 Pavle Banović1,2†
Pavle Banović1,2† Adrian A. Díaz-Sánchez3†
Adrian A. Díaz-Sánchez3† Verica Simin4*†Angélique Foucault-Simonin5
Verica Simin4*†Angélique Foucault-Simonin5 Clemence Galon5
Clemence Galon5 Alejandra Wu-Chuang5Dragana Mijatović1
Alejandra Wu-Chuang5Dragana Mijatović1 Dasiel Obregón6
Dasiel Obregón6 Sara Moutailler5*
Sara Moutailler5* Alejandro Cabezas-Cruz5*
Alejandro Cabezas-Cruz5*
- 1Ambulance for Lyme Borreliosis and Other Tick-Borne Diseases, Department of Prevention of Rabies and Other Infectious Diseases, Pasteur Institute Novi Sad, Novi Sad, Serbia
- 2Department of Microbiology With Parasitology and Immunology, Faculty of Medicine in Novi Sad, University of Novi Sad, Novi Sad, Serbia
- 3Department of Biology, University of Saskatchewan, Saskatoon, SK, Canada
- 4Department for Microbiological & Other Diagnostics, Pasteur Institute Novi Sad, Novi Sad, Serbia
- 5ANSES, INRAE, Ecole Nationale Vétérinaire d’Alfort, UMR BIPAR, Laboratoire de Santé Animale, Maisons-Alfort, France
- 6School of Environmental Sciences, University of Guelph, Guelph, ON, Canada
Ticks carry numerous pathogens that, if transmitted, can cause disease in susceptible humans and animals. The present study describes our approach on how to investigate clinical presentations following tick bites in humans. To this aim, the occurrence of major tick-borne pathogens (TBPs) in human blood samples (n = 85) and the ticks collected (n = 93) from the same individuals were tested using an unbiased high-throughput pathogen detection microfluidic system. The clinical symptoms were characterized in enrolled patients. In patients with suspected TBP infection, serological assays were conducted to test for the presence of antibodies against specific TBPs. A field study based on One Health tenets was further designed to identify components of a potential chain of infection resulting in Rickettsia felis infection in one of the patients. Ticks species infesting humans were identified as Ixodes ricinus, Rhipicephalus sanguineus sensu lato (s.l.), Dermacentor reticulatus, and Haemaphysalis punctata. Five patients developed local skin lesions at the site of the tick bite including erythema migrans, local non-specific reactions, and cutaneous hypersensitivity reaction. Although Borrelia burgdorferi s.l., Babesia microti, Anaplasma phagocytophilum, and Candidatus Cryptoplasma sp. DNAs were detected in tick samples, different Rickettsia species were the most common TBPs identified in the ticks. The presence of TBPs such as Rickettsia helvetica, Rickettsia monacensis, Borrelia lusitaniae, Borrelia burgdorferi, Borrelia afzelii, A. phagocytophilum, and B. microti in ticks was further confirmed by DNA sequencing. Two of the patients with local skin lesions had IgG reactive against spotted fever group rickettsiae, while IgM specific to B. afzelii, Borrelia garinii, and Borrelia spielmanii were detected in the patient with erythema migrans. Although R. felis infection was detected in one human blood sample, none of the components of the potential chain of infection considered in this study tested positive to this pathogen either using direct pathogen detection in domestic dogs or xenodiagnosis in ticks collected from domestic cats. The combination of high-throughput screening of TBPs and One Health approaches might help characterize chains of infection leading to human infection by TBPs, as well as prevalence of emerging rickettsial pathogens in the Balkan region.
Introduction
Ticks (Ixodidae) are obligate blood-feeding ectoparasites of many animal hosts, including mammals, birds, and reptiles. Ticks are currently ranked second to mosquitoes as the most common arthropod vectors of disease-causing agents to humans and the first vector of vector-borne diseases (TBDs) for domestic animals worldwide, including bacterial, parasitic, and viral pathogens (de la Fuente et al., 2017). In recent decades, the global threat of emerging and/or re-emerging TBDs, along with a growing number of potential tick-borne pathogens (TBPs), has become a major problem for human and animal health (Madison-Antenucci et al., 2020). The expanding geographical distribution of several tick species caused by climate change, and anthropogenic influence on ecological systems and animal movements poses a risk of these TBDs expanding to new regions (Rosa et al., 2018). In central, western, and northern Europe, Ixodes ricinus, also known as the castor bean tick, is the most widespread tick species (de la Fuente et al., 2017; Rosa et al., 2018). This species has been frequently reported to infest humans and is (Milutinovic et al., 2008b) the main vector for a large variety of TBPs transmitted to both humans and animals. Other tick species, such as the ornate cow tick Dermacentor reticulatus, the red sheep tick Haemaphysalis punctata, and the brown dog tick Rhipicephalus sanguineus s.l., are also widely distributed across Europe where reports of tick bites by these species in human is increasing (Rubel et al., 2021).
Serbia, a country at the crossroads of central and southeastern Europe, is endemic for a great number of TBPs that comprise the most common vector-borne diseases in the Balkan Peninsula. Ixodes ricinus is the most common and widely distributed tick species in Serbia, where it is responsible for the transmission of Lyme borreliosis (Jovanovic et al., 2015; Berić et al., 2017; Banovic et al., 2021b), tick-borne encephalitis (Potkonjak et al., 2017; Banovic et al., 2021c), and rickettsiosis (Samardzic et al., 2008; Banovic et al., 2021a). The role of I. ricinus as a vector of human granulocytic anaplasmosis, human babesiosis, and tularemia has not yet been reported in Serbia. Lyme borreliosis, caused by spirochetes of the Borrelia burgdorferi sensu lato (s.l.) complex, is the most prevalent tick-borne zoonosis in Europe (Raileanu et al., 2017). To date, at least ten genospecies of B. burgdorferi s.l. complex have been described in I. ricinus, including B. burgdorferi sensu stricto (s.s.), B. afzelii, B. garinii, B. bavariensis, B. spielmanii, B. valaisiana, B. finlandensis, B. bissettii, B. carolinensis, and B. lusitaniae (Raileanu et al., 2017).
Data on the incidence and prevalence of human TBPs associated with I. ricinus are scarce in Serbia, despite being crucial to understanding the risk of human infection (Milutinovic et al., 2008a; Radulovic et al., 2011; Banovic et al., 2021b), partly because Lyme borreliosis is not a notifiable disease in Serbia. Several pathogenic and potentially pathogenic microorganisms were previously detected in I. ricinus removed from tick-infested individuals in Serbia (Banovic et al., 2021a,b,c). In addition, Borrelia spp. and R. felis DNA was detected in the blood of two patients who developed clinically manifested infection after tick removal (Banovic et al., 2021b). In order to gain further insights into possible relationships between emerging TBPs, clinical presentation and course following tick bites, the present study was aimed to investigate (i) the clinical symptoms observed after tick bites, and pathogen transmission in a human study group, (ii) the occurrence of major TBPs in human blood samples and the ticks collected from the same group, through a microfluidic-based high-throughput detection method, and (iii) the identification of potential chains of infection associated to TBP infection.
Materials and Methods
Ethics Statement
This study was approved by the ethical committee of Pasteur Institute Novi Sad (Ethical approval No. 03/2019) and conducted according to the Declaration of Helsinki and The Patient Rights Law of the Republic of Serbia. Written informed consent for publication of this clinical case report was obtained from all the patients. Household animals and their blood samples were handled in accordance with EU Directive 2010/63/EU on animal experimentation.
Patient Recruitment and Clinical Follow Up
In 2020, a total of 650 patients attended the medical consultation at the ‘Ambulance for Lyme borreliosis and other TBDs’ of the Pasteur Institute Novi Sad to report tick bites and tick-associated infections. Only patients that got at least one tick removed within 48 h from the moment of the visit to the institute (n = 195) were considered for inclusion in the study. Approval for inclusion in the study was obtained from 85 patients, with a response rate of 43.6% (85/195), accounting for 13.1% (85/650) of all patients seeking consultation. Patients were requested to visit the Pasteur Institute Novi Sad 2 weeks, 4 weeks, and 3 months after the first visit to undergo a clinical examination and follow up by a medical doctor in this medical institution. Patients were also requested to report to Pasteur Institute Novi Sad if they noticed any clinical symptoms and/or sign between the requested medical appointments. Six months after the first visit, the enrolled patients were contacted via telephone to check for the existence of any signs associated to late stages of tick-borne diseases (TBDs) (e.g., rickettsiosis or Lyme borreliosis). The clinical examination included observation of the skin in general and the skin at the tick bite site in particular. Elevation of body temperature, headache, muscle pain or itching sensation at the place of previous tick infestation, as well as development of cutaneous hypersensitivity reaction were also considered in the clinical examination. If the patients developed any of the abovementioned signs or symptoms, a more specific clinical diagnostic procedure was initiated.
Clinical Diagnosis of Tick-Borne Diseases
Diagnosis of tick-borne bacterial infection was conducted in accordance with the Guidelines of the European Society of Clinical Microbiology and Infectious Diseases guidelines (ESCMID) (Brouqui et al., 2004). Patients who developed expanding dermal redness with or without central clearing (erythema migrans) at the place of the tick bite, following incubation period of at least 72 h after the removal of the tick were clinically diagnosed with early stage Lyme borreliosis. Besides specific Lyme borreliosis manifestation (i.e., erythema migrans), other clinical signs of bacterial tick-borne infection such as development of eschare or itching redness at the site of previous tick infestation were also considered. Skin lesions that developed at the place of the tick bite after a minimum of 72 h were considered as non-specific conditions if their presentation was not matching with given case definitions of early stage Lyme borreliosis, anaplasmosis, tick-borne rickettsioses, or tularemia as described in Guidelines of ESCMID (i.e., cutaneous hypersensitive reaction and non-expanding persistent redness at the place of previous tick bite with or without itching sensation) (Brouqui et al., 2004). Patients who did not develop clinical signs related to TBD in the 6-month follow up period were considered as healthy and were discharged from the study. The molecular and serological analyses described under the Sections “Indirect Immunofluorescence and Immunoblot-Based Serological Analyses” and “Microfluidic Real-Time PCR” below were conducted solely for the retrospective confirmation of the clinical diagnosis.
Antibiotic and Symptomatic Treatment in Patients With Clinical Signs of Tick-Borne Diseases
Patients who presented any of the abovementioned signs (i.e., erythema migrans, eschare, and non-expanding persistent redness) or symptoms (i.e., itching sensation at the skin affected by lesion) related with bacterial TBD were prescribed an antibiotic therapy including doxycycline (100 mg, Dovicin®, Galenika AD, Serbia) twice per day for 10 days or amoxicillin (50 mg/kg, Hemofarm A.D., Serbia) divided in three doses per day for 14 days if patient was child. The case of cutaneous hypersensitive reaction was treated with oral administration of antihistamines. The molecular and serological analyses described below were not considered in any shape or form to inform the decision of therapeutic intervention.
Tick Collection and Morphological and Molecular Characterization
Majority of ticks were removed in local Community Health Center ambulances, while the rest were removed either in Pasteur Institute Novi Sad or by patient themselves. In the medical facilities, ticks were removed via tweezers by grasping the ticks as close to the skin as possible and pulling in upward direction. Patients most often used tweezers, but in some cases they removed ticks using only their fingers, or they picked up the tick after its spontaneous detachment. After tick removal, patients were instructed to keep it in plastic container and bring it to Pasteur Institute Novi Sad as soon as possible. Ticks attached to recruited patients were collected (n = 93) and taxonomically identified based on morphological features and according to standard taxonomic keys described previously (Estrada-Peña et al., 2004). Ticks were further characterized according to sex and life stage. Molecular identification of I. ricinus, the most common tick in Serbia, and Dermacentor reticulatus, were performed by microfluidic PCR including primers/probe ITS2 specific to each tick species as previously described (Michelet et al., 2014). Attachment time of collected ticks was assessed by anamnesis (i.e., information provided by the patient). When the patient was unsure about the time between the tick bite and its detection, the scutal and coxal indices were calculated and used to assess the tick feeding period as previously described (Gray et al., 2005). Attachment times of each tick were recorded. Collected ticks were placed in 70% ethanol and conserved at −80°C until DNA extraction.
Blood Sample Collection and Sera Extraction
After written informed consent was acquired from each patient or patient’s caretakers (in the case of underage individuals), 2 ml of blood was collected in BD Vacutainer® spray-coated K2EDTA tubes (BD, Oakville, CA, United States) for adults or using the BD Vacutainer® Safety-Lok™ system (BD, Oakville, CA, United States) for young patients. Blood samples were stored at −80°C until DNA extraction. Blood and tick samples were labeled to allow for a pairwise analysis of pathogen detection in ticks and humans. For serological analyses (see below), one blood sample (3 ml) was collected in patients who developed lesions suggestive of rickettsial disease or Lyme borreliosis at least 3 weeks after tick removal, using BD Vacutainer® SST™ Tubes (BD, Franklin Lakes, NJ, United States). Blood samples were allowed to clot at room temperature and, after centrifugation at 2000 × g for 10 min, the serum was extracted and stored at −80°C until further use.
