
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Microbiol., 03 November 2021
Sec. Infectious Agents and Disease
Volume 12 - 2021 | https://doi.org/10.3389/fmicb.2021.738894
 Adjoa Holali Ameyapoh1
Adjoa Holali Ameyapoh1 Gnatoulma Katawa1*
Gnatoulma Katawa1* Manuel Ritter2
Manuel Ritter2 Christèle Nguepou Tchopba1Pélagie Edlom Tchadié1Kathrin Arndts2Hélène E. Kamassa1Bassimtou Mazou1Oukoe M. Amessoudji1Akawulu N’djao3Sibabe Agoro4Celina Vogelbusch2
Christèle Nguepou Tchopba1Pélagie Edlom Tchadié1Kathrin Arndts2Hélène E. Kamassa1Bassimtou Mazou1Oukoe M. Amessoudji1Akawulu N’djao3Sibabe Agoro4Celina Vogelbusch2 Millicent A. Omondi5Malewe Kolou6
Millicent A. Omondi5Malewe Kolou6 Simplice D. Karou1
Simplice D. Karou1 William Horsnell5,7,8Achim Hoerauf2,9,10Yaovi Ameyapoh1
William Horsnell5,7,8Achim Hoerauf2,9,10Yaovi Ameyapoh1 Laura E. Layland2,9*
Laura E. Layland2,9*Female reproductive tract infections (FRTIs) have a huge impact on women’s health including their reproductive health in rural areas. Immunomodulation by helminth infections could influence the occurrence of FRTIs. This study aimed to investigate the association between FRTIs, hookworm infections, and sociodemographic factors in six rural areas of the central region of Togo. A semi-structured questionnaire was used to collect sociodemographical information, and parasitological assessments were used to diagnose helminth infections. Moreover, cytobacteriological examination of vaginal swabs was performed for the diagnosis of candidiasis and bacterial vaginosis (BV), and real-time PCR method was used to determine sexually transmitted infections (STIs). Finally, a logistic regression analysis was performed to assess the relationship and association of these factors to FRTIs. The prevalence of FRTIs was 82.3% including STIs (74.38%), BV (31.79%), and vulvovaginal candidiasis (9.85%). In detail, FRTIs were caused by bacteria such as Ureaplasma parvum (50%), Ureaplasma urealyticum (26.5%), and Mycoplasma hominis (17.5%) and viruses such us cytomegalovirus (5%) and human papilloma virus (HPV) (20%). No cases of Haemophilus ducreyi, Treponema pallidum, or varicella-zoster virus (VZV) were observed. Interestingly, women who had hookworm infections were at high risk of HPV. The use of condoms was a protective factor [adjusted odds ratio (aOR) = 0.23; 95% CI [0.11–0.51)], while the use of contraceptive methods was a risk factor [aOR = 2.49; 95% CI (1.19–5.19)] for STIs. The risk of BV was lower among participants who had more than four pregnancies [aOR = 0.27; 95% CI (0.11–0.65)]. Furthermore, women who had ever been paid for sexual intercourse were at high probability risk of vulvovaginal candidiasis [aOR = 16.92; 95% CI (1.46–196.48)]. This study highlighted risk factors associated with FRTIs, the control of which would help to reduce the incidence of these diseases. Health-care professionals could develop education and sensitization strategies based on these risk factors, and anti-hookworm treatment concepts may be taken into consideration to minimize the risk of HPV infections.
Female reproductive tract infections (FRTIs) have a high incidence among various gynecological diseases (Yan et al., 2018). FRTIs comprise (i) endogenous infection such as bacterial vaginosis (BV) and vulvovaginal candidiasis; (ii) sexually transmitted infections (STIs) such as syphilis, gonorrhea, and chlamydia; and (iii) iatrogenic infections (Moragianni et al., 2019). Worldwide, FRTIs are a major public health problem and affect predominantly young women (Torondel et al., 2018). It has been observed that the prevalence of these infections varies a lot between countries and even among regions belonging to the same country (Rabiu et al., 2010). Sequelae of untreated FRTIs affect the well-being of women, such as infertility, cervical cancer, ectopic pregnancy, stillbirth, and spontaneous abortion (Diadhiou et al., 2019). Interestingly, FRTIs seriously impact women in the Sub-Saharan African region causing around 85% infertility (Hussen et al., 2018). Helminth infections could expose the person to various infections, protect from auto-immune diseases, or decrease disease severity and influence vaccine efficacity (Moreau and Chauvin, 2010; Hartmann et al., 2019). Helminthic infections which are predominantly prevalent in Africa could therefore contribute to the establishment of infectious diseases (Arndts et al., 2015; Katawa et al., 2015; Ritter et al., 2018, 2019). The impact of helminthiasis on female reproductive health and associated diseases is widely documented. For instance, (i) Wuchereria bancrofti and Schistosoma haematobium infections were associated with an increased risk of HIV infection, and (ii) an increased prevalence of human papilloma virus (HPV) infection has been observed in the soil-transmitted helminths-endemic area of Peru (Chetty et al., 2020).
Both FRTIs and helminthic infections are co-endemic and have been shown to be highest in low- and middle-income countries (Chetty et al., 2020). Thus, this study was designed to investigate the association between FRTIs, hookworm infections, and sociodemographic factors in the central region of Togo.
This was a cross sectional study conducted in October 2019 in six villages of the central region of Togo, namely, Sakalaoudè, Tseve, Fazao, Sagbadai, Alheridè, and Kikimini. The sample size (367) was calculated using Schwartz formula n = Z2 P (1 - P)/d2 where Z, the accepted risk error, is 1.96; d, the precision, is 0.05; P, the prevalence. In the central region of Togo, the prevalence of STIs is estimated at 25% according to the socio-demographic survey of 2013–2014 (Enquête Démographique et de Santé du Togo 2013–2014, available online) (World Bank, 2017). So using these factors and the prevalence of 25%, the minimum sample size is 288. Therefore, 367 women, sexually active and premenopausal, aged between 18 and 56 years old, were enrolled. Pregnant and/or women positive for HIV were not included in this study. All participants gave their written consent to participate. This study was ethically approved by the “Comité de Bioéthique pour la Recherche en Santé (CBRS)” of the Togo Ministry of Health (N°26/2017/CBRS) and the Ethical Review Board of the University Hospital Bonn (Lfd. Nr. 273/16).
Sociodemographic and helminth infections were assessed as risk factors.
For sociodemographic risk factors, a pre-tested and semi-structured questionnaire was used to collect sociodemographical data. The questionnaire was validated during a pilot study (Katawa et al., 2021) and administered by a trained medical laboratory technician in French or in a local language. Then, the participants who agreed moved freely to the sampling sites with a ticket proving their participation in the study. The probable associated risk factors chosen for analysis included helminth status, age, marital situation, duration of relationship with current partner, level of education, monthly income, average length of menstruation, vaginal hygiene methods, use of objects for intimate cleansing, introduction of products in vagina, having sex during menstruation, number of pregnancies, outcome of the last pregnancy, use of contraception methods, alcohol consumption, tobacco consumption, having sexual relationships during last 6 months, use of condoms, number of sexual partners during lifetime, use of condoms during last sexual intercourse, partner’s HIV positivity, having multiple sexual partners, having a sexual partner who has other sexual partners, and having paid intercourses/sexual relationships. Parasitological assessment was performed for the diagnosis of helminth infections. The confidentiality was maintained by an anonymization number that was attributed to each participant.
For the diagnosis of helminth infections, stool, urine, and skin snips were collected. Using Kato Katz and urine sedimentation methods, helminths and S. haematobium eggs were determined in the stool and urine, respectively. In addition, two skin snips of 1–2 mm were taken from the left and right iliac crests using biopsy forceps. They were then incubated in 100 μl of NaCl (0.9%) in 96-well plates for 18–24 h at room temperature to detect the presence of Onchocerca volvulus microfilariae using microscopy.
FRTIs were defined base on the Nugent score (>6) and the vaginal pH (>5).
Vaginal swabs were collected by physicians for cytobacteriological examination using fresh vaginal swab smears for yeast screening and gram staining for evaluation of bacterial flora by the criteria of Nugent (BV screening).
One vaginal swab and one cervical swab were collected by physicians from each participant and stored in 1 ml of eNAT® medium (COPAN Italia S.P.A., Brescia, Italy). DNA was extracted using the Seegene Microlab Nimbus IVD automation (Seegene Inc., Seoul, South Korea) according to manufacturer’s instructions. Real-time PCR for 27 germs implicated in FRTIs and STIs was performed. Amplification was done on Bio-Rad CFX96 Real-time PCR System (Biorad) using the AllplexTM STI Essential Assay kit that allows the simultaneous detection and identification of seven pathogens: Chlamydia trachomatis, Mycoplasma genitalium, Mycoplasma hominis, Neisseria gonorrhoeae, Trichomonas vaginalis, Ureaplasma parvum, and Ureaplasma urealyticum; the Allplex Genital Ulcer Assay kit that allows the detection of six pathogens: Cytomegalovirus (CMV), Haemophilus ducreyi, herpes simplex virus type 1 (HSV1), herpes simplex virus type 2 (HSV2), Treponema pallidum, and varicella-zoster virus (VZV); and the Anyplex II HPV HR detection kit that allows the detection of HPV infection. All reagents used for DNA extraction and FRTIs diagnosis were manufactured by Seegene Inc. (Seoul, Republic of Korea).
