 Wen-Yi Lv
Wen-Yi Lv Shuai Liu
Shuai Liu Linlin Zhang
Linlin Zhang Jian-Xin Zhou
Jian-Xin Zhou
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Med. , 05 March 2025
Sec. Intensive Care Medicine and Anesthesiology
Volume 12 - 2025 | https://doi.org/10.3389/fmed.2025.1561017
Background: During pressure support ventilation (PSV), the accuracy of non-invasive indicators in diagnosing high or low inspiratory effort has been validated. However, the correlation and agreement of these indicators remain unclear. This study aims to investigate the correlation and agreement among non-invasive inspiratory effort indicators, and to compare characteristics of inspiratory effort in neurocritical and non-neurocritical patients.
Methods: This was a single-centre prospective observational study. We collected three non-invasive inspiratory effort indicators, pressure muscular index (PMI), the maximal negative swing of airway pressure during expiratory occlusion (ΔPocc), and the airway occlusion pressure during the first 100ms (P0.1). Cutoff values for these indicators derived from esophageal pressure-time product (PTPmus) were chosen for this study. The correlation and agreement of these indicators were analyzed using Spearman’s rank correlation test and linear weighted Kappa analysis. Characteristics of PSV settings and inspiratory effort in neurocritical and non-neurocritical patients were compared.
Results: Ninety-seven patients were enrolled in this study. Correlation analysis showed a moderate correlation between PMI and ΔPocc (rho = −0.524, p < 0.001), ΔPocc and P0.1 (rho = 0.588, p < 0.001), while no correlation between PMI and P0.1 (rho = −0.140, p = 0.172). There was a moderate agreement between ΔPocc and P0.1 (k = 0.459, p < 0.001), a fair agreement between PMI and ΔPocc (k = 0.362, p < 0.001), but no agreement between PMI and P0.1 (k = 0.134, p = 0.072). The correlation of these indicators was similar in neurocritical patients compared with non-neurocritical patients, but agreement was poor.
Conclusion: The study showed that PMI and ΔPocc had moderate correlation and fair agreement, ΔPocc and P0.1 had moderate correlation and agreement, while PMI and P0.1 had no correlation and agreement.
Pressure support ventilation (PSV) is one of the most used ventilation modes for mechanically ventilated patients, particularly during the weaning process (1). In clinical practice, lung and diaphragm protective ventilation strategy is recommended to prevent high and low inspiratory efforts (2, 3), which can frequently occur during PSV (4, 5), and lead to complications affecting patient outcomes and increasing hospitalization expenses (2, 6–8).
The esophageal pressure-time product (PTPmus), calculated from esophageal pressure, is considered the gold standard for inspiratory effort (2, 9). However, this parameter is usually used for research purposes and not for routine clinical use because of the need for invasive procedures, special equipment, and complexity of calculations.
Recently, several non-invasive inspiratory effort indicators, such as pressure muscular index (PMI), the maximal negative swing of airway pressure during expiratory occlusion (ΔPocc), and the airway occlusion pressure during the first 100 ms (P0.1), have been found to have good ability to detect high or low inspiratory effort and can be directly measured on the ventilator screen without additional tools (10–14). In previous studies, high and low inspiratory effort cutoff values for PMI, ΔPocc, and P0.1 were derived from PTPmus (5, 14, 15). Although previous studies have validated the diagnostic accuracy of these indicators (5, 10, 13–16), the agreement among these measurements still remains underexplored.
Neurocritical care patients admitted to the intensive care unit (ICU) often require artificial airway and/or ventilation support due to impaired consciousness, poor airway protective ability, and damaged respiratory drive and conduction pathways. These patients face a higher risk of difficult weaning, delayed extubation, extubation failure, and tracheostomy (17–19). The characteristics of inspiratory effort in neurocritical patients and whether they differ from those in non-neurocritical patients are unknown.
The aim of this study was to investigate the correlation and agreement of non-invasive inspiratory effort indicators (PMI, ΔPocc and P0.1) in patients in the intensive care unit (ICU). The secondary aim was to compare characteristics of inspiratory effort in neurocritical and non-neurocritical patients.
