
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Mol. Biosci. , 07 May 2021
Sec. Molecular Diagnostics and Therapeutics
Volume 8 - 2021 | https://doi.org/10.3389/fmolb.2021.643824
This article is part of the Research Topic Molecular Targeted Therapy in Oncology: Lessons from Pharmacogenetics and Pharmacoepigenetics View all 12 articles
 Jacopo Junio Valerio Branca1
Jacopo Junio Valerio Branca1 Donatello Carrino1Massimo Gulisano1
Donatello Carrino1Massimo Gulisano1 Carla Ghelardini2
Carla Ghelardini2 Lorenzo Di Cesare Mannelli2†
Lorenzo Di Cesare Mannelli2† Alessandra Pacini1*†
Alessandra Pacini1*†In the most recent decades, oxaliplatin has been used as a chemotherapeutic agent for colorectal cancer and other malignancies as well. Oxaliplatin interferes with tumor growth predominantly exerting its action in DNA synthesis inhibition by the formation of DNA-platinum adducts that, in turn, leads to cancer cell death. On the other hand, unfortunately, this interaction leads to a plethora of systemic side effects, including those affecting the peripheral and central nervous system. Oxaliplatin therapy has been associated with acute and chronic neuropathic pain that induces physicians to reduce the dose of medication or discontinue treatment. Recently, the capability of oxaliplatin to alter the genetic and epigenetic profiles of the nervous cells has been documented, and the understanding of gene expression and transcriptional changes may help to find new putative treatments for neuropathy. The present article is aimed to review the effects of oxaliplatin on genetic and epigenetic mechanisms to better understand how to ameliorate neuropathic pain in order to enhance the anti-cancer potential and improve patients’ quality of life.
In the last decades, despite early cancer diagnosis, cancer deaths rapidly increased (Kanavos, 2006). Among the most common cancer types, colorectal cancer is one of the most diffuse cancer in both genders worldwide. Indeed, it has been recently reported that more than 1.8 million new cases and about 0.9 million deaths were estimated in 2018, ranking the colorectal cancer third in terms of incidence and second in terms of mortality in both male and female (Bray et al., 2018). Therefore, the researchers are making great efforts in order to counteract this debilitating and mortal health concern.
The platinum-derived drugs are widely used as chemotherapeutic agents and, among these compounds, cisplatin was the first one patented (Rosenberg et al., 1969). However, the poor effects of cisplatin against different cancer types (Taylor and Filby, 2017), its side effects (Lokich, 2001), and the cancer resistance (Stordal and Davey, 2007) limited its use in chemotherapy leading physicians and researchers to explore new paths in order to improve the quality of life of patients.
Within this framework, new platinum analogs have been developed. Although other new platinum-derived drugs are under study (Johnstone et al., 2016; Dai and Wang, 2020), nowadays, carboplatin and oxaliplatin are the most widely used in clinical practice (Fischer and Ganellin, 2006).
Oxaliplatin, a third generation 1,2-diaminocyclohexane platinum compound patented in 1976, shows high efficacy against colorectal cancer (Wiseman et al., 1999). Recently, its efficacy has been found also in other cancer types including lung (Raez et al., 2010), gastric (Cunningham, 2006; Zhang et al., 2019), ovarian, and prostate cancer (Zhou et al., 2017).
The primary anti-cancer effect exerted by oxaliplatin therapy, as well as for the other platinum-derived drugs, is due to DNA damage. Indeed, it has been largely demonstrated that oxaliplatin forms intra-strand crosslinks with DNA, as the main mechanism for the induction of DNA lesions, inhibiting the proliferation of neoplastic cells (Culy et al., 2000). Furthermore, another intriguing anti-cancer effect of oxaliplatin was discovered by Tesniere and colleagues, demonstrating that oxaliplatin-treated CT26 colorectal cancer cells were able to release immunogenic signals that trigger an immune response, thus leading to an enhanced anti-cancer effect promoted by the immune system (Tesniere et al., 2010).
With respect to oxaliplatin pharmacokinetics, it has been reported that the platinum compound can interact with and bind to plasma proteins. In patients affected by cancer, the platinum-plasma protein binding increased around 70% after 2 h of infusion, growing up to 95% 5 days after infusion. However, it can be considered that the maximum platinum concentration is achieved during the first cycle of oxaliplatin administration and no accumulation was reported after single or multiple doses, except for erythrocytes where an accumulation has been found (Culy et al., 2000; Lévi et al., 2000). On the other hand, the main excretion of platinum products occurs mainly by the renal route, consisting in about 50% after 72 h, whereas the excretion by defecation is very low, ranging about 2% after 5 days (Culy et al., 2000).
However, even if the antineoplastic efficacy of oxaliplatin is overt, it also unfortunately generates a series of undesired side effects.
Among the DNA-interfering chemotherapeutic agents, platinum-derived drugs can potentially interact with normal cells with high proliferating turnover, thus altering their physiological features and leading to adverse side effects (Oun et al., 2018).
Over the years, many researchers have highlighted the deleterious events in different organs and tissues resulting from oxaliplatin treatment. For instance, it has been shown that oxaliplatin exhibits irritant properties that may lead to the occurrence of vesicant lesions (Foo et al., 2003; Kennedy et al., 2003; Kretzschmar et al., 2003).
