
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Microbiol., 20 June 2022
Sec. Infectious Agents and Disease
Volume 13 - 2022 | https://doi.org/10.3389/fmicb.2022.895989
This article is part of the Research TopicInsights in Infectious Agents and Disease: 2021View all 37 articles
 Jaime David Acosta-España1,2,3,4†
Jaime David Acosta-España1,2,3,4† Kerstin Voigt1,2*†
Kerstin Voigt1,2*†Mucormycosis is a fungal disease caused by members of the fungal order Mucorales, which are abundantly found in terrestrial environments. The fungi propagate clonally via mitospores, which are transmitted to humans through the air and cause superficial or invasive infections. The disease has emerged in recent years and coincides generally with immunosuppression on the patient side. Mucormycosis is still rarely recognized in the clinical because of its unspecific symptoms which often triggers misdiagnosis with bacterial or viral infections leading to prolonged therapeutic cycles and loss of valuable time to manage mucormycosis properly. Infected patients develop various clinical forms, most notably ranging from rhinocerebral via pulmonary to gastrointestinal forms. Traditional diagnosis is based on culture and histopathologic examinations of the affected tissue. But, the achievement of a precise result is time-consuming, labor-intensive, requires mycological expertise and the finding appears often too late. A rapid and precise diagnosis is mandatory because symptoms are non-specific and the disease is rapidly progressing with often fatal outcome. Mucormycosis was increasingly associated with other infections and underlying conditions and risk factors causing comorbidities, which are difficult to successfully manage. This mini-review summarizes the current knowledge on the epidemiology and causative agents of mucormycosis, transmission, risk factors, clinical presentation, diagnosis, and highlights the lack of appropriate biomarkers on the pathogen and the host sides for rapid pathogen and host susceptibility detection, respectively. Fungal antigens and single nucleotide polymorphisms (SNPs) in human host genes are useful for the assessment of susceptibility. This mini-review addresses possibilities for early prediction of susceptibility to mucormycosis based on forecasting of the risk of infection with fungal pathogens other than Mucorales. The topic of early prediction and diagnosis of mucormycosis represents a current research gap and highlights the importance of potential future developments in the area of risk assessment, susceptibility prognosis in conjunction with early diagnosis to reduce mortality in patients suffering from mucormycosis.
– Summary of the biomarkers currently available for the diagnosis of mucormycosis.
– Overview of predisposing factors and comorbidities from a medical point of view.
– Encourage the exploration of novel biomarkers for pathogen and host susceptibility detection.
Mucormycosis (formerly: zygomycosis) is a group of diseases affecting various anatomical sites. The infections are caused by filamentous fungi of the order Mucorales, a dominant group among zygosporic fungi which were formerly summarized as zygomycetes. The fungi are ubiquitous and predominate in the decomposition of organic matter. Among the clinically important genera (1) Rhizopus, (2) Lichtheimia, (3) Mucor, (4) Rhizomucor, (5) Thermomucor, (6) Syncephalastrum, (7) Cunninghamella, (8) Cokeromyces, (9) Apophysomyces and (10) Saksenaea, we can predominantly observe the following species: (1) Rhizopus arrhizus (formerly: R. oryzae) and R. microsporus, (2) Lichtheimia corymbifera (formerly: Absidia corymbifera), L. ornata, L. ramosa, (3) Mucor circinelloides, M. lusitanicus, M. ramosissimus, M. racemosus, M. hiemalis, (4) Rhizomucor miehei and Rh. pusillus, (5) Thermomucor indicae-seudaticae, (6) Syncephalastrum monosporum and S. racemosum, (7) Cunninghamella elegans (formerly: C. bertholletiae), (8) Cokeromyces recurvatus, (9) Apophysomyces elegans and A. variabilis, and (10) Saksenaea vasiformis (Ribes et al., 2000; Roden et al., 2005; Spellberg et al., 2005; Petrikkos et al., 2012; Hassan and Voigt, 2019; de et al., 2020; Index Fungorum, 2022).
Although inhalation of spores is the most common route of transmission, the disease can also be acquired cutaneously and gastrointestinally (Figure 1). This life-threatening disease primarily affects immunosuppressed, diabetic and all types of immunocompromised patients, which suffer from a primary bacterial or fungal infection (Choi et al., 2019). Most actually, mucormycosis associated with Coronavirus disease 2019 (COVID-19) became a new threat due to high-dose corticosteroid therapy during the SARS-CoV-2 pandemic [as reviewed by Hoenigl et al. (2022)]. Diagnosis in patients with mucormycosis is complicated and delayed. Treatment is based on surgical debridement of the affected areas and antifungal therapy, which has low penetrance, explained by the large areas of necrosis that these infected patients develop in association with angioinvasion (Farmakiotis and Kontoyiannis, 2016; Patel et al., 2020; Pal et al., 2021).
