 Cindy E. Frias1*
Cindy E. Frias1* Nimesh Samarasinghe2
Nimesh Samarasinghe2 Cecilia Cuzco3
Cecilia Cuzco3 Jaseem Koorankot2
Jaseem Koorankot2 Andrés de Juan1
Andrés de Juan1 Husameldin Mohamed Ali Rudwan2
Husameldin Mohamed Ali Rudwan2 Hanan F. Abdul Rahim4
Hanan F. Abdul Rahim4 Adela Zabalegui1Iain Tulley2
Adela Zabalegui1Iain Tulley2 Sanaa T. Al-Harahsheh5Mona Shaheen S. T. Al-Homaiddi2
Sanaa T. Al-Harahsheh5Mona Shaheen S. T. Al-Homaiddi2 Meredith Fendt-Newlin6
Meredith Fendt-Newlin6 Jim Campbell6
Jim Campbell6- 1Hospital Clinic of Barcelona, Barcelona, Spain
- 2Hamad Medical Corporation, Doha, Qatar
- 3Fundamentals and Clinical Nursing Department, University of Barcelona, Barcelona, Spain
- 4College of Health Sciences, Qatar University, Doha, Qatar
- 5Qatar Foundation, Doha, Qatar
- 6World Health Organization, Geneva, Switzerland
Background: Countries globally face challenges in educating, employing and retaining their health and care workforce, largely due to underinvestment in health systems. Health and care workforce report significantly greater levels of job-related burnout and mental health problems, which in turn are associated with poorer patient outcomes, increased medical errors, diminished quality and safety, decreased patient satisfaction, and reduced healthcare efficiency.
Objective: We conducted a rapid review of systematic reviews to evaluate the mental health and well-being of health and care workers since the onset of the COVID-19 pandemic and to identify interventions available at organizational and individual levels.
Methods: PubMed and Epistemonikos were searched for systematic reviews published between May 2022 and February 2024. The inclusion criteria were systematic reviews written in English with quantitative design, with or without meta-analysis.
Results: Fifty articles met the criteria for inclusion in the analysis. Overall, there has not been a significant change in the prevalence of depression and anxiety among health and care workforce since 2022, suggesting the impact of the COVID-19 pandemic on workers’ mental health and well-being was not specific to their experience working during the pandemic. Sixteen studies reported two types of mental health and well-being interventions: individual-level interventions and organizational-level interventions with specific impact on mental health and work environment variables. No specific policy interventions were found. However, some studies suggested policy interventions to improve the mental health and well-being of the health and care workforce.
Discussion: Our analysis highlighted the need for systemic changes to protect the mental health and well-being of the health and care workforce in the post-COVID-19 era. Despite the wealth of evidence on mental health problems and on effective interventions, there remains a notable gap in systemic implementation and organizational accountability. The call to action for a paradigm shift must be embraced and we must strive to build resilient healthcare systems and invest in active support and sustain them, incorporating structural, non-structural and functional aspects of organizational resilience.
1 Introduction
Countries worldwide face significant challenges in educating, employing, and retaining their health and care workforce, largely due to underinvestment in health systems. These challenges are particularly pronounced in low-income countries and among the 55 countries listed on the WHO Support and Safeguards List 2023 (1). Where shortages, low pay, unsafe working conditions, and high-stress levels persist (2). These systemic issues have led to a growing mental health burden among health and care workers (HCWs), exacerbating burnout, absenteeism, and reduced job satisfaction (2, 3). The resulting impacts extend beyond individual workers, contributing to poorer patient outcomes, decreased healthcare efficiency, and widening gaps in healthcare delivery (3, 4).
The World Health Organization (WHO) defines HCWs as individuals engaged in work actions intended to improve health, including doctors, nurses, midwives, public health professionals, community health workers, and traditional medicine practitioners (4). Mental health, defined by the WHO as a state of well-being that enables individuals to cope with life stresses and contribute to their communities, is a critical component of overall health and a fundamental human right (5, 6). Similarly, well-being, encompassing quality of life and societal resilience, is influenced by social, economic, and environmental conditions (7). These definitions highlight the urgent need to address mental health and well-being as central components of workforce sustainability (7, 8).
The COVID-19 pandemic exposed and intensified preexisting vulnerabilities within healthcare systems, placing HCWs under immense pressure. During this period, HCWs experienced increased workloads, emotionally charged situations, and stigma surrounding mental health care, resulting in heightened levels of anxiety, depression, and burnout (9, 10). These challenges highlighted the inadequacy of organizational support structures and the need for systemic changes to safeguard HCWs' mental health and well-being (10–14).Building on the recommendations “Our Duty of Care: A global call to action to protect the mental health of health and care workers,” (15) this rapid review evaluates the mental health and well-being of HCWs since the onset of the COVID-19 pandemic. It is further informed by World Health Assembly (WHA) Resolution 74.14 (16) which called for the development of the Global Compact for Health and Care Workers to alleviate mental health disorders and improve HCW well-being. The review also draws on other WHO guidelines on mental health at work to identify supportive interventions and programs. Specifically, it examines individual and organizational level interventions aimed at addressing these challenges. Despite the wealth of evidence and guidance, the systemic implementation of such measures remains limited. By synthesizing recent findings, this review seeks to address this gap and propose strategies to safeguard HCWs’ mental health and build resilience within healthcare systems (11, 17).
Therefore, this rapid review aims to evaluate the mental health and well-being of health and care workers since the onset of the COVID-19 pandemic and to identify interventions available at organizational and individual levels.
2 Materials and methods
We conducted this Rapid Review using Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) guidelines (18). Two authors independently conducted the literature search, study selection, and data extraction. Any disagreements were resolved by discussion with a third author when necessary.
2.1 Study search
The literature search utilized two electronic databases PubMed and Epistemonikos. Both were also used in the 2022 Our Duty of Care report (15). The latter database focuses on systematic reviews and regularly updates from several databases including the Cochrane Database of Systematic Reviews (CDSR), EMBASE, and PsycINFO. The search strategy used for both databases was partially based on the previous Our Duty of Care report. For PubMed database, the following search strategy was implemented: (“Mental Health”[Mesh] OR “Anxiety”[Mesh] OR “Depression”[Mesh] OR Burnout OR Distress OR Stress) AND (“Nurses”[Mesh]) OR “Physicians”[Mesh] OR Doctors OR Health Care Workers OR Health Workers)] NOT (Pati* OR Qualitative OR Scoping OR Synthesis). For Epistemonikos database, the following search strategy was used with some minor changes respecting the other: Mental Health OR Anxiety OR Depression OR Burnout OR Distress OR Stress AND Nurses OR Physicians OR Doctors OR Health Care Workers OR Health Workers NOT Pati* NOT Qualitative NOT Scoping NOT Synthesis. The search was limited from the period of May 2022 (which was the final period carried out for the Our Duty of Care Report, 2022) to February 2024. The terms chosen for both databases can be seen in Supplementary material S1.
2.2 Inclusion criteria
The inclusion criteria chosen were nearly identical to those used in the previous review 2 years ago to ensure consistency in addressing the same area. However, for this review, the articles did not need to measure the impact of COVID-19 specifically, as many recent studies no longer consider it a primary focus. Inclusion criteria were English-language, quantitative systematic reviews with or without meta-analysis, available in full text and published between May 2022 and February 2024. Additionally, articles were required to include a mental health outcome, including burnout or stress, anxiety, depression, suicidal ideation, trauma, insomnia, and/or sleep disturbances. Moreover, the selected articles focused on or included the health and care workforce, such as physicians, nurses, community health workers, physical therapists, pharmacists, and other related professions. All these criteria were followed based on the duty of care report protocol.
2.3 Exclusion criteria
The exclusion criteria were as follows: studies including healthcare students or the general population with no separate analysis of the health and care workforce, publications other than systematic reviews or with qualitative or mixed methods designs, studies written in languages other than English and studies that did not measure or did not track any mental health related outcome such as those specified in the inclusion criteria.
2.4 Study selection
In the first screening process, two independent researchers (AD and CC) screened the titles and abstracts of the searched documents from both databases to identify potentially related articles meeting the eligibility criteria. To remove duplicates, the Zotero® and Rayyan® platforms were used. The titles and abstracts were initially read, according to the pre-established criteria, by two independent reviewers; besides, the same researchers independently reviewed the selected full texts. The final inclusion of studies was decided through the two-step screening process. In the screening process, discrepancies between the researchers were resolved through discussion with a third researcher (CF). The study selection process is presented following a PRISMA flow diagram in Figure 1.
