 Shuhui Yang
Shuhui Yang Yongsheng Tang
Yongsheng Tang Zenan Yuan
Zenan Yuan- Department of Hepatic Surgery and Liver Transplantation Center, Third Affiliated Hospital of Sun Yat-sen University, Guangzhou, China
Introduction: Inflammatory myofibroblastic tumor (IMT) is a rare low-grade malignant neoplasm in the liver. Timely diagnosis and treatment of IMT are challenging due to its atypical symptoms and imaging results.
Case report: We report a 46-year-old woman who presented to our hospital with persistent hyperpyrexia and discomfort in the right upper abdomen for 2 months post bone marrow transplantation. Radiological findings revealed a space-occupying lesion of uncertain nature in the liver. Since the histological examination of the biopsy specimen indicated IMT, she underwent surgical resection. Subsequently, the postoperative pathology confirmed the diagnosis of IMT. The patient’s febrile condition subsided after the surgery. A magnetic resonance imaging (MRI) scan performed 8 months later showed no signs of recurrence.
Conclusion: IMTs are caused by genetic rearrangements. Diagnosing IMT can be challenging especially in this case as we had to differentiate the tumor from inflammatory diseases associated with bone marrow transplantation. Hence, a thorough pathological immunohistochemical examination is required to confirm its diagnosis. Local IMTs should be treated with radical surgical resection. In cases of distant metastasis or incomplete resection cases, chemotherapy, targeted therapy, or immunotherapy can be utilized. Regular follow-up is crucial for improving the patient’s survival rate.
Introduction
Inflammatory myofibroblastic tumor (IMT) is a rare neoplasm that originates from mesenchymal cells (1). It is mostly observed in the lungs, greater omentum, and mesentery. Although rare, it may also occur in other organs (2). Previously known as inflammatory pseudotumor (IPT) because of its histological features of spindle cell proliferation and inflammatory cell infiltration (3), IMT is now considered a neoplastic lesion rather than a simple inflammatory reaction (1, 4). The occurrence of this condition in the liver is quite rare. Its atypical symptoms and radiographic manifestations complicate the diagnosis and can lead to confusion with other liver tumors. Therefore, immunohistochemistry is essential for diagnosing IMT. In this report, we describe the clinical and imaging features, treatment methods, and prognosis of a patient at our medical center diagnosed with IMT following bone marrow transplantation. The patient’s prognosis improved after surgical resection. This case report offers reliable and practical guidance for diagnosing hepatic IMT and highlights the significance of surgical treatment in these cases.
Case presentation
A 46-year-old woman was admitted to our hospital with fever, mild discomfort in the right upper abdomen, and intermittent shoulder as well as lower extremity myalgia for last 2 months. She did not complain of pharyngalgia, cough, or diarrhea. An abdominal computed tomography (CT) scan performed 1 month back in a nearby hospital had revealed an abnormal density lesion in the S6/7 segments of the liver. Leukemia recurrence was suspected due to her hospitalization for acute myeloid leukemia (AML) and her bone marrow transplant 6 months earlier. Consequently, she underwent bone marrow and percutaneous liver biopsies. The results of these biopsies indicated complete remission of AML. The pathological findings of liver biopsy revealed inflammatory granulation tissues. Subsequently, an infectious etiology was suspected, and anti-infective therapy was initiated. Since her body temperature remained significantly elevated (up to 40°C), she was referred to our hospital. At admission, she weighed 42 kg, was 160 cm tall, and had a body mass index (BMI) of 16.4. She continued taking cyclosporine tablets daily. Additionally, she had hypoproteinemia, bilateral pulmonary scattered inflammatory infiltrates, and minor pericardial effusion. She had an unremarkable psychosocial and family history and denied any previous other chronic diseases.
Her physical examination demonstrated that her abdomen was flat and pliable with no palpable tenderness.