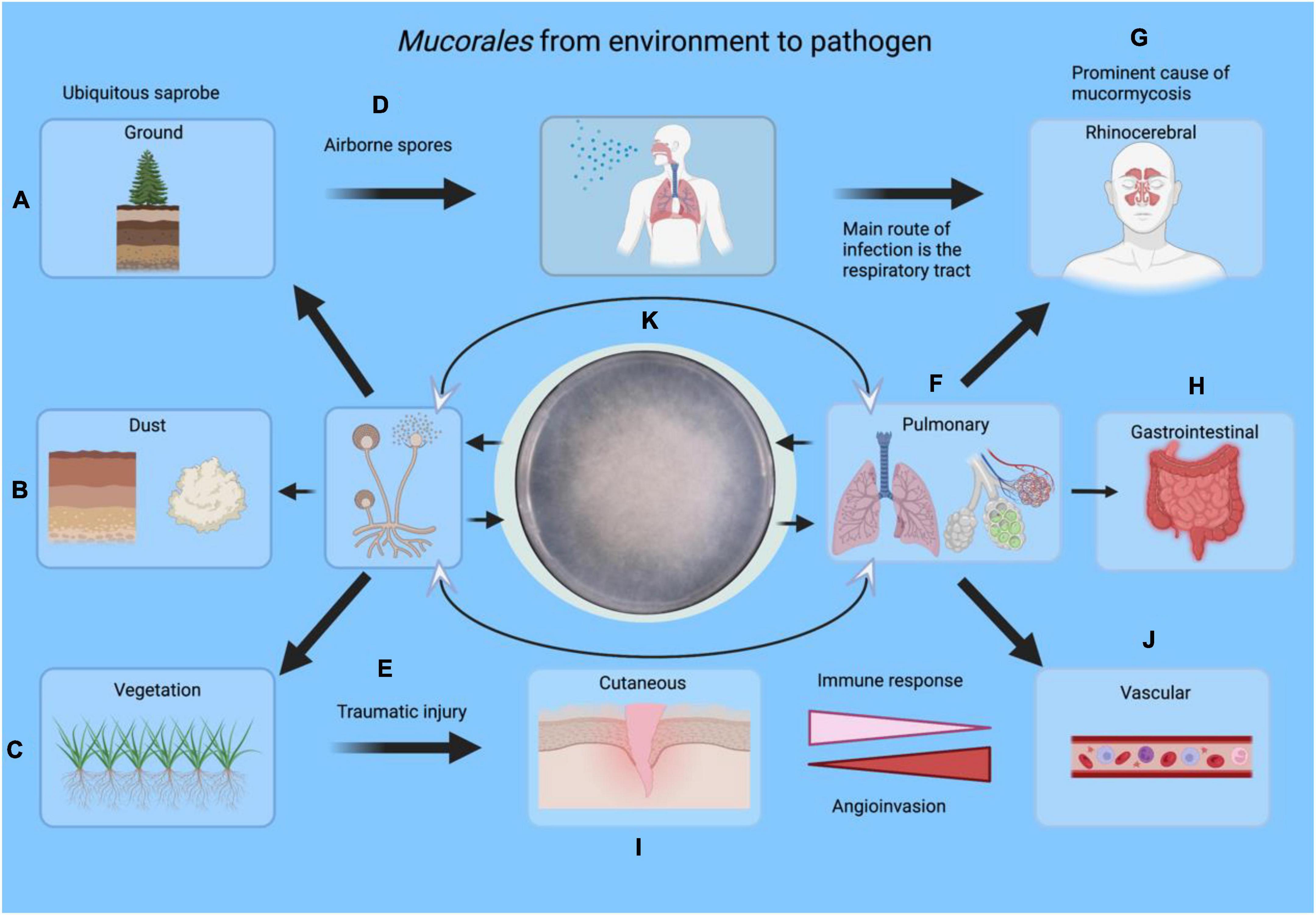
Figure 1. An overview of infection routes of Mucorales from the environment toward the development as pathogens. Mucorales can be found in soil (A), dust (B), and vegetation (C). The spores can infect humans through the respiratory tract via airborne spores (D), injuries (E), pulmonary (F) rhinocerebral (G) or the gastrointestinal tract (H). Cutaneous cases, on the other hand, are associated with vegetal trauma or motor vehicle accidents (I). Any of these local infections can cause vascular spread leading to thrombosis (J). Specimens (F–I) can be obtained for laboratory diagnosis by culture (K) or other methods. Eventually, the fungus returns to the environment where it belongs. This figure was created in BioRender.com.
This mini-review will outline the various fields of research targeting risk assessment, prediction, and prognosis based on human-derived biomarkers and their variants.
In patients with mucormycosis, cellular immunity has been shown to be critical in combating these filamentous fungi. Therefore, comorbidities or diseases that compromise immunity and surface barrier integrity count as risk factors for acquiring the infection. The study by Jeong et al. (2019) showed that the following comorbidities were associated with a higher percentage of mucormycosis: diabetes mellitus, hematologic malignancy, diabetic ketoacidosis, acute myeloid and lymphoblastic leukemia, lymphoma, hematopoietic stem cell transplantation, and others (Ghuman and Voelz, 2017).
On the other hand, in patients without comorbidities, the main risk factors were shown in the population that used voriconazole, suffered injection sites, had a car accident, used corticosteroids, used fluconazole, had neutropenia, among others (Jeong et al., 2019). Increased mortality was observed in patients with diabetes mellitus and immunocompromised states in a follow-up 180 days after their diagnosis (Hong et al., 2013).
COVID-19 patients suffering from mucormycosis have raised the alarm worldwide, with a focus on India. Indeed, it is important to note that India already had a 70-fold higher risk of mucormycosis compared with developed countries. Despite this, an Indian multicenter epidemiologic study reported a two-fold increase in mucormycosis cases in 2019 compared with 2020 (Banerjee et al., 2021; Mathew et al., 2021; Pal et al., 2021; Rocha et al., 2021). The risk factors for COVID-19 associated mucormycosis (CAM) highlighted in the aforementioned studies are: cytokine storm (interleukin 6), islet damage, elevated ferritin, and endotheliitis. It is important to note that it is likely that the sum of cytokine storm, ketoacidosis, and uncontrolled corticosteroid use increases the risk of hyperglycemia and impaired phagocytosis, leaving patients susceptible to CAM (Mathew et al., 2021; Pal et al., 2021). These and other hypotheses are being studied to understand the increase in cases of mucormycosis in patients infected by SARS-CoV-2. A comparison between the risk factors in 3 studies in the general population and in a study in patients with COVID-19 is shown in Table 1.