This was a single-centre prospective observational study that enrolled adult patients aged 18–85 years. A total of 97 patients admitted to the ICU of Beijing Tiantan Hospital using PSV between January and August 2024 were included in this study. Patients younger than 18 years old, older than 85 years old, unable to measure the non-invasive inspiratory effort due to the ventilator incapability, receiving extracorporeal life support, or palliative care were excluded from the study. Neurocritical care patients specifically refer to the adult patients admitted to ICU for primary and/or secondary brain injuries. This study was presented according to STROBE guidelines (Supplementary File) and approved by the Institutional Review Board of Beijing Tiantan Hospital with approval number: KY2023-206-02 (January 2, 2024), and the informed consent was obtained in each participant.
All participants underwent three non-invasive inspiratory effort measurements, PMI, ΔPocc, and P0.1. To reduce the interference from continuous measurements and improve accuracy, each type of measurement was conducted three times, with an interval of at least 1 min between each measurement. The average of the three results was used for data analysis. A total of nine measurements were conducted in one patient.
The definitions and cutoff values for high and low inspiratory effort remain inconsistent across different studies (3, 20–25). PMI, ΔPocc, and P0.1 cutoff values derived from PTPmus were chosen for our study due to PTPmus is considered the gold standard for inspiratory effort (2, 9). According to Yang YL’s study, when high and low effort was defined as PTPmus > 200 and <50 cmH2O⋅s⋅min1, the cutoff values of PMI were 2.1 and 0 cmH2O, ΔPocc were −8.4 and −5.7 cmH2O, P0.1 were −2.2 and −1.1 cmH2O, respectively (5).
PMI. During PSV, after an end-inspiratory airway occlusion, the airway pressure (Paw) will reach a plateau (26). With the ventilator’s screen freeze function activated, the PMI can be measured on the ventilator screen as the difference between the plateau Paw and the peak Paw (11).
ΔPocc. During an expiratory airway occlusion, the patient’s inspiratory effort against the occluded airway causes the Paw to deviate, reaching a minimum value (Pnadir), and then returning to the baseline (13). The difference between Pnadir and the positive end-expiratory pressure (PEEP) on the ventilator screen can be calculated as ΔPocc.
P0.1. P0.1 is directly measured by the ventilators. Previous studies have showed that the P0.1 displayed by various ventilators could accurately reflects the P0.1 calculated using a reference method (14).
The ventilators involved in this study were Dräger Series (Dräger, Lubeck, Germany), Maquet Servo-i (Maquet Critical Care, Solna, Sweden), the Mindray SV Series (Myriad BioMedical Electronics, Shenzhen, China) and Prunus Padus 8 (PB Medical, Shenzhen, China).
All data were analyzed using the Statistical Program for Social Sciences (SPSS) version 25 (IBM Corporation, Armonk, NY, USA). Categorical variables were presented as counts and percentages, while continuous variables were expressed as means with standard deviations (SD) or medians with interquartile ranges (IQR). The Shapiro–Wilk test was used to assess the normality of the non-invasive inspiratory effort data, which was found to be non-normal distributed. The correlation and agreement were tested using Spearman’s rank correlation test and linear weighted Kappa analysis (k), respectively. The Spearman’s rank correlation coefficient (rho) classified the strength of the correlation as follows: negligible (rho = 0.00–0.09), weak (rho = 0.10–0.39), moderate (rho = 0.40–0.69), strong (rho = 0.70–0.89), and very strong (rho = 0.90–1.00) (27). The strength of agreement based on the weight Kappa coefficient (k) was interpreted as: slight (k = 0–0.20), fair (k = 0.21–0.40), moderate (k = 0.41–0.60), substantial (k = 0.61–0.80), and excellent (k = 0.81–1.00) (28). Neurocritical and non-neurocritical data were compared using independent samples t-tests or Mann-Whitney U nonparametric tests. For categorical variables, tests were performed using the chi-square test or Fisher’s exact test. All tests were two-sided, and a p < 0.05 was considered statistically significant.
A total of 97 patients (mean age, 63 ± 17.4 years; 63.9% male) were recruited in the study. The baseline demographics were shown in Table 1. According to the PTPmus-based PMI, ΔPocc, and P0.1 cutoff values, data were categorized into high, normal, and low inspiratory effort groups, respectively. The results showed that 34.0%, 52.6%, and 48.5% of patients may have low inspiratory effort, while 10.3%, 28.9%, and 20.6% of patients may have high inspiratory effort. 51.5% of the observation points showed the same classification between PMI and ΔPocc measurements, 39.2% between PMI and P0.1, and 58.8% between ΔPocc and P0.1.
