 Minjuan Han1
Minjuan Han1 Wanhu Dong
Wanhu Dong
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Microbiol. , 14 February 2024
Sec. Infectious Agents and Disease
Volume 15 - 2024 | https://doi.org/10.3389/fmicb.2024.1345278
Background: Probiotics has been used as an adjuvant therapy for the prevention of ventilator-associated pneumonia (VAP). This study aimed to systematically compile, evaluate, and synthesize previous systematic reviews (SRs) and meta-analyses (MAs) on the prevention of VAP with probiotics.
Methods: The methodological quality, reporting quality, and evidence quality of enrolled studies were, respectively evaluated by Assessment of Multiple Systematic Reviews 2 (AMSTAR-2) tool, Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) checklists, and Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) system.
Results: Thirteen eligible publications were analyzed in this overview. The included studies were rated as generally low methodological quality owing to the lack of a registered protocol or a list of exclusion criteria. The inadequate quality of the reports was demonstrated by the lack of reporting on the registration protocols, the lack of reporting on the search strategy, and the lack of reporting on the additional analyses. For GRADE, there were 36.17% (17/47) outcomes graded to be of moderate quality, 42.55% (20/47) to be of low quality, and 21.28% (10/47) to be of very low quality.
Conclusion: Probiotics may be associated with reduced incidence of VAP. However, caution should be exercised when recommending probiotics for the prevention of VAP owing to the poor quality of the current evidence.
Ventilator-associated pneumonia (VAP) is a common pneumonia occurring more than 48 h after endotracheal intubation in the intensive care unit (ICU) (Metersky and Kalil, 2018). The duration of mechanical ventilation (MV) is positively correlated with the incidence of VAP (François et al., 2019). VAP has been reported to occur in approximately 40% of patients experiencing MV (Goutier et al., 2014; Ferrer and Torres, 2018). By prolonging the duration of MV and ICU stays and increasing antibiotic demands, VAP usually negatively impacts the prognosis of critically ill patients (Warren et al., 2003). A recent study performed in Japan revealed that patients with VAP typically spent $67,080 during their hospital stays, a substantial premium above individuals without VAP ($32,196) (Nanao et al., 2021).
Early and widely used approaches included selective oral decontamination or antibiotic-selective GI decontamination in an attempt to reduce the incidence of VAP by manipulating the microbiota using pharmacologic strategies (Maselli and Restrepo, 2011). The current guideline, which was updated 6 years ago, are ambiguous in recommending these two strategies because neither approach has been conclusively proven to have definitive efficacy (Torres et al., 2017). The application of probiotics is a recently emerging strategy that may be beneficial in regulating microbiota imbalances in critically ill patients (Shimizu et al., 2021). Probiotics are commercially available live microbial preparations defined as “living microorganisms that confer health benefits to the host when administered in sufficient amount” (Hill et al., 2014). To date, there have been a number of overlapping systematic reviews (SRs)/meta-analyses (MAs) evaluating the efficacy of probiotics in the prevention of VAP (Siempos et al., 2010; Gu et al., 2012; Wang et al., 2013; Bo et al., 2014; Weng et al., 2017; Chen et al., 2018; Batra et al., 2020; Su et al., 2020; Ji et al., 2021; Zhao et al., 2021; Cheema et al., 2022; Song et al., 2022; Sun et al., 2022). However, evidence from these SRs/MAs has not been uniform. In evidence-based medicine, SRs/MAs are regarded as the highest level of evidence (Chen et al., 2022; Yang et al., 2022). High-quality SRs/MAs contribute to the production of trustworthy evidence, whereas low-quality SRs/MAs may inadvertently influence decisions (Huang et al., 2021, 2022). Therefore, this study aimed to systematically compile, evaluate, and synthesize evidence from previous SRs/MAs on the prevention of VAP.
We considered the following criteria for inclusion: (a) type of literature was limited to SRs/MAs; (b) critically ill patients who received MV; (c) probiotics compared to placebo or usual care; and (d) incidence of VAP, ICU mortality, hospital mortality, duration of MV, length of ICU stay, and length of hospital stay were used as outcomes. We considered the following criteria for exclusion: (a) studies not related to the topic; (b) conference reports, protocols; and (c) no valid data available.
Searching was performed in Embase, Web of Science, Cochrane Library, and PubMed. The databases were searched from the time they were first created until November 13, 2023. We used a mix of free keywords and Mesh phrases to perform our search. Keywords used for search included “ventilator-associated pneumonia,” “probiotics,” “systematic review,” and “meta-Analyses.” The PubMed search strategy is displayed in Table 1.