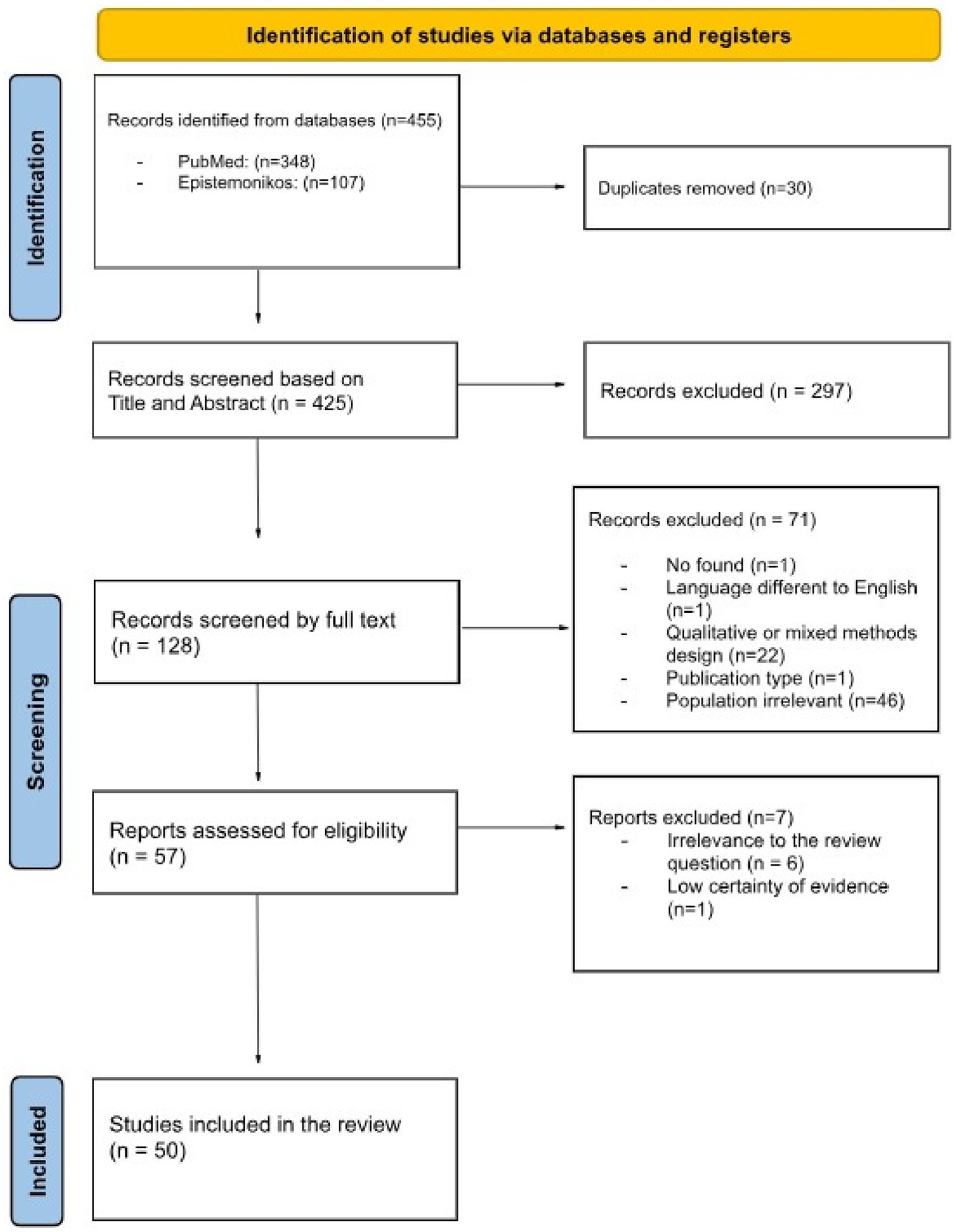
Figure 1. PRISMA flowchart of the study selection process.
2.5 Risk of bias assessment
The current review did not conduct a formal risk of bias or quality assessment, which is often omitted in rapid reviews. Due to the limited time available for data analysis and considering that all included articles were systematic reviews—most of which had already assessed the methodological quality of the studies within them—no additional specific risk of bias assessment was conducted. However, we ensured that all included studies had undergone a prior risk of bias evaluation, thereby enhancing the reliability and robustness of the evidence.
2.6 Data extraction
Data extraction was conducted independently by two reviewers (AD and CC) to ensure accuracy and consistency. Any conflicts were resolved by a third reviewer (CF). To ensure the integrity of the assessment, we piloted the data extraction form on three studies. The extracted data included publication date, author(s), the title of the study, study design, country or geographic area covered, total population size, types of health and care workforce included in the study, an assessment tool to measure mental health burden and well-being, and the aim of studies related to mental health variables and well-being.
2.6.1 Data analysis
To conduct a detailed and comprehensive analysis of the results of each included study, a description table was designed to extract all relevant data related to the main outcomes related to mental health burden, well-being, and work environment. In addition, for each included article, we analyzed whether the interventions aimed at improving health and care workers’ mental health or well-being had been designed for implementation at an organizational or individual level and the benefits obtained on mental health, well-being, and the work environment. Finally, each included study was also analyzed to see if recommendations at the government level based on actions at the policy level were presented.
3 Results
3.1 Study search
The flowchart of the study selection process is shown in Figure 1. The initial search found 455 references. After removing duplicates, 425 records were screened by title and abstract. Then, 128 full-text articles were retrieved for detailed evaluation. After review, 71 articles were removed for the following reasons: wrong study design (i.e., qualitative design only or qualitative design combined with other design) (N = 22), wrong population (N = 46), and other reasons (N = 3). “Wrong population” refers to studies on students or the general population instead of health and care workers. “Other reasons” include studies not being in English, wrong publication type, or not being found. Fifty seven studies were assessed for eligibility, leading to the exclusion of 7 studies. Fifty studies were finally included. Therefore, the intervention of the third reviewer was not necessary.
3.2 Characteristics of the articles included
An overview of the 50 studies selected for data extraction and analysis is presented in Supplementary Table 1. Fifty studies were included, of which 34 included a meta-analysis, and 16 were systematic reviews without meta-analyses. The studies were conducted in China (n = 19), France (n = 5), England (n = 4), Korea (n = 4), and Brazil (n = 3). One study was conducted in each of the following countries: Canada, Greece, South Africa, India, Lebanon, Saudi Arabia, Singapore, Finland, USA, Romania, Spain, Hungary, Indonesia, and Australia.
3.3 Participants
In the studies, the sample sizes ranged from 29 HCWs (19) to more than 341,014 (20) HCWs. Samples were predominantly female (at least more than 50% in 14 of the included studies). Most of the participants were nurses and doctors. Some studies also included the participation of midwives (21), occupational therapists, speech therapists (22), social workers (23), dentists (24, 25), technicians and administrative staff (26), paramedics, laboratory and X-ray technicians (19, 20, 23, 27–29).
3.4 Aim of the articles included
The studies measured mental health outcomes, including anxiety, depression, burden, and Post Traumatic Stress Disorder (PTSD), and well-being outcomes, such as job stress and satisfaction, sleep disorders, quality of life (QoL), general health and job stalking (job stalking is described as unwanted harassing behavior towards health and care workforce from patients or even from patients’ relatives). It is undesirable and repeated behavior, including following or monitoring someone, writing letters, calling by phone, communicating on the Internet, giving unsolicited gifts, and making annoying requests (30) and presenteeism. Likewise, some results associated with the work environment, such as workplace bullying, were evaluated.
3.5 Main results
3.5.1 The mental health and well-being of HCWs since the COVID-19 pandemic
The updated prevalence estimates for anxiety were lower than for the general population, especially for men and women (28) until study estimates ranged from 6 to 90% (20). The level of depression symptoms was also lower than for the general population (28) rates varied until 91.30% (M = 27.23%, M = 23.28%) (23).
