
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Microbiol., 07 May 2024
Sec. Antimicrobials, Resistance and Chemotherapy
Volume 15 - 2024 | https://doi.org/10.3389/fmicb.2024.1379209
 Neda Shadvar1,2,3†
Neda Shadvar1,2,3† Sousan Akrami4†
Sousan Akrami4† Seyyed-Mohammad-Amin Mousavi Sagharchi5Rafee Habib Askandar6Alireza Merati7Masoomeh Aghayari8Nikki Kaviani9
Seyyed-Mohammad-Amin Mousavi Sagharchi5Rafee Habib Askandar6Alireza Merati7Masoomeh Aghayari8Nikki Kaviani9 Hamed Afkhami10,11*Mojtaba Kashfi10,12*
Hamed Afkhami10,11*Mojtaba Kashfi10,12*Gastric ulcers and gastric cancer are brought on by the Helicobacter pylori bacteria, which colonizes under the stomach mucous membrane. Different medication regimens are used to remove it, but the illness returns and becomes more resistant, which lowers the treatment rates. Additionally, this bacterium now exhibits a skyrocketing level of multi-drug resistance, necessitating recurrent therapeutic treatments. The negative effects of synthetic medications in comparison to conventional therapies are another significant factor in favor of non-pharmacological therapy. The most significant side effects of popular anti-gastric ulcer medications include nausea, vomiting, and diarrhea. Stomach ulcers have previously been treated with herbal remedies and complementary treatments like probiotics. When probiotics are ingested, the host experiences several advantages that may be brought about by altering the bacterial flora in the digestive system. Additionally, stronger-acting chemical compounds and plant extracts can be employed to treat patients. In this article, we look at the substances and medications that are utilized in place of synthetic stomach ulcer-curing treatments.
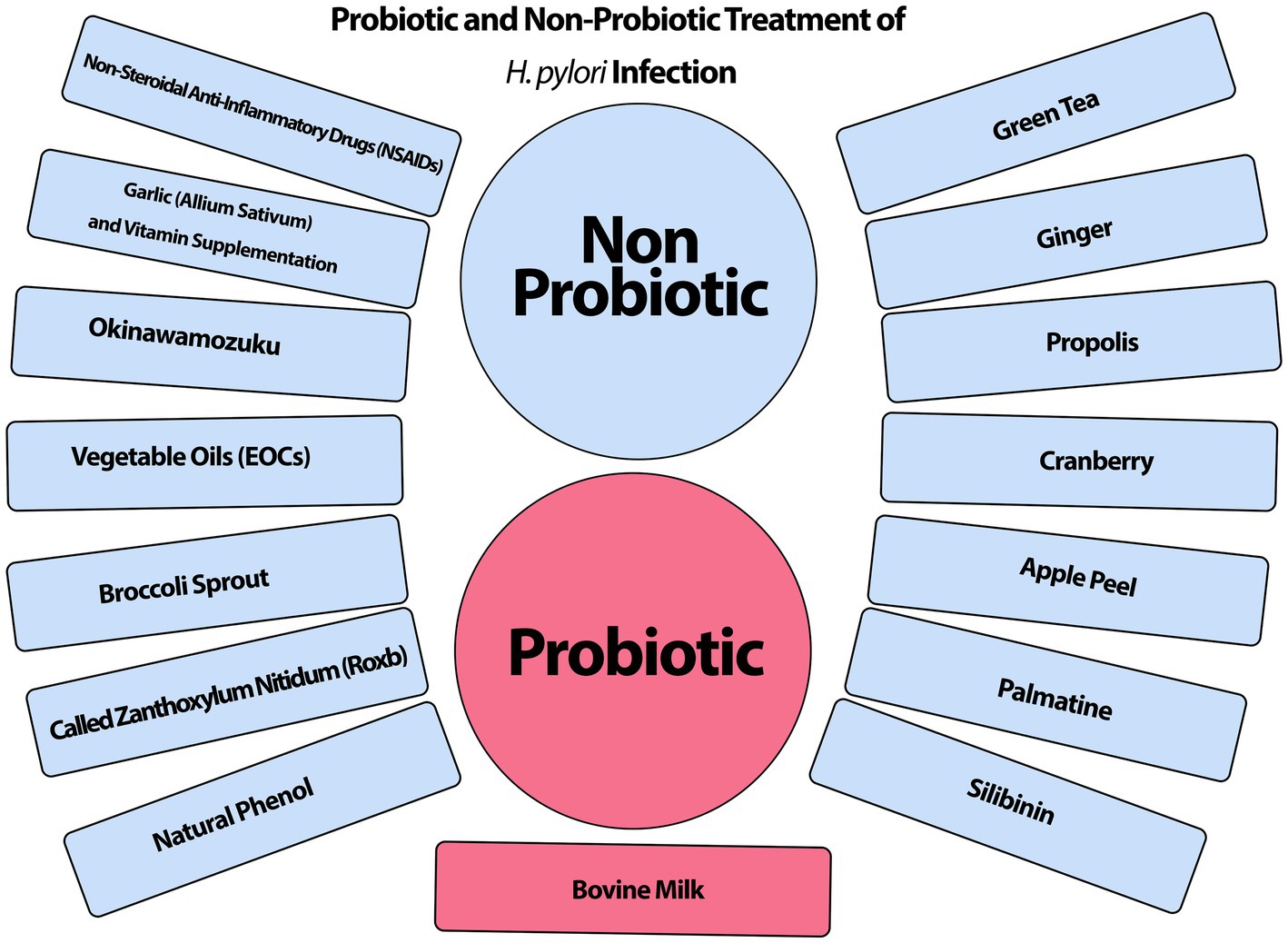
Graphical Abstract. Non-antibiotic treatment for Helicobacter pylori.
Helicobacter pylori (H. pylori) is a gram-negative bacterium, with a curved shape, flagellated. Several virulence factors are known in this bacterium that are involved in the process of pathogenesis, resistance to acid, drug resistance, and damage to the host (Ansari and Yamaoka, 2020; Sukri et al., 2020; Kolinjivadi et al., 2022). Flagella greatly increases the penetration power of bacteria into the submucosa of the stomach, which is important in bacterial pathogenesis (Baj et al., 2020; Khaledi et al., 2020; Afra et al., 2021). Other factors, such as the urease enzyme, are responsible for the survival of bacteria in the acidic conditions of the host’s stomach (Yang et al., 2023). Two other virulence factors include cagA and vacA are closely related to the occurrence of gastric cancer. Cytotoxin-Associated Gene A (CagA) is found in strains with high virulence that EPIYA (glutamic acid-proline-isoleucine-tyrosine-alanine) region in CagA, plays a significant role (Noiri and Nagata, 2023; Wang et al., 2023). VacA is a multifunctional toxin that is responsible for eliciting multiple effects on host cells (Salvatori et al., 2023). Helicobacter pylori is known to cause asymptomatic gastritis to chronic gastritis which, if left untreated, may lead to stomach ulcers, MALT (mucosa-associated lymphoid tissue lymphoma), and stomach cancer (Salama, 2020; Aumpan et al., 2023; Messina et al., 2023). Helicobacter pylori infection is thought to be acquired during early childhood by oral-oral or fecal-oral transmission channels and typically lasts a lifetime. Spontaneous clearance without encountering antibiotics is rare (Engelsberger et al., 2024). This bacterium is responsible for infecting approximately 4.4 billion people on Earth and 9% of all cancer-related deaths are associated with H. pylori (Savoldi et al., 2018). About 15%–25% of individuals in developed countries and up to 70%–90% of people in developing countries are infected with this bacterium (Fang et al., 2019; Abo-Amer et al., 2020). In some parts of the world, the prevalence of this disease and recrudescence is very high. Moreover, in parts of South America and China, and Eastern European about 80% or more have been documented (Choi et al., 2019; Qureshi et al., 2019; Sun and Zhang, 2019). The conventional therapy for H. pylori infection is proton pump inhibitors (PPIs) coupled with two antibiotics and bismuth (Savoldi et al., 2018). However, the development of antibiotic resistance has grown in recent years, resulting in a drop in H. pylori eradication rates. Furthermore, antibiotics may cause negative effects on the human gastrointestinal tract, such as diarrhea, anorexia, emesis, abdominal distension, and discomfort (Poonyam et al., 2019). As a result, there is a rising need for alternate medications to manage H. pylori infection successfully. Plant extract and probiotic-based foods are becoming increasingly popular. These innovative treatments are effective against H. pylori infection. This study includes a thorough assessment of the global prevalence, transmission pathways, and pathophysiology of H. pylori infection, as well as an overview of phytotherapy, probiotics, and new therapeutics, including their potential actions against H. pylori.
The data and literature were searched in the databases SID, Irandoc, Magiran, Google Scholar, Web of Science, PubMed, and Scopus using the keywords H. pylori, alternative therapy, and non-pharmacological treatment from 2003 to 2023. This collection yielded various non-antibiotic therapeutic options, including probiotic therapy and non-probiotic product therapy.
Antimicrobial susceptibility testing (AST) and antibiotic resistance associated with geographical region should be taken into consideration when choosing the best regimen. In certain nations, a treatment regimen based on recommendations and the use of multiple medications (hybrid therapy) may be carried out concurrently for 10–14 days or more (Graham, 2015). In the past, triple therapy by combination of two antibiotics including clarithromycin and amoxicillin and plus one proton pump inhibitor (Di Fermo et al., 2020) such as omeprazole was considered the acceptable first-line regimen (Abadi, 2017; Chey et al., 2017; Malfertheiner et al., 2022). Second-line antibiotics were utilized because bacteria showed significant levels of resistance to first-line medications (Thung et al., 2016). Quadruple therapy by bismuth quadruple therapy (BQT), metronidazole, tetracycline, and omeprazole in some countries like the United States of America and Europe is suggested (Poonyam et al., 2019; Zama et al., 2020).
