 Husam Salah1,2*
Husam Salah1,2* Michaela Lackner3
Michaela Lackner3 Jos Houbraken4
Jos Houbraken4 Bart Theelen2
Bart Theelen2 Cornelia Lass-Flörl3Teun Boekhout2,5Muna Almaslamani6
Cornelia Lass-Flörl3Teun Boekhout2,5Muna Almaslamani6 Saad J. Taj-Aldeen1
Saad J. Taj-Aldeen1- 1Division of Microbiology, Department of Laboratory Medicine and Pathology, Hamad Medical Corporation, Doha, Qatar
- 2Yeast Research, Westerdijk Fungal Biodiversity Institute, Utrecht, Netherlands
- 3Division of Hygiene and Medical Microbiology, Medical University of Innsbruck, Innsbruck, Austria
- 4Applied and Industrial Mycology, Westerdijk Fungal Biodiversity Institute, Utrecht, Netherlands
- 5Institute of Biodiversity and Ecosystem Dynamics (IBED), University of Amsterdam, Netherlands
- 6Department of Medicine, Hamad Medical Corporation, Doha, Qatar
Aspergillus are ubiquitous mold species that infect immunocompetent and immunocompromised patients. The symptoms are diverse and range from allergic reactions, bronchopulmonary infection, and bronchitis, to invasive aspergillosis. The aim of this study was to characterize 70 Aspergillus isolates recovered from clinical specimens of patients with various clinical conditions presented at Hamad general hospital in Doha, Qatar, by using molecular methods and to determine their in vitro antifungal susceptibility patterns using the Clinical and Laboratory Standards Institute (CLSI) M38-A2 reference method. Fourteen Aspergillus species were identified by sequencing β-tubulin and calmodulin genes, including 10 rare and cryptic species not commonly recovered from human clinical specimens. Aspergillus welwitschiae is reported in this study for the first time in patients with fungal rhinosinusitis (n = 6) and one patient with a lower respiratory infection. Moreover, Aspergillus pseudonomius is reported in a patient with fungal rhinosinusitis which is considered as the first report ever from clinical specimens. In addition, Aspergillus sublatus is reported for the first time in a patient with cystic fibrosis. In general, our Aspergillus strains exhibited low MIC values for most of the antifungal drugs tested. One strain of Aspergillus fumigatus showed high MECs for echinocandins and low MICs for the rest of the drugs tested. Another strain of A. fumigatus exhibited high MIC for itraconazole and categorized as non-wild type. These findings require further analysis of their molecular basis of resistance. In conclusion, reliable identification of Aspergillus species is achieved by using molecular sequencing, especially for the emerging rare and cryptic species. They are mostly indistinguishable by conventional methods and might exhibit variable antifungal susceptibility profiles. Moreover, investigation of the antifungal susceptibility patterns is necessary for improved antifungal therapy against aspergillosis.
Introduction
Aspergillus species are common environmental fungi found in soil and decaying vegetative materials. They can infect immunocompetent (Chaturvedi et al., 2017; Emiralioglu et al., 2017; Kumar et al., 2017; Saedi et al., 2017) and immunocompromised (Taccone et al., 2015) patients. Individuals with underlying diseases or immune deficiencies can develop a variety of symptoms ranging from allergies, bronchopulmonary infections, and bronchitis, to invasive aspergillosis (IA) (Ruping et al., 2008; Guinea et al., 2010; Sugui et al., 2014). IA is associated mainly with neutropenic patients suffering from hematological malignancies (Gerson et al., 1984; Abers et al., 2016). Other risk factors include hematopoietic stem cell transplant (HSCT) (Marr et al., 2002), solid organ transplant (SOT) (Patterson et al., 2000), patients receiving prolonged high doses of corticosteroids (Palmer et al., 1991; Lewis and Kontoyiannis, 2009), human immunodeficiency virus (HIV) infection with advanced acquired immune-deficiency syndrome (AIDS) (Libanore et al., 2002) and chronic granulomatous disease (CGD) (Beaute et al., 2011). IA is associated with a high mortality rate among immunocompromised patients (Baddley et al., 2010; Kontoyiannis et al., 2010; Neofytos et al., 2013; Garcia-Vidal et al., 2015). During the last two decades, species other than A. fumigatus, namely, Aspergillus flavus, Aspergillus terreus, Aspergillus niger, and other cryptic and rare species have increasingly been isolated from clinical specimens (Lass-Florl et al., 2005; Krishnan et al., 2009; Alastruey-Izquierdo et al., 2012). This epidemiological shift is attributed to the increasing number of immunocompromised patients, advances in the detection and identification of pathogenic fungi, and the selective pressure caused by extensive use of broad-spectrum antifungal drugs (Krishnan et al., 2009; Alastruey-Izquierdo et al., 2012). Voriconazole is the first line therapy recommended for the management of IA (Patterson et al., 2016; Ullmann et al., 2018). Other alternatives are liposomal amphotericin B and isavuconazole. In patients who exhibit refractory or progressive IA after the initiation of primary therapy, an additional antifungal agent may be added or a combination of antifungal agents from different classes (e.g., a triazole and an echinocandin) may be considered (Patterson et al., 2016; Ullmann et al., 2018). Posaconazole can be used as prophylaxis for patients at high risk for IA (Patterson et al., 2016; Ullmann et al., 2018). Triazole-resistant Aspergillus, particularly A. fumigatus, became a worldwide problem, with high prevalence in Europe (Alastruey-Izquierdo et al., 2013; Abdolrasouli et al., 2018; Buil et al., 2019) and recently in the United States (Berkow et al., 2018). This poses a great challenge for clinicians in patient management. Triazole resistance in Aspergillus has also been reported from other parts of the world, such as India (Chowdhary et al., 2015), Iran (Seyedmousavi et al., 2013; Mohammadi et al., 2016; Nabili et al., 2016), and Tanzania (Chowdhary et al., 2014). In the Middle East, apart from Iran, triazole resistance for A. fumigatus has also been documented in Kuwait, a neighboring Arabian gulf country, in outdoor and hospital environments (Ahmad et al., 2014) as well as from clinical samples (Ahmad et al., 2015).
The aim of the current study was to characterize 70 Aspergillus species isolated from a variety of clinical specimens received at the microbiology laboratory of Hamad general hospital in Doha, Qatar, with emphasis on emerging rare species identified as human pathogens, and to determine their antifungal susceptibility patterns using the Clinical and Laboratory Standards Institute (CLSI) M38-A2 reference method.
Materials and Methods
Patients and Specimens
Seventy Aspergillus species were recovered from clinical specimens of 67 patients, including immunocompromised patients (n = 17, 25.4%) and immunocompetent ones with other underlying diseases (n = 50, 74.6%) (Table 1), presented at Hamad general hospital in Doha, Qatar, between August 2003 and November 2014 with proven or probable infection or colonization by Aspergillus species. The patients represented 15 nationalities, including countries from Southeast Asia (n = 23, 23.3%) and the Middle East (n = 42, 62.7%), South Africa (n = 1, 1.5%) and the United States (n = 1, 1.5%). The isolates were recovered from various clinical specimens, including respiratory samples (sputum, broncho-alveolar lavage (BAL) and bronchial wash), nose and nasal sinuses, ear, wounds, pus/abscess, eye, nail, burn, pleural fluid and an unknown culture plate of clinical specimen received for identification from an external facility (Table 1).
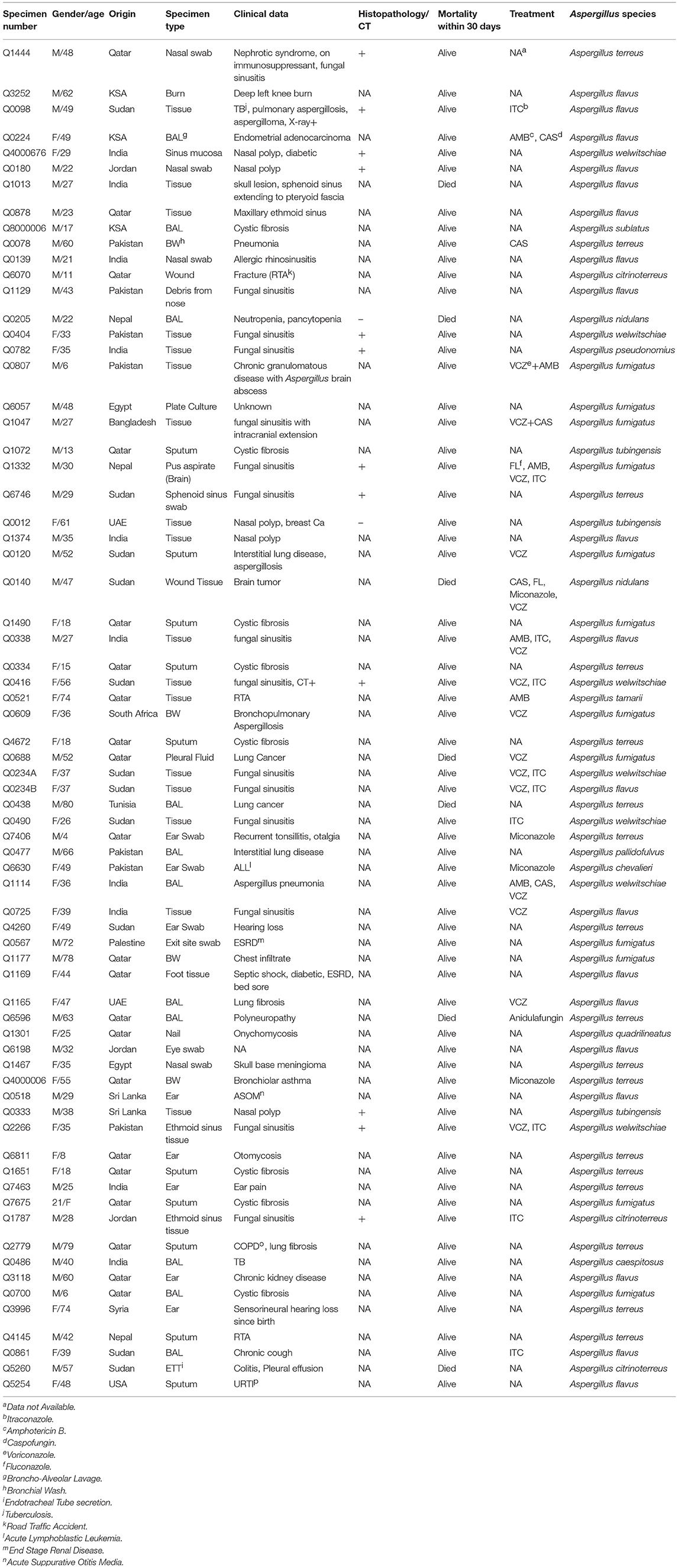
Table 1. Patients demographics, clinical data, antifungal treatment, and Aspergillus spp. isolated.