HCW reported that burnout and moral distress were conditions that had been present since before the pandemic, but that worsened due to the pressure of care at that time. This worsening was more evident in specific health and care groups, such as nurses and doctors. However, no significant differences have been observed compared to the previous report’s data, even if it has been noted that Intensive Care Unit (ICU) doctors and nurses exhibit higher levels of burnout, with 42 and 45%, respectively. An analysis of 20,723 ICU professionals revealed that the prevalence of high burnout levels did not differ significantly (p = 0.63) between ICU physicians (0.41 [95% CI, 0.33; 0.5]) and ICU nurses (0.44 [95% CI, 0.34; 0.55]) However, the proportion of ICU professionals with a high level of emotional exhaustion was higher in ICU nurses than in ICU physicians (0.42 [95% CI, 0.37; 0.48] and 0.28 [0.2; 0.39], respectively, p = 0.022) (31). We found burnout prevalence rates until 95% (32). A meta-regression analysis showed that the association between workplace bullying, and job burnout was stronger in studies with a higher percentage of females (coefficient beta = 0.01, 95% CI = 0.006 to 0.019, p = 0.001) (33). Several studies have examined the relationship between sociodemographic variables and burnout. Findings indicate that gender is not a significant predictor of burnout. However, educational attainment demonstrates a significant association, with nurses holding bachelor’s degrees exhibiting the highest levels of burnout among all academic groups (34).
The overall prevalence of PTSD ranged between 14% and 16% during the pandemic, 19% between 1 and 6 months after the end of the pandemic, then decreased to 8% over a year later. According to the results of our rapid review the prevalence of PTSD was lower after the pandemic ended and tended to be lower after the following year (22). However, it is noted that alterations in the sleep–wake cycle pattern are still present in HCWs. Some authors also found a high level of sleep disturbance with a prevalence of insomnia (46.9, 95% CI: 31.8, 62.5%; I2 = 97.7%, p < 0.001) (35).
A revision showed the prevalence of PTSD was 65.9% (IC 95%: 62.6%, 69%; I2=0%, p < 0.001) (35).Other mental health problems were found: 18.8% of men and 10.7% of women used alcohol to cope. 22.8% reported a lifetime suicidal ideation, with 10.4% reporting serious suicidal ideation and 3.1% reporting having previously attempted suicide. No gender difference was found, but there was a higher prevalence of women who ‘wished they were dead’ (28). One study found the rate of suicidal thoughts to be 1.5 to 3 times higher than the national average, but only 26% of those with suicidal thoughts had sought help, and 60% of those with suicidal ideation were hesitant to seek help due to concerns about their career (36). A review revealed that the rates of fear occurrence were (52.1, 95% CI: 30.1, 73.3%; I2 = 98.1%, p < 0.001) (35) (Supplementary Table 2). Supplementary Table 3 describes the prevalence of mental health disorders by region and occupation.
3.5.2 Evidence of interventions
This rapid review also considered studies that provided interventions that addressed outcomes related to the mental health and well-being of HCWs, in any clinical care setting where health and care workforce provide care.
Of the 50 studies included, 16 studies reported the outcomes of interventions on health and care workforce’s mental health and well-being. After analyzing each one of them, they were classified into two types of interventions: interventions at the individual level and at the organizational level. These types of interventions or categories are based on the WHO guidelines on mental health at work. In these guidelines, the WHO provides evidence-based global public health guidance on organizational and individual interventions for the promotion of positive mental health and the prevention of mental health conditions, as well as recommendations on returning to work after absence associated with mental health conditions and obtaining employment for people living with mental health conditions (37).
3.5.2.1 Individual-level interventions
In the included reviews, various interventions were carried out at the individual level, such as single interventions with one or several sessions, multi-component interventions, and interventions focused on alleviating mental health symptoms to also improve emotional well-being.
a. Interventions with one or more sessions: Well-being Centers: These centers were equipped with staff (‘well-being buddies’) trained to offer psychological first aid to personnel of an acute hospital trust (listening, comforting and directing towards services, as needed) (38). Training Programs: Simulation-based teamwork training to develop leadership and communication skills, crucial during crises (38). Resilience Training Program (“R2 for Leaders”): Comprising virtual sessions to equip healthcare leaders with skills for organizational leadership and staff support (38). Psychoeducation programs showed a significant impact on stress reduction and how nurses cope with challenges using positive coping mechanisms (39).
b. Multi-component interventions: Specific Multi-Component Programs: Workplace recognition; infection protection measures, reasonable work shift arrangements, logistical support, reorganization of wards and increased nurse-to-patient ratios; training on PPE use and its availability; establishment of a psychological help desk, promotion of autonomy among nurses, limiting work hours, adjusting staffing levels, providing information updates, offering immune-boosting supplements, and mental health support services. The multi-component prevention programs demonstrate potential protective effects, such as reducing anxiety and depression, and enhancing the quality of the psychosocial work environment, including job control, managerial and peer support, and workplace relationships. However, the confidence in these findings is low due to reliance on observational study designs and significant risks of selection and confounding bias (38).
c. Interventions focused on alleviating specific symptoms: Mindfulness-based interventions (MBI): focused on stress reduction using relaxation, yoga, breathing, and physical exercise. The evidence suggests that MBI training moderately reduces stress, but it shows no significant effect on anxiety (40). However, some authors concluded that MBI appears to alleviate stress and depression and has beneficial effects on the well-being of nurses (21, 41–43). Yang et al., also confirmed that MBI may be effective in reducing the symptoms of anxiety, depression, and stress. In addition, the training effectively reduces burnout (29, 40).
Evidence claimed by Lee and Chiyoung (44) supported reducing emotional exhaustion and depersonalization but did not support low personal accomplishment. Furthermore, MBI also effectively reduced the oncology nurses’ Compassion Fatigue. However, its effectiveness requires further research confirmation (45, 46). Art Therapy: One of the included reviews revealed significant reductions in anxiety, depression, and perceived stress levels among clinical nurses (47). Music-based interventions: Another review suggested that music interventions may decrease stress parameters even under critical stressful pressure (19). Interventions based on cognitive behavioral therapy (CBT) for PTSD, anxiety, and depression were found to lead to reliable changes in PTSD and anxiety symptoms (48). Some interventions were also found based on resilience programs, mobile applications, and nurse-led interventions that showed some effects on secondary traumatic stress, burnout, and compassion satisfaction (45). Figures 2–5 describe individual interventions by region.
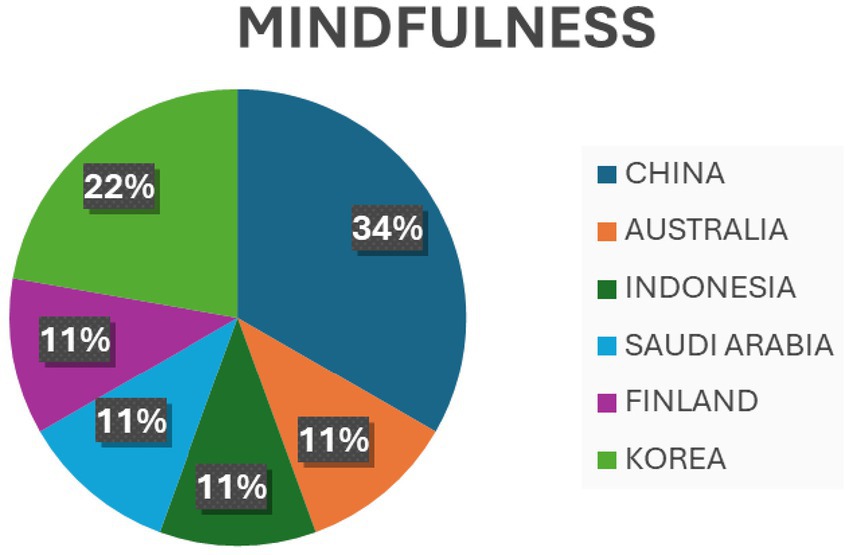
Figure 2. Percentage of individual mindfulness interventions by region.