Patients frequently experience the need to repeat treatments, or complications from the disease reappear months or years after treatment. Helicobacter pylori can overcome environmentally stressed conditions, such as sub-inhibitory drug concentrations or a non-permissive atmosphere, by entering the viable but nonculturable (VBNC) state, in which the microorganism modifies its morphology from a spiral to a coccoid (spherical) form with a loss of cultivability (Cellini, 2014). Chaput et al. (2006) revealed that H. pylori coccoid cells can avoid detection by the immune system due to a considerable change of the cell wall peptidoglycan, which has no IL-8 stimulatory action in gastric epithelial cells. Thus, in the VBNC condition, H. pylori may be able to evade or regulate the host response, allowing it to survive in the human stomach. Wang and Wang (2004) created a coccoid H. pylori population by exposing these cells to a sub-inhibitory dosage of antibiotics, after which the target segment of the cagA gene was amplified, cloned into a plasmid, and transformed in Escherichia coli. The scientists used sequence analysis to show that coccoid H. pylori carried a full cagA gene with 99.7% similarity to the reported original sequence of vegetative forms of H. pylori, confirming conjecture regarding the pathogenicity of these cells. These considerations clearly emphasize that the morphological fickleness of H. pylori occurs in reaction to external stimuli entering the VBNC stage, and represents, over the lifespan of the microorganism, a potent response to promote bacterial “fitness” and species preservation. This critical survival strategy is reinforced when bacterial cells arrange themselves into microbial communities, generating a kind of “free multicellularity” and forming biofilm (Bessa et al., 2013). Helicobacter pylori is well recognized for its ability to create biofilm both outside and within the human host, which presumably provides greater protection under stressful situations. Bessa et al. (2013) found that sub-minimal Inhibitory Concentration (MIC) levels of amoxicillin and clarithromycin might enhance biofilm biomass. The influence of sub-MIC drugs on H. pylori biofilm-forming capability may have clinical implications, as during any antibiotic treatment focused on a specific infection, H. pylori bacteria can be exposed to sub-MICs of antibiotics, which can stimulate the switching from planktonic to sessile cells forming biofilm, resulting in recalcitrance to antibiotic treatment and thus preventing eradication. According to a recent thorough meta-analysis of 132 research (53,934 person-years) from 45 nations or regions, the global yearly reinfection rate of H. pylori was 3.1%, which has been generally consistent over the previous three decades but varied across different locations (Hu et al., 2017). One of the most important causes of treatment failure is multiple resistance to common drugs, which may repeat the course of treatment several times or use alternative drugs (Shah et al., 2021; Wallner et al., 2022). Some studies worldwide have shown that prevalence primary multidrug-resistant (MDR) H. pylori is increasing (Karbalaei et al., 2022). It has been reported that metronidazole resistance grew by nearly 50% in China over 14 years, from 2000 to 2014. Furthermore, during the same period in China, the clarithromycin resistance rate jumped from 14.8% to 52.6% (Thung et al., 2016). In this century, antibiotic resistance to metronidazole, amoxicillin, and clarithromycin has increased significantly (Adachi et al., 2023; Rokkas and Graham, 2023). Clarithromycin has emerged as the foundation for H. pylori treatment in combination therapy because of its minor effect on stomach acidity, low threshold inhibitory concentration, and reasonably excellent mucosal diffusion (Marques et al., 2020). In developing nations, clarithromycin resistance and the frequency of re-infection contribute to the high global incidence of H. pylori infection and consequent inflammatory and neoplastic diseases (Alarcón-Millán et al., 2016). In most European nations and the rest of the world, the prevalence of clarithromycin resistance has reached 20% (Morilla et al., 2019). The discrepancy in clarithromycin resistance rates among the included studies might be attributed to a variety of factors, including variances in antibiotic prescription rates across geographic areas, the use of different breakpoints or erroneous criteria in conducted research, and the introduction of MDR strains. In a comprehensive review of the literature in Iran, H. pylori resistance to several antibiotics, including metronidazole, clarithromycin, amoxicillin, tetracycline, ciprofloxacin, levofloxacin, furazolidone, was 61.6%, 22.4%, 16.0%, 12.2%, 21.0%, 5.3%, and 21.6%, respectively (Khademi et al., 2015). Helicobacter pylori resistance to metronidazole is far higher in Iran than in industrialized nations. Helicobacter pylori resistance to fluoroquinolones (i.e., ciprofloxacin, moxifloxacin, trovafloxacin, and levofloxacin), nitrofurans (i.e., furazolidone), and rifamycins (i.e., rifabutin) is 0% to 20%, 0% to 5%, and 0% to 2%, respectively, in different geographic locations of the world (Hosseini et al., 2012). Antibiotic resistance is minimal in Middle Eastern nations (Khademi et al., 2015). In recent years, furazolidone has been considered a good alternative to metronidazole and tetracycline in quadruple therapy for eradication of H. pylori in Iran, but at the moment, the resistance of H. pylori to furazolidone is detected in 21.6% of cases, which is higher than the global average (Khademi et al., 2015). Resistance rates for rifabutin were 0.0, 6.4% for amoxicillin, 17.4% for clarithromycin, and 43.6% for metronidazole in the largest clinical trial of H. pylori antimicrobial susceptibility in more than 15 years, conducted in 20 states in the United States. The dual resistance rate to metronidazole and clarithromycin was 10.5% (Mestrovic et al., 2020). As treating H. pylori is never an emergency, choosing a regimen based on local susceptibility patterns or, ideally, the susceptibility profile of an individual’s infecting strain would be a better approach, as it would prevent patient exposure to antimicrobials that are ineffective against a resistant H. pylori strain. According to the research, it appears that in addition to antibiotic therapy, it is preferable to employ additional therapies such as probiotics, plant extracts, and any effective combination against H. pylori.
Probiotics are living bacteria that provide several advantages to the body and are used orally to treat gastrointestinal problems (Losurdo et al., 2018). Probiotic preparations are available in a variety of formats, including capsules, solutions, powders, and probiotic foods (Kiepś and Dembczyński, 2022). Probiotics have a lot of potential as antibiotic replacements. Following the investigation by Yoon et al. (2019), a reduction in H. pylori density and histologic inflammation improvement could be detected in individuals treated with fermented milk containing Lactobacillus paracasei HP7 and herbal extract (Glycyrrhiza glabra). In a randomized double-blind placebo-controlled clinical trial, the decrease in the mean H. pylori stool antigen titer showed a significant difference between Saccharomyces boulardii and the control group, indicating that S. boulardii could positively reduce H. pylori colonization in the human gastrointestinal system, but it is incapable of eradication as monotherapy (Namkin et al., 2016). As a result, probiotic monotherapy cannot be utilized to treat H. pylori, even though it may suppress bacterial growth. Probiotics have a good influence on digestive health, reinforce the mucosal barrier on mucus against pathogens, improve immune system, and anti-pathogen action via antimicrobial factor release, aggregation and co-aggregation by attachment to pathogens (Agraib et al., 2021; Keikha and Karbalaei, 2021; Daelemans et al., 2022; Du et al., 2022). In addition, probiotics are used in the treatment of gastrointestinal cancer (Zhang et al., 2021). Clinical experiments have shown that probiotic lactic acid-producing bacteria are a simple, safe, and effective way to prevent cancer patients against radiation-induced diarrhea. Patients with colorectal cancer were randomly assigned to take L. rhamnosus GG supplements and fiber throughout treatment. Patients who took Lactobacillus experienced less grade 3 or 4 diarrhea, reported less abdominal discomfort, required less hospitalization, and had fewer chemotherapy dosage decreases owing to bowel damage. There was no Lactobacillus-related harm found (Delia et al., 2007; Österlund et al., 2007). The study concludes that Lactobacillus GG supplementation is well tolerated and may minimize the incidence of severe diarrhea and abdominal pain associated with 5-FU-based chemotherapy. Generally, probiotics have been added to dairy products such as yogurt and other fermented products.
Lactobacillus and Bifidobacterium are the two most common species found in probiotic products such as yogurt (Xiong, 2018; Ye et al., 2020). In the past, the positive effects of dairy products such as yogurt on digestion were proven (Whiteside et al., 2021; Zhao et al., 2022). Other species accessible on the market include Bacillus spp., Enterococci, E. coli, Weissella spp., and Saccharomyces. Classical probiotic strains containing Lactobacilli and Bifidobacterium have been granted Generally Regarded as Safe (GRAS) status in the United States and are eligible for EFSA (European Food Safety Authority) safety certification. Microbial strains in multi-species probiotics include Bifidobacterium breve, Bifidobacterium infantis, Bifidobacterium longum, Eubacterium faecium, Lactobacillus acidophilus, Lactiplantibacillus plantarum, Lacticaseibacillus casei, and Streptococcus thermophilus. Researchers discovered that probiotic mixes including many strains outperformed single-strain probiotics in terms of pathogenic growth inhibition (Singh et al., 2022). These bacteria may colonize the human gastrointestinal tract and compete with H. pylori for attachment to the host’s mucous membrane (Espinoza et al., 2018). Lactobacillus secretes chemicals that inhibit H. pylori urease activity and colonization. Bifidobacterium reduces H. pylori adherence to intestinal mucus by site competition, and it has been found to lower IL 8 levels in vivo and in vitro H. pylori activity (Koca et al., 2021). In the Maastricht V Consensus Report, it has been agreed that some probiotic strains may have favorable effects on H. pylori elimination (Malfertheiner et al., 2017). Given these findings, it is plausible to expect that utilizing a combination of probiotics that act on H. pylori through diverse routes might result in a synergistic impact. Probiotics used in combination with antibiotics have been demonstrated in studies to improve Helicobacter eradication. When double probiotics were added to the medication, the number of significant adverse effects decreased by 11.2%. Helicobacter eradication was accomplished in 68% of patients in the control group and 89% of patients in the trial group following therapy completion. When double probiotics were added to the therapy, the eradication success rate improved by 21% (Koca et al., 2021). While H. pylori disturbs the normal flora in the stomach microbiota, antibiotic therapy causes a long-term decline in normal strains in the intestinal flora. Probiotics protect the intra-stomach microbiota against the detrimental effects of H. pylori and restore the degraded intestinal flora. Helicobacter pylori can cause an inflammatory response by altering the acid–base balance of the digestive system and, as a result, the gut microenvironment (Chen et al., 2018; Yoon et al., 2019). Hence probiotic supplementation may be beneficial in the treatment of inflammatory and infectious diseases (Chen et al., 2018). Figure 1 shows the use of probiotics in the digestive tract schematically. Epithelial commensals and probiotics promote barrier integrity. Probiotics play a significant function in maintaining immunological balance in the gastrointestinal system by interacting directly with immune cells. Probiotic strains increase IgA synthesis and secretion by altering the cytokine milieu in the gut mucosa. Also, bacteriocins are antimicrobial peptides generated by the majority of bacterial species. They have been thought to contribute to probiotic efficacy by assisting with colonization, direct pathogen eradication, and acting as signaling molecules to other bacteria or the host immune system.