SPSS software (IBM SPSS Statistics 21; Armonk, NY) and GraphPad PRISM software 5.2 for Windows (GraphPap software, Inc., La Jolla, United States) were used to perform statistical analysis. Chi-square test was used to assess the prevalence differences (p-value threshold 0.05). Univariate and multivariate logistic regression analyses were used in order to investigate the risk factors associated with STIs, HPV, BV, and candidiasis including the calculation of odds ratios (OR) with 80% confidence intervals (CI) and adjusted odds ratios (aOR) with 95% CI. A threshold of p-value < 0.2 and < 0.05 were considered for univariate and multivariate analyses, respectively, and we declared the significance of OR/aOR if the value “1” is not included in the CI.
The overall prevalence of FRTIs among women of the Central region of Togo was 82.3% (Figure 1). Considering the prevalence per village, we found a high prevalence at Sakalahoudè (64.29%) and Tcheve (50%).
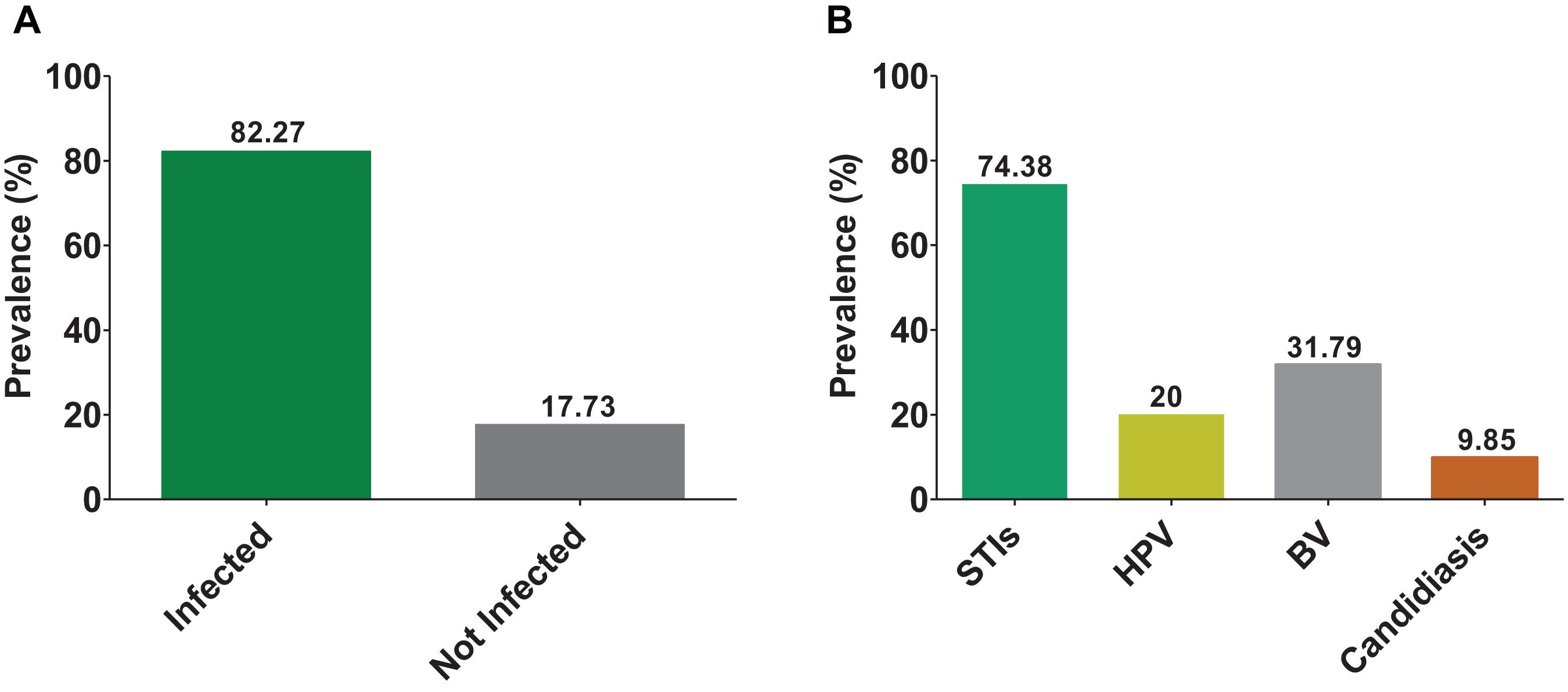
Figure 1. Prevalence of FRTIs. The bars indicate the prevalence of infected and non-infected (A); and sexually transmitted infections (STI without HPV), human papilloma virus (HPV), bacterial vaginosis (BV), and candidiasis (B).
Among all FRTIs screened, STIs were more prevalent (74.38%) than BV (31.79%) and candidiasis (9.85%) (Figure 1). The most infections implicated in STIs were caused by U. parvum (50% of women infected), followed by U. urealyticum (26.5%) and M. hominis (17.5%) (Figure 2). Viral infections detected included: HPV (20%) and CMV (5%). There were no cases of H. ducreyi, T. pallidum, or VZV. The prevalence of FRTIs in our study area was elevated with the predominance of hookworm infections. Therefore, we investigated the association between FRTIs and hookworm infections.
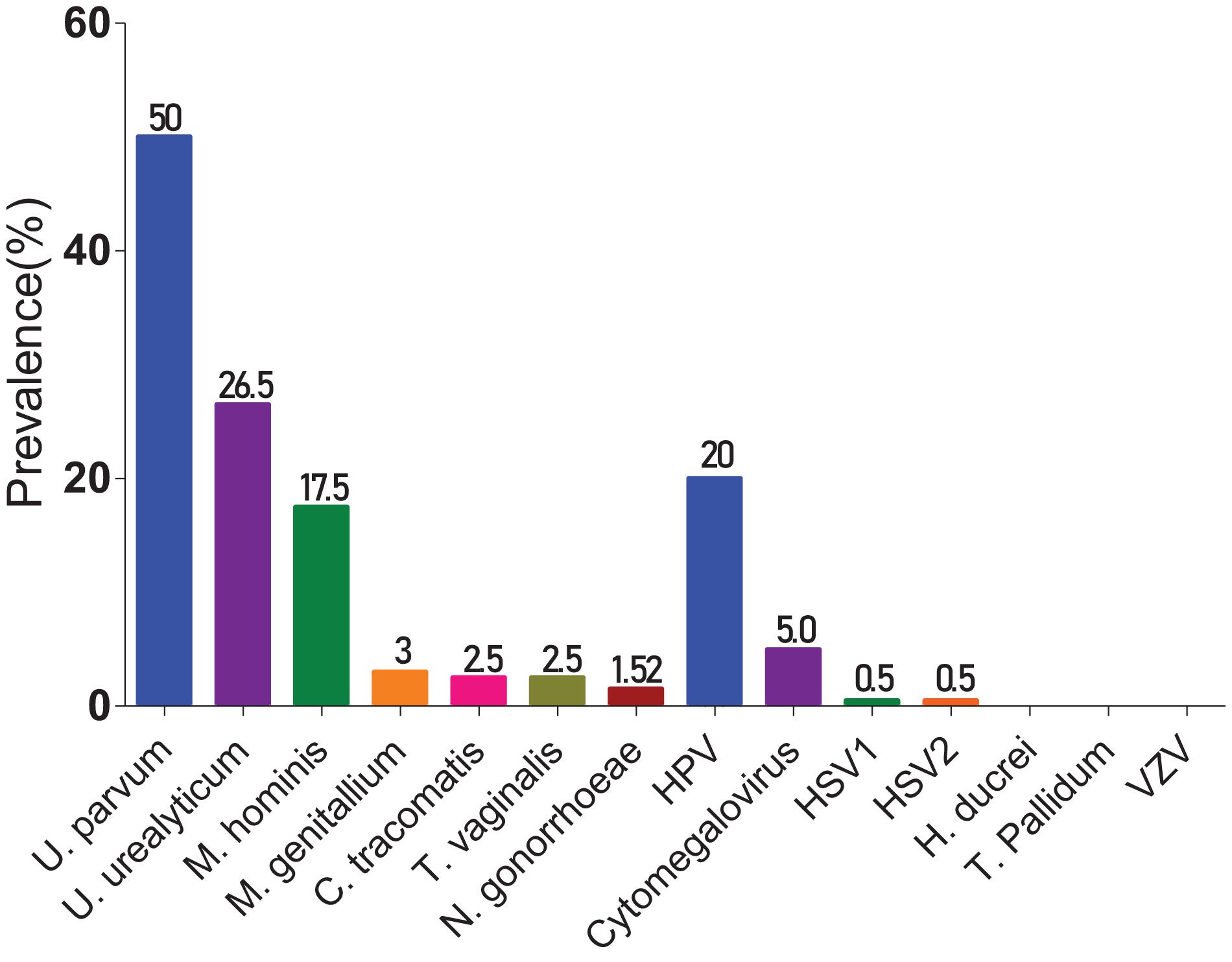
Figure 2. Prevalence of germs responsible for STIs. The bars indicate the prevalence of each germ involved in STIs.