In contrast to cisplatin, oxaliplatin is not nephrotoxic or ototoxic, but it produces various adverse effects, the main one is neurotoxicity. Oxaliplatin-dependent neurotoxicity can be acute and/or chronic, but both types give rise to neuropathic pain (Sałat, 2020). The acute type elicits a transient neuropathy that occurs in 90% of patients within a few hours of chemotherapy administration, lasts for a few days, and recurs with subsequent administrations. The main signs and symptoms of acute neuropathy are exacerbated by cold and consist of dysesthesia and paresthesia of the hands and feet. Motor symptoms may also occur, such as tetanic spasms, fasciculations, and prolonged muscular contractions. It has been demonstrated that acute neuropathy is caused by a Nav channel activation that transiently induces nerve hyperexcitability (Gebremedhn et al., 2018). In 70% of cases, prolonged exposure to oxaliplatin induces a severe chronic peripheral neuropathy, with symptoms very similar to those of acute form that force patients to discontinue the treatment (Miaskowski et al., 2017). Among all, the most relevant mechanism that trigger neuropathic pain (extensively reviewed by Kanat et al., 2017), is the binding of oxaliplatin to the mitochondrial DNA of sensory neurons, thus causing their death. This oxaliplatin-dependent neuronal loss also accounts for the persistence of symptoms for up to years following treatment discontinuation (Kokotis et al., 2016). The loss of sensory neurons is further confirmed by alterations in taste and smell frequently observed in patients who underwent oxaliplatin treatment (reviewed in Gamper et al., 2012). Other relevant side effects consist of fever (Saif, 2007), thrombocytopenia (Jardim et al., 2012), anemia (Cobo et al., 2007), nausea (Fleishman et al., 2012), liver function abnormalities (Lu et al., 2019), and gastro-intestinal dysfunction (Boussios et al., 2012).
This latter side effects, such as diarrhea or constipation, might be ascribed to enteric neuronal loss. In this regard, McQuade and colleagues demonstrated that the use of antioxidant molecules, such as the novel BPF-15, ameliorated the oxidative stress-dependent gastrointestinal symptoms (McQuade et al., 2016, 2018). Also, oxaliplatin can induce cognitive impairment. This debilitating condition was observed in a rat model (Fardell et al., 2012) and in patients who experienced an oxaliplatin-dependent impairment of verbal memory (Cruzado et al., 2014).
Another side effect of oxaliplatin treatment was observed by Okamoto in a Japanese patient who reported the Lhermitte’s sign, a sudden sensation resembling an electric shock that passes down the back of the neck and into the spine and may then radiate out into the arms and legs. This symptom mainly occurs in multiple sclerosis and is believed to be due to a demyelination of the posterior columns of the spinal cord induced by chemotherapy (Okamoto et al., 2020).
Finally, in a very recent study a high increase of serum neurofilament light chain level was observed in patients who referred an oxaliplatin-dependent neuropathic pain. The serological increase of neurofilament light chain has been previously reported in patient with Alzheimer’s disease, frontotemporal dementia, and multiple sclerosis. However, even if the authors concluded that a major part of the serum neurofilament light chain originates from the peripheral nervous system, it is not excluded that something has happened in the CNS, but more insights are needed (Kim et al., 2020).
Many authors have underlined the main effects exerted by oxaliplatin (Table 1) and have evidenced that one of the main causes of the neuropathy onset is its accumulation inside the cells. Within the nervous system, oxaliplatin preferentially accumulates in those cells that express specific membrane transporters such as the multidrug and toxin extrusion proteins (MATEs), the organic anion-transporting polypeptides (OATPs), and the organic cation transporter (OCT) (Huang et al., 2020). The expression of OCT-type transporters by sensory neurons of the dorsal root ganglia (DRG) (Fujita et al., 2019) not only demonstrates the accumulation of the chemotherapy mainly in these cell type, but also that this event could trigger a peripheral neurotoxicity. These data were corroborated by other results demonstrating the oxaliplatin-dependent detrimental effect on DRG neurons causing a reduced volume of the neuronal soma and an increase in the number of multinucleated neuronal nuclei (Di Cesare Mannelli et al., 2017).
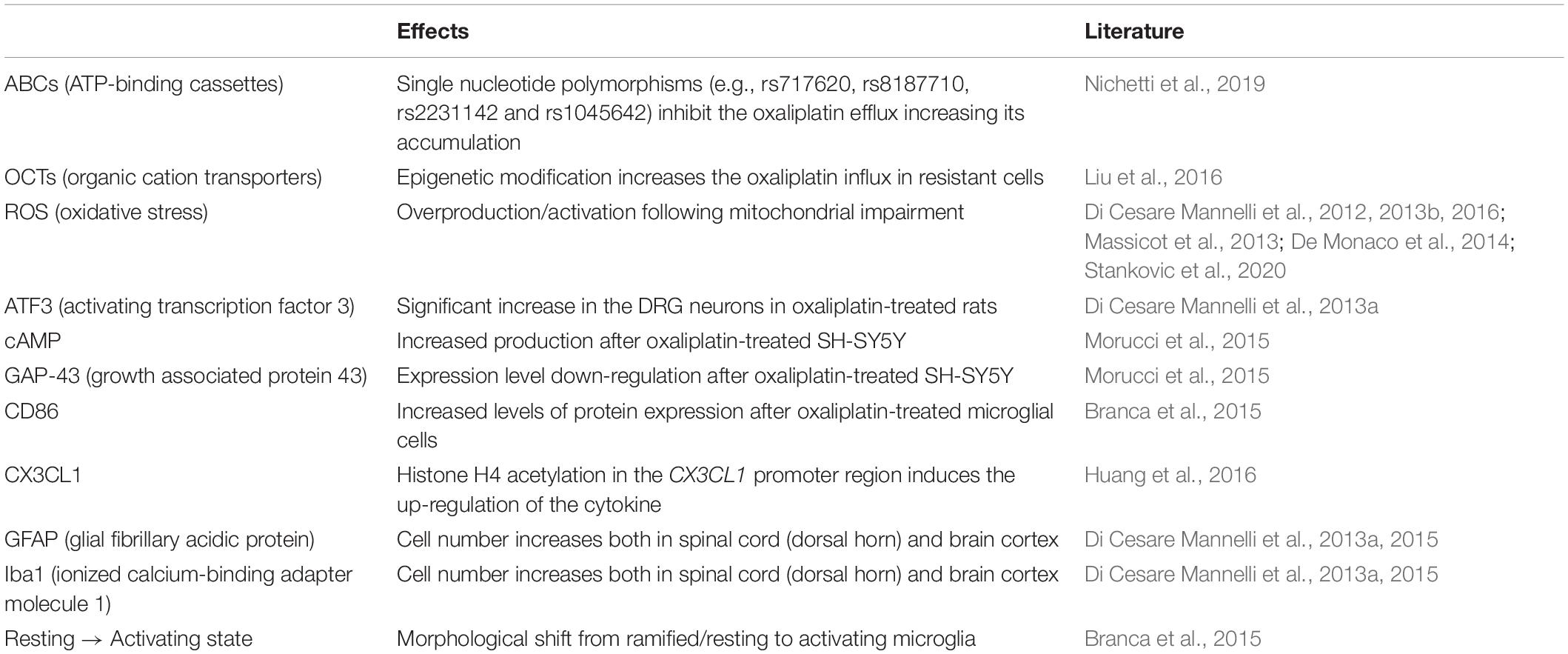
Table 1. Main signaling pathways involved in oxaliplatin-dependent alterations.
