
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Microbiol., 27 March 2025
Sec. Infectious Agents and Disease
Volume 16 - 2025 | https://doi.org/10.3389/fmicb.2025.1566171
This article is part of the Research TopicWomen in Infectious Agents and Disease: 2024View all 10 articles
 Marta Díaz-Navarro1,2
Marta Díaz-Navarro1,2 Álvaro Irigoyen-von-Sierakowski1,2
Álvaro Irigoyen-von-Sierakowski1,2 Imani Delcán3Ariadna Monte3María Palomo1,4
Imani Delcán3Ariadna Monte3María Palomo1,4 Pilar Escribano1,2,4
Pilar Escribano1,2,4 Jesús Guinea1,2,4
Jesús Guinea1,2,4 Almudena Burillo1,4,5Alicia Galar1,2,4
Almudena Burillo1,4,5Alicia Galar1,2,4 Patricia Muñoz1,2,4,5
Patricia Muñoz1,2,4,5 María Guembe1,2*
María Guembe1,2*Background: Despite the pathogenesis of vulvovaginal candidiasis (VVC) is multifactorial, this study aimed to assess whether phenotypic characteristics, such as biofilm production and quality, along with clinical symptoms, are associated with recurrent VVC (RVVC).
Methods: Over 1 year (Oct 2021–Oct 2022), we prospectively included 271 patients ≥18 years who attended our institution, had Candida spp. isolated in vaginal swabs, and provided informed consent. Patients were followed for 1 year. Candida spp. isolates were tested by the following techniques: crystal violet (CV) for biomass quantification, XTT for metabolic activity quantification, and microscopy for biofilm area quantification. Clinical and microbiological data were also collected.
Results: Overall, 55 (20.3%) patients experienced at least one recurrence, with 19 (7.0%) meeting the criteria for RVVC (≥3 episodes/year), with 65 episodes in total. Demographic and clinical characteristics were similar in both study groups. Most isolates were C. albicans (90.0%). Median (interquartile, [IQR]) absorbance values for CV and XTT in 18/19 RVVC and 238/252 non-RVVC isolates were as follows: CV, 1.850 (1.578–2.156) vs. 1.426 (1.081–1.823), p = 0.005; XTT, 0.184 (0.116–0.293) vs. 0.228 (0.147–0.331), p = 0.253. Median (IQR) biofilm occupation area percentage in 16/19 RVVC and 16/252 non-RVVC isolates was, respectively: 13.15 (8.54–16.9) and 10.73 (5.88–17.73), p = 0.710.
Conclusion: RVVC was associated to high biomass production. Additionally, RVVC clinical isolates exhibited a tendency toward lower metabolic activity, which may contribute to treatment failure.
Vulvovaginal Candidiasis (VVC) affects about 75% of women at least once in their lifetime and is characterized by Candida spp. overgrowth, often associated with non-specific bacterial vaginosis symptoms (Arechavala et al., 2021; Kalia et al., 2020). Recurrent vulvovaginal candidiasis (RVVC) affects about 4–9% of women and is defined as three or more symptomatic episodes of VVC per year, with at least two confirmed by microscopy or culture (Lines et al., 2020; Workowski et al., 2021; Yazdy et al., 2024; Neal and Martens, 2022). The dysbiosis caused by an imbalance between Candida spp. and vaginal microbiota is affected by several factors, including prolonged antibiotic usage, childbearing age, and use of contraceptives (Arechavala et al., 2021; Kalia et al., 2020; Neal and Martens, 2022; Brown et al., 2022; Díaz-Navarro et al., 2023; McKloud et al., 2021; Rodríguez-Cerdeira et al., 2020; Tits et al., 2020).
In addition, several Candida virulence factors contribute to its ability to infect the vaginal epithelium, particularly biofilm formation (Kalia et al., 2020; Mayer et al., 2013; Iliev and Underhill, 2013; Monfredini et al., 2018; Li et al., 2022; Roudbarmohammadi et al., 2016; Gonçalves et al., 2020; Wu et al., 2020). Another important aspect is the local immune response, where both a deficient immune response to Candida, allowing fungal proliferation, and an exaggerated inflammatory reaction against Candida are implicated in pathogenesis. These mechanisms have been linked to genetic polymorphisms, including NLRP3 gene variants, and alterations in innate immunity. Besides, it has been suggested that a tightly regulated fungus-host-microbiota interplay might exert a protective role against RVVC (Czechowicz et al., 2022; Rosati et al., 2020; Wang et al., 2024).
VVC treatment typically involves topical antifungal agents or single-dose or two-dose oral antifungal therapy. However, suppressive therapy is required in RVVC patients to achieve full symptom resolution (Denning et al., 2018). Moreover, resistance to conventional antifungals is an increasing problem in recent years, particularly in RVVC (Arechavala et al., 2021; Mesquida et al., 2021). The prevalence of RVVC is expected to rise rather than decline in the future (Denning et al., 2018). Therefore, there is an urgent need to search for alternative treatments that improve patient outcomes (Wang et al., 2024).
However, a deeper understanding of the key factors driving RVVC pathogenesis is essential to identify patients at risk and predict treatment success.
Therefore, the aim of our study was to identify phenotypic and clinical characteristics closely related to RVVC.
The study was carried out at a tertiary Teaching Hospital in Madrid (Spain).