DNA Extraction
Total DNA was extracted from blood using the Nucleospin Tissue kit (Macherey Nagel, Düren, Germany) according to the manufacturer’s instructions. Ticks were homogenized using a Precellys 24 lyser/homogenizer (Bertin Technologies, Montigny-le-Bretonneux, France) at 5,500 rpm for 20 s using 2.8 mm stainless steel beads in 180 μL of lysis buffer and 25 μL of Proteinase K from the Nucleospin Tissue kit (Macherey Nagel, Düren, Germany). Homogenates were incubated for 3 h at 56°C and DNA was extracted according to the manufacturer’s instructions. Purified DNA was eluted into 50 μL elution buffer and stored at −80°C until further processing.
DNA Pre-amplification for Microfluidic Real-Time PCR
To improve detection of pathogen DNA, total DNA was pre-amplified using the PreAmp Master Mix (Fluidigm, CA, United States) according to the manufacturer’s instructions. Primers targeting all pathogens (see next section) were pooled by combining an equal volume of each primer for a final concentration of 200 nM. The reaction was performed in a final volume of 5 μL containing 1 μL Perfecta Preamp 5X, 1.25 μL pooled primer mix, 1.5 μL distilled water and 1.25 μL DNA. The thermocycling program consisted of one cycle at 95°C for 2 min, 14 cycles at 95°C for 15 s and 4 min at 60°C. At the end of the cycling program, the reactions were diluted 1:10 in Milli-Q ultrapure water. All the pre-amplified DNA samples were stored at −20°C until needed.
Microfluidic Real-Time PCR
To detect major TBPs [27 bacterial species (B. burgdorferi s.s., B. garinii, B. afzelii, B. valaisiana, B. lusitaniae, B. spielmanii, B. bissettii, B. miyamotoi, Anaplasma marginale, Anaplasma platys, Anaplasma phagocytophilum, Anaplasma ovis, Anaplasma centrale, Anaplasma bovis, Ehrlichia canis, Neoehrlichia mikurensis, R. conorii, Rickettsia slovaca, Rickettsia massiliae, Rickettsia helvetica, Rickettsia aeschlimannii, R. felis, Bartonella henselae, Francisella tularensis, Francisella-like endosymbionts, Coxiella-like endosymbionts, and Coxiella burnetii), 7 parasite species (Babesia microti, Babesia canis, Babesia ovis, Babesia bovis, Babesia caballi, Babesia venatorum, and Babesia divergens), 5 bacterial genera (Borrelia, Anaplasma, Ehrlichia, Rickettsia, and Mycoplasma), 3 parasite taxa (Apicomplexa, Theileria, and Hepatozoon)], the BioMark™ real-time PCR system (Fluidigm, CA, United States) was used for high-throughput microfluidic real-time PCR amplification using 48.48 Dynamic Array™ IFC chips (Fluidigm, CA, United States). These chips dispense 48 PCR mixes and 48 samples into individual wells, after which on-chip microfluidics assemble real-time PCR reactions in individual chambers before thermal cycling, resulting in 2,304 individual reactions. Briefly, amplifications were performed using 6-carboxyfluorescein (FAM)- and black hole quencher (BHQ1)-labeled TaqMan probes with TaqMan Gene expression master mix according to the manufacturer’s instructions (Applied Biosystems, Courtaboeuf, France). PCR cycling included 2 min at 50°C, 10 min at 95°C, followed by 40 cycles of two-step amplification of 15 s at 95°C, and 1 min at 60°C. One negative water control was included per chip. To determine whether factors present in the sample could inhibit the PCR, Escherichia coli strain EDL933 DNA was added to each sample as an internal inhibition control, and primers and a probe specifically for the E. coli intimin gene (eae) were used. For more details regarding the development of this new high-throughput tool based on real-time microfluidic PCRs (test of sensitivity, specificity, and controls used), please see Michelet et al. (2014) and Grech-Angelini et al. (2020).
Validation of Microfluidic Real-Time PCR System Results by PCR and DNA Sequencing
In order to validate the microfluidic real-time PCR results, some positive samples to infectious agents were selected to undergo additional conventional and nested PCR assays using primers different from those of the BioMark™ system (Table 1; Regnery et al., 1991; Choi et al., 2005; Rar et al., 2005; Loh et al., 2016; Masatani et al., 2017). Amplicon sequencing was commissioned to Eurofins MWG Operon (Ebersberg, Germany) and sequences were assembled using the BioEdit software (Ibis Biosciences, Carlsbad, CA, United States). The final nucleotide sequences were analyzed to identify the sequenced microorganisms using the GenBank database through the Basic Local Alignment Sequence Tool (BLAST) search engine1 of the National Center for Biotechnology Information (NCBI; Bethesda, MD, United States). Nucleotide sequence data reported in the present study are available in the GenBank, EMBL and DDBJ databases under the accession numbers: MW901468-MW901476, MW901478-MW901482, MW900162, MW900163, MW900166, and MW900167.
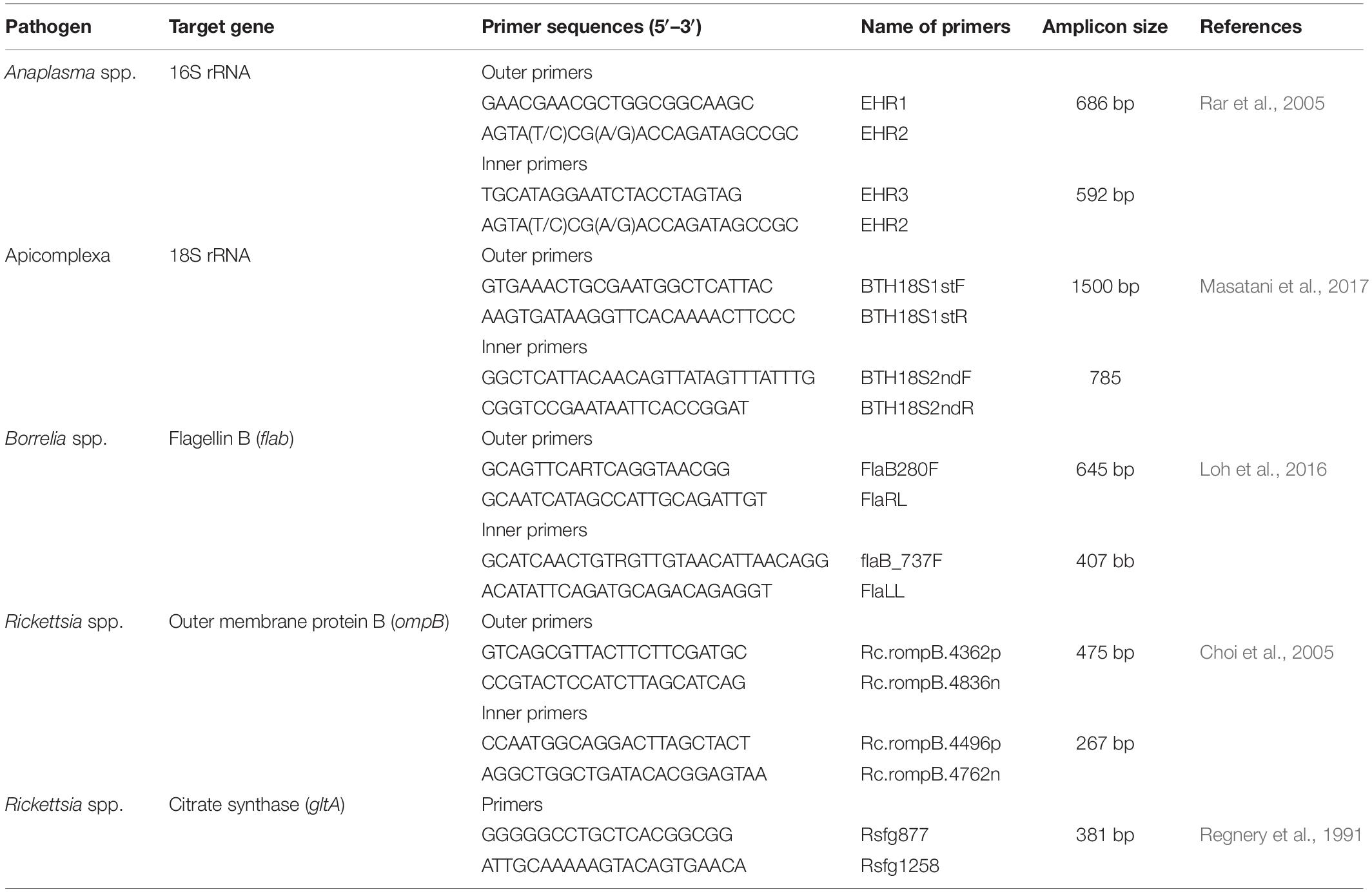
Table 1. Set of primers used to validate microfluidic real-time PCR results.
Indirect Immunofluorescence and Immunoblot-Based Serological Analyses
Serological analyses were performed only in sera samples of patients who developed lesions suggestive of rickettsial disease and/or Lyme borreliosis. The tests were conducted following serum inactivation at 56°C.
Reactivity of patients IgG to spotted fever group rickettsiae (SFGR) antigens was tested using a commercial indirect immunofluorescence (IFA) assay (Vircell, Spain, Ref. ‘PRICOG’), where Rickettsia conorii is used as the source of SFGR antigens. Since the assay was used in a qualitative manner to detect exposure (or not) to SFGR and/or SFGR-related microorganisms (e.g., R. felis), only one sera dilution was used without further sera titration. The cut-off dilution 1:40 was used, according to manufacturer instructions.
Borrelia seropositivity was evaluated via two-tier testing. First tier test consisted of anti-Borrelia IgM (Euroimmun AG, Germany, Cat. FI 2138-1010-2 M) and IgG (Euroimmun AG, Germany, Cat. FI 2138-1010-2 G) detection using commercial IFA assays. Visible fluorescence reactions using sera dilutions ≥1:10 for IgM and ≥1:100 for IgG were considered as positive in the IFA. Fluorescence was visualized using a microscope (Leica DM 3000, Wetzlar, Germany) with a mercury bulb light source and N2.1 filter (Leica, Wetzlar, Germany) with an excitation wavelength of 515–560 nm. Second tier test consisted in the detection of IgM and IgG specific to the proteins p100, VlsE, p58, p41 (flagellin), p39, OspA, four strain-specific OspC proteins (from B. burgdorferi s.s., B. afzelii, B. garinii and B. spielmanii) and five strain-specific p18 antigens (from B. burgdorferi s.s., B. afzelii, B. garinii, B. spielmanii and B. bavariensis) using a commercial immunoblot-based assay (recomLine Borrelia IgM/IgG, Mikrogen diagnostik, Germany, Cat. 4272 and 4273). First and second tier tests were performed and analyzed according to manufacturer instructions.
Field Studies to Identify Components of the Chain of Tick-Borne Pathogen Infection in Humans
If TBPs were detected in a patient’s blood, but not in the tick collected from that patient, a field study was organized to identify, and take samples from, components of a potential chain of infection including humans, domestic animals and ticks in defined locations were the patient could have been exposed to the detected pathogen. Collected samples were analyzed using microfluidic PCR. This approach follows the ‘One Health’ principle that health issues at the human-animal-environment interface are better understood when disease monitoring considers how diseases spread among people, animals, and the environment.
Statistical Analysis
The percentage (%) and 95% confidence interval (CI 95%) calculations were performed using GraphPad Prism v.8.0.1 (GraphPad Software Inc., La Jolla, CA, United States). Yates continuity correction as implemented in GraphPad Prism v.8.0.1 was applied to CI 95% calculations.