The OCT transporter is also expressed on the luminal surface of the blood-brain barrier (BBB) micro-vessel endothelial cells, the OCT role in transporting oxaliplatin inside the cells has been demonstrated (Lin et al., 2010). In this regard, recently it has been reported that in a rat brain endothelial cell line expressing OCT protein (Friedrich et al., 2003), oxaliplatin elicits a dislocation of the Zonula Occludens-1 (ZO-1), one of the tight junction proteins that contribute to constitute the BBB (Branca et al., 2018). The increased permeability of the BBB allows the chemotherapy agent to enter the brain parenchyma, affecting both the neuronal (Park et al., 2009) and glial compartment (Lee and Kim, 2020).
As for the effects of oxaliplatin on neurons, an increase in oxidative stress is the most remarkable event. In vitro experiments have demonstrated that oxaliplatin is able to increase the reactive oxygen species (ROS) and the superoxide anion levels as well as protein carbonylation (Di Cesare Mannelli et al., 2013b), thus suggesting that oxidative stress could be responsible for oxaliplatin-induced neuropathic pain.
In vivo analysis carried out on plasma, sciatic nerves, and lumbar portion of the spinal cord obtained from oxaliplatin-treated rats strengthened the role of oxidative stress in the onset of neuropathic pain (Di Cesare Mannelli et al., 2012).
Analysis of the signaling pathway that triggers neuropathy highlighted the involvement of activating transcription factor 3 (ATF3) protein. This protein is a member of the cAMP-responsive element binding protein family (Li et al., 2019) that, following the activation of the Toll Like receptors (TLRs), regulates a signaling cascade involved in the onset of neuropathy. Also, its expression has been found significatively increased in oxaliplatin-treated nerves and DRGs (Di Cesare Mannelli et al., 2013a) that should be achieved by cAMP-increased levels, as reported by in vitro analysis on oxaliplatin-treated neuronal cells (Morucci et al., 2015). Moreover, an oxaliplatin-dependent alteration of the cell viability and of the expression of the growth associated protein 43 (GAP-43), a well-known marker of axon development (Morucci et al., 2015), was also reported.
With respect to the glial compartment, neuropathic pain has been linked to changes in the gene expression and secretory profile of microglia that elicits a signaling cascade resulting in neuroinflammation (Ji et al., 2016).
As demonstrated by in vitro analysis both in human and murine cells, oxaliplatin induced an increase in pro-inflammatory marker expression such as clusters of differentiation 86 (CD86), and morphological changes shifting from resting to activating shape (Branca et al., 2015). These effects are in accordance with ex vivo experiments carried out in oxaliplatin-treated rats, showing an increase in the number of cells expressing the microglial marker Iba-1 (ionized calcium-binding adapter molecule 1) in the spinal cord as well as in the basal ganglia and “pain matrix” brain areas (Di Cesare Mannelli et al., 2013a).
The onset of microglia-dependent neuroinflammation also induces the recruitment of astrocytes. Indeed, it has been demonstrated that oxaliplatin treatment causes an increase in the expression levels of glial fibrillary acidic protein (GFAP) and a modification of astrocytic shape, both in the spinal cord and in some brain areas (Di Cesare Mannelli et al., 2015).
Microglia and astrocyte activation is strictly related to pain sensitivity since the selective inhibition of one or the other cellular type prevented pain development (Di Cesare Mannelli et al., 2014). On the other hand, an indiscriminate glial cell silencing impaired the neurorestorative mechanisms promoted by these cell types (Di Cesare Mannelli et al., 2014).
Another important target of oxaliplatin-dependent toxicity is the mitochondrion whose dysfunction leads to the generation of reactive oxygen species (ROS). Although the research on the mechanisms underlying mitochondrial toxicity and ROS generation are only beginning to be analyzed, some studies have fully demonstrated that the antioxidant properties of different molecules are able to mitigate the oxaliplatin-dependent neuropathy (Di Cesare Mannelli et al., 2016). These results suggest that ROS generation and mitochondrial impairment are early events in the oxaliplatin-triggered signaling pathway that results in the onset of neuropathy.
Over the last 10 years research has highlighted a very important role of epigenetics in determining variations that induce lasting or permanent changes in neuronal function (Borrelli et al., 2008). Also, it is now evident that drug exposure leads to epigenomic changes that are the basis of the different individual responses to chemotherapy. Indeed, the focus is now centered on improving the chemotherapeutic efficacy of anticancer molecules through pharmacogenetic and pharmacoepigenetic approaches (Mohelnikova-Duchonova, 2014).
Pharmacogenetics, recently changed to the term pharmacogenomics, is the field of research that encompasses all genes in the genome that may determine drug response (Pirmohamed, 2001). Indeed, especially for what may concern drug resistance and chemotherapy, the study of genetic polymorphisms is essential to choose the optimal personalized therapeutic treatment, minimizing the side effects produced by chemotherapy (Lesko, 2007). On the other hand, epigenetic modifications can influence the drug response and a decisive role in personalized medicine is assigned to pharmacoepigenetics (Majchrzak-Celińska, 2017).