≥3 symptomatic episodes of VVC per year, at least 2 of them confirmed by either microscopy or culture (Workowski et al., 2021; Yazdy et al., 2024; Neal and Martens, 2022).
Severity of symptoms (asymptomatic, mild, moderate, and severe) was assessed based on the presence of one or more of the following: vulvar erythema, vaginal itching, leukorrhea, vulvar lichenification.
Prospective study based on the analysis of Candida spp. clinical isolates isolated from vaginal exudate samples of patients with one or more episodes of VVC who attended the Sexually Transmitted Diseases consultation of the Clinical Microbiology Department of our institution.
Vaginal swabs were cultured in CHROMagar™ (BioMérieux, Spain) to isolate yeasts, while MacConkey agar (BioMérieux, Spain) was used to recover lactose-positive Gram-negative bacilli. Clinical isolates were then identified using matrix-assisted laser desorption/ionization time-of-flight mass spectrometry (MALDI-TOF MS). Clinical isolates were stored at −70°C for use in in vitro studies.
Over 1 year (Oct 2021-Oct 2022), patients in whom the presence of Candida spp. was detected in vaginal culture were enrolled in the study, with an additional 1-year follow-up (Oct 2022-Oct 2023). Since the presence or absence of VVC was unknown at the time of consultation, informed consent was obtained via telephone once a positive culture was detected. Additionally, patients who returned for follow-up and had initially provided consent by telephone were subsequently given written informed consent during their visit.
Candida spp. clinical isolates from enrolled patients were stored in the mycology laboratory for genotyping and antifungal susceptibility studies.
Once patient follow-up was completed, they were classified into two groups: non-RVVC (patient reporting <3 episodes/year) and RVVC (patient reporting ≥3 episodes/year). Classification was primarily based on the symptomatology reported by the patient, since it was not always possible to isolate the clinical strains for each episode by microbiological culture. Current guidelines do not require confirmation by culture (the British guidelines define that, if there is symptomatology, at least 1 or 2 is enough in order to identify the species) (Workowski et al., 2021). Symptom severity was categorized as mild, severe or asymptomatic.
For the analysis of variables in patients with multiple VVC episodes, the first isolated strain was selected.
The first Candida spp. isolate from each patient in both study groups was tested for the following characteristics as previously described (24, 25): biomass production using the crystal violet (CV) assay, metabolic activity using the tetrazolium salt (XTT) assay, and biofilm occupation area using confocal laser scanning microscopy (CLSM). Clinical symptoms were also collected.
For the isolation of E. coli in the vaginal swabs, 81 out of 271 samples were available for testing, as its isolation in McConkey agar plates was only performed for a limited period.
A 24-h mature biofilm in vitro model on 96-well plates. Briefly, a 24-h culture of Candida spp. was grown in 20 ml of tryptic soy broth (TSB) at 37°C for 24 h under shaking. The pellets were centrifuged three times, washed with phosphate-buffered saline (PBS), and adjusted to 108 cfu/ml in TSB. Suspensions (100 μl) were inoculated into 96-well plates and incubated overnight at 37°C. The wells were then washed three times with PBS before staining. All assays were performed in triplicate.
For the CV assay, wells were fixed with 125 μl of 99% methanol for 15–20 min at room temperature. Methanol was then removed, and 125 μl of CV was added for 10–15 min at room temperature. After staining, wells were washed with sterile water, and 125 μl of 30% acetic acid was added at room temperature for 10–15 min. Finally, the solubilized CV solution was transferred to a new plate, and absorbance at 550 nm was measured using a spectrophotometer. Results were expressed as the median (interquartile range, [IQR]) of three replicates of biomass absorbance, corrected for the negative control (Høiby et al., 2015; Coenye and Nelis, 2010).
For the XTT assay, 100 μl of XTT (with menadione 1:1000) was added to each well and incubated for 3 h in the dark. Absorbance at 492 nm was measured using a spectrophotometer. Results were expressed as the median (IQR) of three replicates of metabolic activity absorbance value relative to the negative control.
The total number of clinical isolates to be tested was 256/275 (18/19 in RVVC group and 238/252 in non-RVVC group).
For these experiments, 16 clinical isolates from the RVVC group were included (3 out of 19 were not available), including 11 C. albicans, 3 C. glabrata, and 2 C. krusei isolates. Additionally, 16 clinical isolates from the non-RVVC group were arbitrarily selected to match the same species distribution. In vitro biofilm models of 24-well plates were used. Biofilms were formed on glass slides (Labolan, Spain) previously coated with poly-L-lysine for 24 h at 37°C. Then, 300 μl of 108 cfu/ml fungal suspension was added to the coated slides placed in the wells, followed by incubation for 24 h at 37°C. Slides were then washed three times with PBS, and 300 μl of formaldehyde was added to each well. The slides were observed under a 20× objective (Leica Geosystems AG, Heerbrugg, Switzerland), and images were processed using FIJI/ImageJ software (National Institute of Health, Bethesda, MD, USA). The median (IQR) percentage of area occupied by Candida spp. from the three different surfaces of the slides was calculated (Olson et al., 2018).
In addition, one C. parapsilosis strain (arbitrarily selected) and the only C. orthopsilosis strain were included for a qualitative assessment of the biofilm structure, allowing for comparison with the biofilms of other species.