Isolation and Identification
Aspergillus species were identified by macro and microscopy according to the laboratory standard operative protocol of the microbiology laboratory at Hamad general hospital in Qatar. Specimens were cultured on Sabouraud dextrose agar (SDA; Difco Laboratories, Detroit, MI) with and without chloramphenicol. Culture plates were incubated at 26 and 37°C and were observed daily for growth up to 10 days. Direct microscopy from clinical specimens was performed using Blankophor P fluorescent stain (Bayer AG, Germany). Cultures were preserved at −70°C using cryo-tubes (Mast Diagnostics, Bootle, Merseyside, UK) until further use.
Molecular Identification
DNA Extraction
Genomic DNA was extracted as described by Bolano et al. (2001), with minor modifications. In short, Aspergillus biomass, which was grown on oatmeal agar (OA; home-made at Westerdijk Institute) for 5 days, was bead-beaten with sterile sand, 750 μl of lysis buffer, and 750 μl of phenol-chloroform in 2 ml screw-capped tube. The mixture was centrifuged and the supernatant was transferred to 1.5 ml Eppendorf's tube with an equal amount of ice-cold 96% ethanol. One hundred microliter of 3.0 M ice-cold sodium acetate was added, mixed gently, and stored at −20°C for 30–60 min. The mixture was then centrifuged at 4°C. The DNA pellet was air-dried and re-suspended in 100 μl Tris Ethylenediaminetetraacetic acid (TE) buffer. The solution was incubated successively at 37 and 65°C both for 10 min, and stored at −20°C. The DNA quality was checked by 1.5% agarose gel electrophoresis.
PCR and Sequencing
For identification of the isolates, two loci were amplified, namely β-tubulin (BenA), and calmodulin (CaM). A segment of the β-tubulin gene was amplified using primers Bt2a (5′-GGTAACCAAATCGGTGCTGCTTTC-3′) and Bt2b (5′-ACCCTCAGTGTAGTGACCCTTGGC-3′) (Glass and Donaldson, 1995), and a fragment of the calmodulin gene was amplified using primers cmd5 (5′-CCGAGTACAAGGAGGCCTTC-3′) and cmd6 (5′-CCGATAGAGGTCATAACGTGG-3′) (Hong et al., 2005). The amplification of BenA and CaM loci for some of our strains resulted in poor sequence data and these strains were identified by at least one gene (BenA or CaM). Each PCR mixture (final volume 24 μl) contained 16.45 μl water, 0.75 μl (50 mM) Magnesium chloride, 2.5 μl 10 × PCR buffer, 1.95 μl dNTP mix (1 mM), 1.25 μl dimethyl sulfoxide (DMSO), 0.5 μl of each primer (10 μM), 0.1 μl Taq polymerase (BioTaq 5 U/μL), and 1 μl of template DNA.
The PCR and sequencing reactions were performed as described previously (Visagie et al., 2014). Sequences were identified using the Basic Local Alignment Search Tool (BLAST) of The NCBI database (NCBI, 2015). A Westerdijk Institute in-house database with the latest taxonomic names and additions was also used for identification. The sequences were then deposited to the GenBank database and accession numbers are presented in Table 2.
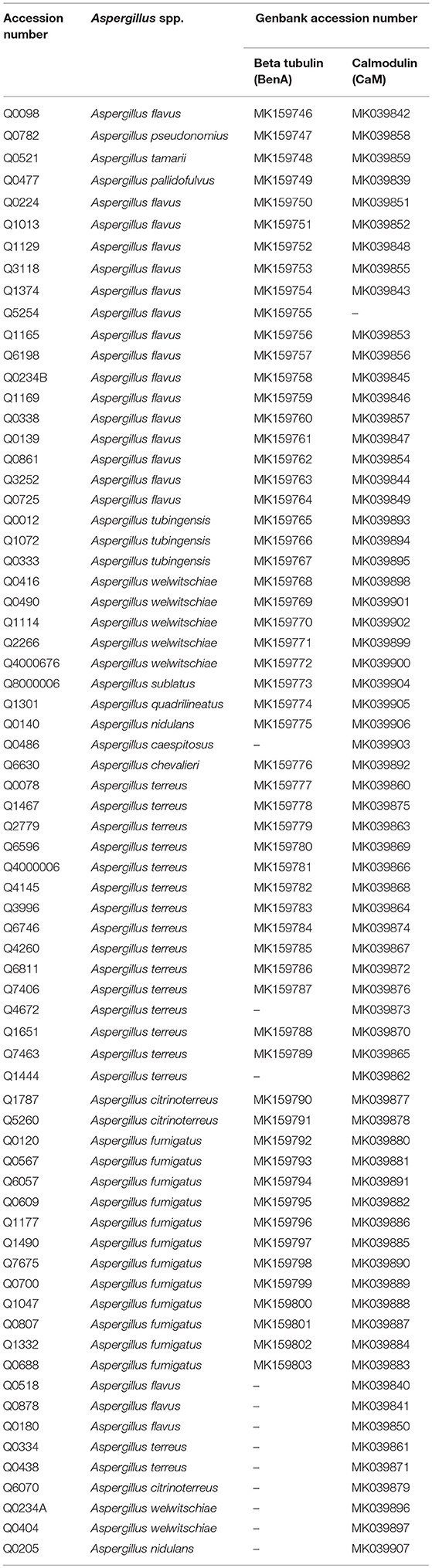
Table 2. Aspergillus spp. isolates with Genbank accession numbers.
Antifungal Susceptibility
In vitro antifungal susceptibility testing was performed according to the CLSI M38-A2 microbroth dilution method for filamentous fungi (Clinical and Laboratory Standards Institute [CLSI], 2008). The antifungal agents tested were: amphotericin B (AMB), voriconazole (VRC), itraconazole (ITC), posaconazole (PCZ) (Sigma-Aldrich, St. Louis, MO, USA), isavuconazole (ISA; Basilea Pharmaceutica, Basel, Switzerland), anidulafungin (ANID; Pfizer Pharma), and micafungin (MICA; Astellas Pharma Inc.). All antifungal drugs were tested in concentrations ranging from 0.03 to 16 μg/ml. Pichia kudriavzevii (Candida krusei) (ATCC 6258) was used as a quality control (QC) strain as indicated in CLSI M38-A2. In addition, we tested Aspergillus fumigatus (ATCC 46645), a reference strain from an official culture collection with known stable MIC values. The susceptibility plates were prepared and stored at −70°C until use. Results were read after 24 and 48 h of incubation at 37°C. The minimum inhibitory concentrations (MICs) for AMB and azoles were determined as the lowest concentration of the antifungal drug that prevents any discernable growth (100% inhibition) whereas the minimum effective concentrations (MECs) for echinocandins were defined as the lowest concentration of the antifungal drug that leads to rounded compact hyphal growth compared with the unchanged growth in the control well. Visual reading of the MICs/MECs was performed with the aid of an inverted mirror (Clinical and Laboratory Standards Institute [CLSI], 2008).
Aspergillus MICs were analyzed using the latest epidemiological cut-off values (ECVs) proposed by CLSI (Clinical and Laboratory Standards Institute [CLSI], 2018) to determine the presence of wild type (WT) and non-wild type (NWT) strains.
Results
Patients Groups and Aspergillosis
Seventy Aspergillus strains were isolated from clinical specimens obtained from 67 patients including 40 males and 27 females. The age of female and male patients ranged from 8 to 74 (media n = 36) and 4 to 80 (media n = 36.5) years old, respectively. Eight patients were under 18 years (17, 15, 13, 11, 8, 4, and 2 patients were 6 years old) and 50% (4/8) of them suffered from cystic fibrosis (Table 1).
The majority of Aspergillus species were isolated from respiratory specimens (n = 28, 40%) and nasal sinuses (n = 24, 34.3%) (Table 3). Two isolates (A. welwitschiae and A. flavus) were recovered from a patient with fungal rhinosinusitis. Three strains (1 A. fumigatus and 2 A. terreus) were isolated separately from sputum samples of a patient with cystic fibrosis with 4 months interval between isolations.