Results
Demographic Features of Tick-Infested Patients, Characterization of Collected Ticks and Assessment of Tick Attachment Time
A total of 85 patients with at least one tick attached were enrolled in the present study. Eighty-three (97.65%, 83/85) patients were from 27 municipalities in Serbia—mostly from the South Baèka district (59.03%, 49/83)—while two (2.35%, 2/85) patients were from the Kneževo and Mrkonjić Grad municipalities in the Banja Luka region of Bosnia and Herzegovina (Figure 1). Of the 85 patients, 80 (94.11%), 4 (4.70%), and 1 (1.18%) reported infestations with one, two, or five ticks, respectively. The ticks collected were morphologically identified to be four different species including I. ricinus (47 females, 34 nymphs, and 6 larvae), R. sanguineus s.l. (2 females and 1 male), D. reticulatus (2 females), and H. punctata (1 nymph), which were collected from 81, 3, 2, and 1 patient(s), respectively (Supplementary Table 1). The attachment time of the removed ticks were determined and resulted in the following distribution: <24 h (35.48%, 33/93), between 24 h and 48 h (26.88%, 25/93) and >72 h (31.18%, 29/93), while in 6.45% of ticks (6/93) the infestation period could not be assessed due to tick destruction during the removal process and inability of the patient to specify the moment of tick attachment. Most of the patients were between 25 and 50 years old (49.41%, 42/85), followed by patients between 50 and 75 (37.64%, 32/85) and patients less than 25 (11.76%, 10/85), while only one patient was older than 75 (1.17%, 1/85) (Supplementary Table 1).
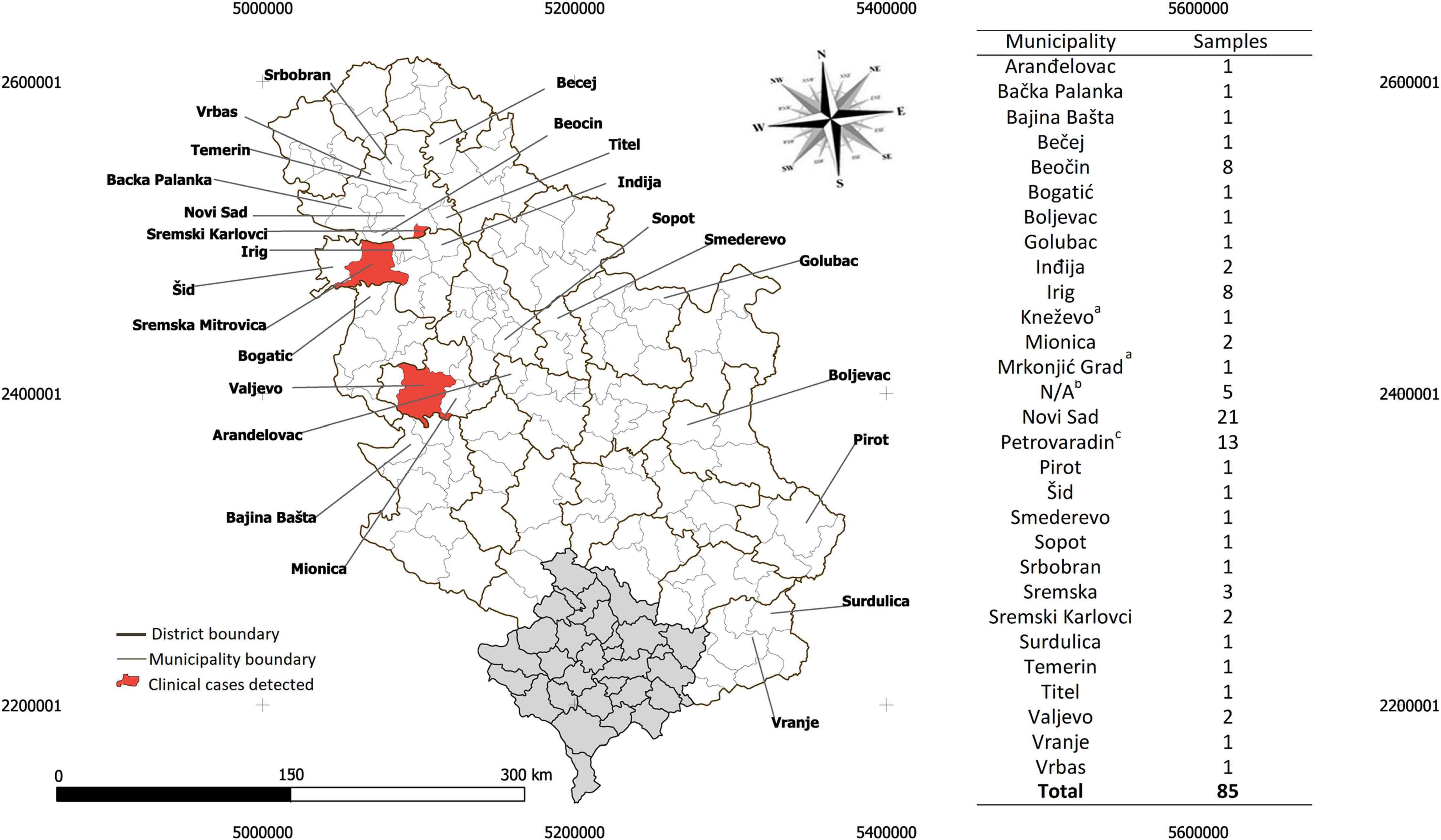
Figure 1. Geographical location of the patients infested by ticks in Serbia and enrolled in the study. The sample distribution is presented by municipalities, across the districts of Serbia (Supplementary Table 1). (‘a’) Two case studies from two municipalities in the neighboring country, Bosnia-Herzegovina, were labeled. (‘b’) Patients from Fruška Gora mountain with no specific municipality were labeled N/A. (‘c’) Petrovaradin is a small municipality adjacent to Novi Sad. The Serbian and Kosovo shapefile for mapping at district and municipality levels is available at the GADM database of Global Administrative Areas (v3.6, April 2020, https://gadm.org/). The map was generated using QGIS v3.12 (QGIS Development Team 2020).
Skin Lesions in Tick-Infested Individuals
Overall, five out of 85 (5.88%) enrolled patients developed at least one of the clinical signs considered (Table 2). Local skin lesions at the site of the tick bite were the most frequent clinical sign observed in the five patients. Among these, patient number 597/20 (1/85; 1.18%) was diagnosed as being in the first stage of Lyme borreliosis. Accordingly, erythema migrans was identified in patient number 597/20. Three other patients (3/85; 3.53%)—identified as 225/20, 370/20 and 374/20—developed local non-specific reactions, while patient 412/20 (1/85; 1.18%) developed cutaneous hypersensitivity reaction on multiple sites of both the most recent and previous tick infestations. Detailed clinical findings in each of these patients are described below.
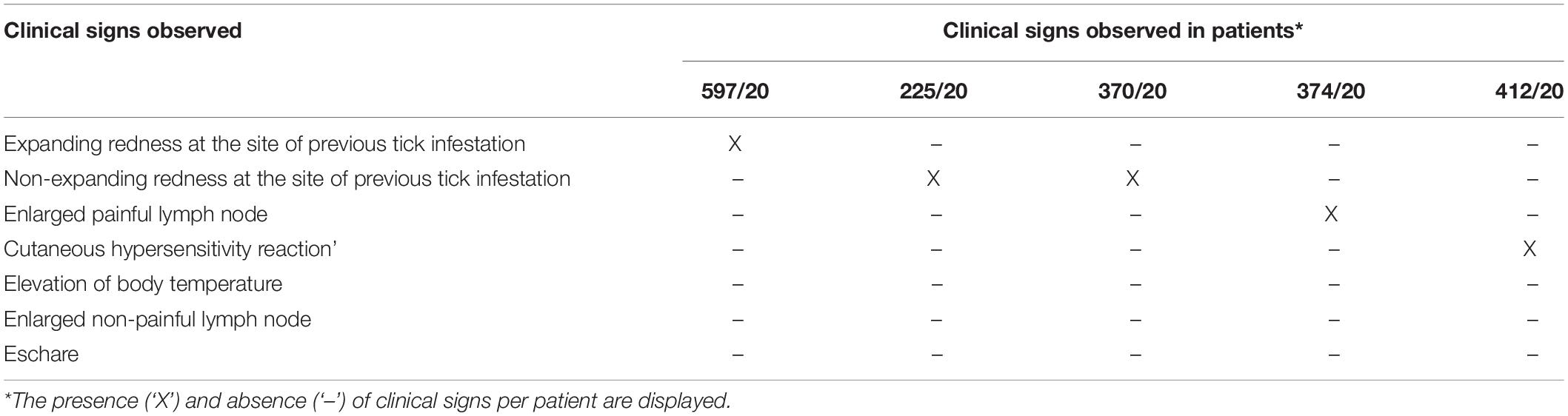
Table 2. Observed clinical signs.
Clinical Findings Associated With Lyme Borreliosis
Patient 597/20
On July 31st, 2020, a 6-year-old boy was admitted to the Pasteur Institute Novi Sad with a tick attached in the left retroaurical space. The tick was identified as an I. ricinus nymph, with an attachment period of approximately 72 h (Supplementary Table 1). As stated by the patient’s father, 3 days earlier they had outdoor activities in the mountainous area of Divèibare, Valjevo municipality (see Figure 1). Eight days later, the boy was admitted for a medical examination due to an expanding circular redness around the site of the tick bite. At the time of examination, the diameter of the lesion was approximately 5 cm and resembled an erythema migrans (Figure 2A). No additional signs of disease were noticed. The first-tier serological examination (see methods) revealed the presence of Borrelia-specific IgM (dilution 1:10) and IgG (dilution 1:100) in the patient’s serum. Anti-OspC IgM specific to B. afzelii, B. garinii and B. spielmanii and anti-p41 IgM and IgG were detected in the second-tier test. Oral amoxicillin 50 mg/kg (Hemofarm A.D., Serbia) t.i.d. treatment for 14 days was prescribed. The erythema migrans disappeared 14 days after starting the treatment. No additional signs of disease were noticed in the 2-month follow-up period.
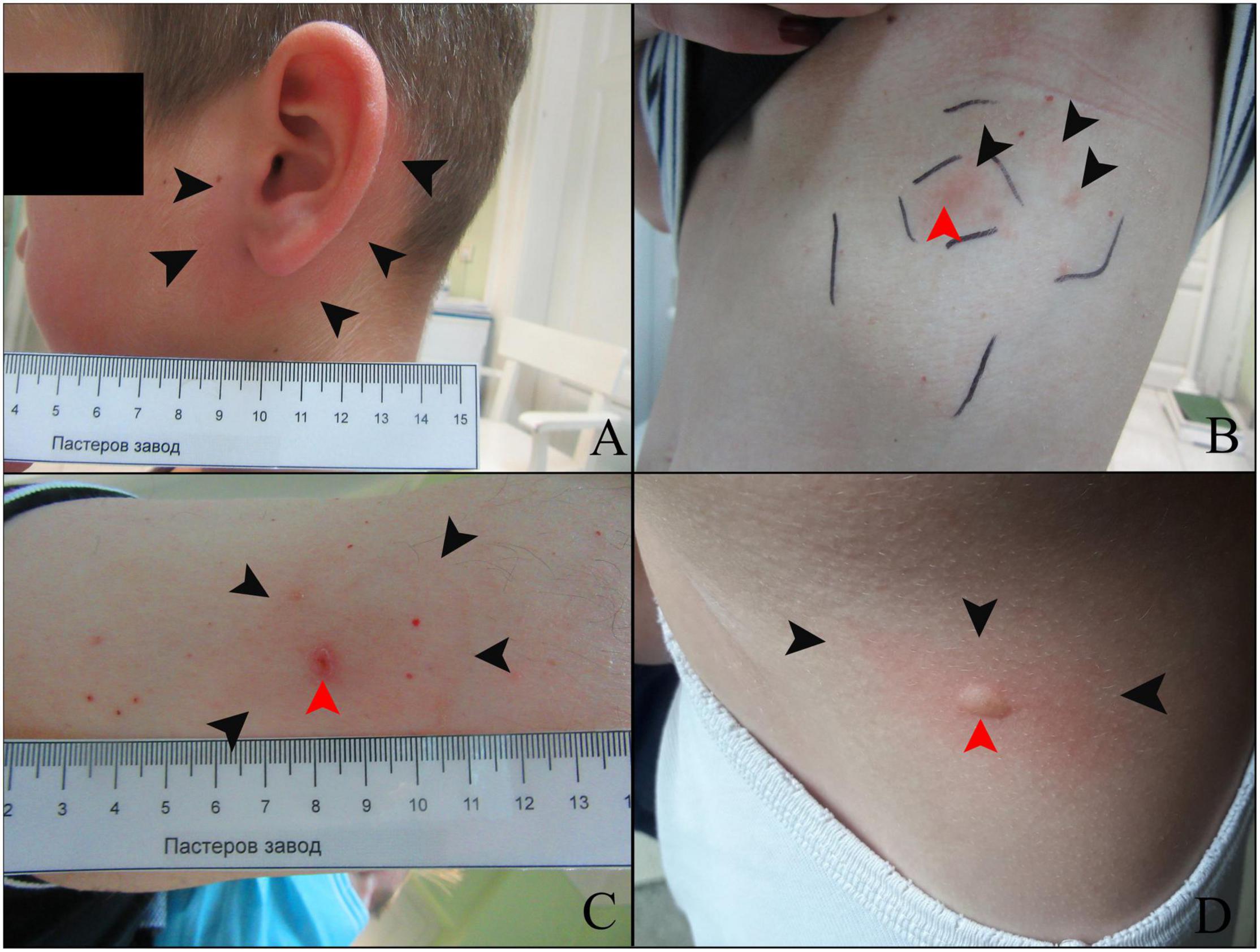
Figure 2. Skin lesions in patients infested with ticks. (A) Patient 597/20; black arrows point to the erythema migrans. (B) Patient 225/20; non-specific condition as consequence of tick bite encircled with outer and inner squares. Black arrows point to a non-specific focal redness, while the red arrow points to the site of the latest tick infestation. (C) Patient 370/20; black arrows point to a non-specific mild red lesion, while the red arrow points to the site of the latest tick infestation. (D) Patient 412/20; black arrows point to a reactive red area surrounding urtica (pointed to by a red arrow) at the site of a previous tick bite.
