials as follows: In numerical terms, a blood glucose value of 3.9 mmol/L (70 mg/dL) or lower with associated symptoms is usually considered a hypoglycemic condition (Workgroup on Hypoglycemia and American Diabetes Association, 2005).
The T2DM group includes patients who meet the following criteria: (a) Diagnosis of T2DM for more than 1 year; (b) No significant speech, visual or hearing impairment; (c) Ability to read and write independently.
All individuals meeting any of the following criteria will be excluded: (a) Traumatic brain injury, intracranial occupancy, cerebrovascular disease, epilepsy, anxiety, depression, dementia, and other psychiatric and neurological disorders; (b) Medications with cognitive impairment adverse effects; (c) History of cognitive impairment predating the diagnosis of T2DM; (d) Acute diabetic complications; (e) Inflammatory diseases, autoimmune diseases, hematological diseases, thyroid diseases, malignancies, cardiac, respiratory, hepatic, and renal failure, among others; (f) Chronic excessive alcohol consumption (more than 60 g per day); (g) Receipt of intravenous anesthesia within the past month.
The patients’ serum was collected and analyzed using the UHPLC-MS technique. A total of 400 μL of methanol extract containing the internal standard (refer to Supplementary Table S1 for details on the internal standard content) was thoroughly mixed with 100 μL of serum sample. The mixture was then vortexed, centrifuged and divided into two separate portions of 180 μL each for analysis in positive and negative ion mode. Prior to analysis, the samples were re-solubilized with 50 μL of 25% acetonitrile. Blank samples were used to equilibrate the system before analyzing the actual samples. Furthermore, during the analysis, one quality control (QC) sample was injected after every 10 injections of the actual sample to monitor the stability of the sample pretreatment and instrument operation.
A Waters BEH C8 column (size: 50 mm × 2.1 mm, 1.7 μm) (Waters, Milford, MA) was utilized for positive ion mode (ESI+) separation, employing a mobile phase consisting of water with 0.1% formic acid (A) and acetonitrile with 0.1% formic acid (B). The gradient began at 5% B and was maintained for 0.5 min, then increased to 40% B over 1.5 min, followed by a linear increase to 100% B over 6 min, which was held for 2 min before returning to the initial gradient of 5% B at 10.1 min and equilibrating for 2 min. An ACQUITY UPLC HSS T3 column (size: 50 mm × 2.1 mm, 1.8 μm) (Waters, Milford, MA) was utilized for negative ion mode (ESI-) separation. The mobile phases consisted of water spiked with 6.5 mM NH4HCO3 (A) and 95% methanol and 6.5 mM NH4HCO3 aqueous solution (B). The gradient commenced at 2% B and was maintained for 0.5 min, then increased to 40% B over 2 min, followed by a linear increase to 100% B over 6 min and held for 2 min before reverting to the initial gradient of 2% B at 10.1 min and equilibrating for 1.9 min. In both ion modes, the column temperature was set at 60°C and the elution flow rate was 0.4 mL/min.
The capillary temperature was set to 300°C, with auxiliary heating gas temperature at 350°C. Sheath and auxiliary gas flow rates were maintained at 45 and 10 (arbitrary units), respectively, while the full scan resolution was set to 7e4. For the positive ion mode, the m/z scan range was 80–1,200 Da, with a spray voltage of 3.50 kV. In the negative ion mode, the m/z scan range was 80–1,200 Da, with a spray voltage of 3.00 kV.
The normally distributed data from clinical parameters of the T2DM-MCI and T2DM-NCI groups were expressed as mean ± standard deviation. Variables with skewed distributions were described with 95% confidence intervals. The differences among the two groups were analyzed using t-tests or non-parametric tests.
All statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS) version 25.0 (SPSS, Chicago, IL, United States). Results were considered statistically significant with two-tailed analyses at p < 0.05. Partial Least Squares Discriminant Analysis (PLS-DA) and Orthogonal Projections to Latent Structures Discriminant Analysis (OPLS-DA) were conducted using SIMCA version 14.1 (Umetrics AB, Umea, Sweden). Serum metabolites with a Variable Important in Projection (VIP) value greater than 1.5 in the OPLS-DA model were assessed for statistical significance using either a t-test or nonparametric test.
The data were normalized using MetaboAnalyst 5.0 (https://www.metaboanalyst.ca/) to reduce systematic bias and improve consistency. Features with >25% missing values were removed, and the remaining missing values were replaced by the mean in the original data. The data were then normalized by sum, mean-centered, and divided by the square root of the standard deviation of each variable. Enrichment analysis and metabolite heatmap generation were conducted using MetaboAnalyst. Correlation analysis was performed by Origin 2021. ROC curves were generated using SPSS to assess the diagnostic efficiency of differential metabolites. Metabolite point plotting was performed using Graph Prism 9.0.
The clinical baseline parameters of the T2DM-MCI and the T2DM-NCI groups are shown in Table 1. In comparison to the T2DM-NCI group, the T2DM-MCI group exhibited a statistically significant difference in years of education (12.00 vs. 15.00 years) and history of insulin application (60.0% vs. 35.8%) (p < 0.05), while other parameters did not demonstrate significance (p > 0.05).
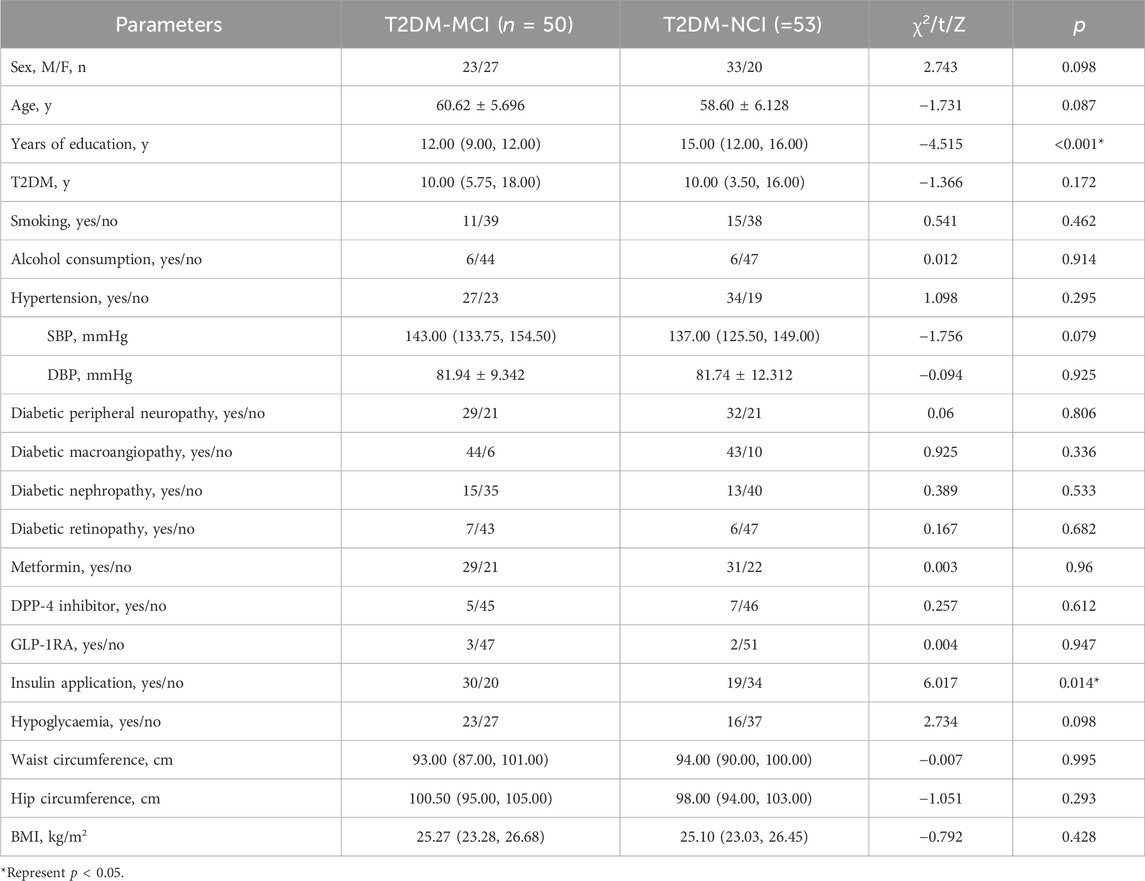
Table 1. Comparison of clinical parameters between the T2DM-MCI and the T2DM-NCI group.
Clinical laboratory findings revealed no significant differences in HbA1c, FPG, insulin, C-P, Homeostatic Model Assessment of β (HOMA-β), insulin-like growth factor 1 (IGF-1), total cholesterol (TC), triglyceride (TG), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), Apolipoprotein (Apo) AⅠ, ApoB, Alanine Aminotransferase (ALT), Aspartate Aminotransferase (AST), Albumin (Alb), Interleukin (IL)-1β, IL-2R, IL-6, IL-8, IL-10, TNF-α, and Tumor Necrosis Factor-alpha (TNF-α) and Urinary Albumin (U-ALB)/Creatinine (Cr) between the T2DM-MCI and T2DM-NCI groups (p > 0.05). However, IGFBP-3 and Cr levels were notably lower, and HOMA-IR (Homeostatic Model Assessment of Insulin Resistance) was significantly higher in T2DM-MCI patients compared to T2DM-NCI subjects (p < 0.05) (Table 2).
