 Iwona Gregorczyk-Maga1†Mateusz Fiema2†
Iwona Gregorczyk-Maga1†Mateusz Fiema2† Michal Kania3,4*†Jolanta Kędzierska5Estera Jachowicz6†Dorota Romaniszyn6†
Michal Kania3,4*†Jolanta Kędzierska5Estera Jachowicz6†Dorota Romaniszyn6† Jadwiga Wójkowska-Mach6†
Jadwiga Wójkowska-Mach6†- 1Faculty of Medicine, Institute of Dentistry, Jagiellonian University Medical College, Krakow, Poland
- 2Department of Endocrinology, University Hospital, Krakow, Poland
- 3Doctoral School of Medicine and Health Sciences, Jagiellonian University Medical College, Krakow, Poland
- 4Chair of Metabolic Diseases, Faculty of Medicine, Jagiellonian University Medical College, Krakow, Poland
- 5Microbiology Unit, University Hospital, Krakow, Poland
- 6Chair of Microbiology, Faculty of Medicine, Jagiellonian University Medical College, Krakow, Poland
Potential interactions between the SARS-CoV-2 virus and the human oral microbiota are currently investigated widely. Patients with COVID-19 requiring mechanical ventilation in an intensive care unit (ICU) setting are at high risk of developing severe complications, including ventilator-associated pneumonia, thus making oral health management important. The aim of this study was to evaluate the oral health status and assess the dysbiosis of cultivable oral bacteriota in COVID-19 patients hospitalized in an ICU with acute respiratory distress within 36 h following intubation. In this prospective cohort study, we recruited 56 adult COVID-19 patients that qualified for mechanical ventilation in the Temporary ICU for COVID-19 Patients of the University Hospital in Krakow. On admission to the ICU, oral health of patients was assessed using the modified Beck Oral Assessment Score (BOAS). Four oral habitats were sampled, namely the buccal mucosa, tongue, buccal dental surface and gingival pocket. Microorganisms were identified by MALDI/TOF mass spectrometry. The mean age of the study population was 66.5 ± 12.7 years, there were 24 (42.9%) females. All patients included in this study were intubated and ventilated in the ICU, with a corresponding high mortality rate (76.8%). On admission to ICU, 76.8% subjects scored 11–20 on the BOAS scale (median 12 [IQR 10–14]), indicating moderate or severe dysfunction of oral health. Potentially pathogenic bacteria were identified in the oral microbiota samples, including Acinetobacter baumannii, Enterococcus faecalis, Escherichia coli and Klebsiella pneumoniae in 23.2%, 39.3%, 17.9%, and 19.6% of patients, respectively. Lactobacillus spp. were present in 57.1% subjects. The mean CFU counts of all bacteria strains in dental brushes were 9.3E+5 (1.4E+6) and in gingival pockets 7.6E+5 (1.4E+6). The highest CFU counts were observed for Enterococcus spp. and, Lactobacillus spp., although these did not differ significantly from CFU counts of Streptococcus spp. and Staphylococcus spp. In this report we comprehensively characterized the oral health condition and cultivable oral bacteriota in COVID-19 patients hospitalized in an ICU with acute respiratory distress within 36 h following intubation. The oral bacteriota showed significant qualitative and quantitative dysbiosis. Hospitalization in an ICU and mechanical ventilation are important factors leading to oral dysbiosis in SARS-CoV-2 patients.
Introduction
Coronavirus disease 2019 (COVID-19), caused by a severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), has caused a global pandemic and resulting serious public health crisis (Zhu et al., 2020; World Health Organization, 2022). While most COVID-19 patients have minor symptoms, ~15% of hospitalized patients require admission to an intensive care unit (ICU; Terlecki et al., 2021). These patients exhibit respiratory failure with a systemic inflammatory reaction and multiple-organ dysfunction, requiring oxygen supplementation and, in some cases mechanical ventilation (Weiss and Murdoch, 2020).
Over 1,000 bacterial species have been reported to reside in the oral cavity (Dewhirst et al., 2010). In healthy individuals the oral bacteriota is dominated by Actinobacteria (Acctinomyces, Corynebacterium and Rothia), Bacteroides (Capnocytophaga, Porphyromonas and Prevotella), Firmicutes (Granulicatella and Streptococcus), Fusobacteria, Proteobacteria (Haemophilus and Neisseria; Zaura et al., 2001). The oral cavity can be divided into several microbiologically distinct niches, including saliva, soft tissue surfaces of the oral mucosa and tongue, and hard tissue surfaces of teeth (Xu et al., 2015; Zhang et al., 2018). Of the most common species, 54% is cultivable and identifiable, 14% is cultivable but not easily identified, and 32% cannot be cultivated, remaining in dormant state (Caselli et al., 2020). Recent research of oral microbiota resulted in two large databases: Human Microbiome Project (HMP) and Human Oral Microbiome Database (HOMD). HMP contains microbiome data from 5 main environments: the oral cavity, nasal cavity, vagina, gut and skin. Data in HOMD encompasses oral microbiota composition (Li et al., 2022).
Previous studies of changes in microbiome, including the oral microbiota, showed a significant reduction of microbial diversity in SARS-CoV-2 affected patients (Iebba et al., 2021; Wu et al., 2021; Uehara et al., 2022). These changes comprised decreased abundance of Neisseria, Corynebacterium, Aggregatibacter, Treponema, and Pseudomonas genus, and Prevotella intermedia in the oral cavity of COVID-19 patients. Importantly, the loss of comensal Neisseria, such as N. subflava and N. mucosa, and Prevotella spp. acting as a local oral probiotic, can lead to severe imbalance in the oral microbiota composition (Weyand, 2017; Rafiqul Islam et al., 2022). Enrichment of Campylobacter, Granulicatella, Veillonella and Filifactor genus was also observed, that can be of clinical significance, as those are taxa associated with periodontitis (Wu et al., 2021). Veilonella spp. has been also reported to induce proinflammatory responses (Haran et al., 2021). Furthermore, increased abundance of opportunistic Hemophilus parainfluenzae in the oral cavity can predispose patients to respiratory tract infections (Iebba et al., 2021; Wu et al., 2021). Another report revealed that COVID-19 patients had a higher abundance of Enterococcus spp. in the oral cavity, linking respiratory pathogens with gut microbiome abnormalities (Rafiqul Islam et al., 2022). The dysbiosis was even more pronounced in severe course of infection and long-COVID-19, suggesting that its extent can be treated as an indicator of infection severity (Haran et al., 2021; Wu et al., 2021; Fiema et al., 2022; Rafiqul Islam et al., 2022). The use of antibiotics in COVID-19 patients was also associated with independent oral and gut microbiome profiles (Wu et al., 2021).
A high prevalence of oral health problems, such as xerostomia, mucosal blistering, mouth rash and lip necrosis has been observed in patients with COVID-19 (Aragoneses et al., 2021). Several trials have correlated poor oral hygiene with hyper-inflammation (Kamel et al., 2021), and poor oral health in patients with caries and periodontitis may play a significant role in the development of severe complications of COVID-19 in patients managed in the ICU (Hocková et al., 2021; Marouf et al., 2021). Moreover, during prolonged endotracheal intubation, dysbiotic oral microbiota can colonize the lower respiratory tract. These patients are at high risk for developing bacterial ventilator-associated pneumonia (VAP). The oral management of these patients in an ICU is critical as oral care has been shown to reduce the incidence of VAP (Bao et al., 2020; Luyt et al., 2020).
The aim of this study was to evaluate the oral health status and assess the dysbiosis of cultivable oral bacteriota in COVID-19 patients hospitalized in an ICU with acute respiratory distress in the early post-intubation period.
Materials and methods
Study design and participants
In this prospective cohort study, we recruited 56 consecutive adult COVID-19 patients that qualified for mechanical ventilation in the Temporary ICU for COVID-19 Patients of the University Hospital in Krakow (UH) between January 31st and September 1st 2021. University Hospital in Krakow coordinated the care for patients with SARS-CoV-2 infection in Lesser Poland and was responsible for the hospitalization of patients with COVID-19 requiring specialized treatment.
Patients were diagnosed with COVID-19 according to WHO and Polish guidelines with the use of RT-PCR (Diagnostic testing for SARS-CoV-2 [internet], 2022; Flisiak et al., 2022). The COVID-19 treatment algorithm in patients admitted to UH was based on constantly updated recommendations of the Polish Association of Epidemiologists and Infectiologists (Flisiak et al., 2022), including concurrent probiotic use in patients undergoing antibiotic therapy.
