 Renqiang Yu
Renqiang Yu Yizhe Ma
Yizhe Ma Zichen Luo
Zichen Luo Ce Qi
Ce Qi Anni Xie
Anni Xie Yifan Jiang4
Yifan Jiang4 Jin Sun
Jin Sun
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
METHODS article
Front. Microbiol., 05 October 2023
Sec. Microorganisms in Vertebrate Digestive Systems
Volume 14 - 2023 | https://doi.org/10.3389/fmicb.2023.1267448
This article is part of the Research TopicRegulating Gut Microbiota by Lactic Acid Bacteria: Effects Based on Probiotic Characteristics and Their MetabolitesView all 21 articles
Background: Atopic dermatitis (AD) has increased rapidly with rapid urbanization; however, the treatment options for AD are lacking because the commonly used therapies can only alleviate symptoms. Limosilactobacillus reuteri (L. reuteri), FN041 is a specific strain isolated from human breast milk, and its protective potential against AD has been confirmed. This study aims to assess the efficacy of maternal consumption of L. reuteri FN041 during late pregnancy and lactation in preventing infantile AD.
Methods: First, a randomized, double-blind, placebo-controlled intervention study will be conducted on 340 pregnant females with babies at high risk for AD. These subjects will be randomly divided into four groups of different doses of L. reuteri FN041 (1 × 109, 5 × 109, and 1 × 1010 CFU/d) along with a placebo. The safety and efficacy of maternal use of L. reuteri FN041 for preventing infantile AD will be analyzed, and the most efficient dosage of L. reuteri FN041 will be determined. Subsequently, a multicenter cohort study of 500 pregnant females with babies at high risk for AD will be conducted to promote the maternal application of L. reuteri FN041. These subjects will be administered L. reuteri FN041 at the optimal dose determined during the first stage of late pregnancy and lactation, and their babies will be analyzed for AD development. Recruitment was initiated in October 2022.
Discussion: The primary outcome is the cumulative incidence of AD at 24 months after maternal consumption of L. reuteri FN041 during late pregnancy and lactation, whereas the secondary outcome is the efficiency of L. reuteri FN041 transfer from the mother’s gut to breast milk and then the infant’s gut after oral supplementation. This study will demonstrate the efficacy of edible probiotics isolated from breast milk in preventing or treating AD in infants. Accordingly, we provide population-based advice for administering specific probiotics for the primary prevention of AD in pregnant females. Understanding the underlying mechanisms of probiotic strains derived from breast milk can promote their application in preventing infant diseases associated with intestinal microbiota imbalance and immune disorders.
Clinical trial registration: https://www.chictr.org.cn/, identifier [ChiCTR2300075611].
Atopic dermatitis (AD) is an immune-associated inflammatory skin disease characterized by recurrent severe itching and dry skin (Langan et al., 2020). Severe itching affects sleep, growth, and development of young children (Nicholas et al., 2022; Wollenberg et al., 2023). Without effective intervention, infants with AD are susceptible to developing asthma, allergic rhinitis, and conjunctivitis (Elezbawy et al., 2023). The prevalence of AD among urban infants in China is rapidly increasing and similar conditions have been observed in other developing countries (Elezbawy et al., 2023). AD usually occurs early in life. In China in 2019, the total prevalence of AD in infants aged 1–12 months was 30.48%; among which, the incidence in infants aged 3 months was approximately 40.81% (Guo et al., 2019). Currently, clinical therapy commonly involves the use of glucocorticoids and immunosuppressive drugs; however, these drugs alleviate the clinical symptoms of AD only to a certain extent and may cause side effects (Wollenberg et al., 2023). Further, treatment with drugs is challenging in terms of limitations in drug selection for infants and young children (Wollenberg et al., 2023). Therefore, it is necessary to find suitable prevention and therapeutic strategies for infants and young children with AD.
Infant gut microbiota colonization and abnormal immune response are involved in the development of AD (Mahmud et al., 2022). In children with AD, the diversity of the gut microbiota and relative abundance of Lactobacilli and Bifidobacteria are substantially decreased, whereas the abundance of pathogenic bacteria such as Escherichia coli, Clostridium difficile, and Staphylococcus aureus is notably increased, compared to healthy individuals (Kim and Kim, 2019). Alterations in the gut bacterial community are correlated with disease severity (Kim and Kim, 2019). Previous data have revealed that exclusive breastfeeding in the first 3 months of life is associated with a lower incidence of AD in infants with a family history of allergic diseases (Gdalevich et al., 2001). This protective effect may be related to the microorganisms supplied by breast milk, which ensures a continuous supply of bacteria throughout the lactation period for infants (Lyons et al., 2020).
Interestingly, a recent meta-analysis summarized 21 relevant randomized controlled trials conducted in different countries and confirmed that supplementing mothers with composite probiotics before and after delivery can prevent infantile AD, whereas supplementing infants with probiotics may not effectively prevent the onset of AD (Amalia et al., 2020). Among these studies, five observed that probiotic mixture interventions during pregnancy and lactation reduced the incidence of AD in infants by approximately 28% (Amalia et al., 2020). However, in studies using a single probiotic strain, lactobacillus rhamnosus HN001 (HN001) or lactobacillus rhamnosus GG (LGG), for maternal supplementation did not reduce the incidence rate of AD in infants (Ou et al., 2012; Wickens et al., 2018). However, supplementation of both mothers and infants with HN001 during pregnancy and lactation can significantly reduce the incidence of AD by 2 years (Wickens et al., 2008). The main reason behind the poor preventive effects of probiotics against AD when administered to mothers during pregnancy and lactation, rather than to infants, may be explained by the fact that probiotics such as LGG cannot be effectively transmitted through breast milk to the infant’s intestines (Simpson et al., 2018). The key to preventing AD in infants via maternal consumption of probiotics is to use strains that can be transmitted from the mother’s gut to breast milk.