Qualitative clinical variables were expressed as counts and percentages and compared using the chi-square test. Quantitative clinical variables were expressed as mean (standard deviation, [SD]) or median (IQR) and compared using the median test.
For the comparison of variables involving 3 or more groups, either the Kruskal-Wallis test or ANOVA was used, depending on data distribution.
Statistical significance was set at p < 0.05. All tests were performed using SPSS Statistics for Windows, v.21.0 (IBM Corp, Armonk, New York, USA).
A total of 271 patients were included in the study, 55 (20.3%) of whom experienced at least one recurrence (≥1 episode/year). Among them, 19 (7.0%) met criteria for RVVC (≥3 episodes/year), accounting for a total of 65 episodes. Particularly, 12 patients had 3 episodes, 6 patients had 4 episodes, and 1 patient had 5 episodes (Table 1). The median (IQR) age of patients was 34.00 (26.00–45.00) years, with no significant differences between study groups (Table 1). Overall, 27.7% of patients had at least one vaginal isolation of Candida spp. in the previous year, with a mean (SD) of 1.60 (1.04) episodes, most with no apparent association with specific factors (67.2%). Only 7.7 and 7.4% of previous episodes were related to the menstrual cycle and sexual activity, respectively, and only 0.7% antimicrobial use (Table 1).
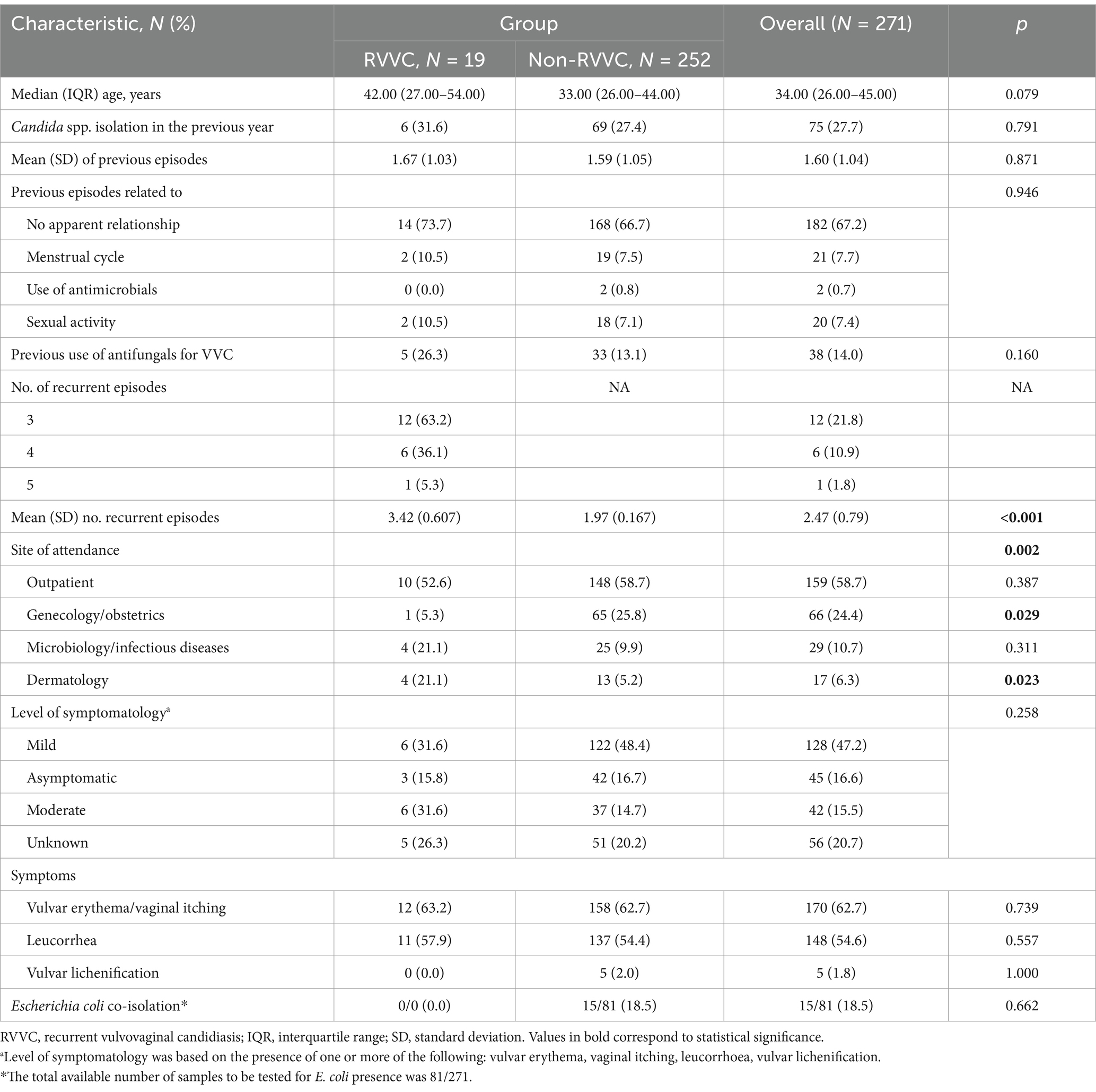
Table 1. Clinical and microbiological characteristics of the participating patients.