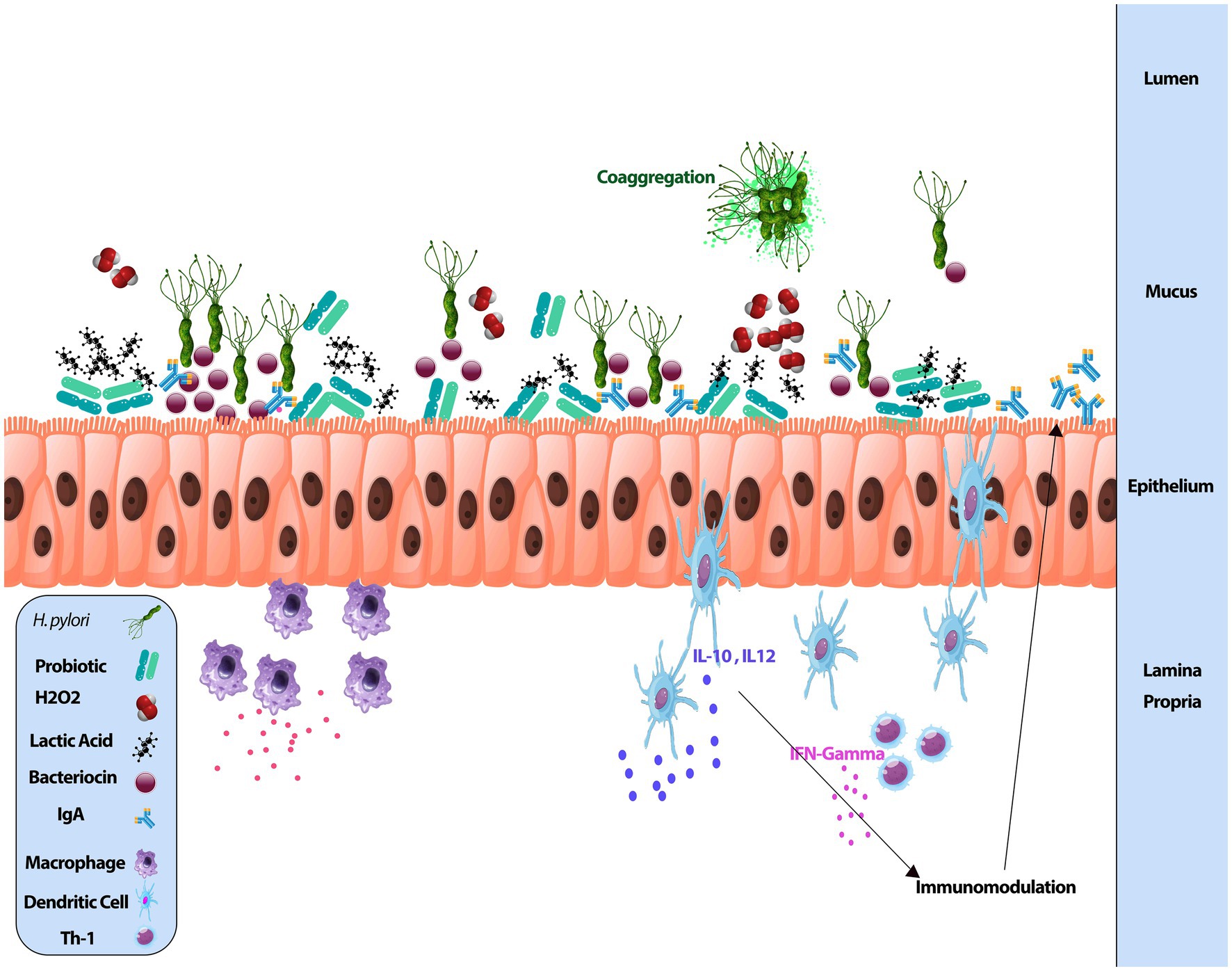
Figure 1. Probiotics in the digestive tract.
Probiotics have few adverse effects associated with bacterial-host interactions. Individuals suffering from immunodeficiency, heart valve disease, short bowel syndrome, or preterm newborns are at risk of severe responses and should avoid using these items (Doron and Snydman, 2015; Singhi and Kumar, 2016). Probiotic therapy is a first medication for H. pylori treatment in order to optimize eradication regimens and reduce antibiotic adverse effects (Chey et al., 2017). As H. pylori has long been seen as a difficult-to-treat disease, due mostly to developed resistance to routinely used antibiotics, there is a rising interest in using probiotics in combination with antibiotic regimens to remove the bacteria. Certain Lactobacillus species produce antibacterial chemicals similar to the bacteriocin class. Bacteriocins are proteinaceous toxins with anti-H. pylori properties. They are tiny, dialyzable peptide structures that possess antibacterial properties. The antibacterial activity of the bacteriocins differed depending on the H. pylori strain and the kind of bacteriocin generated by Lactobacillus sp. Some bacteriocins exhibit more antibacterial action against H. pylori strains than others (Kim et al., 2003). Based on clinical trials with probiotics against H. pylori, probiotics cannot be considered an alternative to anti-H. pylori treatment; however, their use together with standard anti-H. pylori treatment may improve H. pylori treatment by increasing eradication rates while decreasing the adverse effects of current medications. Lactobacillus acidophilus was a little better choice for 7- and 14-day triple therapy, whereas S. boulardii was better suited to 10-day triple therapy. When combined with H. pylori eradication medication, most probiotic regimens proved to be more successful than placebos. Additionally, probiotics are indicated to enhance triple treatment in kids. To augment triple treatment, L. casei was discovered as the best for H. pylori eradication rates, and multi-strain of L. acidophilus and L. rhamnosus for overall adverse effects (Feng et al., 2017; Wang et al., 2017). While it may be generally acknowledged that probiotics may help in the eradication of H. pylori and reduce adverse effects of standard therapy, certain probiotic bacteria species can also benefit pharmacotherapy. The growing prevalence of antibiotic resistance and the decrease in patient compliance with traditional treatment further illustrate the need for alternative therapies. Fakhry et al. (2023) found that patients who received probiotics (Lactobacillus and Bifidobacterium) in addition to regular medicine (triple treatment) had a higher percentage of H. pylori eradication than those who received only conventional therapy. Adding probiotics reduced diarrhea as a side effect of antibiotic treatment. Probiotics may help to repair gut dysbiosis, as demonstrated by stool PCR for Lactobacilli and Bifidobacteria before and following drugs. Probiotic supplements may assist to reestablish a favorable gut microbial composition, especially following eradication treatment.
The composition of the human gastrointestinal microbiota tract has been extensively examined, and various studies have been undertaken to explain the links between microbiota diversity in the human gastrointestinal tract and its impact on health and illness. Differences in gastric bacterial community topologies may govern diverse pathways, affecting stomach physiology and leading to varied H. pylori infection responses (Ge et al., 2018). Commensal gastric microorganisms or their metabolites impact H. pylori’s capacity to colonize the stomach and its pathogenic and carcinogenic potential via influencing host immune responses (Espinoza et al., 2018). Non-H. pylori bacteria may survive as an antigenic stimulation or form a partnership with H. pylori to increase eventual inflammation (Rook et al., 2017). Studies discovered that stomach microbial populations considerably enhanced their alpha-linolenic acid and arachidonic acid metabolism. Therefore, Zheng et al. (2021) hypothesized that the balance between Treg and Th17 cells might be biased toward Treg cells, which is beneficial to bacterial persistence, and the gastric microbiota might generate short-chain fatty acids and small molecules to modulate mucosal Treg responses in H. pylori-infected patients. Furthermore, Satoh-Takayama et al. (2020) demonstrated that ILC2s, controlled by local commensal populations through IL-7 and IL-33 upregulation, are the main ILC subset in the stomach and protect against H. pylori infection via B-cell activation and IgA production.
Probiotics can change the structure of the stomach microbiota. Probiotic therapy increased the amount of beneficial short-chain fatty acid (SCFA) generating bacteria, including Bacteroides, Alloprevotella, and Oscellibacter, in the stomachs of H. pylori-infected mice (He et al., 2022). Sodium butyrate, a typical SCFA, suppressed H. pylori growth, CagA and VacA expression, as well as the host NF-κB pathway by lowering toll-like receptor expression in host cells, resulting in decreased TNF-α and IL-8 production (Huang et al., 2021). However, another bacterial metabolite, trimethylamine N-oxide (TMAO), boosted H. pylori viability and virulence and aggravated H. pylori-induced inflammation (Wu et al., 2020). The synergistic effects of H. pylori and TMAO boosted inflammation-related gene expression, including IL-6, CXCL1, CXCL2, FOS, and complement C3 in the gastric epithelium (Wu et al., 2017). Trimethylamine (TMA) is the TMAO precursor. Firmicutes (e.g., Staphylococcus) are the primary producers, while Bacteroidetes generate it infrequently (Fennema et al., 2016). Overall, probiotics may raise the proportion of helpful metabolite-producing bacteria and/or lower the number of detrimental metabolite-producing bacteria (Zhang et al., 2023). Probiotics can help repair the stomach dysbiosis produced by eradication therapy, however, young adults infected with H. pylori may not need to take probiotics alone (Yuan et al., 2021).
Synbiotics are a mix of probiotics (“live microorganisms that, when administered in adequate amounts, confer a health benefit on the host”) and prebiotics (“indigestible foods that lead to enhancement of probiotic bacteria colonization in the gut”) that can operate synergistically. Several studies have found that some probiotic lactobacilli exhibit anti-H. pylori action and prevent H. pylori colonization in gastric cell lines (Pourmasoumi et al., 2019). A randomized, open-labeled trial examined the efficacy of a synbiotic combination (containing lactobacillus, enterococcus, and bifidobacterium) in clarithromycin-based triple eradication treatment for H. pylori. The data showed no significant difference between the two groups. However, the level of adverse effects and rates of eradication differed considerably between groups. The eradication rate in the synbiotic group was 88.4%, compared to 68.8% in the control group. The inclusion of synbiotics in triple treatment reduces the incidence of antibiotic-related adverse effects. It also improves H. pylori eradication in clarithromycin-based triple treatment (Sahin et al., 2013). A meta-analysis of six randomized controlled studies revealed that synbiotics could increase H. pylori eradication rates while reducing side effects (Pourmasoumi et al., 2019).
A novel biotherapeutic technique includes using microbial bioactive compounds (postbiotics) that display optimal compatibility and intimate interaction with the host’s immune system (Hosseini et al., 2023). Postbiotics can also compete with pathogens for adhesion sites if their adhesions (such as fimbriae and lectins) are still functional after pretreatment. Lactobacillus acidophilus in lyophilized and inactivated form significantly boosts H. pylori eradication rates when added to a standard anti-H. pylori regimen, owing to its strong adhesion to human intestine absorptive and mucous-secreting cells. Given its safety and high patient compliance, it is a simple addition to traditional anti-H. pylori antibiotic treatments (Ma et al., 2023). There is scant evidence that postbiotics are effective in treating human diseases. We uncovered two separate clinical studies using postbiotics for H. pylori infection. Canducci et al. (2000) found that treating patients with H. pylori with clarithromycin, rabeprazole, and amoxicillin with inactivated Lactobacillus acidophilus increased the rate of eradication. Yang et al. found that adding nonviable L. reuteri to triple therapy (esomeprazole, amoxicillin, and clarithromycin) did not increase the rate of H. pylori eradication, but did help to establish a beneficial microbial profile and reduce the occurrences of abdominal distention and diarrhea (Hamzavi and Bashiri, 2023).
The positive benefits of probiotics are well recognized, but other components such as plant extracts, oils, and derivatives of some natural chemicals can help reduce pathogenesis and cancer growth.