Cases of Local Non-specific Skin Reactions
Patient 225/20
On May 14th, 2020, a 43-year-old female arrived at the Pasteur Institute Novi Sad with a tick attached to her abdomen. The tick was identified as an I. ricinus nymph, with an attachment period of approximately 48 h (Supplementary Table 1). The patient recalled having visited Bešenovaèko Lake on the Fruška Gora Mountain (Sremska Mitrovica municipality, see Figure 1) in that time period. On the first scheduled medical examination (June 1st) the patient had no complaints and no signs of disease were noticed. Eight days later (26 days after tick removal), the patient was admitted with an oval-shaped red lesion with prominent macula at the site of the tick bite and several discrete red spots on the periphery of the lesion (Figure 2B). The main lesion was approximately 2 cm × 4 cm in diameter. No additional signs related to this condition were noticed. The lesion was encircled with a flat tip pen and the patient was advised to report immediately if it expanded outside the drawn borders (Figure 2B). No enlargement of inguinal lymph nodes was detected during a physical examination. Five days later (31 days after tick removal), the lesion was still present, but had not expanded. A treatment of oral doxycycline 100 mg (Dovicin, Galenika AD, Serbia) twice per day for 10 days was prescribed. The lesion disappeared during the course of antibiotic treatment and the patient made a complete recovery. The patient’s serum was not reactive to SFGR antigens.
Patient 370/20
On June 12th, 2020, a 57-year-old man visited the Pasteur Institute Novi Sad with a tick attached to his right upper arm. The tick was identified as an adult female I. ricinus with an approximate attachment period of 5 days. The patient recalled having a picnic the previous weekend in Sremski Karlovci village (Sremski Karlovci municipality, see Figure 1). Two weeks after tick removal, the patient reported to the medical service of the Pasteur Institute Novi Sad that he had an itching sensation and redness at the site of the tick bite. In addition, he reported sleep deprivation and tiredness. During the physical examination, a discrete circular erythematous lesion was observed reaching 4 cm in diameter (Figure 2C). The lesion’s surface was at the same level as the non-affected skin. Scratch marks were present in the same area, while a superficial lesion in the epidermis was noticed at the site of a previous tick infestation. No enlargement of axillar lymph nodes was detected during a physical examination. The red area was then encircled with a flat tip pen and the patient was advised to report immediately if the lesion expanded beyond the drawn borders. A week later, no expansion was observed. Despite no additional signs of disease being noticed, the patient’s sensation of tiredness persisted. Since discrete redness and itching persisted, a treatment of oral doxycycline 100 mg (Dovicin, Galenika AD, Serbia) twice per day for 10 days was prescribed. The patient reported that the itching sensation intensified after the first dose of doxycycline and disappeared completely the next day. The skin lesion disappeared during the course of antibiotic treatment and the patient made a complete recovery. The patient’s serum was reactive to SFGR antigens and non-reactive to Borrelia antigens on first tier serology assay.
Patient 374/20
On June 15th, 2020, a 74-year-old female visited the medical service of the Pasteur Institute Novi Sad with an adult female R. sanguineus s.l. tick attached to the occipital region of her scalp. The approximate attachment time was estimated to be 72 h (Supplementary Table 1). The patient could not recall any specific activities in that time period, but mentioned contact with her dogs in nearby Žabalj village (Žabalj municipality). A week later, she was admitted with an enlarged and very painful occipital lymph node. No enlargement of the neck and mandibular lymph nodes was detected during a physical examination. A treatment of oral doxycycline 100 mg (Dovicin, Galenika AD, Serbia) twice per day for 10 days was prescribed. The pain and lymph node both decreased during the course of antibiotic treatment and the patient made a complete recovery. The patient’s serum was reactive to SFGR antigens.
Case of Cutaneous Hypersensitivity Reaction
Patient 412/20
On June 16th, 2020, a 9-year-old girl was admitted with an I. ricinus larva attached to her left lower limb. The attachment period of the tick was estimated to be approximately 48 h. Fruška Gora Mountain (Letenka locality, Sremska Mitrovica municipality) was mentioned as the probable locality of tick aquisition. As stated by the parents, she had many tick infestations in previous years. Three weeks after tick removal, she visited the medical service of the Pasteur Institute Novi Sad with an itching sensation at the site of the last tick bite (tick included in this study) and of previous tick bites. The itching sensation was described as constant during the day but more intense during the night. During a physical examination, urticaria was noticed in several foci on the back (Figure 2D), shoulder and left lower limb at the site of the recent tick infestation. A treatment of oral loratadine 10 mg (Claritine, Schering-Plough Labo N.V., Belgium) once a day was prescribed. After 7 days, the lesions resolved and the patient made a complete recovery.
Tick-Borne Pathogens Identified in Ticks Collected From Humans
A total of 93 tick samples collected from enrolled patients were screened for TBP DNA using a high-throughput microfluidic real-time PCR assay. Of the 93 tick samples, 63 (67.74%; 95% CI: 58.06–77.42) were positive for at least one of the tested pathogens, while 35 (37.63%; 95% CI: 27.60–47.67) harbored a single infection, and 28 (30.11%; 95% CI: 20.61–39.61) were co-infected by up to five pathogens. PCR-positive results for the presence of TBPs were detected in I. ricinus (70.12%, 61/87, 38 females and 23 nymphs), followed by R. sanguineus s.l. (33.33%, 1/3, 1 female), and H. punctata (100%, 1/1, 1 nymph), while no TBPs were detected in the D. reticulatus ticks (2 females). DNA Rickettsia spp. was detected in 41/93 (44.09%; 95% CI: 33.81–54.37) tick samples, followed by Anaplasma/Ehrlichia spp. in 19/93 (20.43%; 95% CI: 12.08–28.78), and Borrelia spp. in 18/93 (19.35%; 95% CI: 11.17–27.54), while DNA of protozoan pathogens Babesia/Hepatozoon spp. was detected in 18/93 (19.35%; 95% CI: 11.17–27.54) tick samples. Overall, 16 different pathogens with variable prevalence were identified using species-specific primers. Rickettsia helvetica 31/93 (33.33%; 95% CI: 23.57–43.09) was the most common TBP detected in ticks, followed by Anaplasma phagocytophilum 9/93 (9.68%; 95% CI: 3.56–15.80), B. garinii 8/93 (8.60%; 95% CI: 2.80–14.41), B. afzelii 7/93 (7.53%; 95% CI: 2.06–12.99), B. spielmanii 5/93 (5.38%; 95% CI: 0.71–10.05), Rickettsia monacensis 5/93 (5.38%; 95% CI: 0.71–10.05), Rickettsia felis 4/93 (4.30%; 95% CI: 0.10–8.50), Borrelia miyamotoi 4/93 (4.30%; 95% CI: 0.10–8.50), Babesia microti 3/93 (3.23%; 95% CI: 0.0–6.88), B. lusitaniae 2/93 (2.15%; 95% CI: 0.0–5.15), and Babesia canis 2/93 (2.15%; 95% CI: 0.0–5.15), whereas Borrelia bissettii 1/93 (1.08%; 95% CI: 0.0–3.21), B. burgdorferi s.s. 1/93 (1.08%; 95% CI: 0.0–3.21), Babesia venatorum 1/93 (1.08%; 95% CI: 0.0–3.21), Neoehrlichia mikurensis 1/93 (1.08%; 95% CI: 0.0–3.21), and Hepatozoon spp. 1/93 (1.08%; 95% CI: 0.0–3.21) were detected in one tick each. The occurrence of single and co-infections with TBPs in ticks is summarized in Table 3.
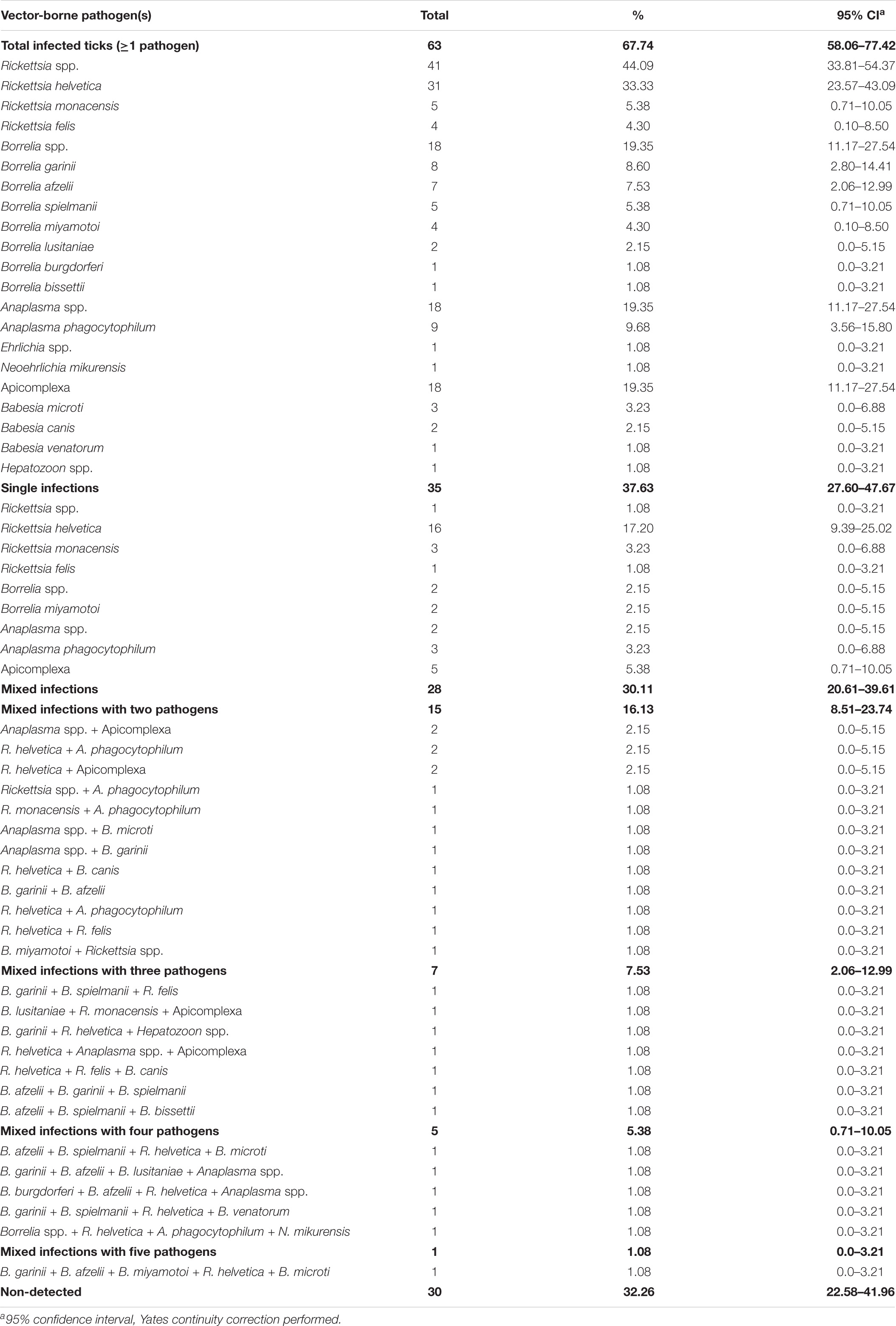
Table 3. Vector-borne pathogens detected in ticks from Serbia using microfluidic PCR.