Despite not being statistically significant, patients with RVVC had a higher prior use of antifungals than those with non-RVVC (26.3% vs. 13.1%, p = 0.160).
Distribution of Candida species in each study group was as follows: RVVC: C. albicans, 73.7%; C. glabrata, 15.8%; and C. krusei, 10.5%; non-RVVC: C. albicans, 91.3%; C. glabrata, 5.2%; C. parapsilosis, 1.6%; C. krusei, 1.6%, and C. orthopsilosis, 0.4%. A significantly higher prevalence of C. albicans was observed in the non-RVVC group compared to the RVVC group (91.3% vs. 73.3%, p = 0.029). Moreover, patients with non-RVVC were more frequently attended at Gynecology/Obstetrics Departments (25.8% vs. 5.3%, p = 0.029), whereas patients with RVVC were more frequently seen at the Dermatology Department (21.1% vs. 5.2%, p = 0.023) (Table 1).
Regarding symptom severity, most patients presented with mild disease (47.2%), followed by asymptomatic cases (16.6%) and those with moderate disease (15.1%), with no statistically significant differences between groups (p = 0.258). The most frequently reported symptoms were vulvar erythema and/or vaginal itching (62.7%) and leucorrhea (54.6%) (Table 1).
Although E. coli presence in vaginal swabs could only be analyzed in 81 out of 271 patients, it was exclusively found in the non-RVVC group (18.5%).
Analysis was performed on 18/19 RVVC and 238/252 non-RVVC clinical isolates. Median (IQR) CV absorbance was significantly higher in the RVVC group (1.850 [1.578–2.156] vs. 1.426 [1.081–1.823], p = 0.005). Despite it did not reach statistical significance, median (IQR) XTT absorbance was slightly higher in the non-RVVC group (0.228 [0.147–0.331] vs. 0.184 [0.116–0.293], p = 0.253) (Figure 1).
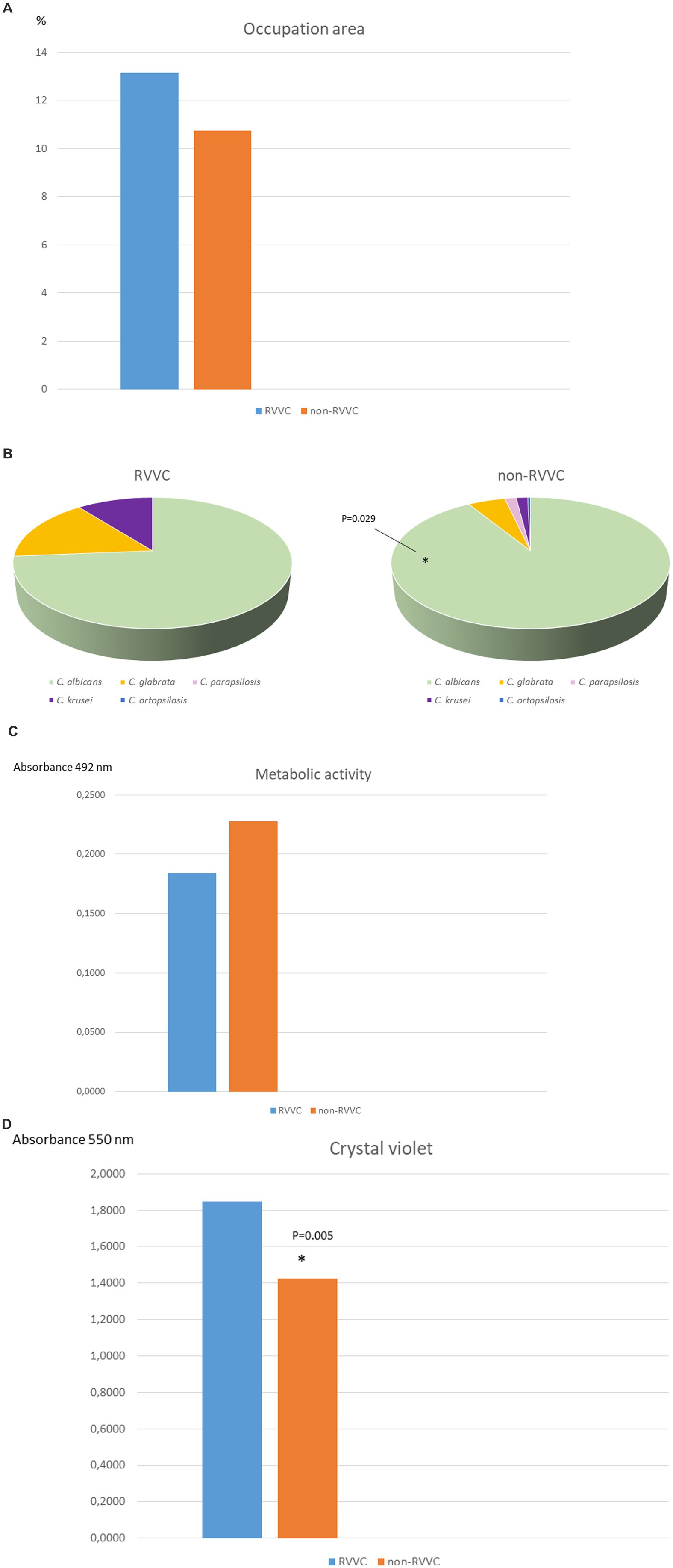
Figure 1. Description of clinical isolates in both study groups. (A) Candida spp. distribution according to species. * statistical significance p = 0.029. (B) Median crystal violet absorbance. * Statistical significance p = 0.005. The total available number of clinical isolates to be tested was 256/275 (18/19 in RVVC group and 238/252 in non-RVVC group). (C) Median metabolic activity absorbance (XTT). NS, non-significant. The total available number of clinical isolates to be tested was 256/275 (18/19 in RVVC group and 238/252 in non-RVVC group). (D) Median percentage of biofilm occupation area. NS, non-significant. The total number of selected and available clinical isolates tested were 32 (16 from RVVC group and 16 from non-RVVC).