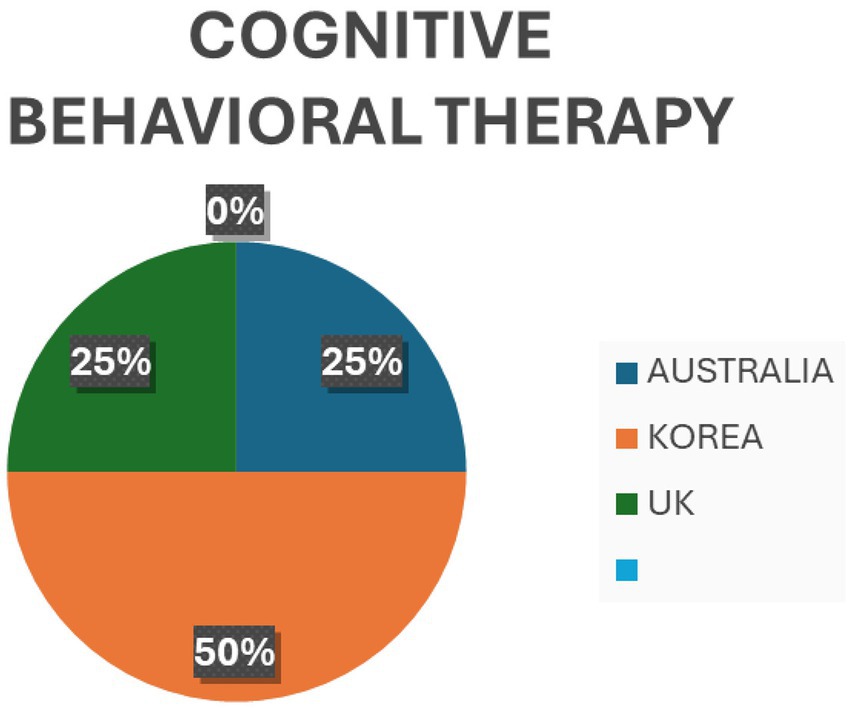
Figure 3. Percentage of cognitive behavioral therapy at individual level by region.
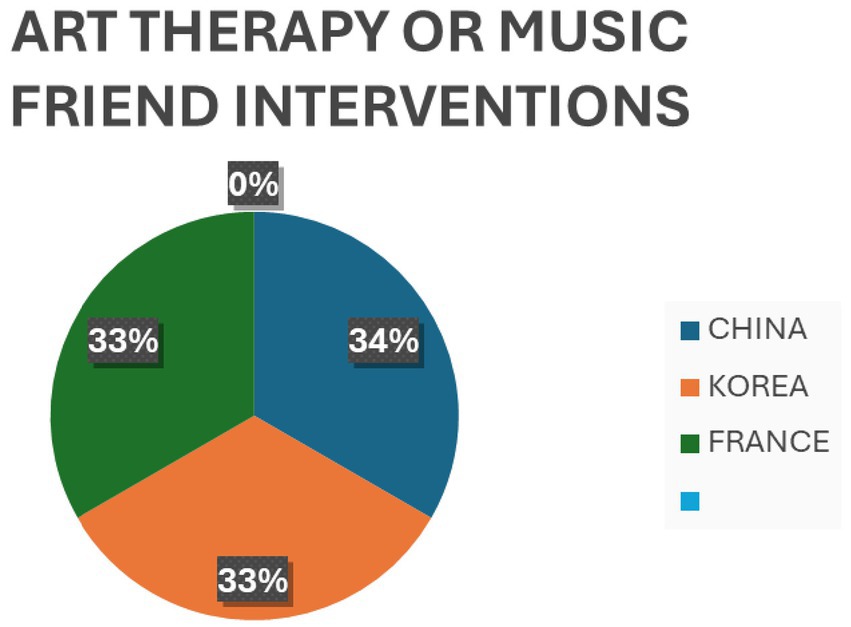
Figure 4. Percentage of art therapy/music intervention at individual level by region.
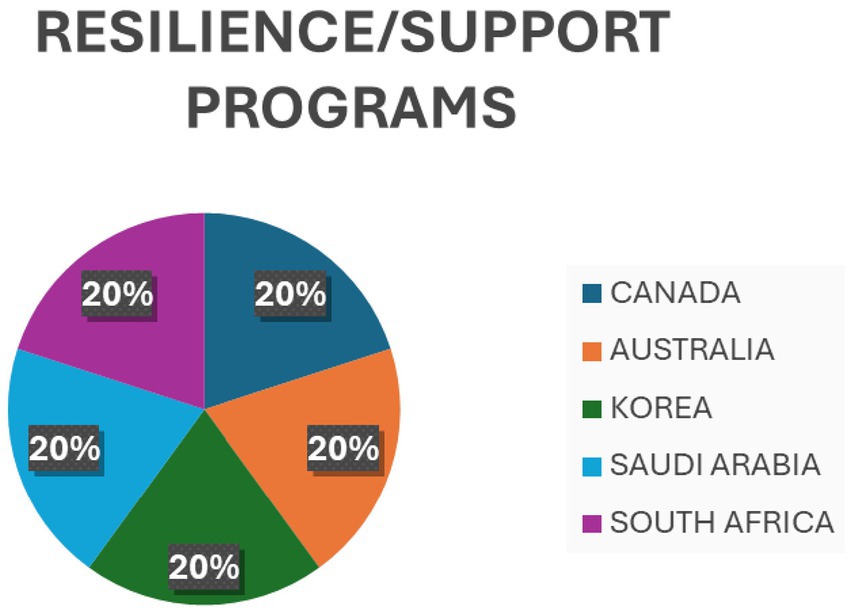
Figure 5. Percentage of resilience/support programs at individual level by region.
3.5.2.2 Organizational-level interventions
The review identified a glaring lack of organizational-level intervention in coping with emotional distress and improving work-related outcomes. However, only one of the reviews concluded that increasing salaries, nurse remuneration or benefits, improving professional skills, empowerment, strengthening mutual support among peers, and engaging in team-building activities can help reduce work alienation, considering these factors as a protective factor (49).
3.5.3 Policy-level interventions
No specific policy interventions were found, but some authors pointed out some recommendations based on their findings. Recommendations included highlighting the need for gender-sensitive policies and programs when addressing the diverse effects of the pandemic on different employment outcomes, such as recent precedents on healthcare pressure and the impact on the mental health and well-being of health and care workforce, they also show that further studies are required to establish successful methods to promote gender equality in the labour market and to point out the underlying causes of the gender differences detected through the analysis (50).
4 Discussion
The Our Duty of Care report highlights the significant mental health challenges confronting the health and care workforce, exacerbated by the COVID-19 pandemic (15, 51). Contributing factors include excessive workloads, inadequate pay, high patient- to-nurse ratios, early burnout, and increasing intention to leave the profession. Additionally, societal shifts such as ageing populations and the rise of chronic illnesses have amplified the demand for nurses, particularly in community and long-term care settings (52–54).
Our review highlighted the need for systemic changes to safeguard HCWs’ mental health and well-being in the post-COVID-19 era. Despite extensive evidence of the mental health burden and effective interventions, there is a notable lack of systemic implementation and organizational accountability. A significant shift is necessary to address ongoing issues like anxiety, depression, burnout, stress, and PTSD among HCWs (22, 36, 50, 55–58). However, depression prevalence data must be cautiously interpreted due to inconsistencies in definitions and measurement methods (23).
Galanis et al. (33) recently found that high levels of compassion satisfaction among nurses reduced workplace bullying’s negative effects, lowering the risk of compassion fatigue, burnout, stress, and depression. This finding should inform future organizational and individual interventions aimed at improving HCWs’ mental health and well-being.
4.1 Shifting the burden: from individual resilience to organizational resilient culture
The COVID-19 pandemic exposed the limitations of focusing solely on individual resilience, highlighting the need to integrate resilience into organizational culture. The Our Duty of Care report (15) highlighted the failure to adequately support HCWs, emphasizing the importance of sustainable interventions. Placing the burden of resilience solely on individuals can harm their mental health, especially when systemic factors are ignored. Evidence suggests that healthcare organizations must provide supportive environments during crises, which enhances both healthcare systems and patient care (33, 39, 59). Therefore, a fundamental shift in organizational culture is needed to foster a resilient healthcare system.
Resilience operates across multiple levels: individual, organizational, and systemic. In times of crisis, resilience should be initiated at the organizational level, as healthcare organizations play a pivotal role in supporting health and care workforce (60, 61). By integrating structural, non-structural, and functional elements of resilience, organizations can effectively support HCWs during disruptions, alleviating individual stress and enhancing crisis management at the system-wide level.
