 Inmaculada Pérez-Prieto
Inmaculada Pérez-Prieto Axel Skafte-Holm
Axel Skafte-Holm Jørgen Skov Jensen
Jørgen Skov Jensen
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Microbiol. , 13 June 2022
Sec. Infectious Agents and Disease
Volume 13 - 2022 | https://doi.org/10.3389/fmicb.2022.914874
This article is part of the Research Topic Mollicutes: From Evolution To Pathogenesis, Volume II View all 20 articles
Mycoplasma penetrans has gained increased attention in relation to sexually transmitted infections, however, its pathogenic potential and prevalence in different populations remains to be elucidated. Among 293 Chlamydia trachomatis positive rectal samples submitted for lymphogranuloma venereum typing, M. penetrans was detected by PCR in 13.4% of 231 male samples.
Sexually transmitted infections (STIs) are caused by a wide range of bacteria, viruses and parasites. According to WHO estimates, more than 1 million STIs occur every day, emerging as an increasing reproductive and sexual health concern worldwide (World Health Organization, 2019). In this context, a high prevalence of STIs among men who have sex with men (MSM) is reported, with Chlamydia trachomatis and Neisseria gonorrhoeae being the most important (Workowski et al., 2021). Serotype L1-L3 of C. trachomatis causes lymphogranuloma venereum (LGV), a destructive and aggressive sexually transmitted infection affecting tissue and lymph nodes, predominantly associated with rectal infection in MSM in developed countries (Stoner and Cohen, 2015). Thus, genotyping of C. trachomatis positive rectal samples has been recommended since these infections require extended duration of therapy (De Vries et al., 2019).
A significant proportion of patients with STI symptoms have no identified etiological agents detected. Advances in molecular methods have allowed the search for unidentified pathogens by non-culture-dependent techniques. In this regard, several studies have reported the presence of Mycoplasma spp., primarily M. genitalium, in conditions such as non-gonococcal urethritis (NGU) (Jensen et al., 1993; Taylor-Robinson et al., 2003). In addition, a recent publication found M. penetrans to be associated with NGU primarily in MSM (Srinivasan et al., 2021). Since anal sex increases the risk for extra-genital infections, we assessed the prevalence of M. penetrans in C. trachomatis positive rectal samples submitted for LGV typing.
Chlamydia trachomatis positive samples from diagnostic laboratories throughout Denmark between March and October 2021 were submitted for molecular LGV typing in the reference laboratory at Statens Serum Institut. Of the 837 original samples, remnants of 293 rectal samples were available and anonymized to gender and age, and analyzed for M. penetrans. According to Danish law, an ethical committee approval was not required due to the anonymized nature of the dataset.
DNA was extracted from the samples submitted in the nucleic acid amplification test transport medium by processing 1 ml of sample using the Large Volume Universal Pathogen Extraction protocol in a MagNA Pure 96 instrument (Roche Diagnostics, Hvidovre, Denmark) and was eluted into 100 μl.
Mycoplasma penetrans was detected by qPCR as previously described (Srinivasan et al., 2021), except that an internal process control (IPC) was constructed in order to detect Taq DNA polymerase inhibitors or suboptimal reaction conditions (Jensen et al., 2003). Each assay was performed in a 50 μl final reaction volume in a 7,500 Real-Time PCR System instrument (Thermo Fisher Scientific, Waltham, MA, United States), programmed for 95°C for 2 min and 50 cycles of 95°C for 15 s and annealing and extension at 60°C for 1 min. Standard curves were prepared with serial dilutions of M. penetrans DNA containing 50,000 to 5 copies.
Results of M. penetrans detection are summarized in Table 1. A total of 293 rectal samples (231 of male and 62 of female origin) were included in this study. The median age was 30 years ranging from 16 to 69. Overall, M. penetrans was detected more frequently in male C. trachomatis positive samples with a prevalence of 13.4% (95%CI 9.30–18.5) compared to 1.6% (95%CI 0.00–8.66), in female samples (p = 0.005, Fisher’s exact test). M. penetrans DNA concentrations ranged from 2 to 31,846 genome equivalents (GEQ)/μl with a median of 33 GEQ/μl.