Nonsteroidal anti-inflammatory drugs (NSAIDs) such as acetaminophen, ibuprofen, diclofenac, and acetyl Salic acid are among the most commonly used antibacterial agents in the world (Zimmermann and Curtis, 2017). Salicylic acid (SAL) has been proven in studies to reduce the growth of H. pylori and Klebsiella pneumonia (Reshetnyak et al., 2019). Other NSAIDs can have an effect on bacteria; for example, ibuprofen can reduce the binding of Escherichia coli to intestinal epithelial cells or uroepithelial cells (Whiteside et al., 2019; Figure 2). Another study published in 2018 found that diclofenac loaded with chitosan nanoparticles may inhibit the growth of S. aureus and B. subtilis (Alqahtani et al., 2019). Resveratrol (RSV) and its derivatives are a kind of natural phenol with anti-inflammatory and antibacterial properties (Vestergaard and Ingmer, 2019). RSV works by inhibiting the urease enzyme and, as a result, preventing the formation of an alkaline environment (Marini et al., 2019; Krzyżek et al., 2020). Several investigations have demonstrated that anti-helicobacter drugs such as levofloxacin have higher bacterial toxicity when combined with Resveratrol and its derivatives (Bouarab Chibane et al., 2019; Di Lodovico et al., 2019; Di Fermo et al., 2020). Polaprezinc (PZN) or zinc carnosine (L-carnosine) are zinc chelate compounds that protect the digestive mucosa (Mahmoud et al., 2022). This antioxidant compound is particularly efficient in protecting against H. pylori and promoting ulcer healing, and unlike other antibiotics, it does not cause drug resistance (Teng et al., 2020; Ibrahim et al., 2022; Mahmoud et al., 2022). PZN has been shown in several trials to be useful in reducing apoptosis and inflammation, healing skin and stomach wounds, and preserving tight junctions (Furihata et al., 2020; Ibrahim et al., 2022). Hence, this substance may be introduced later in the H. pylori treatment protocol (Kawahara et al., 2018; Mahmoud et al., 2022). Palmatine (Pal) is a herbal combination derived from Coptidis Rhizoma that may relieve or diminish chronic atrophic gastritis (CAG) caused by H. pylori. Pal most likely does this by suppressing inflammatory compounds including interleukin 8 (IL-8) and chemokine 16 (CXCL-16; Chen et al., 2020). Silibinin, derived from milk thistle seeds, possesses potent anti-Helicobacter and anti-gastric tumor cell properties (Bittencourt et al., 2020). This chemical affects Penicillin Binding Protein (PBP) and interferes with wall formation, resulting in changes in the bacterial structure. It also has anti-inflammatory properties by decreasing cytokine release by inhibiting macrophages activated by H. pylori (Bittencourt et al., 2020; Cho et al., 2021). Vergara et al. (2005) found that eradicating H. pylori was successful in NSAID-naive users but not in chronic users.
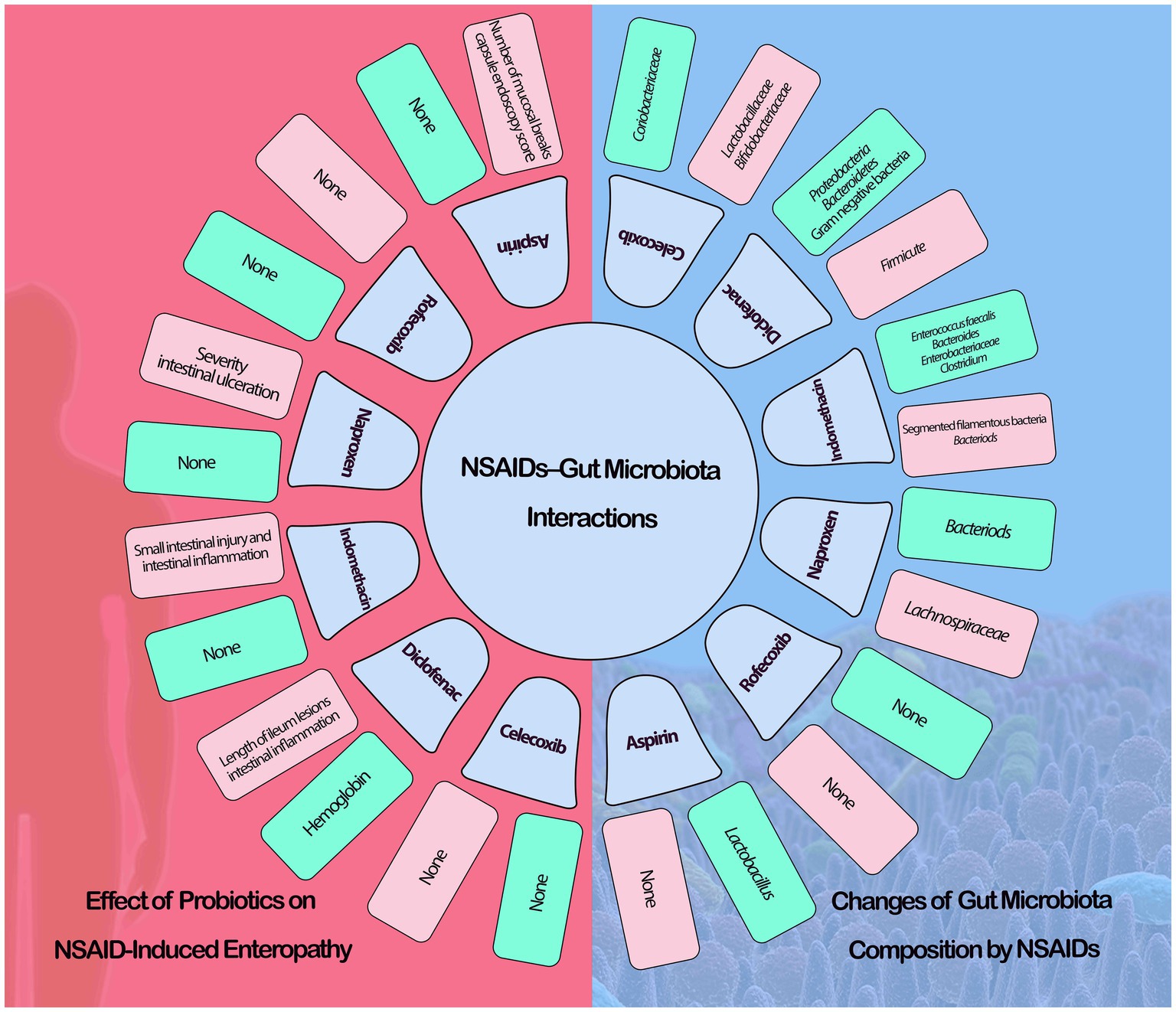
Figure 2. NSAIDs-gut microbiota interactions (green: increase, red: decrease).
Some foods, edible plants, and natural dairy products exhibit antibacterial characteristics in vitro or in vivo, including H. pylori. Most of these drugs’ effective composition is known (Takeuchi et al., 2014). The most well-known compounds that are effective against bacteria that cause stomach ulcers include bovine milk (by Lactoferrin), ginger (6-shogaol or phenolic acids), broccoli sprout (sulforaphane), green tea (Catechin compounds), and garlic (Allicin, diallyl sulfur components; Cellini et al., 1996; Sachdeva and Nagpal, 2009; Sachdeva et al., 2014; Omar et al., 2020; Zhao et al., 2022). In vitro tests showed that bovine lactoferrin (bLF) had a strong antibacterial impact on resistant H. pylori and a synergistic antibacterial effect when paired with clarithromycin. Furthermore, in vivo investigations indicated that bLF might enhance the degree of gastric mucosa damage and minimize the area of the stomach ulcer (Wang et al., 2023). According to the findings of researchers, the methanolic extract of ginger, which contains gingerol, zingiberene, and thymol as major compounds, has potential antibacterial and antibiofilm properties against various multidrug-resistant clinical isolates of H. pylori, as well as anti-inflammatory activity. The results mentioned demonstrate a considerable improvement of gentamicin effectiveness against multidrug-resistant H. pylori when combined with methanolic ginger extract (Elbestawy et al., 2023). To find out if regular broccoli sprout consumption had a similar effect in humans, researchers enrolled 50 H. pylori-infected individuals in a clinical trial. When measurements obtained at baseline were compared with those taken after one or 2 months of intervention, significant decreases in the number of bacteria were evident in individuals eating broccoli sprouts (Tuma, 2006). Yanagawa et al. (2003) demonstrated that epigallocatechin-3-gallate (from green tea) enhanced the antibacterial activity of an antibiotic treatment, with excellent efficacy against H. pylori growth in vitro. García et al. (2023) found that solvent-free garlic extracts containing ethanol and acetone suppressed H. pylori development in vitro under simulated stomach PH conditions at human body temperature. These results imply potentially major medicinal uses of such extracts, which eliminate the usage of proton pump inhibitors during the treatment of H. pylori infections in human patients.
Bactericidal, antitoxin, and antibiofilm properties of vitamin and garlic supplements can protect those at risk of stomach cancer (Li et al., 2019; Bhatwalkar et al., 2021). Garlic contains chemicals that protect the genome structure by suppressing reactive oxygen and radical scavenging (Vega-Hissi et al., 2019). According to these findings, food and other consumable things should be used in combination with antibiotics (Takeuchi et al., 2014). Numerous plants and vegetable oils, such as Chinese chive, are being studied, although the mechanism of action is unknown (Guerra-Valle et al., 2022). Some research has revealed that essential oil components (EOCs) have anti-H. pylori potential, and their mode of action is through immobilized antimicrobials (Ruiz-Rico et al., 2020). Table 1 lists the most important chemicals found in foods and spices, as well as the known mechanisms involved in anti-H. pylori action.
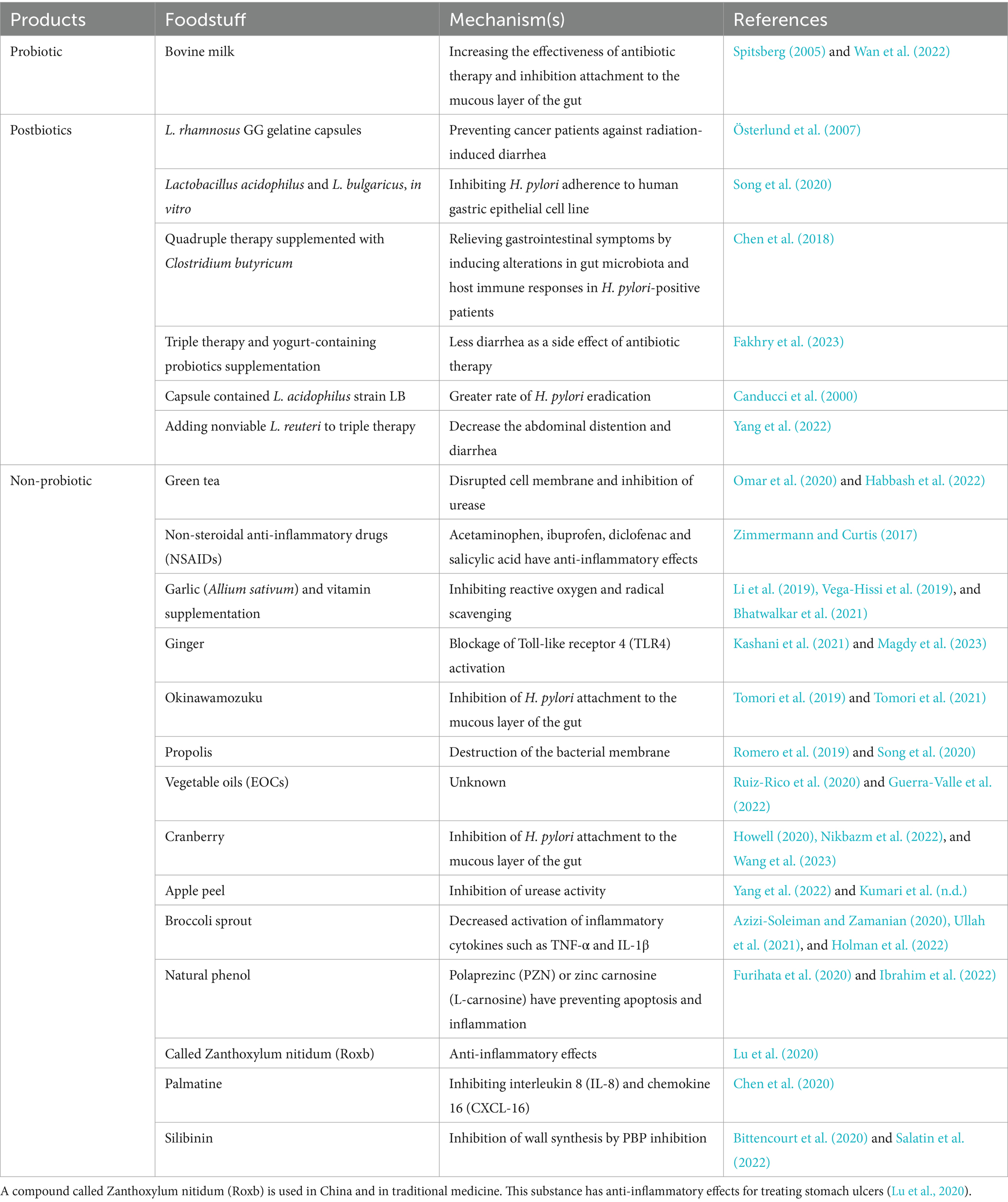
Table 1. Anti-Helicobacter pylori chemicals found in foods.
