 Lili Xu1†
Lili Xu1† Xiwen Jiang2,3†
Xiwen Jiang2,3† Yun Zhu1
Yun Zhu1 Yali Duan1
Yali Duan1 Taosheng Huang2,3
Taosheng Huang2,3 Zhiwen Huang2,3
Zhiwen Huang2,3 Chunyan Liu1
Chunyan Liu1 Baoping Xu4
Baoping Xu4 Zhengde Xie1*
Zhengde Xie1*- 1Beijing Key Laboratory of Pediatric Respiratory Infection Diseases, Key Laboratory of Major Diseases in Children, Ministry of Education, National Clinical Research Center for Respiratory Diseases, National Key Discipline of Pediatrics (Capital Medical University), Beijing Pediatric Research Institute, Beijing Children’s Hospital, Capital Medical University, National Center for Children’s Health, Beijing, China
- 2DAAN Gene Co., Ltd., Sun Yat-sen University, Guangzhou, China
- 3The Medicine and Biological Engineering Technology Research Center of the Ministry of Health, Guangzhou, China
- 4National Clinical Research Center for Respiratory Diseases, Department of Respiratory, Beijing Children’s Hospital, Capital Medical University, National Center for Children’s Health, Beijing, China
The reliable and rapid detection of viral pathogens that cause respiratory infections provide physicians several advantages in treating patients and managing outbreaks. The Luminex respiratory virus panel (RVP) assay has been shown to be comparable to or superior to culture/direct fluorescent-antibody assays (DFAs) and nucleic acid tests that are used to diagnose respiratory viral infections. We developed a multiplex asymmetric reverse transcription (RT)-PCR assay that can simultaneously differentiate all influenza A virus epidemic subtypes. The amplified products were hybridized with an electrochemical DNA sensor, and the results were automatically acquired. The limits of detection (LoDs) of both the Luminex RVP assay and the multiplex RT-PCR-electrochemical DNA sensor were 101 TCID50 for H1N1 virus and 102 TCID50 for H3N2 virus. The specificity assessment of the multiplex RT-PCR-electrochemical DNA sensor showed no cross-reactivity among different influenza A subtypes or with other non-influenza respiratory viruses. In total, 3098 respiratory tract specimens collected from padiatric patients diagnosed with pneumonia were tested. More than half (43, 53.75%) of the specimens positive for influenza A viruses could not be further subtyped using the Luminex RVP assay. Among the remaining 15 specimens that were not subtyped, not degraded, and in sufficient amounts for the multiplex RT-PCR-electrochemical DNA sensor test, all (100%) were H3N2 positive. Therefore, the sensitivity of the Luminex RVP assay for influenza A virus was 46.25%, whereas the sensitivity of the multiplex RT-PCR-electrochemical DNA sensor for the clinical H1N1 and H3N2 specimens was 100%. The sensitivities of the multiplex RT-PCR-electrochemical DNA sensor for the avian H5N1, H5N6, H9N2, and H10N8 viruses were 100%, whereas that for H7N9 virus was 85.19%. We conclude that the multiplex RT-PCR-electrochemical DNA sensor is a reliable method for the rapid and accurate detection of highly variable influenza A viruses in respiratory infections with greater detection sensitivity than that of the Luminex xTAG assay. The high mutation rate of influenza A viruses, particularly H3N2 during the 2014 to 2016 epidemic seasons, has a strong impact on diagnosis. A study involving more positive specimens from all influenza A virus epidemic subtypes is required to fully assess the performance of the assay.
Introduction
Influenza A virus causes morbidity and mortality in humans, and this is overstated during epidemic years, which is a major public health concern (Neuzil et al., 2000; Petrova and Russell, 2018). Based on the antigenic specificity of haemagglutinin (HA) and neuraminidase (NA) proteins, influenza A viruses can be classified into subtypes H1–H18 and N1–N11, respectively (Wu et al., 2014; Pinsent et al., 2016). Currently, H1N1 and H3N2 are the most prevalent human subtypes and continue to co-circulate as two subtypes. Outbreaks of avian influenza viruses, such as H5N1, H5N6, H7N9, H9N2, and H10N8, have shown that these viruses can bypass the species barrier from poultry to humans, causing mortality in both species (Li and Cao, 2017). Rapid detection and subtyping are the first steps in the characterization of influenza A viruses, and can facilitate the appropriate treatments to improve patient clinical outcomes and significantly reduce hospital costs (Bonner et al., 2003).
Traditionally, respiratory viral infections have been diagnosed by culture, a rapid antigen test, or a direct fluorescent-antibody assay (DFA) (Uyeki, 2003). However, many studies have demonstrated that molecular diagnostic assays have superior sensitivity over conventional assays, and these assays are currently considered the new gold standard (Weinberg et al., 2004; Kuypers et al., 2006; Letant et al., 2007; Hodinka and Kaiser, 2013). The introduction of multiplex PCR assays has increased the efficiency of the routine molecular diagnosis of various viruses and has been shown to be cost-effective (Auburn et al., 2011; Jansen et al., 2011; Choudhary et al., 2013). The RVP assay (Luminex Molecular Diagnostics Inc., Toronto, Canada) is a CE-marked, commercially available kit based on suspension microarray technology that enables the detection of many viruses in a single reaction (Krunic et al., 2007; Merante et al., 2007). The Luminex RVP assay has been shown to be more sensitive and specific than culture and antigen detection (Wong et al., 2009; Gadsby et al., 2010). However, the cost of the kit and instrument is a major disadvantage of the Luminex RVP assay.
Biosensors represent a newly developing detection technique that combines biochemical, electrochemical, medical and electronic techniques. Recently, electrochemical DNA sensors have received much interest in many fields due to their unique advantages, such as their innately high sensitivity, simple instrumentation, automation and low cost in the detection of infectious diseases, clinical diagnosis of pathogens, genetic diagnoses, environmental pollutant determination, food safety determination, epidemiological studies, and forensic identification (Kerman et al., 2004). A gold electrode in an electrochemical DNA sensor is functionalized using a DNA probe sequence, oligo phenylmethyl molecular wires, and polyethylene glycol insulator molecules. The target is captured on the electrode and hybridizes to a second reporter sequence labeled with ferrocene designated the signal probe. The electrochemical detection of hybridization is primarily based on the differences in the electrochemical conduction of the labels with or without double-stranded DNA (dsDNA) or single-stranded DNA (ssDNA). Additionally, the use of a sandwich structure for DNA hybridization further improves the selective recognition of the DNA electrochemical sensor; thus, this DNA electrochemical sensor has a high specificity (Kerman et al., 2004).