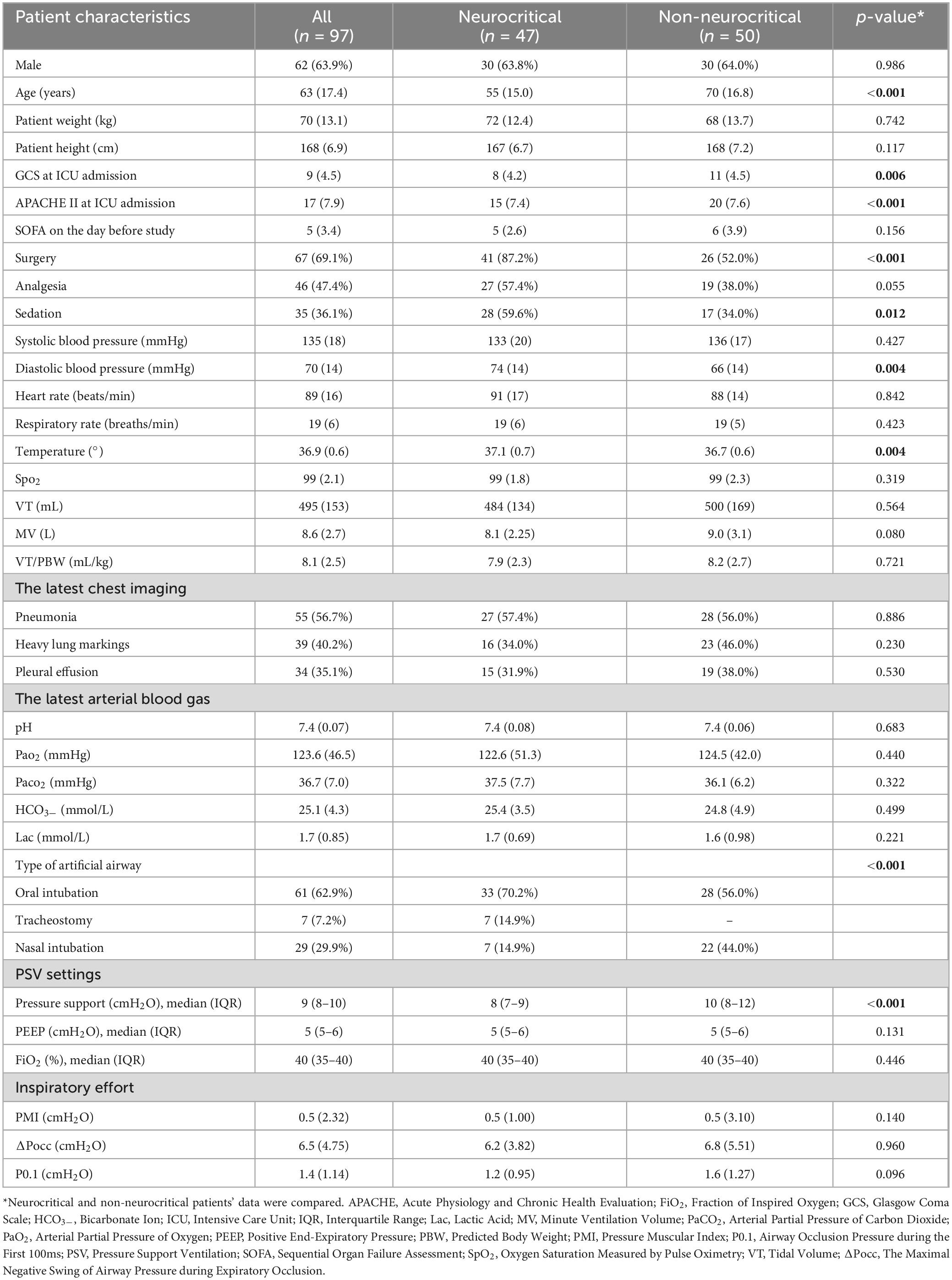
Table 1. Patients’ characteristics.
Compared to non-neurocritical patients, neurocritical patients were younger (55 vs 70 years, p < 0.001), had more postoperative patients (87.2% vs 52%, p < 0.001), lower GSC scores (8 vs 11, p = 0.006), lower APACHE II scores (15 vs 20, p < 0.001), more sedation use (59.6% vs 34%, p = 0.012), more tracheotomized patients (14.9% vs 0, p < 0.001), and lower pressure support (8 vs 10 cmH2O, p < 0.001) (Table 1). In neurocritical patients, based on PMI, ΔPocc, and P0.1 cutoff values, the proportions diagnosed with low inspiratory effort were 23.4, 51.1, and 57.4%, respectively, and the proportions with high inspiratory effort were 2.1, 25.5, and 17.0%, respectively.