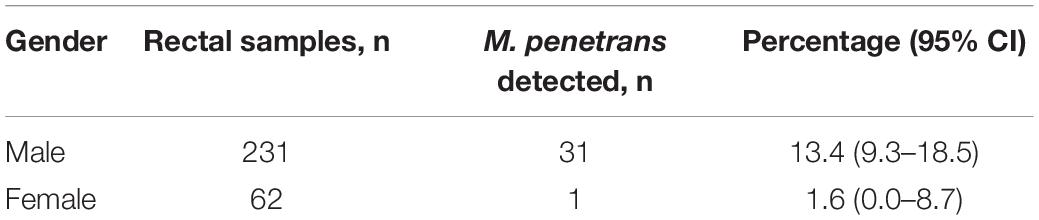
Table 1. Distribution of M. penetrans among C. trachomatis positive rectal samples.
In this report, we describe a high prevalence of M. penetrans in male C. trachomatis positive rectal samples, in accordance to previous results (Taylor-Robinson et al., 2003). Earlier studies have mainly aimed to detect M. penetrans in male populations, including healthy MSM and men who have sex with women (MSW). In the 1990’s, shortly after the discovery of M. penetrans, several publications highlighted its potential role in the progression of HIV infection to AIDS and for development of Kaposi’s sarcoma by analyzing M. penetrans antibodies in serum samples from healthy controls and patients of different risk groups for AIDS (Wang et al., 1992, 1993). In our study, lack of clinical information prevented us to evaluate the association between M. penetrans and HIV positivity.
Two studies have detected M. penetrans by PCR with a prevalence of 1.4 and 1.6%, respectively, in urine samples from HIV-infected individuals (Wang et al., 2012; Chen et al., 2015). One of these studies also included sexually transmitted clinic attendees and healthy controls, where the M. penetrans infection rate was < 1% (Wang et al., 2012). An earlier study of urethral swabs from Japanese men with and without NGU failed to detect M. penetrans in any of the patients (Deguchi et al., 1996). M. penetrans has been detected in rectal samples from 28 MSM with or without NGU with 10 vs. 5.6% positives, respectively. In addition, the study found a 10% prevalence of M. penetrans in urethral and throat samples in the men with NGU (Taylor-Robinson et al., 2003). Recent evidence has suggested a role of M. penetrans in NGU, a syndrome with unknown etiology in > 50% of cases. In search of an etiology for idiopathic NGU, Srinivasan et al. found an association between detection of M. penetrans and NGU by 16S microbiota analysis. They confirmed the findings using qPCR in urine samples from 431 men with and without NGU. M. penetrans was found in 8% of men diagnosed with NGU compared to 1% in men without NGU (Srinivasan et al., 2021). However, the association was found only in MSM where 13% of the NGU cases were M. penetrans positive compared to 3% of MSW with NGU. The present study revealed a 13% prevalence of M. penetrans in male C. trachomatis positive rectal samples. Due to the anonymization, we are not able to determine the proportion of MSM in our population, but it is probably nearly 100%, as rectal swabs are rarely obtained from MSW. Among MSM, bacterial STIs are common in the rectal site, and some studies have found a much higher positive rate in rectal swabs as compared to urine (Munson et al., 2021).
Due to the absence of cell wall, Mycoplasma spp. are naturally resistant to a wide spectrum of antibiotics. The most frequently used treatment of infection are macrolides, tetracyclines and fluoroquinolones, however, in the urogenital pathogen M. genitalium, several mutations associated with macrolide and fluoroquinolone resistance have been identified (Machalek et al., 2020). Only few isolates of M. penetrans are available and the literature is sparse on its antimicrobial susceptibility, however, early studies suggested that most isolates of M. penetrans were susceptible to all three antimicrobial classes (Hayes et al., 1995). In a more recent study, one M. penetrans strain showed evidence of macrolide resistance (Duffy et al., 2000). Similarly, a recent communication found complete resistance to azithromycin on four urogenital isolates from immunocompetent men suffering idiopathic NGU (Schwab et al., 2021). This development suggests that macrolide resistance in M. penetrans may be increasing over time, just as it has been shown for M. genitalium (Machalek et al., 2020). Altogether, these results emphasize the need for collection of contemporary M. penetrans isolates with antimicrobial susceptibility testing and molecular studies to determine the basis for the resistance in this emerging etiologic agent of NGU.