In this study, we developed and evaluated the diagnostic performance of a multiplex asymmetric RT-PCR-electrochemical DNA sensor for the simultaneous differentiation of all influenza A virus epidemic subtypes. The Luminex RVP assay and commercial real-time PCR kits were used to separately detect human and avian influenza viruses for comparison.
Materials and Methods
Positive Control Viruses
The influenza virus isolates A/California/07/2009 (H1N1), A/duck/Wuxi/2/2013 (H2N1), A/Brisbane/10/2007 (H3N2), A/Anhui/1/2005 (H5N1), A/Guangzhou/39715/2014 (H5N6), A/Anhui/1/2013 (H7N9), A/duck/Zhejiang/3/2002 (H9N2), and A/duck/2/Hebei/2014 (H10N8) were kindly provided by Prof. Sanhong Yin and Dr. Xianpeng Zhang from the Dongguan Animal Disease Prevention and Control Center. All experiments involving virus cultures of highly pathogenic viruses were conducted under BSL-3 containment.
Clinical Sample Collection
Between November 2014 and April 2016, 3098 pediatric pneumonia patients with a median age of 2.17 years old (ranging from 7 days old to 16.08 years old) were enrolled at the Pathogen Surveillance Network of Beijing Children’s Hospital. Nasopharyngeal aspirate or throat swab specimens were collected from each patient. This study was performed in strict accordance with human subject protection guidance and was approved by the Ethical Review Committee of Beijing Children’s Hospital. Written informed consent was obtained on the participants’ behalf from their parents or guardians.
Primer and Probe Design
The nucleotide sequences of the influenza A virus matrix (M) gene; the H1, H2, H3, H5, H7, H9, and H10 genes; and the N1, N2, N6, N8, and N9 genes were retrieved from the GenBank database and aligned using the BioEdit v7.1.3 software. The primers were designed and analyzed using the Oligo 7.0 software and aligned using BLAST with relative sequences in GenBank to verify the specific amplification. The top-rated primers and probes from the Oligo 7.0 software with non-annealing, irrelevant sequences in GenBank evaluated by using BLAST were chosen for use. Specific forward and reverse primers were used for M gene amplification, whereas specific forward primers and universal reverse primers were used for HA and NA gene amplification. The capture probes were C6 S-S-labeled (Thiol Modifier), and the signal probes were labeled with ferrocene. The finalized primers and probes are listed in Table 1.
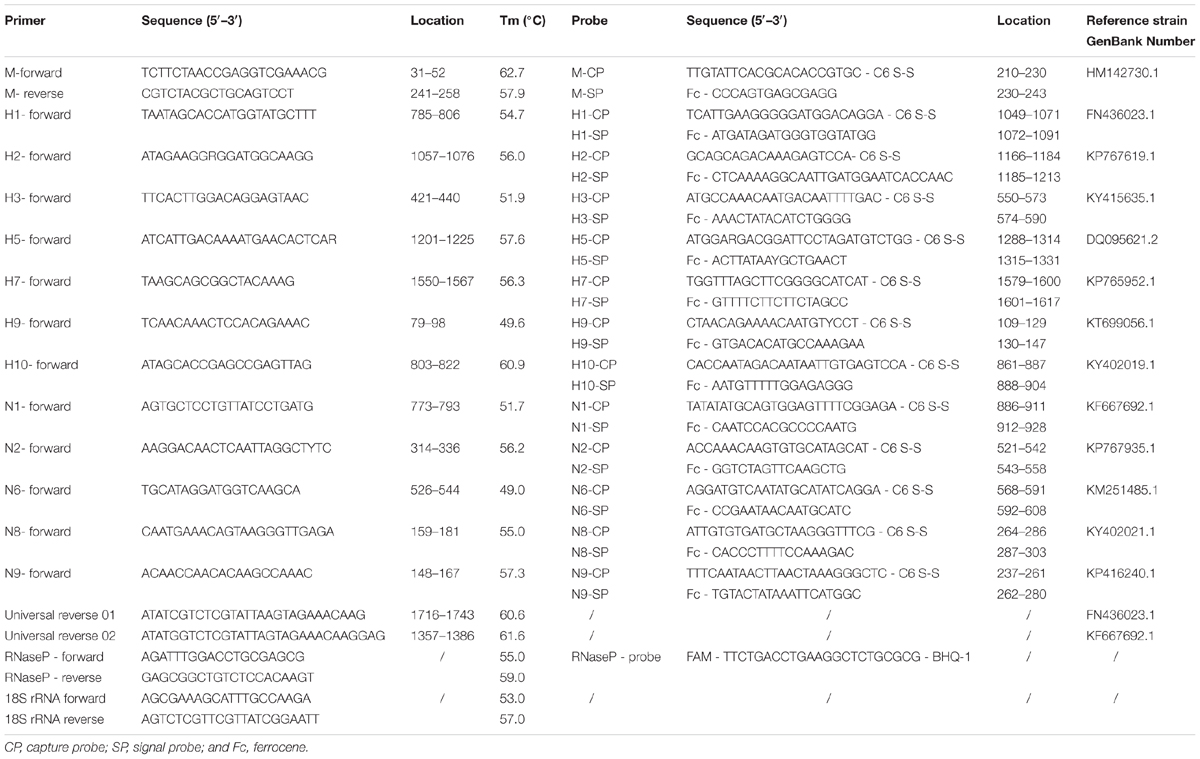
TABLE 1. The primers and probes used for the multiplex asymmetric RT-PCR assay in this study.