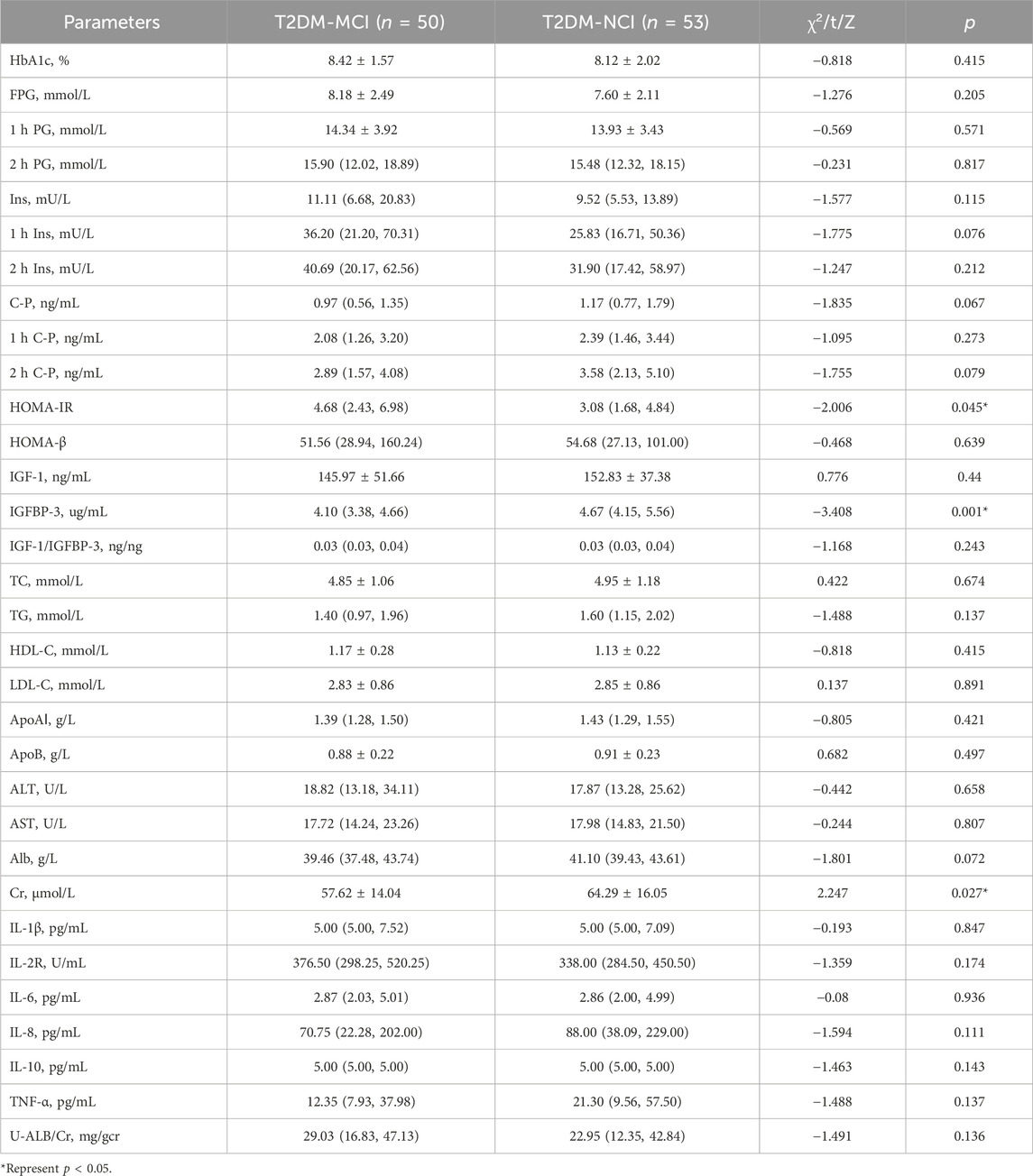
Table 2. Comparison of clinical laboratory parameters between the T2DM-MCI and the T2DM-NCI group.
Multifactorial binary logistic regression analysis was used to evaluate independent risk factors in T2DM patients with or without MCI. Years of education, history of insulin application, HOMA-IR, IGFBP-3, and Cr (p < 0.05 in Analysis of Variance) were employed as independent variables. The results indicated that short education and low serum IGFBP-3 levels were independent risk factors for MCI in T2DM patients. Specifically, each year of education in T2DM patients increased the risk of MCI by 22.2%, and each unit decrease in serum IGFBP-3 increased the risk of MCI by 51.7% (Refer to Table 3 for details).
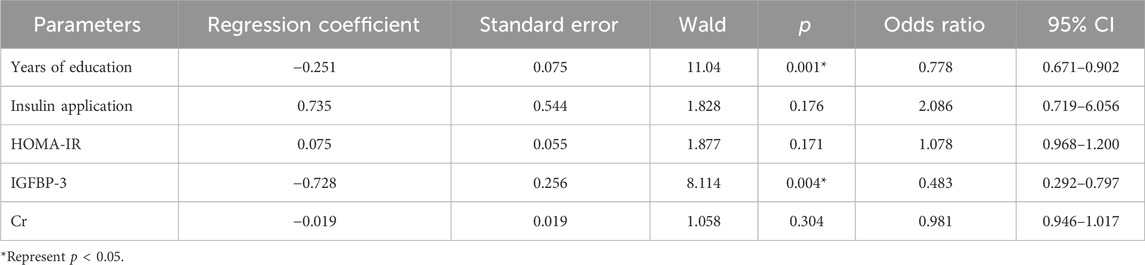
Table 3. Multifactor binary logistic regression analysis of T2DM and MCI.
A total of 103 patients’ sera were collected, from which 12 samples were excluded due to sub-optimal quality. Subsequently, 47 cases in the T2DM-MCI group and 44 cases in the T2DM-NCI group were utilized for the metabolomic data analysis. The study flowchart is depicted in Supplementary Figure S2, and detailed demographic characteristics of the participants are presented in Tables 4, 5. Both groups exhibited significance in years of education, history of insulin application, IGFBP-3, Cr, and MoCA Score (p < 0.05). Furthermore, no significant differences were observed for sex, age, Body Mass Index (BMI), FPG, HbA1c, TC, TG, HDL-C, LDL-C, HOMA-IR, HOMA-β, and IGF-1 between the T2DM-MCI and T2DM-NCI groups (p > 0.05).
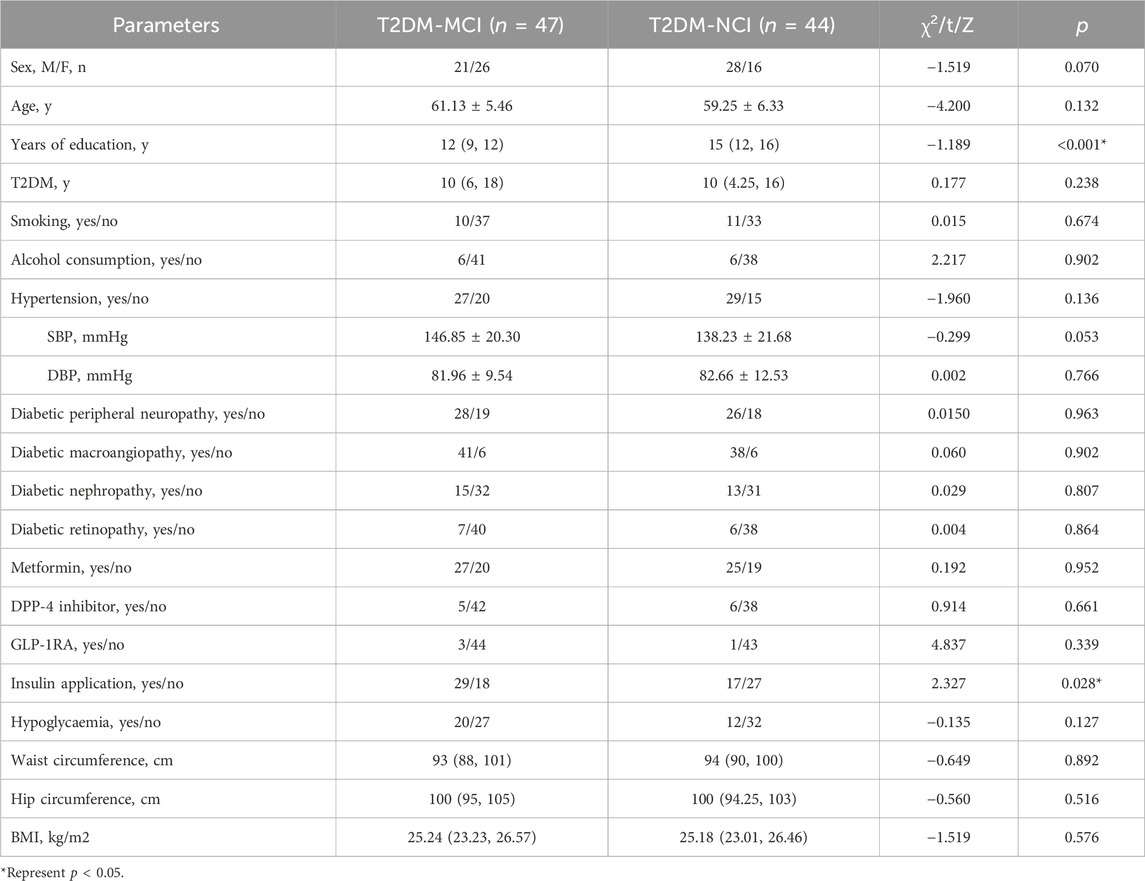
Table 4. Comparison of clinical parameters between the T2DM-MCI and the T2DM-NCI group.