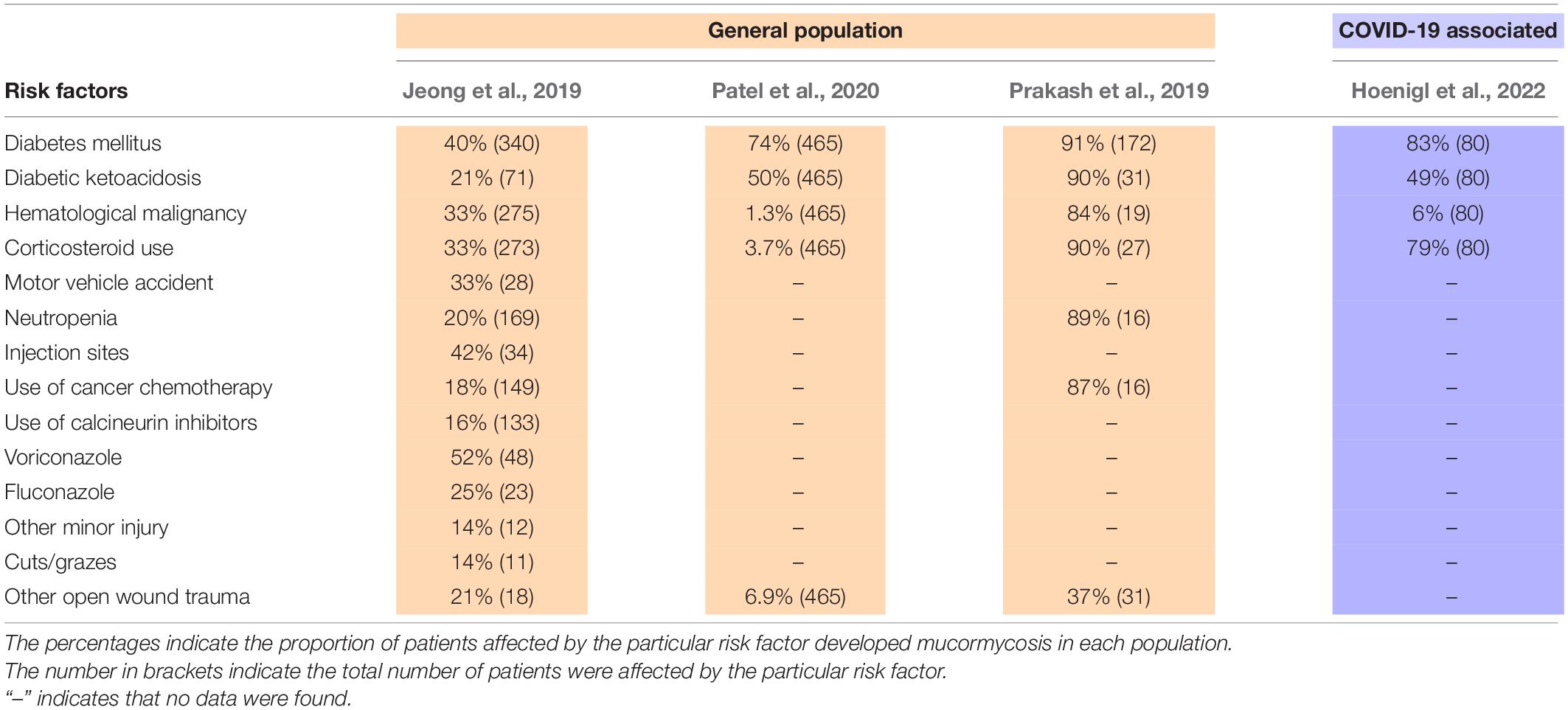
Table 1. Comparison of underlying conditions and predisposing factors for the development of mucormycosis.
Regarding its anatomical localization, mucormycosis is divided into six forms: (1) rhinocerebral, (2) pulmonary, (3) cutaneous, (4) gastrointestinal, (5) disseminated, and (6) uncommon forms. The appearance and clinical manifestations vary according to this classification and are described below (Jeong et al., 2019).
The patients in whom the rhinocerebral variant occurs are usually diabetics and/or patients with ketoacidosis. This variant is characterized by unilateral involvement accompanied by facial pain, retro-orbital headache, fever, hyposmia, numbness, and nasal congestion. Within a few days, this condition develops into a black discharge. Later, invasion of orbital nerves and vessels may be observed, including diplopia and loss of vision, nasal cavity, palate, and face with black eschar, among others. The neurological presentation may include brain involvement and loss of consciousness, which unfortunately means a poor prognosis (Szalai et al., 2006).
This pulmonary presentation is common in patients with hematologic malignancies and a history of neutropenia. Concurrent sinusitis and pulmonary disease may be expected. Pulmonary infection presents with non-specific symptoms of cough, fever, dyspnea, and hemoptysis in patients with necrosis. Auscultation reveals rales and a decreased vesicular murmur. The infection may even be so aggressive that it exceeds the values for mortality compared with other infectious agents. Cellulitis of the affected chest wall may occur in these patients (Peng et al., 2019).
Skin diseases are often associated with trauma and loss of the skin barrier. Cases have even been reported in association with biomedical devices such as catheters, insulin use, etc. Initially, it manifests as cellulitis that progresses to necrosis of the affected tissue with the formation of a black scab. This necrosis, as in other manifestations, is the expression of vascular invasion that clogs blood vessels and leads to tissue damage (Rrapi et al., 2021).
Gastrointestinal infections occur in the severely malnourished patients undergoing organ transplantation. They usually involve mainly the stomach, ileum, colon, and liver. The clinical manifestations are non-specific, characterized by abdominal pain, nausea, vomiting, abdominal distension, and may even present with hematochezia or obstruction. In case of rupture of intestinal integrity, patients present symptoms of peritonitis (Spellberg, 2012; Wotiye et al., 2020).
To a lesser extent, disseminated forms of the disease may also occur, affecting the kidneys, heart, and other organs. The symptoms are related to the site of infection (Devana et al., 2016; Krishnappa et al., 2019).
Clinical criteria, risk factors, histopathologic findings, cultures, and imaging studies should be considered in the diagnosis of mucormycosis, especially in health centers treating patients with COVID-19. For direct microscopic, cultural, and histopathologic analysis, it is advisable to obtain a sample of the affected tissue, preferably by biopsy, although fine-needle aspiration is also possible. Histopathological examination of tissue infected with Mucorales shows damage to the tissue and invasion of the blood vessels, accompanied by the presence of hyphae with the following characteristics:
• Broad, pauciseptate hyphae.