Her laboratory investigations revealed enhanced white blood cell count (17.75/mL), significant iron deficiency anemia with a hemoglobin level of 57 g/dL, a platelet count of 459/mL, and a procalcitonin level of 0.15 ng/mL. The prothrombin time was marginally extended to 15.8 s. Tests for hepatitis B virus DNA and 2019 Novel Coronavirus (19-nCoV) nucleic acid assay results were negative. Her biochemical laboratory parameters were normal, except for a significantly elevated serum ferritin level of 2,140 ng/mL (normal range: 10–291 ng/mL).
A CT scan identified a hypodense tumor, measuring 67 × 58 mm, with an indistinct margin, in the S6/7 segments of the liver. The arterial phase showed the tumor’s heterogeneous enhancement, while the portal venous and delayed phases revealed a reduced enhancement. The tumor had a visible capsule encircling a necrotic core that failed show enhancement (Figures 1A–C). Additionally, the MRI depicted the mass as hypo-intense on T1-weighted images and hyperintense on T2-weighted images. The arterial phase showed a heterogeneous enhancement, while the venous and delayed phases revealed progressive and slightly diminished enhancements (Figures 1D,E).
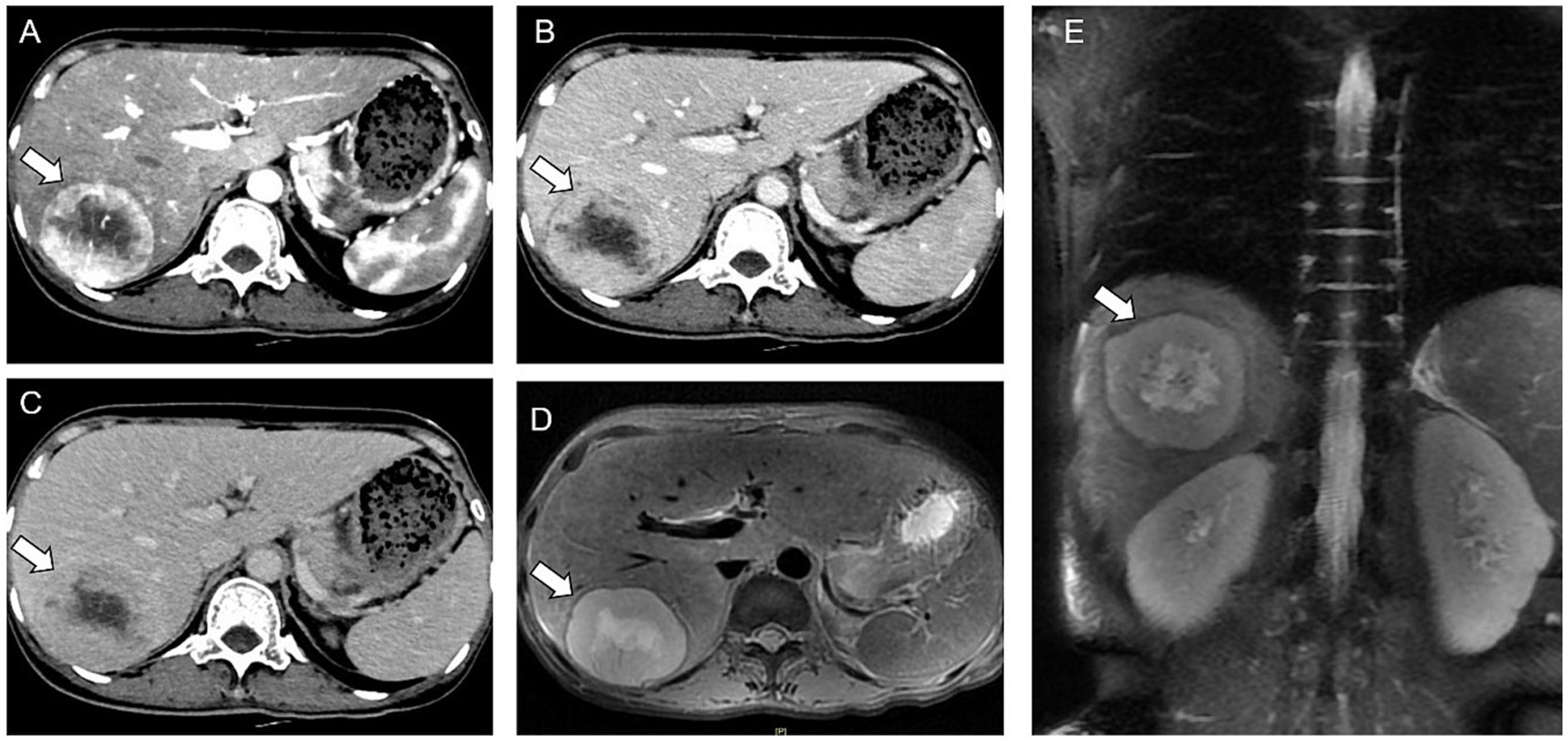
Figure 1. Computed tomography (CT) and magnetic resonance imaging (MRI) results. (A–C) Arterial, venous, and delayed phases of enhanced CT. (D,E) MRI shows a huge round mass.