The focus on resilience has evolved beyond individuals to exploring how organizations can foster resilience within their systems. Recent efforts aim to understand the human elements of resilient systems, including how resilience affects health and care workers, patients, and families. This shift emphasizes informal networks, communication, and the importance of engaging people in maintaining system safety. Additionally, there is a need for further research on everyday clinical work and developing robust research methods, such as simulations, to study resilience in healthcare systems (62).
A resilient healthcare system is characterized by robust leadership, adequate resources, and effective organization. Resilience requires a motivated workforce, strong partnerships, and reliable information systems, alongside financial reserves. Effective leadership is essential to mobilize resources, adapt service delivery, and manage crises. Policymakers must regularly assess their healthcare systems to identify vulnerabilities and prepare for potential risks. Targeting weak areas enhances both resilience and overall system performance (63).
Lessons learned from recent shocks offer valuable insights into building resilient healthcare systems. While effective crisis responses are essential, a comprehensive understanding of resilience necessitates an examination of its broader dimensions, particularly the integration of healthcare systems with external frameworks, such as ecological and socio-political structures. Well-integrated systems demonstrate greater resilience in withstanding shocks. Furthermore, crises often exacerbate existing inequalities, intensifying disparities in health outcomes and access to care. Addressing these inequities is a critical component of resilience-building policies (64).
The transition from merely conceptualizing resilience to actively operationalizing it within healthcare systems is imperative. Strengthening resilience requires the creation of enabling environments through the development of policies, operational frameworks, and evaluation mechanisms. Additionally, integrating health and care workers into governance structures and enhancing their capacities are vital steps in constructing a more resilient healthcare system (65).
4.2 Organizational interventions: a critical need
After analyzing the 50 included articles, no organizational-level interventions aimed at addressing emotional distress and improving work-related outcomes were observed. Review findings also highlighted the lack of training for managers in specific mental health conditions of HCWs. The findings emphasize a considerable need for equipping leaders with skills to help create a supportive environment for the health and care workforce and address the mental health crisis in the workplace. Findings also indicate that organizations with supportive environments facilitate more effective crisis management, enhance work satisfaction, and highlight the significance of fostering resilience in organizations (39, 59). This further emphasizes the importance of providing leaders with the necessary resources to establish such a setting and proactively tackle mental health issues.
Although Cognitive Behavioral Therapy (CBT) and mindfulness interventions have been shown to be effective at the individual level, their integration into organizational-level interventions remains limited (29, 41–43, 48, 66). There is a need for healthcare systems to adopt evidence-based organizational interventions that promote psychological well-being and job satisfaction on a broader scale (38, 39, 59, 67, 68).
Therefore, considering all possible scenarios and stakeholders designing complex interventions attempts to go beyond asking whether an intervention works in terms of achieving the intended outcome, and address a broader range of questions (e.g., identifying the impact on HCW, patient outcomes, economic impact on the organization and the healthcare system). Furthermore, designing complex interventions for system change could use the evidence generated to support real-world decision-making. A complex intervention is one that is designed taking into account other components than the intervention itself, allowing its implementation to vary in different contexts, while maintaining the integrity of the core components of the intervention taking into account the context, key uncertainties, stakeholders, economic considerations and continuous improvement of the intervention based on the aforementioned components, with the aim of refining and adapting it to the context and need (69).
4.3 Assessment tools: a gap in systemic evaluation
Although the mental health burden among HCW has been acknowledged (20, 57, 58), there is a noticeable lack of comprehensive assessment tools designed to evaluate and improve organizational interventions. Existing tools primarily assess individual mental health factors without offering a comprehensive framework for identifying and addressing issues at an early stage. Findings signify the need for developing comprehensive guidelines for assessing organizational and individual interventions (38, 68, 70–74), both universal and specific, to evaluate the implementation and effectiveness of interventions in healthcare organizations to enhance HCWs’ mental health and well-being.
4.4 Strengths and limitations of this rapid review
Although we performed a rigorous rapid review following PRISMA guidelines, our study had some limitations. First, we opted to use English as the language of inclusion to limit the number of articles we could gather, excluding other languages such as Spanish. Second, time constraints necessitated conducting the data analysis within a period of less than 2 months. Although most systematic reviews employed tools to assess the quality of the articles, we did not assess the thoroughness of these evaluations. All included articles were systematic reviews, with the majority having already evaluated the methodological quality of the studies within each review. No additional specific risk of bias assessment was performed on the included studies; however, we ensured that all studies had previously undergone a risk of bias evaluation.
Third, most of the reviewed studies focused on the mental health of nurses and physicians. This emphasis should be considered when applying the findings to other healthcare and care workers. Although this rapid review included studies on other healthcare professionals, such as dentists, psychologists, and physiotherapists, these groups were underrepresented or, in some cases, not studied at all. Fourth, this rapid review excluded qualitative studies, as quantitative research typically involves larger sample sizes and employs standardized measures, making its findings more generalizable. Nonetheless, qualitative research remains essential for capturing the complexities of mental health and well-being, offering valuable insights into the personal, emotional, and cultural factors that may not be adequately addressed through quantitative methods. While quantitative approaches are often prioritized when seeking large-scale, standardized evidence, both methodologies are complementary and contribute to a more comprehensive understanding of the topic. Future reviews would benefit from a mixed-methods approach, incorporating both qualitative and quantitative studies to provide a more comprehensive understanding of the topic.
5 Conclusion
5.1 Towards health system resilience
The findings of this review indicate that, although there has been no significant change in the prevalence of depression and anxiety among health and care workers since 2022, these workers continue to exhibit levels of anxiety and depression. These levels are clearly representative in specific groups of workers and units. This suggests that these mental health issues and burnout are not exclusive to pandemic situations but may be associated with work-related factors, as well as personal and family factors of each worker. Therefore, the findings of this review underscore the significant mental health challenges faced by health and care workers, which are exacerbated by systemic issues such as inadequate working conditions, staff shortages, and evolving societal demands.
Based on the analysis of the interventions offered to health and care workers (HCWs), it was observed that individual interventions are the most commonly provided. These interventions have shown some effectiveness in reducing stress, improving well-being, and developing coping strategies. Among the most notable individual interventions are mindfulness and cognitive-behavioral therapy. However, it is crucial to address the underlying causes of burnout, stress, and anxiety, as this requires broader structural changes within healthcare organizations.
It is evident that relying solely on individual resilience is insufficient and unsustainable. Instead, resilience must be embedded within healthcare systems, with organizations assuming a central role in fostering supportive environments. This necessitates the integration of structural, non-structural, and functional elements of resilience into organizational frameworks. By adopting these strategies, healthcare organizations can not only enhance support for their health and care workforce but also improve overall patient care and system performance, particularly in times of crisis.
The broader implications of these findings highlight the significant, far-reaching consequences of poor mental health among HCWs. Beyond the direct impact on individuals, these challenges affect patient outcomes, healthcare quality, and the efficiency of healthcare systems. To mitigate these issues effectively, a shift towards evidence-based, systemic interventions is required, moving beyond the limited scope of individual-level solutions.
Finally, the findings highlighted the lack of specific policies, with some authors recommending the establishment of policies and programs that consider all stakeholders. Therefore, it is imperative to develop comprehensive guidelines for healthcare organizations to safeguard the mental health and well-being of health and care workers. These guidelines should be aligned with international standards, such as those set by the WHO, and should emphasize systemic accountability, organizational interventions, and continuous evaluation of their effectiveness. Implementing these guidelines is essential to foster a supportive and healthy work environment, more resilient healthcare systems, enhanced workforce retention, and improved patient care outcomes. Safeguarding the mental health of health and care workers is not only an ethical responsibility but also a critical foundation for building resilient and sustainable healthcare systems.
6 Recommendations
Evidence indicates the necessity of proposing and incorporating policies to integrate mental health support into workplace practices. Consequently, organizational strategies that foster resilience, such as adjusting workloads and enhancing peer support, are emphasized.
Incorporation of mental health support in workplace policies
• Develop employee-sensitive mental health policies specific to the needs of health and care workers (HCWs).
• Institutionalise accessible psychological support services at all organisational levels, such as well-being centres and counselling programs.
• Implement Employee Assistance Programs (EAPs) to promote early identification and intervention for mental health concerns among HCWs.
• Implement programs that build awareness and develop psychological safety among health and care workers through ruptured programs.