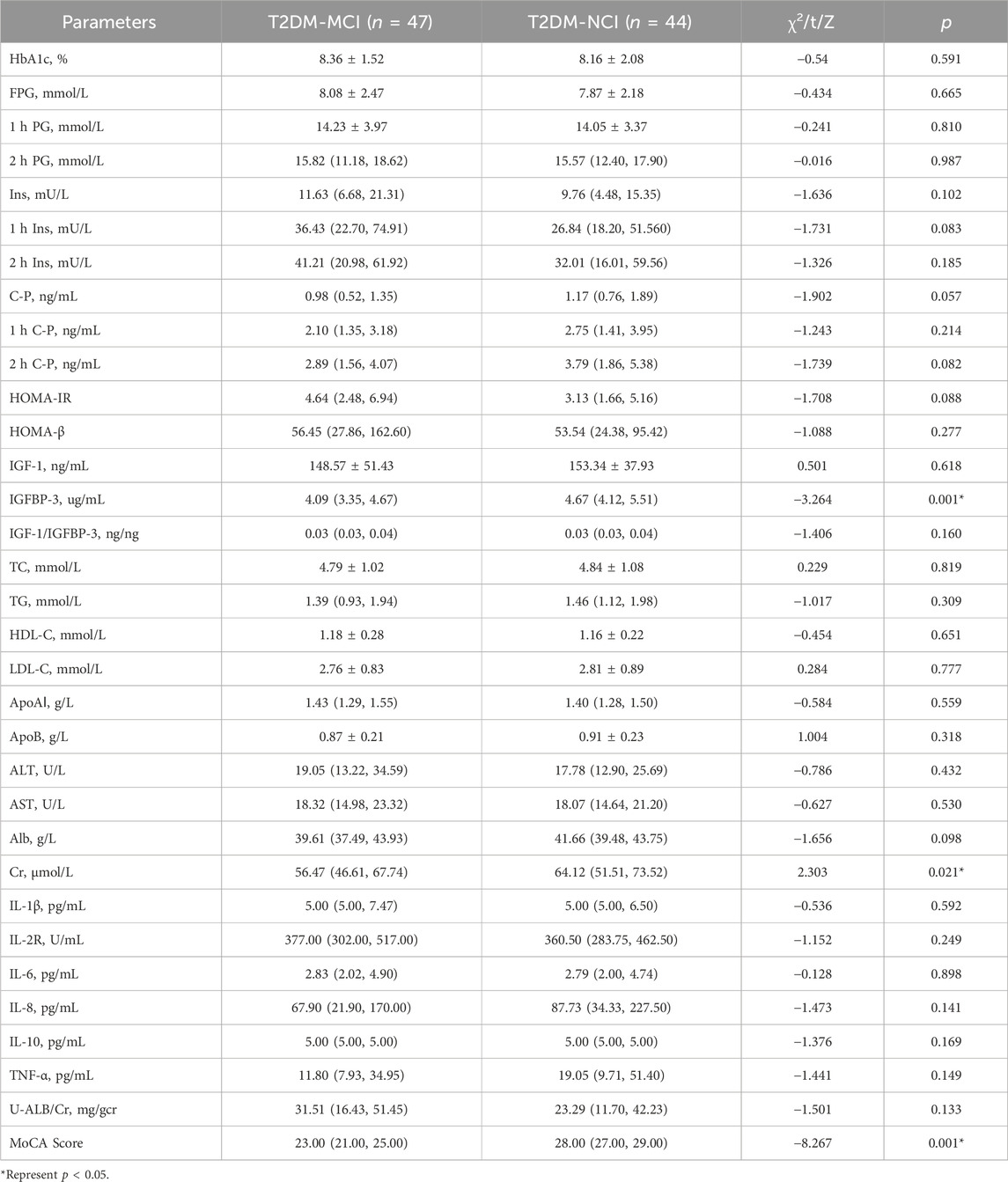
Table 5. Comparison of clinical laboratory parameters between the T2DM-MCI and the T2DM-NCI group.
Partial Least Squares-Discriminant Analysis (PLS-DA) was performed on the metabolomics data, revealing differences in metabolic profiles between the T2DM-MCI and T2DM-NCI groups, indicating aberrant metabolism in T2DM-MCI. The permutation test plots (Figures 1A, B) exhibited permutation test intercepts of (ESI+) R2X = 0.343, R2Y = 0.436, Q2 = 0.238, and (ESI−) R2X = 0.33, R2Y = 0.421, Q2 = 0.269 for the positive and negative ion models, respectively.
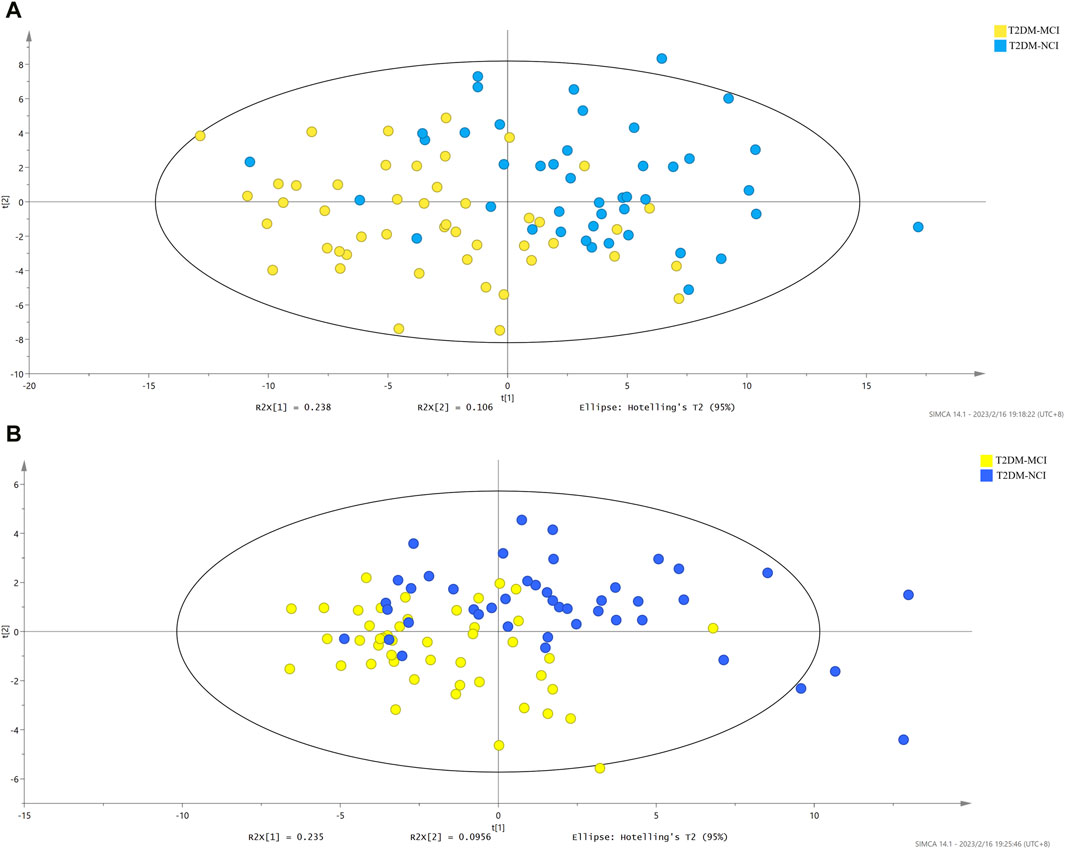
Figure 1. (A) PLS-DA score plot of the T2DM-MCI group vs. the T2DM-NCI group in ESI+ (R2X = 0.343, R2Y = 0.436, Q2 = 0.238). (B) PLS-DA score plot of the T2DM-MCI group vs. the T2DM-NCI group in ESI- (R2X = 0.33, R2Y = 0.421, Q2 = 0.269).