In view of these fascinating scenarios, it has been recently hypothesized that the pivotal role of single nucleotide polymorphisms (SNPs) affects the gene coding for oxaliplatin transporters. The alteration of the expression levels and the functioning of these transporters, in particular, the SNPs occurring in ATP-binding cassette (ABCs) transporters (such as rs717620, rs8187710, rs2231142, and rs1045642), causes an increase in the oxaliplatin concentration inside the cells (in particular, the DRG neurons) that may account for an higher risk to develop an oxaliplatin-dependent neuropathy as previously reported (Nichetti et al., 2019).
It has been reported that a prolonged and high oxaliplatin intracellular accumulation, induced ROS overproduction mediated by mitochondrial impairment (Massicot et al., 2013). Thus, even if specific transporter polymorphisms are not beneficial for patients that unfortunately do not correctly excrete oxaliplatin leading to its accumulation, the simultaneous use of antioxidant molecules during a chemotherapy regimen could help to retrieve and ameliorate the oxaliplatin-induced neuropathic pain (De Monaco et al., 2014; Stankovic et al., 2020).
However, there are many other elements that influence chemotherapeutic drug sensitivity, such as the glutathione S transferase P1 (GSTP1), involved in the inactivation of platinum-DNA adducts (Kweekel et al., 2005). For example, the 105Val allele variant at exon 5 of the GSTP1 gene confers a significantly decreased risk of developing severe oxaliplatin-related neuropathy (Lecomte et al., 2006; Chen et al., 2010, p. 201; McLeod et al., 2010; Hong et al., 2011).
Moreover, genetic polymorphisms play a key role also in adjuvant therapies where opioid drugs are used in order to ameliorate oxaliplatin-induced neuropathic pain (Wang, 2014).
Despite a clear correlation between oxaliplatin-based neuropathy and individual genetic polymorphisms, pharmacotherapy based on genetic profile is not yet routinely introduced, perhaps because different polymorphisms can correlate and a wide range of genomic analysis in a larger population is needed (Peng et al., 2013; Ruzzo et al., 2015).
In the attempt to find the molecular basis for neuropathy induction and maintenance, attention has recently been turned to epigenetic mechanisms. Epigenetic-dependent alterations of gene expression are independent of DNA sequence alterations, but they are heritable and reversible. Recently, environmental stimuli have been observed to induce long-term epigenetic modifications of the gene expression profile that characterizes neuropathic pain (extensively reviewed by Penas and Navarro, 2018).
If SNPs represent a risk of developing neuropathy, epigenetic regulation of the ABC transporters expression levels may lead to a decreased risk. Indeed, these transporters regulate the oxaliplatin efflux from cells (Sparreboom et al., 2003), thus reducing its accumulation (Huo et al., 2010).
A similar fascinating result in this field was obtained by the epigenetic modification of the OCT2 transporter both in vitro and in xenografts. Some authors have promoted the epigenetic expression of this oxaliplatin transporter in renal cancer cells in order to increase the oxaliplatin sensitization of these cells (Liu et al., 2016). It could be argued that the OCT2 epigenetic modification could induce an oxaliplatin accumulation also into other cell compartments, including the brain, thus leading to the induction of neuropathy.
Epigenetic modifications of glial cells have also been shown to play a role in neuropathic pain. Astrocytic DNA methylation and histone modifications, two of the major epigenetic modifications, induce the production of pro-inflammatory cytokines triggering a microglia neuroinflammatory activation that, in turn, contributes to the development of neuropathy (McMahon et al., 2005; Descalzi et al., 2015; Machelska and Celik, 2016).
It has also been demonstrated that oxaliplatin treatment significantly increased the histone H4 acetylation in the CX3CL1 promoter region in spinal cord neurons (Huang et al., 2016), inducing the up-regulation of this cytokine. In vivo studies have demonstrated involvement in the induction of central sensitization and acute pain behavior after oxaliplatin administration (Huang et al., 2016; Zhang et al., 2018). More recently, it has been evidenced that oxaliplatin treatment is able to increase the expression of 10–11 translocation methylcytosine dioxygenase 1 (TET1), a well-known enzyme involved in DNA demethylation. The researchers found that TET1 up-regulation indirectly acts on Homeobox A6 protein (HOX-A6) expression in neurons, thus becoming a pivotal target in ameliorating oxaliplatin-induced neuropathy (Deng et al., 2020).
The oxaliplatin-induced neuropathic pain is a deleterious side effect for patient healthcare that could lead to therapy interruption. In recent years many efforts have been made in order to both increase the oxaliplatin anti-cancer effects and ameliorate neuropathy. Hopefully, genetic and epigenetic information can help physicians toward a personalized therapeutic strategy. However, many other analyses of pharmacogenetics and epigenetics should be performed in order to corroborate and obtain useful data to seriously improve the benefit from chemotherapeutic treatment.
JB, LD, and AP conceived the structure of the manuscript and drafted the manuscript. DC, MG, and CG critically revised the manuscript. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
LD would like to acknowledge support from the Innovative Medicines Initiative 2 Joint Undertaking under grant agreement No. 821528 (NeuroDeRisk: Neurotoxicity De-Risking in Preclinical Drug Discovery). This Joint Undertaking is sustained by the European Union’s Horizon 2020 Research and Innovation Programme and the European Federation of Pharmaceutical Industries and Associations (EFPIA).
Borrelli, E., Nestler, E. J., Allis, C. D., and Sassone-Corsi, P. (2008). Decoding the epigenetic language of neuronal plasticity. Neuron 60, 961–974. doi: 10.1016/j.neuron.2008.10.012
Boussios, S., Pentheroudakis, G., Katsanos, K., and Pavlidis, N. (2012). Systemic treatment-induced gastrointestinal toxicity: incidence, clinical presentation and management. Nausea Vomit. 25, 106–118.