• Coenocytic to irregular branching of hyphae.
• Large branching angle, approximately rectangular.
Fungal culture has a variable sensitivity for diagnosis, it is advisable to send a biopsy fragment of the infected tissue. Unfortunately, the yield of mucormycosis pathogens is low, and these microorganisms may also have slow growth. Another disadvantage of biopsy is that more invasive endoscopic procedures may be required to obtain tissue, especially for infections of the lung and gastrointestinal tract, to name a few.
Complementary laboratory tests may be useful and may reveal neutropenia in the white blood count, low blood pH in diabetic ketoacidosis, and positive urinary ketone levels in diabetic ketoacidosis. Imaging studies can aid in diagnosis, although it should be noted that computed tomography (CT) of the sinuses is less sensitive than magnetic resonance imaging (MRI) for detecting soft tissue invasion. CT thoracic examination with intravenous contrast is a sensitive test for detecting abnormalities in pulmonary mucormycosis, and CT of the brain may not be able to distinguish between abscesses and early infarcts (Gamba et al., 1986; McAdams et al., 1997; Kontoyiannis and Lewis, 2006; Turunc et al., 2008).
Laboratory and imaging studies are helpful, but they are not foolproof, as other pathologies may yield similar results. Early diagnosis is critical for treatment and improving prognosis. Biomarkers have been poorly studied and lack clinically approved options. Therefore, early diagnosis and monitoring of mucormycosis by detection of circulating DNA in serum is mandatory to manage the disease. A cohort study of a total 44 patients described the detection of circulating DNA in one patient with mucormycosis, which demonstrated the diagnostic utility and the accurate quantification of the fungal DNA load enabling therapeutic monitoring (Millon et al., 2016).
In 2014, a study was published on serial monitoring of mucoralean DNA load in serum samples from a patient with disseminated mucormycosis. The qPCR assay was used to detect circulating DNA of Mucor/Rhizopus, Lichtheimia, or Rhizomucor, which showed very high variability and was detectable from day 9 of infection, with elevation peaks at days 15 and 38 (Shigemura et al., 2014). These results contrast with the case report of detection of the circulating fungal DNA by polymerase chain reaction in a fatal case of infection with Cunninghamella elegans (synonym: C. bertholletiae), in which detection of Cunninghamella bertholletiae DNA in serum was highest on day 1 at 18.0 copies/ml and on day 4 (101.0 copies/ml) (Hiramoto et al., 2020).
Especially in the context COVID-19 of evaluating hospital trends in mucormycosis and other fungal infections, this may become essential today. An evaluation of trends for all fungal infections should be considered which uses denominator data to calculate incidence and seasonality. It is recommended that hospitals review 12- to 24-month back microbiologic cultures and histopathologic specimens with evidence of tissue invasion by fungal hyphae to obtain an epidemiologic curve and associated hospital services or areas. If mucormycosis outbreaks are suspected, the environment should also be reviewed through a general inspection for mold, leaks, dirty HVAC systems, cleaning of the environment, construction and maintenance areas, indoor air temperature, and humidity records, including any days when humidity exceeded 60%, dates of air filter changes, etc (Hartnett et al., 2019).
Invasive fungal disease is a challenge for medicine, and a rapid diagnosis can prevent tissue damage and complications and reduce mortality. Currently available biomarkers for rapid detection of fungal infections include carbohydrates derived from the cell wall of fungi, such as galactomannan (Aspergillus, Penicillium, Paracoccidioides, Histoplasma, Fonsecaea, and Cryptococcus). (1→3)-β-D-glucan (Aspergillus spp., Candida spp., Fusarium spp., Trichosporon spp., Saccharomyces cerevisiae, Acremonium spp., Coccidioides immitis, Histoplasma capsulatum, Sporothrix schenckii, and Pneumocystis jirovecii). Candida mannan (C. albicans, C. glabrata, and C. tropicalis) (Huppler et al., 2017).
It is important to remember that the galactomannan levels are low in mucormycosis because Mucorales do not expose gluconic cell wall sugars on the surface of their hyphae (Pickering et al., 2005). It has been used with an approach to aspergillosis that showed sensitivity between 60 and 80% in hematologically neutropenic patients (Pfeiffer et al., 2006; Lamoth, 2016). Detection of dihexasaccharide in serum (MS-DS) was associated with mucormycosis in 9 of 10 patients using matrix-assisted laser desorption/ionization time-of-flight mass spectrometry (MALDI-TOF) (Mercier et al., 2018).
In vitro studies of specific T cells in Mucorales-infected patients could be detected only in patients with invasive mucormycosis which represented elevated production of IL-4, IFN-γ, IL-10, and to a lesser extent IL-17 and belonged to CD4+ subsets or CD8+. Nevertheless, CD8 + Mucorales-specific T cells can produce either IL-4 or IL-10, predominantly in the late phase of infection. These studies should be recruited in a larger population to demonstrate their clinical utility in diagnosing patients, especially in early forms of the disease (Potenza et al., 2011).
The presence of the cell wall carbohydrate fucomannan has been studied as a biomarker in invasive mucormycosis in mice (Orne et al., 2018). During infection, this biomarker is secreted in blood, urine, serum, and bronchoalveolar lavage fluid (BALF). A lateral flow assay (LFA) for the detection of fucomannan was developed (mAb 2DA6). BALF, serum, and urine were collected 3–4 days after intratracheal infection of immunosuppressed or DKA mice with spores of various Mucorales, including Rhizopus arrhizus (synonym: R. delemar and R. oryzae), L. corymbifera, M. circinelloides and C. elegans (synonym: C bertholletiae). Samples collected 3 and 4 days post-infection were positive, demonstrating the ability of LFA to provide early positive results. The highest reactivity was observed in urine samples (Orne et al., 2018).