Failure to treat H. pylori infection can result in gastric cancer; also, the bacterium has a lot of resistance and the diversity of disorders caused by H. pylori will become more apparent with time, requiring the development of stronger or other treatments. The side effects of medications, as well as the problems that patients experience during or after therapy, motivate us to develop treatments with fewer negative effects. Treatment is complex and has several limits due to bacteria’s strong resistance to drugs. Much research in the field of herbal medicines and natural goods has been completed, indicating that therapy should be done concurrently with chemical treatment and natural and effective products. Combination therapy, as well as the use of probiotics and micronutrients such as vitamin C, vitamin B12, vitamin E, and iron in H. pylori-infected persons, appear to be useful in the eradication of H. pylori. Probiotics reduce adverse effects and increase antibiotic effectiveness, most likely because they mirror the function of the human microbiome. Postbiotics can also eradicate infections through competition for adhesion sites. Lactobacillus acidophilus in lyophilized and inactivated form significantly boosts H. pylori eradication rates when added to a routine anti-H. pylori eradication regimen, due to its powerful adherent capacity to human intestine absorptive and mucous-secreting cells. As a result, novel drugs and other treatments for the condition should be developed as quickly as possible.
NS: Writing – original draft, Data curation. SA: Writing – original draft, Data curation SMA.MS: Writing – original draft, Data curation. RHA: Writing – review & editing. AM: Writing – review & editing. MA: Writing – review & editing. NK: Writing – review & editing. HA: Methodology, Project administration, Supervision, Writing – review & editing. MK: Methodology, Project administration, Supervision, Writing – review & editing, Data curation, Software, Writing – original draft.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abadi, A. T. B. (2017). Helicobacter pylori treatment: new perspectives using current experience. J Glob Antimicrob Resist 8, 123–130. doi: 10.1016/j.jgar.2016.11.008
Abo-Amer, Y. E.-E., Sabal, A., Ahmed, R., Hasan, N. F. E., Refaie, R., Mostafa, S. M., et al. (2020). Relationship between Helicobacter pylori infection and nonalcoholic fatty liver disease (NAFLD) in a developing country: a cross-sectional study. Diabetes Metab Syndr Obes 13, 619–625. doi: 10.2147/DMSO.S237866
Adachi, K., Kato, S., Koshino, A., Nagao, K., Sugiyama, T., Yoshimine, T., et al. (2023). A Vonoprazan, clarithromycin, and metronidazole regimen as Helicobacter pylori eradication therapy for patients with penicillin allergy in light of clarithromycin resistance. Intern. Med. 62, 2301–2306. doi: 10.2169/internalmedicine.0789-22
Afra, L. G., Afkhami, H., Khaledi, M., Fathi, J., Taghadosi, R., Hoseini, M. H. M., et al. (2021). Detection of H. pylori in tissues with benign prostatic hyperplasia isolates from hospitalized patient in Qom, Iran. Gene Rep 23:101193. doi: 10.1016/j.genrep.2021.101193
Agraib, L. M., Yamani, M. I., Rayyan, Y. M., Abu-Sneineh, A. T., Tamimi, T. A., Tayyem, R. F. J. D. M., et al. (2021). The probiotic supplementation role in improving the immune system among people with ulcerative colitis: a narrative review. Drug Metab Pers Ther. 23:000010151520210150. doi: 10.1515/dmdi-2021-0150
Alarcón-Millán, J., Fernández-Tilapa, G., Cortés-Malagón, E. M., Castañón-Sánchez, C. A., De Sampedro-Reyes, J., Cruz-del Carmen, I., et al. (2016). Clarithromycin resistance and prevalence of Helicobacter pylori virulent genotypes in patients from southern México with chronic gastritis. Infect. Genet. Evol. 44, 190–198. doi: 10.1016/j.meegid.2016.06.044
Alqahtani, F. Y., Aleanizy, F. S., El Tahir, E., Alquadeib, B. T., Alsarra, I. A., Alanazi, J. S., et al. (2019). Preparation, characterization, and antibacterial activity of diclofenac-loaded chitosan nanoparticles. Saudi Pharm J 27, 82–87. doi: 10.1016/j.jsps.2018.08.001
Ansari, S., and Yamaoka, Y. (2020). Helicobacter pylori virulence factor cytotoxin-associated gene a (cag a)-mediated gastric pathogenicity. Int. J. Mol. Sci. 21:7430. doi: 10.3390/ijms21197430
Aumpan, N., Mahachai, V., and Vilaichone, R. K. (2023). Management of Helicobacter pylori infection. JGH Open 7, 3–15. doi: 10.1002/jgh3.12843
Azizi-Soleiman, F., and Zamanian, M. (2020). Broccoli and Helicobacter Pylori: a systematic review. Complement Med J 10, 2–11. doi: 10.32598/cmja.10.1.440.1
Baj, J., Forma, A., Sitarz, M., Portincasa, P., Garruti, G., Krasowska, D., et al. (2020). Helicobacter pylori virulence factors—mechanisms of bacterial pathogenicity in the gastric microenvironment. Cells 10:27. doi: 10.3390/cells10010027
Bessa, L. J., Grande, R., Iorio, D. D., Giulio, M. D., Campli, E. D., and Cellini, L. (2013). Helicobacter pylori free-living and biofilm modes of growth: behavior in response to different culture media. APMIS 121, 549–560. doi: 10.1111/apm.12020
Bhatwalkar, S. B., Mondal, R., Krishna, S. B. N., Adam, J. K., Govender, P., and Anupam, R. (2021). Antibacterial properties of organosulfur compounds of garlic (Allium sativum). Front. Microbiol. 12:613077. doi: 10.3389/fmicb.2021.613077
Bittencourt, M. L. F., Rodrigues, R. P., Kitagawa, R. R., and Gonçalves, R. D. C. R. (2020). The gastroprotective potential of silibinin against Helicobacter pylori infection and gastric tumor cells. Life Sci. 256:117977. doi: 10.1016/j.lfs.2020.117977
Bouarab Chibane, L., Degraeve, P., Ferhout, H., Bouajila, J., and Oulahal, N. (2019). Plant antimicrobial polyphenols as potential natural food preservatives. J Soc Chem Industry 99, 1457–1474. doi: 10.1002/jsfa.9357
Canducci, F., Armuzzi, A., Cremonini, F., Cammarota, G., Bartolozzi, F., and Pola, P. (2000). A lyophilized and inactivated culture of Lactobacillus acidophilus increases Helicobacter pylori eradication rates. Aliment. Pharmacol. Ther. 14, 1625–1629. doi: 10.1046/j.1365-2036.2000.00885.x
Cellini, L. (2014). Helicobacter pylori: a chameleon-like approach to life. World J. Gastroenterol. 20, 5575–5582. doi: 10.3748/wjg.v20.i19.5575
Cellini, L., Di Campli, E., Masulli, M., Di Bartolomeo, S., and Allocati, N. (1996). Inhibition of Helicobacter pylori by garlic extract (Allium sativum). FEMS Immunol. Med. Microbiol. 13, 273–277. doi: 10.1111/j.1574-695X.1996.tb00251.x
Chaput, C., Ecobichon, C., Cayet, N., Girardin, S. E., Werts, C., Guadagnini, S., et al. (2006). Role of Ami a in the morphological transition of Helicobacter pylori and in immune escape. PLoS Pathog. 2:e97. doi: 10.1371/journal.ppat.0020097
Chen, X., Wang, R., Bao, C., Zhang, J., Zhang, J., Li, R., et al. (2020). Palmatine ameliorates Helicobacter pylori-induced chronic atrophic gastritis by inhibiting MMP-10 through ADAM17/EGFR. Acta Physiol. Pharmacol. Neerl. 882:173267. doi: 10.1016/j.ejphar.2020.173267
Chen, L., Xu, W., Lee, A., He, J., Huang, B., Zheng, W., et al. (2018). The impact of Helicobacter pylori infection, eradication therapy and probiotic supplementation on gut microenvironment homeostasis: an open-label, randomized clinical trial. EBioMedicine 35, 87–96. doi: 10.1016/j.ebiom.2018.08.028
Chey, W. D., Leontiadis, G. I., Howden, C. W., and Moss, S. F. (2017). ACG clinical guideline: treatment of Helicobacter pylori infection. Am. J. Gastroenterol. 112, 212–239. doi: 10.1038/ajg.2016.563
Cho, K., Lee, H. G., Piao, J.-Y., Kim, S.-J., Na, H.-K., and Surh, Y.-J. (2021). Protective effects of silibinin on Helicobacter pylori-induced gastritis: NF-κB and STAT3 as potential targets. J Cancer Prev 26, 118–127. doi: 10.15430/JCP.2021.26.2.118
Choi, Y. K., Ahn, J. Y., Won, S. H., Jung, K., Na, H. K., and Jung, K. W. (2019). Eradication rate of Helicobacter pylori reinfection in Korea: a retrospective study. J. Gastroenterol. Hepatol. 34, 1696–1702. doi: 10.1111/jgh.14639
Daelemans, S., Deseck, V., Levy, E. I., and Vandenplas, Y. (2022). Are pro-and/or synbiotics beneficial in Helicobacter pylori eradication therapy in children? A narrative review. Eur. J. Pediatr. 181, 3225–3234. doi: 10.1007/s00431-022-04523-7
Delia, P., Sansotta, G., Donato, V., Frosina, P., Messina, G., De Renzis, C., et al. (2007). Use of probiotics for prevention of radiation-induced diarrhea. World J. Gastroenterol. 13, 912–915. doi: 10.3748/wjg.v13.i6.912
Di Fermo, P., Di Lodovico, S., Amoroso, R., De Filippis, B., D’Ercole, S., Di Campli, E., et al. (2020). Searching for new tools to counteract the Helicobacter pylori resistance: the positive action of resveratrol derivatives. Antibiotics 9:891. doi: 10.3390/antibiotics9120891