The overall prevalence of helminth infection in the central region of Togo was 21.18% (Figure 3). Helminthiases were most prevalent in Sagbadahi (93.55%), Sakalahoudè (92.86%), Tcheve (88.89%), and Kikimini/Aleheridè (80.39%) (Figure 4).
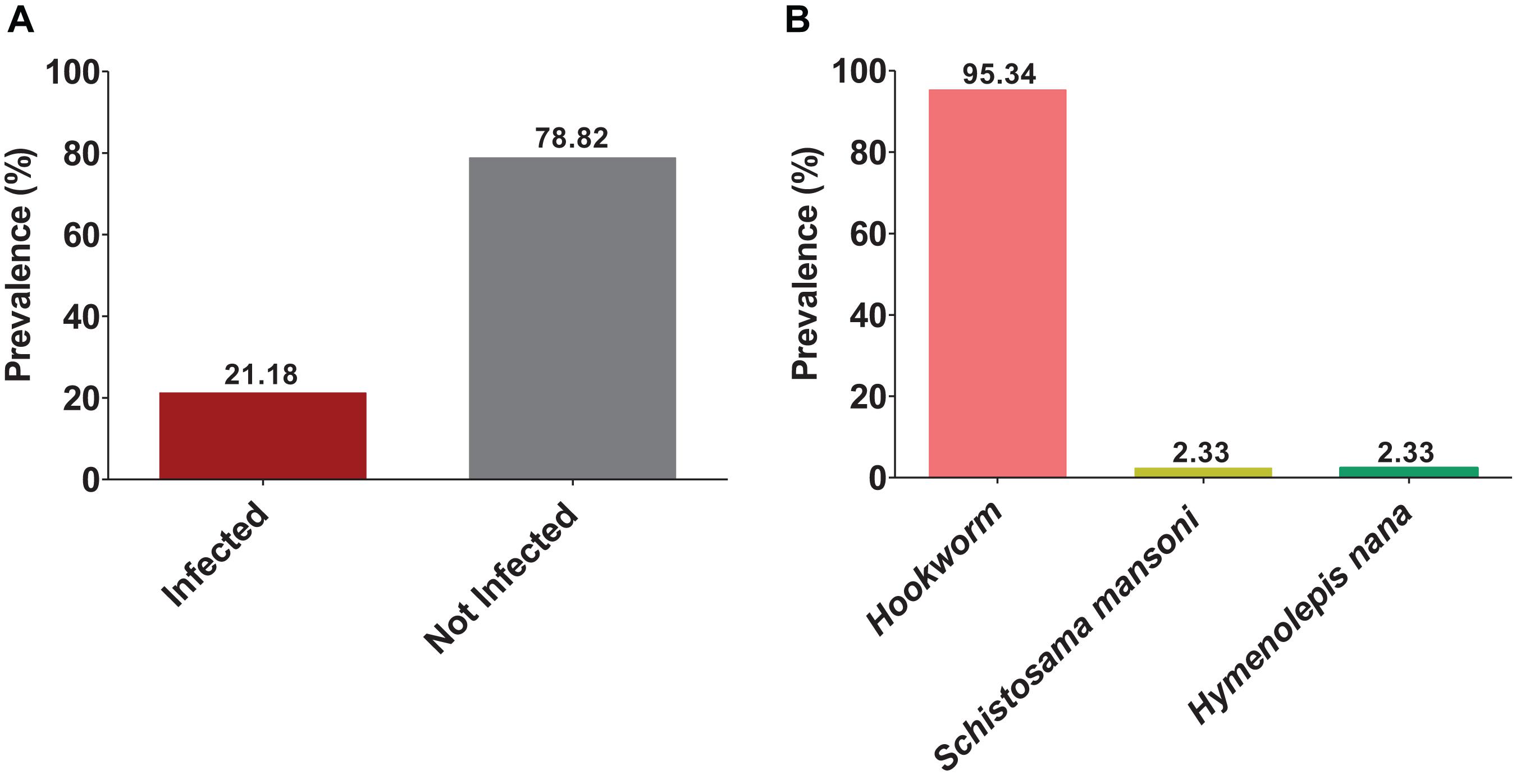
Figure 3. Prevalence of helminthiasis. The bars indicate the prevalence of infected and non-infected (A). Prevalence of each species found on the cohort: hookworm, Schistosoma mansoni, and Hymenolepis nana (B).
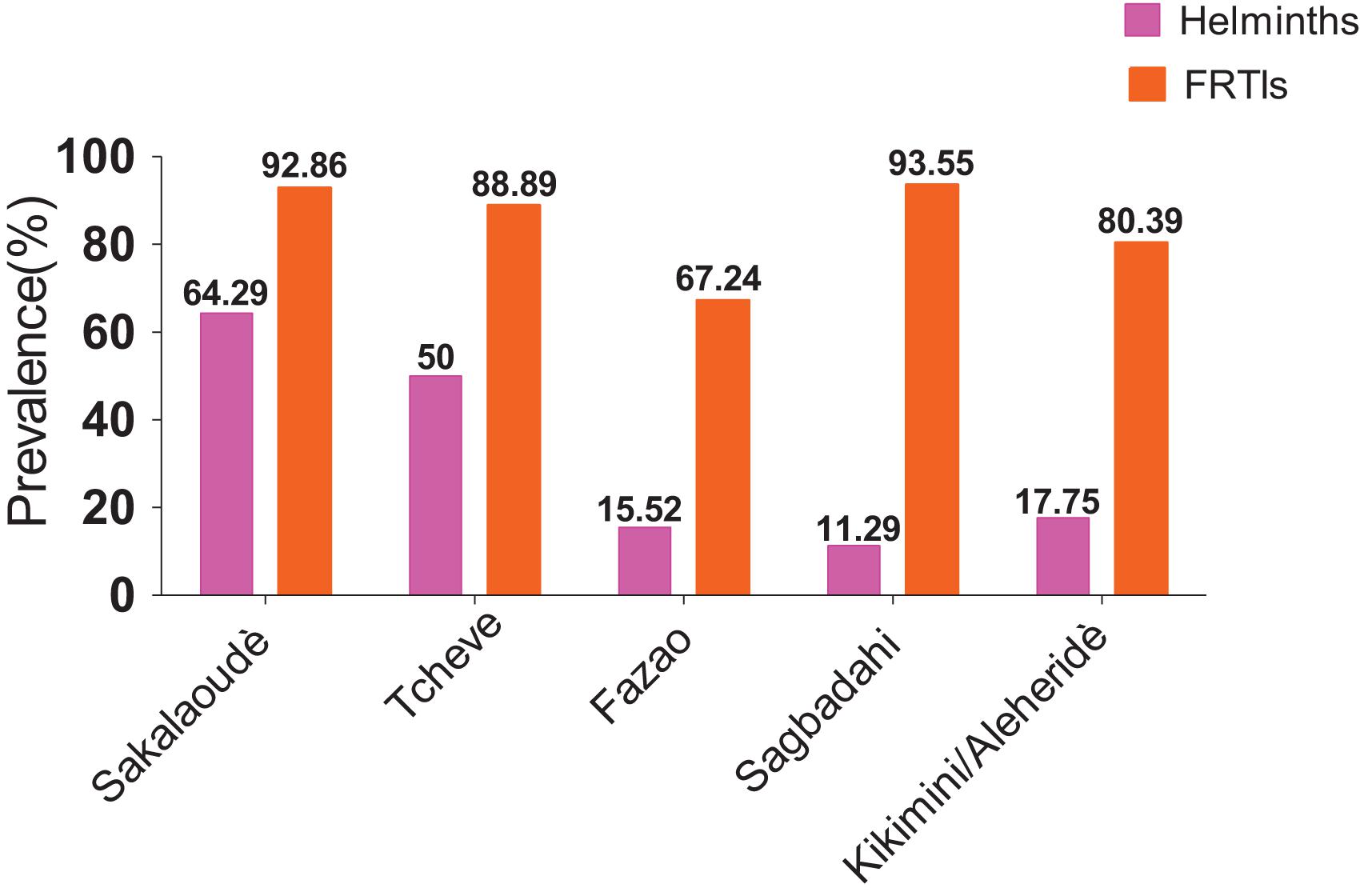
Figure 4. Prevalence of helminthiasis and FRTIs by village. The pink bars present the prevalence of helminthiasis, and the orange bars present the prevalence of FRTIs.
Hookworms were the most frequent helminthic infection (95.34%); Schistosoma mansoni and Hymenolepis nana were found, each on 2.33% of parasites that infected women.
Therefore, univariable logistic regression analysis was performed. We could not observe any association between hookworm infection and STIs [OR = 1.29; 80% CI (0.75–2.19)], HPV [OR = 2.22; 80% CI (1.32–3.75)], BV [OR = 0.86; 80% CI (0.53–1.41)], and candidiasis [OR = 0.98; 80% CI (0.47–2.09)]. Analysis revealed that hookworm infection was a risk factor of HPV infection [OR = 2.22; 80% CI (1.32–3.75)] (Table 1).