Analysis was performed in 16/19 RVVC and 16/252 non-RVVC isolates. Median (IQR) percentage of biofilm occupation area was similar between both study groups: 13.15 (8.54–16.49) and 10.73 (5.88–17.73) in RVVC and non-RVVC, respectively (p = 0.710). In contrast, when biofilm morphology and structure were analysed according to Candida species, we C. albicans showed the highest hyphal formation, whereas C. glabrata was the one displaying higher density and extracellular matrix (Figure 2). Although only one episode of VVC caused by C. orthopsilosis was collected, it showed the lowest biofilm production (Figure 2E).
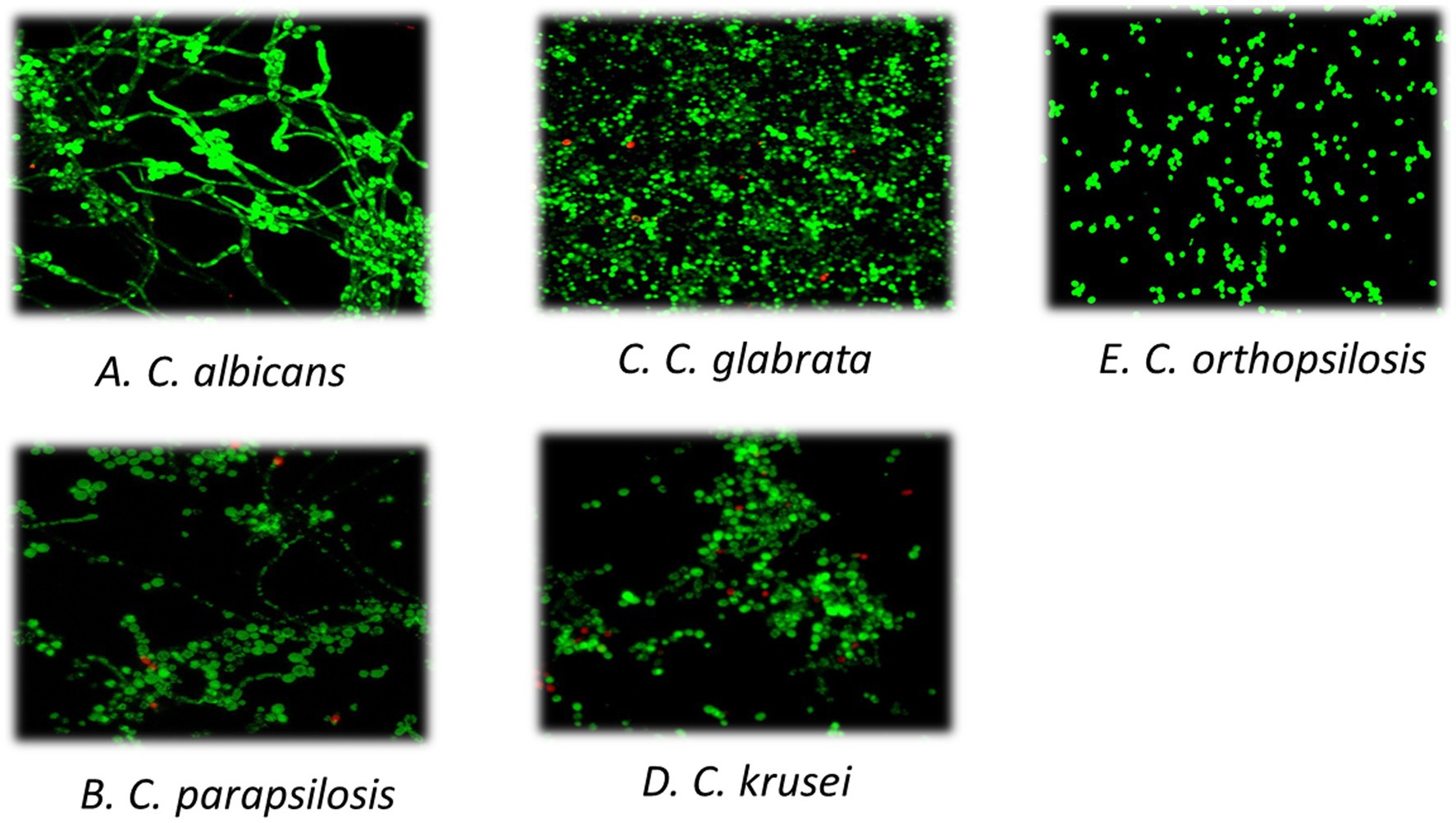
Figure 2. Biofilm structure according to species. We selected a representative image of each Candida species. Biofilm formation was performed on 12 mm circular glass slides pre-treated with Poly-L-lysine (1:100) for 24 h at 37°C and observed using confocal laser scanning microscopy (CLSM, Leica Geosystems AG, Heerbrugg, Switzerland) and the APO 63X glycerol immersion objective. Biofilm images (280×280 μm) were captured from three different areas of the slide in triplicate and then processed using the FIJI/ImageJ software (National Institute of Health, Bethesda, MD). The percentage of area occupied by yeasts and hyphae was calculated for each sample. (A) Candida albicans; (B) Candida parapsilosis; (C) Candida glabrata; (D) Candida krusei; (E) Candida orthopsilosis.