The infant gut microbiota changes rapidly in early life and gradually shifts to the adult composition during the first year after birth (Pickard et al., 2017). Breastfeeding has been suggested to be a key factor in establishing the infant gut microbiome (Baldassarre et al., 2018). According to entero-mammary pathway hypothesis, some bacteria in the mother’s gut can be transported to the breast through the lymphatic system and enter the infant’s gut via breast milk (Rodriguez, 2014). Our previous work demonstrated that secretory immunoglobulin A (sIgA)-coated bacteria are the key bacteria for vertical transmission from mother to child (Ding M. et al., 2022; Qi et al., 2022). In the agricultural and pastoral areas of the Gannan Tibetan Autonomous Prefecture of China, the relative abundance of Limosilactobacillus reuteri in human milk is far higher than that in other urbanized areas, which may contribute to the low incidence of allergic diseases (Chen, 2013; Ding et al., 2019). We previously used targeted sIgA immunomagnetic bead enrichment and separation technology to isolate a strain of sIgA-coated L. reuteri (isolation number FN041, patent strain storage number GDMCC60546) from the breast milk of Gannan females. This strain is included in the list of bacterium strains that can be used for food released by the National Health Commission and is a probiotic that can be used in ordinary food.
We also observed that maternal supplementation with L. reuteri FN041 during late gestation and lactation, along with offspring supplementation with L. reuteri FN041 after weaning, could effectively protect against AD (Zhao et al., 2022). In mice, the protective effect of maternal intervention with the sIgA-coated L. reuteri strain, which can be transmitted to milk, may modulate the intestinal microbiota community and the immune response of the offspring (Zhao et al., 2022; Qi et al., 2023). Moreover, further research has proven that the protective effect imparted by maternal supplementation with L. reuteri FN041 was much stronger than that imparted by the L. reuteri FN041 supplementation only in infant mice to prevent AD after weaning (Zhou et al., 2022). Therefore, assuming that maternal consumption of L. reuteri FN041 during pregnancy and lactation may be effective in preventing AD in offspring, we conducted a randomized controlled trial to provide data on this primary prevention strategy for AD.
This study aims to assess the incidence of infantile AD after maternal consumption of L. reuteri FN041 during late pregnancy and lactation. The optimum dosage will be determined by analyzing the efficacy of maternal supplementation with different doses of L. reuteri FN041 in preventing AD in offspring. Additionally, the secondary objective is to identify the transfer efficiency of L. reuteri FN041 from the mother’s gut to breast milk and then to infant’s gut after oral supplementation.
The study is divided into two stages. In the first stage, a multicenter, randomized, double-blind, placebo-controlled intervention study will be conducted in 340 pregnant females with babies at high risk for AD recruited from the Wuxi Maternity and Child Health Care Hospital affiliated with Jiangnan University and the Affiliated Hospital of Qingdao University. These subjects will be randomly divided into four groups (n = 85 for each group): (1) placebo group administered with the carrier solid beverage daily, (2) group administered with L. reuteri FN041 solid beverage at a dose of 1 × 109 CFU/d, (3) group administered with L. reuteri FN041 solid beverage at a dose of 5 × 109 CFU/d, and (4) group administered with L. reuteri FN041 solid beverage at a dose of 1 × 1010 CFU/d. Their offspring will be examined for AD development during the 2 years after birth so that the efficacy of maternal use of L. reuteri FN041 in the prevention of AD can be analyzed by calculating the cumulative incidence of AD in infants. Adverse reactions will be also recorded. Studies have reported that the most efficient dosage of L. reuteri FN041 can be determined within 6 months after birth, as infantile AD often develops in early life and peaks in the third month of life (Guo et al., 2019).
In the second stage of L. reuteri FN041 promotion and application, a multicenter cohort study in an expanded research population will be conducted. A total of 500 pregnant females with babies at a high risk for AD will be recruited from four tertiary hospitals: Wuxi Maternity and Child Health Care Hospital affiliated with Jiangnan University, Affiliated Hospital of Qingdao University, Suzhou Municipal Hospital, and Changzhou Maternal and Child Health Hospital. These subjects will be administered with L. reuteri FN041 at the optimal dosage determined in the first stage during late pregnancy and lactation; subsequently, their babies will be followed up for AD development for 2 years after birth.
According to the World Allergy Organization guidelines, a child may be considered at high risk for allergy if a biological parent or sibling has a history of allergic rhinitis, asthma, eczema, or food allergy (Fiocchi et al., 2015). The recruited pregnant females with babies at high risk for AD must meet the following inclusion criteria: healthy pregnant female (14–16 weeks of gestation), the mother or father of the fetus, or previous child of the couple diagnosed with any of the allergic diseases, including asthma, eczema, food allergy, or allergic rhinitis. This information will be confirmed by specific recruiters prior to recruitment. The risk of developing AD in infants without a family history of allergies is approximately 27%, whereas that in infants with one or two parents with an atopic history increases to 37.9 and 50.0%, respectively (Böhme et al., 2003). The population we aim to recruit meets the recommended probiotic target audience according to the guidelines of the World Allergy Organization (Fiocchi et al., 2015). The exclusion criteria are as follows: pregnant female under 16 years of age, multiple pregnancies, known fetal abnormalities, oral administration of immunosuppressive drugs or antibiotics, heart valve disease or immunodeficiency, undergoing dental surgery under antibiotic prevention, history of transplantation or HIV, long-term continuous use or ongoing use or intent to use probiotics before admission, external fertilization pregnancy, previous participation in research, deemed unsuitable for inclusion in the study owing to other medical reasons, and gestational diabetes.