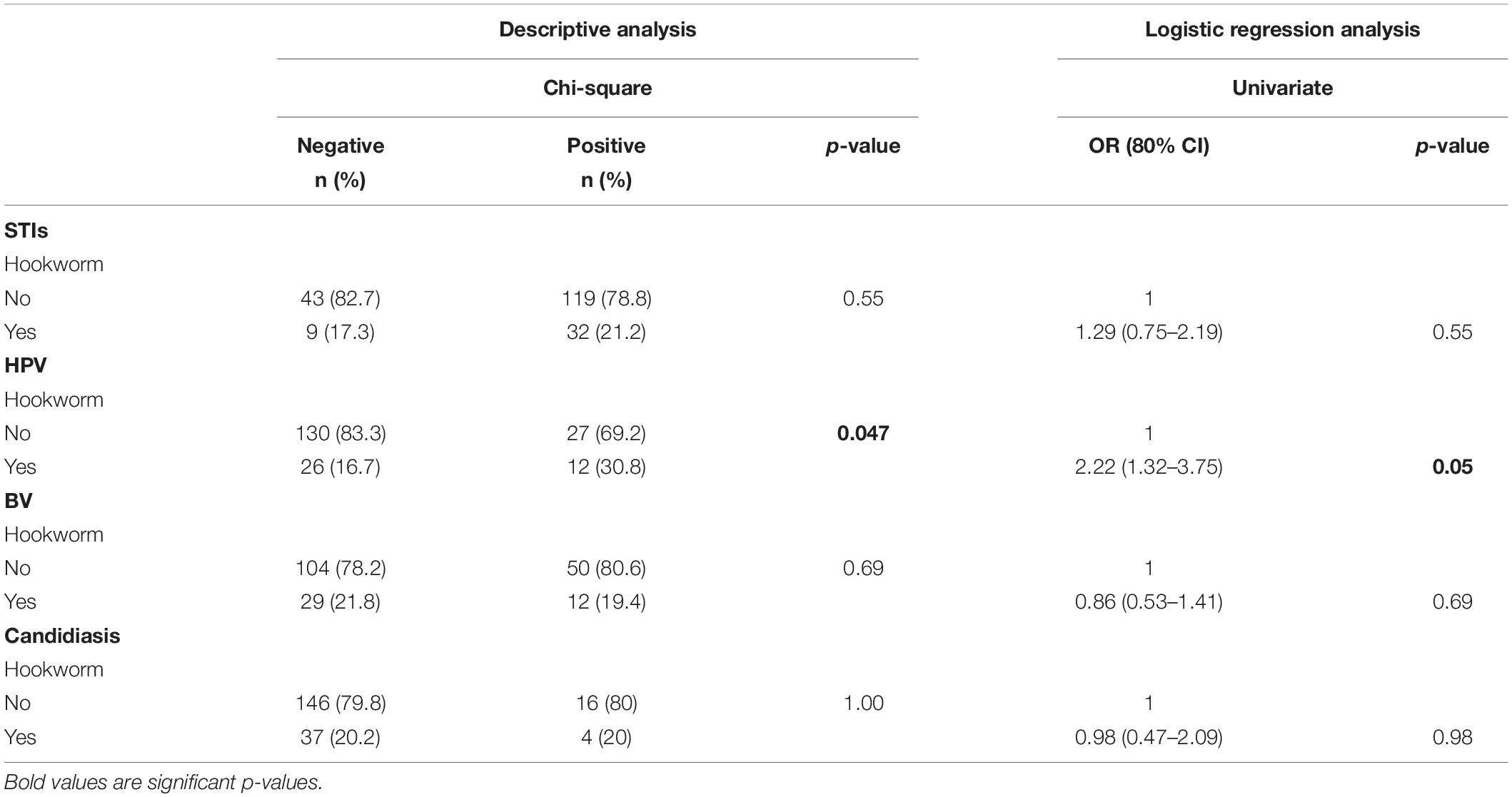
Table 1. Descriptive and logistic regression analysis of hookworm infection associated with FRTIs.
Here we aimed to investigate the association between sociodemographic factors with FRTIs. Univariate logistic regression analysis revealed the independent risk factors associated with STIs (Table 2). The independent risk factors associated with low risk of STIs were the age ranged 33–39 years [OR = 0.51; 80% CI (0.29–0.89)], the fact of being faithful to the same partner for more than 10 years [OR = 0.57; 80% CI (0.36–0.88)], the use of water and soap for vaginal hygiene [OR = 0.48; 80% CI (0.31–0.75)], the use of objects (cotton or tissue) for vaginal cleansing [OR = 0.44; 95% CI (0.28–0.69)], the fact of having had more than four pregnancies [OR = 0.63; 80% CI (0.42–0.96)], and the use of condoms [OR = 0.41; 95% CI (0.27–0.62)].
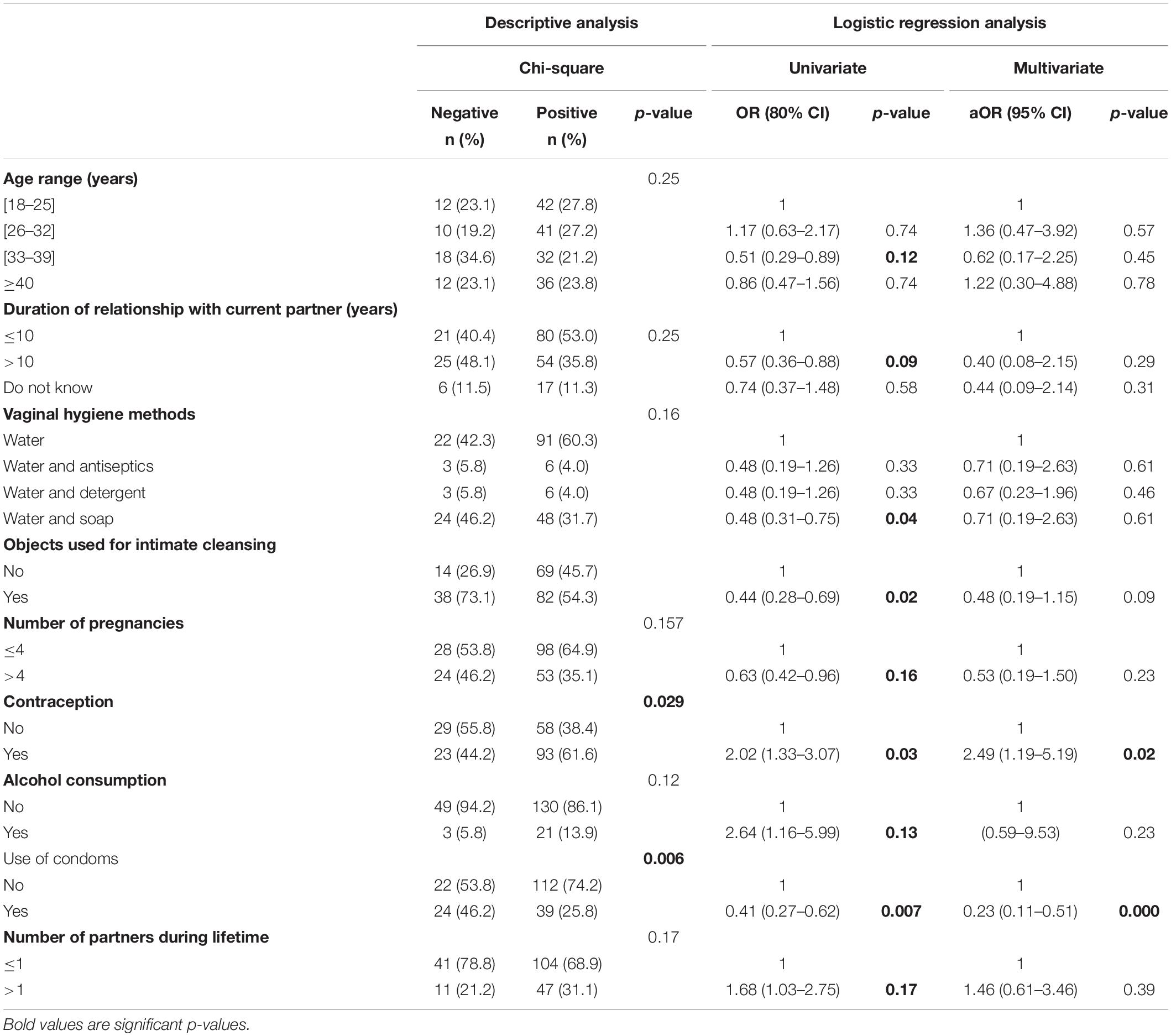
Table 2. Descriptive and logistic regression analysis of factors associated with STIs.
The independent risk factors associated with high risk of STIs were the use of contraceptive methods [OR = 2.02; 80% CI (1.33–3.07)], alcohol consumption [OR = 2.64; 80% CI (1.16–5.99)], and the fact of having had more than one sexual partner in their lifetime [OR = 1.68; 80% CI (1.03–2.75)].
After controlling for confounding parameters through multivariable logistic regression analysis, adjusting independent factors linked to STIs, we found that the use of condoms was a protective factor [aOR = 0.23; 95% CI (0.11–0.51)], while the use of contraceptive methods was a risk factor [aOR = 2.49; 95% CI (1.19–5.19)].