The detection of R. helvetica, R. monacensis, B. lusitaniae, B. burgdorferi, B. afzelii, A. phagocytophilum, and B. microti was confirmed by sequencing fragments of outer-membrane protein (ompB) (Rickettsia spp.), flagellin (flaB) (Borrelia spp.), 18S rRNA (Babesia spp.), and 16S rRNA (Anaplasma spp.) genes in selected I. ricinus tick samples. All obtained nucleotide sequences showed >99% identity with reference strain sequences available in the GenBank database (Table 4). The sequencing analysis of the flaB nucleotide sequences confirmed the presence of B. afzelii, B. burgdorferi, and B. lusitaniae. In addition, the ompB nucleotide sequence confirmed the presence of R. helvetica and R. monacensis in ticks, while 16S rRNA and 18S rRNA nucleotide sequences confirmed the presence of A. phagocytophilum and Candidatus Cryptoplasma sp., and B. microti, respectively.
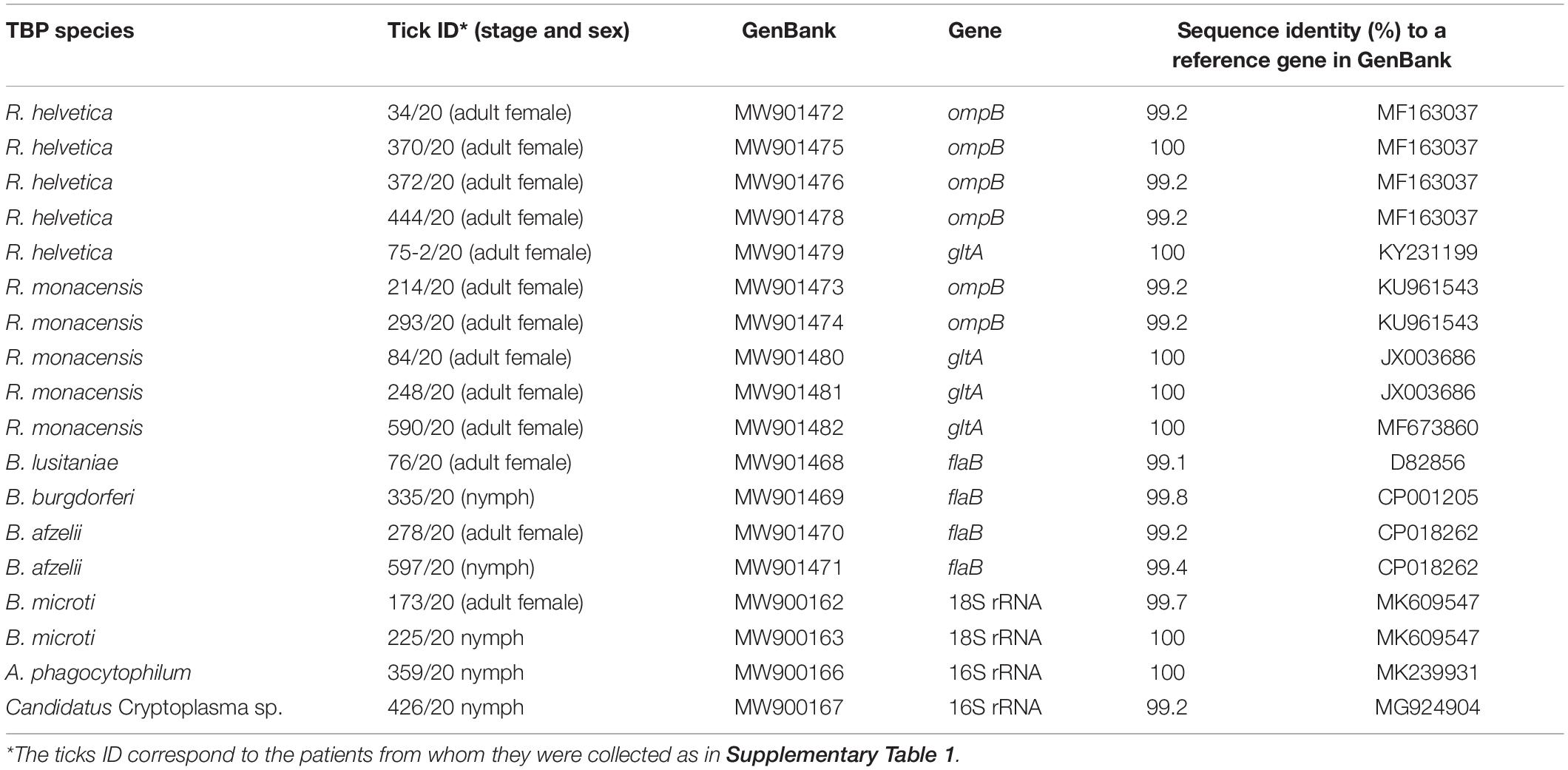
Table 4. Sequence analysis of genes in selected TBPs.
Tick-Borne Pathogens Identified in Ticks Collected From Humans With Skin Lesions
No TBPs were detected in the ticks collected from the patients who developed cutaneous hypersensitivity reaction (i.e., patient 412/20, I. ricinus, 1 larva) or lymph node enlargement with R. felis bacteremia (i.e., patient 374/20, R. sanguineus s.l., 1 female). The ticks collected from patients 370/20 (I. ricinus, 1 female), 225/20 (I. ricinus, 1 nymph), and 597/20 (I. ricinus, 1 nymph) tested positive for R. helvetica, Anaplasma spp. + B. microti, and B. afzelii + B. garinii + B. spielmanii infections, respectively. Three pathogens—B. microti, R. helvetica, and B. afzelii—identified in these ticks were selected for confirmation by sequencing (Table 4).
One Heath Approach to Search for Rickettsia felis in Components of a Potential Chain of Infection
Out of 85 human blood samples, only one (1.18%; 95% CI: 0.0–3.52) tested positive to TBPs. The sample collected from a patient 374/20 was PCR-positive for R. felis orfB and Rickettsia spp. gltA in the microfluidic system. The presence of R. felis was confirmed by sequencing a fragment of R. felis ompB nucleotide sequence (accession number MW901477), which had 99.25% identify with a R. felis ompB reference sequence available in GenBank (accession number MT358275). The tick removed from the skin of patient 374/20 was identified as an adult female R. sanguineus s.l. that was negative for the presence of any of the TBPs tested, including R. felis. In an attempt to identify the origin of this R. felis infection, a field study was organized to test for the presence of this bacterium in components of a potential chain of infection around patient 374/20.
Approximately 4 months after probable pathogen transmission, the patient was contacted and she referred two locations where the tick could have been acquired, one in Žabalj village (45.3730° N, 20.0634° E) and the other in the city of Novi Sad (45.2396° N, 19.8227° E). The patient reported having visited a weekend cottage with two hunting dogs in the Žabalj village before noticing the tick on her scalp. The patient also reported being in contact and petting nearly every day the cat of a neighbor located in the city of Novi Sad. Thus, blood samples were collected from the two dogs and, as we were not able to receive consent from the owner to take a blood sample from the cat, we used ticks collected from the cat as xenodiagnosis method for accessing the animal status as reservoir of vector-borne pathogens. During inspection of the dogs and cat, no fleas were observed on them and no tick was observed on the dogs. None of the dog blood samples tested positive for TBPs. Both ticks collected from the cat, identified as I. ricinus adult females (Supplementary Figure 1), were positive for A. phagocytophilum (confirmed by detection of Anaplasma spp. 16S rRNA and A. phagocytophilum msp2 in the microfluidic system) and R. helvetica (confirmed by detection of Rickettsia spp. gltA and R. helvetica 23S-5S internal transcribed spacer in the microfluidic system).
Discussion
In the present study conducted in Serbia in 2020, clinical examination of atypical TBDs was combined with high-throughput molecular diagnostics, pathogen-specific serological analysis, and field studies with the aim of providing further knowledge on clinical aspects, and on the range of TBD agents in ticks attached to enrolled patients. Clinical manifestations of TBDs were registered in five cases out of a total of 85 enrolled patients. While the majority of ticks were attached to the patients for less than 24 h, all the patients who developed clinical signs of a TBD were found to have had a tick attached for more than 48 h. This finding is in accordance with available data related to the increased ability of a competent tick vector to transmit TBPs when feeding over a longer period of time (Simo et al., 2017). The results based on molecular identification showed an overall infection prevalence of 68.82% with various TBPs among the four ixodid tick species analyzed, including I. ricinus, R. sanguineus s.l., D. reticulatus, and H. punctata, which is in accordance with the average prevalence reported in a recent study from Serbia (Banovic et al., 2021b). The most prevalent TBP found in ticks was Rickettsia spp., with the presence and confirmation of R. felis and the SFGR bacteria R. helvetica, and R. monacensis. The presence of the SFGR members mentioned above have been described in I. ricinus ticks collected from Serbia (Banovic et al., 2021b), as well as several Eastern European countries such as Hungary (Sreter-Lancz et al., 2005), Poland (Biernat et al., 2016), Romania, and Slovakia (Mitkova et al., 2015). Tick-borne rickettsiae are considered as potentially emerging and re-emerging pathogens which can simultaneously infect humans and result in a variety of non-specific clinical symptoms (Parola et al., 2005).
In Europe, human cases of R. helvetica infection have been described in Austria, Denmark, France, Italy, Slovakia, Sweden, and Switzerland by serology and/or molecular-based diagnostic assays (Parola et al., 2013). Although most of the R. helvetica cases reported subclinical or mild non-specific symptoms, its pathogenic potential has been described in patients from Sweden that developed a clinical picture characterized by an unexplained acute febrile illness, rash, and myasthenia, and one case was even associated with fatal perimyocarditis (Nilsson et al., 1999; Nilsson, 2009). In addition, the presence of R. monacensis was found in I. ricinus ticks. This SFGR was first identified almost 20 years ago in I. ricinus ticks collected from a city park in Germany, and has been described as an etiologic agent of Mediterranean Spotted Fever–like illness in Spain and Italy (Jado et al., 2007; Madeddu et al., 2012). Among the cases presented, patient number 370/20 had a local non-specific reaction, which could be associated with R. helvetica infection. For the purpose of differential diagnosis with other pathologic entities presented as redness at the site of the tick bite (mostly erythema migrans produced by Borrelia), it should be considered that the erythematous lesion of this patient was not expanding in the dynamic expected for a Borrelia infection and that the serum of this patient was non-reactive to Borrelia antigens on first tier serology assay. In addition, this patient was in chronic sleep deprivation, which could be associated with immune suppression (Besedovsky et al., 2012), which in turn may increase the susceptibility to infection by facultative TBPs such as R. helvetica. Although the itching sensation, one of this patient’s main symptoms, can be associated with erythema migrans induced by Borrelia infection, itching is not considered as a specific sign of any TBD. It is noteworthy that the itching reported by this patient intensified 10 days after the beginning of the doxycycline treatment, after which patient reached complete recovery. Further investigations should address whether itching could be considered as a sign of rickettsial presence in the lesion and if so, what is the diagnostic strength of that sign for practical use. One important factor to consider in this differential diagnosis is that the tick collected from patient 370/20 was negative to all Borrelia spp. tested, but positive to R. helvetica. In addition, the tick had an attachment period of 5 days that allows for rickettsial transmission and the serum sample from patient 370/20 was found to be reactive against SFGR, confirming exposure to SFGR member.
Another case described here as a non-specific condition associated with a tick bite is the hypersensitivity reaction in a 9-year-old girl (patient 412/20) with a confirmed history of earlier tick bites. Immediate and delayed cutaneous hypersensitivity reactions in humans at the site of a recent tick bite have been described by several authors (Beaudouin et al., 1997; Burke et al., 2005; Nakahigashi et al., 2013). It is considered that such reactions are part of acquired tick resistance (ATR) that can reduce the risk of pathogen transmission from pathogen-infected ticks to hosts (Cabezas-Cruz et al., 2021). These reactions were reported to be mediated by tick-specific IgE antibodies along with dermal and perivascular infiltrates of CD8+ T lymphocytes and Langerhans’ cells in two adult males from Europe (Beaudouin et al., 1997). In addition, the role of basophils in the allergic reactions associated with ATR was thought to occur after exposure to tick antigens such as carbohydrate Galα1-3Gal (α-Gal) (Nakahigashi et al., 2013; Cabezas-Cruz et al., 2021). Interestingly, the case described here is the first description of cutaneous hypersensitivity reactions at various different parts of the body, including the site of the most recent tick bite. Since ATR is considered to be a systemic rather than a localized immune response (Cabezas-Cruz et al., 2021), sensitized components of the immune system may be re-targeted to the sites of previous tick infestations. This is possibly due to the presence of remnants of the tick’s mouthparts previously encapsulated in skin following a foreign body reaction (Haddad et al., 2018). In this case, the patient’s symptoms were effectively treated with an antihistamine, so the etiology of this condition should be further investigated if symptoms re-appear following new tick bites.