Another recently described possibility is the detection of Rhizopus-specific antigen (RSA). For this purpose, a sandwich enzyme-linked immunosorbent assay (ELISA) was developed to detect RSA levels in the serum of vaccinated mice. This proved to be of interest as RSA levels were higher in mice with mucormycosis (15.1 ng/ml) than in mice with aspergillosis (0.53 ng/ml), the latter having levels close to the negative control (0.49 ng/ml) (Shibata et al., 2020).
Homologs of the spore-coat protein CotH are widespread in Mucorales and absent in non-invasive species (Gebremariam et al., 2014). Thus, CotH is a promising target for the early diagnosis of mucormycosis (Baldin et al., 2018). However, a Mucorales-specific marker may neglect concomitant fungal opportunists, as is the case with pioneering invasive mucormycosis, which usually follows invasive aspergillosis. Patients with aspergilloma and invasive aspergillosis develop an antibody response to Aspergillus fumigatus mannoprotein 1 (AFMP1), suggesting that the protein is a target for host humoral immunity (Yuen et al., 2001). Indeed, clinical evaluation revealed that an enzyme-linked immunosorbent assay-based antibody (ELISA) test using the AFMP1 was 100% sensitive for patients with aspergilloma and 33.3% sensitive for patients with invasive aspergillosis (Chan et al., 2002).
For this reason, it is important to analyze surface proteins and even polysaccharides that can be examined in clinical specimens for early detection of infectious Mucorales.
The endothelial cell receptor GRP78 is required for the pathogenesis of mucormycosis in diabetic mice (Liu et al., 2010). Another target could be Pentraxin 3 (PTX3), which has been shown to be a promising marker for aspergillosis (Cunha et al., 2014). Mucormycosis frequently co-occurs with aspergillosis (Alfano et al., 2006; Tsikala-Vafea et al., 2020; Johnson et al., 2021; Zayet et al., 2021). SNPs in PRRs like Toll-like receptors (TLRs) have already been associated with increased susceptibility to fungal infections (Bergantim et al., 2013; Wang et al., 2013; Fischer et al., 2016; Zhang et al., 2019; Aqsa et al., 2020). The TLR2 SNP rs5743708 (R753Q, GA/AA genotype, n = 12) is associated with a higher risk of pneumonia and invasive fungal infections in patients with acute myeloid leukemia undergoing chemotherapy (Fischer et al., 2016). TLR with SNP’s have previously been associated with increased susceptibility to fungal infections (Wang et al., 2013; Fischer et al., 2016). TLR2 SNP rs5743708 (R753Q, GA/AA genotype, n = 12) is associated with a higher risk of pneumonia and invasive fungal infections in patients with acute myeloid leukemia receiving chemotherapy (Fischer et al., 2016).
No studies were found analyzing genetic variations that increase host risk for developing mucormycosis. The discovery of these markers in other diseases such as invasive aspergillosis leads us to hypothesize that this may also be the case in these patients, especially since there may be individual susceptibility, as not all patients with diabetic ketoacidosis or hematologic malignancies are infected (Naik et al., 2021).
Mucormycosis is a rare disease with a high-mortality potential. Several risk factors for the acquisition of mucoralean infections have been described, including a decrease in cellular immunity and disruption of anatomic barriers. Among the most important are diabetic patients, especially with ketoacidosis, malignancies, trauma, neutropenia, use of voriconazole, fluconazole, and corticosteroids. It is important to discuss the differences in prevalence in different regions, which are likely due to population numbers, environmental conditions, control and prevalence of comorbidities such as diabetes, immunity in oncologic diseases, and even underdiagnosis of patients with mucormycosis in each country, among other factors and underlying comorbidities.
In 2020 and 2021, superinfection by mucormycosis raised alarm in patients with COVID-19, although this association is still under investigation, with a significant prevalence in India that is multifactorial. Cytokine storm (IL-6), islet cell damage, elevated ferritin, and corticosteroid use in mainly patients with diabetes patients have led to a doubling of mucormycosis cases in India compared to 2019 and 2020. There are several clinical presentations in these patients, and the rhinocerebral form clearly predominates, although almost any organ can be affected in patients with risk factors. Diagnosis is complex, and late effects, risk factors, clinical presentation, histologic criteria, culture, molecular evidence, imaging, and laboratory testing must be considered. Currently, isolation of the fungus in an axenic culture and detection of fungal structures in histopathology are used to confirm infection. However, it is important to keep in mind that not all hospitals have staff trained in mycological diagnosis and do not have a budget for molecular detection of associated microorganisms, especially in low-resource countries, so biomarkers may be a more viable option for rapid diagnosis.
In patients infected with Mucorales, time is a valuable commodity to reduce mortality. Therefore, SNPs could be of great help in determining which patients are more susceptible to mucormycosis due to mutations in TLRs. Another option could be the detection of early-emerging antigens, such as CotH or Fucomannan. Both detection of SNPs in TLRs and detection of antigens that could be a predictive factor and/or early diagnosis, especially in patients with hematologic and oncologic diseases, diabetics with ketoacidosis, and other high-risk groups. However, these possibilities should be explored in the future. Finally, epidemiologic surveillance and investigation of suspected outbreaks of mucormycosis in health care settings have again become very important, especially because of the increase in COVID-19 associated mucormycosis.
JA-E and KV drafted and revised the manuscript. Both authors contributed to the article and approved the submitted version.
This work was supported by the Deutsche Forschungsgemeinsc haft (DFG) CRC/Transregio 124 Pathogenic fungi and their human host: networks of interaction (FungiNet) project number 210879364 [subproject A6 (to KV)], the Leibniz Institute for Natural Product Research and Infection Biology, Jena – Hans Knöll Institute, and Friedrich Schiller University Jena.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We thank the Jena School for Microbial Communication (JSMC) for generous administrative advice.
Alfano, C., Chiummariello, S., Dessy, L., Bistoni, G., and Scuderi, N. (2006). Combined Mucormycosis and Aspergillosis of the Rhinocerebral Region. In Vivo 20, 311–316.