Resilience-based organisational practices
• Modify workload demands and task distributions to sustainable levels to prevent burnout.
• Strengthen peer support systems by creating opportunities for HCWs to share experiences and coping strategies.
• Adopt multi-component interventions, such as training on personal protective equipment use, emotional first aid desks, and structured resilience-building programs.
Leadership and managerial support
• Train leaders and managers to identify and respond to mental health challenges among their staff effectively.
• Integrate mental health into organisational crisis management frameworks with an emphasis on the role of leaders in supporting HCWs during disruptions.
• Allocate resources for mental health support and resilience enhancement within healthcare settings.
• Establish frameworks for periodic evaluations of healthcare facilities to detect vulnerability areas and engage in preventive practices.
To policymakers
• Design policies that introduce mental health support in organisational settings. This aims to bring about systemic/organisational responsibility.
• Invest in comprehensive interventions targeting HCW mental health, including resilience-building initiatives and welfare programs.
For healthcare organizations
• Invest in managerial training to create supportive work environments that enable early identification of signs of mental distress among staff.
• Focus organisational interventions on reducing burnout through workload adjustments and improvement in peer support systems.
• Regularly review the effectiveness of implemented interventions with validated assessment tools and make improvements accordingly.
For researchers
• Conduct longitudinal studies to determine the sustained effects of organisational and individual-level interventions on HCW mental health.
• Develop and validate assessment tools tailored to organisational resilience and mental health interventions.
• Examine the interaction between sociodemographic factors and intervention outcomes to inform context-specific strategies.
• These recommendations are intended to fill systemic gaps pointed out in the manuscript to create a resilient and supportive healthcare environment that prioritises the well-being of its workforce.
Author contributions
CF: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. NS: Investigation, Methodology, Writing – original draft, Writing – review & editing, Conceptualization, Data curation, Formal analysis. CC: Conceptualization, Data curation, Formal analysis, Investigation, Writing – original draft, Writing – review & editing. JK: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Writing – original draft, Writing – review & editing. AJ: Formal analysis, Investigation, Methodology, Software, Writing – original draft, Writing – review & editing. HA: Supervision, Writing – original draft. HR: Conceptualization, Supervision, Validation, Visualization, Writing – review & editing. AZ: Supervision, Validation, Visualization, Writing – review & editing. IT: Supervision, Visualization, Writing – review & editing, Writing – original draft. SA-H: Supervision, Funding acquisition, Validation, Visualization, Writing – review & editing. MS: Supervision, Writing – original draft. MF-N: Conceptualization, Funding acquisition, Project administration, Supervision, Validation, Writing – review & editing, Formal analysis, Methodology. JC: Supervision, Visualization, Writing – review & editing, Conceptualization, Funding acquisition, Project administration, Resources, Validation.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Acknowledgments
We would like to express our gratitude to Ms. Fatima Haider, Chief of Business Services. We would also like to extend our gratitude to the Director of Nursing, the General Director, and the Director of the Human Resources Department at Hospital Clínic de Barcelona for their unwavering support in maintaining the mental health and well-being of the health and care workforce. We also acknowledge thoughtful contributions, reviews and input from Dr. Mathieu Boniol, Dr. Georgio Cometto, Dr. Michelle McIsaac, and Dr. Pascal Zurn.
Conflict of interest
NS, JK, IT, and MS were employed by Hamad Medical Corporation.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2025.1530287/full#supplementary-material
References
1. World Health Organization. WHO health workforce support and safeguards list 2023 [internet]. Geneva: World Health Organization (2023).
2. de Vries, N, Boone, A, Godderis, L, Bouman, J, Szemik, S, Matranga, D, et al. The race to retain healthcare workers: a systematic review on factors that impact retention of nurses and physicians in hospitals. Inquiry. (2023) 60:00469580231159318. doi: 10.1177/00469580231159318
3. Li, Q, Liu, W, Wang, JY, Wang, XG, Hao, B, Hu, YB, et al. Prevalence and risk factors of post-traumatic stress disorder symptoms among Chinese health care workers following the COVID-19 pandemic. Heliyon. (2023) 9:e14415. doi: 10.1016/j.heliyon.2023.e14415
4. World Health Organization. International Labour Organization. Caring for those who care: guide for the development and implementation of occupational health and safety programmes for health workers [Internet]. Geneva: World Health Organization (2022).
5. United Nations. Refworld. Annual report of the United Nations High Commissioner for Human Rights (A/HRC/34/3); (2017). Available online at: https://www.refworld.org/reference/annualreport/unhrc/2017/en/115587 (accessed October 12, 2024)
6. World Health Organization. Health topics. Key terms and definitions in mental health; (2008). Available online at: https://www.who.int/southeastasia/health-topics/mental-health/key-terms-and-definitions-in-mental-health (accessed October 12, 2024)
7. World Health Organization. Health promotion glossary of terms 2021 [internet]. Geneva: World Health Organization (2021).
8. Gray, M, Downer, T, Hartz, D, Andersen, P, Hanson, J, and Gao, Y. The impact of three-dimensional visualisation on midwifery student learning, compared with traditional education for teaching the third stage of labour: a pilot randomised controlled trial. Nurse Educ Today. (2022) 108:105184. doi: 10.1016/j.nedt.2021.105184
9. Jang, Y, You, M, Lee, H, Lee, M, Lee, Y, Han, JO, et al. Burnout and peritraumatic distress of healthcare workers in the COVID-19 pandemic. BMC Public Health. (2021) 21:2075. doi: 10.1186/s12889-021-11978-0
10. Salyers, MP, Bonfils, KA, Luther, L, Firmin, RL, White, DA, Adams, EL, et al. The relationship between professional burnout and quality and safety in healthcare: a meta-analysis. J Gen Intern Med. (2017) 32:475–82. doi: 10.1007/s11606-016-3886-9
11. Sermeus, W, Aiken, LH, Ball, J, Bridges, J, Bruyneel, L, Busse, R, et al. A workplace organisational intervention to improve hospital nurses’ and physicians’ mental health: study protocol for the Magnet4Europe wait list cluster randomised controlled trial. BMJ Open. (2022) 12:e059159. doi: 10.1136/bmjopen-2021-059159
12. van de Pas, R, Kolie, D, Delamou, A, and Van Damme, W. Health workforce development and retention in Guinea: a policy analysis post-Ebola. Hum Resour Health. (2019) 17:63. doi: 10.1186/s12960-019-0400-6
13. International Labour Organization. Workplace stress: A collective challenge [internet]. Geneva: ILO (2016).
14. Chen, Q, Liang, M, Li, Y, Guo, J, Fei, D, Wang, L, et al. Mental health care for medical staff in China during the COVID-19 outbreak. Lancet Psychiatry. (2020) 7:e15–6. doi: 10.1016/S2215-0366(20)30078-X
15. Abdul Rahim, H, Fendt-Newlin, M, Al-Harahsheh, ST, and Campbell, J. Our duty of care: A global call to action to protect the mental health of health and care workers [Internet]; (2022) Available online at: https://www.who.int/publications/m/item/wish_report (accessed August 26, 2024)
16. World Health Organization. Resolution WHA74.14: Protecting, safeguarding and investing in the health and care workforce; (2021). Available online at: https://apps.who.int/gb/e/e_WHA74.html (accessed July 26, 2024)
17. World Health Organization. Resolution WHA75.17: Human resources for health; (2022). Available online at: https://apps.who.int/gb/e/e_wha75.html (Accessed April 19, 2024).