The cumulative incidence of AD in high-risk infants at 1 and 2 years of age is reported to be approximately 40.1 and 41%, respectively, based on previous studies conducted in other countries (Rautava et al., 2012; Chaoimh et al., 2023). According to a previous study carried out in 2022 in our hospital, the overall point prevalence of AD in infants aged 0–24 months was 50.5% in Wuxi (Ding Y. et al., 2022). The expected cumulative incidence of AD after L. reuteri administration is approximately 20%, with a relative 20% reduction in AD incidence of 40% through intervention. Assuming that the first type of error would be 2.5% and the efficacy would be 80%, we calculated the sample using online tools.1 The sample size in each group would be 74. Considering a 10% dropout rate, each group should recruit 85 research subjects in the first stage. In the second stage of the trial, the sample size is expected to be approximately 500, which is considered sufficient to further verify the efficacy of maternal use of L. reuteri FN041 in the prevention of infantile AD.
The researchers will screen and record the medical history of participants and obtain written informed consent from the recruited participants with a detailed explanation. On the informed consent form, the recruited subjects will be asked whether they agree to share their data and donate their breast milk, cord blood, and feces.
The L. reuteri strain used in this study is a probiotic supplement derived from breast milk and formulated in the form of a solid beverage with highly acceptable properties. The solid beverage contained fructooligosaccharides, erythritol, stachyose, resistant dextrin, strawberry juice powder, and vitamin C. The products of the solid beverages with and without L. reuteri have the same taste and are packed at 1.5 g per package. Limosilactobacillus reuteri has been reported to colonize the intestines of almost all vertebrates and mammals, has good biocompatibility, and is widely used for food production. We previously used targeted sIgA immunomagnetic bead enrichment and separation technology (patent number ZL201610975479. X) to isolate a strain of sIgA-coated L. reuteri FN041 (patent strain storage number: GDMCC60546) from Gannan breast milk. This species is included in the list of bacterium strains that can be used for food released by the National Health Commission and is a probiotic that can be used in ordinary food. Genome sequencing analysis revealed that L. reuteri FN041 has no horizontally transmissible antibiotic resistance or pathogenic genes.
The selected doses (1 × 109, 5 × 109, and 1 × 1010 CFU/d) of L. reuteri FN041 in the first stage are in the reported safe range and the optimal dosage will be determined and subsequently applied in the second stage. The World Allergy Organization recommends probiotic administration to pregnant females at high risk of bearing a child with allergy during pregnancy and, in case of breastfeeding, lactation (Fiocchi et al., 2015). Therefore, oral intervention with the respective solid drinks for the recruited subjects in the two stages will start from the gestational age of 32–36 weeks until delivery. The mothers will continue to consume the corresponding solid drinks daily for 6 months, from 1 to 3 days after delivery, during the lactation period. All the solid drinks are suggested to be taken orally at bedtime once daily.
Participants will be allowed to withdraw from the research at any time without consequences.
The project team comprises pediatricians, dermatologists, pediatric nurses, and clinical researchers. This study will ensure that the health or interests of the research subjects are not harmed. We will acknowledge the support of research participants to gain active cooperation. At the beginning of the project, technical training will be provided to the researchers, and specific researchers will regularly contact the subjects to record data. Researchers will regularly follow up, promptly inquire, and collect information on changes in the physical condition of pregnant females and infants and ensure the consumption of probiotics. A mobile app will be developed to strengthen the interaction between researchers and subjects. Participants who fail to complete the entire experimental process will be inquired about their reasons. To ensure the reliability of the results, every effort should be made to keep the number of dropouts below 10%; otherwise, additional research will have to be conducted.
During the research period, neither mothers nor infants will use any probiotic products other than those used in this experiment. Mothers will be encouraged to breastfeed their infants and will be provided with the necessary medical guidance.
The participants recruited in this study will be grouped randomly in the first stage of project implementation so that they are consistent with each group according to their age, economic situation, educational level, and other influencing factors.
In the first stage, both the on-site and laboratory analyses will be conducted using a double-blind method. The samples of L. reuteri and placebo used in the experiment will be processed and produced by a third-party company. The project organizer, researchers, and participants will not be informed about the intervention methods they receive. The biological samples analyzed by laboratory technicians (including blood, breast milk, and feces) will be blinded to their specific sources and grouping situations until the end of all experiments.
In the second stage, a multicenter cohort study will be conducted, in which the recruited subjects will not be blinded because this stage has been designed to explore the efficacy of maternal intervention with L. reuteri in preventing infantile AD.
The data obtained in this study can be divided into continuous and categorical variables, which are presented as the mean ± standard deviation or median with interquartile range and frequency with percentage, respectively. Continuous variables will be analyzed for differences among the groups using ANOVA, whereas categorical variables will be analyzed using the chi-squared test. A two-sided p-value of <0.05 will be considered statistically significant.
Pregnant females will be recruited at 14–16 weeks of gestation and receive intervention strategy at 32–36 weeks of gestation. Their infants will be followed-up for 2 years after birth. Clinical follow-up will be conducted in the hospital at 1, 3, 6, 8, and 12 months of age, and telephone follow-up will be conducted at 2, 4, 5, 10, and 24 months of age. Two specific pediatric attending doctors are responsible for the clinical follow-up of the infants. Infants suspected of having AD will be referred to the pediatric dermatology clinic, and two designated pediatric dermatologists will jointly diagnose and assess disease severity. Questionnaire surveys will be completed at each clinical and telephone follow-up. Parents will be instructed to contact the project team immediately and take the infant to two designated pediatric dermatologists for diagnosis and treatment if the baby is suspected of developing AD during 0–2 years of age. A detailed flowchart of the study is shown in Figure 1.