As shown in Table 3, independent factors associated with low risk of HPV infections were the age ranged 26–32 years [OR = 0.47; 80% CI (0.23–0.94)], a live birth at last pregnancy [OR = 0.15; 80% CI (0.05–0.49)], the use of condoms [OR = 0.15; 80% CI (0.07–0.33)], and the fact of knowing that the current partner has other sexual partners [OR = 0.54; 80% CI (0.32–0.90)]. The risk of HPV infection was the highest in unmarried women or women not in a relationship [OR = 5.83; 80% CI (2.13–15.97)], who had more than one partner during their lifetime [OR = 2.66; 80% CI (1.65–4.28)], who had multiple partners [OR = 7.50; 80% CI (2.85–18.72)], and who did not know if their partner had other sexual partners [OR = 2.45; 80% CI (1.09–5.51)].
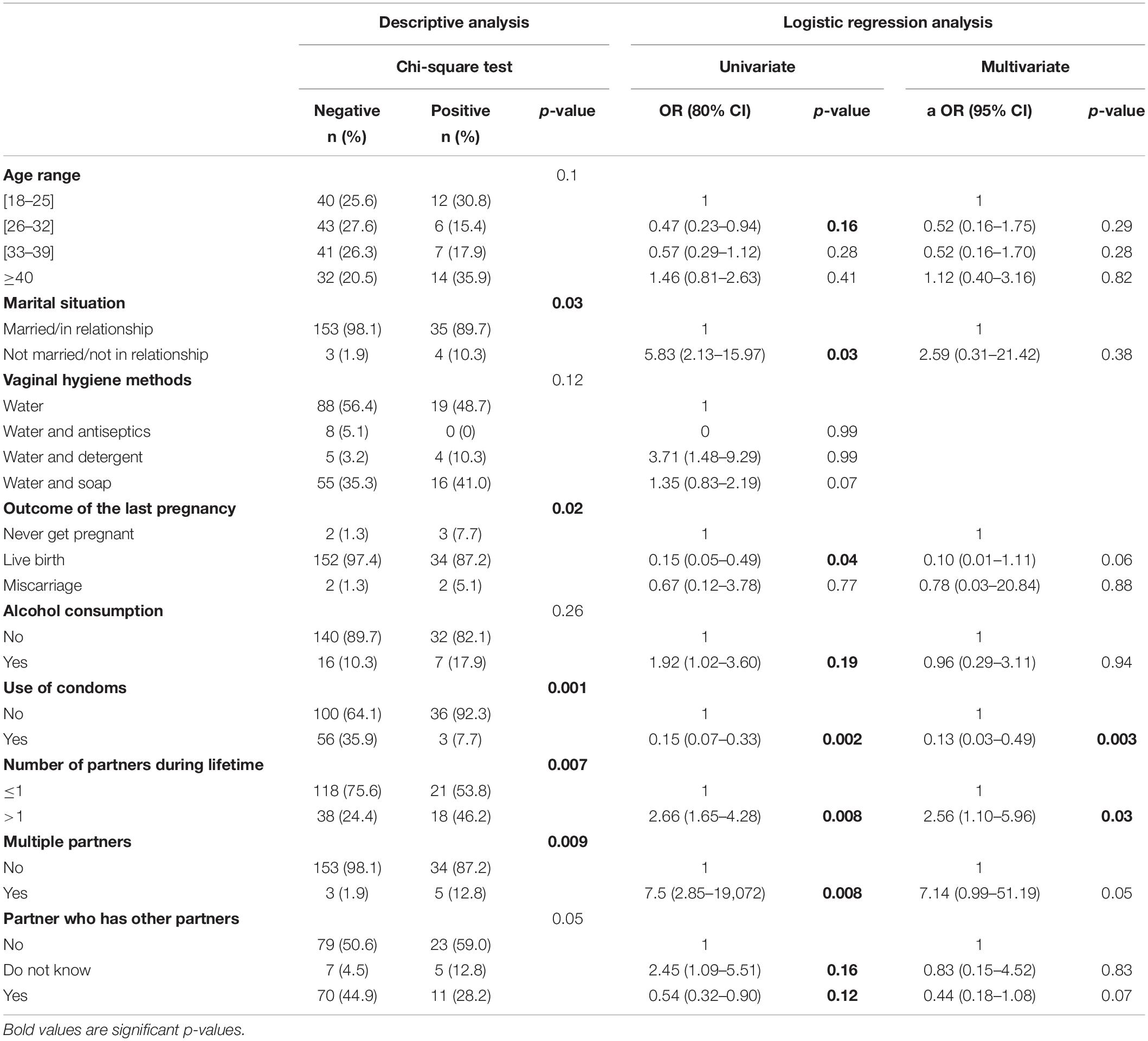
Table 3. Descriptive and logistic regression analysis of factors associated with HPV.
Following the multivariate logistic regression analysis, the use of condoms [aOR = 0.13; 95% CI (0.03–0.49)] appeared to be a protective factor against HPV infections. while having more than one partner during the lifetime [aOR = 2.79; 95% CI (1.32–5.95)] appeared as a risk factor for HPV infections.
In Table 4, the univariate regression analysis revealed that the risk of BV infections was low among participants who had more than four pregnancies [OR = 0.49; 80% CI (0.32–0.75)], had a miscarriage in their last pregnancy [OR = 0.08; 80% CI (0.01–0.65)], had a live birth at their last pregnancy [OR = 0.11; 80% CI (0.26–0.47)], and used condoms [OR = 0.45; 80% CI (0.28–0.73)]. The risk probability of BV was high among women who were not married or not in a relationship [OR = 3.80; 80% CI (1.46–9.91)], did not know the length of their relationship with their current partner [OR = 3.00; 80% CI (1.63–5.53)], did not know if their sexual partner was HIV positive [OR = 1.82; 80% CI (1.22–2.70)], and had multiple partners [OR = 3.80; 80% CI (1.46–9.91)].
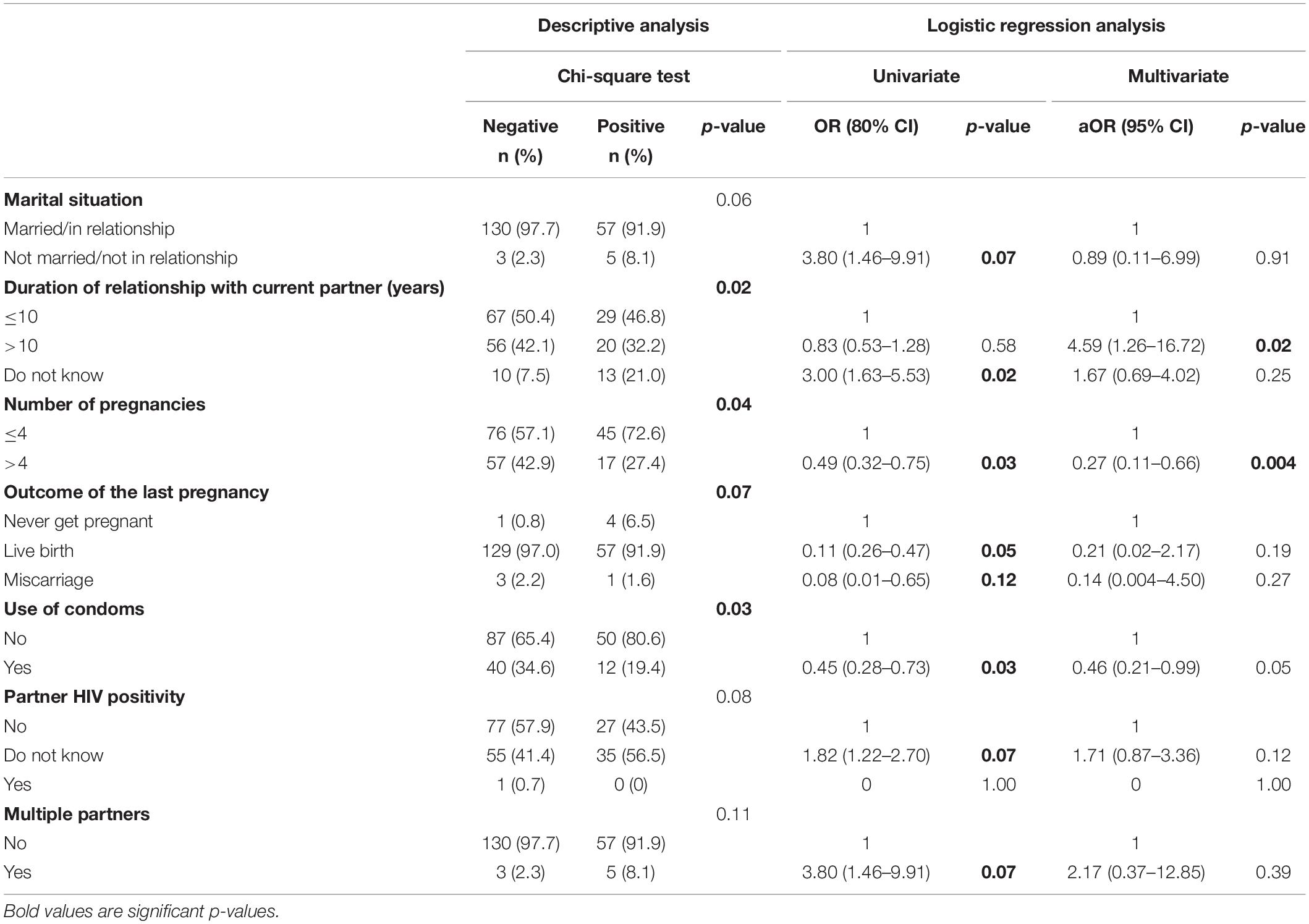
Table 4. Descriptive and logistic regression analysis of factors associated with BV.