The inclusion criteria for this study were as follows: 1. SARS-CoV-2 infection confirmed by RT-PCR assay of nasal and pharyngeal swabs upon hospital admission, 2. Admission to the ICU, 3. Signed consent to participate in the study and 4. Intubation due to COVID-19 related pneumonia and acute respiratory distress syndrome (ARDS) within the preceding 36 h from commencement of the study procedures.
The patients included in the study were admitted from emergency wards (either at UH or non-UH) or transferred from another ward dedicated for COVID-19 patients (UH or outside UH).
Demographic and clinical data were gathered from the hospital electronic medical records. The database included information on age, sex, date of COVID-19 diagnosis (defined as the first positive result of antigen and PCR test from nasopharyngeal swab), date of admission to the hospital, institution of the patients’ origin (emergency ward, hospital ward), date of discharge or death, date of admission to the ICU, date of intubation, COVID-19 severity on WHO Clinical Progression Scale (Supplementary Table S1; Marshall et al., 2020), comorbidities [previous diagnosis of diabetes, arterial hypertension, heart failure (HF), history of MI or stroke, ischemic heart disease, atrial fibrillation (AF), chronic kidney disease (CKD), chronic obstructive pulmonary disease (COPD)] and pre-intubation treatment [remdesivir, antibiotic, days of antibiotic treatment (DOT) before intubation (the number of days a patient receives an antibiotic independent of dose), proton pump inhibitor]. CVD and cardiovascular risk factors were identified based on a medical history of prehospital diagnosis or treatment. Other chronic comorbidities were also diagnosed based on earlier clinical notes available in the medical records. Baseline laboratory results [C-reactive protein (CRP), procalcytonin (PCT), interleukin-6 (IL-6), D-dimer, white blood count (WBC), creatinine] were also extracted.
Oral health assessment
On admission to the ICU, oral health was assessed using a modified BOAS, consisting of five subscales, namely assessment of lips, mucosa and gingiva, tongue, teeth, and saliva. A higher score reflects dysfunction or tissue injury. BOAS scores range from 5 (no oral dysfunction) to 20 (severe dysfunction), and a score >5 is abnormal (Beck, 1979; Ames et al., 2011; Supplementary Table S2).
Oral cavity sampling methods
Four oral habitats were sampled by a trained dentist: the buccal mucosa, the tongue, buccal dental surface and gingival pocket, with the latter two only in patients with dentition. Specimens from the posterior dorsum of the tongue and buccal mucosa were collected using ESwab™ (Demuyser et al., 2018), which combines a COPAN-invented flocked swab with 1 ml of Liquid Amies in a plastic, screw cap tube. Dental plaque was collected from buccal dental surface side using Tooth Cleanic KerrHawe-KWX-OP-SZ-011, and after collection the brush was placed in 1 ml of Liquid Amies in a plastic screw cap tube. PerioPaper Strips (n = 3; Guentsch et al., 2011), designed to absorb or carry 0–1.2 μl of fluid, were used to collect gingival crevicular fluid (GCF) samples. The strips were placed in the gingival pocket for 30–45 s till its surface moistened. To minimize the risk of pre-analytical errors during sample collection, sterile gauze was used to remove excess saliva from the mucosa and dry the dental surfaces, preventing salivary contamination of GCF.
Microbiological cultures
The samples were immediately delivered to the microbiological laboratory, where they were inoculated by the dilution method (dilutions −1 to −6) or qualitative culture method (swabs only) on the following media: McConkey (Graso, Biotech), Columbia (Lab-Agar, Biomaxima), Scheadler (Scheadler-Agra, Biomaxima), Bile Esculine Azide (Lab-Agar, Biomaxima), MRS Agar (Oxoid), Sabouraud Agar (Biomaxima). Media were aerobically incubated at 37°C (McConkey, Columbia, Bile Esculine Azide) or anaerobically at 37°C (M.R.S and Scheadler, GENbag Atmosphere Generators [BioMérieux, France] for 48 h). After incubation, the phenotypical colonies were counted and reported, and results were presented as CFU/ml (colony forming unit). After isolation, the microorganisms were identified by MALDI TOF mass spectrometry (Vitek MS Home bioMérieux).
Multiple analyses were performed to identify factors associated with oral health status, biodiversity and composition of oral commensal and potentially pathogenic bacterial microbiota, and in-hospital mortality.
Ethics statement
The study and its protocol were approved by the Jagiellonian University Bioethics Committee, decision number 1072.6120.333.2020; December 7, 2020. Written informed consent was obtained from each subject prior to participation.
Statistical analysis
PS Imago Pro v.6.0 and Statistica v.13 were used for all statistical analysis. The normality of continuous variable distribution was assessed using the Shapiro–Wilk test. Differences between groups were analyzed with Student’s t-test or nonparametric tests (Mann–Whitney U-test, Kruskal–Wallis ANOVA) when appropriate. Paired data were analyzed using the Wilcoxon test or Friedman’s ANOVA along with appropriate post-hoc tests. Continuous variables were presented as arithmetic means (x̄) ± standard deviations (SD) or as the median with interquartile range (IQR) when the data were not normally distributed. The distribution of categorical variables was described as counts and percentages. Statistical testing was completed to compare categorical variables using an independent sample Chi-squared test or Fisher’s exact test when appropriate, and dependent samples with McNemar’s test and Cochran’s Q ANOVA. A p-value of <0.05 was considered statistically significant. The Bonferroni correction was used for multiple comparisons.
Results
Demographic data and background
The study population included 56 patients admitted to an ICU ward with ARDS due to COVID-19 related pneumonia. The mean age was 66.5 ± 12.7 years, there were 24 (42.9%) females. The subjects for whom data was available were classified as obese (mean BMI 31.9 ± 5.8, data available for 35 subjects). The most prevalent comorbidities were hypertension (46.4%), diabetes (35.7%) and coronary artery disease (28.6%).
The median WHO Clinical Progression Scale score was 6 on admission to ICU, meaning patients required oxygen by NIV or high flow (Figure 1). Of the enrolled patients, 16 (28.6%) were transferred directly from the emergency department, 30 (53.6%) were transferred from another UH ward, and 10 (17.9%) were transferred from another ward outside UH. The mean time between admission to UH and intubation was 4.91 ± 5.56 days.
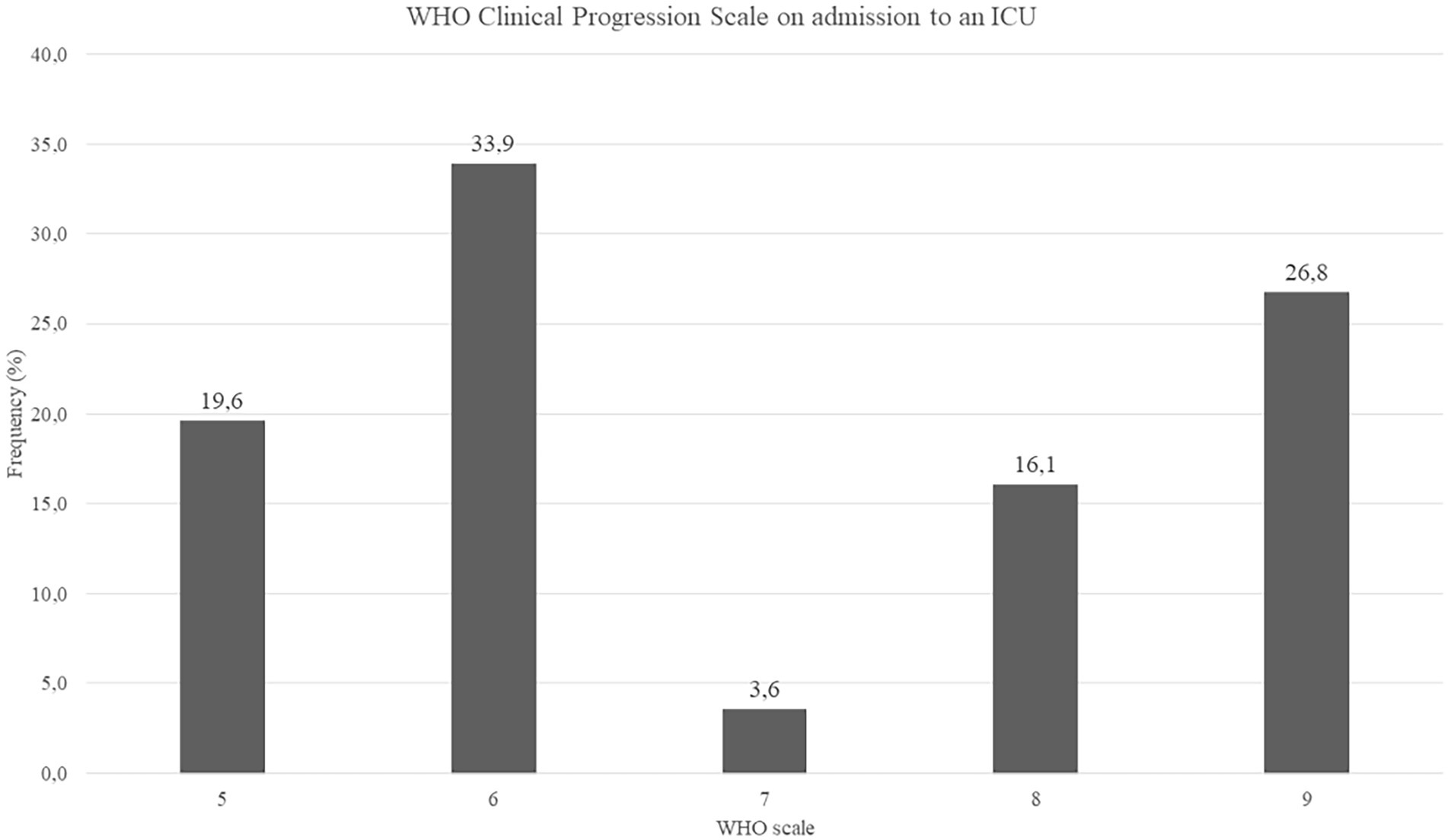
Figure 1. WHO Clinical Progression Scale on admission to an ICU, N = 56, data presented as percentages.