Multiplex Reverse Transcription-PCR and DNA Sensor Hybridization
Total nucleic acids were extracted from the clinical samples using a NucliSens easyMAG system (BioMérieux, Marcy-l’Etoile, France) according to the manufacturer’s instructions. A mixed positive control containing each positive control influenza virus and one negative control consisting of cultured, uninfected human epithelial cells was processed with each batch of clinical specimens.
For each sample, reverse transcription-PCR was performed using three microcentrifuge tubes with three different PCR mixes. Tube A targeted H1, H2, H3, H5, H7, H9, and H10 genes of influenza A viruses; Tube B targeted N1, N2, N6, N8, and N9 genes of influenza A viruses; and Tube C targeted the M gene of influenza A virus. The 50-μL reaction mixture consisted of 10 mM of Tris-HCl (pH 8.3), 3.5 mM of MgCl2, 20 mM of KCl, 200 mM of dNTPs, forward primers (10 μM each), reverse primers (1 μM each) and 50 ng of extracted RNA. PCR was performed using an ABI9700 Thermal Cycler (Applied Biosystems, United States). The PCR conditions were as follows: (Neuzil et al., 2000) 50°C for 30 min; (Petrova and Russell, 2018) 95°C for 15 min; (Pinsent et al., 2016) 45 cycles of 94°C for 30 s, 50°C for 30 s, and 72°C for 30 s; and (Wu et al., 2014) a final extension at 72°C for 7 min. Each batch of PCR runs included nucleic acid extracted from the positive mix and negative controls, and a further amplification and quantification of the RNaseP gene (forward, 5′-AGATTTGGACCTGCGAGCG-3′; reverse, 5′-GAGCGGCTGTCTCCACAAGT-3′; and probe, 5′-TTCTGACCTGAAGGCTCTGCGCG-3′) was carried out as an internal reference control (World Health Organisation [WHO], 2013).
Because unequal amounts of reverse primers were used in the asymmetric PCR process, after PCR amplification, large amounts of ssDNA that could be directly hybridized were generated using the signal probes (100 μM each), 10 μL of foetal bovine serum (FBS), and 20 μL of sodium perchlorate for 30 min without heat denaturation.
The electrochemical DNA sensor consisted of 72 gold electrodes. Electrode pretreatment and capture probe immobilization were performed according to a previously reported protocol (Lao et al., 2005). The electrochemical signal was recorded when the target DNA hybridized to the capture probe and ferrocene-labeled signal probe, thereby connecting the reporter molecule ferrocene to the self-assembled monolayer on the gold electrode. Voltmeter measurements and data analysis were performed using a DA9100 Electrochemical Workstation (DAAN Gene Co., Ltd.). All positive amplicons were further confirmed by sequencing.
Luminex RVP Assay
A Luminex RVP assay was performed to detect 18 common respiratory viral pathogens and subtypes, including influenza A, influenza A subtype H1, influenza A subtype H3, 2009 H1N1, influenza B, HAdV, HPIV 1–4, RSV A and B, human metapneumovirus (HMPV), enteroviruses and rhinoviruses (EV/Rh), human coronavirus (HCoV) HKU1, 229E, NL63, and OC43, and human bocavirus (HBoV), in the nucleic acid samples. An internal positive control was added to each specimen before the nucleic acid extraction procedure was performed, and a positive PCR control (Lambda DNA) was added to each PCR run according to the manufacturer’s manual. In this study, blank VTM served as a negative control for nucleic acid extraction.
Comparison of the Sensitivity and Limits of Detection (LoDs) Between the Luminex RVP Assay and Multiplex RT-PCR-Electrochemical DNA Sensor
To compare the detection sensitivities of the two methods, a true positive was defined as a positive specimen in both tests or any specimen positive in only one test that was further confirmed by sequencing. All specimens with concordant or discordant results were tested using both methods in duplicate.
We compared the LoDs of these two detection methods using 10-fold serial dilutions of positive control viruses ranging from 104 TCID50 to 100 TCID50. The LoD procedure was carried out as described by Bustin et al. (2009). All dilutions were detected in three duplex reactions.
Specificity Detection of the Multiplex RT-PCR-Electrochemical DNA Sensor
The specificity of the multiplex RT-PCR assay was evaluated by detecting pediatric pneumonia specimens that were positive for other pathogens, including RSV, HAdV, HMPV, HPIV, EV/Rh, HCoV, and HBoV (five positive specimens for each pathogen) using a Luminex RVP assay.
Comparison of Detection Sensitivity for Avian Influenza Virus Positive Specimens Between the Multiplex RT-PCR-Electrochemical DNA Sensor and Real-Time PCR Kits
In total, 186 specimens positive for avian influenza viruses collected from poultry or birds in southern China from 2006 to 2014 and verified by gene sequencing were used to assess the detection sensitivity of the multiplex RT-PCR-electrochemical DNA sensor for avian influenza viruses. Several commercial real-time PCR kits produced by DAAN Gene Co., Ltd. were used to detect the H5N1, H5N6, H7N9, H9N2, and H10N8 viruses for comparison. Sample quality was controlled by using 18S rRNA as housekeeping control gene with bird-conserved primers (forward, 5′-AGCGAAAGCATTTGCCAAGA-3′; reverse, 5′-AGTCTCGTTCGTTATCGGAATT-3′), validated against a variety of bird species (including chicken, duck, goose, and crow) and tissues (spleen, brain, lung, trachea, cecum, and liver) (Kerman et al., 2004). All avian specimens were kindly provided by Prof. Sanhong Yin and Dr. Xianpeng Zhang at the Dongguan Animal Disease Prevention and Control Center, and the study was conducted under BSL-3 containment. The animal specimen usage was approved by the Ethical Review Committee of Dongguan Animal Disease Prevention and Control Center.
Statistical Analysis
The exact (Clopper-Pearson) method was used to calculate the 95% confidence intervals (95% CI). The sensitivity estimates for each virus were calculated based on two-by-two tables from the entire prospective data set.