Di Lodovico, S., Napoli, E., Di Campli, E., Di Fermo, P., Gentile, D., Ruberto, G., et al. (2019). Pistacia vera L. oleoresin and levofloxacin is a synergistic combination against resistant Helicobacter pylori strains. Sci. Rep. 9:4646. doi: 10.1038/s41598-019-40991-y
Doron, S., and Snydman, D. R. (2015). Risk and safety of probiotics. Clin. Infect. Dis. 60, S129–S134. doi: 10.1093/cid/civ085
Du, L., Chen, B., Cheng, F., Kim, J., and Kim, J. (2022). Effects of Helicobacter pylori therapy on gut microbiota: a systematic review and meta-analysis. Dig. Dis. 42, 102–112. doi: 10.1159/000527047
Elbestawy, M. K., El-Sherbiny, G. M., Moghannem, S. A., and Farghal, E. E. (2023). Antibiofilm, and anti-inflammatory activities of ginger extract against Helicobacter pylori. Microbiol. Res. 14, 1124–1138. doi: 10.3390/microbiolres14030075
Engelsberger, V., Gerhard, M., and Mejías-Luque, R. (2024). Effects of Helicobacter pylori infection on intestinal microbiota, immunity and colorectal cancer risk. Front. Cell. Infect. Microbiol. 14:1339750. doi: 10.3389/fcimb.2024.1339750
Espinoza, J. L., Matsumoto, A., Tanaka, H., and Matsumura, I. (2018). Gastric microbiota: an emerging player in Helicobacter pylori-induced gastric malignancies. Cancer Lett. 414, 147–152. doi: 10.1016/j.canlet.2017.11.009
Fakhry, S. M., Kandyl, M. A.-H., Hashish, A. F., Kandeel, W., El-Shenawy, A. M., El-Sayed, H. S., et al. (2023). Can probiotics play a role in Helicobacter pylori (H. pylori) eradication? Egypt. Liver J. 13:64. doi: 10.1186/s43066-023-00294-4
Fang, Y., Fan, C., and Xie, H. (2019). Effect of Helicobacter pylori infection on the risk of acute coronary syndrome: a systematic review and meta-analysis. Medicine 98:e18348. doi: 10.1097/MD.0000000000018348
Feng, J.-R., Wang, F., Qiu, X., McFarland, L. V., Chen, P.-F., Zhou, R., et al. (2017). Efficacy and safety of probiotic-supplemented triple therapy for eradication of Helicobacter pylori in children: a systematic review and network meta-analysis. Eur. J. Clin. Pharmacol. 73, 1199–1208. doi: 10.1007/s00228-017-2291-6
Fennema, D., Phillips, I. R., and Shephard, E. A. (2016). Trimethylamine and trimethylamine N-oxide, a flavin-containing monooxygenase 3 (FMO3)-mediated host-microbiome metabolic axis implicated in health and disease. Drug Metab. Dispos. 44, 1839–1850. doi: 10.1124/dmd.116.070615
Furihata, K., Tsuchikawa, M., Miwa, T., Naito, Y., Oba, K., and Sakagami, M. (2020). Efficacy and safety of polaprezinc (zinc compound) on zinc deficiency: a systematic review and dose–response meta-analysis of randomized clinical trials using individual patient data. Nutrients 12:1128. doi: 10.3390/nu12041128
García, M. T., Garcia-Vargas, J. M., Fernández, L. A. G., Cuevas, P., and Gracia, I. J. L. (2023). Garlic extracts: effect of pH on inhibition of Helicobacter pylori. Life 13:1434. doi: 10.3390/life13071434
Ge, Z., Sheh, A., Feng, Y., Muthupalani, S., Ge, L., Wang, C., et al. (2018). Helicobacter pylori-infected C57BL/6 mice with different gastrointestinal microbiota have contrasting gastric pathology, microbial and host immune responses. Sci. Rep. 8:8014. doi: 10.1038/s41598-018-25927-2
Graham, D. Y. (2015). Helicobacter pylori update: gastric cancer, reliable therapy, and possible benefits. Gastroenterology 148, 719–731.e3. e713. doi: 10.1053/j.gastro.2015.01.040
Guerra-Valle, M., Orellana-Palma, P., and Petzold, G. (2022). Plant-based polyphenols: anti-Helicobacter pylori effect and improvement of gut microbiota. Antioxidants 11:109. doi: 10.3390/antiox11010109
Habbash, F., Alalwan, T. A., Perna, S., Ahmed, N., Sharif, O., Al Sayyad, A., et al. (2022). Association between dietary habits and Helicobacter pylori infection among Bahraini adults. Nutrients 14:4215. doi: 10.3390/nu14194215
Hamzavi, Y., and Bashiri, H. (2023). The effect of quadruple therapy plus probiotics on Helicobacter Pylori eradication and antibiotic-associated side effects: a randomized placebo-controlled trial. J. Kerman Univ. Med. Sci. 27:7908. doi: 10.5812/jkums-137908
He, C., Peng, C., Xu, X., Li, N., Ouyang, Y., Zhu, Y., et al. (2022). Probiotics mitigate Helicobacter pylori-induced gastric inflammation and premalignant lesions in INS-GAS mice with the modulation of gastrointestinal microbiota. Helicobacter 27:e12898. doi: 10.1111/hel.12898
Holman, J., Hurd, M., Moses, P. L., Mawe, G. M., Zhang, T., Ishaq, S. L., et al. (2022). Interplay of broccoli/broccoli sprout bioactives with gut microbiota in reducing inflammation in inflammatory bowel diseases. J. Nutr. Biochem. 113:109238. doi: 10.1016/j.jnutbio.2022.109238
Hosseini, H., Abbasi, A., Sabahi, S., Akrami, S., Yousefi-Avarvand, A. J. P., and Proteins, A. (2023). Assessing the potential biological activities of postbiotics derived from saccharomyces cerevisiae: an in vitro study. Probiotics Antimicrob Proteins, 1–17. doi: 10.1007/s12602-023-10117-y
Hosseini, E., Poursina, F., Van de Wiele, T., Safaei, H. G., and Adibi, P. (2012). Helicobacter pylori in Iran: a systematic review on the association of genotypes and gastroduodenal diseases. J. Res. Med. Sci. 17, 280–292.
Howell, A. B. (2020). Clinical evidence supporting cranberry as a complementary approach to Helicobacter pylori management. Food Front. 1, 329–331. doi: 10.1002/fft2.47
Hu, Y., Wan, J. H., Li, X. Y., Zhu, Y., Graham, D., and Lu, N. H. (2017). Systematic review with meta-analysis: the global recurrence rate of Helicobacter pylori. Aliment. Pharmacol. Ther. 46, 773–779. doi: 10.1111/apt.14319
Huang, Y., Ding, Y., Xu, H., Shen, C., Chen, X., and Li, C. (2021). Effects of sodium butyrate supplementation on inflammation, gut microbiota, and short-chain fatty acids in Helicobacter pylori-infected mice. Helicobacter 26:e12785. doi: 10.1111/hel.12785
Ibrahim, N., El Said, H., and Choukair, A. (2022). Zinc carnosine-based modified bismuth quadruple therapy vs standard triple therapy for Helicobacter pylori eradication: a randomized controlled study. World J. Clin. Cases 10, 227–235. doi: 10.12998/wjcc.v10.i1.227
Karbalaei, M., Keikha, M., and Abadi, A. T. B. (2022). Prevalence of primary multidrug-resistant Helicobacter pylori in children: a systematic review and Meta-analysis. Arch. Med. Res. 53, 634–640. doi: 10.1016/j.arcmed.2022.08.010
Kashani, B., Zandi, Z., Pourbagheri-Sigaroodi, A., Bashash, D., and Ghaffari, S. H. (2021). The role of toll-like receptor 4 (TLR4) in cancer progression: a possible therapeutic target? J. Cell. Comp. Physiol. 236, 4121–4137. doi: 10.1002/jcp.30166
Kawahara, M., Tanaka, K.-I., and Kato-Negishi, M. (2018). Zinc, carnosine, and neurodegenerative diseases. Nutrients 10:147. doi: 10.3390/nu10020147
Keikha, M., and Karbalaei, M. (2021). Probiotics as the live microscopic fighters against Helicobacter pylori gastric infections. Gastroenterology 21, 388–318. doi: 10.1186/s12876-021-01977-1
Khademi, F., Poursina, F., Hosseini, E., Akbari, M., and Safaei, H. G. (2015). Helicobacter pylori in Iran: a systematic review on the antibiotic resistance. Iran. J. Basic Med. Sci. 18:2, doi: 10.22038/ijbms.2015.3878
Khaledi, M., Bagheri, N., Validi, M., Zamanzad, B., Afkhami, H., Fathi, J., et al. (2020). Determination of cag a EPIYA motif in Helicobacter pylori strains isolated from patients with digestive disorder. Heliyon 6:e04971. doi: 10.1016/j.heliyon.2020.e04971
Kiepś, J., and Dembczyński, R. (2022). Current trends in the production of probiotic formulations. Food Secur. 11:2330. doi: 10.3390/foods11152330
Kim, T.-S., Hur, J.-W., Yu, M.-A., Cheigh, C.-I., Kim, K.-N., Hwang, J.-K., et al. (2003). Antagonism of Helicobacter pylori by bacteriocins of lactic acid bacteria. J. Milk Food Technol. 66, 3–12. doi: 10.4315/0362-028X-66.1.3
Koca, B., Kılıç, E., Yürüker, S. S., Yıldırım, M., Bostan, M. S., Uğurlu, C., et al. (2021). Evaluation of the effectiveness of using two different probiotics in helicobacter eradication treatment. Laparosc Endosc Surg Sci 28, 176–181. doi: 10.14744/less.2021.03764
Kolinjivadi, A. M., Sankar, H., Choudhary, R., Tay, L. S., Tan, T. Z., Murata-Kamiya, N., et al. (2022). The H. pylori cag a Oncoprotein induces DNA double Strand breaks through Fanconi Anemia pathway downregulation and replication fork collapse. Int. J. Mol. Sci. 23:1661. doi: 10.3390/ijms23031661
Krzyżek, P., Paluch, E., and Gościniak, G. (2020). Synergistic therapies as a promising option for the treatment of antibiotic-resistant Helicobacter pylori. Antibiotics 9:658. doi: 10.3390/antibiotics9100658
Kumari, H., Aishwarya, R., and Padmavathi, R. (n.d.). Effect of Ethanolic extract of Malus domestica Peel on gentamicin-induced nephrotoxicity in rats. 21:425.