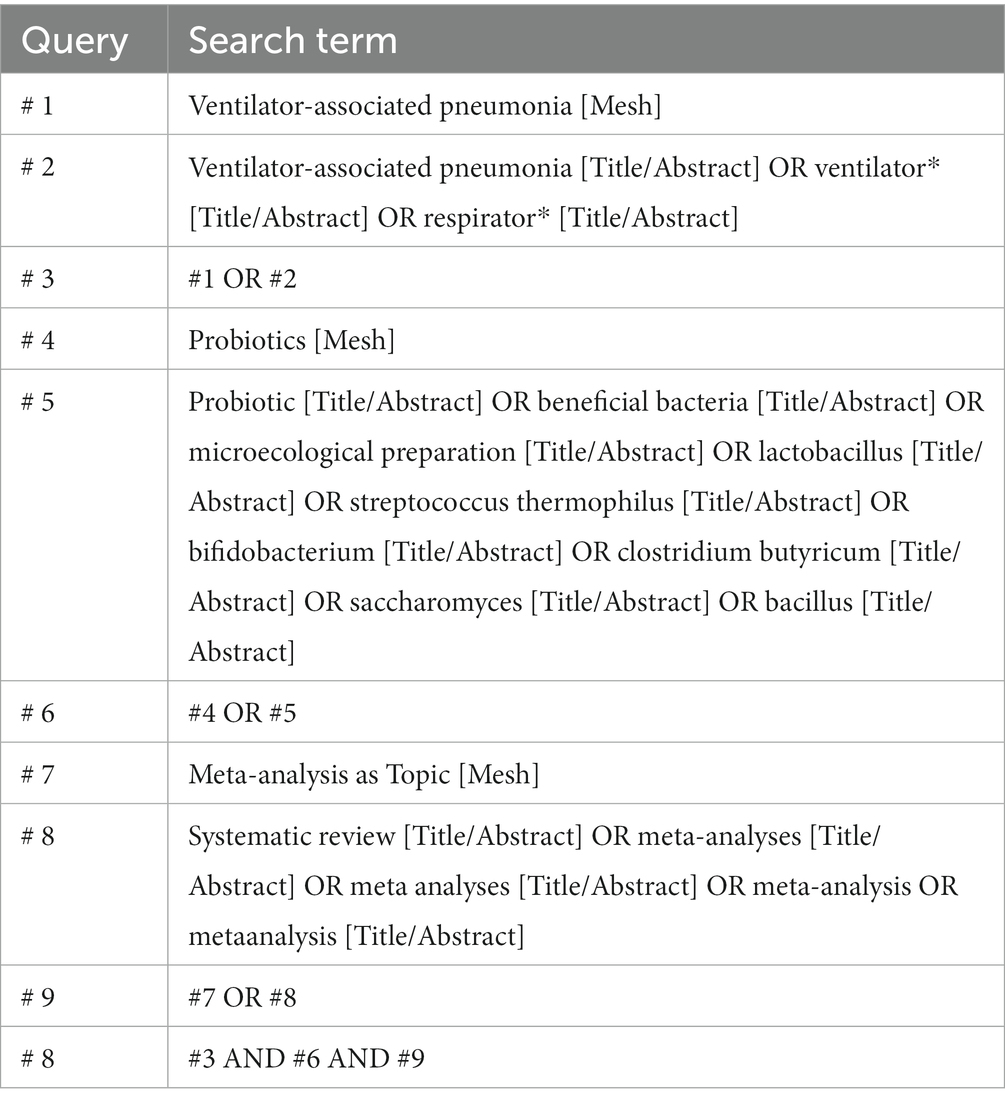
Table 1. Search strategy for PubMed.
Data collection and extraction were performed by two reviewers independently. Prior to reviewing the complete text of possibly eligible reviews to ascertain whether they matched the inclusion criteria, the abstract and title of the literature were first read. Publication year, authors, nation, risk of bias, interventions, methods of quality evaluation, and a summary of the intervention effects were retrieved for the included reviews.
Assessment of Multiple Systematic Reviews 2 (AMSTAR-2) tool was used independently by two reviewers to assess the methodological quality of the included reviews (Shea et al., 2017). In AMSTAR-2, there are 16 items, of which seven are key items. The items can be rated on three levels: “yes,” “partially yes,” and “no” (Shea et al., 2017).
Two reviewers independently assessed the reporting quality of each included review based on Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) checklists (Moher et al., 2009). There are 27 checklists in PRISMA, each rated either “no” (not reported), “partially yes” (partially reported), or “yes” (fully reported) (Moher et al., 2009).
Two reviewers independently graded the evidence quality of the included reviews using Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) system (Atkins et al., 2004). There are several possible causes of evidence downgrading, including indirectness, inconsistency, publication bias, imprecision, and bias risk (Atkins et al., 2004).