Between-group differences were assessed using independent samples t-tests or Mann-Whitney U tests. Based on the VIP and significant differences between the two groups, 10 metabolites were identified (p < 0.05, VIP > 1.5, and FDR < 0.05, as shown in Table 6). In the comparison between the T2DM-MCI and T2DM-NCI groups, lysophosphatidylcholine (LPC) 16:0 sn-1, LPC 16:0 sn-2, LPC 18:0 sn-1, phosphatidylcholine (PC) 38:6, sphingomyelin (SM) 34:1, free fatty acid (FFA) 19:0, FFA 24:1, LPC 16:0, and LPC 18:0 were higher in T2DM-NCI patients, while SM 36:2 was lower (Figure 2; Table 6). The heatmap of metabolites is displayed in Figure 3.
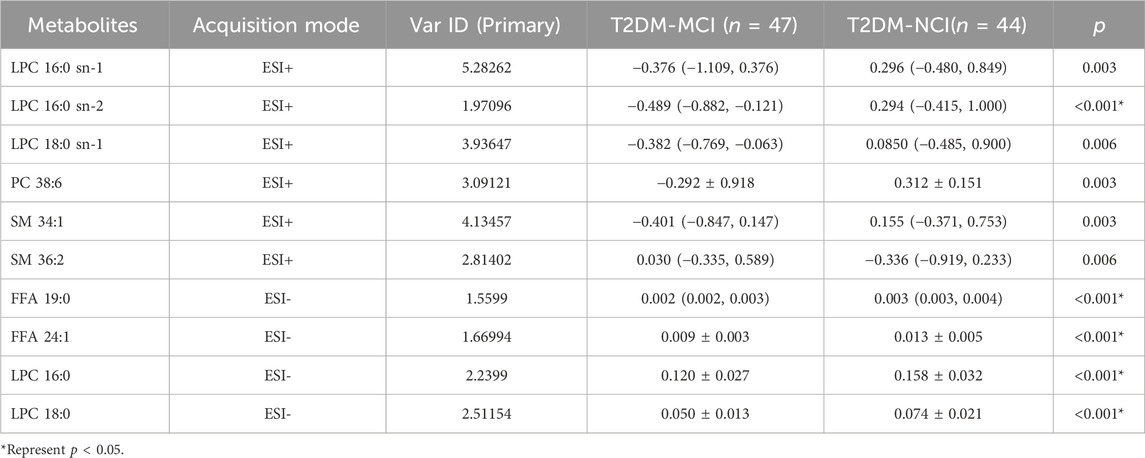
Table 6. Identified metabolites between the T2DM-MCI and the T2DM-NCI group.
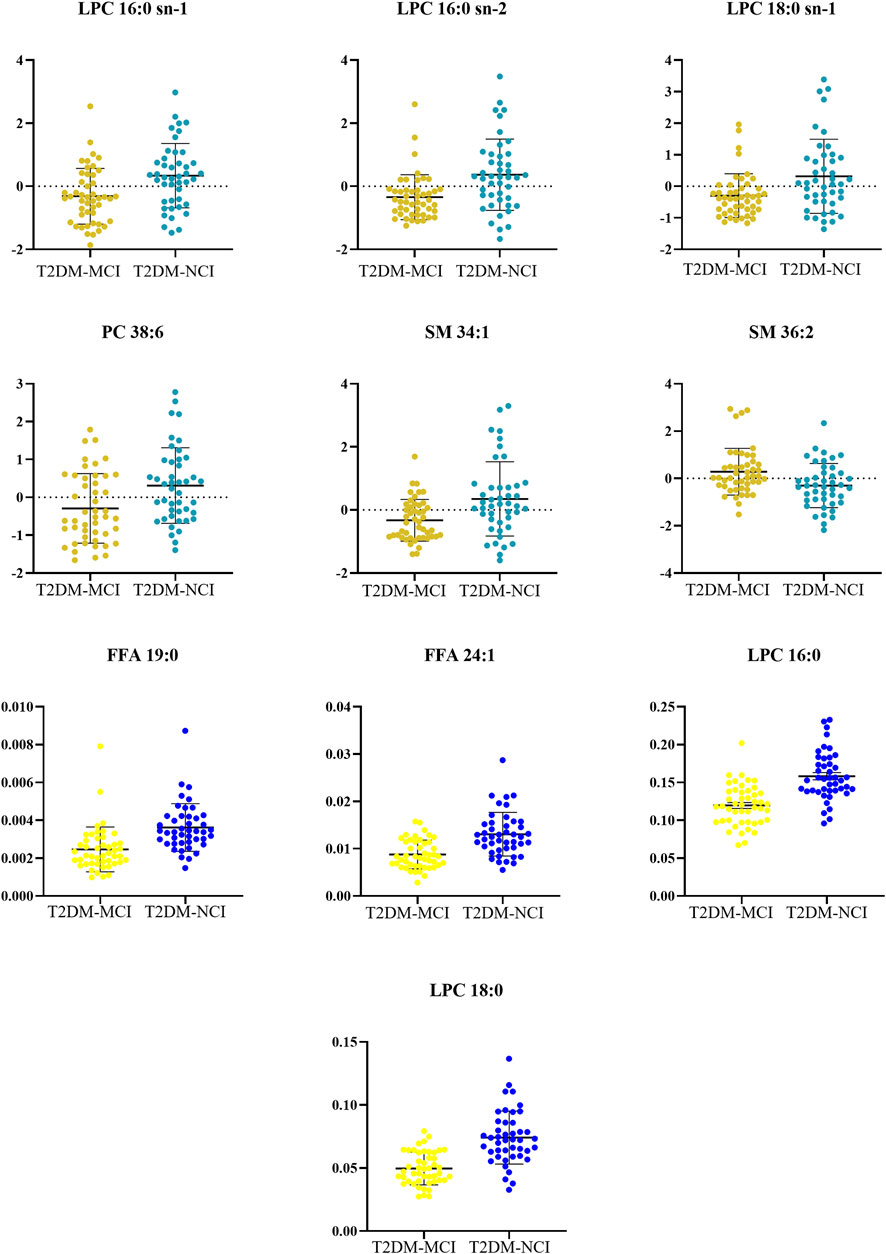
Figure 2. The metabolites from comparison between the T2DM-MCI and the T2DM-NCI group.
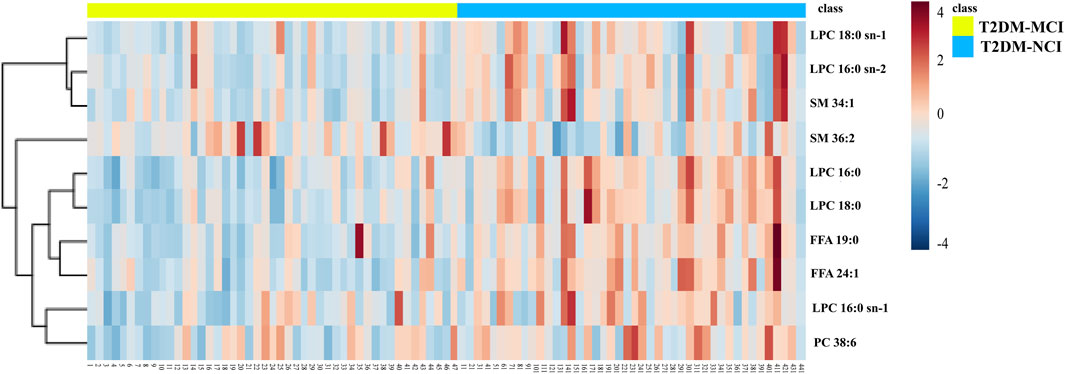
Figure 3. The heatmap metabolites from comparison between the T2DM-MCI and the T2DM-NCI group.
We calculated the area under the curve (AUC), sensitivity, and specificity of the metabolites screened as potential biomarkers, which showed that each metabolite had good predictability (AUC > 0.6, Figures 4A–I, Table 7). LPC18:0 was the most diagnostically efficient in distinguishing T2DM-MCI from T2DM-NCI (Figure 4J, AUC = 0.848, 95% CI: 0.767–0.928). Additionally, the AUC values for FFA 19:0 and LPC16:0 were also greater than 0.8 (Figures 4G, I).