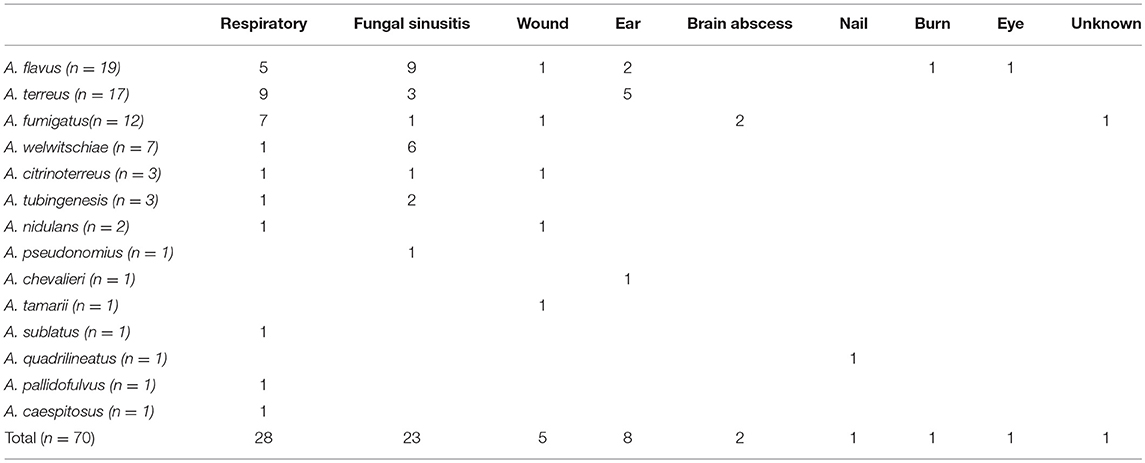
Table 3. Occurrence of Aspergillus spp. in clinical specimens.
Fourteen patients (20.9%) presented with IA and 55 patients with non-invasive infections. The underlying conditions of these patients were immune suppression (cancer, on immunosuppressant drugs, and diabetes), chronic pulmonary disease (tuberculosis and cystic fibrosis), pneumonia, rhinosinusitis, and onychomycosis, in addition to ear, wound, skin, and eye infections. Seventeen patients were immunocompromised (24.3%) and seven patients (10.4%) died within 30 days of diagnosis irrespective of antifungal treatment. Two of the deceased patients were infected with Aspergilus terreus, 2 with Aspergillus nidulans, and 3 patients each with Aspergillus citrinoterreus, A. flavus, and A. fumigatus, respectively. Patients' demographics, clinical information and Aspergillus species isolated are listed in Table 1.
Fourteen Aspergillus species belonging to seven sections were recovered (Table 1). In addition, we detected cryptic Aspergillus species in 29% of our isolates (n = 20) which belong to 6 species complexes namely A. welwitschiae (n = 7, 10%) (section Nigri), Aspergillus tubingensis (n = 3, 4.3%) (section Nigri), A. citrinoterreus (n = 3, 4.3%) (section Terrei), A. pseudonomius (n = 1, 1.4%) (section Flavi), Aspergillus chevalieri (n = 1, 1.4%) (section Aspergillus), A. sublatus (1.4%) (section Nidulantes), Aspergillus quadrilineatus (1.4%) (section Nidulantes), Aspergillus pallidofulvus (1.4%) (section Circumdati), Aspergillus tamarii (1.4%) (section Flavi) and Aspergillus caespitosus (1.4%) (section Nidulantes).
A. welwitschiae was the most isolated cryptic species (n = 7, 35%), followed by A. tubingensis and A. citrinoterreus (each n = 3, 15%) A. terreus was isolated from 62.5% (5/8) of the ear specimens and 47.4% (9/19) of A. flavus isolates were recovered from patients presented with fungal rhinosinusitis.
Antifungal Susceptibility
All the MICs were within the required ranges for the QC and reference strains tested. Since there are no Clinical Break Points (CBPs) available for Aspergillus spp. by the CLSI, MIC data were analyzed and interpreted according to the ECVs indicated in the CLSI M59-ED2 (Clinical and Laboratory Standards Institute [CLSI], 2018). There are neither CPBs nor ECVs available for ANID and MICA.
One isolate of A. fumigatus showed a MIC of 2.0 μg/ml for ITC and was therefore categorized as NWT (ECV = 1). Another A. fumigatus strain exhibited high MEC values for ANID and MICA (4 and 16 μg/ml, respectively). One A. flavus showed an elevated MIC of 16 μg/ml for AMB and was considered to be NWT (ECV = 4). All A. nidulans isolated (n = 2) had elevated MICs of 2.0 μg/ml to AMB. Antifungal susceptibilities were not determined for A. chevalieri since it repeatedly failed to grow in the susceptibility test medium. The antifungal susceptibility data are presented in Table 4.
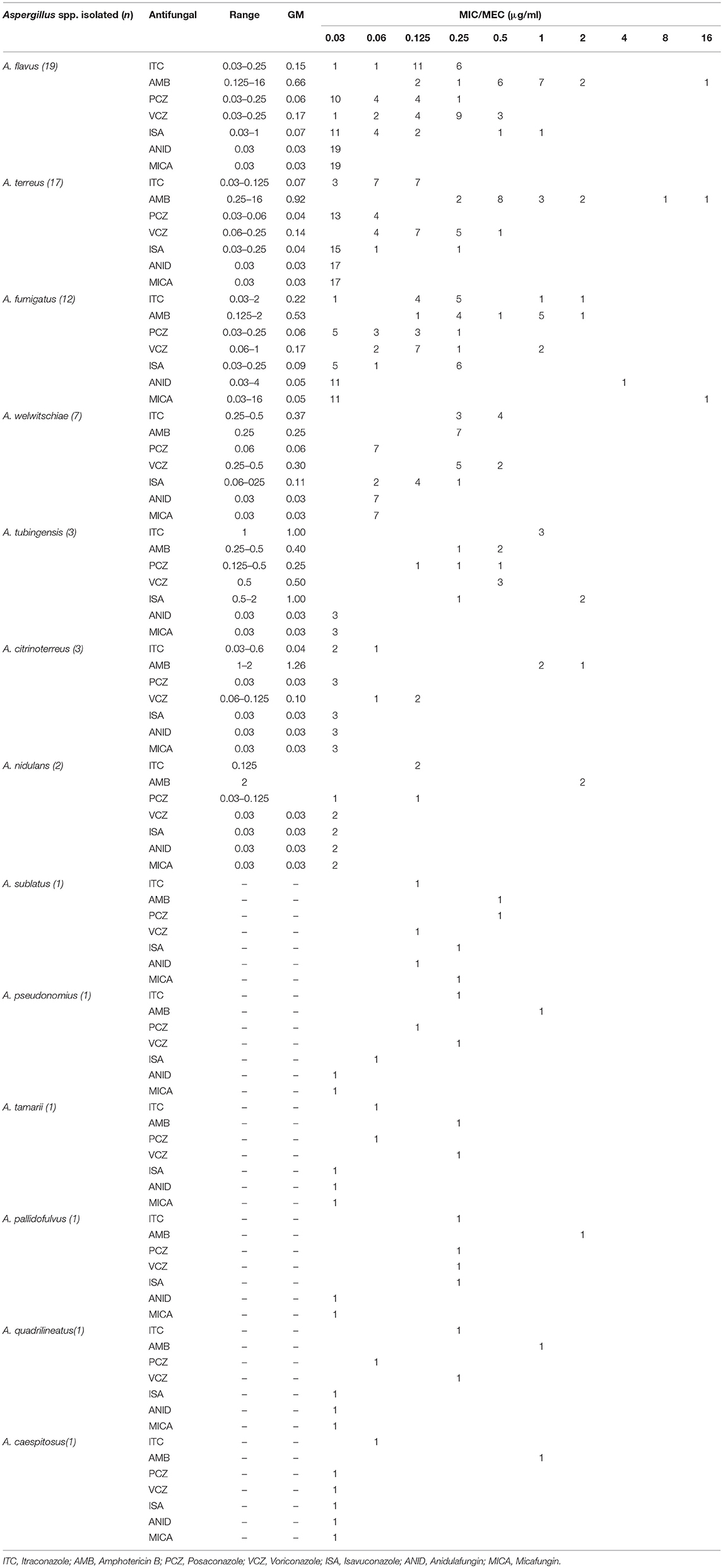
Table 4. In vitro antifungal susceptibility results of Aspergillus spp.
For all Aspergillus isolates, the range of MICs/MECs for triazoles, AMB, and echinocandins were: ITC (0.03–2.0 μg/ml), PCZ (0.03–0.5 μg/ml), VRC (0.03–1 μg/ml), ISA (0.03–2.0 μg/ml), AMB (0.125–16 μg/ml), ANID (0.03–4.0 μg/ml) and MICA (0.03–16 μg/ml). The overall geometric mean (GM), MIC50 and MIC90 are listed in Table 5.
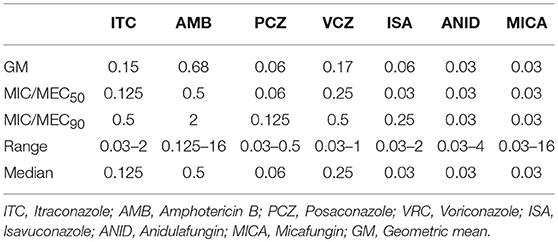
Table 5. Geometric mean (GM), MIC/MEC50/90, range and median of Aspergillus MICs.
Discussion
The present study describes the molecular identification and susceptibility patterns of 70 Aspergillus strains isolated from clinical specimens of 67 patients from Hamad general hospital in Qatar, including adults (88%) and pediatric patients (12%). To our knowledge, this is considered as the first study exploring the molecular identification and antifungal susceptibility profiles of clinical aspergilli in this country.
Twenty isolates (29%) of cryptic Aspergillus spp. were recovered from patients' samples representing 10 different species that belong to six sections. Previous studies from Spain and Brazil reported a prevalence of 14.5% (Alastruey-Izquierdo et al., 2013) and 19% (Negri et al., 2014) for cryptic Aspergillus spp., respectively, which is lower than what we found in the current study. The majority of the cryptic species isolated in this study were members of section Nigri (n = 10/20, 50%). No cryptic species were isolated from section Fumigati.