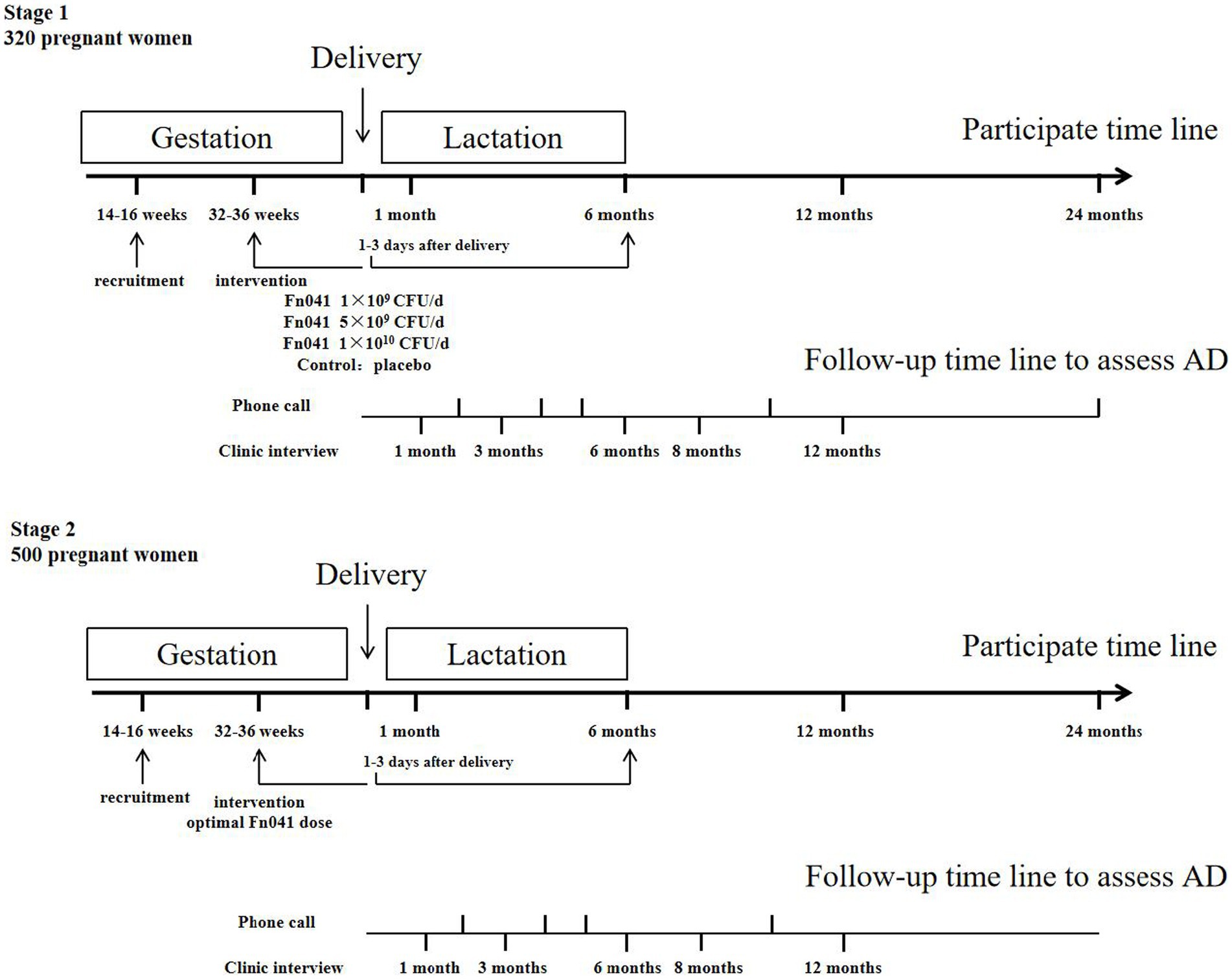
Figure 1. Timeline of the study.
Clinical follow-up of the infants will be conducted at 7 and 42 days of age, and telephone follow-up will be conducted at 6, 12, and 24 months of age. Questionnaire surveys will be completed at each clinical and telephone follow-up. The infant-specific questionnaire is designed based on the International Study on Asthma and Allergy in Children. Detailed information on birth parity, number of births (single or multiple births), gestational age, mode of delivery, weight (including birth weight), length (including birth length), feeding mode (breast, formula-, or mixed-fed), maternal and infant exposure to antibiotics and probiotics, parental smoking, family history of allergic diseases, infection, and other potential confounding factors will be recorded.
The mother’s feces will be collected within 1 week before intervention with solid beverage and the first week after delivery, whereas breast milk samples (approximately 5–10 mL each time) will be collected at 1–6 (colostrum), 7–15 (transitional milk), and 16–30 (mature milk) d after childbirth. Cord blood will be collected at the time of birth. Fecal samples (approximately 0.5–6 g each time) will be collected from infants in the colostrum, during transitional lactation, and at the ages of 1, 6, and 12 months after birth.
The maternal dietary survey is designed to be carried out before and after probiotic intervention (that is, 6 months after delivery). The dietary and nutritional status survey will be conducted using a 24-h dietary recall method to investigate the intake of various foods by the study participants within 3 days. Their energy and nutrient intake will be analyzed. The food frequency questionnaire will be used to collect information on the types and frequencies of food intake among all study participants and evaluate their dietary structure.