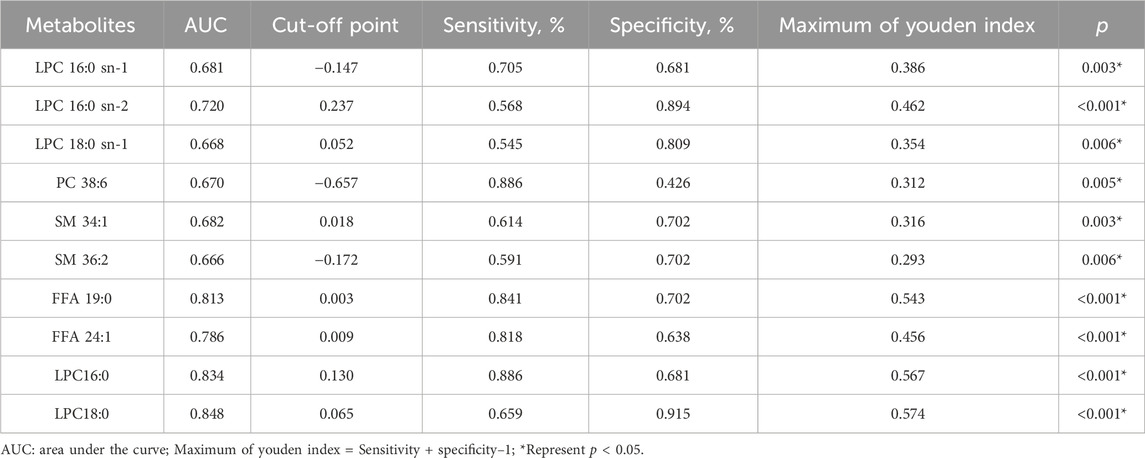
Table 7. Receiver operating characteristic curve analysis of 10 metabolites.
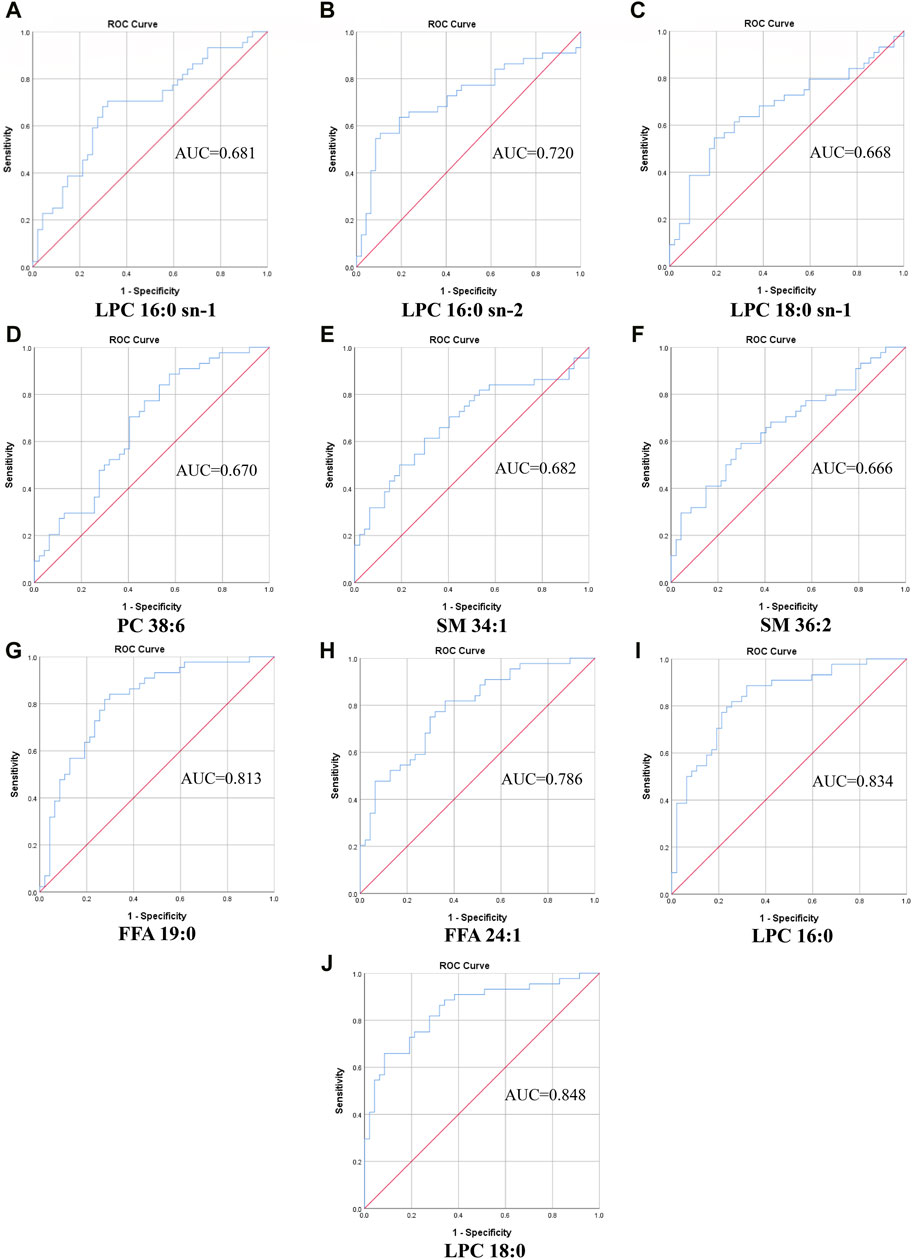
Figure 4. The ROC curve of selected metabolomics. (A) LPC 16:0 sn-1, AUC = 0.681. (B) LPC 16:0 sn-2, AUC = 0.720. (C) LPC 18:0 sn-1, AUC = 0.668. (D) PC 38:6, AUC = 0.670. (E) SM 34:1, AUC = 0.682. (F) SM 36:2, AUC = 0.666. (G) FFA 19:0, AUC = 0.813. (H) FFA 24:1, AUC = 0.786. (I) LPC16:0, AUC = 0.834. (J) LPC18:0, AUC = 0.848.
Enrichment analysis was conducted to confirm the significantly altered metabolic pathways based on the Kyoto Encyclopedia of Genes and Genomes (KEGG) database using Metaboanalyst. Fatty acid degradation, ubiquinone and other terpenoid-quinone biosynthesis, and tyrosine metabolism had a significant impact on T2DM-MCI (Figures 5A, B).
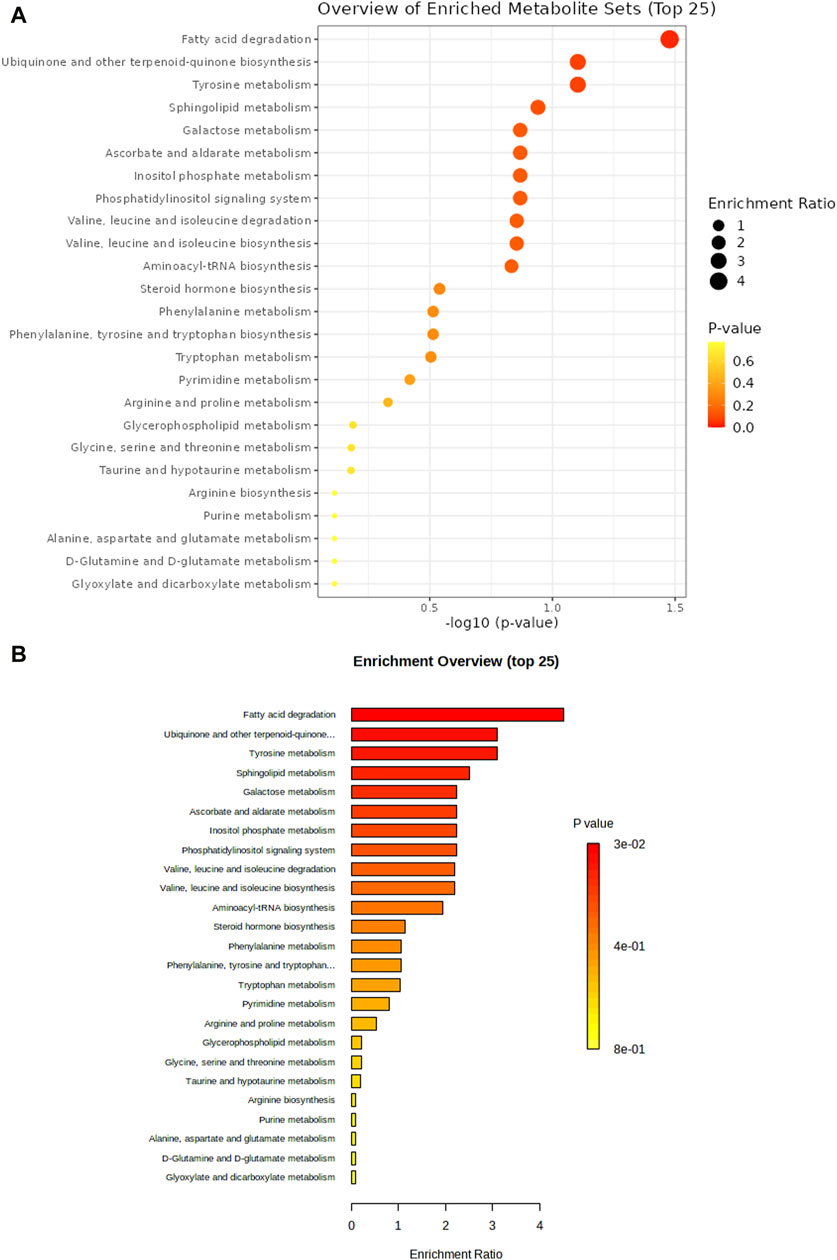
Figure 5. Enrichment analysis was performed to confirm the significantly changed metabolic pathway based on the Kyoto Encyclopedia of Genes and Genomes database through Metaboanalyst (A,B).