Branca, J. J. V., Maresca, M., Morucci, G., Becatti, M., Paternostro, F., Gulisano, M., et al. (2018). Oxaliplatin-induced blood brain barrier loosening: a new point of view on chemotherapy-induced neurotoxicity. Oncotarget 9, 23426–23438. doi: 10.18632/oncotarget.25193
Branca, J. J. V., Morucci, G., Malentacchi, F., Gelmini, S., Ruggiero, M., and Pacini, S. (2015). Effects of oxaliplatin and oleic acid Gc-protein-derived macrophage-activating factor on murine and human microglia: effects of oxaliplatin and GcMAF on microglia. J. Neurosci. Res. 93, 1364–1377. doi: 10.1002/jnr.23588
Bray, F., Ferlay, J., Soerjomataram, I., Siegel, R. L., Torre, L. A., and Jemal, A. (2018). Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 68, 394–424. doi: 10.3322/caac.21492
Chen, Y.-C., Tzeng, C.-H., Chen, P.-M., Lin, J.-K., Lin, T.-C., Chen, W.-S., et al. (2010). Influence of GSTP1 I105V polymorphism on cumulative neuropathy and outcome of FOLFOX-4 treatment in Asian patients with colorectal carcinoma. Cancer Sci. 101, 530–535. doi: 10.1111/j.1349-7006.2009.01418.x
Cobo, F., Celis, G. D., Pereira, A., Latorre, X., Pujadas, J., and Albiol, S. (2007). Oxaliplatin-induced immune hemolytic anemia: a case report and review of the literature. Anticancer. Drugs 18, 973–976.
Cruzado, J. A., López-Santiago, S., Martínez-Marín, V., José-Moreno, G., Custodio, A. B., and Feliu, J. (2014). Longitudinal study of cognitive dysfunctions induced by adjuvant chemotherapy in colon cancer patients. Support Care Cancer 22, 1815–1823. doi: 10.1007/s00520-014-2147-x
Culy, C. R., Clemett, D., and Wiseman, L. R. (2000). Oxaliplatin: a review of its pharmacological properties and clinical efficacy in metastatic colorectal cancer and its potential in other malignancies. Drugs 60, 895–924. doi: 10.2165/00003495-200060040-200060045
Cunningham, D. (2006). Is oxaliplatin the optimal platinum agent in gastric cancer? Eur. J. Cancer Suppl. 4, 10–13. doi: 10.1016/S1359-6349(06)70003-70009
Dai, Z., and Wang, Z. (2020). Photoactivatable platinum-based anticancer drugs: mode of photoactivation and mechanism of action. Molecules 25: 5167.
De Monaco, A., Valente, D., Di Paolo, M., Troisi, A., D’Orta, A., and Del Buono, A. (2014). Oxaliplatin-based therapy: strategies to prevent or minimize neurotoxicity. World Cancer Res. J. 1:e232.
Deng, J., Ding, H., Long, J., Lin, S., Liu, M., Zhang, X., et al. (2020). Oxaliplatin-induced neuropathic pain involves HOXA6 via a TET1 -dependent demethylation of the SOX10 promoter. Int. J. Cancer 147, 2503–2514. doi: 10.1002/ijc.33106
Descalzi, G., Ikegami, D., Ushijima, T., Nestler, E. J., Zachariou, V., and Narita, M. (2015). Epigenetic mechanisms of chronic pain. Trends Neurosci. 38, 237–246. doi: 10.1016/j.tins.2015.02.001
Di Cesare Mannelli, L., Pacini, A., Bonaccini, L., Zanardelli, M., Mello, T., et al. (2013a). Morphologic features and glial activation in rat oxaliplatin-dependent neuropathic pain. J. Pain 14, 1585–1600. doi: 10.1016/j.jpain.2013.08.002
Di Cesare Mannelli, L., Zanardelli, M., Failli, P., and Ghelardini, C. (2013b). Oxaliplatin-induced oxidative stress in nervous system-derived cellular models: could it correlate with in vivo neuropathy? Free Radical Biol. Med. 61, 143–150. doi: 10.1016/j.freeradbiomed.2013.03.019
Di Cesare Mannelli, L., Pacini, A., Corti, F., Boccella, S., Luongo, L., et al. (2015). Antineuropathic profile of N-Palmitoylethanolamine in a rat model of oxaliplatin-induced neurotoxicity. PLoS One 10:e0128080. doi: 10.1371/journal.pone.0128080
Di Cesare Mannelli, L., Pacini, A., Micheli, L., Femia, A. P., Maresca, M., et al. (2017). Astragali radix: could it be an adjuvant for oxaliplatin-induced neuropathy? Sci. Rep. 7:42021. doi: 10.1038/srep42021
Di Cesare Mannelli, L., Pacini, A., Micheli, L., Tani, A., Zanardelli, M., et al. (2014). Glial role in oxaliplatin-induced neuropathic pain. Exp. Neurol. 261, 22–33.
Di Cesare Mannelli, L., Zanardelli, M., Failli, P., and Ghelardini, C. (2012). Oxaliplatin-Induced neuropathy: oxidative stress as pathological mechanism. protective effect of silibinin. J. Pain 13, 276–284. doi: 10.1016/j.jpain.2011.11.009
Di Cesare Mannelli, L., Zanardelli, M., Landini, I., Pacini, A., Ghelardini, C., et al. (2016). Effect of the SOD mimetic MnL4 on in vitro and in vivo oxaliplatin toxicity: possible aid in chemotherapy induced neuropathy. Free Radical Biol. Med. 93, 67–76. doi: 10.1016/j.freeradbiomed.2016.01.023
Fardell, J. E., Vardy, J., Shah, J. D., and Johnston, I. N. (2012). Cognitive impairments caused by oxaliplatin and 5-fluorouracil chemotherapy are ameliorated by physical activity. Psychopharmacology 220, 183–193. doi: 10.1007/s00213-011-2466-2462
Fleishman, S. B., Mahajan, D., Rosenwald, V., Nugent, A. V., and Mirzoyev, T. (2012). Prevalence of delayed nausea and/or vomiting in patients treated with oxaliplatin-based regimens for colorectal Cancer. JOP 8, 136–140. doi: 10.1200/JOP.2010.000151
Foo, K. F., Michael, M., Toner, G., and Zalcberg, J. (2003). A case report of oxaliplatin extravasation. Ann. Oncol. 14, 961–962. doi: 10.1093/annonc/mdg252
Friedrich, A., Prasad, P. D., Freyer, D., Ganapathy, V., and Brust, P. (2003). Molecular cloning and functional characterization of the OCTN2 transporter at the RBE4 cells, an in vitro model of the blood–brain barrier. Brain Res. 968, 69–79.