Aspergillus pseudonomius is reported in the current study for the first time ever from clinical specimens and was isolated from a patient with fungal rhinosinusitis proven by histopathology. It exhibited low MIC values for all the antifungal drugs tested (Table 4). Echinocandins were the most active drugs (MEC = 0.03 μg/ml) and ISA was the most active triazole drug against A. pseudonomius with a MIC of 0.06 μg/ml.
In addition, we report the first isolation of A. welwitschiae from six patients with fungal rhinosinusitis, three of them were proven by histopathology and one by computed tomography (CT) as invasive infections. A. welwitschiae was previously isolated from patients with respiratory infections (Pinto et al., 2018) and onychomycosis (Tsang et al., 2016). Low MICs were observed for all of the antifungal agents investigated and PCZ was the most active triazole with a MIC of 0.06 μg/ml. A. welwitschiae was also isolated in our study from a BAL of a patient with Aspergillus pneumonia.
Invasive infections caused by A. sublatus were previously reported from patients with HSCT (de Fontbrune et al., 2014; Chrenkova et al., 2018). Here we report it for the first time from BAL specimen of an adult cystic fibrosis patient with moderate obstructive pulmonary disease. However, we were unable to discern between colonization and infection caused by A. sublatus. Echinocandins MICs were relatively higher for A. sublatus compared to the other Aspergillus spp. in our set, with MIC values of 0.125 and 0.25 μg/ml for ANID and MICA, respectively. Previously reported MICs of ANID and MICA for A. sublatus were <0.0312 μg/ml (Chrenkova et al., 2018) which is lower than our findings. ITC and voriconazole were the most active triazoles with MICs of 0.125 μg/ml for both drugs (Table 4). A. sublatus belongs to Aspergillus section Nidulantes and is very closely related to A. quadrilineatus (Hubka et al., 2016). These species are indistinguishable by sequencing BenA alone (Hubka et al., 2016), whereas reliable identification can be achieved by sequencing CaM gene (Hubka et al., 2016). In our case, we identified A. sublatus by sequencing both BenA and CaM genes. AMB exhibited low MIC (0.5 μg/ml) in comparison to A. nidulans (2.0 μg/ml) which is known to be resistant to AMB (Van't Hek et al., 1998; Kontoyiannis et al., 2002; Bowman et al., 2006). A low AMB MIC was also reported in other studies for A. sublatus (de Fontbrune et al., 2014; Chrenkova et al., 2018).
Aspergillus pallidofulvus was isolated in the present study from a BAL sample of a patient with interstitial lung disease, which is considered as the second report of this species from clinical specimens after a previous report from India where it was isolated from a BAL sample of a patient with invasive pulmonary aspergillosis (IPA) (Masih et al., 2016). The single strain isolated in the current study showed a high MIC value for AMB (2 μg/ml), which was also observed previously for this species (Masih et al., 2016). With the available data, it was not possible to recognize A. pallidofulvus as the cause of infection or colonization.
The recently described A. citrinoterreus, which belongs to section Terrei, was reported mainly from patients with respiratory infections, in addition to wound, abscess, nail and sinus infections (Guinea et al., 2015; Imbert et al., 2018; Vaezi et al., 2018). In a global study of 498 strains of A. terreus and phenotypically related species, 6 different species of section Terrei were identified and A. citrinoterreus was the second most isolated species (8.4%) (Zoran et al., 2018). In our case, among 20 strains of members of section Terrei, 3 strains (15%) were identified as A. citrinoterreus. We report the second isolation of this species from a case of fungal rhinosinusitis which was proven by histology. This patient was treated with ITC which exhibited a low in vitro MIC of 0.03 μg/ml and for AMB 1 μg/ml. However, there were no data available regarding the therapeutic outcome. The second isolate of A. citrinoterreus was from an endotracheal secretion of a patient with colitis and pleural effusion, with no other details about the underlying diseases or the immune status. Antifungal therapy information was not available for this patient who died few days after sample collection, and low MICs were observed (Table 4) for all the tested drugs including AMB MIC of 1 μg/ml. The third case of A. citrinoterreus was from a wound sample of a patient who had a road traffic accident. Antifungal therapy details were not available and the isolate showed low MICs in vitro except for AMB which showed an elevated MIC of 2 μg/ml. It was not possible to categorize the later 2 cases as infection or colonization.
Aspergillus tamarii is rarely encountered as a human pathogen. It was reported from few cases of cutaneous aspergillosis (Sharma et al., 2013; Kimura et al., 2018), onychomycosis (Kristensen et al., 2005), burn wound (Renner et al., 2018), keratitis (Kredics et al., 2007), respiratory (Castro et al., 2019) and sinus infections (Paludetti et al., 1992). In the current study, we report the isolation of A. tamarii from wound tissue of a patient who experienced a road traffic accident. This patient received AMB with unknown treatment outcome and the in vitro MIC of AMB was 0.25 μg/ml. We could not determine whether Aspergillus tamarii was the cause of infection or a colonizer.
Aspergillus chevalieri is one of the most common species present in indoor environments (Hubka et al., 2013). Clinically, it has been recovered from a case of cutaneous aspergillosis (Naidu and Singh, 1994), a fatal cerebral aspergillosis case (Masih et al., 2016), and respiratory, corneal and sinus infections (Siqueira et al., 2018). In our study, we isolated A. chevalieri from an ear swab of a patient with acute lymphoblastic leukemia (ALL). The patient received miconazole, a topical antifungal drug.
Aspergillus tubingensis was found to be a major fungus associated with bronchial colonization in patients with lung disease (Reynaud-Gaubert et al., 2016). Previous reports of A. tubingensis were from patients with cutaneous aspergillosis (Balajee et al., 2009; Pagiotti et al., 2010), otomycosis (Szigeti et al., 2012a,b), keratitis (Dóczi et al., 2009), onychomycosis (Nouripour-Sisakht et al., 2015), and osteomyelitis (Hedayati et al., 2007). We recovered A. tubingensis from three patients: one with unknown underlying diseases presented with fungal rhinosinusitis and was proven by histopathology. The second patient suffered from breast cancer and presented with rhinosinusitis. It was considered as either colonization or the allergic type of Aspergillus rhinosinusitis due to the negative histology investigation. The third patient had cystic fibrosis with unknown status of invasion or colonization. The antifungal therapy data were unavailable for those patients. In general, low antifungal MICs were exhibited for A. tubingensis strains except for ISA which showed high MIC of 2.0 μg/ml for the first and the second cases. No A. niger sensu stricto was isolated in our set of strains.
Invasive aspergillosis caused by A. quadrilineatus, which is closely related to A. nidulans, was previously reported from 2 patients who presented with fungal rhinosinusitis and had undergone bone marrow transplantation for hematological malignancy (Polacheck et al., 1992; Drakos et al., 1993), three cases of IPA in patients with CGD (Verweij et al., 2008), a patient with cerebral aspergillosis (Verweij et al., 2008) and another with onychomycosis (Gugnani et al., 2004). Our isolate was recovered from a case of onychomycosis, however, it was not possible to confirm that A. quadrilineatus was the direct cause of infection or colonization. A lower MIC value for AMB was observed (1 μg/ml) in comparison to A. nidulans (2 μg/ml) which is in agreement with a previous report (Verweij et al., 2008).
Aspergillus caespitosus is a soil fungus (Raper and Thoms, 1944; Chen et al., 2016) and has not been reported previously as a human pathogen. In the current study, it was isolated from a BAL specimen of a patient suffering from tuberculosis and showed low MICs for all the antifungal drugs tested. It was unknown whether A. caespitosus was the cause of true infection or colonization.
Aspergillus fumigatus has been reported as the most prevalent species causing IA in different parts of the world, including the United States, Europe and Brazil (Balajee et al., 2009; Alastruey-Izquierdo et al., 2013; Negri et al., 2014). In this study, A. flavus was the most prevalent species (27%), which is consistent with reports from India (47%) (Xess et al., 2004), Iran (75%) (Zanganeh et al., 2018), and Tunisia (79%) (Hadrich et al., 2010). The predominance of A. flavus in these parts of the world is attributed to arid and semi-arid climates (Kameswaran et al., 1992; Hedayati et al., 2007). The second most prevalent species in our set was A. terreus (24%), followed by A. fumigatus (17%). This could be due to ecological preferences for environments specific to Qatar, such as the highly arid deserts, which needs to be investigated thoroughly by an environmental sampling of different ecological niches. A. terreus and A. fumigatus were the most isolated species (29%) from immunocompromised patients and A. terreus was the most recovered species from respiratory samples (9/27, 33%), followed by A. fumigatus (6/27, 22%). Infections caused by A. terreus are of concern due to its reduced susceptibility to AMB in vitro and in vivo (Sutton et al., 1999; Walsh et al., 2003). This species was also found to be prevalent in Tyrol, Austria, from environmental and clinical sources (Lass-Florl et al., 2005; Lackner et al., 2016). Moreover, a previous multicentre study from the United States reported that the incidence of A. terreus following HSCT and SOT was found to be 16 and 11.8%, respectively (Morgan et al., 2005).