On admission to the hospital, inflammatory markers were increased, indicating a severe response to COVID-19 infection (Table 1). Systemic steroid therapy was used in 40 (76.9%) and antibiotics in 33 (63.5%, of whom 32 were treated with β-Lactam antibiotics) patients before admission to an ICU. Median antibiotic DOT before intubation was 8 (range 4–13 days).
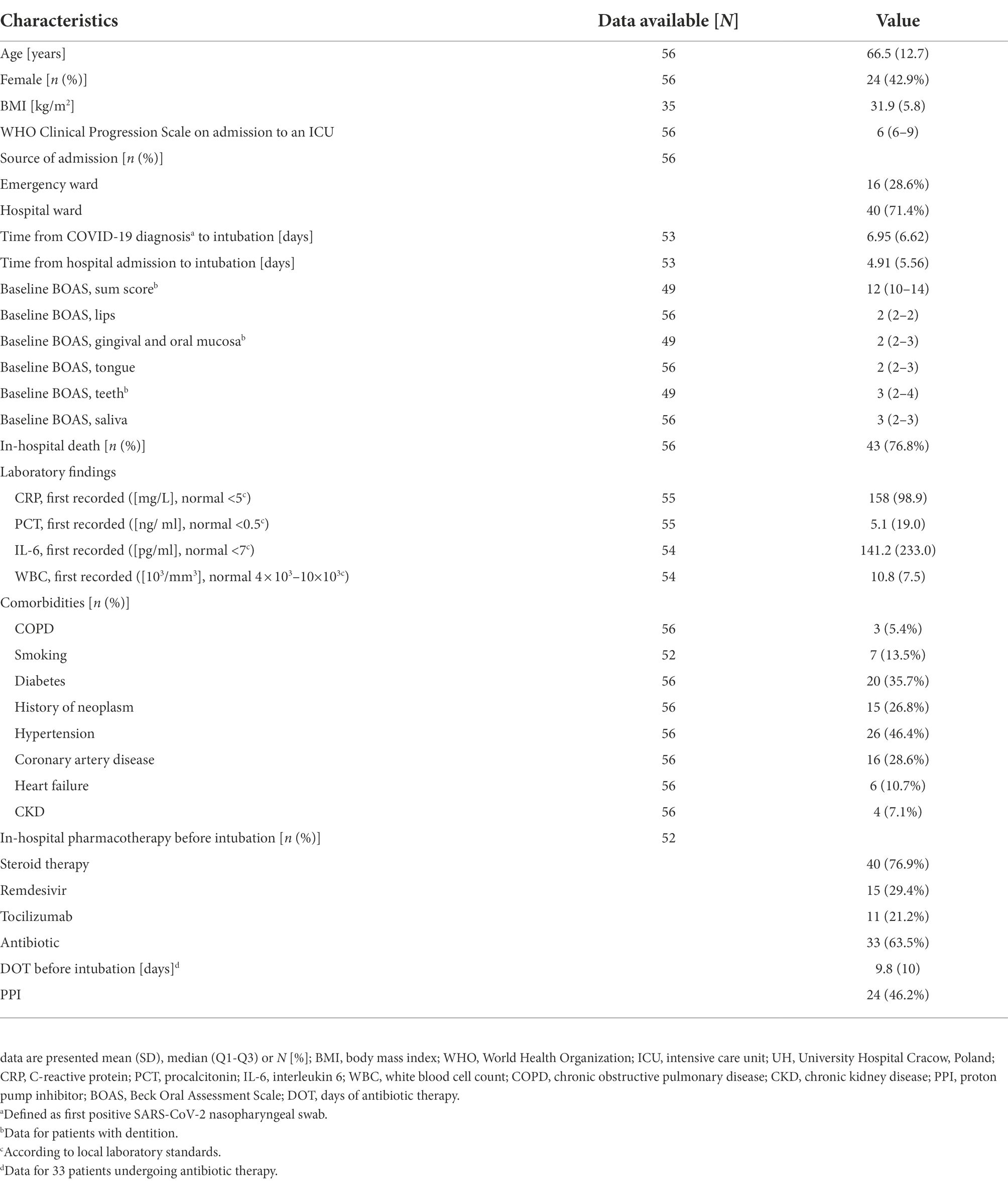
Table 1. Baseline characteristics of study participants and outcomes of hospitalization.
Clinical outcomes
All patients were intubated and ventilated in the ICU, and a corresponding high mortality rate was observed in the recruited patients (76.8%). There were no significant differences between survivors and non-survivors with regards to demographic characteristics, laboratory findings and oral health status (Supplementary Table S3).
Furthermore, there were no clinically relevant differences in the demographic characteristics, laboratory findings and mortality between the patients with different severities of COVID-19 on the WHO Progression Scale, the ward preceding admission to ICU, or previous steroid or antibiotic treatment.
Oral health assessment
On admission to ICU, the median BOAS was 12 (IQR 10–14), and we found 76.8% subjects scored 11–20, indicating moderate or severe dysfunction of oral health (Figure 2). Furthermore, the BOAS score differed significantly between the subcategories (p < 0.001). Our data indicated teeth had a significantly higher BOAS score than lips and gingival/oral mucosa (p = 0.003, p = 0.011). Comparison of subjects with no or mild vs. moderate or severe dysfunction in BOAS score revealed that the latter were older (60, IQR 48–68 vs. 69.5, IQR 63–75, p = 0.006), had higher initial inflammatory markers (PCT 0.17, IQR 0.08–0.46 vs. 0.42, IQR 0.17–1.16, p = 0.034) and higher HbA1c% (5.9, IQR 5.3–6.35 vs. 6.75 IQR 6.15–8.28, p = 0.029). There was also a trend toward higher WHO Progression Scale score in patients with moderate or severe dysfunction as indicated by their BOAS score, but it did not reach statistical significance. Finally, there was a significant but weak positive correlation between the selected BOAS subscales and the time from COVID-19 infection detection.