Fujita, S., Hirota, T., Sakiyama, R., Baba, M., and Ieiri, I. (2019). Identification of drug transporters contributing to oxaliplatin-induced peripheral neuropathy. J. Neurochem. 148, 373–385. doi: 10.1111/jnc.14607
Gamper, E.-M., Zabernigg, A., Wintner, L. M., Giesinger, J. M., Oberguggenberger, A., Kemmler, G., et al. (2012). Coming to your senses: detecting taste and smell alterations in chemotherapy patients. a systematic review. J. Pain Symptom Manag. 44, 880–895. doi: 10.1016/j.jpainsymman.2011.11.011
Gebremedhn, E. G., Shortland, P. J., and Mahns, D. A. (2018). The incidence of acute oxaliplatin-induced neuropathy and its impact on treatment in the first cycle: a systematic review. BMC Cancer 18:410. doi: 10.1186/s12885-018-4185-4180
Hong, J., Han, S. W., Ham, H. S., Kim, T. Y., Choi, I. S., Kim, B.-S., et al. (2011). Phase II study of biweekly S-1 and oxaliplatin combination chemotherapy in metastatic colorectal cancer and pharmacogenetic analysis. Cancer Chemother. Pharmacol. 67, 1323–1331. doi: 10.1007/s00280-010-1425-1427
Huang, K. M., Leblanc, A. F., Uddin, M. E., Kim, J. Y., Chen, M., Eisenmann, E. D., et al. (2020). Neuronal uptake transporters contribute to oxaliplatin neurotoxicity in mice. J. Clin. Investigat. 130, 4601–4606. doi: 10.1172/JCI136796
Huang, Z.-Z., Li, D., Ou-Yang, H.-D., Liu, C.-C., Liu, X.-G., Ma, C., et al. (2016). Cerebrospinal fluid oxaliplatin contributes to the acute pain induced by systemic administration of oxaliplatin. Anesthesiology 124, 1109–1121. doi: 10.1097/ALN.0000000000001084
Huo, H., Magro, P. G., Pietsch, E. C., Patel, B. B., and Scotto, K. W. (2010). Histone methyltransferase MLL1 regulates MDR1 transcription and chemoresistance. Cancer Res. 70, 8726–8735.
Jardim, D. L., Rodrigues, C. A., Novis, Y. A. S., Rocha, V. G., and Hoff, P. M. (2012). Oxaliplatin-related thrombocytopenia. Ann. Oncol. 23, 1937–1942. doi: 10.1093/annonc/mds074
Ji, R. R., Chamessian, A., and Zhang, Y. Q. (2016). Pain regulation by non-neuronal cells and inflammation. Science 354, 572–577. doi: 10.1126/science.aaf8924
Johnstone, T. C., Suntharalingam, K., and Lippard, S. J. (2016). The next generation of platinum drugs: targeted Pt(II) agents, nanoparticle delivery, and Pt(IV) prodrugs. Chem. Rev. 116, 3436–3486.
Kanat, O., Ertas, H., and Caner, B. (2017). Platinum-induced neurotoxicity: a review of possible mechanisms. WJCO 8, 329–335. doi: 10.5306/wjco.v8.i4.329
Kennedy, J. G., Donahue, J. P., Hoang, B., and Boland, P. J. (2003). Vesicant characteristics of oxapliplatin following antecubital extravasation. Clin. Oncol. 15, 237–239. doi: 10.1016/S0936-6555(02)00338-332
Kim, S.-H., Choi, M. K., Park, N. Y., Hyun, J.-W., Lee, M. Y., Kim, H. J., et al. (2020). Serum neurofilament light chain levels as a biomarker of neuroaxonal injury and severity of oxaliplatin-induced peripheral neuropathy. Sci. Rep. 10:7995. doi: 10.1038/s41598-020-64511-64515
Kokotis, P., Schmelz, M., Kostouros, E., Karandreas, N., and Dimopoulos, M.-A. (2016). Oxaliplatin-Induced neuropathy: a long-term clinical and neurophysiologic follow-up study. Clin. Colorectal Cancer 15, e133–e140. doi: 10.1016/j.clcc.2016.02.009
Kretzschmar, A., Pink, D., Thuss-Patience, P., Dörken, B., Reichart, P., and Eckert, R. (2003). Extravasations of oxaliplatin. JCO 21, 4068–4069. doi: 10.1200/JCO.2003.99.095
Kweekel, D., Gelderblom, H., and Guchelaar, H. (2005). Pharmacology of oxaliplatin and the use of pharmacogenomics to individualize therapy. Cancer Treat. Rev. 31, 90–105. doi: 10.1016/j.ctrv.2004.12.006
Lecomte, T., Landi, B., Beaune, P., Laurent-Puig, P., and Loriot, M. A. (2006). Glutathione S-Transferase P1 polymorphism (Ile105Val) predicts cumulative neuropathy in patients receiving oxaliplatin-based chemotherapy. Clin. Cancer Res. 12, 3050–3056.