18. Moher, D, Liberati, A, Tetzlaff, J, and Altman, DGthe PRISMA Group. Reprint—preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Phys Ther. (2009) 89:873–80. doi: 10.1093/ptj/89.9.873
19. Colin, C, Prince, V, Bensoussan, JL, and Picot, MC. Music therapy for health workers to reduce stress, mental workload and anxiety: a systematic review. J Public Health (Oxf). (2023) 45:e532–41. doi: 10.1093/pubmed/fdad059
20. Huang, J, Huang, ZT, Sun, XC, Chen, TT, and Wu, XT. Mental health status and related factors influencing healthcare workers during the COVID-19 pandemic: a systematic review and meta-analysis. PLoS One. (2024) 19:e0289454. doi: 10.1371/journal.pone.0289454
21. Musker, M, and Othman, S. Effective interventions to reduce burnout in nurses: a meta-analysis. Complement Ther Clin Pract. (2024) 54:101827. doi: 10.1016/j.ctcp.2023.101827
22. Alberque, B, Laporte, C, Mondillon, L, Baker, JS, Mermillod, M, Brousse, G, et al. Prevalence of post-traumatic stress disorder (PTSD) in healthcare workers following the first SARS-CoV epidemic of 2003: a systematic review and Meta-analysis. Int J Environ Res Public Health. (2022) 19:13069. doi: 10.3390/ijerph192013069
23. Saade, S, Parent-Lamarche, A, Bazarbachi, Z, Ezzeddine, R, and Ariss, R. Depressive symptoms in helping professions: a systematic review of prevalence rates and work-related risk factors. Int Arch Occup Environ Health. (2022) 95:67–116. doi: 10.1007/s00420-021-01783-y
24. Long, H, Li, Q, Zhong, X, Yang, L, Liu, Y, Pu, J, et al. The prevalence of professional burnout among dentists: a systematic review and meta-analysis. Psychol Health Med. (2023) 28:1767–82. doi: 10.1080/13548506.2023.2208364
25. Da S, MJ, Soares, JP, Massignan, C, Oliveira, LB, Ribeiro, DM, Cardoso, M, et al. Burnout syndrome among dentists: a systematic review and meta-analysis. J Evid Based Dent Pract. (2022) 22:101724. doi: 10.1016/j.jebdp.2022.101724
26. Xiong, N, Fritzsche, K, Pan, Y, Löhlein, J, and Leonhart, R. The psychological impact of COVID-19 on Chinese healthcare workers: a systematic review and meta-analysis. Soc Psychiatry Psychiatr Epidemiol. (2022) 57:1515–29. doi: 10.1007/s00127-022-02264-4
27. Chen, B, Yang, T, Tao, L, Song, Y, Liu, Y, Wang, Y, et al. Effects of mobile-based mindfulness meditation for mental health of nurses: a protocol for systematic review and meta-analysis. BMJ Open. (2022) 12:e058686. doi: 10.1136/bmjopen-2021-058686
28. Thielmann, B, Schnell, J, Böckelmann, I, and Schumann, H. Analysis of work related factors, behavior, well-being outcome, and job satisfaction of workers of emergency medical service: a systematic review. Int J Environ Res Public Health [Internet] (2022);19. Available online at: http://www.epistemonikos.org/documents/1bd85ce8922abd2b853e9003e6c 29f9c82464be2
29. Yang, JM, Ye, H, Long, Y, Zhu, Q, Huang, H, Zhong, YB, et al. Effects of web-based mindfulness-based interventions on anxiety, depression, and stress among frontline health care workers during the COVID-19 pandemic: systematic review and meta-analysis. J Med Internet Res. (2023) 25:e44000. doi: 10.2196/44000
30. Harris, LK, Skou, ST, Juhl, CB, Jäger, M, and Bricca, A. Recruitment and retention rates in randomised controlled trials of exercise therapy in people with multimorbidity: a systematic review and meta-analysis. Trials. (2021) 22:396. doi: 10.1186/s13063-021-05346-x
31. Papazian, L, Hraiech, S, Loundou, A, Herridge, MS, and Boyer, L. High-level burnout in physicians and nurses working in adult ICUs: a systematic review and meta-analysis. Intensive Care Med. (2023) 49:387–400. doi: 10.1007/s00134-023-07025-8
32. Sauder, M, Zagales, I, Zagales, R, Das, S, Sen-Crowe, B, Bilski, T, et al. Comprehensive assessment of burnout among surgical trainees and practicing surgeons: a systematic review. J Surg Educ. (2022) 79:1188–205. doi: 10.1016/j.jsurg.2022.04.009
33. Galanis, P, Moisoglou, I, Katsiroumpa, A, and Mastrogianni, M. Association between workplace bullying, job stress, and professional quality of life in nurses: a systematic review and meta-analysis. Healthcare (Basel). (2024) 12:623. doi: 10.3390/healthcare12060623
34. Xia, M, Wang, J, Bi, D, He, C, Mao, H, Liu, X, et al. Predictors of job burnout among Chinese nurses: a systematic review based on big data analysis. Biotechnol Genet Eng Rev. (2023) 39:1163–86. doi: 10.1080/02648725.2023.2168910
35. de Vargas, D, Volpato, RJ, Dos Santos, LC, Pereira, CF, de Oliveira, SR, da Silva, RR, et al. Prevalence of psychological and mental health symptoms among nursing professionals during the COVID-19 pandemic in the Americas: systematic review and meta-analysis. Int J Ment Health Nursing [Internet] (2023); Available online at: http://www.epistemonikos.org/documents/0fed66cf33166d499a947b4ef4a89 56f9ba36a76
36. Egbe, A, and El Boghdady, M. Anxiety and depression in surgeons: a systematic review. Surgeon. (2024) 22:6–17. doi: 10.1016/j.surge.2023.09.009
37. World Health Organization. WHO guidelines on mental health at work [internet]. Geneva: World Health Organization (2022).
38. Nicolakakis, N, Lafantaisie, M, Letellier, MC, Biron, C, Vézina, M, Jauvin, N, et al. Are organizational interventions effective in protecting healthcare worker mental health during epidemics/pandemics? A systematic literature review. Int J Environ Res Public Health. (2022) 19:9653. doi: 10.3390/ijerph19159653
39. Bekelepi, N, and Martin, P. Support interventions for nurses working in acute psychiatric units: A systematic review. Health SA. (2022) 27:1811. doi: 10.4102/hsag.v27i0.1811
40. Wang, J, Liu, M, Bai, J, Chen, Y, Xia, J, Liang, B, et al. Prevalence of common mental disorders among medical students in China: a systematic review and meta-analysis. Front Public Health. (2023) 11:1116616. doi: 10.3389/fpubh.2023.1116616
41. Kang, MJ, and Myung, SK. Effects of mindfulness-based interventions on mental health in nurses: a meta-analysis of randomized controlled trials. Issues Ment Health Nurs. (2022) 43:51–9. doi: 10.1080/01612840.2021.1949765
42. Karo, M, Simorangkir, L, Daryanti Saragih, I, Suarilah, I, and Tzeng, HM. Effects of mindfulness-based interventions on reducing psychological distress among nurses: a systematic review and meta-analysis of randomized controlled trials. J Nurs Scholarsh. (2023); Available online at: http://www.epistemonikos.org/documents/48c89585a331e1a0af8863acd38e 47ad8213b302
43. Sulosaari, V, Unal, E, and Cinar, FI. The effectiveness of mindfulness-based interventions on the psychological well-being of nurses: a systematic review. Appl Nurs Res. (2022) 64:151565. doi: 10.1016/j.apnr.2022.151565
44. Lee, M, and Chiyoung, C. Interventions to reduce burnout among clinical nurses: systematic review and meta-analysis. Sci Rep. (2023) 13:10971. doi: 10.1038/s41598-023-38169-8
45. Algamdi, M. Prevalence of oncology nurses’ compassion satisfaction and compassion fatigue: systematic review and meta-analysis. Nurs Open. (2022) 9:44–56. doi: 10.1002/nop2.1070
46. Zhou, XQ, Han, YF, and Xu, MX. Effects of different intervention methods on psychological anxiety, stress, and fatigue among healthcare workers during COVID-19 pandemic: a systematic review and meta-analysis. Eur Rev Med Pharmacol Sci. (2024) 28:1614–23. doi: 10.26355/eurrev_202402_35491
47. Zhang, N, Chen, S, Li, Q, He, Z, and Jiang, W. Efficacy of art therapy in enhancing mental health of clinical nurses: a meta-analysis. J Psychiatr Ment Health Nurs. (2024) 31:729–41. doi: 10.1111/jpm.13026
48. Ottisova, L, Gillard, JA, Wood, M, Langford, S, John-Baptiste Bastien, R, Madinah Haris, A, et al. Effectiveness of psychosocial interventions in mitigating adverse mental health outcomes among disaster-exposed health care workers: a systematic review. J Trauma Stress. (2022) 35:746–58. doi: 10.1002/jts.22780
49. You, Q, Bai, D, Wu, C, Gao, J, and Hou, C. Status of work alienation among nurses in China: a systematic review. Front Psych. (2022) 13:986139. doi: 10.3389/fpsyt.2022.986139
50. Athe, R, Dwivedi, R, Singh, K, Babusab Hulmani, S, Karadi, N, Boraiah, C, et al. Impact of COVID-19 on the mental health of healthcare workers and job loss from a gender perspective in India: a systematic review and meta-analysis. Cureus. (2023) 15:e48219. doi: 10.7759/cureus.48219
51. Søvold, LE, Naslund, JA, Kousoulis, AA, Saxena, S, Qoronfleh, MW, Grobler, C, et al. Prioritizing the mental health and well-being of healthcare workers: an urgent global public health priority. Front Public Health [Internet]. (2021) 9:679397. doi: 10.3389/fpubh.2021.679397
52. Cabrera, E, and Zabalegui, A. Nurses workforce and competencies. A challenge for health systems more than ever. Nurse Educ Pract. (2020) 48:102858. doi: 10.1016/j.nepr.2020.102858
53. Laurant, M, van der Biezen, M, Wijers, N, Watananirun, K, Kontopantelis, E, and van Vught, AJ. Nurses as substitutes for doctors in primary care. Cochrane Database Syst Rev. (2018) 7:CD001271. doi: 10.1002/14651858.CD001271.pub3
54. Rafferty, AM, Busse, R, Zander-Jentsch, B, Sermeus, W, and Bruyneel, L eds. Strengthening health systems through nursing: Evidence from 14 European countries [internet]. Copenhagen (Denmark): European Observatory on Health Systems and Policies (2019).