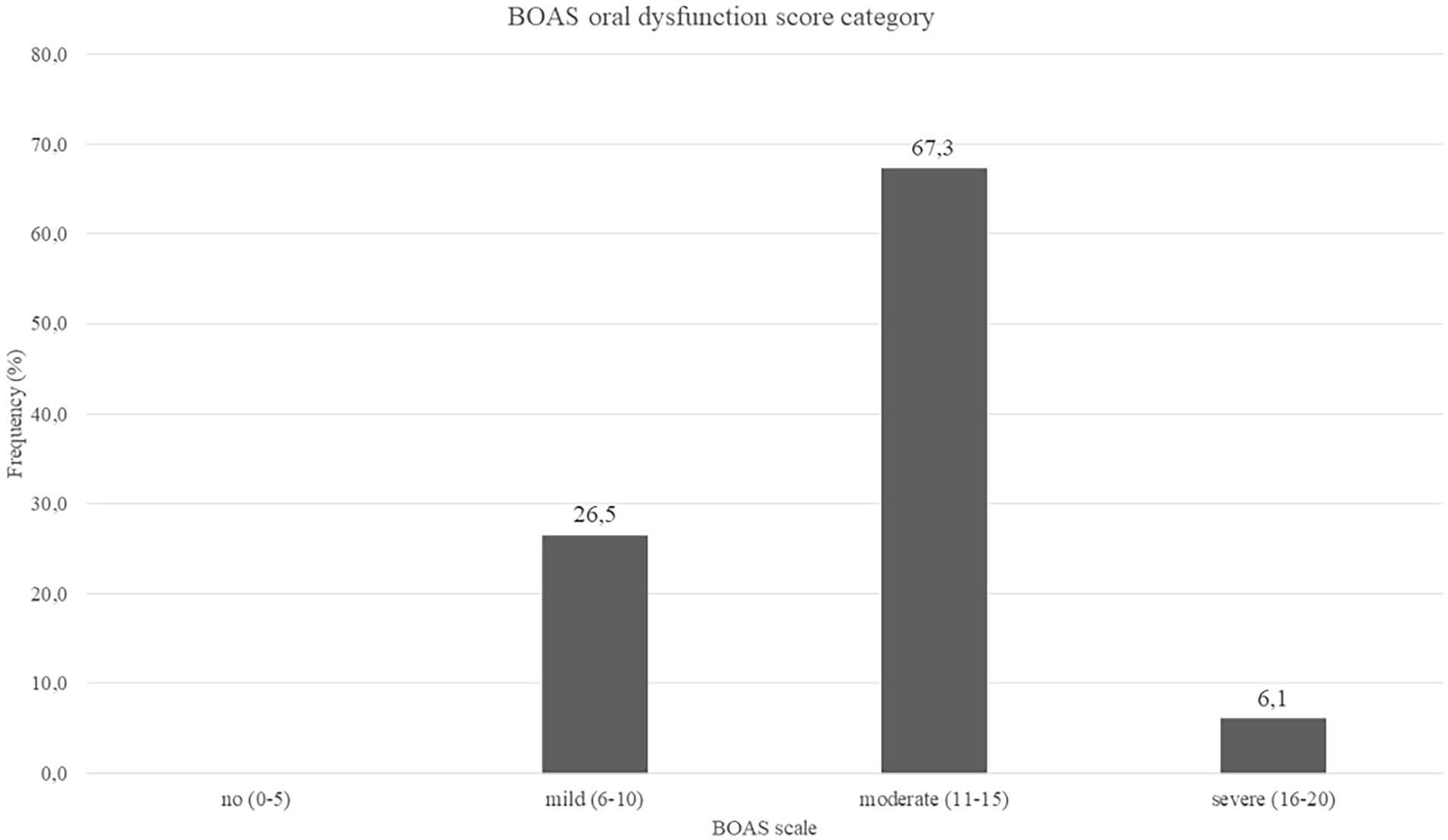
Figure 2. Baseline BOAS oral dysfunction score category, N = 49, data presented as percentages.
Bacteriological findings
In total, 32 genera and 70 bacterial species were identified in the study subjects (Table 2, full list in Supplementary Table S4). A number of strains were identified on the genera level [Lactobacillus acidophilus/gasseri (39 strains), Streptococcus mitis/oralis (100 strains), Streptococcus salivarius ssp thermophilus/Str.salivarius ssp salivarius/Str. Vestibularis (38 strains), Lactobacillus casei/paracasei/rhamosus (26 strains)]. Furthermore, multiple, potentially pathogenic bacteria were identified in the oral microbiota samples, including Acinetobacter baumannii, Enterococcus faecalis, Escherichia coli and Klebsiella pneumoniae in 23.2%, 39.3%, 17.9%, and 19.6% of patients, respectively (Figure 3). Lactobacillus spp. was present in 57.1% of patients, and Cariogenic S. mutans was identified in one subject.
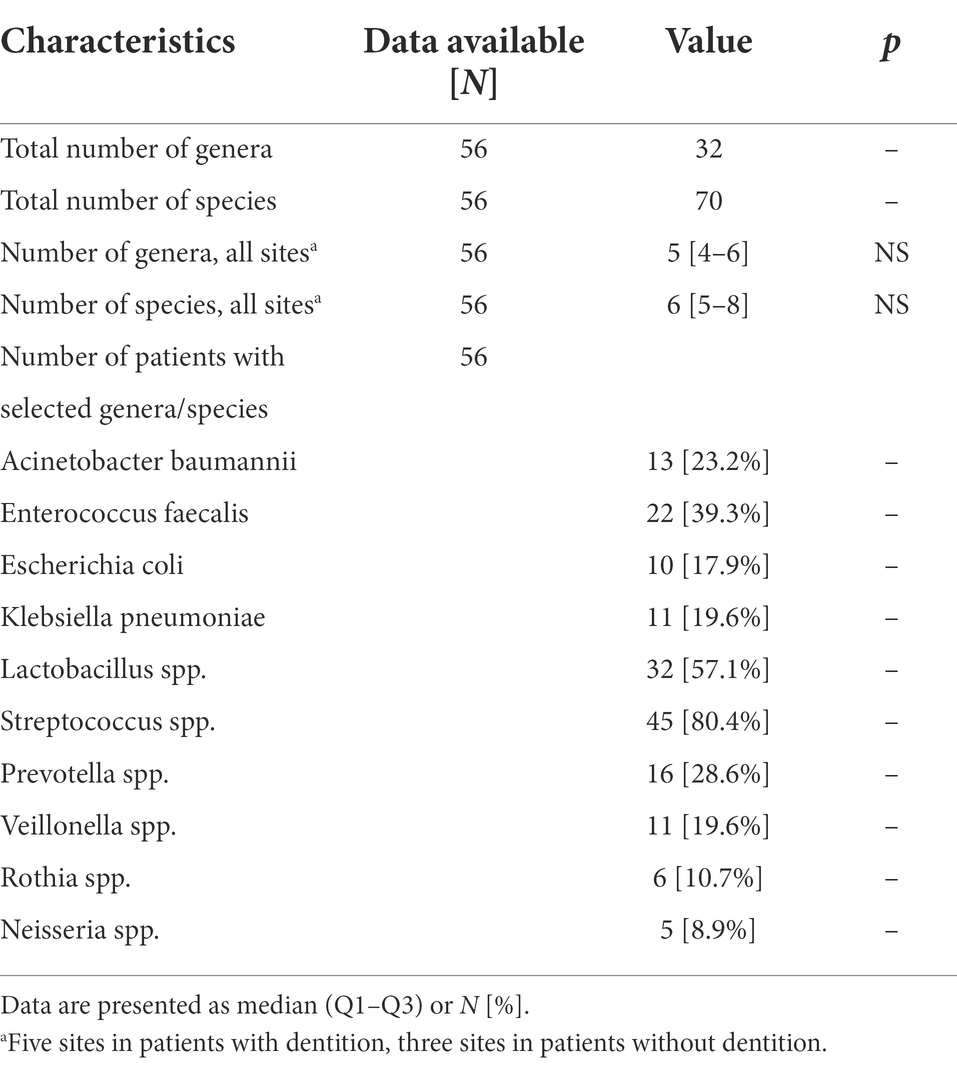
Table 2. Baseline qualitative microbiological characteristics of study participants.