Aqsa, A., Droubi, S., and Glaser, A. (2020). Aspergillus and Rhizopus Fungal Coinfection in a Patient With Multiple Myeloma. Cureus 12:e8050. doi: 10.7759/CUREUS.8050
Baldin, C., Soliman, S. S. M., Jeon, H. H., Alkhazraji, S., Gebremariam, T., Gu, Y., et al. (2018). PCR-Based Approach Targeting Mucorales-Specific Gene Family for Diagnosis of Mucormycosis.. J. Clin. Microbiol. 56, e746–e718. doi: 10.1128/JCM.00746-18
Banerjee, M., Pal, R., and Bhadada, S. K. (2021). Intercepting the deadly trinity of mucormycosis, diabetes and COVID-19 in India. Postgrad. Med. J. 2021:140537. doi: 10.1136/POSTGRADMEDJ-2021-140537
Bergantim, R., Rios, E., Trigo, F., and Guimarães, J. E. (2013). Invasive coinfection with Aspergillus and Mucor in a patient with acute myeloid leukemia. Clin. Drug Investig. 33, S51–S55. doi: 10.1007/S40261-012-0022-4
Chan, C.-M., Woo, P. C. Y., Leung, A. S. P., Lau, S. K. P., Che, X.-Y., Cao, L., et al. (2002). Detection of Antibodies Specific to an Antigenic Cell Wall Galactomannoprotein for Serodiagnosis of Aspergillus fumigatus Aspergillosis. J. Clin. Microbiol. 40, 2041–2045. doi: 10.1128/JCM.40.6.2041-2045.2002
Choi, S., Master, Son, H.-J., Master, Jung, J., Kim, M., et al. (2019). 1703. Bacterial or Fungal Co-Infection in Patients with Mucormycosis. Open Forum Infect. Dis. 6, S623–S624. doi: 10.1093/OFID/OFZ360.1567
Cunha, C., Aversa, F., Lacerda, J. F., Busca, A., Kurzai, O., Grube, M., et al. (2014). Genetic PTX3 Deficiency and Aspergillosis in Stem-Cell Transplantation. N. Engl. J. Med. 370, 421–432. doi: 10.1056/NEJMOA1211161/SUPPL_FILE/NEJMOA1211161_DISCLOSURES.PDF
de, H., Guarro, J., Gené, S. A., Ahmed, A. M. S., Al-Hatmi, M. J., et al. (2020). Atlas of Clinical Fungi Volume 1 Introductions, Lower Fungi, Basidiomycetes, Yeasts, Filamentous Ascomycetes A-B. Available online at: https://webshop.atlasclinicalfungi.org/index.php/component/eshop/atlas-of-clinical-fungi (accessed April 7, 2022).
Devana, S. K., Bora, G. S., Mavuduru, R. S., Panwar, P., Kakkar, N., and Mandal, A. (2016). Successful management of renal mucormycosis with antifungal therapy and drainage. J. Urol. Soc. Ind. 32:154. doi: 10.4103/0970-1591.179192
Farmakiotis, D., and Kontoyiannis, D. P. (2016). Mucormycoses. Infect. Dis. Clin. 30, 143–163. doi: 10.1016/J.IDC.2015.10.011
Fischer, M., Spies-Weisshart, B., Schrenk, K., Gruhn, B., Wittig, S., Glaser, A., et al. (2016). Polymorphisms of Dectin-1 and TLR2 Predispose to Invasive Fungal Disease in Patients with Acute Myeloid Leukemia. PLoS One 11:e0150632. doi: 10.1371/JOURNAL.PONE.0150632
Gamba, J. L., Woodruff, W. W., Djang, W. T., and Yeates, A. E. (1986). Craniofacial mucormycosis: assessment with CT. Radiology 160, 207–212. doi: 10.1148/RADIOLOGY.160.1.3715034
Gebremariam, T., Liu, M., Luo, G., Bruno, V., Phan, Q. T., Waring, A. J., et al. (2014). CotH3 mediates fungal invasion of host cells during mucormycosis. J. Clin. Invest. 124, 237–250. doi: 10.1172/JCI71349
Ghuman, H., and Voelz, K. (2017). Innate and Adaptive Immunity to Mucorales. J. Fungi 3:48. doi: 10.3390/JOF3030048
Hartnett, K. P., Jackson, B. R., Perkins, K. M., Glowicz, J., Kerins, J. L., Black, S. R., et al. (2019). A Guide to Investigating Suspected Outbreaks of Mucormycosis in Healthcare. J. Fungi 5:69. doi: 10.3390/JOF5030069
Hassan, M. I. A., and Voigt, K. (2019). Pathogenicity patterns of mucormycosis: epidemiology, interaction with immune cells and virulence factors. Med. Mycol. 57, S245–S256. doi: 10.1093/MMY/MYZ011
Hiramoto, R., Miyachi, M., Nitta, Y., Yoshida, H., Kuwahara, Y., Tsuchiya, K., et al. (2020). Detection of circulating fungal DNA by polymerase chain reaction in a fatal case of Cunninghamella bertholletiae infection. IDCases 20:e00760. doi: 10.1016/J.IDCR.2020.E00760
Hoenigl, M., Seidel, D., Carvalho, A., Rudramurthy, S. M., Arastehfar, A., Gangneux, J.-P., et al. (2022). The emergence of COVID-19 associated mucormycosis: a review of cases from 18 countries. Lancet Microb. [Epub online ahead of print]. doi: 10.1016/S2666-5247(21)00237-8
Hong, H. L., Lee, Y. M., Kim, T., Lee, J. Y., Chung, Y. S., Kim, M. N., et al. (2013). Risk Factors for Mortality in Patients with Invasive Mucormycosis. Infect. Chem. 45:292. doi: 10.3947/IC.2013.45.3.292
Huppler, A. R., Fisher, B. T., Lehrnbecher, T., Walsh, T. J., and Steinbach, W. J. (2017). Role of Molecular Biomarkers in the Diagnosis of Invasive Fungal Diseases in Children. J. Pediatric. Infect. Dis. Soc. 6, S32–S44. doi: 10.1093/JPIDS/PIX054
Index Fungorum. (2022). Index Fungorum Home Page. Available Online at: http://www.indexfungorum.org/ (Accessed April 21, 2022)