After adjusting the variable associated with BV, the risk of BV infections was low among participants who had a number of pregnancies superior to 4 [aOR = 0.27; 95% CI (0.11–0.66)].
The high risk of candidiases was observed among women aged between 26 and 32 years old [OR = 4.84; 80% CI (1.69–13.78)], women older than 40 years [OR = 3.71; 80% CI (1.26–10.93)], who earned less than 70 US dollars [OR = 4.08; 80% CI (1.07–15.56)], used objects (tissue or cotton) for vaginal cleansing [OR = 2.23; 80% CI (1.12–4.44)], had multiple partners [OR = 3.28; 80% CI (1.09–9.78)], did not know if their partner had other partners [OR = 2.88; 80% CI (1.12–7.42)], and who had ever been paid for sex [OR = 4.97; 80% CI (1.57–15.77)]. Finally, using a backward stepwise logistic regression analysis, in a model with age range, monthly income, use of objects for intimate cleansing, practice of paid sexual intercourse, having current multiple partners, having a partner who has other partners, and practicing paid sexual intercourse, it appeared that women who practiced paid sexual intercourse were at high probability risk of candidiasis [aOR = 16.92; 95% CI (1.46–196.48)] (Table 5).
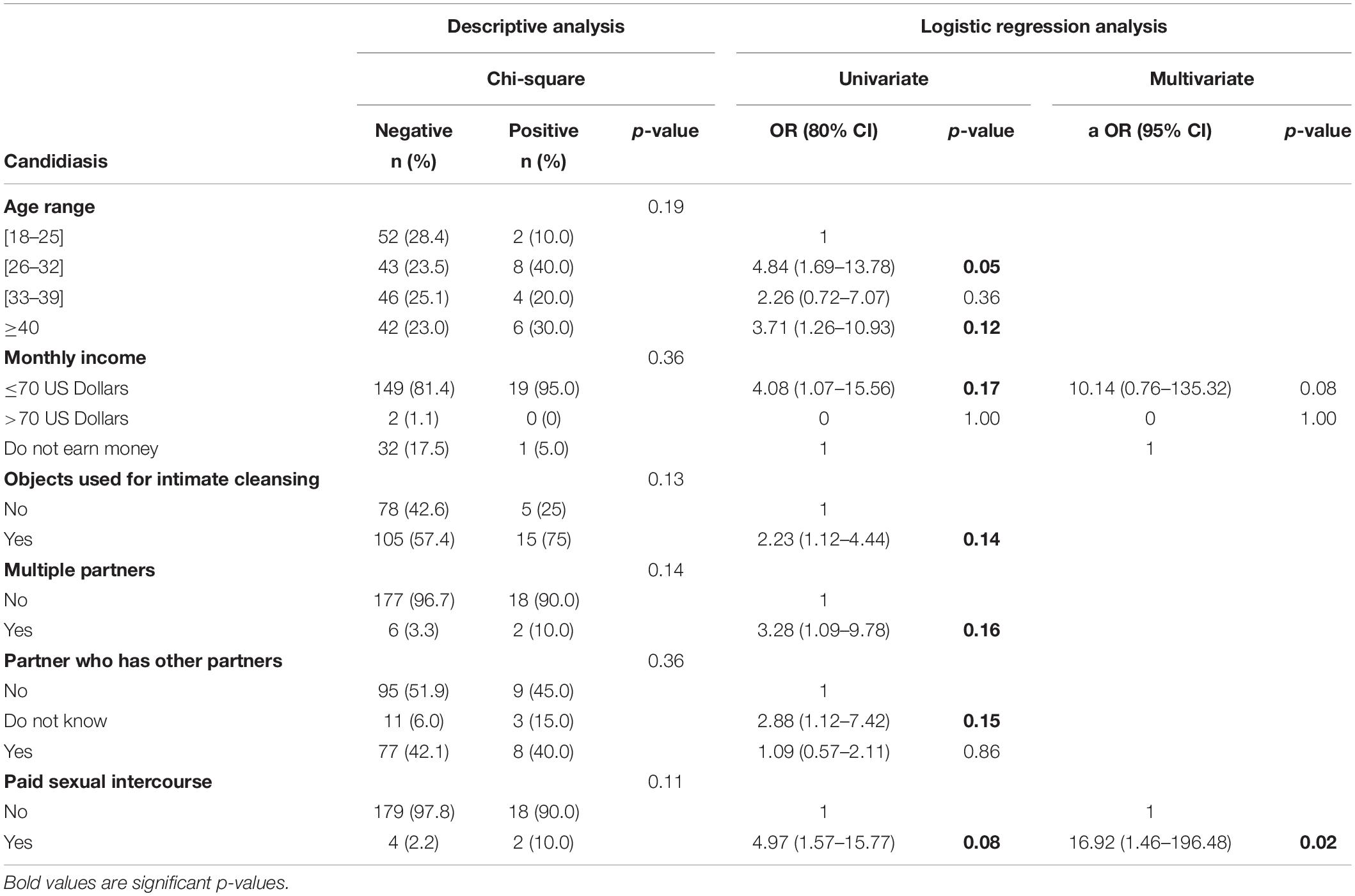
Table 5. Descriptive and logistic regression analysis of factors associated with candidiasis.
This study revealed that STIs were predominantly prevalent (74.38%) in six rural villages of the central region of Togo. Serious complications of STIs are ectopic pregnancy, pelvic inflammatory disease, preterm labor, miscarriage, stillbirth, and congenital infection, and they may lead to chronic disability (such as infertility and genital cancer) and death. Here, we diagnosed 27 germs incriminated in STIs. In detail, U. parvum was the most prevalent affecting 50% of women, followed by U. urealyticum (26.5%) and M. hominis (17.5%). Those three species belong to the gender Mycoplasma, a gender of bacteria frequently isolated from the genital tract of both men and women (Kokkayil and Dhawan, 2015). In Italy, Leli et al. (2018) found that U. parvum was the most isolated mycoplasma among women with a prevalence of 38.3%, and a study in South Africa revealed that U. parvum was isolated from 72.4% vaginal samples of pregnant women (Redelinghuys et al., 2013). In general, U. parvum is associated with intrauterine inflammation (Kasper et al., 2010).
Among viruses found in the cohort, human CMV was predominately prevalent (5%). In Africa, CMV is a neglected pathogen, but its burden is important with a seroprevalence close to 100% (Bates and Brantsaeter, 2016). CMV is a member of Herpesviridae family and is classified as an emerging STI (Kent, 2017) that is transmitted through direct contact with multiple fluids of the body like saliva, urine, milk, and genital secretions. In addition, it can also be transmitted from an infected mother to her fetus (CDC, 2020b). The virus can stay latent in infected persons until the immune system weakening allows the virus to reactivate (Grinde, 2013).
In regards to risk factors, this study revealed that the use of contraceptive methods appeared as a high risk of STIs. Contraceptives are used for birth control and have a socio-economic impact. According to Deese et al. (2018) some contraceptive methods have related to STIs, but robust studies should be conducted to provide accurate information and facilitate contraceptive choice by women. Moreover, the presence of STIs was also associated with alcohol consumption, confirming other studies showing that increased risk of STIs was influenced by alcohol drinking across a wide variety of populations (Arasteh et al., 2008; Hutton et al., 2008). That is justified by the fact that alcohol drinking can lead to immune deficiency and increase sensitivity to infectious diseases (Zitkute and Bumbuliene, 2016). Another independent factor associated with STIs was the type of relationship and sexual behavior, especially the number of sexual partners during the lifetime, confirming a study in Brazil among rural women, which revealed that a higher number of partners in life was a risk factor for STIs (Oliveira et al., 2008). In addition, having had more than one partner during the lifetime appeared as a high-risk factor for HPV infections, confirming a previous study from Molano et al. (2002) who found that having had more than one regular sexual partner increased HPV infection risk (OR 1.9).
In general, HPV plays an important role as a leading cause of most cervical cancers. More than 100 types of HPV have been identified and at least 14 of them are associated as risk factors for cancer and especially 2 types (HPV 16 and HPV 18) cause 70% of cervical cancers and pre-cancerous cervical lesions (WHO, 2019). Nevertheless, in our cohort, HPV 16 and HPV 18 were less prevalent (respectively, 1.54 and 1.03%), but associations to cancer diseases need to be investigated in future studies.
Interestingly, the impact of helminth immune regulation on susceptibility to STIs is known. Given the global incidence of helminths and their detrimental impact on public health (WHO, 2017), the geographical overlap between helminth exposure and STIs might be a result of parasite-induced changes on female reproductive health (Gopinath et al., 2000; Wolday et al., 2002) and helminth-induced immunomodulation (Brown et al., 2005). Indeed, here we showed that women who had hookworm infections had a 2.22 times risk of HPV infection than those who were not infected by hookworm. Gravitt et al. (2015) found that women infected with soil-transmitted helminths (STHs) had 60% higher prevalence of HPV, compared with those without STHs infection with a prevalence ratio of 1.6. The helminth-induced Th2 response in vagina could explain the plausibility of high HPV occurrence (Gravitt et al., 2015).