Patient 374/20 was positive for R. felis infection by PCR diagnosis. This result was confirmed by DNA sequencing analysis. The physical examination of patient 374/20 revealed an enlarged and very painful occipital lymph node without an enlargement of the neck and mandibular lymph nodes. The occurrence of rickettsiae infections in human populations from different regions of Serbia has already been described (Samardzic et al., 2008), including the report of antibodies specific to Rickettsia typhi, Rickettsia akari, and Rickettsia conorii antigens in human sera (Samardzic et al., 2008). Furthermore, a previous study provided molecular evidence of the presence of an R. felis infection in a Serbian patient who developed local skin lesions at the site of a tick bite described as atypical erythema migrans (Banovic et al., 2021b). Interestingly, none of the tested TBPs, including R. felis, was detected in the R. sanguineus s.l. tick collected from patient 374/20, which suggests that the rickettsiae infection was not acquired from the R. sanguineus s.l. tick. Rickettsiosis in humans caused by R. felis is considered to be an emerging disease since R. felis is considered to be closely related to SFGR members (Lai et al., 2014), and is referred to as flea-borne spotted fever (FBSF), cat flea typhus or cat flea spotted fever, due to vector preference (Perez-Osorio et al., 2008). The clinical syndrome associated with FBSF includes several symptoms that range from non-specific flu-like illness (i.e., pyrexia, arthralgia, myalgia, headache, and fatigue) to severe multi-systemic disease accompanied by a maculopapular rash, due to widespread vasculitis (Maina et al., 2012). In this case, we have confirmed seroreactivity of patient sample to SFGR antigens. Knowing that anti-R. felis antibodies cross react with SFGR antigens (in this case R. conorii) (Lai et al., 2014), we concluded that detected seroreactivity is consequence of exposure to R. felis and not to R. conorii. The biological transmission of R. felis via competent ixodid tick vectors remains unclear to date. The analysis of the biological transmission of FBSF is further complicated by mounting evidence of the presence of this infectious agent in more than 40 species of fleas, ticks, mites, and mosquitoes (Brown and Macaluso, 2016). Considering that antibody cross-reactivity against SFGR/SFGR-related microorganism (R. felis) are known to be common, a limitation of the serological assay used here is that we only utilized R. conorii antigen for detection of exposure to SFGR member or R. felis (Fournier et al., 2002; Lai et al., 2014). Another limitation is that we did not used paired sera samples to confirm seroconversion or titer growth in tested patients (Nelder et al., 2020). Thus, this limitation can be easily explained if one considers that physicians are not able to know which patient is going to develop a disease at the time when tick is removed (Wood and Artsob, 2012). In addition, all sera samples were obtained during regular check-ups before or after therapy administration.
Based on the One Health tenets applied to TBDs (Banovic et al., 2021a), we designed a field study to identify R. felis infection in components of a potential chain of infection in the patient’s local environment. We hypothesized that infected domestic animals could be the source of R. felis infection in vectors that could transmit this pathogen to patient 374/20. We found no evidence of R. felis infection in the tested components of a potential epidemiologic chain. Although the ticks recovered from the cat could be from different area, one should keep in mind that tick sample was used here as a xenodiagnosis method for accessing the animal status as reservoir of vector-borne pathogens. Accordingly, if the animal is active reservoir for at least one of the tested pathogens, we expected them to be present in the tick feeding on that animal regardless of tick vector competence.
Babesia canis, B. microti, and B. venatorum (formerly Babesia sp. EU1) was detected in I. ricinus ticks collected from humans, although the overall prevalence was low. In Serbia, B. canis was previously identified in dogs and D. reticulatus ticks (Tomanović et al., 2013; Davitkov et al., 2015), while B. microti and B. venatorum were identified in questing I. ricinus (Potkonjak et al., 2016). Babesia microti has been described as the main etiologic agent of human babesiosis in the United States, while the B. venatorum genospecies is one of the main species causing human infections in Europe (Krause, 2019). Interestingly, marked differences have been reported in the epidemiology of B. microti since in the United States this is a well-known human pathogen, while in Europe its pathogenic potential remains unclear (Moniuszko-Malinowska et al., 2016). These differences amongst B. microti strains from the United States and Europe might be due (de la Fuente et al., 2017) to involvement of different tick species as competent vectors in the enzootic cycle of the pathogen (Krause, 2019; Madison-Antenucci et al., 2020) to the circulation of genetically diverse species as suggested by phylogenetic studies (Nakajima et al., 2009); and/or (Rosa et al., 2018) to the underestimation of actual prevalence in humans due to the occurrence of subclinical infections or coinfection with other TBPs such as A. phagocytophilum, B. burgdorferi s.l. complex, and Rickettsia spp. (Parija et al., 2015). Although B. venatorum infection rarely occurs in humans, it has been associated with mild clinical symptoms in patients from Austria, Belgium, Italy, and Germany (Herwaldt et al., 2003; Haselbarth et al., 2007; Lempereur et al., 2015). The human babesiosis cases associated with B. microti or B. venatorum infection are being given increased importance, since the clinical presentation of disease ranges from an asymptomatic form to a life-threatening infection characterized by severe hemolysis (Poisnel et al., 2013). Therefore, B. microti and B. venatorum herein reported in I. ricinus ticks should be considered among infectious hazards in the Republic of Serbia.
In this study, the presence of seven genospecies of the Borrelia genus, namely B. afzelii, B. bissettii, B. burgdorferi s.s., B. garinii, B. lusitaniae, B. spielmanii, and B. miyamotoi, was confirmed in I. ricinus ticks removed from human skin. Although a B. spielmanii infection has already been indirectly confirmed in a patient with erythema migrans (Banovic et al., 2019), we herein report the occurrence of B. bissettii and B. spielmanii in I. ricinus ticks for the first time in Serbia. Lyme borreliosis is the most common tick-borne zoonosis in Europe, where I. ricinus is the main vector for transmitting the causal agents belonging to B. burgdorferi s.l. complex (Sykes and Makiello, 2017). When the overall Borrelia prevalence found in the present study is compared to results of other similar studies in Serbia, we see wide variations between localities, ranging from 10 to 40.7% (Simin et al., 2020; Banovic et al., 2021b; Stosic et al., 2021). Compared to neighboring countries of Serbia, the Borrelia prevalence in ticks found in our study is higher compared to that of Croatia (Tadin et al., 2016), Bulgaria (Nader et al., 2018), and Romania (Kalmar et al., 2020). In contrast, Borrelia spp. infection in ticks reported here is lower than infection prevalence found in ticks removed from humans in Sarajevo city (Bosnia and Herzegovina) (Lasić et al., 2020). Interestingly, the clinical evidence and the detection of three Borrelia spp. in the tick attached to patient 597/20, as well as the presence of specific anti-OspC antibodies against same three species (i.e., B. afzelii + B. garinii + B. spielmanii) confirms that this patient had a mixed Borrelia infection. The patient was finally considered seroreactive only in IgM class, since the presence of anti-p41 (anti-flagellin) antibodies by itself has low diagnostic value. It is known that anti-flagellin antibodies can be generated after exposure to bacteria other than Borrelia (e.g., Helicobacter pylori and Escherichia coli), while anti-OspC antibodies are considered to be Borrelia-specific (Luft et al., 1993). The fact that patient did not reached seroconversion in IgG class is probably due to timely administration of antibiotic therapy. Another explanation would be that blood sample was acquired early and before specific anti-OspC IgG have reached detectable levels. Nevertheless, it should be mentioned that a limitation of this study is that serological tests were performed only in patients displaying specific clinical signs related to possible TBDs. For that reason, we were not able to assess the frequency of positive serological status suggesting asymptomatic or subclinical TBP infection in enrolled patients. This bias could be addressed in further studies where sera samples would be acquired from enrolled patients during the first (within 48 h after tick removal) and second (4 weeks after tick removal) examinations in order to detect seroconversion against TBPs in IgM and IgG. Additionally, the response rate below 50% (85 enrolled patients out of 195 who met the “case definition” criteria), may have represented an additional source of selection bias, with possible effects on results (e.g., positivity rates for TBPs) of the study.
In addition, the presence of A. phagocytophilum was only detected in I. ricinus ticks, with an infection prevalence similar to that previously described in Serbia (Tomanović et al., 2010; Banovic et al., 2021b). The presence of N. mikurensis was also detected in I. ricinus ticks which agree with a previous report from Serbia (Potkonjak et al., 2016). In Europe, the overall prevalence rates of N. mikurensis in I. ricinus ticks range from below 1% to over 20%, and its presence has been reported in countries neighboring Serbia such as Hungary (Tomanović et al., 2010), Romania (Kalmar et al., 2016), and Slovakia (Svitalkova et al., 2016). The pathogenic potential of N. mikurensis has already been described in febrile patients from Germany (von Loewenich et al., 2010), Switzerland (Maurer et al., 2013), France (Boyer et al., 2021) and Sweden (Welinder-Olsson et al., 2010). Interestingly, the analysis of Anaplasma spp. 16S rRNA sequences led to the identification of Candidatus Cryptoplasma sp. in an I. ricinus nymph, which is its first molecular report in Serbia. This bacterium of the family Anaplasmataceae has been described as being associated with infections in green lizards (Lacerta viridis) and their feeding on I. ricinus ticks in Slovakia (Kocikova et al., 2018). Although it has been suggested that reptiles such as lizards and snakes play a role as hosts for ixodid ticks, their role in maintaining tick-borne Anaplasmataceae bacteria in the environment has never been described. This finding should therefore be interpreted with caution since further studies are necessary to determine the enzootic maintenance and circulation of Candidatus Cryptoplasma sp. in Serbia. In this study, the overall prevalence of A. phagocytophilum, B. microti, B. venatorum, genospecies of the B. burgdorferi s.l. complex, N. mikurensis, and Candidatus Cryptoplasma sp. was relatively low, a finding that is in accordance with previous reports from neighboring countries, which suggests widespread distribution of these TBPs in the Balkan Peninsula.
Conclusion
Tick-infested humans are exposed to a diverse group of TBPs in Serbia. These pathogens include extracellular (i.e., Borrelia spp.), and intracellular bacteria (e.g., Rickettsia spp.) and hemoparasites (i.e., Babesia spp.). The frequency of detection of these microbes in ticks collected from the enrolled patients was unequal, Rickettsia spp. being the most common pathogen to which tick-infested humans could be exposed in Serbia. The observed health disorders associated with tick bites in humans were both infectious (cases 597/20, 370/20, and 374/20) and allergic (case 412/20), while etiology of condition recorded in patient 225/20 was possibly multifactorial. Additionally, here we presented two clinical cases caused by emerging pathogens, R. felis and R. helvetica. Although both were successfully treated, there is as great risk for them to be non-recognized by medical practitioners due to unawareness of their presence and clinical presentation. A surveillance system and joint network to facilitate rapid communication should be established to examine true prevalence and of diseases caused by emerging rickettsial pathogens in Serbia and nearby Balkan countries. The implementation of a One Health approach can be used to study the circulation of TBPs in human habitats, since a previous study conducted by Banovic et al. (2021a) showed that the active components of chains of infection are poorly characterized for TBPs affecting humans. The approach used in this study for pathogen detection led to the identification of unexpected pathogens. To the best of the authors’ knowledge, this is the first molecular evidence of the occurrence of B. bissettii, B. spielmanii, and Candidatus Cryptoplasma sp. in I. ricinus ticks feeding on humans in Serbia.
Data Availability Statement
During the study, we generated gene sequences that were submitted to GenBank. The accession number(s) of these sequences can be found in the article (Table 4).
Ethics Statement
The studies involving human participants were reviewed and approved by the Ethical Committee of Pasteur Institute Novi Sad (Ethical approval No. 03/2019). The patients/participants provided their written informed consent to participate in this study. Ethical review and approval was not required for the animal study because the household animals samples were collected and analyzed as part of public health intervention in order to detect possible disease spreading foci and to implement measures for pathogen control if needed. Household animals and their blood samples were handled in accordance with EU Directive 2010/63/EU on animal experimentation. Written informed consent for participation was not obtained from the owners because before any sample was collected from the animals, we consulted the owners and received their verbal approval to collect blood samples. Written informed consent was obtained from the individual(s), and minor(s)’ legal guardian/next of kin, for the publication of any potentially identifiable images or data included in this article.