The majority of Aspergillus spp. were isolated from patients with non-invasive infections and a low rate of IA was observed in our study. Aspergillus rhinosinusitis was the second highest clinical presentation (23/67, 34.3%) after respiratory infections. These findings are in accordance with a report by Taj-Aldeen et al. (2015), which estimated the burden of fungal infections in Qatar (Taj-Aldeen et al., 2015). The study reported that Aspergillus rhinosinusitis in Qatar has a relatively high rate (2.31 cases/100,000 individuals). This is attributed to the hot and arid climate in the country and atopic young patients who develop allergic Aspergillus rhinosinusitis, in addition to the high number of residents who came from countries with elevated incidences of Aspergillus rhinosinusitis (Taj-Aldeen et al., 2003, 2004, 2015). The human population of Qatar is extremely mixed with high number of Southeast Asians, particularly Indians. In our set, the majority (13/23, 57%) of patients affected with Aspergillus rhinosinusitis originated from Southeast Asia and more than half of them (n = 7/13, 54%) were from India. Additionally, 4/13 (31%), patients were from Sudan. Previous reports showed that Aspergillus rhinosinusitis is common in these regions (Milošev et al., 1969; El Daoud et al., 1973; Chatterjee and Chakrabarti, 2010; Garg et al., 2013; Chakrabarti et al., 2015; Jain et al., 2015; Krishnan et al., 2015; Mahgoub et al., 2016). Two patients with Aspergillus rhinosinusitis, one of which infected with A. flavus and the other by A. fumigatus, died due to extension of the fungus to the brain (Table 1). Two patients were immunocompromised, one patient who was infected with A. tubingensis suffered from breast cancer. The other patient presented with nephrotic syndrome and received immunosuppressive therapy, and was infected with A. terreus. The latter case was proven by histology (Table 1).
Taj-Aldeen et al. (2015) also showed that among respiratory aspergillosis in Qatar the rate of infection for chronic pulmonary aspergillosis post-tuberculosis (CPA-TB) was 0.75/100 000 and the other CPA was 26.82/100,000. Allergic bronchopulmonary aspergillosis (ABPA) and severe asthma with fungal sensitization (SAFS) were more common at 60.2/100 000 and 79.46/100 000, respectively (Taj-Aldeen et al., 2015). We were unable to retrieve the complete set of clinical details about the manifestation of aspergillosis. The available clinical presentations are presented in Table 1. Overall, most of the isolates showed low MIC values for the systemic antifungal agents investigated. PCZ was the most active drug with MICs ranging from 0.03 to 0.5 μg/ml (Table 5). Echinocandins are generally potent against Aspergillus spp. and are used as salvage therapy or in combination with other classes of antifungal drugs (Patterson et al., 2016). However, a recent report detected a point mutation in the fks1 gene of a strain of A. fumigatus, which caused echinocandin resistance and subsequent treatment failure (Jimenez-Ortigosa et al., 2017). We observed echinocandin resistance in one strain of A. fumigatus with high MECs for ANID and MICA i.e., 4.0 and 16 μg/ml, respectively. Another strain of A. fumigatus showed a MIC of 2.0 μg/ml for ITC and was categorized as NWT based on CLSI ECVs (Clinical and Laboratory Standards Institute [CLSI], 2018). VRC, POS, and ISA MICs for the same strain were 1, 0.25 and 0.25 μg/ml, respectively, which were categorized as WT based on CLSI ECVs (Espinel-Ingroff et al., 2010). These findings need to be investigated by analyzing the molecular mechanism(s) of resistance. One A. flavus strain showed high MIC of 16 μg/ml for AMB and therefore is considered to be non-wild type (NWT) based on CLSI ECVs. Previous studies have shown that in vitro resistance of A. flavus to AMB is correlated with treatment failure (Hadrich et al., 2012; Barchiesi et al., 2013). Most of the A. terreus strains, a species that is considered as intrinsically resistant to AMB (Lass-Florl et al., 2005), showed high MIC values for AMB (range; 0.25–8.0 μg/ml). A. chevalieri failed to grow in susceptibility medium due to its xerophilic nature, therefore, no MIC values were determined.
Patients' therapeutic outcome was not calculated in our study since the data set was incomplete. We were able to retrieve the antifungal therapeutic regimes for 26 out of 67 patients indicated in Table 1. Therapy was dependent on the site of infection and underlying disease. In short, patients with IA (n = 6): 2 received ITC, 2 ITC, and VCZ, 1 received ITC in addition to AMB, VCZ and fluconazole, and 1 was treated with VCZ and caspofungin; immunocompromised patients (n = 5): 1 was treated with AMB and caspofungin, 1 with VCZ and AMB, 1 with caspofungin, fluconazole, miconazole and VCZ, and 2 patients each with VCZ and miconazole; patients diagnosed with fungal rhinosinusitis (n = 9): 8 received either VCZ and/or ITC, and 1 treated with VCZ in addition to caspofungin. Patients with respiratory Aspergillus infection or colonization (n = 11): 4 received VCZ, 2 treated with ITC, 1 with caspofungin, 1 with caspofungin and AMB, 1 with AMB, caspofungin and VCZ, 1 with ANID, and 1 patient received miconazole probably for a superficial infection. Among 3 patients who died within 30 days of diagnosis, 1 was treated with caspofungin, miconazole and VCZ, 1 with VCZ, and 1 with ANID. For patients treated with multiple antifungal drugs, it was unknown whether the drugs were administered singly or in combinations.
The current study highlights the molecular identification and antifungal susceptibility profiles of 70 clinical Aspergillus species in Qatar. Future studies with larger sample size, including clinical and environmental samples, would provide more insight into the epidemiology of clinical aspergilli in the country.
Conclusion
In conclusion, we report the molecular identification and in vitro antifungal susceptibility profiles of 70 Aspergillus spp. recovered from various clinical specimens in Qatar. Rare and cryptic Aspergillus species with variable antifungal susceptibilities were detected. Triazole resistance, and recently Echinocandin resistance, is emerging in many parts of the world. Further investigation of resistance mechanism(s) is warranted for species with reduced susceptibilities to antifungal drugs. Infectious disease physicians must be aware of the emerging and resistant species to decide on accurate treatment and improved clinical outcomes.
Data Availability
The datasets generated for this study were deposited in Genbank. The accession numbers are listed in Table 2.
Author Contributions
HS performed the technical work and wrote the manuscript draft. JH, ML, and BT provided technical assistance. ST-A and TB assisted in designing the manuscript and writing the first draft. MA and CL-F advised on clinical aspects of the manuscript. All authors contributed to manuscript revision, editing, and approved the submitted version.
Funding
This study was supported by Qatar National Research Fund (QNRF), a member of Qatar Foundation, grant: NPRP 5-298-3-086.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
Abdolrasouli, A., Petrou, M. A., Park, H., Rhodes, J. L., Rawson, T. M., Moore, L. S. P., et al. (2018). Surveillance for azole-resistant Aspergillus fumigatus in a centralized diagnostic mycology service, London, United Kingdom, 1998–2017. Front. Microbiol. 9:2234. doi: 10.3389/fmicb.2018.02234
Abers, M. S., Ghebremichael, M. S., Timmons, A. K., Warren, H. S., Poznansky, M. C., and Vyas, J. M. (2016). A critical reappraisal of prolonged neutropenia as a risk factor for invasive pulmonary aspergillosis. Open forum Infect. Dis. 3:ofw036. doi: 10.1093/ofid/ofw036
Ahmad, S., Joseph, L., Hagen, F., Meis, J. F., and Khan, Z. (2015). Concomitant occurrence of itraconazole-resistant and -susceptible strains of Aspergillus fumigatus in routine cultures. J. Antimicrob. Chemother. 70, 412–415. doi: 10.1093/jac/dku410
Ahmad, S., Khan, Z., Hagen, F., and Meis, J. F. (2014). Occurrence of triazole-resistant Aspergillus fumigatus with TR34/L98H mutations in outdoor and hospital environment in Kuwait. Environ. Res. 133, 20–26. doi: 10.1016/j.envres.2014.05.009
Alastruey-Izquierdo, A., Mellado, E., and Cuenca-Estrella, M. (2012). Current section and species complex concepts in Aspergillus: recommendations for routine daily practice. Ann. N. Y. Acad. Sci. 1273, 18–24. doi: 10.1111/j.1749-6632.2012.06822.x
Alastruey-Izquierdo, A., Mellado, E., Pelaez, T., Peman, J., Zapico, S., Alvarez, M., et al. (2013). Population-based survey of filamentous fungi and antifungal resistance in Spain (FILPOP Study). Antimicrob. Agents Chemother. 57, 3380–3387. doi: 10.1128/AAC.00383-13
Baddley, J. W., Andes, D. R., Marr, K. A., Kontoyiannis, D. P., Alexander, B. D., Kauffman, C. A., et al. (2010). Factors associated with mortality in transplant patients with invasive aspergillosis. Clin. Infect. Dis. 50, 1559–1567. doi: 10.1086/652768
Balajee, S. A., Kano, R., Baddley, J. W., Moser, S. A., Marr, K. A., Alexander, B. D., et al. (2009). Molecular identification of Aspergillus species collected for the Transplant-Associated Infection Surveillance Network. J. Clin. Microbiol. 47, 3138–3141. doi: 10.1128/JCM.01070-09
Barchiesi, F., Spreghini, E., Sanguinetti, M., Giannini, D., Manso, E., Castelli, P., et al. (2013). Effects of amphotericin B on Aspergillus flavus clinical isolates with variable susceptibilities to the polyene in an experimental model of systemic aspergillosis. J. Antimicrob. Chemother. 68, 2587–2591. doi: 10.1093/jac/dkt232