Results
We first assessed the LoD and specificity of the developed multiplex RT-PCR-electrochemical DNA sensor. The LoD of the Luminex RVP assay and multiplex RT-PCR-electrochemical DNA sensor was evaluated using serially diluted positive control viruses for H1N1 or H3N2. Based on three duplex reactions, an excellent reproducibility result showed that the LoDs using both methods were 101 TCID50 for H1N1 and 102 TCID50 for H3N2. According to the specificity analysis, the multiplex RT-PCR assay developed in this study specifically amplified 7 HA genes, 5 NA genes, and the M gene from the influenza A viruses. No cross-reactivity was observed among the subtypes, and no spurious PCR amplification or voltmeter measurements were observed in the specimens positive for RSV, HAdV, HMPV, HPIV, EV/Rh, HCoV, and HBoV.
Second, the clinical specimens were used to compare the sensitivity of the multiplex RT-PCR-electrochemical DNA sensor using comparative methods. Using the Luminex RVP assay, 149 (4.81%) influenza-positive cases were detected among 3098 pediatric pneumonia patients between November 2014 and April 2016, including 79 (2.55%) cases infected with influenza A, 71 (2.29%) cases infected with influenza B, and 1 case co-infected with influenza A and B. The influenza A positive specimens were simultaneously differentiated into H1N1 and H3N2 using the Luminex RVP assay; however, only 23.75% (19/80) and 22.50% (18/80) of the specimens were identified as 2009 H1N1 and H3N2, respectively, and 43 specimens (53.75%) could not be subtyped using the Luminex RVP assay.
The influenza A-positive specimens which were verified by the Luminex RVP assay were then tested using the multiplex RT-PCR-electrochemical DNA sensor. For all 19 2009 H1N1-positive and 18 H3N2-positive specimens detected by the Luminex RVP assay, the results obtained using the multiplex RT-PCR-electrochemical DNA sensor were in total agreement. However, for the 42 non-subtyped influenza A specimens detected by the Luminex RVP assay, due to repeated detection based on the negative results, only 17 specimens were available in sufficient amounts for the multiplex RT-PCR-electrochemical DNA sensor test. Two of these specimens were negative for the RNaseP gene, which indicated that these two specimens were too degraded for detection. The remaining 15 (88.24%) specimens were H3N2-positive, and no H1N1-positive specimens were detected. All the positive amplicons detected by the multiplex RT-PCR-electrochemical DNA sensor were confirmed by sequencing. To further detect the sensitivity of the multiplex RT-PCR-electrochemical DNA sensor, we randomly selected 96 specimens that showed negative results for all viruses by using the Luminex RVP assay. In accordance with the Luminex RVP assay, no influenza virus was detected.
In summary, based on the above data, the sensitivity of the Luminex RVP assay for the influenza A virus was 46.25% (95% CI, 45.03–47.47%). The true number of positive specimens using the multiplex RT-PCR-electrochemical DNA sensor was 52 (37 positive by both tests and 15 specimens positive by the multiplex RT-PCR-electrochemical DNA sensor, followed by further confirmation by sequencing). The sensitivity of the multiplex RT-PCR-electrochemical DNA sensor for the influenza A virus (including H1N1 and H3N2) was 100% (95% CI, 93.15–100%) (Table 2).

TABLE 2. Comparison of the detection sensitivity for the clinical H1N1- and H3N2-positive specimens between the Luminex RVP assay and the multiplex RT-PCR-electrochemical DNA sensor.
Furthermore, to evaluate the practical application of the multiplex RT-PCR-electrochemical DNA sensor for the detection of avian influenza viruses, which were lacking in the pediatric pneumonia specimens, we compared the sensitivity of this detection method using a series of real-time PCR kits to separately detect the H5N1, H5N6, H7N9, H9N2, and H10N8 viruses. According to the real-time PCR results, of the 186 avian specimens, 18S rRNA genes showed equal orders of magnitude and 16, 56, 27, 82, and 5 specimens were positive for H5N1, H5N6, H7N9, H9N2, and H10N8, respectively. The detection sensitivities of these real-time PCR kits were 100% (186/186; 95% CI, 98.04–100%). Using the multiplex RT-PCR-electrochemical DNA sensor, the detection sensitivities for H5N1, H5N6, H9N2, and H10N8 were also 100%. However, 4 H7N9-positive specimens showed negative results, indicating that the detection sensitivity for the avian H7N9 virus was 85.19% (23/27; 95% CI, 82.61–87.76%), while that for all detected avian influenza viruses was 97.85% (182/186; 95% CI, 97.70–98.00%) (Table 3). Compared to the real-time PCR results, the copy numbers of the 4 negative specimens detected using the multiplex RT-PCR-electrochemical DNA sensor were less than 102 copies/mL, and the other 23 specimens with positive results showed viral copy numbers greater than 102 copies/mL. Thus, specimens with less than 102 copies/mL H7N9 viral DNA may not be detected by using the multiplex RT-PCR-electrochemical DNA sensor. We also randomly selected 50 avian specimens that showed negative results by using real-time PCR for all avian influenza viruses, aiming to detect influenza viruses with the multiplex RT-PCR-electrochemical DNA sensor; however, no positive samples were found.
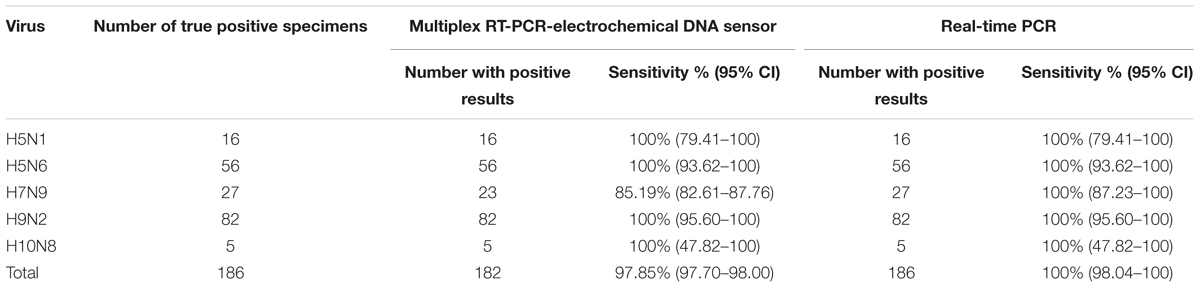
TABLE 3. Comparison of the detection sensitivity for the avian influenza virus-positive specimens between the multiplex RT-PCR-electrochemical DNA sensor and the real-time PCR kits.