Lee, J. H., and Kim, W. (2020). The role of satellite glial cells, astrocytes, and microglia in oxaliplatin-induced neuropathic pain. Biomedicines 8:324. doi: 10.3390/biomedicines8090324
Lesko, L. J. (2007). Personalized medicine: elusive dream or imminent reality? Clin. Pharmacol. Ther. 81, 807–816. doi: 10.1038/sj.clpt.6100204
Lévi, F., Metzger, G., Massari, C., and Milano, G. (2000). Oxaliplatin: pharmacokinetics and chronopharmacological aspects. Clin. Pharmacokinet 38, 1–21. doi: 10.2165/00003088-200038010-200038011
Li, X., Zang, S., Cheng, H., Li, J., and Huang, A. (2019). Overexpression of activating transcription factor 3 exerts suppressive effects in HepG2 cells. Mol. Med. Rep. 19, 869–876.
Lin, C. J., Tai, Y., Huang, M.-T., Tsai, Y.-F., Hsu, H.-J., Tzen, K.-Y., et al. (2010). Cellular localization of the organic cation transporters, OCT1 and OCT2, in brain microvessel endothelial cells and its implication for MPTP transport across the blood-brain barrier and MPTP-induced dopaminergic toxicity in rodents: OCT-mediated transport of MPTP across the BBB in rodents. J. Neurochem. 114, 717–727. doi: 10.1111/j.1471-4159.2010.06801.x
Liu, Y., Zheng, X., Yu, Q., Wang, H., Tan, F., Zhu, Q., et al. (2016). Epigenetic activation of the drug transporter OCT2 sensitizes renal cell carcinoma to oxaliplatin. Sci. Transl. Med. 8:348ra97. doi: 10.1126/scitranslmed.aaf3124
Lokich, J. (2001). What is the “Best” platinum: cisplatin, carboplatin, or oxaliplatin? Cancer Investigat. 19, 756–760. doi: 10.1081/CNV-100106152
Lu, Y., Lin, Y., Huang, X., Wu, S., Wei, J., and Yang, C. (2019). Oxaliplatin aggravates hepatic oxidative stress, inflammation and fibrosis in a non-alcoholic fatty liver disease mouse model. Int. J. Mol. Med. 43, 2398–2408. doi: 10.3892/ijmm.2019.4154
Machelska, H., and Celik, M. Ö (2016). Recent advances in understanding neuropathic pain: glia, sex differences, and epigenetics. F1000Res 5:2743. doi: 10.12688/f1000research.9621.1
Majchrzak-Celińska, A. (2017). Pharmacoepigenetics: an element of personalized therapy? Expert Opin. Drug Metab. Toxicol. 13, 387–398. doi: 10.1080/17425255.2017.1260546
Massicot, F., Hache, G., David, L., Chen, D., Leuxe, C., Garnier-Legrand, L., et al. (2013). P2X7 cell death receptor activation and mitochondrial impairment in oxaliplatin-induced apoptosis and neuronal injury: cellular mechanisms and in vivo approach. PLoS One 8:e66830. doi: 10.1371/journal.pone.0066830
McLeod, H. L., Sargent, D. J., Marsh, S., Green, E. M., King, C. R., Fuchs, C. S., et al. (2010). Pharmacogenetic predictors of adverse events and response to chemotherapy in metastatic colorectal cancer: results from north american gastrointestinal intergroup trial N9741. JCO 28, 3227–3233. doi: 10.1200/JCO.2009.21.7943
McMahon, S. B., Cafferty, W. B. J., and Marchand, F. (2005). Immune and glial cell factors as pain mediators and modulators. Exp. Neurol. 192, 444–462. doi: 10.1016/j.expneurol.2004.11.001
McQuade, R. M., Carbone, S. E., Stojanovska, V., Rahman, A., Gwynne, R. M., Robinson, A. M., et al. (2016). Role of oxidative stress in oxaliplatin-induced enteric neuropathy and colonic dysmotility in mice. Br. J. Pharmacol. 173, 3502–3521. doi: 10.1111/bph.13646
McQuade, R. M., Stojanovska, V., Stavely, R., Timpani, C., Petersen, A. C., Abalo, R., et al. (2018). Oxaliplatin-induced enteric neuronal loss and intestinal dysfunction is prevented by co-treatment with BGP-15: BGP-15 prevents oxaliplatin-induced side effects. Br. J. Pharmacol. 175, 656–677. doi: 10.1111/bph.14114
Miaskowski, C., Mastick, J., Paul, S. M., Topp, K., Smoot, B., Abrams, G., et al. (2017). Chemotherapy-Induced neuropathy in Cancer survivors. J. Pain Symptom Manage 54, 204–218.e2. doi: 10.1016/j.jpainsymman.2016.12.342
Mohelnikova-Duchonova, B. (2014). FOLFOX/FOLFIRI pharmacogenetics: the call for a personalized approach in colorectal cancer therapy. WJG 20:10316. doi: 10.3748/wjg.v20.i30.10316
Morucci, G., Branca, J. J. V., Gulisano, M., Ruggiero, M., Paternostro, F., Pacini, A., et al. (2015). Gc-protein-derived macrophage activating factor counteracts the neuronal damage induced by oxaliplatin. Anti-Cancer Drugs 26, 197–209. doi: 10.1097/CAD.0000000000000177
Nichetti, F., Falvella, F. S., Miceli, R., Cheli, S., Gaetano, R., Fucà, G., et al. (2019). Is a pharmacogenomic panel useful to estimate the risk of oxaliplatin-related neurotoxicity in colorectal cancer patients? Pharmacogenomics J. 19, 465–472. doi: 10.1038/s41397-019-0078-70
Okamoto, T., Takagi, K., and Fukuda, K. (2020). Oxaliplatin-Induced lhermitte’s sign in gastric Cancer. Case Rep. Oncol. Med. 2020:8826657. doi: 10.1155/2020/8826657
Oun, R., Moussa, Y. E., and Wheate, N. J. (2018). The side effects of platinum-based chemotherapy drugs: a review for chemists. Dalton Trans. 47, 6645–6653. doi: 10.1039/C8DT00838H