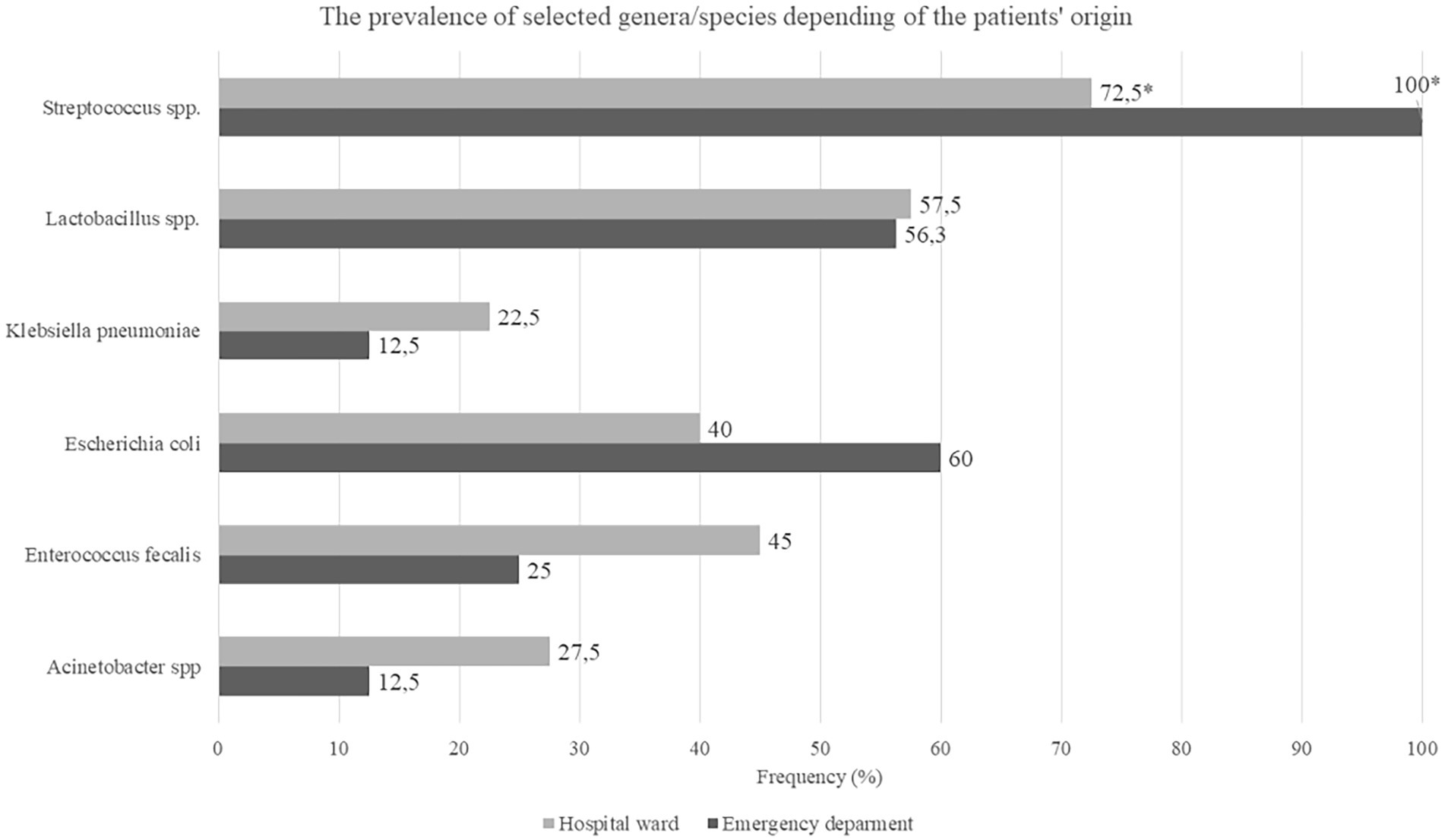
Figure 3. Number of patients with selected genera/species depending of the patients’s origin, N = 56, data presented as percentage.
Escherichia coli and Streptococci spp. were identified more frequently in patients admitted from the emergency department than in those transferred from other hospital wards (100% vs. 64.4%, p = 0.023 and 100% vs. 72.5%, p < 0.001; Figure 3). Moreover, patients in whom no Streptococci strains were identified had higher DOT before intubation when compared to those with Streptococci strains present (12, IQR 8–26.5 vs. 5, IQR 2–8.5, p = 0.013). Escherichia coli was more frequently found in patients with diabetes (70% vs. 30%, p = 0.025) and CAD (37.5% vs. 10%, p = 0.024) than in those without. Finally, non-survivors had lower baseline prevalence of Lactobacillus spp. as compared to survivors (48.8% vs. 84.6%, p = 0.028).
There were no associations between the sum BOAS scores and microbiological findings, although more detailed analyses revealed Lactobacillus spp. positive patients had lower BOAS saliva score as compared to those with no Lactobacillus spp. (median 2.5 vs. 3, IQR 2–3 and 2–3 respectively, p = 0.045). The BOAS saliva score was lower in patients using antibiotic treatment before intubation (median 2 vs. 3, IQR 2–3 and 2–3 respectively, p = 0.05).
The CFU counts were available for samples acquired by the dental brush and from gingival pockets, and the median CFU counts from all sites were 3.0E+5 (6.3E+4–1.0E+6). The median CFU counts of all bacterial strains in dental brushes was 4.0E+5 (1.0E+5–1.4E+6) and in gingival pockets 2.0E+5 (4.0E+4–8.0E+5), with data available for 81.2 and 68.4% samples, respectively. There were no differences in the median CFU counts between the BOAS score categories in dental brushes and gingival pockets (p = 0.198). Interestingly, patients with previous antibiotic use had lower CFU counts than those without (median 2.0E+5 [4.0E+4–8.8E+5] vs. 4.5E+5 [1.2E+5–1.5E+6], p = 0.007), while patients transferred from the emergency department had higher CFU counts than those transferred from other hospital wards (median 6.0E+5 [2.8E+4–1.5E+6] vs. 3.0E+5 [IQR 4.0E+4–1.0E+6], p = 0.016).
The CFU counts for Gram-positive bacteria were higher than for Gram negative (median 5.0E+5 [1.1E+5–1.5E+6] vs. 1.0E+5 [5.0E+3–3.0E+5], p < 0.001). Finally, the highest median CFU counts from all sites were observed for Enterococcus spp., Lactobacillus spp., Streptococcus spp. and Staphylococcus spp. (Table 3; Figure 4).
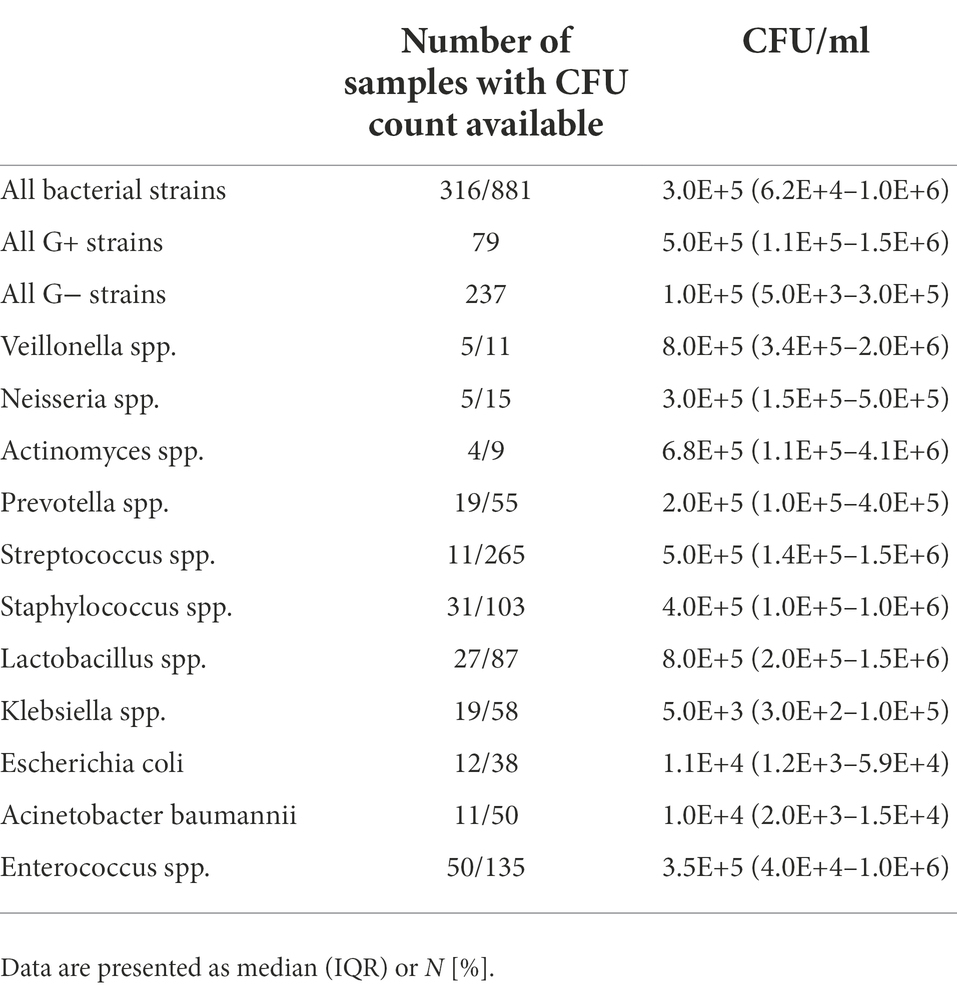
Table 3. Baseline quantitative microbiological characteristics of study participants.