Considering that RVVC is common condition among women and significantly impacts their sexual health, fertility and reproductive capacity, it is important to investigate the factors contributing to its occurrence to identify effective solutions (Yazdy et al., 2024). Various predisposition factors act as molecular drivers that lead to dysbiosis of the normal vaginal microbiota. Therefore, understanding the molecular mechanisms underlying the virulence pathways driven by these factors is crucial for identifying potential drug targets (David and Solomon, 2023).
In the present study, 20.3% of patients experienced at least one recurrence, and 7.0% were classified as RVVC, having ≥3 episodes/year. Our findings indicate that Candida species isolated from women with RVVC had higher biomass and lower metabolic activity. This suggests that sessile cells not only form thicker and denser biofilms but also avoid antifungal action without being fully eradicated. In their dormant state, these cells can persist and later re-infect the vaginal site under conditions of dysbiosis that favor regrowth. In RVVC, dormancy of Candida species plays a crucial role in the antifungal treatment failure and subsequent reinfection. Dormant fungal cells, such as persister cells and biofilm-associated Candida, exhibit a slowed metabolic state that reduces their susceptibility to antifungal treatments, which primarily target actively growing cells. This resistance mechanism allows Candida to survive treatment and later reactivate, leading to reinfection. Additionally, biofilms provide a protective environment that shields the fungus from antifungal agents and immune responses, further contributing to therapeutic failure. As a result, even after apparent resolution, Candida can persist in the vaginal mucosa or recolonize from the gut or sexual partners, leading to recurrent episodes despite treatment (Muzny and Schwebke, 2015).
It was also observed that most patients with non-RVVC were diagnosed in the Gynecology/Obstetrics department, while patients with RVVC were mainly diagnosed and followed up in the Dermatology department. This suggests that non-RVVC cases were often incidentally detected during routine pregnancy exams, whereas more complicated, symptomatic and recurrent cases were intentionally monitored by dermatologists. This was corroborated by the higher proportion of moderate-to-severe episodes in the RVVC group (31.6%) compared to the non-RVVC group (14.7%), although this difference was not statistically significant (p = 0.258).
Another interesting finding in our study was that biofilm morphology varied depending on the Candida species, being C. albicans the one that exhibited the highest hyphal formation and C. glabrata the one with the lowest hyphae formation, consistent with previous studies (Olson et al., 2018; Ferreira et al., 2009; Pierce et al., 2017). However, these morphological differences were not observed according to biofilm occupation area, as median (IQR) percentage of occupation was similar between RVVC and non-RVVC groups (13.15 [8.54–16.49] vs. 10.73 [5.88–17.73], p = 0.710).
Regarding the simultaneous presence of E. coli in vaginal cultures, we observed that E. coli was only present in non-RVVC patients. This finding warrants further investigation, as it suggests that the simultaneous presence of E. coli may protect against recurrence, as we previously demonstrated (Díaz-Navarro et al., 2023).
Moreover, it is important to highlight the need for further research into potential therapeutic strategies for VVC, particularly those targeting probiotics and vaginal microbiota transplantation as means to restore the balance of dysbiotic vaginal microbiota (Wang et al., 2024).
One of the main limitations of the study is that we were not able to recover all clinical isolates for experimental analysis. However, the sample size was high enough to yield reliable results. In addition, we did not included information on the use intrauterine devices. Thus, future studies should evaluate the association between Candida biofilms on IUDs and their potential role as reservoirs for reinfection. Moreover, a more in-depth investigation into the role of genetic and immune factors in the pathogenesis of RVVC is necessary.
RVVC was associated to high biomass production. Although no statistically significant difference was observed, there was a tendency for RVVC clinical isolates to exhibit lower metabolic activity. This may contribute to treatment failure, as antifungal agents have limited efficacy against metabolically inactive cells. We suggest that quantifying biofilm production in Candida spp. clinical isolates causing RVVC could provide a better understanding of treatment failures and improve therapeutic strategies.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
The studies involving humans were approved by our local ethics committee (MICRO.HGUGM.2021-028). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
MD-N: Data curation, Formal analysis, Investigation, Methodology, Software, Writing – original draft. AI-v-S: Data curation, Investigation, Methodology, Writing – original draft. ID: Data curation, Investigation, Methodology, Writing – original draft. AM: Investigation, Methodology, Writing – original draft. MP: Data curation, Investigation, Methodology, Supervision, Writing – original draft. PE: Data curation, Investigation, Methodology, Supervision, Writing – review & editing. JG: Investigation, Methodology, Supervision, Writing – review & editing. AB: Conceptualization, Supervision, Writing – review & editing. AG: Data curation, Methodology, Writing – review & editing. PM: Supervision, Writing – review & editing. MG: Conceptualization, Funding acquisition, Resources, Supervision, Validation, Writing – review & editing.