Li, W.-Q., Zhang, J.-Y., Ma, J.-L., Li, Z.-X., Zhang, L., Zhang, Y., et al. (2019). Effects of Helicobacter pylori treatment and vitamin and garlic supplementation on gastric cancer incidence and mortality: follow-up of a randomized intervention trial. BMJ 366:l5016. doi: 10.1136/bmj.l5016
Losurdo, G., Cubisino, R., Barone, M., Principi, M., Leandro, G., Ierardi, E., et al. (2018). Probiotic monotherapy and Helicobacter pylori eradication: a systematic review with pooled-data analysis. World J. Gastroenterol. 24, 139–149. doi: 10.3748/wjg.v24.i1.139
Lu, Q., Li, C., and Wu, G. (2020). Insight into the inhibitory effects of Zanthoxylum nitidum against Helicobacter pylori urease and jack bean urease: kinetics and mechanism. J. Ethnopharmacol. 249:112419. doi: 10.1016/j.jep.2019.112419
Ma, L., Tu, H., and Chen, T. (2023). Postbiotics in human health: a narrative review. Nutrients 15:291. doi: 10.3390/nu15020291
Magdy, H., Rady, M. H., Salama, M. S., Sayed, H. A., Hamza, D., and Azzam, M. (2023). Isolation of multidrug-resistant Helicobacter pylori from wild houseflies Musca domestica with a new perspective for the treatment. Vector Borne Zoonotic Dis. 23, 63–74. doi: 10.1089/vbz.2022.0033
Mahmoud, A., Abuelazm, M., Ahmed, A. A. S., Abdalshafy, H., Abdelazeem, B., and Brašić, J. R. (2022). Efficacy and safety of Polaprezinc-based therapy versus the standard triple therapy for Helicobacter pylori eradication: a systematic review and Meta-analysis of randomized controlled trials. Nutrients 14:4126. doi: 10.3390/nu14194126
Malfertheiner, P., Mégraud, F., O'Morain, C. A., Gisbert, J. P., Kuipers, E. J., Axon, A. T., et al. (2017). Management of Helicobacter pylori infection—the Maastricht V/Florence consensus report. Gut 66, 6–30. doi: 10.1136/gutjnl-2016-312288
Malfertheiner, P., Megraud, F., Rokkas, T., Gisbert, J. P., Liou, J.-M., Schulz, C., et al. (2022). Management of Helicobacter pylori infection: the Maastricht VI/Florence consensus report. Gut 71, 1724–1762. doi: 10.1136/gutjnl-2022-327745
Marini, E., Di Giulio, M., Ginestra, G., Magi, G., Di Lodovico, S., Marino, A., et al. (2019). Efficacy of carvacrol against resistant rapidly growing mycobacteria in the planktonic and biofilm growth mode. PLoS One 14:e0219038. doi: 10.1371/journal.pone.0219038
Marques, A. T., Vítor, J. M., Santos, A., Oleastro, M., and Vale, F. F. (2020). Trends in Helicobacter pylori resistance to clarithromycin: from phenotypic to genomic approaches. Microb Genome 6:e000344. doi: 10.1099/mgen.0.000344
Messina, B., Lo Sardo, F., Scalera, S., Memeo, L., Colarossi, C., and Mare, M. (2023). Hippo pathway dysregulation in gastric cancer: from Helicobacter pylori infection to tumor promotion and progression. Cell Death Dis. 14, 21–12. doi: 10.1038/s41419-023-05568-8
Mestrovic, A., Perkovic, N., Bozic, J., Pavicic Ivelja, M., Vukovic, J., Kardum, G., et al. (2020). Randomised clinical trial comparing concomitant and hybrid therapy for eradication of Helicobacter pylori infection. PLoS One 15:e0244500. doi: 10.1371/journal.pone.0244500
Morilla, A. M., Álvarez-Argüelles, M. E., Duque, J. M., Armesto, E., Villar, H., and Melón, S. (2019). Primary antimicrobial resistance rates and prevalence of Helicobacter pylori infection in the north of Spain. A 13-year retrospective study. Gastroenterol. Hepatol. 42, 476–485. doi: 10.1016/j.gastrohep.2019.05.002
Namkin, K., Zardast, M., and Basirinejad, F. (2016). Saccharomyces boulardii in Helicobacter pylori eradication in children: a randomized trial from Iran. Iran. J. Pediatr. 26:e3768. doi: 10.5812/ijp.3768
Nikbazm, R., Rahimi, Z., Moradi, Y., Alipour, M., and Shidfar, F. (2022). The effect of cranberry supplementation on Helicobacter pylori eradication in H. pylori positive subjects: a systematic review and meta-analysis of randomised controlled trials. Br. J. Nutr. 128, 1090–1099. doi: 10.1017/S0007114521004256
Noiri, Y., and Nagata, R. (2023). Current status of gastric and oral infection/diseases caused by Helicobacter pylori. Oral Sci Int J. 20, 182–189. doi: 10.1002/osi2.1172
Omar, M. S., Adnan, N. N., Kumolosasi, E., Azmi, N., Damanhuri, N. S., and Buang, F. (2020). Green tea (Camellia sinensis) extract reduces peptic ulcer induced by Helicobacter pylori in Sprague Dawley rats. Sains Malays 49, 2793–2800. doi: 10.17576/jsm-2020-4911-18
Österlund, P., Ruotsalainen, T., Korpela, R., Saxelin, M., Ollus, A., Valta, P., et al. (2007). Lactobacillus supplementation for diarrhoea related to chemotherapy of colorectal cancer: a randomised study. Br. J. Cancer 97, 1028–1034. doi: 10.1038/sj.bjc.6603990
Poonyam, P., Chotivitayatarakorn, P., and Vilaichone, R.-K. (2019). High effective of 14-day high-dose PPI-bismuth-containing quadruple therapy with probiotics supplement for Helicobacter pylori eradication: a double blinded-randomized placebo-controlled study. Asian Pac. J. Cancer Prev. 20, 2859–2864. doi: 10.31557/APJCP.2019.20.9.2859
Pourmasoumi, M., Najafgholizadeh, A., Hadi, A., Mansour-Ghanaei, F., and Joukar, F. (2019). The effect of synbiotics in improving Helicobacter pylori eradication: a systematic review and meta-analysis. Complement. Ther. Med. 43, 36–43. doi: 10.1016/j.ctim.2019.01.005
Qureshi, N., Li, P., and Gu, Q. (2019). Probiotic therapy in Helicobacter pylori infection: a potential strategy against a serious pathogen? Appl. Microbiol. Biotechnol. 103, 1573–1588. doi: 10.1007/s00253-018-09580-3
Reshetnyak, T. M., Doroshkevich, I. A., Seredavkina, N. V., Nasonov, E. L., Maev, I. V., and Reshetnyak, V. I. J. I. (2019). The contribution of drugs and Helicobacter pylori to gastric mucosa changes in patients with systemic lupus erythematosus and antiphospholipid syndrome. Int. J. Rheumatol. 2019, 1–18. doi: 10.1155/2019/9698086
Rokkas, T., and Graham, D. Y. (2023). How widespread and convenient H. pylori susceptibility testing will result in pharmacological opportunities. (just-accepted). Expert Rev. Gastroenterol. Hepatol. 17, 1–7. doi: 10.1080/17474124.2023.2162502
Romero, M., Freire, J., Pastene, E., García, A., Aranda, M., and González, C. (2019). Propolis polyphenolic compounds affect the viability and structure of Helicobacter pylori in vitro. Rev. Bras 29, 325–332. doi: 10.1016/j.bjp.2019.03.002
Rook, G., Bäckhed, F., Levin, B. R., McFall-Ngai, M. J., and McLean, A. R. J. T. L. (2017). Evolution, human-microbe interactions, and life history plasticity. Lancet 390, 521–530. doi: 10.1016/S0140-6736(17)30566-4
Ruiz-Rico, M., Moreno, Y., and Barat, J. (2020). In vitro antimicrobial activity of immobilised essential oil components against Helicobacter pylori. World J. Microbiol. Biotechnol. 36, 1–9. doi: 10.1007/s11274-019-2782-y
Sachdeva, A., and Nagpal, J. (2009). Effect of fermented milk-based probiotic preparations on Helicobacter pylori eradication: a systematic review and meta-analysis of randomized-controlled trials. Eur. J. Gastroenterol. Hepatol. 21, 45–53. doi: 10.1097/MEG.0b013e32830d0eff
Sachdeva, A., Rawat, S., and Nagpal, J. (2014). Efficacy of fermented milk and whey proteins in Helicobacter pylori eradication: a review. World J. Gastroenterol. 20, 724–737. doi: 10.3748/wjg.v20.i3.724
Sahin, O., Yesil, A., Senates, E., Akdogan, M., Konur, S., Erdem, E., et al. (2013). Synbiotic therapy increases eradication rate in Helicobacter pylori eradication. Acta Medica Mediterranea 29:569,
Salama, N. R. (2020). Cell morphology as a virulence determinant: lessons from Helicobacter pylori. Curr. Opin. Microbiol. 54, 11–17. doi: 10.1016/j.mib.2019.12.002
Salatin, S., Bazmani, A., Shahi, S., Naghili, B., Memar, M. Y., and Dizaj, S. M. (2022). Antimicrobial benefits of flavonoids and their Nanoformulations. Curr. Pharm. Des. 28, 1419–1432. doi: 10.2174/1381612828666220509151407
Salvatori, S., Marafini, I., Laudisi, F., Monteleone, G., and Stolfi, C. (2023). Helicobacter pylori and gastric Cancer: Pathogenetic mechanisms. Int. J. Mol. Sci. 24:2895. doi: 10.3390/ijms24032895
Satoh-Takayama, N., Kato, T., Motomura, Y., Kageyama, T., Taguchi-Atarashi, N., Kinoshita-Daitoku, R., et al. (2020). Bacteria-induced group 2 innate lymphoid cells in the stomach provide immune protection through induction of IgA. Immunity 52, 635–649.e4. doi: 10.1016/j.immuni.2020.03.002
Savoldi, A., Carrara, E., Graham, D. Y., Conti, M., and Tacconelli, E. (2018). Prevalence of antibiotic resistance in Helicobacter pylori: a systematic review and meta-analysis in World Health Organization regions. Gastroenterology 155, 1372–1382.e17. doi: 10.1053/j.gastro.2018.07.007
Shah, S. C., Iyer, P. G., and Moss, S. F. (2021). AGA clinical practice update on the management of refractory Helicobacter pylori infection: expert review. Gastroenterology 160, 1831–1841. doi: 10.1053/j.gastro.2020.11.059
Singh, R. P., Shadan, A., Ma, Y., and Proteins, A. (2022). Biotechnological applications of probiotics: a multifarious weapon to disease and metabolic abnormality. Probiotics Antimicrob Proteins 14, 1184–1210. doi: 10.1007/s12602-022-09992-8
Singhi, S., and Kumar, S. (2016). Probiotics in critically ill children. F1000Res 5:407. doi: 10.12688/f1000research.7630.1
Song, M.-Y., Lee, D.-Y., and Kim, E.-H. (2020). Anti-inflammatory and anti-oxidative effect of Korean propolis on Helicobacter pylori-induced gastric damage in vitro. J. Microbiol. 58, 878–885. doi: 10.1007/s12275-020-0277-z