Given the patient’s history of leukemia and lack of any previous episodes of hepatocellular carcinoma related to hepatitis or other etiological factors, the probability of leukemic hepatic infiltration was considered. A percutaneous liver tumor biopsy was performed. The pathological results of the tumor biopsy identified it as an inflammatory fibroblastic tumor. Subsequently, the patient underwent a laparoscopic anatomic resection of the right posterior hepatic lobe. Intraoperatively, the liver exhibited a soft parenchymal texture, and certain areas exhibited a bluish discoloration, particularly in the right posterior hepatic lobe. This was attributed to hepatic sinusoidal stasis post chemotherapy. The tumor measured approximately 2.6 × 5 × 5 cm and was firmly adherent to the diaphragm. Considering the tumor’s invasion of the diaphragm, an open surgerical approach was adopted. The tumor, along with a segment of the diaphragm, was excised en bloc; the diaphragm was then repaired by continuous suturing with a barbed wire, and an indwelling thoracic drainage catheter was placed. The surgery lasted for 5 h and 50 min, with a total blood loss of 500 mL. Postoperatively, an immunohistochemical staining assay identified the gross specimen as an IMT. The tumor surface exhibited a grayish-yellow hue with a distinct margin, and the cut surface was grayish-yellow intermingled with red (Figure 2). The histopathological evaluation revealed that the tumor comprised spindle cells arranged in a scattered or fascicular pattern. The heterogeneous cells with nucleoli and mitotic figures revealed focal necrosis. Numerous lymphocytes, plasma cells, and neutrophils were infiltrated within the stroma. Immunohistochemical staining results revealed positive outcomes for smooth muscle actin (SMA), anaplastic lymphoma kinase (ALK), S100, desmin, and myeloperoxidase (MPO). However, the Ki-67 index exhibited approximately 10% positivity (Figure 3). Additionally, hepatitis-associated antigen (HEP) and Epstein–Barr virus were not detected.

Figure 2. Macroscopic pathology of inflammatory myofibroblastic tumor (IMT) postoperatively.