Park, S. B., Lin, C. S. Y., Krishnan, A. V., Goldstein, D., Friedlander, M. L., and Kiernan, M. C. (2009). Oxaliplatin-induced neurotoxicity: changes in axonal excitability precede development of neuropathy. Brain 132, 2712–2723. doi: 10.1093/brain/awp219
Penas, C., and Navarro, X. (2018). Epigenetic modifications associated to neuroinflammation and neuropathic pain after neural trauma. Front. Cell. Neurosci. 12:158. doi: 10.3389/fncel.2018.00158
Peng, Z., Wang, Q., Gao, J., Ji, Z., Yuan, J., Tian, Y., et al. (2013). Association between GSTP1 Ile105Val polymorphism and oxaliplatin-induced neuropathy: a systematic review and meta-analysis. Cancer Chemother. Pharmacol. 72, 305–314. doi: 10.1007/s00280-013-2194-x
Pirmohamed, M. (2001). Pharmacogenetics and pharmacogenomics. Br. J. Clin. Pharmacol. 52, 345–347. doi: 10.1046/j.0306-5251.2001.01498.x
Raez, L. E., Kobina, S., and Santos, E. S. (2010). Oxaliplatin in first-line therapy for advanced non–small-cell lung Cancer. Clin. Lung Cancer 11, 18–24. doi: 10.3816/CLC.2010.n.003
Rosenberg, B., VanCamp, L., Trosko, J. E., and Mansour, V. H. (1969). Platinum compounds: a new class of potent antitumour agents. Nature 222, 385–386. doi: 10.1038/222385a0
Ruzzo, A., Graziano, F., Galli, F., Giacomini, E., Floriani, I., Galli, F., et al. (2015). Genetic markers for toxicity of adjuvant oxaliplatin and fluoropyrimidines in the phase III TOSCA trial in high-risk colon cancer patients. Sci. Rep. 4:6828. doi: 10.1038/srep06828
Saif, M. W. (2007). Fever as the only manifestation of hypersensitivity reactions associated with oxaliplatin in a patient with colorectal Cancer oxaliplatin-induced hypersensitivity reaction. WJG 13:5277. doi: 10.3748/wjg.v13.i39.5277
Sałat, K. (2020). Chemotherapy-induced peripheral neuropathy—part 2: focus on the prevention of oxaliplatin-induced neurotoxicity. Pharmacol. Rep. 72, 508–527. doi: 10.1007/s43440-020-00106-101
Sparreboom, A., Danesi, R., Ando, Y., Chan, J., and Figg, W. D. (2003). Pharmacogenomics of ABC transporters and its role in cancer chemotherapy. Drug Resist. Update 6, 71–84. doi: 10.1016/S1368-7646(03)00005-0
Stankovic, J. S. K., Selakovic, D., Mihailovic, V., and Rosic, G. (2020). Antioxidant supplementation in the treatment of neurotoxicity induced by platinum-based chemotherapeutics—a review. Int. J. Mol. Sci. 21:7753.
Stordal, B., and Davey, M. (2007). Understanding cisplatin resistance using cellular models. TBMB 59, 696–699. doi: 10.1080/15216540701636287
Taylor, M., and Filby, A. (2017). Health impact analysis of cisplatin, carboplatin and oxaliplatin. Johnson Matthey Technol. Rev. 61, 32–39.
Tesniere, A., Schlemmer, F., Boige, V., Kepp, O., Martins, I., Ghiringhelli, F., et al. (2010). Immunogenic death of colon cancer cells treated with oxaliplatin. Oncogene 29, 482–491. doi: 10.1038/onc.2009.356
Wang, W. S. (2014). Advances in the management of oxaliplatin-induced neuropathy: focus on glutamine and using pharmacogenomics to predict the effectiveness of opioid drugs. J. Cancer Res. Pract. 1, 175–185. doi: 10.6323/JCRP.2014.1.3.01
Wiseman, L. R., Adkins, J. C., Plosker, G. L., and Goa, K. L. (1999). Oxaliplatin: a review of its use in the management of metastatic colorectal Cancer. Drugs Aging 14, 459–475. doi: 10.2165/00002512-199914060-199914066
Zhang, F., Zhang, Y., Jia, Z., Wu, H., and Gu, K. (2019). Oxaliplatin-Based regimen is superior to cisplatin-based regimen in tumour remission as first-line chemotherapy for advanced gastric Cancer: a meta-analysis. J. Cancer 10, 1923–1929. doi: 10.7150/jca.28896
Zhang, M., Zhi, Y., Xie, H., Li, P., Jiao, D., He, J., et al. (2018). The role of chemokine CX3CL1 in the anterior cingulate cortex in a rat model of chronic pathological pain. Int J. Clin. Exp. Med. 11, 11988–11994.
Keywords: oxaliplatin, neuropathic pain, glial cells, genetic mechanisms, epigenetic mechanisms
Citation: Branca JJV, Carrino D, Gulisano M, Ghelardini C, Di Cesare Mannelli L and Pacini A (2021) Oxaliplatin-Induced Neuropathy: Genetic and Epigenetic Profile to Better Understand How to Ameliorate This Side Effect. Front. Mol. Biosci. 8:643824. doi: 10.3389/fmolb.2021.643824
Received: 18 December 2020; Accepted: 24 February 2021;
Published: 07 May 2021.
Edited by:
Md. Asaduzzaman Khan, Southwest Medical University, ChinaReviewed by:
Snehal M. Gaikwad, National Cancer Institute, United StatesCopyright © 2021 Branca, Carrino, Gulisano, Ghelardini, Di Cesare Mannelli and Pacini. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Alessandra Pacini, YWxlc3NhbmRyYS5wYWNpbmlAdW5pZmkuaXQ=
†These authors have contributed equally to this work and share senior authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.