Author Contributions
PB and AC-C contributed to the conceptualization. PB, DO, and SM contributed to the methodology. DM, VS, AF-S, CG, and AD-S contributed to the validation. AD-S, PB, AF-S, CG, AW-C, and DO contributed to the formal analysis. DM, VS, PB, and AF-S contributed to the investigation. PB, DM, AC-C, and SM contributed to the resources. PB and AW-C contributed to the data curation. AD-S, PB, and AC-C contributed to the writing—original draft preparation. PB, DO, AD-S, and AC-C contributed to the writing—review and editing. DO and PB contributed to the visualization. PB, SM, and AC-C contributed to the supervision. All authors have read and agreed to the published version of the manuscript.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
UMR BIPAR was supported by the French Government’s Investissement d’Avenir Program, Laboratoire d’Excellence “Integrative Biology of Emerging Infectious Diseases” (Grant No. ANR-10-LABX-62-IBEID). AW-C was supported by Programa Nacional de Becas de Postgrado en el Exterior “Don Carlos Antonio López” (Grant No. 205/2018).
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmicb.2021.797399/full#supplementary-material
Supplementary Figure 1 | Dorsal (on left) and ventral (on right) views of the two engorged Ixodes ricinus female ticks collected from the cat.
Supplementary Table 1 | Information about the geographic distribution and age of enrolled patients and ticks collected from the patients, including tick species, developmental stage, tick attachment time, and information on the integrity of the tick specimen after removal.
Footnotes
References
Banovic, P., Capo, I., Ogorelica, D., Vranjes, N., Simin, V., and Lalosevic, D. (2019). Mysterious path of Borrelia spielmanii: spreading without morphological alteration of collagen type I and IV. Future Microbiol. 14, 1469–1475. doi: 10.2217/fmb-2019-0217
Banovic, P., Diaz-Sanchez, A. A., Galon, C., Foucault-Simonin, A., Simin, V., Mijatovic, D., et al. (2021a). A One Health approach to study the circulation of tick-borne pathogens: a preliminary study. One Health 13:100270.
Banovic, P., Diaz-Sanchez, A. A., Galon, C., Simin, V., Mijatovic, D., Obregon, D., et al. (2021b). Humans infested with Ixodes ricinus are exposed to a diverse array of tick-borne pathogens in Serbia. Ticks Tick Borne Dis. 12:101609. doi: 10.1016/j.ttbdis.2020.101609
Banovic, P., Obregon, D., Mijatovic, D., Simin, V., Stankov, S., Budakov-Obradovic, Z., et al. (2021c). Tick-Borne encephalitis virus seropositivity among tick infested individuals in Serbia. Pathogens 10:301. doi: 10.3390/pathogens10030301
Beaudouin, E., Kanny, G., Guerin, B., Guerin, L., Plenat, F., and Moneret-Vautrin, D. A. (1997). Unusual manifestations of hypersensitivity after a tick bite: report of two cases. Ann. Allergy Asthma Immunol. 79, 43–46. doi: 10.1016/S1081-1206(10)63082-7
Berić, D. K., Molnar, T., Miković, M., and Savić, S. (2017). Lyme borreliosis in North Backa district. Arh. Vet. Med. 10, 81–94. doi: 10.46784/e-avm.v10i2.75
Besedovsky, L., Lange, T., and Born, J. (2012). Sleep and immune function. Pflugers Arch. 463, 121–137.
Biernat, B., Stanczak, J., Michalik, J., Sikora, B., and Cieniuch, S. (2016). Rickettsia helvetica and R. monacensis infections in immature Ixodes ricinus ticks derived from sylvatic passerine birds in west-central Poland. Parasitol. Res. 115, 3469–3477. doi: 10.1007/s00436-016-5110-6
Boyer, P. H., Baldinger, L., Degeilh, B., Wirth, X., Kamdem, C. M., Hansmann, Y., et al. (2021). The emerging tick-borne pathogen Neoehrlichia mikurensis: first French case series and vector epidemiology. Emerg. Microbes Infect. 10, 1731–1738. doi: 10.1080/22221751.2021.1973347
Brouqui, P., Bacellar, F., Baranton, G., Birtles, R., Bjoërsdorff, A., Blanco, J., et al. (2004). ESCMID study group on Coxiella, Anaplasma, rickettsia and Bartonella; European network for surveillance of tick-borne diseases. Guidelines for the diagnosis of tick-borne bacterial diseases in Europe. Clin. Microbiol. Infect. 10, 1108–1132.
Brown, L. D., and Macaluso, K. R. (2016). Rickettsia felis, an emerging Flea-Borne Rickettsiosis. Curr. Trop. Med. Rep. 3, 27–39.
Burke, G., Wikel, S. K., Spielman, A., Telford, S. R., McKay, K., Krause, P. J., et al. (2005). Hypersensitivity to ticks and Lyme disease risk. Emerg. Infect. Dis. 11, 36–41. doi: 10.3201/eid1101.040303
Cabezas-Cruz, A., Hodzic, A., Mateos-Hernandez, L., Contreras, M., and de la Fuente, J. (2021). Tick-human interactions: from allergic klendusity to the alpha-Gal syndrome. Biochem. J. 478, 1783–1794. doi: 10.1042/BCJ20200915
Choi, Y. J., Lee, S. H., Park, K. H., Koh, Y. S., Lee, K. H., Baik, H. S., et al. (2005). Evaluation of PCR-based assay for diagnosis of spotted fever group rickettsiosis in human serum samples. Clin. Diagn. Lab. Immunol. 12, 759–763.
Davitkov, D., Vucicevic, M., Stevanovic, J., Krstic, V., Tomanovic, S., Glavinic, U., et al. (2015). Clinical babesiosis and molecular identification of Babesia canis and Babesia gibsoni infections in dogs from Serbia. Acta Vet. Hung. 63, 199–208. doi: 10.1556/AVet.2015.017
de la Fuente, J., Antunes, S., Bonnet, S., Cabezas-Cruz, A., Domingos, A. G., Estrada-Pena, A., et al. (2017). Tick-Pathogen interactions and vector competence: identification of molecular drivers for Tick-Borne Diseases. Front. Cell. Infect. Microbiol. 7:114. doi: 10.3389/fcimb.2017.00114
Estrada-Peña, A., Bouattour, A., Camicas, J., and Walker, A. (2004). Ticks of Domestic Animals in the Mediterranean Region: A Guide to Identification of Species. Zaragoza: University of Zaragoza, 131.
Fournier, P. E., Jensenius, M., Laferl, H., Vene, S., and Raoult, D. (2002). Kinetics of antibody responses in Rickettsia africae and Rickettsia conorii infections. Clin. Diagn. Lab. Immunol. 9, 324–328.
Gray, J., Stanek, G., Kundi, M., and Kocianova, E. (2005). Dimensions of engorging Ixodes ricinus as a measure of feeding duration. Int. J. Med. Microbiol. 295, 567–572. doi: 10.1016/j.ijmm.2005.05.008
Grech-Angelini, S., Stachurski, F., Vayssier-Taussat, M., Devillers, E., Casabianca, F., Lancelot, R., et al. (2020). Tick-borne pathogens in ticks (Acari: Ixodidae) collected from various domestic and wild hosts in Corsica (France), a Mediterranean island environment. Transbound. Emerg. Dis. 67, 745–757. doi: 10.1111/tbed.13393
Haddad, V. Jr., Haddad, M. R., Santos, M., and Cardoso, J. L. C. (2018). Skin manifestations of tick bites in humans. An. Bras. Dermatol. 93, 251–255. doi: 10.1590/abd1806-4841.20186378
Haselbarth, K., Tenter, A. M., Brade, V., Krieger, G., and Hunfeld, K. P. (2007). First case of human babesiosis in Germany – Clinical presentation and molecular characterisation of the pathogen. Int. J. Med. Microbiol. 297, 197–204. doi: 10.1016/j.ijmm.2007.01.002
Herwaldt, B. L., Cacciò, S., Gherlinzoni, F., Aspöck, H., Slemenda, S. B., Piccaluga, P., et al. (2003). Molecular characterization of a non–Babesia divergens organism causing zoonotic babesiosis in Europe. Emerg. Infect. Dis. 9, 943. doi: 10.3201/eid0908.020748
Jado, I., Oteo, J. A., Aldamiz, M., Gil, H., Escudero, R., Ibarra, V., et al. (2007). Rickettsia monacensis and human disease, Spain. Emerg. Infect. Dis. 13, 1405–1407. doi: 10.3201/eid1309.060186
Jovanovic, D., Atanasievska, S., Protic-Djokic, V., Rakic, U., Lukac-Radoncic, E., and Ristanovic, E. (2015). Seroprevalence of Borrelia burgdorferi in occupationally exposed persons in the Belgrade area, Serbia. Braz. J. Microbiol. 46, 807–814. doi: 10.1590/S1517-838246320140698
Kalmar, Z., Dumitrache, M. O., D’Amico, G., Matei, I. A., Ionica, A. M., Gherman, C. M., et al. (2020). Multiple tick-borne pathogens in Ixodes ricinus ticks collected from humans in Romania. Pathogens 9:390. doi: 10.3390/pathogens9050390
Kalmar, Z., Sprong, H., Mihalca, A. D., Gherman, C. M., Dumitrache, M. O., Coipan, E. C., et al. (2016). Borrelia miyamotoi and Candidatus Neoehrlichia mikurensis in Ixodes ricinus ticks, Romania. Emerg. Infect. Dis. 22, 550–551.
Kocikova, B., Majlath, I., Vichova, B., Malinicova, L., Pristas, P., Connors, V. A., et al. (2018). Candidatus Cryptoplasma associated with green lizards and Ixodes ricinus ticks, Slovakia, 2004-2011. Emerg. Infect. Dis. 24, 2348–2351. doi: 10.3201/eid2412.161958
Lai, C. H., Chang, L. L., Lin, J. N., Tsai, K. H., Hung, Y. C., Kuo, L. L., et al. (2014). Human spotted fever group rickettsioses are underappreciated in southern Taiwan, particularly for the species closely-related to Rickettsia felis. PLoS One 9:e95810. doi: 10.1371/journal.pone.0095810
Lasić, L., Ušanović, L., Ćakić, S., Hanjalić, J., and Kalamujić Stroil, B. (2020). First molecular detection of Borrelia burgdorferi sensu lato in Ixodes ricinus ticks collected from humans in the Sarajevo Canton (Bosnia and Herzegovina). Syst. Appl. Acarol. 25, 169–172.
Lempereur, L., Shiels, B., Heyman, P., Moreau, E., Saegerman, C., Losson, B., et al. (2015). A retrospective serological survey on human babesiosis in Belgium. Clin. Microbiol. Infect. 21, 96.e1–e7. doi: 10.1016/j.cmi.2014.07.004
Loh, S. M., Gofton, A. W., Lo, N., Gillett, A., Ryan, U. M., Irwin, P. J., et al. (2016). Novel Borrelia species detected in echidna ticks, Bothriocroton concolor, in Australia. Parasit. Vectors 9:339. doi: 10.1186/s13071-016-1627-x
Luft, B. J., Dunn, J. J., Dattwyler, R. J., Gorgone, G., Gorevic, P. D., and Schubach, W. H. (1993). Cross-reactive antigenic domains of the flagellin protein of Borrelia burgdorferi. Res. Microbiol. 144, 251–257. doi: 10.1016/0923-2508(93)90009-q
Madeddu, G., Mancini, F., Caddeo, A., Ciervo, A., Babudieri, S., Maida, I., et al. (2012). Rickettsia monacensis as cause of Mediterranean spotted fever-like illness, Italy. Emerg. Infect. Dis. 18, 702–704. doi: 10.3201/eid1804.111583
Madison-Antenucci, S., Kramer, L. D., Gebhardt, L. L., and Kauffman, E. (2020). Emerging tick-borne diseases. Clin. Microbiol. Rev. 33:e00083-18.