Discussion
Nucleic acid detection, particularly PCR-based approaches used to detect the influenza A virus, has recently expanded exponentially. Several multiplex RT-PCR methods have been developed for the identification of influenza A viruses (Chang et al., 2008; Chen et al., 2011; Fang et al., 2011; Tang et al., 2012; Wu et al., 2013). Electrochemical DNA sensors represent a novel developing technique that combines nucleic acid hybridization with electronic techniques and is simple, reliable, inexpensive, sensitive and selective for genetic detection; this method has become a hot topic in the fields of biochemistry and medicine. In this study, we developed a multiplex asymmetric PCR assay to simultaneously differentiate seven HA (H1, H2, H3, H5, H7, H9, and H10) and five NA (N1, N2, N6, N8, and N9) subtypes from three reaction mixtures and achieved detection using an electrochemical DNA sensor in less than 30 min. Multiplexing technologies are becoming increasingly popular since they offer increased testing throughput capacity and can reduce overall cost. The frequently reduced sensitivity and specificity are disadvantages of multiplex molecular assays. In particular, the hybridization of a labeled target DNA can be less than optimal due to the steric hindrance of the microarray surfaces, leading to the preferential binding of the target to the non-labeled antisense strand (Shchepinov et al., 1997). In this study, the primers and probes were designed and homologically aligned using BLAST. All the relative sequences in GenBank were used to verify the specific amplification rather than by downloading limited gene sequences to identify conserved regions that may be unsuitable for all strains collected at various times and locations worldwide. We used this multiplex RT-PCR-electrochemical DNA sensor to test clinical specimens from the 2017 autumn–winter season. Based on our results, the application of this method exhibited perfect performance in terms of the sensitivity and specificity in detecting clinical influenza A viruses (unpublished data, not shown).
Furthermore, the sensitivity of the assay was greatly improved by adapting an asymmetric PCR reaction based on temperature-differential primer design. Asymmetric PCR could result in a higher sensitivity than symmetric PCR because the target strand alone is a higher proportion of the product, which can non-competitively hybridize with the probe. Asymmetric PCR with a high sensitivity and specificity has been developed for the detection of various pathogens, such as influenza B virus, adenovirus, HIV, Treponema pallidum, Ureaplasma urealyticum, and Chlamydia trachomatis (Poddar, 2000; Cao et al., 2006; Tang et al., 2009; Wong et al., 2014).
The Luminex RVP is a multiplex PCR assay approved by the United States Food and Drug Administration (FDA). This assay has been shown to be comparable or superior to culture/DFA and nucleic acid tests in the diagnosis of respiratory viral infections (Pabbaraju et al., 2008; Jokela et al., 2012). However, in this study, the sensitivity of the Luminex RVP assay for influenza A viruses during the 2014–2016 seasons was only 46.25%. The sensitivity of the Luminex RVP assay for influenza A virus was 54.2% in a report by Choudhary et al. (2016), 68.8% in a report by Gadsby et al. (2010), and only 14% for H1N1 and 0% for H3N2 in a report by Raymaekers et al. (2011). In contrast, the sensitivity of the Luminex RVP assay for the influenza A virus was reported to be 98.0% by Pabbaraju et al. (2008), 96.6% by Kim et al. (2013), and 100% for H1N1 and 92.9% for H3N2 by Popowitch et al. (2013). Because the LoD of both methods was highly consistent, we hypothesize that the sensitivity results were inconsistent because the specimens were collected during different epidemic seasons from different regions worldwide, and the sequence variation rate of the influenza A viruses in the primer-probe binding region of the Luminex RVP assay is high, leading to negative results. Munro described the development of a multiplex RT-PCR assay using Luminex microarray hybridization to detect influenza virus subtypes and showed sensitivities of 97.3% for FluA, 90.5% for H1, 96.9% for H3, and 88.9% for FluB in 2010–2011 season specimens, whereas the detection of the 2011–2012 season specimens showed a sensitivity of 100% for FluA, 89.9% for H1, 96.4% for H3, and 95.6% for FluB (Munro et al., 2013). This study supported our hypothesis that the high mutation rate of influenza A viruses in various epidemic seasons has a strong impact on the sensitivity of the Luminex RVP assay for influenza A virus detection due to primer/probe mismatches. In this study, of the remaining 15 specimens that were non-subtyped by the Luminex RVP assay, not degraded, and present in sufficient amounts for the multiplex RT-PCR-electrochemical DNA sensor test, all (100%) were H3N2-positive. Thus, the mutation rate of the H3N2 viruses during the 2014–2016 epidemic seasons was much higher than that of the H1N1 viruses in China. Genetic surveillance of the H3N2 viruses from 2014 to 2016 indeed showed multiple substitutions in the antigenic sites and reassortant events worldwide (Skowronski et al., 2016; Valenciano et al., 2016; Goldstein et al., 2017; Ma et al., 2017; Monamele et al., 2017; Suntronwong et al., 2017; Korsun et al., 2018). More importantly, the non-subtyped H3N2 strains using the Luminex RVP assay in this study were further subjected to genetic sequencing, and the occurrence of mutations and reassortment was verified (unpublished data, not shown). However, we could not exclude the possibility that a portion of these 15 specimens were positive for both H1N1 and H3N2, and the H1N1 virus could not be detected by both assays because it has been reported that post-pandemic 2009 influenza H1N1 viruses have been antigenically drifting (Clark et al., 2017). More sensitive but complicated and time-consuming detection methods such as metagenomic analysis could be carried out for further verification.
In this study, we have randomly selected 96 clinical pneumonia specimens with negative results for all viruses by using the Luminex RVP assay and further tested these specimens by using the multiplex RT-PCR-electrochemical DNA sensor. However, no more influenza A-positive specimens were detected. It appears that the M gene is relatively conserved and that the primers/probes used for identifying influenza A viruses in both assays are credible.
According to the sequencing confirmation of the positive specimens, we report the disappearance of seasonal H1N1 (which was oseltamivir-resistant), demonstrating that there is no current clinical need to offer information regarding seasonal H1N1. However, the subtype information is helpful for our epidemiology and infection control colleagues and may be beneficial for antiviral susceptibility development.