The correlation and agreement analysis were shown in Table 2. In all patients, a moderate correlation was found between PMI and ΔPocc (rho = −0.524, p < 0.001), ΔPocc and P0.1 (rho = 0.588, p < 0.001), while no correlation between PMI and P0.1 (rho = −0.140, p = 0.172). There was a moderate agreement between ΔPocc and P0.1 (k = 0.459, p < 0.001), a fair agreement between PMI and ΔPocc (k = 0.362, p < 0.001), but no agreement between PMI and P0.1 (k = 0.134, p = 0.072).
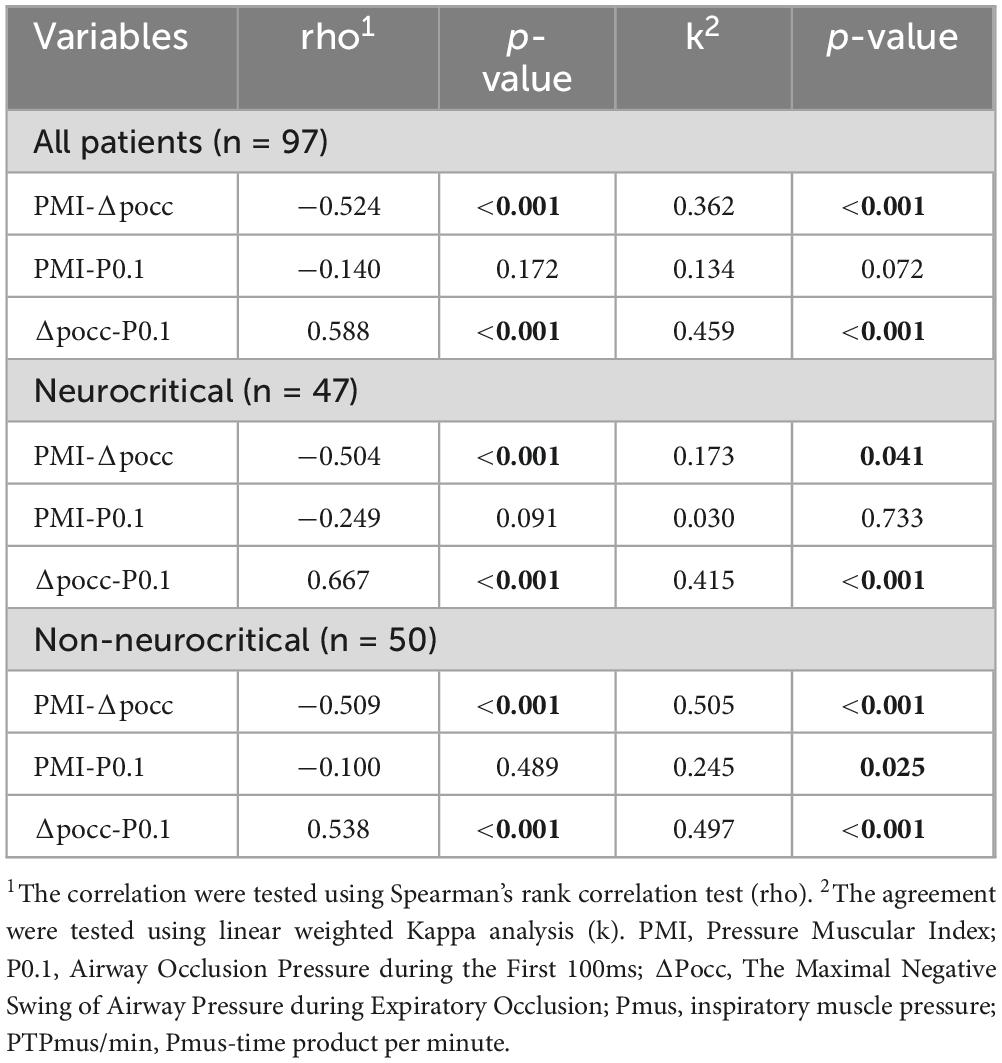
Table 2. Correlation and Agreement of PMI, ΔPocc, and P0.1.