T2DM and MCI are highly prevalent among middle-aged and elderly individuals, with a global increase in incidence attributed to population aging. Accumulating epidemiological evidence supports the notion that T2DM serves as a risk factor for cognitive impairment (Xue et al., 2019; You et al., 2021). Consequently, our study focused on analyzing the risk factors associated with T2DM-MCI, utilizing metabolomic analysis to investigate aberrant metabolic profiles. This approach facilitated the identification of potential specific biomarkers, offering valuable insights for the prevention, early diagnosis, and interventional treatment of T2DM-MCI.
Our research indicated that a shorter duration of education served as an independent risk factor for T2DM-MCI, consistent with previous findings (Exalto et al., 2013; Sun et al., 2020; Suain Bon et al., 2021). Secondary and higher education were associated with lower odds of cognitive impairment compared to those with no formal education or primary education only (Suain Bon et al., 2021). Domestic studies further demonstrated that receiving more than 12 years of education served as an independent protective factor (Xu et al., 2021). Sun et al. (2020) observed that individuals with higher levels of education and those engaged in intellectually stimulating occupations tend to exhibit a higher density of synapses in the cerebral cortex, subsequently enhancing the brain’s storage capacity and delaying dementia symptoms. Consequently, both T2DM patients and those without the condition should aim to improve their educational attainment and engage in brain-stimulating activities to reduce the risk of cognitive impairment.
Our findings suggest that decreased serum levels of IGFBP-3 serve as an independent risk factor for T2DM-MCI, consistent with the observations of Wennberg et al., who reported a positive association between higher IGFBP-3 levels and cognition among female subjects (Wennberg et al., 2018). Furthermore, Duron et al. (2012)’s study showed a significant increase in IGFBP-3 levels in the T2DM-MCI group compared to the control group, suggesting that IGFBP-3 also contributes to preserving cognitive function.
In our study, a statistically significant difference was observed in the history of insulin application between the T2DM-MCI group and the T2DM-NCI group. The potential mechanism involves the Insulin-degrading Enzyme (IDE), which degrades both insulin and amyloid-β (Aβ). Insulin competes with Aβ for IDE, leading to reduced degradation of Aβ and an increased risk of cognitive impairment due to Aβ deposition in the brain (Qiu and Folstein, 2006). Additionally, some scholars have suggested that T2DM patients receiving insulin treatment may experience a longer disease duration, increased complications, poorer islet function, and hypoglycemia, all of which can contribute to brain impairment.
Previous studies have reported that hypoglycemic episodes may increase the risk of cognitive impairment (Ye et al., 2024). In our study, although the frequency of hypoglycemic episodes in both groups of patients did not reach statistical significance, the T2DM-MCI group showed a higher occurrence of hypoglycemic episodes compared to the T2DM-NCI group.
Our findings suggest a link between insulin resistance (IR) and cognitive decline among patients with type 2 diabetes mellitus (T2DM). IR is characterized by decreased insulin sensitivity in target organs or tissues, leading to suboptimal biological effects of insulin secretion. This condition triggers compensatory elevations in peripheral insulin levels to sustain normal insulin function. IR has been recognized as a risk factor for mild cognitive impairment (MCI) in patients with T2DM (Kong et al., 2018; Pal et al., 2018). The pathogenesis of cognitive impairment associated with IR is complex and may encompass hyperinsulinemia, resistance to IGF-1, IR deposition, tau protein phosphorylation, inflammatory response, and oxidative stress. These processes lead to pathological changes closely linked to Alzheimer’s disease (AD), such as amyloid plaque formation, neuronal degeneration, and cognitive decline (Takahashi et al., 2017; Kellar and Craft, 2020). IR can be effectively managed in patients with T2DM through dietary and exercise interventions, which may improve IR and mitigate the risk of IR-related cognitive impairment.
Our findings demonstrated that the serum creatinine level in the T2DM-MCI group was significantly lower (57.62 ± 14.04 umol/L) compared to the T2DM-NCI group (64.29 ± 16.05 umol/L). Consistently, metabolomic analysis revealed lower creatinine levels in the T2DM-MCI group, indicating a potential association between decreased serum creatinine levels and cognitive impairment among T2DM patients. Serum creatinine primarily arises from muscle creatine and serves as a reliable marker of muscle mass in healthy individuals. Skeletal muscle, being a primary target tissue for insulin, exhibits a strong association with T2DM. Elevated blood glucose levels and peripheral nerve and vascular complications among T2DM patients are associated with decreased muscle mass, as reported in (Izzo et al., 2021). Evidence supports a correlation between decreased skeletal muscle mass and function, and impaired cognitive function, as cited in (Sui et al., 2020). Furthermore, additional evidence indicates that creatine supplementation may enhance cognitive function, as referenced in (Rawson and Venezia, 2011). Consequently, T2DM patients can potentially mitigate cognitive impairment by engaging in creatine supplementation and physical activity. Serum creatinine levels could potentially serve as a marker for identifying individuals at high risk of cognitive impairment among T2DM patients without kidney disease.
Besides the aforementioned factors, domestic scholars have identified various risk factors for T2DM-MCI, including age, diabetes duration, fasting blood glucose (FBG), HbA1c, low serum C-P levels, TC TG, LDL-C, waist circumference, and BMI. Additionally, moderate alcohol consumption and HDL-C levels serve as protective factors for T2DM-MCI, whereas diabetic macrovascular and microangiopathy are strongly associated with cognitive decline among patients, as documented in (Sun et al., 2020; Xia et al., 2020).
Previous studies have reported associations between cognitive decline and interleukin-1β (IL-1β), hypoglycemia, hypertension, elevated diabetic complications, smoking, and excessive alcohol consumption (Gorska-Ciebiada et al., 2016; Nilsson et al., 2019). Contrary to the aforementioned studies, our investigation did not detect any significant differences in age, disease duration, diabetic complications, smoking and alcohol consumption habits, hypertension, hypoglycemia, waist circumference, BMI, blood glucose levels, C-peptide concentrations, lipid profiles, or inflammatory markers. We hypothesize that these disparities may be attributed to variations in study design, sample size, assessment methodologies, and unique characteristics of T2DM.
We performed a serum metabolomic analysis on samples from T2DM-MCI patients and T2DM-NCI controls, identifying abnormalities in 10 metabolites between the T2DM-MCI and T2DM-NCI groups. Notably, decreased levels were observed in T2DM-MCI patients for LPC 16:0 sn-1, LPC 16:0 sn-2, LPC 18:0 sn-1, LPC 16:0, LPC 18:0, PC 38:6, SM 34:1, FFA 19:0, and FFA 24:1, whereas SM 36:2 levels were elevated. Additionally, LPC18:0 emerged as a potential biomarker for T2DM-MCI through ROC curve analysis.
Phospholipids play several crucial biological roles in the human body, and there is substantial evidence indicating that disorders of phospholipid metabolism are associated with cognitive impairment (Mapstone et al., 2014; Gorska-Ciebiada et al., 2016; Zhang et al., 2017; Nilsson et al., 2019; Xia et al., 2020). Phospholipids are classified into several categories based on their molecular structure, including phosphatidylcholine (PC), sphingomyelin (SM), and other phospholipids. These compounds serve as integral components of cell membranes in living organisms, playing a crucial role in maintaining membrane integrity and physiological functions. Previous research has reported abnormalities in membrane phospholipids in patients with Alzheimer’s disease (AD) (Nitsch et al., 1992). Mapstone et al. (2014) found significantly lower plasma phosphatidylcholine (PC) levels in subjects with cognitive impairment compared to controls, a finding that is consistent with our results. This could be attributed to the physiological function of phosphatidylcholine (PC), which encompasses regulating glucose and lipoprotein homeostasis, in addition to serving as a constituent part of cell membranes (Vance, 2008; Furse and de Kroon, 2015). In a prospective study involving 2,497 participants with a follow-up period exceeding 2 years, Ylilauri et al. (2019) found that higher dietary intake of phosphatidylcholine (PC) was associated with a lower risk of dementia and improved cognitive performance. Therefore, patients with type 2 diabetes mellitus and mild cognitive impairment (T2DM-MCI) may mitigate the progression of cognitive impairment by consuming foods rich in phosphatidylcholine (PC).
LPC levels are significantly reduced in schizophrenia patients compared to healthy controls, indicating a correlation between LPC levels and cognitive function (Orešič et al., 2012). Mapstone et al. (2014) reported a transition from normal cognition to MCI among subjects with depleted plasma LPC levels compared to controls with cognitive impairment. LPC serves as the primary carrier of docosahexaenoic acid (DHA) across the blood-brain barrier, supporting brain function through its multiple biological effects (Lagarde et al., 2001). LPC has also been implicated in demyelination, inflammatory responses, atherosclerosis, and other detrimental biological effects on cognitive function, contrary to previous evidence (Song et al., 2021).