Beaute, J., Obenga, G., Le Mignot, L., Mahlaoui, N., Bougnoux, M.-E., Mouy, R., et al. (2011). Epidemiology and outcome of invasive fungal diseases in patients with chronic granulomatous disease: a multicenter study in France. Pediatr. Infect. Dis. J. 30, 57–62. doi: 10.1097/INF.0b013e3181f13b23
Berkow, E. L., Nunnally, N. S., Bandea, A., Kuykendall, R., Beer, K., and Lockhart, S. R. (2018). Detection of TR34/L98H CYP51A mutation through passive surveillance for azole-resistant Aspergillus fumigatus in the United States from 2015 to 2017. Antimicrob. Agents Chemother. 62:e02240–17. doi: 10.1128/AAC.02240-17
Bolano, A., Stinchi, S., Preziosi, R., Bistoni, F., Allegrucci, M., Baldelli, F., et al. (2001). Rapid methods to extract DNA and RNA from Cryptococcus neoformans. FEMS Yeast Res. 1, 221–224. doi: 10.1016/S1567-1356(01)00030-7
Bowman, J. C., Abruzzo, G. K., Flattery, A. M., Gill, C. J., Hickey, E. J., Hsu, M. J., et al. (2006). Efficacy of caspofungin against Aspergillus flavus, Aspergillus terreus, and Aspergillus nidulans. Antimicrob. Agents Chemother. 50, 4202–4205. doi: 10.1128/AAC.00485-06
Buil, J. B., Snelders, E., Denardi, L. B., Melchers, W. J. G., and Verweij, P. E. (2019). Trends in azole resistance in Aspergillus fumigatus, the Netherlands, 1994–2016. Emerg. Infect. Dis. 25, 176–178. doi: 10.3201/eid2501.171925
Castro, C., Galán-Sanchez, F., Linares, M. J., Tejero, R., Ruiz, M., Serrano, M. L., et al. (2019). A prospective survey of Aspergillus spp. in respiratory tract samples: species identification and susceptibility patterns. Med. Mycol. 57, 412–420. doi: 10.1093/mmy/myy080
Chakrabarti, A., Rudramurthy, S. M., Panda, N., Das, A., and Singh, A. (2015). Epidemiology of chronic fungal rhinosinusitis in rural India. Mycoses. 58, 294–302. doi: 10.1111/myc.12314
Chatterjee, S. S., and Chakrabarti, A. (2010). Epidemiology and medical mycology of fungal Rhinosinusitis. Otorhinolaryngol. Clin. An Int. J. 13, 1–14. doi: 10.5005/jp-journals-10003-1001
Chaturvedi, R., Kolhe, A., Pardeshi, K., Naik, L., and Wanjare, S. (2017). Primary cutaneous aspergillosis, mimicking malignancy, a rare presentation in an immunocompetent patient. Diagn. Cytopathol. 46, 434–437. doi: 10.1002/dc.23869
Chen, A. J., Frisvad, J. C., Sun, B. D., Varga, J., Kocsubé, S., Dijksterhuis, J., et al. (2016). Aspergillus section Nidulantes (formerly Emericella): polyphasic taxonomy, chemistry and biology. Stud. Mycol. 84, 1–118. doi: 10.1016/j.simyco.2016.10.001
Chowdhary, A., Sharma, C., Kathuria, S., Hagen, F., and Meis, J. F. (2015). Prevalence and mechanism of triazole resistance in Aspergillus fumigatus in a referral chest hospital in Delhi, India and an update of the situation in Asia. Front. Microbiol. 6:428. doi: 10.3389/fmicb.2015.00428
Chowdhary, A., Sharma, C., van den Boom, M., Yntema, J. B., Hagen, F., Verweij, P. E., et al. (2014). Multi-azole-resistant Aspergillus fumigatus in the environment in Tanzania. J. Antimicrob. Chemother. 69, 2979–2983. doi: 10.1093/jac/dku259
Chrenkova, V., Hubka, V., Cetkovsky, P., Kouba, M., Weinbergerova, B., Lyskova, P., et al. (2018). Proven invasive pulmonary aspergillosis in stem cell transplant recipient due to Aspergillus sublatus, a cryptic species of A. nidulans. Mycopathologia 183, 423–429. doi: 10.1007/s11046-017-0223-8
Clinical and Laboratory Standards Institute [CLSI] (2008). Reference Method for Broth Dilution Antifungal Susceptibility Testing of Filamentous Fungi. 2nd Edn. Wayne, PA: Clinical and Laboratory Standard Institute.
Clinical and Laboratory Standards Institute [CLSI] (2018). Epidemiological Cutoff Values for Antifungal Susceptibility Testing. 2nd Edn. Wayne, PA: Clinical and Laboratory standards Institute.
de Fontbrune, F. S., Denis, B., Meunier, M., Garcia-Hermoso, D., Bretagne, S., and Alanio, A. (2014). Iterative breakthrough invasive aspergillosis due to TR(34) /L98H azole-resistant Aspergillus fumigatus and Emericella sublata in a single hematopoietic stem cell transplant patient. Transpl. Infect. Dis. 16, 687–691. doi: 10.1111/tid.12231
Dóczi, I., Németh, T. M., Bhaskar, M., Samson, R. A., Rajaraman, R., Venkatapathy, N., et al. (2009). Infectious keratitis caused by Aspergillus tubingensis. Cornea 28, 951–954. doi: 10.1097/ico.0b013e3181967098
Drakos, P. E., Or, A. N. R., Naparstek, E., Kapelushnik, J. D., Engelhard, G., Rahav, D. N., et al. (1993). Invasive fungal sinusitis in patients undergoing bone marrow transplantation. Bone Marrow Transplant. 12, 203–208.
El Daoud, S., El Tayeb, A. A., Malik, O. A., Veress, B., El Hassan, A. M., and Mahgoub, E. S. (1973). Further observations on the primary paranasal Aspergillus granuloma in the Sudan: a morphological study of 46 cases. Am. J. Trop. Med. Hyg. 22, 765–772. doi: 10.4269/ajtmh.1973.22.765
Emiralioglu, N., Ozcan, H. N., Orhan, D., Haliloglu, M., Cengiz, A. B., Yalcin, E. E., et al. (2017). Chronic necrotizing pulmonary aspergillosis in an immunocompetent patient after the surgery of hydatid cyst. Tuberk. Toraks 65, 157–160. doi: 10.5578/tt.13957
Espinel-Ingroff, A., Diekema, D. J., Fothergill, A., Johnson, E., Pelaez, T., Pfaller, M. A., et al. (2010). Wild-type MIC distributions and epidemiological cutoff values for the triazoles and six Aspergillus spp. for the CLSI broth microdilution method (M38-A2 document). J. Clin. Microbiol. 48, 3251–3257. doi: 10.1128/JCM.00536-10
Garcia-Vidal, C., Peghin, M., Cervera, C., Gudiol, C., Ruiz-Camps, I., Moreno, A., et al. (2015). Causes of death in a contemporary cohort of patients with invasive aspergillosis. PLoS ONE 10:e0120370. doi: 10.1371/journal.pone.0120370
Garg, S., Songara, P., Sherwal, B. L., Agarwal, S., Rakshit, P., and Kumar, S. (2013). Fungal rhinosinusitis in Delhi-National Capital Region. Clin. Rhinol. 6, 28–31. doi: 10.5005/jp-journals-10013-1144
Gerson, S. L., Talbot, G. H., Hurwitz, S., Strom, B. L., Lusk, E. J., and Cassileth, P. A. (1984). Prolonged granulocytopenia: the major risk factor for invasive pulmonary aspergillosis in patients with acute leukemia. Ann. Intern. Med. 100, 345–351.
Glass, N. L., and Donaldson, G. C. (1995). Development of primer sets designed for use with the PCR to amplify conserved genes from filamentous ascomycetes. Appl. Environ. Microbiol. 61, 1323–1330.
Gugnani, H. C., Vijayan, V. K., Tyagi, P., Sharma, S., Stchigel, A. M., and Guarro, J. (2004). Onychomycosis due to Emericella quadrilineata. J. Clin. Microbiol. 42, 914–916. doi: 10.1128/JCM.42.2.914-916.2004
Guinea, J., Sandoval-Denis, M., Escribano, P., Pelaez, T., Guarro, J., and Bouza, E. (2015). Aspergillus citrinoterreus, a new species of section Terrei isolated from samples of patients with nonhematological predisposing conditions. J. Clin. Microbiol. 53, 611–617. doi: 10.1128/JCM.03088-14
Guinea, J., Torres-Narbona, M., Gijon, P., Munoz, P., Pozo, F., Pelaez, T., et al. (2010). Pulmonary aspergillosis in patients with chronic obstructive pulmonary disease: incidence, risk factors, and outcome. Clin. Microbiol. Infect. 16, 870–877. doi: 10.1111/j.1469-0691.2009.03015.x
Hadrich, I., Makni, F., Neji, S., Cheikhrouhou, F., Bellaaj, H., Elloumi, M., et al. (2012). Amphotericin B in vitro resistance is associated with fatal Aspergillus flavus infection. Med. Mycol. 50, 829–834. doi: 10.3109/13693786.2012.684154
Hadrich, I., Makni, F., Sellami, H., Cheikhrouhou, F., Sellami, A., Bouaziz, H., et al. (2010). Invasive aspergillosis: epidemiology and environmental study in haematology patients (Sfax, Tunisia). Mycoses 53, 443–447. doi: 10.1111/j.1439-0507.2009.01710.x
Hedayati, M. T., Pasqualotto, A. C., Warn, P. A., Bowyer, P., and Denning, D. W. (2007). Aspergillus flavus: human pathogen, allergen and mycotoxin producer. Microbiology 153, 1677–1692. doi: 10.1099/mic.0.2007/007641-0
Hong, S.-B., Go, S.-J., Shin, H.-D., Frisvad, J. C., and Samson, R. A. (2005). Polyphasic taxonomy of Aspergillus fumigatus and related species. Mycologia 97, 1316–1329. doi: 10.1080/15572536.2006.11832738
Hubka, V., Kolarík, M., Kubátová, A., and Peterson, S. W. (2013). Taxonomic revision of Eurotium and transfer of species to Aspergillus. Mycologia 105, 912–937. doi: 10.3852/12-151
Hubka, V., Nováková, A., Peterson, S. W., Frisvad, J. C., Sklenár, F., Matsuzawa, T., et al. (2016). A reappraisal of Aspergillus section Nidulantes with descriptions of two new sterigmatocystin-producing species. Plant Syst. Evol. 302, 1267–1299. doi: 10.1007/s00606-016-1331-5
Imbert, S., Normand, A. C., Ranque, S., Costa, J. M., Guitard, J., Accoceberry, I., et al. (2018). Species identification and in vitro antifungal susceptibility of Aspergillus terreus species complex clinical isolates from a french multicenter study. Antimicrob. Agents Chemother. 62, e02315–e02317. doi: 10.1128/AAC.02315-17
Jain, R., Singhal, S. K., Singla, N., Punia, R. S., and Chander, J. (2015). Mycological profile and antifungal susceptibility of fungal isolates from clinically suspected cases of fungal rhinosinusitis in a tertiary care hospital in North India. Mycopathologia. 180, 51–59. doi: 10.1007/s11046-015-9873-6
Jimenez-Ortigosa, C., Moore, C., Denning, D. W., and Perlin, D. S. (2017). Emergence of echinocandin resistance due to a point mutation in the fks1 gene of Aspergillus fumigatus in a patient with chronic pulmonary aspergillosis. Antimicrob. Agents Chemother. 61:17. doi: 10.1128/AAC.01277-17
Kameswaran, M., Al-Wadei, A., Khurana, P., and Okafor, B. C. (1992). Rhinocerebral aspergillosis. J. Laryngol. Otol. 106, 981–985.