Maina, A. N., Knobel, D. L., Jiang, J., Halliday, J., Feikin, D. R., Cleaveland, S., et al. (2012). Rickettsia felis infection in febrile patients, western Kenya, 2007-2010. Emerg. Infect. Dis. 18, 328–331. doi: 10.3201/eid1802.111372
Masatani, T., Hayashi, K., Andoh, M., Tateno, M., Endo, Y., Asada, M., et al. (2017). Detection and molecular characterization of Babesia, Theileria, and Hepatozoon species in hard ticks collected from Kagoshima, the southern region in Japan. Ticks Tick Borne Dis. 8, 581–587. doi: 10.1016/j.ttbdis.2017.03.007
Maurer, F. P., Keller, P. M., Beuret, C., Joha, C., Achermann, Y., Gubler, J., et al. (2013). Close geographic association of human neoehrlichiosis and tick populations carrying Candidatus Neoehrlichia mikurensis in eastern Switzerland. J. Clin. Microbiol. 51, 169–176. doi: 10.1128/JCM.01955-12
Michelet, L., Delannoy, S., Devillers, E., Umhang, G., Aspan, A., Juremalm, M., et al. (2014). High-throughput screening of tick-borne pathogens in Europe. Front. Cell. Infect. Microbiol. 4:103. doi: 10.3389/fcimb.2014.00103
Milutinovic, M., Radulovic, Z., and Tomanovic, S. (2008b). Assessment of the risk of contracting Lyme disease in areas with significant human presence. Arq. Bras. Med. Vet. Zootec. 60, 121–129. doi: 10.1590/s0102-09352008000100018
Milutinovic, M., Masuzawa, T., Tomanovic, S., Radulovic, Z., Fukui, T., and Okamoto, Y. (2008a). Borrelia burgdorferi sensu lato, Anaplasma phagocytophilum, Francisella tularensis and their co-infections in host-seeking Ixodes ricinus ticks collected in Serbia. Exp. Appl. Acarol. 45, 171–183. doi: 10.1007/s10493-008-9166-6
Mitkova, K., Berthova, L., Kaluz, S., Kazimirova, M., Burdova, L., and Kocianova, E. (2015). First detections of Rickettsia helvetica and R. monacensis in ectoparasitic mites (Laelapidae and Trombiculidae) infesting rodents in south-western Slovakia. Parasitol. Res. 114, 2465–2472. doi: 10.1007/s00436-015-4443-x
Moniuszko-Malinowska, A., Swiecicka, I., Dunaj, J., Zajkowska, J., Czupryna, P., Zambrowski, G., et al. (2016). Infection with Babesia microti in humans with non-specific symptoms in North East Poland. Infect. Dis. (Lond.) 48, 537–543. doi: 10.3109/23744235.2016.1164339
Nader, J., Krol, N., Pfeffer, M., Ohlendorf, V., Marklewitz, M., Drosten, C., et al. (2018). The diversity of tick-borne bacteria and parasites in ticks collected from the Strandja Nature Park in South-Eastern Bulgaria. Parasit. Vectors 11:165. doi: 10.1186/s13071-018-2721-z
Nakahigashi, K., Otsuka, A., Tomari, K., Miyachi, Y., and Kabashima, K. (2013). Evaluation of basophil infiltration into the skin lesions of tick bites. Case Rep. Dermatol. 5, 48–51. doi: 10.1159/000348650
Nakajima, R., Tsuji, M., Oda, K., Zamoto-Niikura, A., Wei, Q., Kawabuchi-Kurata, T., et al. (2009). Babesia microti-group parasites compared phylogenetically by complete sequencing of the CCTeta gene in 36 isolates. J. Vet. Med. Sci. 71, 55–68. doi: 10.1292/jvms.71.55
Nelder, M. P., Russell, C. B., Johnson, S., Li, Y., Cronin, K., Warshawsky, B., et al. (2020). Assessing human exposure to spotted fever and typhus group rickettsiae in Ontario, Canada (2013-2018): a retrospective, cross-sectional study. BMC Infect. Dis. 20:523. doi: 10.1186/s12879-020-05244-8
Nilsson, K. (2009). Septicaemia with Rickettsia helvetica in a patient with acute febrile illness, rash and myasthenia. J. Infect. 58, 79–82. doi: 10.1016/j.jinf.2008.06.005
Nilsson, K., Lindquist, O., and Pahlson, C. (1999). Association of Rickettsia helvetica with chronic perimyocarditis in sudden cardiac death. Lancet 354, 1169–1173. doi: 10.1016/S0140-6736(99)04093-3
Parija, S. C., Kp, D., and Venugopal, H. (2015). Diagnosis and management of human babesiosis. Trop. Parasitol. 5, 88–93. doi: 10.4103/2229-5070.162489
Parola, P., Paddock, C. D., and Raoult, D. (2005). Tick-borne rickettsioses around the world: emerging diseases challenging old concepts. Clin. Microbiol. Rev. 18, 719–756. doi: 10.1128/CMR.18.4.719-756.2005
Parola, P., Paddock, C. D., Socolovschi, C., Labruna, M. B., Mediannikov, O., Kernif, T., et al. (2013). Update on tick-borne rickettsioses around the world: a geographic approach. Clin. Microbiol. Rev. 26, 657–702. doi: 10.1128/CMR.00032-13
Perez-Osorio, C. E., Zavala-Velazquez, J. E., Arias Leon, J. J., and Zavala-Castro, J. E. (2008). Rickettsia felis as emergent global threat for humans. Emerg. Infect. Dis. 14, 1019–1023. doi: 10.3201/eid1407.071656
Poisnel, E., Ebbo, M., Berda-Haddad, Y., Faucher, B., Bernit, E., Carcy, B., et al. (2013). Babesia microti: an unusual travel-related disease. BMC Infect. Dis. 13:99. doi: 10.1186/1471-2334-13-99
Potkonjak, A., Gutierrez, R., Savic, S., Vracar, V., Nachum-Biala, Y., Jurisic, A., et al. (2016). Molecular detection of emerging tick-borne pathogens in Vojvodina, Serbia. Ticks Tick Borne Dis. 7, 199–203. doi: 10.1016/j.ttbdis.2015.10.007
Potkonjak, A., Petrovic, T., Ristanovic, E., Lalic, I., Vracar, V., Savic, S., et al. (2017). Molecular detection and serological evidence of Tick-Borne Encephalitis Virus in Serbia. Vector Borne Zoonotic Dis. 17, 813–820. doi: 10.1089/vbz.2017.2167
Radulovic, Z., Chochlakis, D., Tomanovic, S., Milutinovic, M., Tselentis, Y., and Psaroulaki, A. (2011). First detection of spotted fever group Rickettsiae in ticks in Serbia. Vector Borne Zoonotic Dis. 11, 111–115. doi: 10.1089/vbz.2009.0254
Raileanu, C., Moutailler, S., Pavel, I., Porea, D., Mihalca, A. D., Savuta, G., et al. (2017). Borrelia diversity and co-infection with other tick-borne pathogens in ticks. Front. Cell. Infect. Microbiol. 7:36. doi: 10.3389/fcimb.2017.00036
Rar, V. A., Fomenko, N. V., Dobrotvorsky, A. K., Livanova, N. N., Rudakova, S. A., Fedorov, E. G., et al. (2005). Tick-borne pathogen detection, Western Siberia, Russia. Emerg. Infect. Dis. 11, 1708–1715.
Regnery, R. L., Spruill, C. L., and Plikaytis, B. D. (1991). Genotypic identification of rickettsiae and estimation of intraspecies sequence divergence for portions of two rickettsial genes. J. Bacteriol. 173, 1576–1589. doi: 10.1128/jb.173.5.1576-1589.1991
Rosa, R., Andreo, V., Tagliapietra, V., Barakova, I., Arnoldi, D., Hauffe, H. C., et al. (2018). Effect of climate and land use on the spatio-temporal variability of Tick-Borne Bacteria in Europe. Int. J. Environ. Res. Public Health 15:732. doi: 10.3390/ijerph15040732
Rubel, F., Brugger, K., Chitimia-Dobler, L., Dautel, H., Meyer-Kayser, E., and Kahl, O. (2021). Atlas of ticks (Acari: Argasidae, Ixodidae) in Germany. Exp. Appl. Acarol. 84, 183–214. doi: 10.1007/s10493-021-00619-1
Samardzic, S., Marinkovic, T., Marinkovic, D., Djuricic, B., Ristanovic, E., Simovic, T., et al. (2008). Prevalence of antibodies to Rickettsiae in different regions of Serbia. Vector Borne Zoonotic Dis. 8, 219–224. doi: 10.1089/vbz.2007.0122
Simin, V., Lalošević, D., Mijatović, D., Tomanović, S., Miljević, M., Čabrilo, B., et al. (2020). Borellia burgdorferi infection in removed ticks and anti-borrelia antibodies in infested patients admitted to the Pasteur Institute, Novi Sad. Vet. Glas. 74, 164–177.
Simo, L., Kazimirova, M., Richardson, J., and Bonnet, S. I. (2017). The essential role of tick salivary Glands and Saliva in tick feeding and pathogen transmission. Front. Cell. Infect. Microbiol. 7:281. doi: 10.3389/fcimb.2017.00281
Sreter-Lancz, Z., Sreter, T., Szell, Z., and Egyed, L. (2005). Molecular evidence of Rickettsia helvetica and R. monacensis infections in Ixodes ricinus from Hungary. Ann. Trop. Med. Parasitol. 99, 325–330.
Stosic, M. Z., Tomanović, S., Sukara, R., Milošević, S., and Savic, S. (2021). Detection of Borrelia spirochetes in ticks with q16 real-time PCR. Arch. Vet. Med. 14, 85–98.
Svitalkova, Z. H., Harustiakova, D., Mahrikova, L., Mojsova, M., Berthova, L., Slovak, M., et al. (2016). Candidatus Neoehrlichia mikurensis in ticks and rodents from urban and natural habitats of South-Western Slovakia. Parasit. Vectors 9:2. doi: 10.1186/s13071-015-1287-2
Sykes, R. A., and Makiello, P. (2017). An estimate of Lyme borreliosis incidence in Western Europe. J. Public Health (Oxf.) 39, 74–81. doi: 10.1093/pubmed/fdw017
Szekeres, S., Claudia Coipan, E., Rigo, K., Majoros, G., Jahfari, S., Sprong, H., et al. (2015). Candidatus Neoehrlichia mikurensis and Anaplasma phagocytophilum in natural rodent and tick communities in Southern Hungary. Ticks Tick Borne Dis. 6, 111–116. doi: 10.1016/j.ttbdis.2014.10.004
Tadin, A., Tokarz, R., Markotic, A., Margaletic, J., Turk, N., Habus, J., et al. (2016). Molecular survey of zoonotic agents in rodents and other small mammals in Croatia. Am. J. Trop. Med. Hyg. 94, 466–473. doi: 10.4269/ajtmh.15-0517
Tomanović, S., Chochlakis, D., Radulovic, Z., Milutinovic, M., Cakic, S., Mihaljica, D., et al. (2013). Analysis of pathogen co-occurrence in host-seeking adult hard ticks from Serbia. Exp. Appl. Acarol. 59, 367–376. doi: 10.1007/s10493-012-9597-y
Tomanović, S., Radulović, Ž, Masuzawa, T., Milutinović, M., and Stanisavljević, L. (2010). Potential infectivity of Anaplasma phagocytophilum strains in Ixodes ricinus ticks from Serbia. Acta Vet. Hung. 58, 231–242.
von Loewenich, F. D., Geissdorfer, W., Disque, C., Matten, J., Schett, G., Sakka, S. G., et al. (2010). Detection of Candidatus Neoehrlichia mikurensis in two patients with severe febrile illnesses: evidence for a European sequence variant. J. Clin. Microbiol. 48, 2630–2635. doi: 10.1128/JCM.00588-10
Welinder-Olsson, C., Kjellin, E., Vaht, K., Jacobsson, S., and Wenneras, C. (2010). First case of human Candidatus Neoehrlichia mikurensis infection in a febrile patient with chronic lymphocytic leukemia. J. Clin. Microbiol. 48, 1956–1959. doi: 10.1128/jcm.02423-09
Keywords: ticks, tick-borne pathogens, coinfections, rickettsial pathogens, One Health
Citation: Banović P, Díaz-Sánchez AA, Simin V, Foucault-Simonin A, Galon C, Wu-Chuang A, Mijatović D, Obregón D, Moutailler S and Cabezas-Cruz A (2022) Clinical Aspects and Detection of Emerging Rickettsial Pathogens: A “One Health” Approach Study in Serbia, 2020. Front. Microbiol. 12:797399. doi: 10.3389/fmicb.2021.797399
Received: 18 October 2021; Accepted: 24 December 2021;
Published: 26 January 2022.
Edited by:
Antonio Battisti, Experimental Zooprophylactic Institute of the Lazio and Tuscany Regions (IZSLT), ItalyReviewed by:
Yuanzhi Wang, Shihezi University, ChinaKatarzyna Kubiak, University of Warmia and Mazury in Olsztyn, Poland
Copyright © 2022 Banović, Díaz-Sánchez, Simin, Foucault-Simonin, Galon, Wu-Chuang, Mijatović, Obregón, Moutailler and Cabezas-Cruz. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Alejandro Cabezas-Cruz, YWxlamFuZHJvLmNhYmV6YXNAdmV0LWFsZm9ydC5mcg==; Sara Moutailler, c2FyYS5tb3V0YWlsbGVyQGFuc2VzLmZy; Verica Simin, THVrZXRpYy5zQG10cy5ycw==
†These authors have contributed equally to this work