Databases provided 611 potential publications, of which 100 were duplicated. Our review of titles and abstracts revealed 493 records to be excluded. For full-text evaluation, the remaining 18 records were retrieved. As a result, 13 publications (Siempos et al., 2010; Gu et al., 2012; Wang et al., 2013; Bo et al., 2014; Weng et al., 2017; Chen et al., 2018; Batra et al., 2020; Su et al., 2020; Ji et al., 2021; Zhao et al., 2021; Cheema et al., 2022; Song et al., 2022; Sun et al., 2022) were included in this review. The study selection process is depicted in Figure 1.
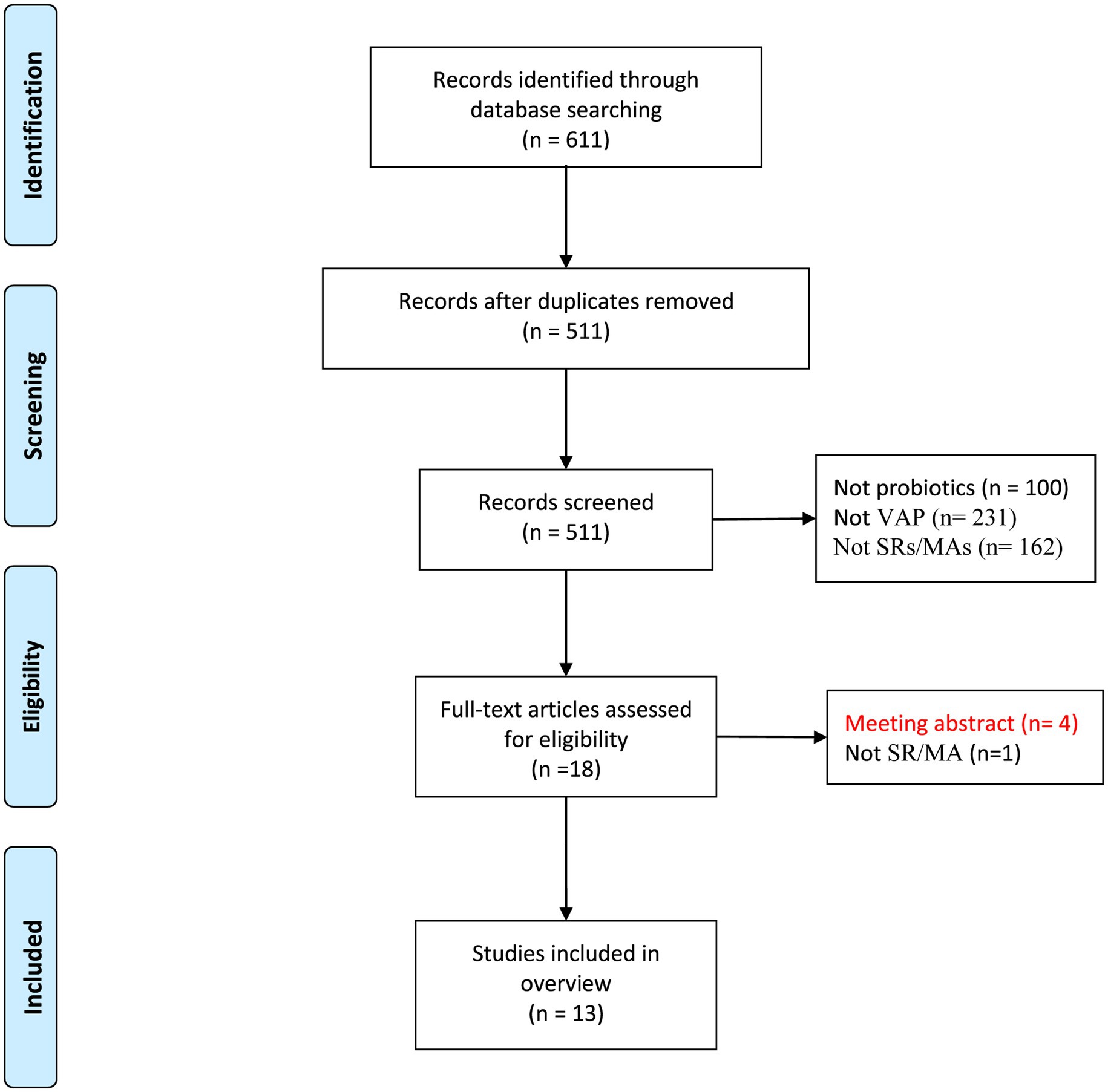
Figure 1. Flow diagram of the literature selection process.
Inclusion of SRs/MAs were published between 2010 and 2023 (Table 2). Of the 13 included studies, nine were conducted in China, while the remaining four were conducted in the United States, Brazil, India, and Pakistan. The smallest sample size was found in five trials with 795 cases, while the largest was found in 23 trials with 5,543 cases. Participants in experimental group received probiotics, whereas participants in control group received placebos. Summary of intervention of the included reviews is given in Table 3.

Table 2. Characteristics of the included reviews.
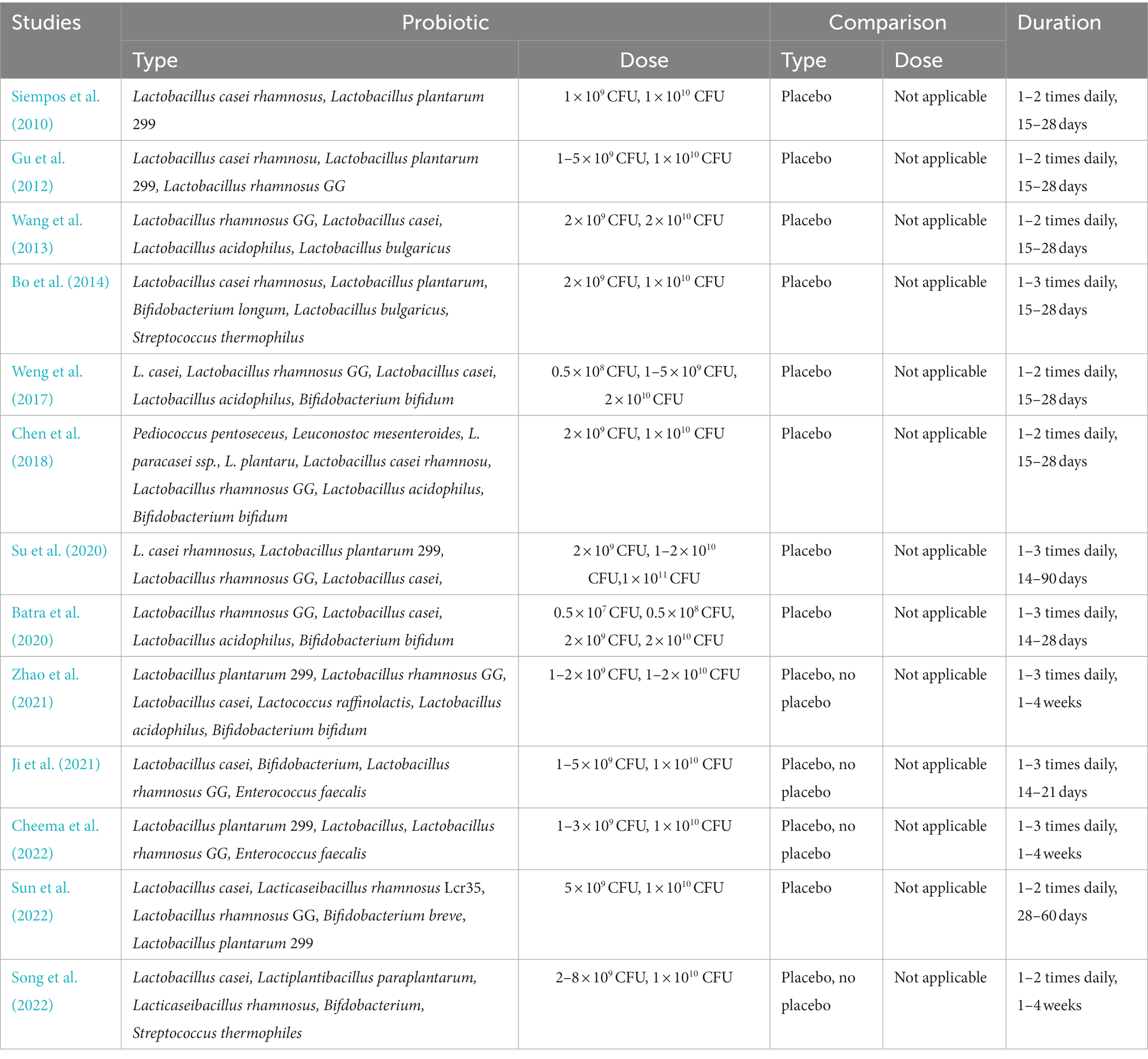
Table 3. Summary of intervention of the included reviews.