In both stages of the trial, the cumulative incidence of AD within 2 years of delivery will be analyzed as the primary outcome. The diagnosis of AD is based on the Williams standard, as previously described, which is widely applicable to outpatient and general population epidemiological investigations in research (Williams et al., 1994). Skin itching is the primary criterion. The secondary criteria are as follows: (1) history of skin involvement on the flexor side, including the cubital fossa, cochineal fossa, anterior malleolus, and neck; (2) history of asthma, allergic rhinitis, or AD in first-degree relatives of children under 4 years of age; (3) history of dry skin throughout the body; (4) eczema on the flexed side (on the cheek or forehead and limbs on the extended side in children under 4 years of age); and (5) onset before the age of 2 years. Infants who meet the main criteria, along with three or more secondary criteria, will be diagnosed with AD. Once diagnosed with AD, disease severity will be assessed using the SCORAD index. Accordingly, infants will be divided into mild (SCORAD: 0–24 points), moderate (SCORAD: 25–50 points), and severe (SCORAD: >50 points) groups (Oranje et al., 2007).
The severity of gastrointestinal and respiratory symptoms will be analyzed as a secondary outcome. Meanwhile, regulatory T cells in umbilical cord blood at birth (n = 20 for each group) will be analyzed via flow cytometry and the levels of transforming growth factor-β, interleukin (IL)-10, IL-12, IL-13, IL-4, interferon-γ (IFN-γ), tumor necrosis factor-α, and total IgE will be determined using enzyme-linked immunosorbent assay. Further, colostrum and 42-day mature milk level of transforming growth factor-β and IL-10 will be tested. Moreover, the relative abundance of sIgA-coated L. reuteri FN041 will be analyzed in breast milk and infant feces using strain-specific PCR, depending on the genome sequence information. Lactobacillus strains will be isolated and determined using 16 s rRNA sequencing, metagenomic sequencing will be performed to analyze L. reuteri FN041 (n = 10 for each group), and StrainPhlAn3 will be used to analyze the data at the strain level (Walsh et al., 2017).
Given that AD is a common pediatric skin disease with an increasing economic burden and limitations of clinical medication, there is an urgent need to develop new strategies for disease prevention in infants. Studies on the gut–skin axis have revealed the key role of gut microbiome dysbiosis in the development of immune-mediated AD (Mahmud et al., 2022). Supplementing mothers with probiotics during late pregnancy and lactation is effective in preventing AD in their offspring, whereas supplementing infants alone with probiotics may not be effective in alleviating AD (Baldassarre et al., 2018). Probiotic supplementation during pregnancy increases the IFN-γ level in cord blood and immunomodulatory factors in breast milk (Prescott et al., 2008). Infants may develop AD when they have impaired IFN-γ activation, which disrupts the Th1/Th2 balance and leads to AD (Herberth et al., 2010; Brar and Leung, 2016). Studies have also revealed that human breast milk is a source of commensal bacteria that are beneficial for the gut health of offspring (Lyons et al., 2020). Gut-specific strict anaerobes and facultative anaerobic bacteria such as Bifidobacteria and Lactobacilli can be detected in breast milk (Gronlund et al., 2007). Two IgA molecules in the intestinal tract bind to each other through secreted fragments to form sIgA, which can wrap around bacteria in the intestinal tract (Rochereau et al., 2013). sIgA-coated bacteria can be transported into intestinal Peyer’s patches and carried by dendritic cells to the mammary glands (Macpherson and Uhr, 2004).
The mechanism of probiotic transmission from mothers to infants remains unclear, which hinders the isolation, screening, and application of probiotic strains for AD prevention. We previously observed that sIgA-coated bacteria are key functional bacteria for vertical transmission between mother and child and that breast milk is a good source of sIgA-coated probiotics (Cui et al., 2020; Ding M. et al., 2022). Limosilactobacillus reuteri is a well-studied probiotic bacterium detected in breast milk (Mu et al., 2018). Previous studies have reported the therapeutic potential of L. reuteri in the management of allergic diseases (Forsythe et al., 2007; Karimi et al., 2009). Using a patented technology developed by our group, sIgA-coated L. reuteri FN041 was isolated. Preclinical experiments have confirmed the therapeutic potential of L. reuteri FN041 in preventing AD (Qi et al., 2021; Zhou et al., 2022). Maternal mice supplemented with L. reuteri FN041 can promote the expression of intestinal antimicrobial peptides and enhance the mucosal barrier function and intestinal sIgA production by remodeling the gut microbiota in their offspring (Qi et al., 2021).
A previous study showed that no adverse reactions were observed in individuals supplemented with live L. reuteri at a daily dose of 1 × 108 to 1 × 1010 CFU (Mobini et al., 2017). A meta-analysis of eight randomized controlled trials of probiotic application in >1,500 pregnant females also revealed that probiotic consumption from 32 to 36 weeks of gestation did not increase the incidence of abortion or malformations and had no effect on birth weight, gestational age, or delivery mode (Dugoua et al., 2009). In the first stage of this clinical trial, we will assess the safety of maternal L. reuteri FN041 supplementation. We aim to determine the optimal dose of maternal L. reuteri FN041 during pregnancy and lactation for infantile AD prevention. In the second stage of the study, we intend to promote the application of maternal L. reuteri FN041 supplementation in a multicenter setting to evaluate the incidence of AD after the intervention. In addition, L. reuteri FN041 in breast milk and infant feces, detected using metagenomic sequencing and StrainPhlAn3 analysis, indicate that a specific strain L. reuteri FN041 can be transmitted to infants through breast milk, providing new evidence for vertical transmission in maternal and infant microbiomes.
Importantly, previous clinical studies have confirmed the protective action of a mixture of probiotics against AD. Here, we aim to identify the potential role of a more efficient single strain of L. reuteri FN041 in AD prevention. We have discovered that its ability to adhere to mucus is far superior to that of LGG and L. reuteri DSM17938 (unpublished data), which may explain its better preventive effect against AD than LGG and L. reuteri DSM17938 in an established AD mouse model (Zhou et al., 2022).