Correlations among PMI, ΔPocc, and P0.1 were similar between neurocritical and non-neurocritical patients (Table 2). The agreement of inspiratory effort diagnosis was inferior in neurocritical patients (kPMI–ΔPocc = 0.173, p = 0.041; kPMI–P0.1 = 0.030, p = 0.733, kΔPocc–P0.1 = 0.415, p < 0.001) than in non-neurocritical patients (kPMI–ΔPocc = 0.505, p < 0.001; kPMI–P0.1 = 0.245, p = 0.025, kΔPocc–P0.1 = 0.497, p < 0.001) (Table 2).
In this study, the results indicated that PMI and ΔPocc had moderate correlation and fair agreement, ΔPocc and P0.1 had moderate correlation and moderate agreement, while PMI and P0.1 had no correlation and agreement. The correlation of non-invasive inspiratory effort indicators was similar in neurocritical patients compared with non-neurocritical patients, but agreement was poor. To our knowledge, this is the first study describing characteristics of inspiratory effort in neurocritical patients.
In our study, a larger proportion of patients had inspiratory effort outside the recommended physiologic range, which is similar to previous findings. According to the PTPmus-based PMI, ΔPocc, and P0.1 cutoff values, the results showed that 34.0%, −52.6% patients may have low inspiratory effort, while 10.3%–28.9% patients may have high inspiratory effort. Previous studies have also shown that over-assistance under PSV is not uncommon (4, 29).
Previous studies have shown that PMI, ΔPocc, and P0.1 have good accuracy in detecting high and low inspiratory effort in mechanical ventilation patients. However, the definitions and cutoff values for high and low inspiratory effort remain inconsistent across different studies (3, 20–25). For detecting high inspiratory effort [defined as changes in transdiaphragmatic pressure [ΔPdi] > 12 cmH2O (10), changes in esophageal pressure [ΔPes] > 12 cmH2O (16), Pmus > 10 cmH2O (5, 13), or PTPmus > 200 cmH2O⋅s⋅min1 (5, 14, 15)], PMI cutoff values range between 2.1 and 3.8 cmH2O (5, 16) (AUC 0.93, sensitivity 68%–88%, specificity 81%–92%); ΔPocc cutoff values between 8.4 and 17.9 cmH2O (5, 10, 13, 16) (AUC 0.86–0.93, sensitivity 80%–100%, specificity 67%–84%); and P0.1 cutoff values between 2.0 and 4.0 cmH2O (5, 10, 15, 16, 30) (AUC 0.73–0.95, sensitivity 52%–100%, specificity 72%–94%). On the other hand, for detecting low inspiratory effort [defined as ΔPdi < 3 cmH2O (10), ΔPes < 5 cmH2O (16), Pmus < 5 cmH2O (5), or PTPmus < 50 cmH2O⋅s⋅min1 (5, 14)], PMI cutoff values range between −0.4 and 0.0 cmH2O (5, 16) (AUC 0.89–0.95, sensitivity 30%–96%, specificity 86%–95%), ΔPocc cutoff values between 5.7 and 7.5 cmH2O (5, 10, 16) (AUC 0.93–0.97, sensitivity 60%–88%, specificity 85%–95%), and P0.1 cutoff values between 0.9 and 1.3 cmH2O (5, 10, 16, 30) (AUC 0.87–0.93, sensitivity 65%–100%, specificity 61%–89%).
Due to the lack of uniform definitions for high and low inspiratory effort, various criteria have been used across studies, resulting in different cutoff values. In our study, only the gold standard PTPmus-based cutoff values of PMI, ΔPocc, and P0.1 were selected for the diagnosis of high or low inspiratory effort. However, only one study derived cutoff values for PMI, ΔPocc, and P0.1 based on the PTPmus (5). These suggest that the cutoff values used in our study may not accurately diagnose high or low inspiratory effort, which may lead to discrepancies in diagnosis based on PMI, ΔPocc, and P0.1, which explains their limited agreements.
In our study, we found that the correlations among PMI, ΔPocc, and P0.1 were similar in neurocritical patients compared with non-neurocritical patients, but agreement was poor. This may be because cutoff values provided by previous studies were not specific to neurocritical care patients, the thresholds used in our study may not be applicable to these population. In our study, nearly half of the study participants were neurocritical care patients, who differ from non-neurological patients in their need for mechanical ventilation, not only due to pulmonary or cardiac causes, but also brain-related factors such as impaired consciousness, decreased airway protection, and disrupted respiratory drive (17, 18, 31–33).