The AMSTAR-2 assesses one SR/MA as high quality, while the rest were low quality or very low quality (Table 4). Significant deficiencies in methodological quality were demonstrated by the lack of registration protocols (Q2), the lack of exhaustive search strategies (Q4), and the lack of excluded literature lists (Q7). A more detailed explanation can be found in Table 4.

Table 4. Quality assessment of the included reviews by the AMSTAR-2 tool.
Reporting quality was generally well, with most SRs/MAs following the PRISMA (Table 5). The inadequate quality of the reports was demonstrated by the lack of reporting on the registration protocols (Q5), the lack of reporting on the search strategy (Q8), the lack of reporting on the additional analyses of the methodology section (Q16), and the lack of reporting on the additional analyses of the results section (Q23). A more detailed explanation can be found in Table 5.
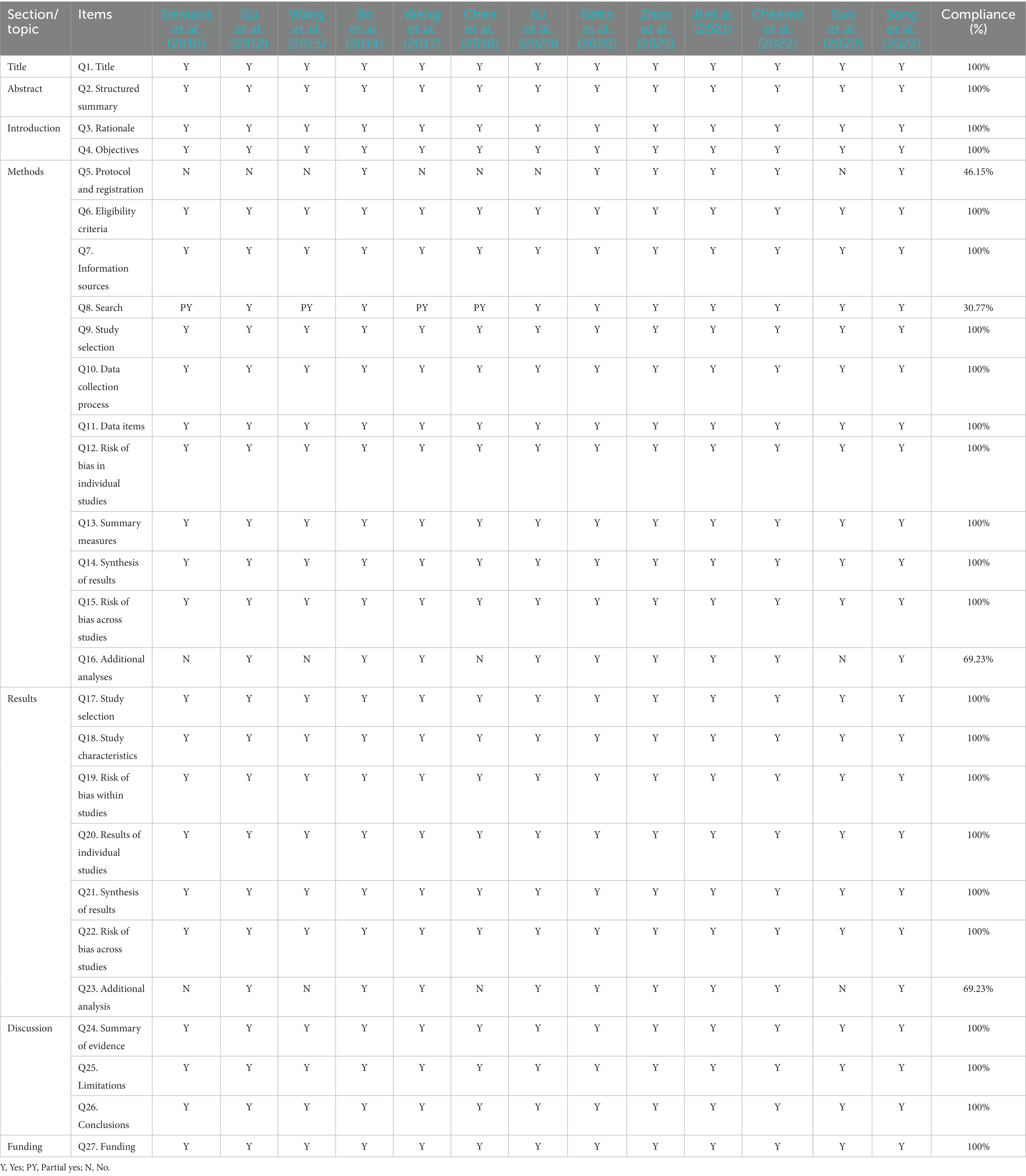
Table 5. Results of the reporting quality.
The GRADE system assessed 47 outcomes related to the prevention of VAP with probiotics. There were 36.17% (17/47) outcomes graded to be of moderate quality, 42.55% (20/47) to be of low quality, and 21.28% (10/47) to be of very low quality. Evidence was destroyed primarily because of bias risk, heterogeneity, and imprecision. A more detailed explanation can be found in Table 6.