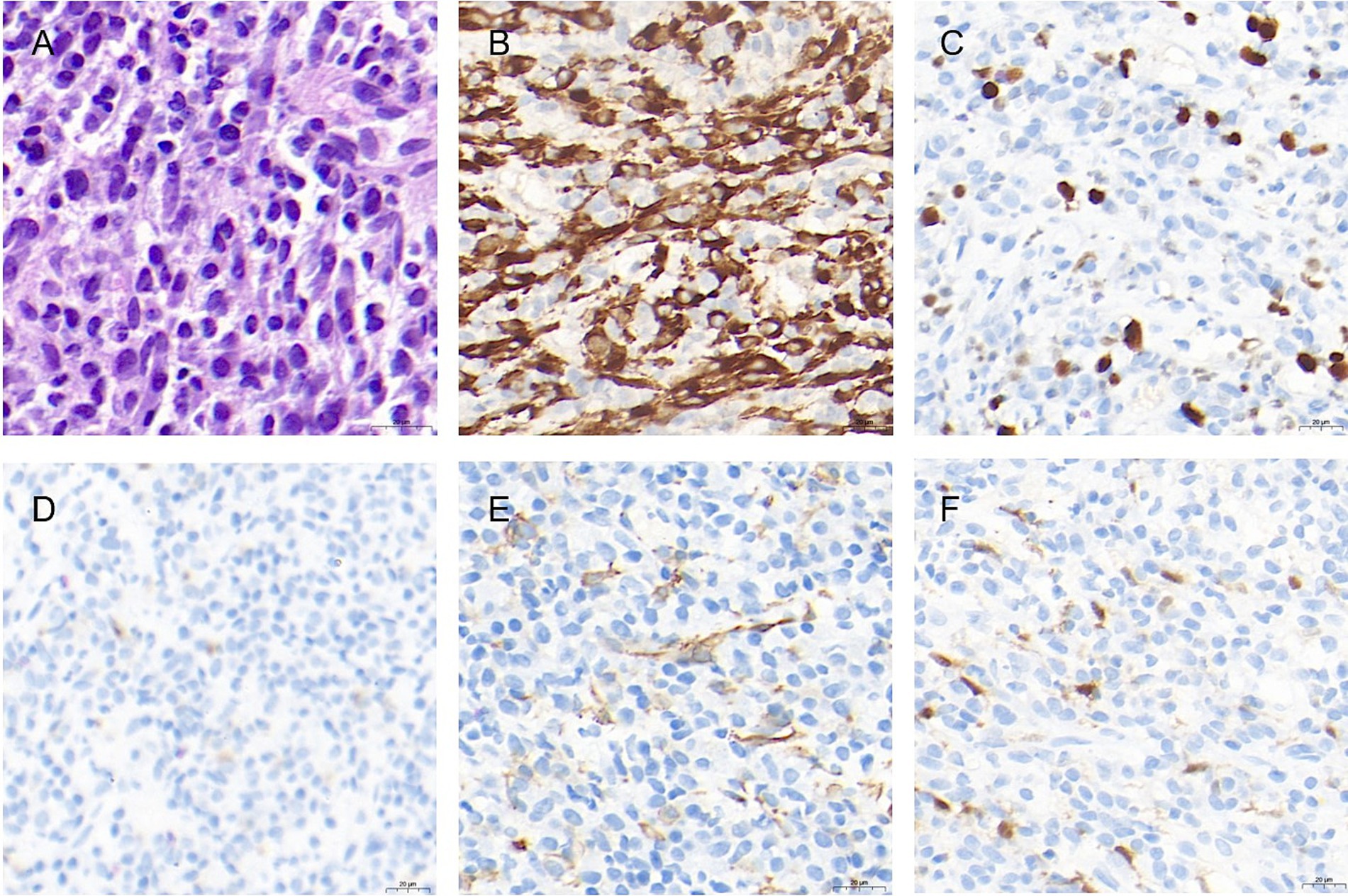
Figure 3. Staining of the tumor specimen. (A) Proliferation of spindle-shaped cells, with heterogeneity, enriched nucleoli, and mitotic figures. Multiple lymphocytes, plasma cells, and neutrophils were seen infiltrating the stroma (hematoxylin and eosin stain, ×70). (B) Immunopositivity for anaplastic lymphoma kinase (original magnification ×50). (C) Approximately 10–15% of Ki-67 immunopositivity (original magnification ×50); (D) Desmin immunopositivity (original magnification ×50). (E) Immunopositivity of smooth muscle actin (original magnification ×60). (F) S100 immunopositivity (original magnification×50).
The patient’s febrile episodes ceased postoperatively, and no additional postoperative complications were observed. She was discharged on the ninth postoperative day. The patient demonstrated good compliance and attended regular outpatient follow-up appointments without any adverse events (Table 1). A postoperative MRI scan after 8 months showed no evidence of recurrence (Figure 4).