Kimura, H., Mitsuto, I., Taguchi, R., Anzawa, K., and Mochizuki, T. (2018). Primary cutaneous aspergillosis caused by Aspergillus tamarii in a premature infant with extremely low birthweight: a case report with short review. J. Dermatol. 45, 622–625. doi: 10.1111/1346-8138.14263
Kontoyiannis, D. P., Lewis, R. E., May, G. S., Osherov, N., and Rinaldi, M. G. (2002). Aspergillus nidulans is frequently resistant to amphotericin B. Mycoses 407, 406–407. doi: 10.1046/j.1439-0507.2002.00797.x
Kontoyiannis, D. P., Marr, K. A., Park, B. J., Alexander, B. D., Anaissie, E. J., Walsh, T. J., et al. (2010). Prospective surveillance for invasive fungal infections in hematopoietic stem cell transplant recipients, 2001–2006: overview of the Transplant-Associated Infection Surveillance Network (TRANSNET) Database. Clin. Infect. Dis. 50, 1091–1100. doi: 10.1086/651263
Kredics, L., Varga, J., Kocsube, S., Doczi, I., Samson, R. A., Rajaraman, R., et al. (2007). Case of keratitis caused by Aspergillus tamarii. J. Clin. Microbiol. 45, 3464–3467. doi: 10.1128/JCM.00920-07
Krishnan, K. U., Selvi, R., and Agatha, D. (2015). Fungal rhinosinusitis: a clinicomycological perspective. Indian J. Med. Microbiol. 33, 1–120. doi: 10.4103/0255-0857.148407
Krishnan, S., Manavathu, E. K., and Chandrasekar, P. H. (2009). Aspergillus flavus: an emerging non-fumigatus Aspergillus species of significance. Mycoses 52, 206–222. doi: 10.1111/j.1439-0507.2008.01642.x
Kristensen, L., Stenderup, J., and Otkjær, A. (2005). Onychomycosis due to Aspergillus tamarii in a 3-year-old boy. Acta Derm. Venereol. 1:1. doi: 10.1080/00015550510025605
Kumar, D., Nepal, P., Singh, S., Ramanathan, S., Khanna, M., Sheoran, R., et al. (2017). CNS aspergilloma mimicking tumors: review of CNS Aspergillus infection imaging characteristics in the immunocompetent population. J. Neuroradiol. 45, 169–176. doi: 10.1016/j.neurad.2017.11.001
Lackner, M., Coassin, S., Haun, M., Binder, U., Kronenberg, F., Haas, H., et al. (2016). Geographically predominant genotypes of Aspergillus terreus species complex in Austria: s microsatellite typing study. Clin. Microbiol. Infect. 22, 270–276. doi: 10.1016/j.cmi.2015.10.021
Lass-Florl, C., Griff, K., Mayr, A., Petzer, A., Gastl, G., Bonatti, H., et al. (2005). Epidemiology and outcome of infections due to Aspergillus terreus: 10-year single centre experience. Br. J. Haematol. 131, 201–207. doi: 10.1111/j.1365-2141.2005.05763.x
Lewis, R. E., and Kontoyiannis, D. P. (2009). Invasive aspergillosis in glucocorticoid-treated patients. Med. Mycol. 47, S271–S281. doi: 10.1080/13693780802227159
Libanore, M., Prini, E., Mazzetti, M., Barchi, E., Raise, E., Gritti, F. M., et al. (2002). Invasive Aspergillosis in Italian AIDS patients. Infection 30, 341–345. doi: 10.1007/s15010-002-2033-1
Mahgoub, E. S., Ismail, M. A. I., and Gabr, A. (2016). Fungal sinusitis: Sudanese experience. Austin J Otolaryngol 3:1085. Available online at: https://www.austinpublishinggroup.com/otolaryngology/fulltext/ajo-v3-id1085.php
Marr, K. A., Carter, R. A., Boeckh, M., Martin, P., and Corey, L. (2002). Invasive aspergillosis in allogeneic stem cell transplant recipients: changes in epidemiology and risk factors. Blood 100, 4358–4366. doi: 10.1182/blood-2002-05-1496
Masih, A., Singh, P. K., Kathuria, S., Agarwal, K., Meis, J. F., and Chowdhary, A. (2016). Identification by molecular methods and matrix-assisted laser desorption ionization-time of flight mass spectrometry and antifungal susceptibility profiles of clinically significant rare Aspergillus species in a referral chest hospital in Delhi, India. J. Clin. Microbiol. 54, 2354–2364. doi: 10.1128/JCM.00962-16
Milošev, B., Mahgoub, E. S., Aal, O. A., and El Hassan, A. M. (1969). Primary aspergilloma of paranasal sinuses in the Sudan. A review of seventeen cases. Br. J. Surg. 56, 132–137. doi: 10.1002/bjs.1800560213
Mohammadi, F., Hashemi, S. J., Zoll, J., Melchers, W. J. G., Rafati, H., Dehghan, P., et al. (2016). Quantitative analysis of single-nucleotide polymorphism for rapid detection of TR34/L98H- and TR46/Y121F/T289A-positive Aspergillus fumigatus isolates obtained from patients in Iran from 2010 to 2014. Antimicrob. Agents Chemother. 60, 387–392. doi: 10.1128/AAC.02326-15
Morgan, J., Wannemuehler, K. A., Marr, K. A., Hadley, S., Kontoyiannis, D. P., Walsh, T. J., et al. (2005). Incidence of invasive aspergillosis following hematopoietic stem cell and solid organ transplantation: interim results of a prospective multicenter surveillance program. Med. Mycol. 43 (Suppl. 1), S49–S58. doi: 10.1080/13693780400020113
Nabili, M., Shokohi, T., Moazeni, M., Khodavaisy, S., Aliyali, M., Badiee, P., et al. (2016). High prevalence of clinical and environmental triazole-resistant Aspergillus fumigatus in Iran: is it a challenging issue? J. Med. Microbiol. 65, 468–475. doi: 10.1099/jmm.0.000255
Naidu, J., and Singh, S. M. (1994). Aspergillus chevalieri (Mangin) Thom and Church: a new opportunistic pathogen of human cutaneous aspergillosis. Mycoses 37, 271–274. doi: 10.1111/j.1439-0507.1994.tb00425.x
NCBI (2015). Nucleotide BLAST: Search Nucleotide Databases Using a Nucleotide Query. Basic Local Alignment Search Tool. Available online at: https://blast.ncbi.nlm.nih.gov/Blast.cgi?PROGRAM=blastn&PAGE_TYPE=BlastSearch&LINK_LOC=blasthome (accessed May 7, 2019).
Negri, C. E., Goncalves, S. S., Xafranski, H., Bergamasco, M. D., Aquino, V. R., Castro, P. T. O., et al. (2014). Cryptic and rare Aspergillus species in Brazil: prevalence in clinical samples and in vitro susceptibility to triazoles. J. Clin. Microbiol. 52, 3633–3640. doi: 10.1128/JCM.01582-14
Neofytos, D., Treadway, S., Ostrander, D., Alonso, C. D., Dierberg, K. L., Nussenblatt, V., et al. (2013). Epidemiology, outcomes, and mortality predictors of invasive mold infections among transplant recipients: a 10-year, single-center experience. Transpl. Infect. Dis. 15, 233–242. doi: 10.1111/tid.12060
Nouripour-Sisakht, S., Mirhendi, H., Shidfar, M. R., Ahmadi, B., Rezaei-Matehkolaei, A., Geramishoar, M., et al. (2015). Aspergillus species as emerging causative agents of onychomycosis. J. Mycol. Med. 25, 101–107. doi: 10.1016/j.mycmed.2014.12.001
Pagiotti, R., Venanzoni, R., Tirillini, B., Granetti, B., Rubini, A., and Angelini, P. (2010). Identification and characterisation of human pathogenic filamentous fungi and susceptibility to Thymus schimperi essential oil. Mycoses 54, e364–e376. doi: 10.1111/j.1439-0507.2010.01926.x
Palmer, L. B., Greenberg, H. E., and Schiff, M. J. (1991). Corticosteroid treatment as a risk factor for invasive aspergillosis in patients with lung disease. Thorax 46, 15–20.
Paludetti, G., Rosignoli, M., Ferri, E., Cesari, M. R., Morace, G., Fantoni, M., et al. (1992). Invasive nasosinusal aspergillosis in an immunocompetent patient. Acta Otorhinolaryngol. Ital. 12, 581–591.