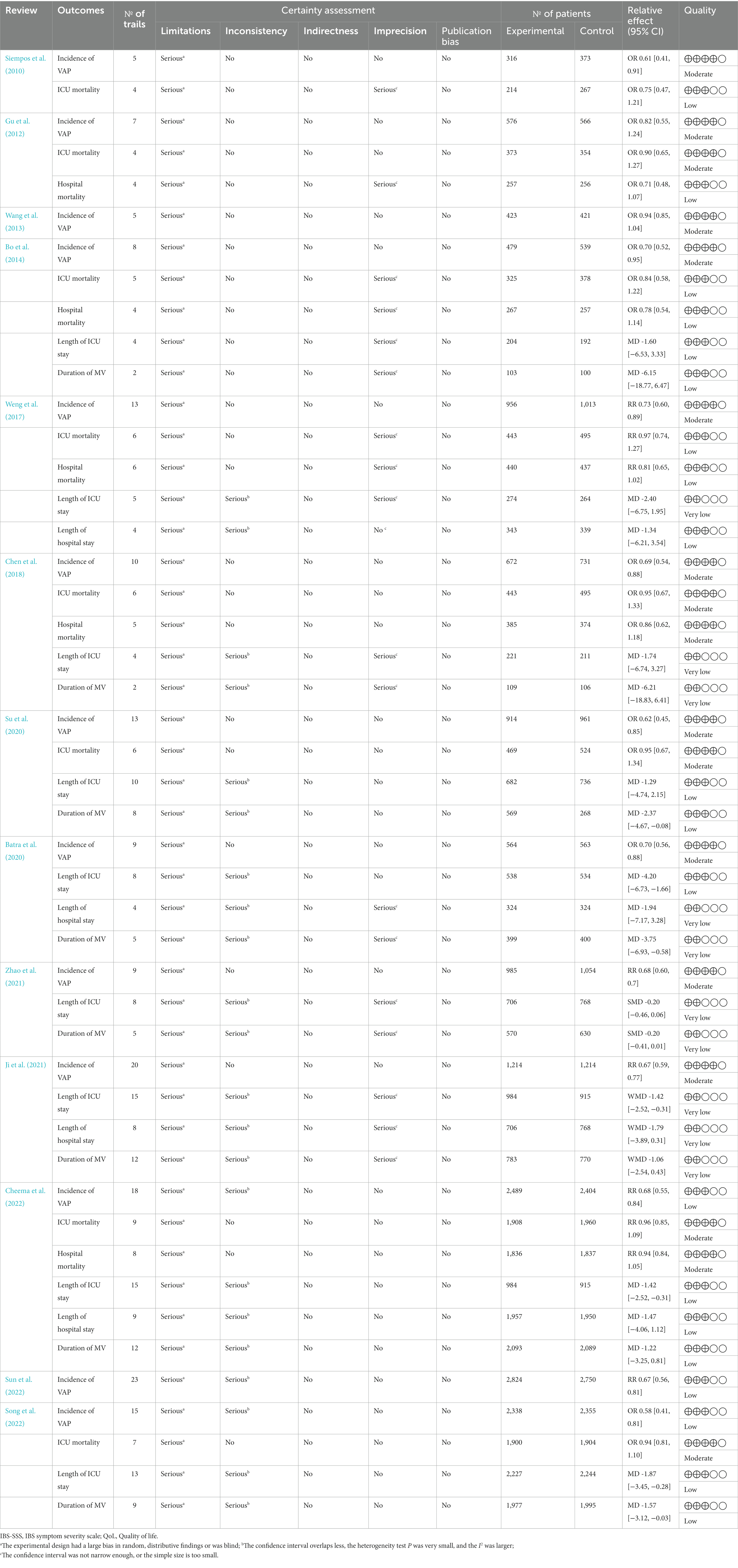
Table 6. Results of evidence quality.
Probiotics as adjuvant therapy for VAP prophylaxis should be used cautiously, as a definitive conclusion cannot be reached on the basis of currently published evidence. First, 11 of the 13 studies suggested that probiotics reduce the incidence of VAP, while the other two (Gu et al., 2012; Wang et al., 2013) studies suggested probiotics failed in the prevention of VAP. It should be noted that the number of patients in each study is quite significant and the number of outcomes for each study is medium high. The contradictory conclusions between these studies seem to be explainable, as the types of probiotics used in these two studies were not consistent with the dose, frequency, and duration of probiotics administered. Therefore, the same probiotic type as well as a standard uniform dosing regimen are more conducive to the comparability of conclusions between different studies. Second, even though 11 of the 13 studies suggested positive results, their unsatisfactory methodological quality limited the credibility of their conclusions. The AMSTAR-2 assesses one SR/MA as high quality, while the rest were low quality or very low quality. In addition, the reporting quality evaluation revealed that the included studies had varying degrees of missing reports in terms of registration protocols, search strategies, and additional analyses. It is well known that convincing evidence from SRs/MAs presupposes that they are sufficiently transparent, scientific and standardized in the production of evidence. Furthermore, the quality of evidence for all outcome indicators was categorized as very low to moderate due to the risk of bias and high degree of heterogeneity, meaning that the effect sizes of these indicators may not exactly match the true picture. Therefore, based on our assessment of the included SRs/MAs, we recommend that probiotics should be used cautiously to prevent VAP.
Deficiencies in methodology, reporting quality, and evidence quality need to be improved during the SR/MA process. Deficiencies in the methodology of SR/MA can reduce the validity of results; weaknesses in the reporting of SR/MA might obscure unfavorable occurrences or overstate the impact of treatments; and inadequately persuasive evidence can cast doubt on the accuracy of findings (McAuley et al., 2000). Evidence can be contaminated by these shortcomings, and clinical decisions can be misled as a result. We found that many of the SRs/MAs we reviewed did not have pre-registered protocols, had inadequate thorough searches, or did not provide an assessment of the design choices made in the studies. It should be noted that only one study (Bo et al., 2014) presents a high-quality assessment by the AMSTAR-2 tool. This study also comments that evidence suggests that use of probiotics is associated with a reduction in the incidence of VAP. Which could confirm the beneficial role of probiotics in VAP. However, this manuscript was published on 2014, which indicates that the missing Q2, Q4, and Q7 in the rest of the articles could have been improved taking this publication as a reference.