Concerning endogenous infections, 31.79% of women were affected by BV and 9.85% had candidiasis. In Sokodé, the principal city of the central region of Togo, Tchelougou et al. (2013) found on pregnant women a prevalence of 55.31% of Gardnerella vaginalis and 50.77% of candidiasis, which is caused by Candida species and has been shown to be responsible for inflammatory changes in the vaginal and vulvar epithelium (Jeanmonod and Jeanmonod, 2020). However, the differences between the studies could be due to pregnancy status with unbalance vaginal flora.
In addition, BV, which is the most common vaginal condition in women aged between 15 and 44 years (CDC, 2020a), is known to increase predisposition to STIs (Lata et al., 2010; Bautista et al., 2017). In detail, it is characterized by an altered vaginal microflora including an increase in the vaginal pH, reduced lactobacilli species, and increased hydrogen peroxide producing species and facultative and anaerobic bacteria numbers and/or types (Eschenbach et al., 2000).
Interestingly, the risk probability of BV was high among those who were not married or not in a relationship and those who had multiple partners. Ranjit et al. (2018) found that 100% of unmarried women were more prone to BV, and indeed, another study revealed that BV has been associated with having three or more male sexual partners in the past 12 months (OR = 1.60, 95% CI: 1.19–2.04) (Smart et al., 2004). Moreover, the number of pregnancies more than 4 was a protective factor against BV infections. This was in line with a study conducted in Ghana where Konadu et al. (2019) found that the fact of having more than four pregnancies was protective for BV.
In a logistic regression model with monthly income and practicing paid sexual intercourse, we found that women who practiced paid sexual intercourse were at high probability risk of candidiasis. Unlike our results, Konadu et al. (2019) did not find any possible risk factor associated with candidiasis, although they did not include the practice of paid sexual intercourse as a possible risk factor. We can notice that the study population of Konadu et al. (2019) was pregnant women attending antenatal clinic, whereas our study population was exclusively non-pregnant women.
Finally, the use of condoms was a protective factor against STIs, confirming a previous study (Ginindza et al., 2017). Moreover, several studies revealed that consistent condom use was also associated with significantly decreased risk of gonorrhea, chlamydia, genital ulcer disease, BV, HPV, and pelvic inflammatory disease but did not have an impact on candidiasis (Baeten et al., 2001).
The present study had some limitations including the final samples size and one stool sample per participant.
This study depicted a high prevalence of FRTIs in six villages of the central region of Togo. Among them, STIs were predominately prevalent, and factors such as helminth infection, the use of contraceptives, the number of pregnancies, the number of partners, the monthly income, the methods of cleansing, the marital status, and alcohol drinking were associated with the occurrence of FRTIs. Local healthcare authorities must focus on women education and sensitization strategies based on these risk factors to optimize prevention and control measures against FRTIs.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by the Comité de Bioéthique pour la Recherche en Santé (CBRS) du ministère de la santé du Togo. The patients/participants provided their written informed consent to participate in this study.
GK, AHA, CNT, PT, CV, AN’d, SA, HK, BM, and OA carried out the survey and the field work. CV, MR, GK, AHA, MO, CNT, and PT analyzed the samples. GK, MR, LEL, AH, WH, MK, YA, and SK designed the study protocol, analyzed, interpreted, and validated all the data. GK, WH, MR, CNT, and LEL wrote the manuscript which was then read and approved by all other authors. All authors contributed to the article and approved the submitted version.
This study was funded by the German Research Foundation (DFG; Grant LA 2746/2-1) within the “German–African Cooperation Projects in Infectiology” through grants awarded to GK, WH, and LEL. Additionally, AH was financially supported by the Federal Ministry of Education and Research (BMBF; initiative Research Networks for Health Innovations in sub-Saharan Africa: TAKeOFF) and was a member of the Excellence Cluster Immunosensation (DFG, EXC 1023). LEL and AH were also members of the German Center of Infectious Disease (DZIF).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We thank all villagers from the central region of Togo and the women that agreed to participate in this study.
Arasteh, K., Des Jarlais, D. C., and Perlis, T. E. (2008). Alcohol and HIV sexual risk behaviors among injection drug users. Drug Alcohol Depend. 95, 54–61. doi: 10.1016/j.drugalcdep.2007.12.008
Arndts, K., Klarmann-Schulz, U., Batsa, L., Debrah, A. Y., Epp, C., Fimmers, R., et al. (2015). Reductions in microfilaridermia by repeated ivermectin treatment are associated with lower plasmodium-specific Th17 immune responses in Onchocerca volvulus-infected individuals. Parasites Vectors 8:184. doi: 10.1186/s13071-015-0786-5
Baeten, J., Nyange, P., Richardson, B., Lavreys, L., Chohan, B., Martin, H., et al. (2001). Hormonal contraception and risk of sexually transmitted disease acquisition: results from a prospective study. Am. J. Obstet. Gynecol. 185, 380–385. doi: 10.1067/mob.2001.115862
Bates, M., and Brantsaeter, A. B. (2016). Human cytomegalovirus (CMV) in Africa: a neglected but important pathogen. J. Virus Erad. 2, 136–142. doi: 10.1016/S2055-6640(20)30456-8
Bautista, C. T., Wurapa, E. K., Sateren, W. B., Morris, S. M., Hollingsworth, B. P., and Sanchez, J. L. (2017). Association of bacterial vaginosis with chlamydia and gonorrhea among women in the U.S. Army. Am. J. Prev. Med. 52, 632–639. doi: 10.1016/j.amepre.2016.09.016
Brown, M., Mawa, P. A., Joseph, S., Bukusuba, J., Watera, C., Whitworth, J. A., et al. (2005). Treatment of Schistosoma mansoni infection increases helminth-specific type 2 cytokine responses and HIV-1 loads in coinfected ugandan adults. J. Infect. Dis. 191, 1648–1657. doi: 10.1086/429668
CDC (2020b). Cytomegalovirus (CMV) and Congenital CMV Infection: About Cytomegalovirus (CMV). Atlanta, GA: CDC.
Chetty, A., Omondi, M. A., Butters, C., Smith, K. A., Katawa, G., Ritter, M., et al. (2020). Impact of helminth infections on female reproductive health and associated diseases. Front. Immunol. 2020:577516. doi: 10.3389/fimmu.2020.577516
Deese, J., Pradhan, S., Goetz, H., and Morrison, C. (2018). Contraceptive use and the risk of sexually transmitted infection: systematic review and current perspectives. Open Access J. Contracept. 9, 91–112. doi: 10.2147/OAJC.S135439
Diadhiou, M., Ba Diallo, A., Barry, M. S., Alavo, S. C., Mall, I., Gassama, O., et al. (2019). Prevalence and risk factors of lower reproductive tract infections in symptomatic women in dakar. Senegal. Infect Dis. (Auckl) 12:1178633719851825. doi: 10.1177/1178633719851825
Eschenbach, D. A., Thwin, S. S., Patton, D. L., Hooton, T. M., Stapleton, A. E., Agnew, K., et al. (2000). Influence of the normal menstrual cycle on vaginal tissue, discharge, and microflora. Clin. Infect. Dis. 30, 901–907. doi: 10.1086/313818
Ginindza, T. G., Stefan, C. D., Tsoka-Gwegweni, J. M., Dlamini, X., Jolly, P. E., Weiderpass, E., et al. (2017). Prevalence and risk factors associated with sexually transmitted infections (STIs) among women of reproductive age in Swaziland. Infect. Agent Cancer 12:29. doi: 10.1186/s13027-017-0140-y
Gopinath, R., Ostrowski, M., Justement, S. J., Fauci, A. S., and Nutman, T. B. (2000). Filarial infections increase susceptibility to human immunodeficiency virus infection in peripheral blood mononuclear cells in vitro. J. Infect. Dis. 182, 1804–1808. doi: 10.1086/317623
Gravitt, P., Marks, M., Kosek, M., Huang, C., Cabrera, L., Olortegui, M., et al. (2015). Soil transmitted helminth infections are associated with an increase in human papillomavirus prevalence and a Th2 cytokine signature in cervical fluids. J. Infect. Dis. 212, 723–730. doi: 10.1093/infdis/jiv498
Grinde, B. (2013). Herpesviruses: latency and reactivation - viral strategies and host response. J. Oral Microbiol. 5:10.3402/jom.v5i0.22766 doi: 10.3402/jom.v5i0.22766
Hartmann, W., Brunn, M. L., Stetter, N., Gagliani, N., Muscate, F., Stanelle-Bertram, S., et al. (2019). Helminth infections suppress the efficacy of vaccination against seasonal influenza. Cell Rep. 29, 2243–2256. doi: 10.1016/j.celrep.2019.10.051
Hussen, S., Wachamo, D., Yohannes, Z., and Tadesse, E. (2018). Prevalence of chlamydia trachomatis infection among reproductive age women in sub Saharan Africa: a systematic review and meta-analysis. BMC Infect. Dis. 18:596. doi: 10.1186/s12879-018-3477-y
Hutton, H. E., McCaul, M. E., Santora, P. B., and Erbelding, E. J. (2008). The relationship between recent alcohol use and sexual behaviors: gender differences among sexually transmitted disease clinic patients. Alcohol Clin. Exp. Res. 32, 2008–2015. doi: 10.1111/j.1530-0277.2008.00788.x
Jeanmonod, R., and Jeanmonod, D. (2020). Vaginal Candidiasis (Vulvovaginal Candidiasis) StatPearls. Treasure Island (FL): StatPearls Publishing.