We observed a downregulation of SM in the T2DM-MCI group in our study. Consistent with our findings, a study demonstrated significantly lower plasma SM levels in AD patients compared to controls (Han et al., 2011). Conversely, other studies have found that elevated SM levels are associated with the severity of AD pathology at autopsy and its progression in prodromal and preclinical stages (Varma et al., 2018). Mielke et al. (2010) conducted a study among elderly women, revealing that serum SM levels fluctuate depending on the timing of memory impairment episodes, with low levels associated with memory impairment and high levels predictive of future memory impairment up to 9 years later. This indicates that serum SM may serve as a reliable preclinical predictor or biomarker for memory impairment (Mielke et al., 2010). Further investigation into the relationship between SM and cognition across various cognitive function stages and different populations is essential.
The metabolism of fatty acids is significantly disrupted in T2DM-MCI. Fatty acids undergo catabolism for energy production through fatty acid β-oxidation. In our research, the serum levels of FFA were decreased in T2DM-MCI patients. Previous studies have consistently demonstrated lower FFA levels in AD patients compared to controls, encompassing various saturated and unsaturated fatty acids, such as FFA 16:0 and FFA 18:0. However, elevated levels of FFA 18:3 were observed, aligning with our results. It is important to note that the impact of different types of FFA on cognition may differ. Unsaturated fatty acids have been shown to preserve cell membrane fluidity, suppress inflammatory processes, enhance vascular endothelial cell function, inhibit platelet aggregation, and regulate lipid metabolism (Wiktorowska-Owczarek et al., 2015).
This study suggests that T2DM patients with low education level, history of insulin application, high insulin resistance, low serum IGFBP-3, and low creatinine values are more susceptible to MCI. Shorter duration of education and low serum IGFBP-3 levels are independent risk factors for T2DM-MCI. There are significant differences in serum metabolites between T2DM-MCI and T2DM-NCI. Abnormal lipid metabolism plays a important role in the development of cognitive impairment in T2DM patients. LPC 18:0 can effectively differentiate T2DM-MCI and T2DM-NCI. This study aims to identify characteristic biomarkers of MCI in patients with T2DM, thereby providing new insights for the effective intervention and treatment of cognitive impairment in this population in the future.
Although this study reports novel findings, it has several limitations. Firstly, our study is a cross-sectional study with a small sample size and relatively limited results, which reduce the ability to detect risk factors for T2DM-MCI, and further validation is necessary. Secondly, predictive signatures may vary among different studies due to differences in the genetic and environmental background of the study population. Therefore, we plan to further expand the sample size in future studies and conduct additional research to validate the identified biomarkers.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
The studies involving humans were approved by the Ethics Committee of The Second Affiliated Hospital of Dalian Medical University. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
TL: Data curation, Investigation, Methodology, Software, Writing–original draft. XJ: Data curation, Investigation, Software, Writing–original draft. NX: Data curation, Investigation, Writing–review and editing. XZ: Investigation, Validation, Writing–review and editing. XnX: Investigation, Writing–review and editing. XuX: Data curation, Writing–review and editing. XB: Data curation, Writing–review and editing. HL: Funding acquisition, Project administration, Resources, Supervision, Writing–review and editing.
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This study was supported by the following grants: the “Xingliao Talent Plan” of Liaoning, China (YXMJ-QN-05), Dalian Science and Technology Innovation Fund, Dalian Science and Technology Bureau (2022JJ12SN048), “1 + X” program for Clinical Competency enhancement–Clinical Research Incubation Project, The Second Hospital of Dalian Medical University (2022LCYJZD03).
Thanks for the approval of The Second Affiliated Hospital of Dalian Medical University. Thanks for the support of the Dalian Institute of Chemical Physics, Chinese Academy of Sciences.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmolb.2024.1341290/full#supplementary-material
Albert, M. S., DeKosky, S. T., Dickson, D., Dubois, B., Feldman, H. H., Fox, N. C., et al. (2011). The diagnosis of mild cognitive impairment due to Alzheimer's disease: recommendations from the National Institute on Aging-Alzheimer's Association workgroups on diagnostic guidelines for Alzheimer's disease. Alzheimer's dementia J. Alzheimer's Assoc. 7 (3), 270–279. doi:10.1016/j.jalz.2011.03.008
American Diabetes Association Professional Practice Committee (2022). 2. Classification and diagnosis of diabetes: standards of medical care in diabetes-2022. Diabetes care 45 (Suppl. 1), S17–S38. doi:10.2337/dc22-S002
Chen, R., Zeng, Y., Xiao, W., Zhang, L., and Shu, Y. (2021). LC-MS-Based untargeted metabolomics reveals early biomarkers in STZ-induced diabetic rats with cognitive impairment. Front. Endocrinol. 12, 665309. doi:10.3389/fendo.2021.665309
Duron, E., Funalot, B., Brunel, N., Coste, J., Quinquis, L., Viollet, C., et al. (2012). Insulin-like growth factor-I and insulin-like growth factor binding protein-3 in Alzheimer's disease. J. Clin. Endocrinol. metabolism 97 (12), 4673–4681. doi:10.1210/jc.2012-2063
Exalto, L. G., Biessels, G. J., Karter, A. J., Huang, E. S., Katon, W. J., Minkoff, J. R., et al. (2013). Risk score for prediction of 10 year dementia risk in individuals with type 2 diabetes: a cohort study. lancet. Diabetes and Endocrinol. 1 (3), 183–190. doi:10.1016/S2213-8587(13)70048-2
Furse, S., and de Kroon, A. I. (2015). Phosphatidylcholine's functions beyond that of a membrane brick. Mol. Membr. Biol. 32 (4), 117–119. doi:10.3109/09687688.2015.1066894
Gorska-Ciebiada, M., Saryusz-Wolska, M., Borkowska, A., Ciebiada, M., and Loba, J. (2016). Adiponectin, leptin and IL-1 β in elderly diabetic patients with mild cognitive impairment. Metab. brain Dis. 31 (2), 257–266. doi:10.1007/s11011-015-9739-0
Han, X., Rozen, S., Boyle, S. H., Hellegers, C., Cheng, H., Burke, J. R., et al. (2011). Metabolomics in early Alzheimer's disease: identification of altered plasma sphingolipidome using shotgun lipidomics. PloS one 6 (7), e21643. doi:10.1371/journal.pone.0021643
Harding, J. L., Pavkov, M. E., Magliano, D. J., Shaw, J. E., and Gregg, E. W. (2019). Global trends in diabetes complications: a review of current evidence. Diabetologia 62 (1), 3–16. doi:10.1007/s00125-018-4711-2
Izzo, A., Massimino, E., Riccardi, G., and Della Pepa, G. (2021). A narrative review on sarcopenia in type 2 diabetes mellitus: prevalence and associated factors. Nutrients 13 (1), 183. doi:10.3390/nu13010183
Kellar, D., and Craft, S. (2020). Brain insulin resistance in Alzheimer's disease and related disorders: mechanisms and therapeutic approaches. Lancet. Neurology 19 (9), 758–766. doi:10.1016/S1474-4422(20)30231-3
Kong, S. H., Park, Y. J., Lee, J. Y., Cho, N. H., and Moon, M. K. (2018). Insulin resistance is associated with cognitive decline among older Koreans with normal baseline cognitive function: a prospective community-based cohort study. Sci. Rep. 8 (1), 650. doi:10.1038/s41598-017-18998-0
Lagarde, M., Bernoud, N., Brossard, N., Lemaitre-Delaunay, D., Thiès, F., Croset, M., et al. (2001). Lysophosphatidylcholine as a preferred carrier form of docosahexaenoic acid to the brain. J. Mol. Neurosci. MN 16 (2-3), 201–204. doi:10.1385/JMN:16:2-3:201
Mapstone, M., Cheema, A. K., Fiandaca, M. S., Zhong, X., Mhyre, T. R., MacArthur, L. H., et al. (2014). Plasma phospholipids identify antecedent memory impairment in older adults. Nat. Med. 20 (4), 415–418. doi:10.1038/nm.3466