There are several limitations to our study. Due to the anonymized nature of the samples, important clinical, demographic and behavioral data are missing. Furthermore, it was not possible to evaluate whether multiple samples from the same subject were included, which could affect numbers. The high prevalence of M. penetrans in male rectal swabs supports the findings from previous studies of a strong link between MSM behavioral factors and M. penetrans detection. Future research should evaluate the role of M. penetrans as a pathogen potentially implicated in different STIs but should emphasize differences in sexual behavior.
The prevalence of M. penetrans in C. trachomatis positive male rectal swabs was surprisingly high at 13%. Although clinical data were missing because of anonymization, the presence of M. penetrans appears to be strongly associated with MSM behavior as suggested also in previous studies. Our findings indicate that M. penetrans may cause coinfection with C. trachomatis, however, the implications for symptoms and treatment outcomes require further research.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Ethical review and approval was not required for the study on human participants in accordance with the Local Legislation and Institutional Requirements. Written informed consent for participation was not required for this study in accordance with the National Legislation and the Institutional Requirements.
IP-P performed the experimental assays and wrote the manuscript. AS-H participated in writing phase and statistical analysis, elaborated the table, and reviewed the initial manuscript draft for important intellectual content. JSJ conceptualized and designed the study, supervised the manuscript, and reviewed the manuscript for important intellectual content. All authors contributed to the article and approved the submitted version.
This work was supported by the Spanish Ministry of Science, Innovation and Universities (FPU19/05561) and the European Society of Human Reproduction and Embryology Traveling Fellowship to IP-P.
JSJ reports grants, personal fees, and non-financial support from Hologic, personal fees from Roche, grants and personal fees from SpeeDx, grants and personal fees from Nabriva, grants and personal fees from Cepheid, grants and personal fees from Abbott, and grants and personal fees from GSK all outside the submitted work.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
This study was part of a Ph.D. thesis conducted at the Biomedicine Doctoral Studies of the University of Granada, Spain.
Chen, L. S., Wu, J. R., Wang, B., Yang, T., Yuan, R., Zhao, Y. Y., et al. (2015). Epidemiology of Mycoplasma acquisition in male HIV-1 infected patients: a multistage cross-sectional survey in Jiangsu, China. Epidemiol. Infect. 143, 3327–3334. doi: 10.1017/S0950268815000461
De Vries, H. J. C., De Barbeyrac, B., De Vrieze, N. H. N., Viset, J. D., White, J. A., Vall-Mayans, M., et al. (2019). 2019 European guideline on the management of lymphogranuloma venereum. J. Eur. Acad. Dermatol. Venereol. 33, 1821–1828. doi: 10.1111/jdv.15729
Deguchi, T., Gilroy, C. B., and Taylor-Robinson, D. (1996). Failure to detect Mycoplasma fermentans, Mycoplasma penetrans, or Mycoplasma pirum in the urethra of patients with acute nongonococcal urethritis. Eur. J. Clin. Microbiol. Infect. Dis. 15, 169–171. doi: 10.1007/BF01591493
Duffy, L. B., Crabb, D., Searcey, K., and Kempf, M. C. (2000). Comparative potency of gemifloxacin, new quinolones, macrolides, tetracycline and clindamycin against Mycoplasma spp. J. Antimicrob. Chemother. 45 (Suppl 1), 29–33. doi: 10.1093/jac/45.suppl_3.29
Hayes, M. M., Foo, H. H., Timenetsky, J., and Lo, S. C. (1995). In vitro antibiotic susceptibility testing of clinical isolates of Mycoplasma penetrans from patients with AIDS. Antimicrob. Agents Chemother. 39, 1386–1387.