Figure 4. CFU counts of selected identified bacteria genera.
Discussion
In this report, we comprehensively characterized the oral health condition and cultivable oral bacteriota in COVID-19 patients hospitalized in an ICU with ARDS within 36 h following intubation. In this population, the oral microbiota from mucosal swabs, dental samples, and gingival pockets showed significant qualitative and quantitative dysbiosis and was distinct from healthy patients. SARS-CoV-2 infection, hospitalization in an ICU and mechanical ventilation are important factors leading to oral dysbiosis in patients.
Our study population comprised a homogenous group of patients with COVID-19 infection that were hospitalized in a temporary ICU dedicated to SARS-CoV-2-positive patients. These patients, with severe COVID-19 and ARDS, required specialist medical care, including mechanical ventilation or hemodialysis. Our data demonstrated a significantly higher mortality rate compared to normal COVID admissions, although our election criteria biased patient selection toward the most severe COVID-19 cases. Our study population was also older, with multiple comorbidities that have confirmed deleterious effects on COVID-19 survival, such as diabetes and cardiovascular disease (Harrison et al., 2021).
Our study population presented with moderate or severe dysfunction of oral health. We believe that this resulted from first, poor oral health status in the elderly adult Polish population as presented in one recent report (Malicka et al., 2022). The authors noted that 21% of 70-year-olds were completely toothless. On average, the number of teeth was 12.97 ± 9.5., with 4.7 ± 4.8 teeth in the occlusion. 30.8% of patients wore a partial removable denture, and 25% a complete removable maxillary denture. 20% of study participants had a partial removable denture, and 22.6% had a complete removable mandibular denture. Oral dryness was observed in ca. one-third of the studied cohort, nearly 20% had periodontitis and ~30% required treatment for caries. They emphasized that more than 60% of patients required professional dental prophylaxis (Malicka et al., 2022). Secondly, another report from a similar cohort (age and comorbidities) revealed patients hospitalized due to myocardial infarction presented higher plaque and periodontal indices as compared to patients with stable angina pectoris (Wozakowska-Kapłon et al., 2013). Still, this subject is under researched and further exploration is required. Finally, previous studies of ICU COVID-19 patients reported xerostomia, mucosal blistering and ulcers, rash, lip necrosis, and loss of taste and smell (Kamel et al., 2021; Eduardo et al., 2022; Yoshino et al., 2022). These can exacerbate such conditions as periodontitis, being an important risk factor for complications in patients with COVID-19 hospitalized in the ICU (Marouf et al., 2021). Pre-COVID-19 reports showed that hospitalization in an ICU together with mechanical ventilation can have a deleterious effect on oral health (Terezakis et al., 2011), including accumulation of the dental plaque and emergence of mucosal lesions. Due to the deterioration of oral health, critically ill patients in the ICU represent a group vulnerable to further complicates including VAP (Luyt et al., 2020).
Another noteworthy finding was a significant and alarming qualitative and quantitative dysbiosis of the cultivable oral bacteriota in our study population, as early as up to 36 h following intubation. Potentially pathogenic bacteria including Acinetobacter baumannii, Enterococcus faecalis, Escherichia coli and Klebsiella pneumoniae occurred frequently with large CFU counts in our study population. While previous studies showed that these species are found in the oral cavity, their prevalence was not as high as in our patient population (Beck, 1979; Marshall et al., 2020; Diagnostic testing for SARS-CoV-2 [internet], 2022).
The CFU counts of such species as Enterococcus faecalis and Acinetobacter baumannii were as high as commensal Streptococci and Staphylococci, indicating significant abnormalities in the oral bacteriobiota hemeostasis.
In one study, oral rinse samples from COVID-19 patients with a wide spectrum of symptoms showed a comparable extent of oral dysbiosis, with lower bacterial diversity, higher abundance of Lactobacillus spp., Enterococcus spp., Acinetobacter baumannii, and lower amounts of Gemella spp., Fusobacterium spp. and Haemophilus spp. (Soffritti et al., 2021).
The prevalence of E. coli was surprisingly high in our population. Escherichia coli is not a member of commensal oral microbiota, however it was detected in oral cavities of elderly patients with systemic diseases (Zawadzki et al., 2017). Recently, E. coli was reported to successfully colonize a supragingival biofilm (Pérez-Chaparro et al., 2014), so under special nutritional and environmental circumstances, E. coli can likely survive and even dominate this niche, especially in immunocompromised patients (Thurnheer and Belibasakis, 2014). Additionally, we found a higher prevalence of E. coli in patients admitted from the emergency ward than in those transferred from other hospital wards. To date, there have been no other reports on this issue, warranting further research.
Conversely, Enterococcus faecalis was more frequent in patients transferred from other hospital wards than those originating from the emergency department. Previous studies showed similar results, with changes in the oral bacteriobiota composition result from the exposure to hospital bacteria and each subsequent day of hospitalization increases the risk of Enterococci infections (Russo Fiorino et al., 2021). Moreover, E. coli and E. faecalis can employ antagonistic interactions against S. mutans (Thurnheer and Belibasakis, 2014), partially explaining our observations.
Our analyses revealed that the prevalence of commensal Streptococcus strains was lower in patients with a higher antibiotic consumption prior to intubation. We consider that antibiotics could be a major factor contributing to oral dysbiosis and disappearance of “healthy” commensal strains. Of all antibiotics, β-Lactam antibiotics were most commonly used in our cohort. Prospective cohort studies revealed that Shannon biodiversity index was decreased during amoxicillin treatment and was subject to further reduction in the following 6 months’ time period (Menon et al., 2019; Monroy-Pérez et al., 2020; Nel Van Zyl et al., 2022). The density of Neisseria, Streptococcus and Veillonella strains in the oral cavity was also reported to decrease during treatment with amoxicillin (Larsson Wexell et al., 2016; Moraes et al., 2020). Save commonly used amoxicillin, other groups of antibiotics with various mechanisms of action can influence the oral microbiota and promote the selection of multi-drug resistant strains and their horizontal transmission (Zaura et al., 2015; Moraes et al., 2020). Other factors that can lead to oral dysbiosis include: local and systemic diseases, improper oral hygiene, unbalanced diet, smoking tobacco and immunosuppression (Li et al., 2022).
Lactobacillus was more prevalent in survivors in our study population, but there were no associations with antibiotic use, or with probiotic use according to the care standards in UH wards. One previous study reported the relative abundance of various bacterial genera, including Lactobacillus spp. in COVID-19 patients (Soffritti et al., 2021). These findings are notable, as Lactobacillus spp. may play some role in the protection against SARS-CoV-2, acting as an inhibitor of viral contamination by multiple mechanisms, including production of metabolites with antiviral activity, stimulation of mucosal immune system cells and local cytokines production (Zrelli et al., 2021).
Previous studies of COVID-19 patients tested saliva or nasopharyngeal swabs (Lloréns-Rico et al., n.d.; Miller et al., 2021). One notable strength of our study is that we investigated mucosal and dental brushes, highly representative for microbiota analysis (Zaura et al., 2001). Considering a proper and complex oral health evaluation, we used the BOAS scale. Among oral assessment tools, BOAS has been proposed as the most appropriate for ICU patients, with the mucosal-dental plaque score most applicable during observation (Ames et al., 2011).
Our study also had some limitations. First, we focused only on the SARS-CoV-2-positive patients. Moreover, in this study we used traditional methods for identification of microorganisms on the species level. As it is known, NGS it also allows obtaining information on non-cultivable microorganisms. But the method we used allowed the establishment of a microbial bank, for future studies in healthcare-associated-infections.
Conclusion
COVID-19 patients hospitalized in an ICU in the early post-intubation period presented an alarming qualitative and quantitative dysbiosis of the cultivable oral bacteriota. Abnormalities in the oral health status can trigger deterioration and dysbiosis of the oral microbiota. Poor oral hygiene, cough, increased inhalation and mainly mechanical ventilation provide a pathway for oral microorganisms to enter the lower respiratory tract, leading to pneumonia. A proper assessment of oral health can provide information on how to treat and diagnose these patients. Effective oral health care measures are necessary to reduce these infections, especially in severe COVID-19 patients.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by by the Jagiellonian University Bioethics Committee (Komisja Bioetyczna, Uniwersytet Jagielloński). The patients/participants provided their written informed consent to participate in this study.