Kasper, D. C., Mechtler, T. P., Reischer, G. H., Witt, A., Langgartner, M., Pollak, A., et al. (2010). The bacterial load of Ureaplasma parvum in amniotic fluid is correlated with an increased intrauterine inflammatory response. Diag. Microbiol. Infect. Dis. 67, 117–121. doi: 10.1016/j.diagmicrobio.2009.12.023
Katawa, G., Layland, L. E., Debrah, A. Y., Von Horn, C., Batsa, L., Kwarteng, A., et al. (2015). Hyperreactive onchocerciasis is characterized by a combination of Th17-Th2 immune responses and reduced regulatory T cells. PLoS Negl. Trop. Dis. 9:e3414. doi: 10.1371/journal.pntd.0003414
Katawa, G., Tchopba, C., Ritter, M., da Silva, M., and Ameyapoh, A. (2021). Female reproductive tract health: prevalence and risk factors associated with infections in Lomé. (Female reproductive tract infections in Lomé). Clin. Res. Trials 7, 1–9. doi: 10.15761/CRT.1000342
Kent, B. N. (2017). Emerging sexually transmitted diseases. ASCLS 30, 124–128. doi: 10.29074/ascls.30.2.124
Kokkayil, P., and Dhawan, B. (2015). Ureaplasma: current perspectives. Indian J. Med. Microbiol. 33, 205–214. doi: 10.4103/0255-0857.154850
Konadu, D. G., Owusu-Ofori, A., Yidana, Z., Boadu, F., Iddrisu, L. F., Adu-Gyasi, D., et al. (2019). Prevalence of vulvovaginal candidiasis, bacterial vaginosis and trichomoniasis in pregnant women attending antenatal clinic in the middle belt of Ghana. BMC Pregnancy Childbirth 19:341. doi: 10.1186/s12884-019-2488-z
Lata, I., Pradeep, Y., and Sujata, J. A. (2010). Estimation of the incidence of bacterial vaginosis and other vaginal infections and its consequences on maternal/fetal outcome in pregnant women attending an antenatal clinic in a tertiary care hospital in North India. Indian J. Community Med. 35, 285–289. doi: 10.4103/0970-0218.66855
Leli, C., Mencacci, A., Latino, M. A., Clerici, P., Rassu, M., Perito, S., et al. (2018). Prevalence of cervical colonization by Ureaplasma parvum, Ureaplasma urealyticum, Mycoplasma hominis and Mycoplasma genitalium in childbearing age women by a commercially available multiplex real-time PCR: an Italian observational multicentre study. J. Microbiol. Immunol. Infect. 51, 220–225. doi: 10.1016/j.jmii.2017.05.004
Molano, M., Posso, H., Weiderpass, E., van den Brule, A. J. C., Ronderos, M., Franceschi, S., et al. (2002). Prevalence and determinants of HPV infection among Colombian women with normal cytology. Br. J. Cancer 87, 324–333. doi: 10.1038/sj.bjc.6600442
Moragianni, D., Dryllis, G., Andromidas, P., Kapeta-Korkouli, R., Kouskouni, E., Pessach, I., et al. (2019). Genital tract infection and associated factors affect the reproductive outcome in fertile females and females undergoing in vitro fertilization. Biomed. Rep. 10, 231–237. doi: 10.3892/br.2019.1194
Moreau, E., and Chauvin, A. (2010). Immunity against helminths: interactions with the host and the intercurrent infections. J. Biomed. Biotechnol. 2010:428593. doi: 10.1155/2010/428593
Oliveira, F., Lang, K., Ehrig, V., Heukelbach, J., Fraga, F., Stoffler-Meilicke, M., et al. (2008). Risk factors for sexually transmitted infections in women in rural Northeast Brazil. J. Infect. Dev. Ctries 2, 211–217. doi: 10.3855/jidc.265
Rabiu, K. A., Adewunmi, A. A., Akinlusi, F. M., and Akinola, O. I. (2010). Female reproductive tract infections: understandings and care seeking behaviour among women of reproductive age in Lagos, Nigeria. BMC Womens Health 10:8. doi: 10.1186/1472-6874-10-8
Ranjit, E., Raghubanshi, R. B., Maskey, S., and Parajuli, P. (2018). Prevalence of bacterial vaginosis and its association with risk factors among nonpregnant women: a hospital based study. Int. J. Microbiol. 2018:8349601. doi: 10.1155/2018/8349601
Redelinghuys, M. J., Ehlers, M. M., Dreyer, A. W., Lombaard, H., and Kock, M. M. (2013). P3.035 prevalence of genital mycoplasmas and bacterial vaginosis in pregnant women in gauteng, South Africa. Sex Transm. Infect. 89, (Suppl. 1): A159. doi: 10.1136/sextrans-2013-051184.0495
Ritter, M., Ndongmo, W. P. C., Njouendou, A. J., Nghochuzie, N. N., Nchang, L. C., Tayong, D. B., et al. (2018). Mansonella perstans microfilaremic individuals are characterized by enhanced type 2 helper T and regulatory T and B cell subsets and dampened systemic innate and adaptive immune responses. PLoS Negl. Trop. Dis. 12:e0006184. doi: 10.1371/journal.pntd.0006184
Ritter, M., Osei-Mensah, J., Debrah, L. B., Kwarteng, A., Mubarik, Y., Debrah, A. Y., et al. (2019). Wuchereria bancrofti-infected individuals harbor distinct IL-10-producing regulatory B and T cell subsets which are affected by anti-filarial treatment. PLoS Negl. Trop. Dis. 13:e0007436. doi: 10.1371/journal.pntd.0007436
Smart, S., Singal, A., and Mindel, A. (2004). Social and sexual risk factors for bacterial vaginosis. Sex Transm. Infect. 80, 58–62. doi: 10.1136/sti.2003.004978
Tchelougou, D., Karou, D. S., Kpotsra, A., Balaka, A., Assih, M., Bamoke, M., et al. (2013). [Vaginal infections in pregnant women at the Regional Hospital of Sokode (Togo) in 2010 and 2011]. Med. Sante Trop. 23, 49–54. doi: 10.1684/mst.2013.0142
Torondel, B., Sinha, S., Mohanty, J. R., Swain, T., Sahoo, P., Panda, B., et al. (2018). Association between unhygienic menstrual management practices and prevalence of lower reproductive tract infections: a hospital-based cross-sectional study in Odisha. India. BMC Infect. Dis. 18:473. doi: 10.1186/s12879-018-3384-2
WHO (2017). Sexually Transmitted Infections: Implementing the Global STI Strategy: Evidence-to-action Brief. Geneva: WHO.
Wolday, D., Mayaan, S., Mariam, Z. G., Berhe, N., Seboxa, T., Britton, S., et al. (2002). Treatment of intestinal worms is associated with decreased HIV plasma viral load. J. Acquir. Immune Defic. Syndr. 31, 56–62. doi: 10.1097/00126334-200209010-00008
Yan, L., Luan, T., Hua, Q., Gu, Y., Fu, Z., Liu, X., et al. (2018). Peptidomic analysis of female reproductive tract secretion to identify putative anti-infection peptides in the female genital system via nanotechnologies. J. Biomed. Nanotechnol. 14, 215–226. doi: 10.1166/jbn.2018.2500
Keywords: female reproductive tract infections, risk factors, helminth infections, rural areas, central region of Togo
Citation: Holali Ameyapoh A, Katawa G, Ritter M, Tchopba CN, Tchadié PE, Arndts K, Kamassa HE, Mazou B, Amessoudji OM, N’djao A, Agoro S, Vogelbusch C, Omondi MA, Kolou M, Karou SD, Horsnell W, Hoerauf A, Ameyapoh Y and Layland LE (2021) Hookworm Infections and Sociodemographic Factors Associated With Female Reproductive Tract Infections in Rural Areas of the Central Region of Togo. Front. Microbiol. 12:738894. doi: 10.3389/fmicb.2021.738894
Received: 09 July 2021; Accepted: 04 October 2021;
Published: 03 November 2021.
Edited by:
Celia Holland, Trinity College Dublin, IrelandReviewed by:
Claudette Poole, University of Alabama at Birmingham, United StatesCopyright © 2021 Holali Ameyapoh, Katawa, Ritter, Tchopba, Tchadié, Arndts, Kamassa, Mazou, Amessoudji, N’djao, Agoro, Vogelbusch, Omondi, Kolou, Karou, Horsnell, Hoerauf, Ameyapoh and Layland. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Gnatoulma Katawa, bWFoa2F0YXdhQHlhaG9vLmZy; Laura E. Layland, bGF1cmEubGF5bGFuZEBzYmNvbXB1dGluZy5kZQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.