In addition, the regulations regarding the consumption of probiotics by infants in China are strict. Currently, only 14 strains of probiotics are allowed for infants under 1 year of age, and the approval of these 14 strains for infant consumption is mainly based on safety considerations rather than functional perspectives. Notably, all commercial strains used to prevent AD in clinical practice are isolated from the intestines of Western adults, and China has not yet developed probiotics for preventing AD. Therefore, there is an urgent need to identify probiotics in domestic breast milk that can effectively prevent infantile AD. The results of this clinical trial provide evidence for the efficacy of L. reuteri strain FN041 isolated from breast milk in preventing or curing AD in infants and provide practical advice for the supplementation of specific probiotics for the primary prevention of AD in pregnant females. Because the immunological mechanisms of AD are similar to those of other allergic diseases, understanding the mechanisms of breast milk-derived probiotic strains can contribute to their application in maternal nutritional intervention strategies to prevent diseases caused by the interaction between the infant intestinal microbiota and the immune system.
This study is in its first stage, from October 2022 to December 2025. Subject recruitment in the first stage commenced from July 2023 and will be continued till December 2023. Subject recruitment in the second stage will start from July 2024 to December 2024.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding authors.
RY: Conceptualization, Funding acquisition, Writing – original draft. YM: Funding acquisition, Writing – original draft. ZL: Conceptualization, Writing – original draft. CQ: Methodology, Supervision, Validation, Writing – review & editing. AX: Methodology, Writing – review & editing. YJ: Software, Writing – review & editing. BZ: Project administration, Resources, Supervision, Visualization, Writing – review & editing. JS: Conceptualization, Methodology, Supervision, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work is supported by the Jiangsu Provincial Department of Science and Technology (No. BE2022698), the Wuxi Science and Technology Bureau (No. Y20222003), the Wuxi Municipal Medical Innovation Team (No. CXTD2021013), and the Wuxi Commission of Health and Family Planning (Nos. SW202201 and FYKY202109).
We would like to thank Bullet Edits for English language editing.
The authors declare that the research is conducted in the absence of any commercial or financial relationships that can be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
AD, Atopic dermatitis; L. reuteri, Limosilactobacillus reuteri; RCT, randomized controlled trial; HN001, Lactobacillus rhamnosus HN001; LGG, Lactobacillus rhamnosus GG; sIgA, secretory immunoglobulin A; IFN-γ, interferon-γ; Tregs, regulatory T cells; IL, interleukin.
Amalia, N., Orchard, D., Francis, K. L., and King, E. (2020). Systematic review and meta-analysis on the use of probiotic supplementation in pregnant mother, breastfeeding mother and infant for the prevention of atopic dermatitis in children. Australas. J. Dermatol. 61, e158–e173. doi: 10.1111/ajd.13186
Baldassarre, M. E., Palladino, V., Amoruso, A., Pindinelli, S., Mastromarino, P., Fanelli, M., et al. (2018). Rationale of probiotic supplementation during pregnancy and neonatal period. Nutrients 10:1693. doi: 10.3390/nu10111693
Böhme, M. W., Nordvall, S. L., Svartengren, M., and Wahlgren, C. F. (2003). Family history and risk of atopic dermatitis in children up to 4 years. Clin. Exp. Allergy 33, 1226–1231. doi: 10.1046/j.1365-2222.2003.01749.x
Brar, K., and Leung, D. Y. (2016). Recent considerations in the use of recombinant interferon gamma for biological therapy of atopic dermatitis. Expert. Opin. Biol. Ther. 16, 507–514. doi: 10.1517/14712598.2016.1135898
Chaoimh, C. N., Lad, D., Nico, C., Puppels, G. J., Wong, X. F. C. C., Common, J. E., et al. (2023). Early initiation of short-term emollient use for the prevention of atopic dermatitis in high-risk infants-the STOP-AD randomised controlled trial. Allergy 78, 984–994. doi: 10.1111/all.15491
Chen, Y. (2013). Third nationwide survey of childhood asthma in urban areas of China. Zhonghua Er Ke Za Zhi 51, 729–735. doi: 10.3760/cma.j.issn.0578-1310.2013.10.003
Cui, M., Qi, C., Yang, L., Zhang, M., Wang, H., She, G., et al. (2020). A pregnancy complication-dependent change in SIgA-targeted microbiota during third trimester. Food Funct. 11, 1513–1524. doi: 10.1039/c9fo02919b
Ding, M., Chen, H., Yu, R., Ross, R. P., Stanton, C., Zhang, H., et al. (2022). Shared and non-shared sIgA-coated and -uncoated Bacteria in intestine of mother-infant pairs. Int. J. Mol. Sci. 23:9873. doi: 10.3390/ijms23179873
Ding, M., Qi, C., Yang, Z., Jiang, S., Bi, Y., Lai, J., et al. (2019). Geographical location specific composition of cultured microbiota and Lactobacillus occurrence in human breast milk in China. Food Funct. 10, 554–564. doi: 10.1039/c8fo02182a