In this study, four H7N9-positive specimens detected with the real-time PCR assay showed negative results using the multiplex RT-PCR-electrochemical DNA sensor. Compared to the real-time PCR results, the copy numbers of the four negative specimens detected using the multiplex RT-PCR-electrochemical DNA sensor were less than 102 copies/mL, while the other 23 H7N9-positive specimens with viral copies greater than 102 copies/mL showed positive results using the multiplex RT-PCR-electrochemical DNA sensor. Thus, although the sensitivity of the multiplex RT-PCR-electrochemical DNA has been found comparable to the real-time PCR regarding the detection of H5N1, H5N6, H7N9, H9N2, and H10N8, it was less sensitive in detection of H7N9 influenza virus. However, the advantage of the multiplex RT-PCR-electrochemical DNA sensor is that it can simultaneously detect and subtype influenza A viruses, whereas the focus of the real-time PCR kit is only one subtype; therefore, more time and more specimens will be consumed. We are currently designing a new batch of primers and probes for the H7N9 virus and aim to find one group with more sensitivity without cross-reaction with the other subtypes to further optimize the multiplex RT-PCR-electrochemical DNA sensor.
Conclusion
A sensitive, reliable, simultaneous detection system generated based on multiplex asymmetric PCR coupled to an electrochemical DNA sensor was developed to simultaneously detect and subtype influenza A viruses. This system might serve as a better alternative for hospitals and clinical laboratories that must identify viral pathogens earlier in the treatment continuum.
Author Contributions
LX performed the data analysis and drafted the manuscript. YZ, YD, TH, ZH, and CL performed the laboratory experiments. ZX and XJ participated in the study design and coordinated the drafting of the manuscript. All the authors read and approved the final manuscript.
Funding
This study was supported by grants from the National Major S&T Research Projects for the Control and Prevention of Major Infectious Diseases in China (2017ZX10103004-004 and 2018ZX10305409-001-004), the Capital Health Research and Development of Special Projects (2016-2-1142), and the Beijing Municipal Administration of Hospitals’ Youth Program (QML20171201).
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We thank Prof. Sanhong Yin and Dr. Xianpeng Zhang from the Dongguan Animal Disease Prevention and Control Centre for supplying the partial positive control viruses and all avian specimens. We also thank Prof. Ming Liao and Prof. Xinwei Jia from South China Agricultural University for providing the BSL-3 laboratory for handling the highly pathogenic viruses.
References
Auburn, H., Zuckerman, M., Broughton, S., Greenough, A., and Smith, M. (2011). Detection of nine respiratory RNA viruses using three multiplex RT-PCR assays incorporating a novel RNA internal control transcript. J. Virol. Methods 176, 9–13. doi: 10.1016/j.jviromet.2011.05.017
Bonner, A. B., Monroe, K. W., Talley, L. I., Klasner, A. E., and Kimberlin, D. W. (2003). Impact of the rapid diagnosis of influenza on physician decision-making and patient management in the pediatric emergency department: results of a randomized, prospective, controlled trial. Pediatrics 112, 363–367. doi: 10.1542/peds.112.2.363
Bustin, S. A., Benes, V., Garson, J. A., Hellemans, J., Huggett, J., Kubista, M., et al. (2009). The MIQE guidelines: minimum information for publication of quantitative real-time PCR experiments. Clin. Chem. 55, 611–622. doi: 10.1373/clinchem.2008.112797
Cao, X., Wang, Y. F., Zhang, C. F., and Gao, W. J. (2006). Visual DNA microarrays for simultaneous detection of Ureaplasma urealyticum and Chlamydia trachomatis coupled with multiplex asymmetrical PCR. Biosens. Bioelectron. 22, 393–398. doi: 10.1016/j.bios.2006.05.011
Chang, H. K., Park, J. H., Song, M. S., Oh, T. K., Kim, S. Y., Kim, C. J., et al. (2008). Development of multiplex rt-PCR assays for rapid detection and subtyping of influenza type A viruses from clinical specimens. J. Microbiol. Biotechnol. 18, 1164–1169.
Chen, Y., Cui, D., Zheng, S., Yang, S., Tong, J., Yang, D., et al. (2011). Simultaneous detection of influenza A, influenza B, and respiratory syncytial viruses and subtyping of influenza A H3N2 virus and H1N1 (2009) virus by multiplex real-time PCR. J. Clin. Microbiol. 49, 1653–1656. doi: 10.1128/JCM.02184-10
Choudhary, M. L., Anand, S. P., Heydari, M., Rane, G., Potdar, V. A., Chadha, M. S., et al. (2013). Development of a multiplex one step RT-PCR that detects eighteen respiratory viruses in clinical specimens and comparison with real time RT-PCR. J. Virol. Methods 189, 15–19. doi: 10.1016/j.jviromet.2012.12.017
Choudhary, M. L., Anand, S. P., Tikhe, S. A., Walimbe, A. M., Potdar, V. A., Chadha, M. S., et al. (2016). Comparison of the conventional multiplex RT-PCR, real time RT-PCR and Luminex xTAG((R)) RVP fast assay for the detection of respiratory viruses. J. Med. Virol. 88, 51–57. doi: 10.1002/jmv.24299
Clark, A. M., DeDiego, M. L., Anderson, C. S., Wang, J., Yang, H., Nogales, A., et al. (2017). Antigenicity of the 2015-2016 seasonal H1N1 human influenza virus HA and NA proteins. PLoS ONE 12:e0188267. doi: 10.1371/journal.pone.0188267