Patterson, J. E., Peters, J., Calhoon, J. H., Levine, S., Anzueto, A., Al-Abdely, H., et al. (2000). Investigation and control of aspergillosis and other filamentous fungal infections in solid organ transplant recipients. Transpl. Infect. Dis. 2, 22–28. doi: 10.1034/j.1399-3062.2000.020105.x
Patterson, T. F., Thompson, G. R. III, Denning, D. W., Fishman, J. A., Hadley, S., Herbrecht, R., et al. (2016). Practice guidelines for the diagnosis and management of aspergillosis: 2016 update by the Infectious Diseases Society of America. Clin. Infect. Dis. 63, e1–e60. doi: 10.1093/cid/ciw326
Pinto, E., Monteiro, C., Maia, M., Faria, M. A., Lopes, V., Lameiras, C., et al. (2018). Aspergillus species and antifungals susceptibility in clinical setting in the North of Portugal: cryptic species and emerging azoles resistance in A. fumigatus. Front. Microbiol. 9:1656. doi: 10.3389/fmicb.2018.01656
Polacheck, I., Nagler, A., Okon, E., Drakos, P., Plaskowitz, J., and Kwon-Chung, K. J. (1992). Aspergillus quadrilineatus, a new causative agent of fungal sinusitis. J. Clin. Microbiol. 30, 3290–3293.
Raper, K. B., and Thoms, C. (1944). New Aspergilli from Soil. Mycologia 36, 555–575. doi: 10.1080/00275514.1944.12017576
Renner, J., Leclerc, T., Hoffmann, C., Masson, Y., Donat, N., Aries, P., et al. (2018). Aspergillus tamarii: an uncommon burn wound infection. J. Clin. Pathol. 71, 379–380. doi: 10.1136/jclinpath-2017-204858
Reynaud-Gaubert, M., Normand, A.-C., Piarroux, R., Dubus, J.-C., Brégeon, F., Cassagne, C., et al. (2016). Aspergillus tubingensis: a major filamentous fungus found in the airways of patients with lung disease. Med. Mycol. 54, 459–470. doi: 10.1093/mmy/myv118
Ruping, M. J., Vehreschild, J. J., and Cornely, O. A. (2008). Patients at high risk of invasive fungal infections: when and how to treat. Drugs 68, 1941–1962. doi: 10.2165/00003495-200868140-00002
Saedi, S., Khajali, Z., and Alizadehasl, A. (2017). Aspergillus infection in an immunocompetent host with supravalvular aortic stenosis. World J. Pediatr. Congenit. Heart Surg. doi: 10.1177/2150135117725456. [Epub ahead of print].
Seyedmousavi, S., Hashemi, S. J., Zibafar, E., Zoll, J., Hedayati, M. T., Mouton, J. W., et al. (2013). Azole-resistant Aspergillus fumigatus, Iran. Emerg. Infect. Dis. 19, 832–834. doi: 10.3201/eid1905.130075
Sharma, S., Yenigalla, B. M., Naidu, S. K., and Pidakala, P. (2013). Primary cutaneous aspergillosis due to Aspergillus tamarii in an immunocompetent host. BMJ Case Rep. 2013:bcr2013010128. doi: 10.1136/bcr-2013-010128
Siqueira, J. P. Z., Sutton, D. A., Gené, J., García, D., Wiederhold, N., and Guarro, J. (2018). Species of Aspergillus section Aspergillus from clinical samples in the United States. Med. Mycol. 56, 541–550. doi: 10.1093/mmy/myx085
Sugui, J. A., Kwon-Chung, K. J., Juvvadi, P. R., Latge, J.-P., and Steinbach, W. J. (2014). Aspergillus fumigatus and related species. Cold Spring Harb. Perspect. Med. 5:a019786. doi: 10.1101/cshperspect.a019786
Sutton, D. A., Sanche, S. E., Revankar, S. G., Fothergill, A. W., and Rinaldi, M. G. (1999). In vitro amphotericin B resistance in clinical isolates of Aspergillus terreus, with a head-to-head comparison to voriconazole. J. Clin. Microbiol. 37, 2343–2345.
Szigeti, G., Kocsubé, S., Dóczi, I., Bereczki, L., Vágvölgyi, C., and Varga, J. (2012a). Molecular identification and antifungal susceptibilities of black Aspergillus isolates from otomycosis cases in Hungary. Mycopathologia 174, 143–147. doi: 10.1007/s11046-012-9529-8
Szigeti, G., Sedaghati, E., Mahmoudabadi, A. Z., Naseri, A., Kocsubé, S., Vágvölgyi, C., et al. (2012b). Species assignment and antifungal susceptibilities of black aspergilli recovered from otomycosis cases in Iran. Mycoses 55, 333–338. doi: 10.1111/j.1439-0507.2011.02103.x
Taccone, F. S., Van den Abeele, A.-M., Bulpa, P., Misset, B., Meersseman, W., Cardoso, T., et al. (2015). Epidemiology of invasive aspergillosis in critically ill patients: clinical presentation, underlying conditions, and outcomes. Crit. Care 19:7. doi: 10.1186/s13054-014-0722-7
Taj-Aldeen, S. J., Chandra, P., and Denning, D. W. (2015). Burden of fungal infections in Qatar. Mycoses 58 (Suppl. 5), 51–57. doi: 10.1111/myc.12386
Taj-Aldeen, S. J., Hilal, A. A., and Chong-Lopez, A. (2003). Allergic Aspergillus flavus rhinosinusitis: a case report from Qatar. Eur. Arch. Oto-Rhino-Laryngol. 260, 331–335. doi: 10.1007/s00405-002-0547-x
Taj-Aldeen, S. J., Hilal, A. A., and Schell, W. A. (2004). Allergic fungal rhinosinusitis: a report of 8 cases. Am. J. Otolaryngol. Head Neck Med. Surg. 25, 213–218. doi: 10.1016/j.amjoto.2003.12.003
Tsang, C.-C., Hui, T. W. S., Lee, K.-C., Chen, J. H. K., Ngan, A. H. Y., Tam, E. W. T., et al. (2016). Genetic diversity of Aspergillus species isolated from onychomycosis and Aspergillus hongkongensis sp. nov., with implications to antifungal susceptibility testing. Diagn. Microbiol. Infect. Dis. 84, 125–134. doi: 10.1016/j.diagmicrobio.2015.10.027
Ullmann, A. J., Aguado, J. M., Arikan-Akdagli, S., Denning, D. W., Groll, A. H., Lagrou, K., et al. (2018). Diagnosis and management of Aspergillus diseases: executive summary of the 2017 ESCMID-ECMM-ERS guideline. Clin. Microbiol. Infect. 24, e1–e38. doi: 10.1016/j.cmi.2018.01.002
Vaezi, A., Fakhim, H., Arastehfar, A., Shokohi, T., Hedayati, M. T., Khodavaisy, S., et al. (2018). In vitro antifungal activity of amphotericin B and 11 comparators against Aspergillus terreus species complex. Mycoses 61, 134–142. doi: 10.1111/myc.12716
Van't Hek, L. G., Verweij, P. E., Weemaes, C. M., Van Dalen, R., Yntema, J. B., and Meis, J. F. (1998). Successful treatment with voriconazole of invasive aspergillosis in chronic granulomatous disease. Am. J. Respir. Crit. Care Med. 157, 1694–1696. doi: 10.1164/ajrccm.157.5.9709068
Verweij, P. E., Varga, J., Houbraken, J., Rijs, A. J. M. M., Verduynlunel, F. M., Blijlevens, N. M. A., et al. (2008). Emericella quadrilineata as cause of invasive aspergillosis. Emerg. Infect. Dis. 14, 566–572. doi: 10.3201/eid1404.071157
Visagie, C. M., Houbraken, J., Frisvad, J. C., Hong, S.-B., Klaassen, C. H. W., Perrone, G., et al. (2014). Identification and nomenclature of the genus Penicillium. Stud. Mycol. 78, 343–371. doi: 10.1016/J.SIMYCO.2014.09.001
Walsh, T. J., Petraitis, V., Petraitiene, R., Field-Ridley, A., Sutton, D., Ghannoum, M., et al. (2003). Experimental pulmonary aspergillosis due to Aspergillus terreus: pathogenesis and treatment of an emerging fungal pathogen resistant to amphotericin B. J. Infect. Dis. 188, 305–319. doi: 10.1086/377210
Xess, I., Mohanty, S., Jain, N., and Banerjee, U. (2004). Prevalence of Aspergillus species in clinical samples isolated in an Indian tertiary care hospital. Indian J. Med. Sci. 58, 513–519. Available online at: http://journal.indianjmedsci.com/index.php/ijms/issue/archive
Zanganeh, E., Zarrinfar, H., Rezaeetalab, F., Fata, A., Tohidi, M., Najafzadeh, M. J., et al. (2018). Predominance of non-fumigatus Aspergillus species among patients suspected to pulmonary aspergillosis in a tropical and subtropical region of the Middle East. Microb. Pathog. 116, 296–300. doi: 10.1016/j.micpath.2018.01.047
Keywords: aspergillosis, molecular identification, antifungal susceptibility, Qatar, Middle East
Citation: Salah H, Lackner M, Houbraken J, Theelen B, Lass-Flörl C, Boekhout T, Almaslamani M and Taj-Aldeen SJ (2019) The Emergence of Rare Clinical Aspergillus Species in Qatar: Molecular Characterization and Antifungal Susceptibility Profiles. Front. Microbiol. 10:1677. doi: 10.3389/fmicb.2019.01677
Received: 09 May 2019; Accepted: 08 July 2019;
Published: 30 July 2019.
Edited by:
Hector Mora Montes, University of Guanajuato, MexicoReviewed by:
Hamid Badali, Mazandaran University of Medical Sciences, IranOrazio Romeo, University of Messina, Italy
Copyright © 2019 Salah, Lackner, Houbraken, Theelen, Lass-Flörl, Boekhout, Almaslamani and Taj-Aldeen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Husam Salah, aG9zYW1vXzIwMDBAaG90bWFpbC5jb20=