The author(s) declare that financial support was received for the research and/or publication of this article. This research was funded by Fundación Mutua Madrileña, grant number FMM24/01, by the IiSGM (2022-PI-II-COOPTR-01) and by the ISCIII and the European Regional Development Fund (FEDER) “A way of making Europe,” grant number PI21/00344. M. Guembe was supported by the Miguel Servet Program (ISCIII-MICINN and MSII18/00008) from the Health Research Fund (FIS) of the Carlos III Health Institute (ISCIII), Madrid, Spain. M. Díaz-Navarro is supported by the ISCIII (FI22/00022). P. Escribano was supported by the Miguel Servet Program (ISCIII-MICINN and CPII20/00015) from the Health Research Fund (FIS) of the Carlos III Health Institute (ISCIII), Madrid, Spain.
We thank the laboratory and all the installations of Surgery and Experimental Medicine Unit for the technical support.
JG reports a relationship with Pfizer Inc., Gilead Sciences Inc., Merck Sharp & Dohme UK Ltd. that includes: speaking and lecture fees.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
The author(s) declare that no Gen AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Arechavala, A., Negroni, R., Santiso, G., Depardo, R., and Bonvehí, P. (2021). Chronic recurrent vulvovaginitis is not only due to Candida. Rev. Iberoam. Micol. 38, 132–137. doi: 10.1016/j.riam.2021.03.002
Brown, L., Chamula, M., Weinberg, S., Jbueen, F., and Rautemaa-Richardson, R. (2022). Compliance with the updated BASHH recurrent vulvovaginal candidiasis guidelines improves patient outcomes. J. Fungi 8:924. doi: 10.3390/jof8090924
Coenye, T., and Nelis, H. J. (2010). In vitro and in vivo model systems to study microbial biofilm formation. J. Microbiol. Methods 83, 89–105. doi: 10.1016/j.mimet.2010.08.018
Czechowicz, P., Nowicka, J., and Gościniak, G. (2022). Virulence factors of Candida spp. and host immune response important in the pathogenesis of vulvovaginal candidiasis. Int. J. Mol. Sci. 23:5895. doi: 10.3390/ijms23115895
David, H., and Solomon, A. P. (2023). Molecular association of Candida albicans and vulvovaginal candidiasis: focusing on a solution. Microorganisms 13:1245808. doi: 10.3389/fcimb.2023.1245808
Denning, D. W., Kneale, M., Sobel, J. D., and Rautemaa-Richardson, R. (2018). Global burden of recurrent vulvovaginal candidiasis: a systematic review. Lancet Infect. Dis. 18, e339–e347. doi: 10.1016/S1473-3099(18)30103-8
Díaz-Navarro, M., Irigoyen Von-Sierakowski, Á., Palomo, M., Escribano, P., Guinea, J., Burillo, A., et al. (2023). In vitro study to assess modulation of Candida biofilm by Escherichia coli from vaginal strains. Biofilms 5:100116. doi: 10.1016/j.bioflm.2023.100116
Ferreira, J. A., Carr, J. H., Starling, C. E., de Resende, M. A., and Donlan, R. M. (2009). Biofilm formation and effect of caspofungin on biofilm structure of Candida species bloodstream isolates. Antimicrob. Agents Chemother. 53, 4377–4384. doi: 10.1128/AAC.00316-09
Gonçalves, B., Azevedo, N. M., Henriques, M., and Silva, S. (2020). Hormones modulate Candida vaginal isolates biofilm formation and decrease their susceptibility to azoles and hydrogen peroxide. Med. Mycol. 58, 341–350. doi: 10.1093/mmy/myz070
Høiby, N., Bjarnsholt, T., Moser, C., Bassi, G. L., Coenye, T., Donelli, G., et al. (2015). ESCMID guideline for the diagnosis and treatment of biofilm infections 2014. Clin. Microbiol. Infect. 21, S1–S25. doi: 10.1016/j.cmi.2014.10.024
Iliev, I. D., and Underhill, D. M. (2013). Striking a balance: fungal commensalism versus pathogenesis. Curr. Opin. Microbiol. 16, 366–373. doi: 10.1016/j.mib.2013.05.004
Kalia, N., Singh, J., and Kaur, M. (2020). Microbiota in vaginal health and pathogenesis of recurrent vulvovaginal infections: a critical review. Ann. Clin. Microbiol. Antimicrob. 19:5. doi: 10.1186/s12941-020-0347-4
Li, X., Chen, S., Lyu, X., and Tian, J. (2022). Virulence is one of the mechanisms of vulvovaginal candidiasis recurrence, rather than drug resistance. Med. Mycol. 60:myac087. doi: 10.1093/mmy/myac087
Lines, A., Vardi-Flynn, I., and Searle, C. (2020). Recurrent vulvovaginal candidiasis. BMJ (Clin. Res. Ed.) 369:m1995. doi: 10.1136/bmj.m1995
Mayer, F. L., Wilson, D., and Hube, B. (2013). Candida albicans pathogenicity mechanisms. Virulence 4, 119–128. doi: 10.4161/viru.22913