Jensen, J. S., Borre, M. B., and Dohn, B. (2003). Detection of Mycoplasma genitalium by PCR amplification of the 16S rRNA gene. J. Clin. Microbiol. 41, 261–266. doi: 10.1128/JCM.41.1.261-266.2003
Jensen, J. S., Orsum, R., Dohn, B., Uldum, S., Worm, A. M., and Lind, K. (1993). Mycoplasma genitalium: a cause of male urethritis? Genitourin Med. 69, 265–269. doi: 10.1136/sti.69.4.265
Machalek, D. A., Tao, Y., Shilling, H., Jensen, J. S., Unemo, M., Murray, G., et al. (2020). Prevalence of mutations associated with resistance to macrolides and fluoroquinolones in Mycoplasma genitalium: a systematic review and meta-analysis. Lancet Infect. Dis. 20, 1302–1314. doi: 10.1016/S1473-3099(20)30154-7
Munson, E., Morgan, E., Sienkiewicz, L., Thomas, Y., Buehler, K., Ryan, D., et al. (2021). Molecular screening in a longitudinal cohort of young men who have sex with men and young transgender women: associations with focus on the emerging sexually transmitted pathogen Mycoplasma genitalium. Sex Transm. Infect. 97, 434–440. doi: 10.1136/sextrans-2020-054463
Schwab, N., Toh, E., Nzenwata, D., Mikulin, J., Timothy, W., Nelson, D., et al. (2021). “Characterization of Mycoplasma penetrans isolates acting as possible etiologic agents of idiopathic urethritis in immunocompetent men,” in Proceeding of the XXIII Biennial Congress of the International Organization for Mycoplasmology (IOM) (Tel Aviv), 81–82.
Srinivasan, S., Chambers, L. C., Tapia, K. A., Hoffman, N. G., Munch, M. M., Morgan, J. L., et al. (2021). Urethral microbiota in men: association of Haemophilus influenzae and Mycoplasma penetrans With Nongonococcal Urethritis. Clin Infect Dis 73, e1684–e1693. doi: 10.1093/cid/ciaa1123
Stoner, B. P., and Cohen, S. E. (2015). Lymphogranuloma venereum 2015: clinical presentation, diagnosis, and treatment. Clin. Infect. Dis. 61 (Suppl 8), S865–S873. doi: 10.1093/cid/civ756
Taylor-Robinson, D., Gilroy, C. B., and Keane, F. E. (2003). Detection of several Mycoplasma species at various anatomical sites of homosexual men. Eur. J. Clin. Microbiol. Infect. Dis. 22, 291–293. doi: 10.1007/s10096-003-0910-x
Wang, B., Wu, J. R., Guo, H. J., Yang, H. T., Ai, J., Hui, M., et al. (2012). The prevalence of six species of Mycoplasmataceae in an HIV/AIDS population in Jiangsu Province, China. Int. J. STD AIDS 23, e7–e10. doi: 10.1258/ijsa.2009.009396
Wang, R. Y., Shih, J. W., Grandinetti, T., Pierce, P. F., Hayes, M. M., Wear, D. J., et al. (1992). High frequency of antibodies to Mycoplasma penetrans in HIV-infected patients. Lancet 340, 1312–1316.
Wang, R. Y., Shih, J. W., Weiss, S. H., Grandinetti, T., Pierce, P. F., Lange, M., et al. (1993). Mycoplasma penetrans infection in male homosexuals with AIDS: high seroprevalence and association with Kaposi’s sarcoma. Clin. Infect. Dis. 17, 724–729. doi: 10.1093/clinids/17.4.724
Workowski, K. A., Bachmann, L. H., Chan, P. A., Johnston, C. M., Muzny, C. A., Park, I., et al. (2021). Sexually transmitted infections treatment guidelines, 2021. MMWR Recomm. Rep. 70, 1–187.
Keywords: Mycoplasma penetrans, Chlamydia trachomatis, coinfection, sexually transmitted infections, rectum
Citation: Pérez-Prieto I, Skafte-Holm A and Jensen JS (2022) High Prevalence of Mycoplasma penetrans in Chlamydia trachomatis Positive Rectal Samples From Men: A Brief Report. Front. Microbiol. 13:914874. doi: 10.3389/fmicb.2022.914874
Received: 16 March 2022; Accepted: 23 May 2022;
Published: 13 June 2022.
Edited by:
Meghan May, University of New England, United StatesReviewed by:
Ellen Kersh, Centers for Disease Control and Prevention (CDC), United StatesCopyright © 2022 Pérez-Prieto, Skafte-Holm and Jensen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jørgen Skov Jensen, anNqQHNzaS5kaw==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.