Respiration is a complex process involving multiple organs and systems. Respiratory movements in mammals are driven by rhythmic neural activity generated spatially and functionally by a brainstem neural network consisting of the respiratory central pattern generator (RCPG) (34). Neurological influences on respiration also include chemoreceptor modulation (35), airway protective reflexes (32), respiratory functional plasticity (36), and neurotransmitter remodeling of respiratory patterns (37). These complex respiratory regulatory systems are susceptible to brain damage. Neurocritical care patients may exhibit different inspiratory effort cutoff values compared to non-neurological patients. The cutoff value of the noninvasive inspiratory effort indicators in neurocritical care patients may require further study.
In our study, we averaged three separate measurements of PMI, ΔPocc, and P0.1, with at least a 1-min interval between each measurement, to reduce the interference from continuous measurements and improve accuracy. The patient’s inspiratory effort may vary from breath to breath. The inspiratory effort values obtained from PMI, ΔPocc, and P0.1 did not represent the same breath, which may weaken correlation and agreement.
There are several limitations to our study. First, the study included a small number of patients and measurement points. Since the study only included patients from a single medical center and nearly half of the study participants were neurocritical care patients, the findings might not be generalizable to other patients. Second, our study did not include the gold standard for comparison. We did not perform oesophageal manometry, so the accuracy of the diagnosis based on PMI, POCC, and P0.1 is not known. Finally, the order of measurement of noninvasive inspiratory effort indicators was fixed, which increased the bias of our study.
In conclusion, this study compared PMI, ΔPocc, and P0.1 as non-invasive tools for measuring inspiratory effort in ICU patients. The study showed that PMI and ΔPocc had moderate correlation and fair agreement, ΔPocc and P0.1 had moderate correlation and agreement, while PMI and P0.1 had no correlation and agreement.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by Institutional Review Board of Beijing Tiantan Hospital with approval number: KY2023-206-02. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
W-YL: Conceptualization, Data curation, Formal Analysis, Methodology, Writing – original draft. SL: Data curation, Formal Analysis, Writing – review and editing. LZ: Conceptualization, Methodology, Supervision, Writing – review and editing. J-XZ: Conceptualization, Funding acquisition, Methodology, Supervision, Writing – review and editing.
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This work was supported by Capital’s Funds for Health Improvement and Research (CFH 2024-1-2081) and the Clinical and Research Center Program of Capital Medical University (CMU-2023-45).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors declare that no Generative AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2025.1561017/full#supplementary-material
1. Brochard LJ, Lellouche F. Pressure support ventilation. In: MJ Tobin editor. Principles and Practice of Mechanical Ventilation. New York: McGraw Hill Companies (2013). 199–227.
2. Goligher E, Jonkman A, Dianti J, Vaporidi K, Beitler J, Patel B, et al. Clinical strategies for implementing lung and diaphragm-protective ventilation: Avoiding insufficient and excessive effort. Intensive Care Med. (2020) 46:2314–26. doi: 10.1007/s00134-020-06288-9
3. Bertoni M, Spadaro S, Goligher E. Monitoring patient respiratory effort during mechanical ventilation: Lung and diaphragm-protective ventilation. Crit Care. (2020) 24:106. doi: 10.1186/s13054-020-2777-y
4. Al-Bassam W, Dade F, Bailey M, Eastwood G, Osawa E, Eyeington C, et al. Likely overassistance” during invasive pressure support ventilation in patients in the intensive care unit: A multicentre prospective observational study. Crit Care Resusc. (2019) 21:18–24.