55. Albazoon, F, Khogali, F, Burjaq, R, Chandra, P, Alabdulla, M, Abdulaziz, M, et al. Burnout among healthcare professionals in Qatar: a systematic review. Asian J Psychiatr. (2023) 85:103601. doi: 10.1016/j.ajp.2023.103601
56. Aymerich, C, Pedruzo, B, Pérez, JL, Laborda, M, Herrero, J, Blanco, J, et al. COVID-19 pandemic effects on health workers’ mental health: systematic review and meta-analysis. Eur Psychiatry. (2022) 65:1–20. doi: 10.1192/j.eurpsy.2022.1
57. Meira-Silva, VST, Freire, ACTN, Zinezzi, DP, Ribeiro, FCR, Coutinho, GD, Lima, IMB, et al. Burnout syndrome in healthcare workers during the COVID-19 pandemic: a systematic review. Rev Bras Med Trab. (2022) 20:122–31. doi: 10.47626/1679-4435-2022-849
58. Shen, X, Xu, H, Feng, J, Ye, J, Lu, Z, and Gan, Y. The global prevalence of burnout among general practitioners: a systematic review and meta-analysis. Fam Pract. (2022) 39:943–50. doi: 10.1093/fampra/cmab180
59. Kunzler, AM, Chmitorz, A, Röthke, N, Staginnus, M, Schäfer, SK, Stoffers-Winterling, J, et al. Interventions to foster resilience in nursing staff: a systematic review and meta-analyses of pre-pandemic evidence. Int J Nurs Stud. (2022) 134:104312. doi: 10.1016/j.ijnurstu.2022.104312
60. Gröschke, D, Hofmann, E, Müller, ND, and Wolf, J. Individual and organizational resilience—insights from healthcare providers in Germany during the COVID-19 pandemic. Front Psychol [Internet]. (2022) 13:965380. doi: 10.3389/fpsyg.2022.965380
61. Tan, JYA, Ong, GYQ, Cheng, LJ, Pikkarainen, M, and He, HG. Effectiveness of mHealth-based psychosocial interventions for breast cancer patients and their caregivers: a systematic review and meta-analysis. J Telemed Telecare. (2023) 31:184–97. doi: 10.1177/1357633X231187432
62. Ellis, LA, Churruca, K, Clay-Williams, R, Pomare, C, Austin, EE, Long, JC, et al. Patterns of resilience: a scoping review and bibliometric analysis of resilient health care. Saf Sci. (2019) 118:241–57. doi: 10.1016/j.ssci.2019.04.044
63. Thomas, S, Sagan, A, Larkin, J, Cylus, J, Figueras, J, and Karanikolos, M. Strengthening health systems resilience: Key concepts and strategies [Internet]. Copenhagen (Denmark): European Observatory on Health Systems and Policies (2020).
64. Hanefeld, J, Mayhew, S, Legido-Quigley, H, Martineau, F, Karanikolos, M, Blanchet, K, et al. Towards an understanding of resilience: responding to health systems shocks. Health Policy Plan. (2018) 33:355–67. doi: 10.1093/heapol/czx183
65. World Health Organization. Health systems resilience toolkit: A WHO global public health good to support building and strengthening of sustainable health systems resilience in countries with various contexts [internet] (2022). Available online at: https://www.who.int/publications/i/item/9789240048751 (accessed August 26, 2024)
66. Yoo, IG. The effects of the type of delivery of cognitive-behavioral therapy for healthcare workers: a systematic review. J Clin Psychol. (2022) 78:149–66. doi: 10.1002/jclp.23215
67. Ladino, MDM, Bolaños, C, Ramírez, VAC, Giraldo, EJS, Álzate, JP, Cubides, A, et al. Effects of internet-based, psychosocial, and early medical interventions on professional burnout in health care workers: {systematic} literature review and meta-analysis. Internet Interv. (2023) 34:100682. doi: 10.1016/j.invent.2023.100682
68. Townsley, AP, Li-Wang, J, and Katta, R. Healthcare workers’ well-being: a systematic review of positive psychology interventions. Cureus. (2023) 15:e34102. doi: 10.7759/cureus.34102
69. Skivington, K, Matthews, L, Simpson, SA, Craig, P, Baird, J, Blazeby, JM, et al. A new framework for developing and evaluating complex interventions: update of Medical Research Council guidance. BMJ. (2021) 374:n2061. doi: 10.1136/bmj.n2061
70. Hiver, C, Villa, A, Bellagamba, G, and Lehucher-Michel, MP. Burnout prevalence among European physicians: a systematic review and meta-analysis. Int Arch Occup Environ Health. (2022) 95:259–73. doi: 10.1007/s00420-021-01782-z
71. Crawshaw, J, Konnyu, K, Castillo, G, van Allen, Z, Grimshaw, JM, and Presseau, J. Behavioural determinants of COVID-19 vaccination acceptance among healthcare workers: a rapid review. Public Health. (2022) 210:123–33. doi: 10.1016/j.puhe.2022.06.003
72. Crocker, KM, Gnatt, I, Haywood, D, Butterfield, I, Bhat, R, Lalitha, ARN, et al. The impact of COVID-19 on the mental health workforce: a rapid review. Int J Ment Health Nurs. (2023) 32:420–45. doi: 10.1111/inm.13097
73. Dittborn, M, Micolich, C, Rojas, D, and Salas, SP. Ethical challenges experienced by healthcare workers delivering clinical care during health emergencies and disasters: a rapid review of qualitative studies and thematic synthesis. AJOB Empir Bioeth. (2022) 13:179–95. doi: 10.1080/23294515.2022.2063996
Keywords: public health workforce, rapid review, healthcare workers, mental health, burnout, depression, anxiety, health systems resilience
Citation: Frias CE, Samarasinghe N, Cuzco C, Koorankot J, de Juan A, Ali Rudwan HM, Rahim HFA, Zabalegui A, Tulley I, Al-Harahsheh ST, Al-Homaiddi MSST, Fendt-Newlin M and Campbell J (2025) Strategies to support the mental health and well-being of health and care workforce: a rapid review of reviews. Front. Med. 12:1530287. doi: 10.3389/fmed.2025.1530287
Edited by:
Kim Walker, University of Aberdeen, United KingdomReviewed by:
Kata Ivanišević, University of Rijeka, CroatiaSandra Nicholson, University of Worcester, United Kingdom
Copyright © 2025 Frias, Samarasinghe, Cuzco, Koorankot, de Juan, Ali Rudwan, Rahim, Zabalegui, Tulley, Al-Harahsheh, Al-Homaiddi, Fendt-Newlin and Campbell. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Cindy E. Frias, Y2ZyaWFzQGNsaW5pYy5jYXQ=
†ORCID: Cecilia Cuzco, orcid.org/0000-0003-2201-4879
Adela Zabalegui, orcid.org/0000-0003-1205-3997