Registration or publication of study protocols beforehand can reduce any potential bias and enhance process openness. A full search tactic is advantageous to ensuring that the study can be replicated. A list of trials excluded and the reasons for their exclusion is also helpful for reducing publication bias. Sensitivity analyses and subgroup analyses could be taken into account as supplementary analytical techniques when doing data analysis in order to investigate causes of heterogeneity or even to rule out doing a pooled analyses in the event that there is a considerable amount of variation among studies. In particular, high-quality trials published in peer-reviewed journals are a guarantee of high-quality SR/MA. Thus, trials should be designed and conducted according to the Consolidated Standards to ensure high quality evidence and clinical relevance (Shimizu et al., 2021). Furthermore, SR/MA must be designed and implemented in strict compliance with AMSTAR-2 and PRISMA to ensure evidence availability.
Because of illness and different types of treatment (e.g., broad-spectrum antibiotics for infection management, MV for respiratory failure), it is challenging to maintain a healthy gut microbiota in critically ill patients (Shimizu et al., 2021). In comparison to healthy individuals, patients had 100 times greater levels of Staphylococcus and almost 10,000 times fewer total anaerobes, such as Lactobacillus and Bifidobacterium (Shimizu et al., 2006). When comparing critically ill patients to healthy persons, butyric acid, acetic acid, and organic acids generated from gut microbiota are reduced dramatically (Shimizu et al., 2006). These findings brought to light how the gut microbiota deteriorate during a serious illness (Shimizu et al., 2011). Levels of Lactobacilli, Bifidobacteria, and microbial products were significantly higher in patients taking probiotics compared to critically ill patients not taking probiotics (Shimizu et al., 2005). In patients receiving probiotics in ICU, there were significantly greater levels of organic acids, Lactobacilli, and Bifidobacteria than in those receiving no probiotics (Shimizu et al., 2009). Probiotics are thought to reduce the incidence of VAP as they regulate the composition of the gut microbiota and reduce pathogenic bacterial overgrowth and bacterial translocation through both local and systemic effects, which in turn increase host cell antimicrobial peptides to enhance the immune function (Tegegne and Kebede, 2022). Therefore, the mechanism of probiotics has been interpreted as involving the activity of probiotic metabolites and cellular components to modulate host immunity and inhibit systemic inflammation (Bron et al., 2011).
Lactobacillus and Bifidobacterium are the main genera of probiotic strains used to prevent VAP, according to the included studies (Siempos et al., 2010; Gu et al., 2012; Wang et al., 2013; Bo et al., 2014; Weng et al., 2017; Chen et al., 2018; Batra et al., 2020; Su et al., 2020; Ji et al., 2021; Zhao et al., 2021; Cheema et al., 2022; Song et al., 2022; Sun et al., 2022). Lactobacillus plantarum 299, Lactobacillus casei, Lactobacillus rhamnosus GG, Enterococcus faecalis, Bifidobacterium bifidum, Lactobacillus bulgaricus, Streptococcus thermophilus, and Lacticaseibacillus rhamnosus Lcr35 are widely used as probiotics. Lactobacillus plantarum 299 was evaluated by six studies, and the results showed that patients who underwent probiotic treatment had a lower incidence of VAP and a significantly shorter length of stay in ICU as well as a shorter duration of MV than the control group. Similarly, Lactobacillus casei was evaluated by six studies, and the results showed that patients who underwent probiotic treatment had a lower incidence of VAP, ICU mortality, hospital mortality, and a significantly shorter length of stay in ICU, length of stay in hospital as well as a shorter duration of MV than the control group. Nine studies assessed the effects of Lactobacillus rhamnosus GG for VAP, and the pooled analysis revealed considerable benefits in VAP incidence, mortality, length of hospital stay, and duration of MV in patients treated with the probiotic. Two studies evaluated the effects of Enterococcus faecalis and Lactobacillus bulgaricus, and the pooled results showed that patients receiving probiotics had a lower incidence of VAP and a significantly shorter hospital stay compared to controls. Two studies evaluated outcomes in patients treated with Bifidobacterium bifidum and the results indicated that probiotics were also beneficial in patients with VAP. Furthermore, Streptococcus thermophilus and Lacticaseibacillus rhamnosus Lcr35 were evaluated by one review, and the pooled analysis revealed considerable benefits in VAP incidence, mortality, length of hospital stay, and duration of MV in patients treated with probiotics. The quality of evidence for both of these widely used probiotics’ effect sizes was graded as low, despite the fact that they both demonstrated therapeutic potential against VAP. As such, care should be taken when suggesting probiotics as preventative therapy for VAP.
To the best of our knowledge, this study presents the first comprehensive assessment and summary of the data supporting the use of probiotics for the prevention of VAP. However, limitations must be recognized. First, it should be indicated the importance of including the appropriate diet (low in carbohydrates) along with probiotics immediately, to prevent VAP or to avoid the death of the hospitalized patient or large hospital stay. Furthermore, notwithstanding the fact that our evaluation was examined and approved by two separate researchers, different researchers may have differing opinions on any given project due to the subjective nature of quality assessment.
Probiotics may be associated with reduced incidence of VAP. However, caution should be exercised when recommending probiotics for the prevention of VAP owing to the poor quality of the current evidence.
The original contributions presented in the study are included in the article/supplementary material; further inquiries can be directed to the corresponding author.