Author contributions
IG-M: conceptualization, investigation, methodology, project administration, resources, supervision, and writing–review and editing. MF: data curation, methodology, investigation, writing–original draft preparation, and writing–review and editing. MK: formal analysis, methodology, visualization, writing–original draft preparation, writing–review and editing. EJ: formal analysis, methodology, validation. DR: formal analysis, methodology, validation. JW-M: methodology, formal analysis, validation, writing–review and editing, resources. All authors contributed to the article and approved the submitted version.
Funding
This publication was supported by the National Center for Research and Development CRACoV-HHS project (Model of multi-specialist hospital and non-hospital care for patients with SARS-CoV-2 infection) through the initiative “Support for specialist hospitals in fighting the spread of SARS-CoV-2 infection and in treating COVID-19” (contract number SZPITALE-JEDNOIMIENNE/18/2020). The described research was implemented by consortium of the University Hospital in Krakow and the Jagiellonian University Medical College.
Acknowledgments
The authors would like to thank all the patients who participated in this study.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmicb.2022.1013559/full#supplementary-material
References
Ames, N. J., Sulima, P., Yates, J. M., McCullagh, L., Gollins, S. L., Soeken, K., et al. (2011). Effects of systematic Oral Care in Critically ill Patients: a multicenter study. Am. J. Crit. Care 20:e103, –e114. doi: 10.4037/ajcc2011359
Aragoneses, J., Suárez, A., Algar, J., Rodríguez, C., López-Valverde, N., and Aragoneses, J. M. (2021). Oral manifestations of COVID-19: updated systematic review with meta-analysis. Front. Med. 8:1423. doi: 10.3389/fmed.2021.726753
Bao, L., Zhang, C., Dong, J., Zhao, L., Li, Y., and Sun, J. (2020). Oral microbiome and SARS-CoV-2: beware of lung co-infection. Front. Microbiol. 11:1840. doi: 10.3389/fmicb.2020.01840
Beck, S. (1979). Impact of a systematic oral care protocol on stomatitis after chemotherapy. Cancer Nurs. 2, 185–299. doi: 10.1097/00002820-197906000-00002
Caselli, E., Fabbri, C., D’Accolti, M., Soffritti, I., Bassi, C., Mazzacane, S., et al. (2020). Defining the oral microbiome by whole-genome sequencing and resistome analysis: the complexity of the healthy picture. BMC Microbiol. 20, 1–19. doi: 10.1186/s12866-020-01801-y
Demuyser, T., De Geyter, D., Van Dorpe, D., Vandoorslaer, K., and Wybo, I. (2018). Extensive evaluation of fastidious anaerobic bacteria recovery from the Copan eSwab® transport system. J. Microbiol. Methods 144, 73–78. doi: 10.1016/j.mimet.2017.11.009
Dewhirst, F. E., Chen, T., Izard, J., Paster, B. J., Tanner, A. C. R., Yu, W. H., et al. (2010). The human oral microbiome. J. Bacteriol. 192, 5002–5017. doi: 10.1128/JB.00542-10
Eduardo, F. P., Bezinelli, L. M., Gobbi, M. F., Bergamin, L. G., DLC, D. C., and Corrêa, L. (2022). Oral lesions and saliva alterations of COVID-19 patients in an intensive care unit: a retrospective study. Spec. Care Dentist. doi: 10.1111/scd.12705
Fiema, M., Wlodarczyk, A., Wojkowska-Mach, J., Garlicki, J., and Gregorczyk-Maga, I. (2022). Atypical presentation of aspergillus Niger infection in the oral cavity as a prediction of invasive pulmonary aspergillosis in a patient with COVID-19: case report and literature review. Microorg 10:1630. doi: 10.3390/microorganisms10081630
Flisiak, R., Horban, A., Jaroszewicz, J., Kozielewicz, D., Mastalerz-Migas, A., Owczuk, R., et al. (2022). Zalecenia postępowania w zakażeniach SARS-CoV-2 Polskiego Towarzystwa Epidemiologów i Lekarzy Chorób Zakaźnych, na dzień 23 lutego.
Guentsch, A., Kramesberger, M., Sroka, A., Pfister, W., Potempa, J., and Eick, S. (2011). Comparison of gingival Crevicular fluid sampling methods in patients with severe chronic periodontitis. J. Periodontol. 82, 1051–1060. doi: 10.1902/jop.2011.100565
Haran, J. P., Bradley, E., Zeamer, A. L., Cincotta, L., Salive, M. C., Dutta, P., et al. (2021). Inflammation-type dysbiosis of the oral microbiome associates with the duration of COVID-19 symptoms and long COVID. JCI Insight 6:e152346. doi: 10.1172/jci.insight.152346
Harrison, S. L., Buckley, B. J. R., Rivera-Caravaca, J. M., Zhang, J., and Lip, G. Y. H. (2021). Cardiovascular risk factors, cardiovascular disease, and COVID-19: an umbrella review of systematic reviews. Eur. Hear J. – Qual. Care Clin. Outcomes 7, 330–339. doi: 10.1093/ehjqcco/qcab029
Hocková, B., Riad, A., Valky, J., Šulajová, Z., Stebel, A., Slávik, R., et al. (2021). Oral complications of ICU patients with COVID-19: case-series and review of two hundred ten cases. J. Clin. Med. 10, 1–13. doi: 10.3390/jcm10040581
Iebba, V., Zanotta, N., Campisciano, G., Zerbato, V., Di Bella, S., Cason, C., et al. (2021). Profiling of oral microbiota and cytokines in COVID-19 patients. Front. Microbiol. 12:1603. doi: 10.3389/fmicb.2021.671813
Kamel, A. H. M., Basuoni, A., Salem, Z. A., and AbuBakr, N. (2021). The impact of oral health status on COVID-19 severity, recovery period and C-reactive protein values. Br. Dent. J. 2021, 1–7. doi: 10.1038/s41415-021-2656-1
Larsson Wexell, C., Ryberg, H., Sjöberg Andersson, W. A., Blomqvist, S., Colin, P., Van Bocxlaer, J., et al. (2016). Antimicrobial effect of a single dose of amoxicillin on the oral microbiota. Clin. Implant. Dent. Relat. Res. 18, 699–706. doi: 10.1111/cid.12357
Li, X., Liu, Y., Yang, X., Li, C., and Song, Z. (2022). The oral microbiota: community composition, influencing factors, pathogenesis, and interventions. Front. Microbiol. 13:1491. doi: 10.3389/fmicb.2022.895537
Lloréns-Rico, V., Gregory, A. C., Van Weyenbergh, J., Jansen, S., Van Buyten, T., Qian, J., et al. (n.d.). Mechanical ventilation affects respiratory microbiome of COVID-19 patients and its 1 interactions with the host 2 3 chronic diseases and metabolism. Contag. Collab. 10:13. doi: 10.1101/2020.12.23.20248425
Luyt, C. E., Sahnoun, T., Gautier, M., Vidal, P., Burrel, S., Pineton de Chambrun, M., et al. (2020). Ventilator-associated pneumonia in patients with SARS-CoV-2-associated acute respiratory distress syndrome requiring ECMO: a retrospective cohort study. Ann. Intensive Care 10:158. doi: 10.1186/s13613-020-00775-4
Malicka, B., Skośkiewicz-Malinowska, K., and Kaczmarek, U. (2022). The impact of socioeconomic status, general health and oral health on health-related quality of life, oral health-related quality of life and mental health among polish older adults. BMC Geriatr. 22, 1–15. doi: 10.1186/s12877-021-02716-7
Marouf, N., Cai, W., Said, K. N., Daas, H., Diab, H., Chinta, V. R., et al. (2021). Association between periodontitis and severity of COVID-19 infection: a case–control study. J. Clin. Periodontol. 48, 483–491. doi: 10.1111/jcpe.13435
Marshall, J. C., Murthy, S., Diaz, J., Adhikari, N., Angus, D. C., Arabi, Y. M., et al. (2020). A minimal common outcome measure set for COVID-19 clinical research. Lancet Infectious Diseases, 20, e192–e197. doi: 10.1016/S1473-3099(20)30483-7