5. Yang Y, Liu Y, Gao R, Song D, Zhou Y, Miao M, et al. Use of airway pressure-based indices to detect high and low inspiratory effort during pressure support ventilation: A diagnostic accuracy study. Ann Intensive Care. (2023) 13:111. doi: 10.1186/s13613-023-01209-7
6. Goligher E, Dres M, Fan E, Rubenfeld G, Scales D, Herridge M, et al. Mechanical ventilation-induced diaphragm atrophy strongly impacts clinical outcomes. Am J Respir Crit Care Med. (2018) 197:204–13. doi: 10.1164/rccm.201703-0536OC
7. Goligher E, Brochard L, Reid W, Fan E, Saarela O, Slutsky A, et al. Diaphragmatic myotrauma: A mediator of prolonged ventilation and poor patient outcomes in acute respiratory failure. Lancet Respir Med. (2019) 7:90–8. doi: 10.1016/S2213-2600(18)30366-7
8. Vaporidi K, Akoumianaki E, Telias I, Goligher E, Brochard L, Georgopoulos D. Respiratory drive in critically Ill patients. Pathophysiology and clinical implications. Am J Respir Crit Care Med. (2020) 201:20–32. doi: 10.1164/rccm.201903-0596SO
9. Doorduin J, van Hees H, van der Hoeven J, Heunks L. Monitoring of the respiratory muscles in the critically Ill. Am J Respir Crit Care Med. (2013) 187:20–7. doi: 10.1164/rccm.201206-1117CP
10. de Vries H, Tuinman P, Jonkman A, Liu L, Qiu H, Girbes A, et al. Performance of noninvasive airway occlusion maneuvers to assess lung stress and diaphragm effort in mechanically ventilated critically Ill patients. Anesthesiology (2023) 138:274–88. doi: 10.1097/ALN.0000000000004467
11. Kyogoku M, Shimatani T, Hotz J, Newth C, Bellani G, Takeuchi M, et al. Direction and magnitude of change in plateau from peak pressure during inspiratory holds can identify the degree of spontaneous effort and elastic workload in ventilated patients. Crit Care Med. (2021) 49:517–26. doi: 10.1097/ccm.0000000000004746
12. Albani F, Pisani L, Ciabatti G, Fusina F, Buizza B, Granato A, et al. Flow index: A novel, non-invasive, continuous, quantitative method to evaluate patient inspiratory effort during pressure support ventilation. Crit Care. (2021) 25:196. doi: 10.1186/s13054-021-03624-3
13. Bertoni M, Telias I, Urner M, Long M, Del Sorbo L, Fan E, et al. A novel non-invasive method to detect excessively high respiratory effort and dynamic transpulmonary driving pressure during mechanical ventilation. Crit Care. (2019) 23:346. doi: 10.1186/s13054-019-2617-0
14. Telias I, Junhasavasdikul D, Rittayamai N, Piquilloud L, Chen L, Ferguson N, et al. Airway occlusion pressure as an estimate of respiratory drive and inspiratory effort during assisted ventilation. Am J Respir Crit Care Med. (2020) 201:1086–98. doi: 10.1164/rccm.201907-1425OC
15. Rittayamai N, Beloncle F, Goligher E, Chen L, Mancebo J, Richard J, et al. Effect of inspiratory synchronization during pressure-controlled ventilation on lung distension and inspiratory effort. Ann Intensive Care. (2017) 7:100. doi: 10.1186/s13613-017-0324-z
16. Ito Y, Herrera M, Hotz J, Kyogoku M, Newth C, Bhalla A, et al. Estimation of inspiratory effort using airway occlusion maneuvers in ventilated children: A secondary analysis of an ongoing randomized trial testing a lung and diaphragm protective ventilation strategy. Crit Care. (2023) 27:466. doi: 10.1186/s13054-023-04754-6
17. Pelosi P, Ferguson N, Frutos-Vivar F, Anzueto A, Putensen C, Raymondos K, et al. Management and outcome of mechanically ventilated neurologic patients. Crit Care Med. (2011) 39:1482–92. doi: 10.1097/CCM.0b013e31821209a8
18. Karanjia N, Nordquist D, Stevens R, Nyquist PA. Clinical description of extubation failure in patients with primary brain injury. Neurocrit Care. (2011) 15:4–12. doi: 10.1007/s12028-011-9528-5
19. Zhang L, Liu S, Wang S, Zhou J. Diseases tNCfHQMiN, medicine CSOCC, et al. Chinese expert consensus on sedation and analgesia for neurocritical care patients. Chin Med J. (2024) 137:1261–3.
20. de Vries H, Jonkman A, de Grooth H, Duitman J, Girbes A, Ottenheijm C, et al. Lung- and diaphragm-protective ventilation by titrating inspiratory support to diaphragm effort: A randomized clinical trial. Crit Care Med. (2022) 50:192–203. doi: 10.1097/CCM.0000000000005395
21. Lassola S, Miori S, Sanna A, Cucino A, Magnoni S, Umbrello M. Central venous pressure swing outperforms diaphragm ultrasound as a measure of inspiratory effort during pressure support ventilation in Covid-19 patients. J Clin Monit Comput. (2022) 36:461–71. doi: 10.1007/s10877-021-00674-4
22. Giustivi D, Giustivi D, Bottazzini F, Bottazzini F, Belliato M, Belliato M. Respiratory monitoring at bedside in Covid-19 patients. J Clin Med. (2021) 10: 4943.