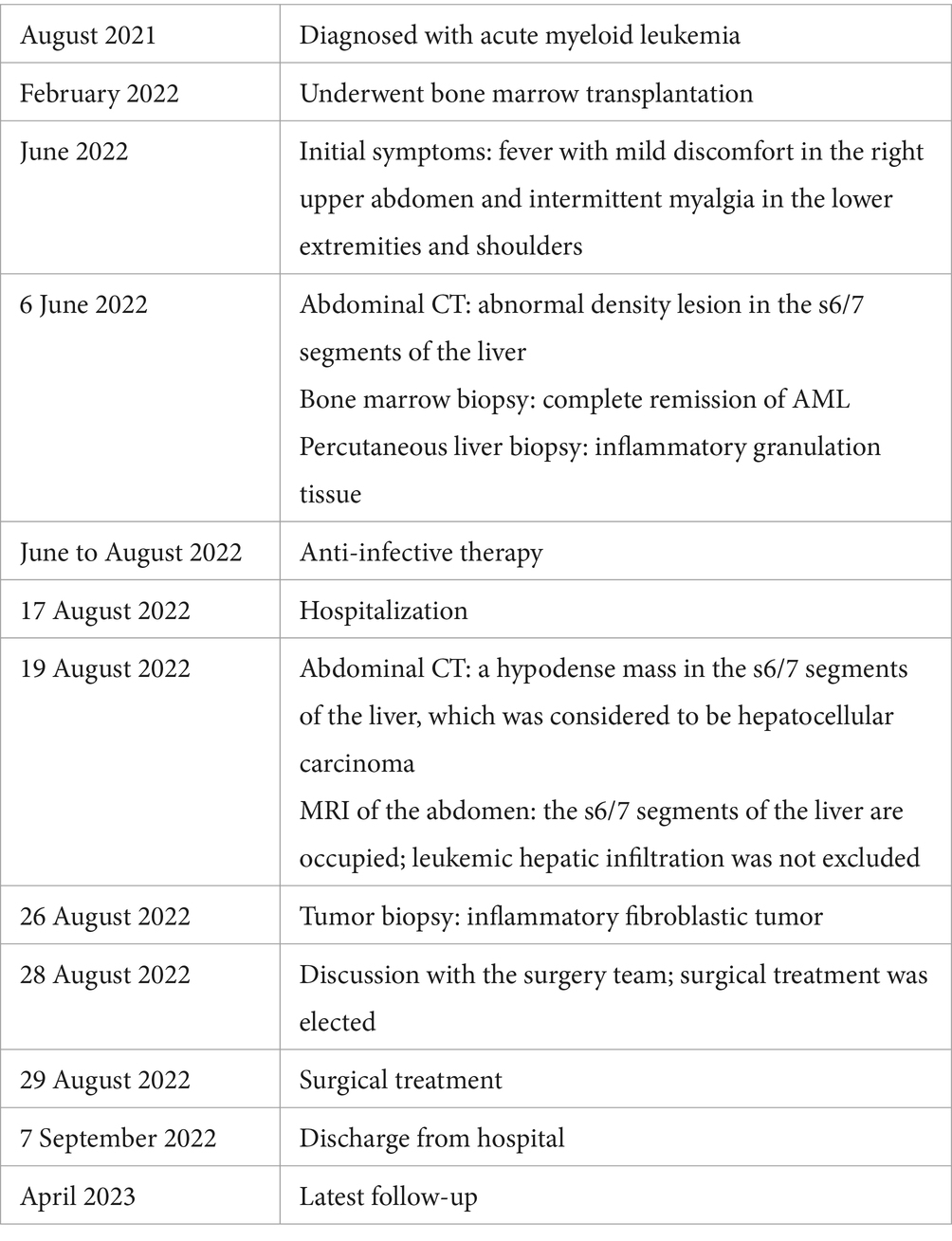
Table 1. Timeline.

Figure 4. A postoperative MRI scan 8 months later showed no evidence of IMT recurrence.
We inquired about the patient’s opinions regarding the treatment 8 months postoperatively. She expressed her satisfaction with the course of the treatment, noting that the treatment alleviated her high-grade fever, which had been severely impacting her daily activities and quality of life. She appreciated the speedy postoperative recovery and readily agreed to the publication of her case as she considered that it might benefit other IMT patients.