Fang, S. S., Li, J. X., Cheng, X. W., Zhao, C. Y., Wang, T., Lv, X., et al. (2011). Simultaneous detection of influenza virus type B and influenza A virus subtypes H1N1, H3N2, and H5N1 using multiplex real-time RT-PCR. Appl. Microbiol. Biotechnol. 90, 1463–1470. doi: 10.1007/s00253-011-3192-8
Gadsby, N. J., Hardie, A., Claas, E. C. J., and Templeton, K. E. (2010). Comparison of the luminex respiratory virus panel fast assay with in-house real-time PCR for respiratory viral infection diagnosis. J. Clin. Microbiol. 48, 2213–2216. doi: 10.1128/JCM.02446-09
Goldstein, E. J., Harvey, W. T., Wilkie, G. S., Shepherd, S. J., MacLean, A. R., Murcia, P. R., et al. (2017). Integrating patient and whole-genome sequencing data to provide insights into the epidemiology of seasonal influenza A(H3N2) viruses. Microb. Genom. 4:e000137. doi: 10.1099/mgen.0.000137
Hodinka, R. L., and Kaiser, L. (2013). Is the era of viral culture over in the clinical microbiology laboratory? J. Clin. Microbiol. 51, 2–8. doi: 10.1128/JCM.02593-12
Jansen, R. R., Schinkel, J., Koekkoek, S., Pajkrt, D., Beld, M., de Jong, M. D., et al. (2011). Development and evaluation of a four-tube real time multiplex PCR assay covering fourteen respiratory viruses, and comparison to its corresponding single target counterparts. J. Clin. Virol. 51, 179–185. doi: 10.1016/j.jcv.2011.04.010
Jokela, P., Piiparinen, H., Mannonen, L., Auvinen, E., and Lappalainen, M. (2012). Performance of the luminex xTAG respiratory viral panel fast in a clinical laboratory setting. J. Virol. Methods 182, 82–86. doi: 10.1016/j.jviromet.2012.03.015
Kerman, K., Kobayashi, M., and Tamiya, E. (2004). Recent trends in electrochemical DNA biosensor technology. Meas. Sci. Technol. 15, R1–R11. doi: 10.1088/0957-0233/15/2/R01
Kim, H. K., Oh, S. H., Yun, K. A., Sung, H., and Kim, M. N. (2013). Comparison of Anyplex II RV16 with the xTAG respiratory viral panel and seeplex RV15 for detection of respiratory viruses. J. Clin. Microbiol. 51, 1137–1141. doi: 10.1128/JCM.02958-12
Korsun, N., Angelova, S., Trifonova, I., Tzotcheva, I., Mileva, S., Voleva, S., et al. (2018). Predominance of influenza A(H3N2) viruses during the 2016/2017 season in Bulgaria. J. Med. Microbiol. 67, 228–239. doi: 10.1099/jmm.0.000668
Krunic, N., Yager, T. D., Himsworth, D., Merante, F., Yaghoubian, S., and Janeczko, R. (2007). xTAG RVP assay: analytical and clinical performance. J. Clin. Virol. 40(Suppl. 1), S39–S46. doi: 10.1016/S1386-6532(07)70009-4
Kuypers, J., Wright, N., Ferrenberg, J., Huang, M. L., Cent, A., Corey, L., et al. (2006). Comparison of real-time PCR assays with fluorescent-antibody assays for diagnosis of respiratory virus infections in children. J. Clin. Microbiol. 44, 2382–2388. doi: 10.1128/JCM.00216-06
Lao, R. J., Song, S. P., Wu, H. P., Wang, L. H., Zhang, Z. Z., He, L., et al. (2005). Electrochemical interrogation of DNA monolayers on gold surfaces. Anal. Chem. 77, 6475–6480. doi: 10.1021/ac050911x
Letant, S. E., Ortiz, J. I., Tammero, L. F. B., Birch, J. M., Derlet, R. W., Cohen, S., et al. (2007). Multiplexed reverse transcriptase PCR assay for identification of viral respiratory pathogens at the point of care. J. Clin. Microbiol. 45, 3498–3505. doi: 10.1128/JCM.01712-07
Li, H., and Cao, B. (2017). Pandemic and avian influenza a viruses in humans: epidemiology, virology, clinical characteristics, and treatment strategy. Clin. Chest Med. 38, 59–70. doi: 10.1016/j.ccm.2016.11.005
Ma, C. N., Pan, Y., Zhang, L., Zhang, Y., Wu, S. S., Sun, Y., et al. (2017). Influenza vaccine effectiveness against medically attended influenza illness in Beijing, China, 2014/15 season. Hum. Vaccin. Immunother. 13, 2379–2384. doi: 10.1080/21645515.2017.1359364
Merante, F., Yaghoubian, S., and Janeczko, R. (2007). Principles of the xTAG respiratory viral panel assay (RVP Assay). J. Clin. Virol. 40(Suppl. 1), S31–S35. doi: 10.1016/S1386-6532(07)70007-0
Monamele, G. C., Vernet, M. A., Njankouo, M. R., Victoir, K., Akoachere, J. F., Anong, D., et al. (2017). Genetic and antigenic characterization of influenza A(H3N2) in Cameroon during the 2014-2016 influenza seasons. PLoS One 12:e0184411. doi: 10.1371/journal.pone.0184411
Munro, S. B., Kuypers, J., and Jerome, K. R. (2013). Comparison of a multiplex real-time PCR assay with a multiplex Luminex assay for influenza virus detection. J. Clin. Microbiol. 51, 1124–1129. doi: 10.1128/JCM.03113-12
Neuzil, K. M., Mellen, B. G., Wright, P. F., Mitchel, E. F. Jr., and Griffin, M. R. (2000). The effect of influenza on hospitalizations, outpatient visits, and courses of antibiotics in children. N. Engl. J. Med. 342, 225–231. doi: 10.1056/NEJM200001273420401
Pabbaraju, K., Tokaryk, K. L., Wong, S., and Fox, J. D. (2008). Comparison of the Luminex xTAG respiratory viral panel with in-house nucleic acid amplification tests for diagnosis of respiratory virus infections. J. Clin. Microbiol. 46, 3056–3062. doi: 10.1128/JCM.00878-08
Petrova, V. N., and Russell, C. A. (2018). The evolution of seasonal influenza viruses. Nat. Rev. Microbiol. 16, 47–60. doi: 10.1038/nrmicro.2017.146