Jeong, W., Keighley, C., Wolfe, R., Lee, W. L., Slavin, M. A., Kong, D. C. M., et al. (2019). The epidemiology and clinical manifestations of mucormycosis: a systematic review and meta-analysis of case reports. Clin. Microbiol. Infect. 25, 26–34. doi: 10.1016/J.CMI.2018.07.011
Johnson, A. K., Ghazarian, Z., Cendrowski, K. D., and Persichino, J. G. (2021). Pulmonary aspergillosis and mucormycosis in a patient with COVID-19. Med. Mycol. Case Rep. 32, 64–67. doi: 10.1016/J.MMCR.2021.03.006
Kontoyiannis, D. P., and Lewis, R. E. (2006). Invasive zygomycosis: update on pathogenesis, clinical manifestations, and management. Infect. Dis. Clin. North Am. 20, 581–607. doi: 10.1016/J.IDC.2006.06.003
Krishnappa, D., Naganur, S., Palanisamy, D., and Kasinadhuni, G. (2019). Cardiac mucormycosis: a case report. Eur. Heart J. Case Rep. 3:ytz130. doi: 10.1093/EHJCR/YTZ130
Lamoth, F. (2016). Galactomannan and 1,3-β-d-Glucan Testing for the Diagnosis of Invasive Aspergillosis. J. Fungi 2:22. doi: 10.3390/JOF2030022
Liu, M., Spellberg, B., Phan, Q. T., Fu, Y., Fu, Y., Lee, A. S., et al. (2010). The endothelial cell receptor GRP78 is required for mucormycosis pathogenesis in diabetic mice. J. Clin. Invest. 120, 1914–1924. doi: 10.1172/JCI42164
Mathew, J., Id, A., Id, A. M., Ibrahim, H., Razack, A., and Mathew, S. T. (2021). COVID-19–associated mucormycosis: evidence-based critical review of an emerging infection burden during the pandemic’s second wave in India. PLoS Neglec. Tropic. Dis. 15:e0009921. doi: 10.1371/JOURNAL.PNTD.0009921
McAdams, H. P., de Christenson, M. R., Strollo, D. C., and Patz, E. F. (1997). Pulmonary mucormycosis: radiologic findings in 32 cases. AJR Am. J. Roentgenol. 168, 1541–1548. doi: 10.2214/AJR.168.6.9168721
Mercier, T., Guldentops, E., van Daele, R., and Maertens, J. (2018). Diagnosing Invasive Mold Infections: what Is Next. Curr. Fungal Infect. Rep. 4, 161–169. doi: 10.1007/S12281-018-0322-0
Millon, L., Herbrecht, R., Grenouillet, F., Morio, F., Alanio, A., Letscher-Bru, V., et al. (2016). Early diagnosis and monitoring of mucormycosis by detection of circulating DNA in serum: retrospective analysis of 44 cases collected through the French Surveillance Network of Invasive Fungal Infections (RESSIF). Clin. Microbiol. Infect. 22, .e1–.e810. doi: 10.1016/J.CMI.2015.12.006
Naik, B., Ahmed, S. M. Q., Laha, S., and Das, S. P. (2021). Genetic Susceptibility to Fungal Infections and Links to Human Ancestry. Front. Genet. 12:1417. doi: 10.3389/FGENE.2021.709315/BIBTEX
Orne, C., Burnham-Marusich, A., Baldin, C., Gebremariam, T., Ibrahim, A., Kvam, A., et al. (2018). Cell Wall Fucomannan is a Biomarker for Diagnosis of Invasive Murine Mucormycosis. 28th European Congress of Clinical Microbiology and Infectious Disease (ECCMID) 1. Available online at: https://www.escmid.org/escmid_publications/escmid_elibrary/material/?mid=62799
Pal, R., Singh, B., Bhadada, S. K., Banerjee, M., Bhogal, R. S., Hage, N., et al. (2021). COVID-19-associated mucormycosis: an updated systematic review of literature. Mycoses 64, 1452–1459. doi: 10.1111/MYC.13338
Patel, A., Kaur, H., Xess, I., Michael, J. S., Savio, J., Rudramurthy, S., et al. (2020). A multicentre observational study on the epidemiology, risk factors, management and outcomes of mucormycosis in India. Clin. Microbiol. Infect. 26, .e9–.e944. doi: 10.1016/j.cmi.2019.11.021
Peng, M., Meng, H., Sun, Y., Xiao, Y., Zhang, H., Lv, K., et al. (2019). Clinical features of pulmonary mucormycosis in patients with different immune status. J. Thorac. Dis. 11:5042. doi: 10.21037/JTD.2019.12.53
Petrikkos, G., Skiada, A., Lortholary, O., Roilides, E., Walsh, T. J., and Kontoyiannis, D. P. (2012). Epidemiology and clinical manifestations of mucormycosis. Clin. Infect. Dis. 54S23-34. doi: 10.1093/CID/CIR866
Pfeiffer, C. D., Fine, J. P., and Safdar, N. (2006). Diagnosis of invasive aspergillosis using a galactomannan assay: a meta-analysis. Clin. Infect. Dis. 42, 1417–1427. doi: 10.1086/503427/2/42-10-1417-TBL006.GIF
Pickering, J. W., Sant, H. W., Bowles, C. A. P., Roberts, W. L., and Woods, G. L. (2005). Evaluation of a (1→3)-β-D-glucan assay for diagnosis of invasive fungal infections. J. Clin. Microbiol. 43, 5957–5962. doi: 10.1093/mmy/myx021
Potenza, L., Vallerini, D., Barozzi, P., Riva, G., Forghieri, F., Zanetti, E., et al. (2011). Mucorales-specific T cells emerge in the course of invasive mucormycosis and may be used as a surrogate diagnostic marker in high-risk patients. Blood 118, 5416–5419. doi: 10.1182/BLOOD-2011-07-366526