McKloud, E., Delaney, C., Sherry, L., Kean, R., Williams, S., Metcalfe, R., et al. (2021). Recurrent vulvovaginal candidiasis: a dynamic Interkingdom biofilm disease of Candida and Lactobacillus. mSystems 6:e0062221. doi: 10.1128/mSystems.00622-21
Mesquida, A., Vicente, T., Reigadas, E., Palomo, M., Sánchez-Carrillo, C., Muñoz, P., et al. (2021). In vitro activity of ibrexafungerp and comparators against Candida albicans genotypes from vaginal samples and blood cultures. Clin. Microbiol. Infect. 27, 915.e5–915.e8. doi: 10.1016/j.cmi.2021.02.006
Monfredini, P. M., Souza, A. C. R., Cavalheiro, R. P., Siqueira, R. A., and Colombo, A. L. (2018). Clinical impact of Candida spp. biofilm production in a cohort of patients with candidemia. Med. Mycol. 56, 803–808. doi: 10.1093/mmy/myx133
Muzny, C. A., and Schwebke, J. R. (2015). Biofilms: an underappreciated mechanism of treatment failure and recurrence in vaginal infections. Clin. Infect. Dis. 61, 601–606. doi: 10.1093/cid/civ353
Neal, C. M., and Martens, M. G. (2022). Clinical challenges in diagnosis and treatment of recurrent vulvovaginal candidiasis. J. Fungi 10:20503121221115201. doi: 10.1177/20503121221115201
Olson, M. L., Jayaraman, A., and Kao, K. C. (2018). Relative abundances of Candida albicans and Candida glabrata in in vitro Coculture biofilms impact biofilm structure and formation. Appl. Environ. Microbiol. 84, e02769–e02717. doi: 10.1128/AEM.02769-17
Pierce, C. G., Vila, T., Romo, J. A., Montelongo-Jauregui, D., Wall, G., Ramasubramanian, A., et al. (2017). The Candida albicans biofilm matrix: composition, structure and function. J. Fungi 3:14. doi: 10.3390/jof3010014
Rodríguez-Cerdeira, C., Martínez-Herrera, E., Carnero-Gregorio, M., López-Barcenas, A., Fabbrocini, G., Fida, M., et al. (2020). Pathogenesis and clinical relevance of Candida biofilms in vulvovaginal candidiasis. Front. Microbiol. 11:544480. doi: 10.3389/fmicb.2020.544480
Rosati, D., Bruno, M., Jaeger, M., Ten Oever, J., and Netea, M. G. (2020). Recurrent vulvovaginal candidiasis: an immunological perspective. Microorganisms 8:144. doi: 10.3390/microorganisms8020144
Roudbarmohammadi, S., Roudbary, M., Bakhshi, B., Katiraee, F., Mohammadi, R., and Falahati, M. (2016). ALS1 and ALS3 gene expression and biofilm formation in Candida albicans isolated from vulvovaginal candidiasis. Adv. Biomed. Res. 5:105. doi: 10.4103/2277-9175.183666
Tits, J., Cools, F., De Cremer, K., De Brucker, K., Berman, J., Verbruggen, K., et al. (2020). Combination of Miconazole and Domiphen bromide is fungicidal against biofilms of resistant Candida spp. Antimicrob. Agents Chemother. 64, e01296–e01220. doi: 10.1128/AAC.01296-20
Wang, Y., Liu, Z., and Chen, T. (2024). Vaginal microbiota: potential targets for vulvovaginal candidiasis infection. Heliyon 10:e27239. doi: 10.1016/j.heliyon.2024.e27239
Workowski, K. A., Bachmann, L. H., Chan, P. A., Johnston, C. M., Muzny, C. A., Park, I., et al. (2021). Sexually transmitted infections treatment guidelines, 2021. MMWR Recomm. Rep. 70, 1–187. doi: 10.15585/mmwr.rr7004a1
Wu, X., Zhang, S., Li, H., Shen, L., Dong, C., Sun, Y., et al. (2020). Biofilm formation of Candida albicans facilitates fungal infiltration and Persister cell formation in vaginal candidiasis. Front. Microbiol. 11:1117. doi: 10.3389/fmicb.2020.01117
Keywords: biofilm, recurrent vulvovaginal candidiasis, pathogenesis, biomass, metabolic activity
Citation: Díaz-Navarro M, Irigoyen-von-Sierakowski Á, Delcán I, Monte A, Palomo M, Escribano P, Guinea J, Burillo A, Galar A, Muñoz P and Guembe M (2025) New insights in the role of Candida biofilm in the pathogenesis of recurrent vulvovaginal candidiasis: a prospective clinical study. Front. Microbiol. 16:1566171. doi: 10.3389/fmicb.2025.1566171
Edited by:
Alina Maria Holban, University of Bucharest, RomaniaReviewed by:
Guillermo Quindós, University of the Basque Country, SpainCopyright © 2025 Díaz-Navarro, Irigoyen-von-Sierakowski, Delcán, Monte, Palomo, Escribano, Guinea, Burillo, Galar, Muñoz and Guembe. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: María Guembe, bWFyaWFndWVtYmVAaG90bWFpbC5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.