Pinsent, A., Fraser, C., Ferguson, N. M., and Riley, S. (2016). A systematic review of reported reassortant viral lineages of influenza A. BMC Infect. Dis. 16:3. doi: 10.1186/s12879-015-1298-9
Poddar, S. K. (2000). Symmetric vs asymmetric PCR and molecular beacon probe in the detection of a target gene of adenovirus. Mol. Cell. Probes 14, 25–32. doi: 10.1006/mcpr.1999.0278
Popowitch, E. B., O’Neill, S. S., and Miller, M. B. (2013). Comparison of the biofire filmArray RP, Genmark eSensor RVP, Luminex xTAG RVPv1, and Luminex xTAG RVP fast multiplex assays for detection of respiratory viruses. J. Clin. Microbiol. 51, 1528–1533. doi: 10.1128/JCM.03368-12
Raymaekers, M., de Rijke, B., Pauli, I., Van den Abeele, A. M., and Cartuyvels, R. (2011). Timely diagnosis of respiratory tract infections: evaluation of the performance of the Respifinder assay compared to the xTAG respiratory viral panel assay. J. Clin. Virol. 52, 314–316. doi: 10.1016/j.jcv.2011.08.017
Shchepinov, M. S., Case-Green, S. C., and Southern, E. M. (1997). Steric factors influencing hybridisation of nucleic acids to oligonucleotide arrays. Nucleic Acids Res. 25, 1155–1161. doi: 10.1093/nar/25.6.1155
Skowronski, D. M., Chambers, C., Sabaiduc, S., De Serres, G., Winter, A. L., Dickinson, J. A., et al. (2016). A perfect storm: impact of genomic variation and serial vaccination on low influenza vaccine effectiveness during the 2014-2015 season. Clin. Infect. Dis. 63, 21–32. doi: 10.1093/cid/ciw176
Suntronwong, N., Klinfueng, S., Vichiwattana, P., Korkong, S., Thongmee, T., Vongpunsawad, S., et al. (2017). Genetic and antigenic divergence in the influenza A(H3N2) virus circulating between 2016 and 2017 in Thailand. PLoS One 12:e0189511. doi: 10.1371/journal.pone.0189511
Tang, J., Zhou, L., Gao, W., Cao, X., and Wang, Y. (2009). Visual DNA microarrays for simultaneous detection of human immunodeficiency virus type-1 and Treponema pallidum coupled with multiplex asymmetric polymerase chain reaction. Diagn. Microbiol. Infect. Dis. 65, 372–378. doi: 10.1016/j.diagmicrobio.2009.07.017
Tang, Q., Wang, J., Bao, J., Sun, H., Sun, Y., Liu, J., et al. (2012). A multiplex RT-PCR assay for detection and differentiation of avian H3, H5, and H9 subtype influenza viruses and Newcastle disease viruses. J. Virol. Methods 181, 164–169. doi: 10.1016/j.jviromet.2012.02.003
Uyeki, T. M. (2003). Influenza diagnosis and treatment in children: a review of studies on clinically useful tests and antiviral treatment for influenza. Pediatr. Infect. Dis. J. 22, 164–177. doi: 10.1097/01.inf.0000050458.35010.b6
Valenciano, M., Kissling, E., Reuss, A., Rizzo, C., Gherasim, A., Horvath, J. K., et al. (2016). Vaccine effectiveness in preventing laboratory-confirmed influenza in primary care patients in a season of co-circulation of influenza A(H1N1)pdm09, B and drifted A(H3N2), I-MOVE Multicentre Case-Control Study, Europe 2014/15. Eurosurveillance 21, 15–31. doi: 10.2807/1560-7917.ES.2016.21.7.30139
Weinberg, G. A., Erdman, D. D., Edwards, K. M., Hall, C. B., Walker, F. J., Griffin, M. R., et al. (2004). Superiority of reverse-transcription polymerase chain reaction to conventional viral culture in the diagnosis of acute respiratory tract infections in children. J. Infect. Dis. 189, 706–710. doi: 10.1086/381456
Wong, C. K., Tsang, G. C., Chan, K. H., Li, O. T., Peiris, M., and Poon, L. L. (2014). A novel molecular test for influenza B virus detection and lineage differentiation. J. Med. Virol. 86, 2171–2176. doi: 10.1002/jmv.23955
Wong, S., Pabbaraju, K., Lee, B. E., and Fox, J. D. (2009). Enhanced viral etiological diagnosis of respiratory system infection outbreaks by use of a multitarget nucleic acid amplification assay. J. Clin. Microbiol. 47, 3839–3845. doi: 10.1128/JCM.01469-09
World Health Organisation [WHO] (2013). Real-Time RT-PCR Protocol for the Detection of A(H7N9) Influenza Virus. Available at: http://www.chinacdc.cn/en/Research_5311/Guidelines/201304/W020130412821472784925.pdf
Wu, L., Ding, L., Pei, Z., Huo, X., Wen, G., and Pan, Z. (2013). A multiplex reverse transcription-PCR assay for the detection of influenza A virus and differentiation of the H1, H3, H5 and H9 subtypes. J. Virol. Methods 188, 47–50. doi: 10.1016/j.jviromet.2012.11.032
Keywords: multiplex asymmetric reverse transcription-PCR assay, electrochemical DNA sensor, Luminex RVP assay, influenza A viruses, subtype
Citation: Xu L, Jiang X, Zhu Y, Duan Y, Huang T, Huang Z, Liu C, Xu B and Xie Z (2018) A Multiplex Asymmetric Reverse Transcription-PCR Assay Combined With an Electrochemical DNA Sensor for Simultaneously Detecting and Subtyping Influenza A Viruses. Front. Microbiol. 9:1405. doi: 10.3389/fmicb.2018.01405
Received: 02 March 2018; Accepted: 07 June 2018;
Published: 27 June 2018.
Edited by:
Erna Geessien Kroon, UFMG – Universidade Federal de Minas Gerais, BrazilReviewed by:
Alexandre M. Vieira Machado, Fiocruz – Research Center Renê Rachou, BrazilPedro Augusto Alves, Fiocruz – Research Center Renê Rachou, Brazil
Copyright © 2018 Xu, Jiang, Zhu, Duan, Huang, Huang, Liu, Xu and Xie. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Zhengde Xie, eGllemhlbmdkZUBiY2guY29tLmNu
†These authors have contributed equally to this work.