Spitsberg, V. (2005). Invited review: bovine milk fat globule membrane as a potential nutraceutical. J. Dairy Sci. 88, 2289–2294. doi: 10.3168/jds.S0022-0302(05)72906-4
Sukri, A., Hanafiah, A., Mohamad Zin, N., and Kosai, N. R. (2020). Epidemiology and role of Helicobacter pylori virulence factors in gastric cancer carcinogenesis. APMIS 128, 150–161. doi: 10.1111/apm.13034
Sun, Y., and Zhang, J. (2019). Helicobacter pylori recrudescence and its influencing factors. J. Cell. Mol. Med. 23, 7919–7925. doi: 10.1111/jcmm.14682
Takeuchi, H., Trang, V. T., Morimoto, N., Nishida, Y., Matsumura, Y., and Sugiura, T. (2014). Natural products and food components with anti-Helicobacter pylori activities. World J. Gastroenterol. 20, 8971–8978. doi: 10.3748/wjg.v20.i27.8971
Teng, G., Liu, Y., Wu, T., Wang, W., Wang, H., and Hu, F. (2020). Efficacy of sucralfate-combined quadruple therapy on gastric mucosal injury induced by Helicobacter pylori and its effect on gastrointestinal flora. Biomed. Res. Int. 2020, 1–14. doi: 10.1155/2020/4936318
Thung, I., Aramin, H., Vavinskaya, V., Gupta, S., Park, J., and Crowe, S. (2016). The global emergence of Helicobacter pylori antibiotic resistance. Aliment. Pharmacol. Ther. 43, 514–533. doi: 10.1111/apt.13497
Tomori, M., Nagamine, T., Miyamoto, T., and Iha, M. (2019). Evaluation of the immunomodulatory effects of fucoidan derived from Cladosiphon okamuranus Tokida in mice. Mar. Drugs 17:547. doi: 10.3390/md17100547
Tomori, M., Nagamine, T., Miyamoto, T., and Iha, M. (2021). Effects of ingesting Fucoidan derived from Cladosiphon okamuranus Tokida on human NK cells: a randomized, double-blind, parallel-group, placebo-controlled pilot study. Mar. Drugs 19:340. doi: 10.3390/md19060340
Tuma, R. S. (2006). Broccoli sprout consumption reduces H. pylori colonization. Oncol Times 28, 27–29. doi: 10.1097/01.COT.0000294723.80359.ea
Ullah, H., Di Minno, A., Santarcangelo, C., Khan, H., Xiao, J., Arciola, C. R., et al. (2021). Vegetable extracts and nutrients useful in the recovery from Helicobacter pylori infection: a systematic review on clinical trials. Mol. Ther. 26:2272. doi: 10.3390/molecules26082272
Vega-Hissi, E. G., Andrada, M. F., Díaz, M. G., and Garro Martinez, J. C. (2019). Computational study of the hydrogen peroxide scavenging mechanism of allyl methyl disulfide, an antioxidant compound from garlic. Mol. Divers. 23, 985–995. doi: 10.1007/s11030-019-09927-6
Vergara, M., Catalan, M., Gisbert, J., and Calvet, X. (2005). Meta-analysis: role of Helicobacter pylori eradication in the prevention of peptic ulcer in NSAID users. Aliment. Pharmacol. Ther. 21, 1411–1418. doi: 10.1111/j.1365-2036.2005.02444.x
Vestergaard, M., and Ingmer, H. (2019). Antibacterial and antifungal properties of resveratrol. Antimicrob Agents Annual 53, 716–723. doi: 10.1016/j.ijantimicag.2019.02.015
Wallner, J., Rieder, M., Schwaiger, M., Pau, M., Zrnc, T., Zemann, W., et al. (2022). Metronidazole-spectrum of activity, use and side effects. Swiss Dent J 132, 433–435. doi: 10.61872/sdj-2022-06-03
Wan, G.-Y., Lam, K.-M., Wong, I.-I., Fong, P., and Meng, L.-R. (2022). Extraction of antibacterial peptides against Helicobacter pylori from bovine milk casein. Arch. Med. Sci. 18, 376–381. doi: 10.5114/aoms/109942
Wang, N., Cai, T., Liu, X., and Zhu, W. (2023). Bovine lactoferrin inhibits resistant Helicobacter pylori in vitro and protects gastric mucosal injury in vivo. Int. Dairy J. 147:105770. doi: 10.1016/j.idairyj.2023.105770
Wang, F., Feng, J., Chen, P., Liu, X., Ma, M., and Zhou, R. (2017). Probiotics in Helicobacter pylori eradication therapy: systematic review and network meta-analysis. Gastroenterology 41, 466–475. doi: 10.1016/j.clinre.2017.04.004
Wang, B., Gan, Q., Tong, Y., Qiao, Y., Han, M., Zhang, R., et al. (2023). A visual diagnostic detection of Helicobacter pylori and the gastric carcinoma-related virulence genes (cagA and vacA) by a fluorescent loop-mediated isothermal amplification (LAMP). Talanta 256:124260. doi: 10.1016/j.talanta.2023.124260
Wang, K.-X., and Wang, X.-F. (2004). Cloning and sequencing of cagA gene fragment of Helicobacter pylori with coccoid form. World J. Gastroenterol. 10, 3511–3513. doi: 10.3748/wjg.v10.i23.3511
Wang, Q., Yao, C., Li, Y., Luo, L., Xie, F., Xiong, Q., et al. (2023). Effect of polyphenol compounds on Helicobacter pylori eradication: a systematic review with meta-analysis. BMJ Open 13:e062932. doi: 10.1136/bmjopen-2022-062932
Whiteside, S. A., Dave, S., Reid, G., and Burton, J. P. (2019). Ibuprofen lacks direct antimicrobial properties for the treatment of urinary tract infection isolates. J. Med. Microbiol. 68, 1244–1252. doi: 10.1099/jmm.0.001017
Whiteside, S. A., Mohiuddin, M. M., Shlimon, S., Chahal, J., Mac Pherson, C. W., Jass, J., et al. (2021). In vitro framework to assess the anti-Helicobacter pylori potential of lactic acid bacteria secretions as alternatives to antibiotics. Int. J. Mol. Sci. 22:5650. doi: 10.3390/ijms22115650
Wu, D., Cao, M., Li, N., Zhang, A., Yu, Z., Cheng, J., et al. (2020). Effect of trimethylamine N-oxide on inflammation and the gut microbiota in Helicobacter pylori-infected mice. Int. J. Immunopharmacol. 81:106026. doi: 10.1016/j.intimp.2019.106026
Wu, D., Cao, M., Peng, J., Li, N., Yi, S., Song, L., et al. (2017). The effect of trimethylamine N-oxide on Helicobacter pylori-induced changes of immunoinflammatory genes expression in gastric epithelial cells. Int. Immunopharmacol. 43, 172–178. doi: 10.1016/j.intimp.2016.11.032
Xiong, J. (2018). Progress in the gut microbiota in exploring shrimp disease pathogenesis and incidence. Appl. Microbiol. Biotechnol. 102, 7343–7350. doi: 10.1007/s00253-018-9199-7
Yanagawa, Y., Yamamoto, Y., Hara, Y., and Shimamura, T. (2003). A combination effect of epigallocatechin gallate, a major compound of green tea catechins, with antibiotics on Helicobacter pylori growth in vitro. Curr. Microbiol. 47, 244–0249. doi: 10.1007/s00284-002-3956-6
Yang, R., Li, J., Wang, J., Wang, Y., Ma, F., Zhai, R., et al. (2022). Kaempferol inhibits the growth of Helicobacter pylori in a manner distinct from antibiotics. J. Food Biochem. 46:e14210. doi: 10.1111/jfbc.14210
Yang, W., Peng, Z., and Wang, G. (2023). An overview: metal-based inhibitors of urease. J. Enzyme Inhib. Med. Chem. 38, 361–375. doi: 10.1080/14756366.2022.2150182
Ye, Q., Shao, X., Shen, R., Chen, D., and Shen, J. (2020). Changes in the human gut microbiota composition caused by Helicobacter pylori eradication therapy: a systematic review and meta-analysis. Helicobacter 25:e12713. doi: 10.1111/hel.12713
Yoon, J. Y., Cha, J. M., Hong, S. S., Kim, H. K., Kwak, M. S., Jeon, J. W., et al. (2019). Fermented milk containing Lactobacillus paracasei and Glycyrrhiza glabra has a beneficial effect in patients with Helicobacter pylori infection: a randomized, double-blind, placebo-controlled study. Medicine 98:e16601. doi: 10.1097/MD.0000000000016601
Yuan, Z., Xiao, S., Li, S., Suo, B., Wang, Y., Meng, L., et al. (2021). The impact of Helicobacter pylori infection, eradication therapy, and probiotics intervention on gastric microbiota in young adults. Helicobacter 26:e12848. doi: 10.1111/hel.12848
Zama, D., Bossù, G., Leardini, D., Muratore, E., Biagi, E., Prete, A., et al. (2020). Insights into the role of intestinal microbiota in hematopoietic stem-cell transplantation. Ther Adv Hematol 11:204062071989696. doi: 10.1177/2040620719896961
Zhang, Q., Xu, W., Xu, X., Lu, W., Zhao, J., and Zhang, H. (2021). Effects of Limosilactobacillus fermentum CCFM1139 on experimental periodontitis in rats. Food Funct. 12, 4670–4678. doi: 10.1039/D1FO00409C
Zhang, L., Zhao, M., and Fu, X. (2023). Gastric microbiota dysbiosis and Helicobacter pylori infection. Front. Microbiol. 14:1153269. doi: 10.3389/fmicb.2023.1153269
Zhao, T., Li, C., Wang, S., and Song, X. (2022). Green tea (Camellia sinensis): a review of its phytochemistry, pharmacology, and toxicology. Mol. Ther. 27:3909. doi: 10.3390/molecules27123909
Zhao, Y., Li, Z., Zhao, L., Wang, J., Wang, F., and Zhang, Q. (2022). Two novel lactic acid bacteria, Limosilactobacillus fermentum MN-LF23 and Lactobacillus gasseri MN-LG80, inhibited Helicobacter pylori infection in C57BL/6 mice. Food Funct. 13, 11061–11069. doi: 10.1039/D2FO02034C
Zheng, W., Miao, J., Luo, L., Long, G., Chen, B., Shu, X., et al. (2021). The effects of Helicobacter pylori infection on microbiota associated with gastric mucosa and immune factors in children. Front. Immunol. 12:625586. doi: 10.3389/fimmu.2021.625586
Keywords: Helicobacter pylori (H. pylori), probiotic therapy, quadruple therapy, triple therapy, antibiotic
Citation: Shadvar N, Akrami S, Mousavi Sagharchi S-M-A, Askandar RH, Merati A, Aghayari M, Kaviani N, Afkhami H and Kashfi M (2024) A review for non-antibiotic treatment of Helicobacter pylori: new insight. Front. Microbiol. 15:1379209. doi: 10.3389/fmicb.2024.1379209
Edited by:
Rossella Grande, University "G. d'Annunzio" of Chieti-Pescara, ItalyReviewed by:
Dawn Israel, Vanderbilt University, United StatesCopyright © 2024 Shadvar, Akrami, Mousavi Sagharchi, Askandar, Merati, Aghayari, Kaviani, Afkhami and Kashfi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hamed Afkhami, aGFtZWRhZmtoYW1pNzBAZ21haWwuY29t; Mojtaba Kashfi, bW9qdGFiYWthc2hmaTkwQHlhaG9vLmNvbQ==
†These authors share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.