Ding, Y., Qiu, T., and Zhang, H. (2022). An analysis of influencing factors for eczema in 301 infants. Jiangsu Med. J. 48, 606–608. doi: 10.19460/j.cnki.0253-3685.2022.06.016
Dugoua, J. J., Machado, M., Zhu, X., Chen, X., Koren, G., and Einarson, T. R. (2009). Probiotic safety in pregnancy: a systematic review and meta-analysis of randomized controlled trials of Lactobacillus, Bifidobacterium, and Saccharomyces spp. J. Obstet. Gynaecol. Can. 31, 542–552. doi: 10.1016/S1701-2163(16)34218-9
Elezbawy, B., Fasseeh, A. N., Fouly, E., Tannira, M., Dalle, H., Aderian, S., et al. (2023). Humanistic and economic burden of atopic dermatitis for adults and adolescents in the Middle East and Africa region. Dermatol. Ther. 13, 131–146. doi: 10.1007/s13555-022-00857-0
Fiocchi, A., Pawankar, R., Cuello-Garcia, C., Ahn, K., Al-Hammadi, S., Agarwal, A., et al. (2015). World allergy organization-McMaster University guidelines for allergic disease prevention (GLAD-P): probiotics. World Allergy Organ. J. 8:4. doi: 10.1186/s40413-015-0055-2
Forsythe, P., Inman, M. D., and Bienenstock, J. (2007). Oral treatment with live Lactobacillus reuteri inhibits the allergic airway response in mice. Am. J. Respir. Crit. Care Med. 175, 561–569. doi: 10.1164/rccm.200606-821OC
Gdalevich, M., Mimouni, D., David, M., and Mimouni, M. (2001). Breast-feeding and the onset of atopic dermatitis in childhood: a systematic review and meta-analysis of prospective studies. J. Am. Acad. Dermatol. 45, 520–527. doi: 10.1067/mjd.2001.114741
Gronlund, M. M., Gueimonde, M., Laitinen, K., Kociubinski, G., Gronroos, T., Salminen, S., et al. (2007). Maternal breast-milk and intestinal bifidobacteria guide the compositional development of the Bifidobacterium microbiota in infants at risk of allergic disease. Clin. Exp. Allergy 37, 1764–1772. doi: 10.1111/j.1365-2222.2007.02849.x
Guo, Y., Zhang, H., Liu, Q., Wei, F., Tang, J., Li, P., et al. (2019). Phenotypic analysis of atopic dermatitis in children aged 1-12 months: elaboration of novel diagnostic criteria for infants in China and estimation of prevalence. J. Eur. Acad. Dermatol. Venereol. 33, 1569–1576. doi: 10.1111/jdv.15618
Herberth, G., Heinrich, J., Roder, S., Figl, A., Weiss, M., Diez, U., et al. (2010). Reduced IFN-gamma- and enhanced IL-4-producing CD4+ cord blood T cells are associated with a higher risk for atopic dermatitis during the first 2 yr of life. Pediatr. Allergy Immunol. 21, 5–13. doi: 10.1111/j.1399-3038.2009.00890.x
Karimi, K., Inman, M. D., Bienenstock, J., and Forsythe, P. (2009). Lactobacillus reuteri-induced regulatory T cells protect against an allergic airway response in mice. Am. J. Respir. Crit. Care Med. 179, 186–193. doi: 10.1164/rccm.200806-951OC
Kim, J. E., and Kim, H. S. (2019). Microbiome of the skin and gut in atopic dermatitis (AD): understanding the pathophysiology and finding novel management strategies. J. Clin. Med. 8:444. doi: 10.3390/jcm8040444
Langan, S. M., Irvine, A. D., and Weidinger, S. (2020). Atopic dermatitis. Lancet 396, 345–360. doi: 10.1016/S0140-6736(20)31286-1
Lyons, K. E., Ryan, C. A., Dempsey, E. M., Ross, R. P., and Stanton, C. (2020). Breast Milk, a source of beneficial microbes and associated benefits for infant health. Nutrients 12:1039. doi: 10.3390/nu12041039
Macpherson, A. J., and Uhr, T. (2004). Induction of protective IgA by intestinal dendritic cells carrying commensal bacteria. Science 303, 1662–1665. doi: 10.1126/science.1091334
Mahmud, M. R., Akter, S., Tamanna, S. K., Mazumder, L., Esti, I. Z., Banerjee, S., et al. (2022). Impact of gut microbiome on skin health: gut-skin axis observed through the lenses of therapeutics and skin diseases. Gut Microbes 14:2096995. doi: 10.1080/19490976.2022.2096995
Mobini, R., Tremaroli, V., Stahlman, M., Karlsson, F., Levin, M., Ljungberg, M., et al. (2017). Metabolic effects of Lactobacillus reuteri DSM 17938 in people with type 2 diabetes: a randomized controlled trial. Diabetes Obes. Metab. 19, 579–589. doi: 10.1111/dom.12861
Mu, Q., Tavella, V. J., and Luo, X. M. (2018). Role of Lactobacillus reuteri in human health and diseases. Front. Microbiol. 9:757. doi: 10.3389/fmicb.2018.00757
Nicholas, M. N., Keown-Stoneman, C. D. G., Maguire, J. L., and Drucker, A. M. (2022). Association between atopic dermatitis and height, body mass index, and weight in children. JAMA Dermatol. 158, 26–32. doi: 10.1001/jamadermatol.2021.4529
Oranje, A. P., Glazenburg, E. J., Wolkerstorfer, A., and de Waard-van der Spek, F. B. (2007). Practical issues on interpretation of scoring atopic dermatitis: the SCORAD index, objective SCORAD and the three-item severity score. Br. J. Dermatol. 157, 645–648. doi: 10.1111/j.1365-2133.2007.08112.x
Ou, C. Y., Kuo, H. C., Wang, L., Hsu, T. Y., Chuang, H., Liu, C. A., et al. (2012). Prenatal and postnatal probiotics reduces maternal but not childhood allergic diseases: a randomized, double-blind, placebo-controlled trial. Clin. Exp. Allergy 42, 1386–1396. doi: 10.1111/j.1365-2222.2012.04037.x