23. Mauri T, Yoshida T, Bellani G, Goligher E, Carteaux G, Rittayamai N, et al. Esophageal and transpulmonary pressure in the clinical setting: Meaning, usefulness and perspectives. Intensive Care Med. (2016) 42:1360–73. doi: 10.1007/s00134-016-4400-x
24. de Vries H, Jonkman A, Shi Z, Spoelstra-de Man A, Heunks L. Assessing breathing effort in mechanical ventilation: Physiology and clinical implications. Ann Transl Med. (2018) 6:387. doi: 10.21037/atm.2018.05.53
25. Tams C, Euliano N, Martin A, Banner M, Gabrielli A, Bonnet S, et al. Patients alter power of breathing as the primary response to changes in pressure support ventilation. J Crit Care. (2020) 57:208–13. doi: 10.1016/j.jcrc.2020.03.004
26. Natalini G, Buizza B, Granato A, Aniballi E, Pisani L, Ciabatti G, et al. Non-Invasive assessment of respiratory muscle activity during pressure support ventilation: Accuracy of end-inspiration occlusion and least square fitting methods. J Clin Monit Comput. (2021) 35:913–21. doi: 10.1007/s10877-020-00552-5
27. Schober P, Boer C, Schwarte L. Correlation coefficients: Appropriate use and interpretation. Anesth Analg. (2018) 126:1763–8. doi: 10.1213/ANE.0000000000002864
28. Landis J, Koch G. The measurement of observer agreement for categorical data. Biometrics. (1977) 33:159–74.
29. Miao M, Chen W, Zhou Y, Gao R, Song D, Wang S, et al. Validation of the flow index to detect low inspiratory effort during pressure support ventilation. Ann Intensive Care. (2022) 12:89. doi: 10.1186/s13613-022-01063-z
30. Telias I, Damiani F, Brochard L. The airway occlusion pressure (P(0.1)) to monitor respiratory drive during mechanical ventilation: Increasing awareness of a not-so-new problem. Intensive Care Med. (2018) 44:1532–5. doi: 10.1007/s00134-018-5045-8
31. Schaller B, Graf R, Jacobs A. Pathophysiological changes of the gastrointestinal tract in ischemic stroke. Am J Gastroenterol. (2006) 101:1655–65. doi: 10.1111/j.1572-0241.2006.00540.x
32. Seeholzer L, Julius D. Neuroendocrine cells initiate protective upper airway reflexes. Science. (2024) 384:295–301. doi: 10.1126/science.adh5483
33. Luo X, He X, Zhou Y, Zhou J, Chen G, Li H, et al. Ineffective effort in patients with acute brain injury undergoing invasive mechanical ventilation. Respir Care. (2023) 68:1202–12. doi: 10.4187/respcare.10596
34. Smith J, Abdala A, Borgmann A, Rybak I, Paton J. Brainstem Respiratory Networks: Building Blocks and Microcircuits. Trends Neurosci. (2013) 36:152–62. doi: 10.1016/j.tins.2012.11.004
35. Guyenet P, Mulkey D, Stornetta R, Bayliss D. Regulation of ventral surface chemoreceptors by the central respiratory pattern generator. J Neurosci. (2005) 25:8938–47. doi: 10.1523/JNEUROSCI.2415-05.2005
36. Feldman J, Mitchell G, Nattie E. Breathing: Rhythmicity, plasticity, chemosensitivity. Annu Rev Neurosci. (2003) 26:239–66. doi: 10.1146/annurev.neuro.26.041002.131103
Keywords: mechanical ventilation, pressure support ventilation, inspiratory effort, PMI, ΔPocc, P0.1
Citation: Lv W-Y, Liu S, Zhang L and Zhou J-X (2025) Assessing agreement among non-invasive indicators for inspiratory effort during pressure support ventilation. Front. Med. 12:1561017. doi: 10.3389/fmed.2025.1561017
Received: 15 January 2025; Accepted: 20 February 2025;
Published: 05 March 2025.
Edited by:
Penglin Ma, Guiqian International General Hospital, ChinaReviewed by:
Feng Shen, Affiliated Hospital of Guizhou Medical University, ChinaCopyright © 2025 Lv, Liu, Zhang and Zhou. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Linlin Zhang, YWJsdWVsZW1vbkAxNjMuY29t; Jian-Xin Zhou, emhvdWp4LmNuQGljbG91ZC5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.