Menon, R. K., Gomez, A., Brandt, B. W., Leung, Y. Y., Gopinath, D., Watt, R. M., et al. (2019). Long-term impact of oral surgery with or without amoxicillin on the oral microbiome-a prospective cohort study. Sci. Rep. 9, 1–10. doi: 10.1038/s41598-019-55056-3
Miller, E. H., Annavajhala, M. K., Chong, A. M., Park, H., Nobel, Y. R., Soroush, A., et al. (2021). Oral microbiome alterations and SARS-CoV-2 saliva viral load in patients with COVID-19. Microbiol. Spectr. 9:e0005521. doi: 10.1128/Spectrum.00055-21
Monroy-Pérez, E., Rodríguez-Bedolla, R. M., Garzón, J., Vaca-Paniagua, F., Arturo-Rojas Jiménez, E., and Paniagua-Contreras, G. L. (2020). Marked virulence and azole resistance in Candida albicans isolated from patients with periodontal disease. Microb. Pathog. 148:104436. doi: 10.1016/j.micpath.2020.104436
Moraes, L. C., Lang, P. M., Arcanjo, R. A., Rampelotto, P. H., Fatturi-Parolo, C. C., Ferreira, M. B. C., et al. (2020). Microbial ecology and predicted metabolic pathways in various oral environments from patients with acute endodontic infections. Int. Endod. J. 53, 1603–1617. doi: 10.1111/iej.13389
Nel Van Zyl, K., Matukane, S. R., Hamman, B. L., Whitelaw, A. C., and Newton-Foot, M. (2022). Effect of antibiotics on the human microbiome: a systematic review. Int. J. Antimicrob. Agents 59:106502. doi: 10.1016/j.ijantimicag.2021.106502
Pérez-Chaparro, P. J., Gonçalves, C., Figueiredo, L. C., Faveri, M., Lobão, E., Tamashiro, N., et al. (2014). Newly identified pathogens associated with periodontitis: a systematic review. J. Dent. Res. 93, 846–858. doi: 10.1177/0022034514542468
Rafiqul Islam, S. M., Foysal, M. J., Hoque, M. N., Mehedi, H. M. H., Rob, M. A., Salauddin, A., et al. (2022). Dysbiosis of oral and gut microbiomes in SARS-CoV-2 infected patients in Bangladesh: elucidating the role of opportunistic gut microbes. Front. Med. 9:163. doi: 10.3389/fmed.2022.821777
Russo Fiorino, G., Maniglia, M., Marchese, V., Aprea, L., Torregrossa, M. V., Campisi, F., et al. (2021). Healthcare-associated infections over an eight year period in a large university hospital in Sicily (Italy, 2011–2018). J. Infect. Prev. 22, 220–230. doi: 10.1177/17571774211012448
Soffritti, I., D’Accolti, M., Fabbri, C., Passaro, A., Manfredini, R., Zuliani, G., et al. (2021). Oral microbiome Dysbiosis is associated with symptoms severity and local immune/inflammatory response in COVID-19 patients: a cross-sectional study. Front. Microbiol. 12:1397. doi: 10.3389/fmicb.2021.687513
Terezakis, E., Needleman, I., Kumar, N., Moles, D., and Agudo, E. (2011). The impact of hospitalization on oral health: a systematic review. J. Clin. Periodontol. 38, 628–636. doi: 10.1111/j.1600-051X.2011.01727.x
Terlecki, M., Wojciechowska, W., Klocek, M., Olszanecka, A., Stolarz-Skrzypek, K., Grodzicki, T., et al. (2021). Association between cardiovascular disease, cardiovascular drug therapy, and in-hospital outcomes in patients with COVID-19: data from a large single-center registry in Poland. Kardiol. Pol. 79, 773–780. doi: 10.33963/KP.15990
Thurnheer, T., and Belibasakis, G. N. (2014). Integration of non-oral bacteria into in vitro oral biofilms. Virulence 6, 258–264. doi: 10.4161/215055942014967608
Uehara, O., Abiko, Y., Nagasawa, T., Morikawa, T., Hiraki, D., Harada, F., et al. (2022). Alterations in the oral microbiome of individuals with a healthy oral environment following COVID-19 vaccination. BMC Oral Health 22, 1–9. doi: 10.1186/s12903-022-02093-6
Weiss, P., and Murdoch, D. R. (2020). Clinical course and mortality risk of severe COVID-19. Lancet 395, 1014–1015. doi: 10.1016/S0140-6736(20)30633-4
Weyand, N. J. (2017). Neisseria models of infection and persistence in the upper respiratory tract. Pathog Dis. 75. doi: 10.1093/femspd/ftx031
World Health Organization (2022). WHO COVID-19 dashboard. [online] World Health Organization. Available at: https://covid19.who.int/. [cited May 12, 2022].
Wozakowska-Kapłon, B., Włosowicz, M., Gorczyca-Michta, I., and Górska, R. (2013). Oral health status and the occurrence and clinical course of myocardial infarction in hospital phase: a case-control study. Cardiol. J. 20, 370–377. doi: 10.5603/CJ.2013.0095
Wu, Y., Cheng, X., Jiang, G., Tang, H., Ming, S., Tang, L., et al. (2021). Altered oral and gut microbiota and its association with SARS-CoV-2 viral load in COVID-19 patients during hospitalization. NPJ Biofilms Microbiomes 7, 1–9. doi: 10.1038/s41522-021-00232-5
Xu, X., He, J., Xue, J., Wang, Y., Li, K., Zhang, K., et al. (2015). Oral cavity contains distinct niches with dynamic microbial communities. Environ. Microbiol. 17, 699–710. doi: 10.1111/1462-2920.12502
Yoshino, A., Nakamura, Y., Irie, Y., Kitamura, T., Takata, T., Ishikura, H., et al. (2022). Oral health of COVID-19 patients using extracorporeal membrane oxygenation: a clinical study of 19 cases. J. Clin. Med. 11:42. doi: 10.3390/jcm11010042
Zaura, E., Brandt, B. W., de Mattos, M. J. T., Buijs, M. J., Caspers, M. P. M., Rashid, M. U., et al. (2015). Same exposure but two radically different responses to antibiotics: resilience of the salivary microbiome versus long-term microbial shifts in feces. MBio. 6:e01693-15. doi: 10.1128/mBio.01693-15
Zaura, E., Pappalardo, V. Y., Buijs, M. J., Volgenant, C. M. C., and Brandt, B. W. (2001). Optimizing the quality of clinical studies on oral microbiome: a practical guide for planning, performing, and reporting. Periodontol 2000 85, 210–236. doi: 10.1111/prd.12359
Zawadzki, P. J., Perkowski, K., Padzik, M., Mierzwińska-Nastalska, E., Szaflik, J. P., Conn, D. B., et al. (2017). Examination of Oral microbiota diversity in adults and older adults as an approach to prevent spread of risk factors for human infections. Biomed. Res. Int. 2017, 1–7. doi: 10.1155/2017/8106491
Zhang, Y., Wang, X., Li, H., Ni, C., Du, Z., and Yan, F. (2018). Human oral microbiota and its modulation for oral health. Biomed. Pharmacother. 99, 883–893. doi: 10.1016/j.biopha.2018.01.146
Zhu, N., Zhang, D., Wang, W., Li, X., Yang, B., Song, J., et al. (2020). A novel coronavirus from patients with pneumonia in China, 2019. N. Engl. J. Med. 382, 727–733. doi: 10.1056/NEJMoa2001017
Keywords: oral microbiota, dysbiosis, COVID-19, mechanical ventilation, ARDS
Citation: Gregorczyk-Maga I, Fiema M, Kania M, Kędzierska J, Jachowicz E, Romaniszyn D and Wójkowska-Mach J (2022) Cultivable oral bacteriota dysbiosis in mechanically ventilated COVID-19 patients. Front. Microbiol. 13:1013559. doi: 10.3389/fmicb.2022.1013559
Edited by:
George Grant, University of Aberdeen, United KingdomReviewed by:
Valerio Iebba, University of Trieste, ItalyStéphane Viennot, Université Claude Bernard Lyon 1, France
Copyright © 2022 Gregorczyk-Maga, Fiema, Kania, Kędzierska, Jachowicz, Romaniszyn and Wójkowska-Mach. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Michal Kania, bWljaC5rYW5pYUB1ai5lZHUucGw=
†ORCID: Iwona Gregorczyk-Maga https://orcid.org/0000-0002-1384-9439
Mateusz Fiema https://orcid.org/0000-0001-5453-6917
Michal Kania https://orcid.org/0000-0002-4288-1024
Estera Jachowicz https://orcid.org/0000-0002-1067-9964
Dorota Romaniszyn https://orcid.org/0000-0002-6964-4264
Jadwiga Wójkowska-Mach https://orcid.org/0000-0003-0756-1639