MH: Writing – original draft, Writing – review & editing. KW: Conceptualization, Writing – original draft. LS: Conceptualization, Writing – original draft. WL: Conceptualization, Writing – original draft. WD: Visualization, Writing – original draft, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work was funded by the National Natural Science Foundation of China (No. 82205268) and Conventional Project of Shaanxi Provincial Sports Bureau (No. 2023132).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Atkins, D., Eccles, M., Flottorp, S., Guyatt, G. H., Henry, D., Hill, S., et al. (2004). Systems for grading the quality of evidence and the strength of recommendations I: critical appraisal of existing approaches the GRADE working group. BMC Health Serv. Res. 4. doi: 10.1186/1472-6963-4-38
Batra, P., Soni, K. D., and Mathur, P. (2020). Efficacy of probiotics in the prevention of VAP in critically ill ICU patients: an updated systematic review and meta-analysis of randomized control trials. J. Intensive Care 8:81. doi: 10.1186/s40560-020-00487-8
Bo, L., Li, J., Tao, T., Bai, Y., Ye, X., Hotchkiss, R. S., et al. (2014). Probiotics for preventing ventilator-associated pneumonia. Cochrane Database Syst. Rev. 10:CD009066. doi: 10.1002/14651858.CD009066.pub2
Bron, P. A., van Baarlen, P., and Kleerebezem, M. (2011). Emerging molecular insights into the interaction between probiotics and the host intestinal mucosa. Nat. Rev. Microbiol. 10, 66–78. doi: 10.1038/nrmicro2690
Cheema, H. A., Shahid, A., Ayyan, M., Mustafa, B., Zahid, A., Fatima, M., et al. (2022). Probiotics for the prevention of ventilator-associated pneumonia: an updated systematic review and Meta-analysis of randomised controlled trials. Nutrients 14:1600. doi: 10.3390/nu14081600
Chen, Z., Jiang, T., Peng, Y., Qiang, X., Yang, F., Haiyin, H., et al. (2022). Acupuncture and moxibustion treating lower urinary tract symptoms due to benign prostatic hyperplasia: a systematic review and network meta-analysis. Acupunct. Herb. Med. 2, 84–90. doi: 10.1097/HM9.0000000000000029
Chen, C., Wang, J., Yin, M., and Zhao, Q. (2018). Probiotics are effective in decreasing the incidence of ventilator-associated pneumonia in adult patients: a meta-analysis of randomized controlled trials. Int. J. Clin. Exp. Med. 11, 10269–10277.
Ferrer, M., and Torres, A. (2018). Epidemiology of ICU-acquired pneumonia. Curr. Opin. Crit. Care 24, 325–331. doi: 10.1097/MCC.0000000000000536
François, B., Cariou, A., Clere-Jehl, R., Dequin, P. F., Renon-Carron, F., Daix, T., et al. (2019). Prevention of early ventilator-associated pneumonia after cardiac arrest. N. Engl. J. Med. 381, 1831–1842. doi: 10.1056/NEJMoa1812379
Goutier, J. M., Holzmueller, C. G., Edwards, K. C., Klompas, M., Speck, K., and Berenholtz, S. M. (2014). Strategies to enhance adoption of ventilator-associated pneumonia prevention interventions: a systematic literature review. Infect. Control Hosp. Epidemiol. 35, 998–1005. doi: 10.1086/677152
Gu, W. J., Wei, C. Y., and Yin, R. X. (2012). Lack of efficacy of probiotics in preventing ventilator-associated pneumonia probiotics for ventilator-associated pneumonia: a systematic review and meta-analysis of randomized controlled trials. Chest 142, 859–868. doi: 10.1378/chest.12-0679
Hill, C., Guarner, F., Reid, G., Gibson, G. R., Merenstein, D. J., Pot, B., et al. (2014). Expert consensus document. The international scientific Association for Probiotics and Prebiotics consensus statement on the scope and appropriate use of the term probiotic. Nat. Rev. Gastroenterol. Hepatol. 11, 506–514. doi: 10.1038/nrgastro.2014.66
Huang, J., Liu, J., Liu, Z., Ma, J., Ma, J., Lv, M., et al. (2022). Reliability of the evidence to guide decision-making in acupuncture for functional dyspepsia. Front. Public Health 10:842096. doi: 10.3389/fpubh.2022.842096
Huang, J., Lu, M., Zheng, Y., Ma, J., Ma, X., Wang, Y., et al. (2021). Quality of evidence supporting the role of acupuncture for the treatment of irritable bowel syndrome. Pain Res. Manag. 2021:2752246. doi: 10.1155/2021/2752246
Ji, T., Zhu, X., Shang, F., and Zhang, X. (2021). Preventive effect of probiotics on ventilator-associated pneumonia: a Meta-analysis of 2428 patients. Ann. Pharmacother. 55, 949–962. doi: 10.1177/1060028020983021
Maselli, D. J., and Restrepo, M. I. (2011). Strategies in the prevention of ventilator-associated pneumonia. Ther. Adv. Respir. Dis. 5, 131–141. doi: 10.1177/1753465810395655
McAuley, L., Pham, B., Tugwell, P., and Moher, D. (2000). Does the inclusion of grey literature influence estimates of intervention effectiveness reported in meta-analyses? Lancet 356, 1228–1231. doi: 10.1016/S0140-6736(00)02786-0
Metersky, M. L., and Kalil, A. C. (2018). Management of ventilator-associated pneumonia: guidelines. Clin. Chest Med. 39, 797–808. doi: 10.1016/j.ccm.2018.08.002
Moher, D., Liberati, A., Tetzlaff, J., and Altman, D. G.PRISMA Group (2009). Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ 339:b2535. doi: 10.1136/bmj.b2535
Nanao, T., Nishizawa, H., Fujimoto, J., and Ogawa, T. (2021). Additional medical costs associated with ventilator-associated pneumonia in an intensive care unit in Japan. Am. J. Infect. Control 49, 340–344. doi: 10.1016/j.ajic.2020.07.027