Prakash, H., Ghosh, A. K., Rudramurthy, S. M., Singh, P., Xess, I., Savio, J., et al. (2019). A prospective multicenter study on mucormycosis in India: epidemiology, diagnosis, and treatment. Med. Mycol. 57, 395–402. doi: 10.1093/MMY/MYY060
Ribes, J. A., Vanover-Sams, C. L., and Baker, D. J. (2000). Zygomycetes in human disease. Clin. Microbiol. Rev. 13, 236–301. doi: 10.1128/CMR.13.2.236
Rocha, I. C. N., Hasan, M. M., Goyal, S., Patel, T., Jain, S., Ghosh, A., et al. (2021). COVID-19 and mucormycosis syndemic: double health threat to a collapsing healthcare system in India. Trop. Med. Int. Health 26, 1016–1018. doi: 10.1111/TMI.13641
Roden, M. M., Zaoutis, T. E., Buchanan, W. L., Knudsen, T. A., Sarkisova, T. A., Schaufele, R. L., et al. (2005). Epidemiology and outcome of zygomycosis: a review of 929 reported cases. Clin. Infect. Dis. 41, 634–653. doi: 10.1086/432579
Rrapi, R., Chand, S., Gaffney, R., Lo, J. A., Smith, J. S., di Xia, F., et al. (2021). CASE SERIES Cutaneous mucormycosis arising in the skin folds of immunocompromised patients: a case series. JAAD Case Rep. 17, 92–95. doi: 10.1016/j.jdcr.2021.06.022
Shibata, W., Niki, M., Sato, K., Fujimoto, H., Yamada, K., Watanabe, T., et al. (2020). Detection of Rhizopus-specific antigen in human and murine serum and bronchoalveolar lavage. Med. Mycol. 58, 958–964. doi: 10.1093/MMY/MYAA001
Shigemura, T., Nakazawa, Y., Matsuda, K., Motobayashi, M., Saito, S., and Koike, K. (2014). Evaluation of Mucorales DNA load in cerebrospinal fluid in a patient with possible cerebral mucormycosis treated with intravenous liposomal amphotericin B. Int. J. Infect. Dis. 29, e200–e202. doi: 10.1016/J.IJID.2014.10.019
Spellberg, B. (2012). Gastrointestinal Mucormycosis: an Evolving Disease. Gastroenterol. Hepatol. 8:140.
Spellberg, B., Edwards, J., and Ibrahim, A. (2005). Novel perspectives on mucormycosis: pathophysiology, presentation, and management. Clin. Microbiol. Rev. 18, 556–569. doi: 10.1128/CMR.18.3.556-569.2005
Szalai, G., Fellegi, V., Szabó, Z., and Vitéz, L. C. (2006). Mucormycosis mimicks sinusitis in a diabetic adult. Ann. N. Y. Acad. Sci. 1084, 520–530. doi: 10.1196/ANNALS.1372.010
Tsikala-Vafea, M., Cao, W., Olszewski, A. J., Donahue, J. E., and Farmakiotis, D. (2020). Fatal Mucormycosis and Aspergillosis in an Atypical Host: what Do We Know about Mixed Invasive Mold Infections? Case Rep. Infect. Dis. 2020:8812528. doi: 10.1155/2020/8812528
Turunc, T., Demiroglu, Y. Z., Aliskan, H., Colakoglu, S., and Arslan, H. (2008). Eleven cases of mucormycosis with atypical clinical manifestations in diabetic patients. Diabetes Res. Clin. Pract. 82, 203–208. doi: 10.1016/j.diabres.2008.07.011
Wang, N., Zhao, G. Q., Gao, A., Che, C. Y., Qu, X. L., Liu, Y., et al. (2013). Association of TLR2 and TLR4 Gene Single Nucleotide Polymorphisms with Fungal Keratitis in Chinese Han Population. Curr. Eye Res. 39, 47–52. doi: 10.3109/02713683.2013.827212
Wotiye, A. B., Ks, P., and Ayele, B. A. (2020). Invasive intestinal mucormycosis in a 40-year old immunocompetent patient - A rarely reported clinical phenomenon: a case report. BMC Gastroenterol. 20:1–6. doi: 10.1186/S12876-020-01202-5/FIGURES/5
Yuen, K. Y., Chan, C. M., Chan, K. M., Woo, P. C. Y., Che, X. Y., Leung, A. S. P., et al. (2001). Characterization of AFMP1: a novel target for serodiagnosis of Aspergillosis. J. Clin. Microbiol. 39, 3830–3837. doi: 10.1128/JCM.39.11.3830-3837.2001
Zayet, S., Zaghdoudi, A., Ammari, L., Kilani, B., and Tiouiri Benaissa, H. (2021). Cerebro-rhino-orbital mucormycosis and aspergillosis coinfection in a patient with diabetes mellitus: a case report. IDCases 23:e01022. doi: 10.1016/J.IDCR.2020.E01022
Keywords: fungal infection, immunocompromised patients, COVID-19-associated mucormycosis, host markers, host genetics, assessment, prognosis
Citation: Acosta-España JD and Voigt K (2022) Mini Review: Risk Assessment, Clinical Manifestation, Prediction, and Prognosis of Mucormycosis: Implications for Pathogen- and Human-Derived Biomarkers. Front. Microbiol. 13:895989. doi: 10.3389/fmicb.2022.895989
Received: 14 March 2022; Accepted: 03 May 2022;
Published: 20 June 2022.
Edited by:
Axel Cloeckaert, Institut National de Recherche pour l’Agriculture, l’Alimentation et l’Environnement (INRAE), FranceReviewed by:
Victoriano Garre, University of Murcia, SpainCopyright © 2022 Acosta-España and Voigt. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Kerstin Voigt, a2Vyc3Rpbi52b2lndEBsZWlibml6LWhraS5kZQ==
†ORCID: Jaime David Acosta-España, orcid.org/0000-0001-5299-2732; Kerstin Voigt, orcid.org/0000-0002-1345-9991
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.