Mielke, M. M., Bandaru, V. V., Haughey, N. J., Rabins, P. V., Lyketsos, C. G., and Carlson, M. C. (2010). Serum sphingomyelins and ceramides are early predictors of memory impairment. Neurobiol. aging 31 (1), 17–24. doi:10.1016/j.neurobiolaging.2008.03.011
Nilsson, M., Jensen, N., Gejl, M., Bergmann, M. L., Storgaard, H., Zander, M., et al. (2019). Experimental non-severe hypoglycaemia substantially impairs cognitive function in type 2 diabetes: a randomised crossover trial. Diabetologia 62 (10), 1948–1958. doi:10.1007/s00125-019-4964-4
Nitsch, R. M., Blusztajn, J. K., Pittas, A. G., Slack, B. E., Growdon, J. H., and Wurtman, R. J. (1992). Evidence for a membrane defect in Alzheimer disease brain. Proc. Natl. Acad. Sci. U. S. A. 89 (5), 1671–1675. doi:10.1073/pnas.89.5.1671
Orešič, M., Seppänen-Laakso, T., Sun, D., Tang, J., Therman, S., Viehman, R., et al. (2012). Phospholipids and insulin resistance in psychosis: a lipidomics study of twin pairs discordant for schizophrenia. Genome Med. 4 (1), 1. doi:10.1186/gm300
Pal, K., Mukadam, N., Petersen, I., and Cooper, C. (2018). Mild cognitive impairment and progression to dementia in people with diabetes, prediabetes and metabolic syndrome: a systematic review and meta-analysis. Soc. psychiatry psychiatric Epidemiol. 53 (11), 1149–1160. doi:10.1007/s00127-018-1581-3
Qiu, W. Q., and Folstein, M. F. (2006). Insulin, insulin-degrading enzyme and amyloid-beta peptide in Alzheimer's disease: review and hypothesis. Neurobiol. aging 27 (2), 190–198. doi:10.1016/j.neurobiolaging.2005.01.004
Rawson, E. S., and Venezia, A. C. (2011). Use of creatine in the elderly and evidence for effects on cognitive function in young and old. Amino acids 40 (5), 1349–1362. doi:10.1007/s00726-011-0855-9
Simó, R., Ciudin, A., Simó-Servat, O., and Hernández, C. (2017). Cognitive impairment and dementia: a new emerging complication of type 2 diabetes-The diabetologist's perspective. Acta diabetol. 54 (5), 417–424. doi:10.1007/s00592-017-0970-5
Song, L., Zhuang, P., Lin, M., Kang, M., Liu, H., Zhang, Y., et al. (2017). Urine metabonomics reveals early biomarkers in diabetic cognitive dysfunction. J. proteome Res. 16 (9), 3180–3189. doi:10.1021/acs.jproteome.7b00168
Song, M. H., Gupta, A., Kim, H. O., and Oh, K. (2021). Lysophosphatidylcholine aggravates contact hypersensitivity by promoting neutrophil infiltration and IL17 expression. BMB Rep. 54 (4), 203–208. doi:10.5483/BMBRep.2021.54.4.193
Srikanth, V., Sinclair, A. J., Hill-Briggs, F., Moran, C., and Biessels, G. J. (2020). Type 2 diabetes and cognitive dysfunction-towards effective management of both comorbidities. lancet. Diabetes and Endocrinol. 8 (6), 535–545. doi:10.1016/S2213-8587(20)30118-2
Suain Bon, R., Ariaratnam, S., Mat Saher, Z., Mohamad, M., and Lee, F. S. (2021). Cognitive impairment and its associated risk factors in the elderly with type 2 diabetes mellitus. Front. psychiatry 12, 669725. doi:10.3389/fpsyt.2021.669725
Sui, S. X., Williams, L. J., Holloway-Kew, K. L., Hyde, N. K., and Pasco, J. A. (2020). Skeletal muscle health and cognitive function: a narrative review. Int. J. Mol. Sci. 22 (1), 255. doi:10.3390/ijms22010255
Sun, H., Saeedi, P., Karuranga, S., Pinkepank, M., Ogurtsova, K., Duncan, B. B., et al. (2022). IDF Diabetes Atlas: global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Res. Clin. Pract. 183, 109119. doi:10.1016/j.diabres.2021.109119
Sun, L., Diao, X., Gang, X., Lv, Y., Zhao, X., Yang, S., et al. (2020). Risk factors for cognitive impairment in patients with type 2 diabetes. J. diabetes Res. 2020, 4591938. doi:10.1155/2020/4591938
Takahashi, R. H., Nagao, T., and Gouras, G. K. (2017). Plaque formation and the intraneuronal accumulation of β-amyloid in Alzheimer's disease. Pathol. Int. 67 (4), 185–193. doi:10.1111/pin.12520
Umpierrez, G., and Korytkowski, M. (2016). Diabetic emergencies - ketoacidosis, hyperglycaemic hyperosmolar state and hypoglycaemia. Nat. Rev. Endocrinol. 12 (4), 222–232. doi:10.1038/nrendo.2016.15
Vance, D. E. (2008). Role of phosphatidylcholine biosynthesis in the regulation of lipoprotein homeostasis. Curr. Opin. Lipidol. 19 (3), 229–234. doi:10.1097/MOL.0b013e3282fee935
Varma, V. R., Oommen, A. M., Varma, S., Casanova, R., An, Y., Andrews, R. M., et al. (2018). Brain and blood metabolite signatures of pathology and progression in Alzheimer disease: a targeted metabolomics study. PLoS Med. 15 (1), e1002482. doi:10.1371/journal.pmed.1002482
Wennberg, A. M. V., Hagen, C. E., Machulda, M. M., Hollman, J. H., Roberts, R. O., Knopman, D. S., et al. (2018). The association between peripheral total IGF-1, IGFBP-3, and IGF-1/IGFBP-3 and functional and cognitive outcomes in the Mayo Clinic Study of Aging. Neurobiol. aging 66, 68–74. doi:10.1016/j.neurobiolaging.2017.11.017
Wiktorowska-Owczarek, A., Berezińska, M., and Nowak, J. Z. (2015). PUFAs: structures, metabolism and functions. Adv. Clin. Exp. Med. official organ Wroclaw Med. Univ. 24 (6), 931–941. doi:10.17219/acem/31243
Workgroup on Hypoglycemia, American Diabetes Association (2005). Defining and reporting hypoglycemia in diabetes: a report from the American diabetes association workgroup on hypoglycemia. Diabetes care 28 (5), 1245–1249. doi:10.2337/diacare.28.5.1245
Xia, S. S., Xia, W. L., Huang, J. J., Zou, H. J., Tao, J., and Yang, Y. (2020). The factors contributing to cognitive dysfunction in type 2 diabetic patients. Ann. Transl. Med. 8 (4), 104. doi:10.21037/atm.2019.12.113
Xu, W., Hu, X., Zhang, X., Ling, C., Wang, C., and Gao, L. (2021). Cognitive impairment and related factors among middle-aged and elderly patients with type 2 diabetes from a bio-psycho-social perspective. Diabetes, metabolic syndrome Obes. targets Ther. 14, 4361–4369. doi:10.2147/DMSO.S333373
Xue, M., Xu, W., Ou, Y. N., Cao, X. P., Tan, M. S., Tan, L., et al. (2019). Diabetes mellitus and risks of cognitive impairment and dementia: a systematic review and meta-analysis of 144 prospective studies. Ageing Res. Rev. 55, 100944. doi:10.1016/j.arr.2019.100944
Ye, M., Yuan, A. H., Yang, Q. Q., Li, Q. W., Li, F. Y., and Wei, Y. (2024). Association of hypoglycemic events with cognitive impairment in patients with type 2 diabetes mellitus: protocol for a dose-response meta-analysis. PloS one 19 (2), e0296662. doi:10.1371/journal.pone.0296662
Ylilauri, M. P. T., Voutilainen, S., Lönnroos, E., Virtanen, H. E. K., Tuomainen, T. P., Salonen, J. T., et al. (2019). Associations of dietary choline intake with risk of incident dementia and with cognitive performance: the Kuopio Ischaemic Heart Disease Risk Factor Study. Am. J. Clin. Nutr. 110 (6), 1416–1423. doi:10.1093/ajcn/nqz148
You, Y., Liu, Z., Chen, Y., Xu, Y., Qin, J., Guo, S., et al. (2021). The prevalence of mild cognitive impairment in type 2 diabetes mellitus patients: a systematic review and meta-analysis. Acta diabetol. 58 (6), 671–685. doi:10.1007/s00592-020-01648-9
Zhang, J. B., Cong, Y. N., Li, Z. G., Sun, H. R., Zhang, J. S., Wang, P. F., et al. (2017). Plasma phospholipids are associated with mild cognitive impairment in type 2 diabetic patients. Curr. Alzheimer Res. 14 (6), 592–597. doi:10.2174/1567205013666161201200722
Zhao, L., Dong, M., Ren, M., Li, C., Zheng, H., and Gao, H. (2018). Metabolomic analysis identifies lactate as an important pathogenic factor in diabetes-associated cognitive decline rats. Mol. Cell. proteomics MCP 17 (12), 2335–2346. doi:10.1074/mcp.RA118.000690
Keywords: type 2 diabetes mellitus, mild cognitive impairment, risk factors, metabolomics, LPC
Citation: Luo T, Jiang X, Xu N, Zhao X, Xie X, Xia X, Bian X and Liu H (2024) Risk factors and metabolomics of mild cognitive impairment in type 2 diabetes mellitus. Front. Mol. Biosci. 11:1341290. doi: 10.3389/fmolb.2024.1341290
Received: 20 November 2023; Accepted: 08 April 2024;
Published: 18 April 2024.
Edited by:
Chongbo Yang, Cornell University, United StatesReviewed by:
Shuhang Xu, Nanjing University of Chinese Medicine, ChinaCopyright © 2024 Luo, Jiang, Xu, Zhao, Xie, Xia, Bian and Liu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Haixia Liu, ZGxsaHgxMDE3QDE2My5jb20=
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.