Shea, B. J., Reeves, B. C., Wells, G., Thuku, M., Hamel, C., Moran, J., et al. (2017). AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ 358:j4008. doi: 10.1136/bmj.j4008
Shimizu, K., Hiroshi, O., Goto, M., Tasaki, O., Kuwagata, Y., Tanaka, H., et al. (2005). Synbiotics reduce the septic complications in patients with severe Sirs. Crit. Care Med. 33:A9. doi: 10.1097/00003246-200512002-00035
Shimizu, K., Ogura, H., Goto, M., Asahara, T., Nomoto, K., Morotomi, M., et al. (2009). Synbiotics decrease the incidence of septic complications in patients with severe SIRS: a preliminary report. Dig. Dis. Sci. 54, 1071–1078. doi: 10.1007/s10620-008-0460-2
Shimizu, K., Ogura, H., Goto, M., Asahara, T., Nomoto, K., Morotomi, M., et al. (2006). Altered gut flora and environment in patients with severe SIRS. J. Trauma 60, 126–133. doi: 10.1097/01.ta.0000197374.99755.fe
Shimizu, K., Ogura, H., Hamasaki, T., Goto, M., Tasaki, O., Asahara, T., et al. (2011). Altered gut flora are associated with septic complications and death in critically ill patients with systemic inflammatory response syndrome. Dig. Dis. Sci. 56, 1171–1177. doi: 10.1007/s10620-010-1418-8
Shimizu, K., Ojima, M., and Ogura, H. (2021). Gut microbiota and probiotics/Synbiotics for modulation of immunity in critically ill patients. Nutrients 13:2439. doi: 10.3390/nu13072439
Siempos, I. I., Ntaidou, T. K., and Falagas, M. E. (2010). Impact of the administration of probiotics on the incidence of ventilator-associated pneumonia: a meta-analysis of randomized controlled trials. Crit. Care Med. 38, 954–962. doi: 10.1097/CCM.0b013e3181c8fe4b
Song, H., Hu, W., Zhou, X., Tao, J., Zhang, S., Su, X., et al. (2022). Clinical benefits from administering probiotics to mechanical ventilated patients in intensive care unit: a PRISMA-guided meta-analysis. Front. Nutr. 8:798827. doi: 10.3389/fnut.2021.798827
Su, M., Jia, Y., Li, Y., Zhou, D., and Jia, J. (2020). Probiotics for the prevention of ventilator-associated pneumonia: a meta-analysis of randomized controlled trials. Respir. Care 65, 673–685. doi: 10.4187/respcare.07097
Sun, Y. C., Wang, C. Y., Wang, H. L., Yuan, Y., Lu, J. H., and Zhong, L. (2022). Probiotic in the prevention of ventilator-associated pneumonia in critically ill patients: evidence from meta-analysis and trial sequential analysis of randomized clinical trials. BMC Pulm. Med. 22:168. doi: 10.1186/s12890-022-01965-5
Tegegne, B. A., and Kebede, B. (2022). Probiotics, their prophylactic and therapeutic applications in human health development: a review of the literature. Heliyon 8:e09725. doi: 10.1016/j.heliyon.2022.e09725
Torres, A., Niederman, M. S., Chastre, J., Ewig, S., Fernandez-Vandellos, P., Hanberger, H., et al. (2017). International ERS/ESICM/ESCMID/ALAT guidelines for the management of hospital-acquired pneumonia and ventilator-associated pneumonia: guidelines for the management of hospital-acquired pneumonia (HAP)/ventilator-associated pneumonia (VAP) of the European Respiratory Society (ERS), European Society of Intensive Care Medicine (ESICM), European Society of Clinical Microbiology and Infectious Diseases (ESCMID) and Asociación Latinoamericana del Tórax (ALAT). Eur. Respir. J. 50:1700582. doi: 10.1183/13993003.00582-2017
Wang, J., Liu, K. X., Ariani, F., Tao, L. L., Zhang, J., and Qu, J. M. (2013). Probiotics for preventing ventilator-associated pneumonia: a systematic review and meta-analysis of high-quality randomized controlled trials. PLoS One 8:e83934. doi: 10.1371/journal.pone.0083934
Warren, D. K., Shukla, S. J., Olsen, M. A., Kollef, M. H., Hollenbeak, C. S., Cox, M. J., et al. (2003). Outcome and attributable cost of ventilator-associated pneumonia among intensive care unit patients in a suburban medical center. Crit. Care Med. 31, 1312–1317. doi: 10.1097/01.CCM.0000063087.93157.06
Weng, H., Li, J. G., Mao, Z., Feng, Y., Wang, C. Y., Ren, X. Q., et al. (2017). Probiotics for preventing ventilator-associated pneumonia in mechanically ventilated patients: a Meta-analysis with trial sequential analysis. Front. Pharmacol. 8:717. doi: 10.3389/fphar.2017.00717
Yang, K., Zhang, J., Zhao, L., Cheng, L., Li, Y., Kang, Y., et al. (2022). An umbrella review of Lianhua Qingwen combined with Western medicine for the treatment of coronavirus disease 2019. Acupunct. Herb. Med. 2, 143–151. doi: 10.1097/HM9.0000000000000041
Keywords: treatment, probiotics, ventilator-associated pneumonia, evidence, adjunctive
Citation: Han M, Wang K, Sun L, Liu W and Dong W (2024) Prevention of ventilator-associated pneumonia with probiotics: an overview of systematic reviews. Front. Microbiol. 15:1345278. doi: 10.3389/fmicb.2024.1345278
Edited by:
Jesús Muñoz-Rojas, Meritorious Autonomous University of Puebla, MexicoReviewed by:
Ricardo Carreno-Lopez, Benemérita Autonomous University of Puebla, MexicoCopyright © 2024 Han, Wang, Sun, Liu and Dong. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Wanhu Dong, ZG9jdG9yZG9uZzEyM0BzaW5hLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.