Pickard, J. M., Zeng, M. Y., Caruso, R., and Nunez, G. (2017). Gut microbiota: role in pathogen colonization, immune responses, and inflammatory disease. Immunol. Rev. 279, 70–89. doi: 10.1111/imr.12567
Prescott, S. L., Wickens, K., Westcott, L., Jung, W., Currie, H., Black, P. N., et al. (2008). Supplementation with Lactobacillus rhamnosus or Bifidobacterium lactis probiotics in pregnancy increases cord blood interferon-gamma and breast milk transforming growth factor-beta and immunoglobin a detection. Clin. Exp. Allergy 38, 1606–1614. doi: 10.1111/j.1365-2222.2008.03061.x
Qi, C., Ding, M., Li, S., Zhou, Q., Li, D., Yu, R., et al. (2021). Sex-dependent modulation of immune development in mice by secretory IgA-coated Lactobacillus reuteri isolated from breast milk. J. Dairy Sci. 104, 3863–3875. doi: 10.3168/jds.2020-19437
Qi, C., Tu, H., Zhao, Y., Zhou, J., Chen, J., Hu, H., et al. (2023). Breast Milk-derived Limosilactobacillus reuteri prevents atopic dermatitis in mice via activating retinol absorption and metabolism in Peyer's patches. Mol. Nutr. Food Res. 67:e2200444. doi: 10.1002/mnfr.202200444
Qi, C., Zhou, J., Tu, H., Tu, R., Chang, H., Chen, J., et al. (2022). Lactation-dependent vertical transmission of natural probiotics from the mother to the infant gut through breast milk. Food Funct. 13, 304–315. doi: 10.1039/d1fo03131g
Rautava, S., Kainonen, E., Salminen, S., and Isolauri, E. (2012). Maternal probiotic supplementation during pregnancy and breast-feeding reduces the risk of eczema in the infant. J. Allergy Clin. Immunol. 130, 1355–1360. doi: 10.1016/j.jaci.2012.09.003
Rochereau, N., Drocourt, D., Perouzel, E., Pavot, V., Redelinghuys, P., Brown, G. D., et al. (2013). Dectin-1 is essential for reverse transcytosis of glycosylated SIgA-antigen complexes by intestinal M cells. PLoS Biol. 11:e1001658. doi: 10.1371/journal.pbio.1001658
Rodriguez, J. M. (2014). The origin of human milk bacteria: is there a bacterial entero-mammary pathway during late pregnancy and lactation? Adv. Nutr. 5, 779–784. doi: 10.3945/an.114.007229
Simpson, M. R., Avershina, E., Storro, O., Johnsen, R., Rudi, K., and Oien, T. (2018). Breastfeeding-associated microbiota in human milk following supplementation with Lactobacillus rhamnosus GG, Lactobacillus acidophilus La-5, and Bifidobacterium animalis ssp. lactis Bb-12. J. Dairy Sci. 101, 889–899. doi: 10.3168/jds.2017-13411
Walsh, A. M., Crispie, F., Daari, K., O'Sullivan, O., Martin, J. C., Arthur, C. T., et al. (2017). Strain-level metagenomic analysis of the fermented dairy beverage Nunu highlights potential food safety risks. Appl. Environ. Microbiol. 83, e01144–e01117. doi: 10.1128/AEM.01144-17
Wickens, K., Barthow, C., Mitchell, E. A., Stanley, T. V., Purdie, G., Rowden, J., et al. (2018). Maternal supplementation alone with Lactobacillus rhamnosus HN001 during pregnancy and breastfeeding does not reduce infant eczema. Pediatr. Allergy Immunol. 29, 296–302. doi: 10.1111/pai.12874
Wickens, K., Black, P. N., Stanley, T. V., Mitchell, E., Fitzharris, P., Tannock, G. W., et al. (2008). A differential effect of 2 probiotics in the prevention of eczema and atopy: a double-blind, randomized, placebo-controlled trial. J. Allergy Clin. Immunol. 122, 788–794. doi: 10.1016/j.jaci.2008.07.011
Williams, H. C., Burney, P. G., Hay, R. J., Archer, C. B., Shipley, M. J., Hunter, J. J., et al. (1994). The U.K. working Party's diagnostic criteria for atopic dermatitis. I. Derivation of a minimum set of discriminators for atopic dermatitis. Br. J. Dermatol. 131, 383–396. doi: 10.1111/j.1365-2133.1994.tb08530.x
Wollenberg, A., Werfel, T., Ring, J., Ott, H., Gieler, U., and Weidinger, S. (2023). Atopic dermatitis in children and adults-diagnosis and treatment. Dtsch. Arztebl. Int. 120, 224–234. doi: 10.3238/arztebl.m2023.0011
Zhao, Y., Qi, C., Li, X., Lu, M., Zhang, H., Zhou, J., et al. (2022). Prevention of atopic dermatitis in mice by Lactobacillus Reuteri Fn041 through induction of regulatory T cells and modulation of the gut microbiota. Mol. Nutr. Food Res. 66:e2100699. doi: 10.1002/mnfr.202100699
Zhou, J., Xu, G., Li, X., Tu, H., Li, H., Chang, H., et al. (2022). Limosilactobacillus reuteri FN041 prevents atopic dermatitis in pup mice by remodeling the ileal microbiota and regulating gene expression in Peyer's patches after vertical transmission. Front. Nutr. 9:987400. doi: 10.3389/fnut.2022.987400
Keywords: atopic dermatitis, Limosilactobacillus reuteri, infant, microbiota, breast milk, probiotics
Citation: Yu R, Ma Y, Luo Z, Qi C, Xie A, Jiang Y, Zhu B and Sun J (2023) Maternal supplementation with Limosilactobacillus reuteri FN041 for preventing infants with atopic dermatitis: study protocol for a randomized controlled trial. Front. Microbiol. 14:1267448. doi: 10.3389/fmicb.2023.1267448
Edited by:
Renpeng Du, Heilongjiang University, ChinaReviewed by:
Xiang Hong, Southeast University, ChinaCopyright © 2023 Yu, Ma, Luo, Qi, Xie, Jiang, Zhu and Sun. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Baoli Zhu, NDc1MTc4MTUxQHFxLmNvbQ==; Jin Sun, c3VuakBxZHUuZWR1LmNu
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.