Discussion
IMT is a rare mesenchymal neoplasm that is currently classified as an intermediate-grade malignancy. Characterized by low-grade malignant features, it has a lower metastatic rate but a higher risk of recurrence (5). IMT is more common in children and young adults, with a higher prevalence in women than in men (6). The etiological underpinnings are unknown. A previous study has suggested its potential association with viral infections, immunosuppressive conditions, and traumatic injuries (7). However, this perspective might be attributed to a limited understanding of IMT in previous studies because they did not specifically elaborate the mechanism. Parker et al. (4) suggested that the laboratory analysis and the inflammation-associated manifestations are its outcomes rather than etiological factors. In light of recent developments, IMT can be now regarded as a neoplastic transformation; however, its local invasiveness also possesses the characteristics of a malignant tumor (6, 7). Gene rearrangements are the probable causes of tumorigenesis. Approximately 50% of IMT cases possess ALK gene rearrangement, which causes IMT to be ALK-positive (8). The ALK gene encodes tyrosine kinase receptor, which was initially discovered in mesenchymal large cell lymphoma and is usually expressed only in neural tissues (9). Therefore, ALK positivity can be used for distinguishing between IMT and inflammatory pseudotumors. Although many patterns and fusion proteins leading to ALK gene fusion have been identified, the staining pattern of ALK is linked to fusion proteins (6). However, the molecular configuration of ALK gene fusion partners in significant IMT cases comprises transcriptional activator elements and oligomerization motifs, which causes aberrant activation of ALK (7, 10–13). Currently, available cases have not been evaluated regarding the types of gene fusion and prognosis. However, another study has reported that ALK positivity might indicate a good prognosis (6), while patients with gene rearrangements involving both RAN binding protein 2 (RanBP2) and ALK exhibit a higher tumor recurrence rate and a relatively poor prognosis (14).
Histologically, IMT possesses different morphological features ranging from inflammatory pseudotumor to malignant sarcoma, associated with various gene rearrangements. Some cases have a typical morphology. The study by Antonescu et al. (6) reported that in ALK rearranged cases, tumors comprised mild spindle cells, with low mitotic activity, mild-to-moderate inflammation, and fibromyxoid stroma. However, the tumor cells exhibited round cell morphology in RanBP2 and ALK gene rearrangements cases (14–16). Immunohistochemistry can be useful for investigating the nature and origin of the tumor in IMT cases. In liver IMT cases, it is important to distinguish the IMT from the gastrointestinal stromal tumor (GIST) and liver metastasis. The presence of abundant myofibroblasts in IMT cases can help in confirming the diagnosis. However, CD117 positivity is observed in GISTs (17), which is different from IMTs. Several muscle cell markers such as vimentin, SMA, and desmin can be used to identify the tumor originating from mesenchymal tissues as an auxiliary diagnosis (18). Owing to the scarce prevalence of IMT, the diagnosis of ALK-negative IMT cases becomes challenging. Thus, the diagnostic modality of IMT remains exclusive and is primarily based on pathological findings (19).
Clinically, IMT exhibits a few inflammation-related symptoms, such as pyrexia, emaciation, and abdominalgia. Laboratory tests reveal common findings such as microcytic hypochromic anemia, reactive thrombocytosis, and elevated erythrocyte sedimentation rate (ESR). Although these findings are similar to those of malignant tumors, they lack specificity in the context of IMT diagnosis. Moreover, a delay in diagnosis and treatment might worsen the prognosis. The liver is a rare site for IMT, accounting for only a few cases (Table 2). Moreover, abdominal pain and fever are more prevalent in patients with hepatic IMT, compared to those with IMTs occurring in other organs (20). Since IMT commonly comprises inflammatory and fibrotic constituents, it may exhibit moderate to significant homogeneous or heterogeneous enhancements in contrast-enhanced scans (21). In the study by Gros et al. (22), imaging often shows low-density shadows on CT scans. Additionally, MRI might not show specific diffusion-limiting features (23). Moreover, the clinical manifestations of IMT are significantly associated with its location (6).
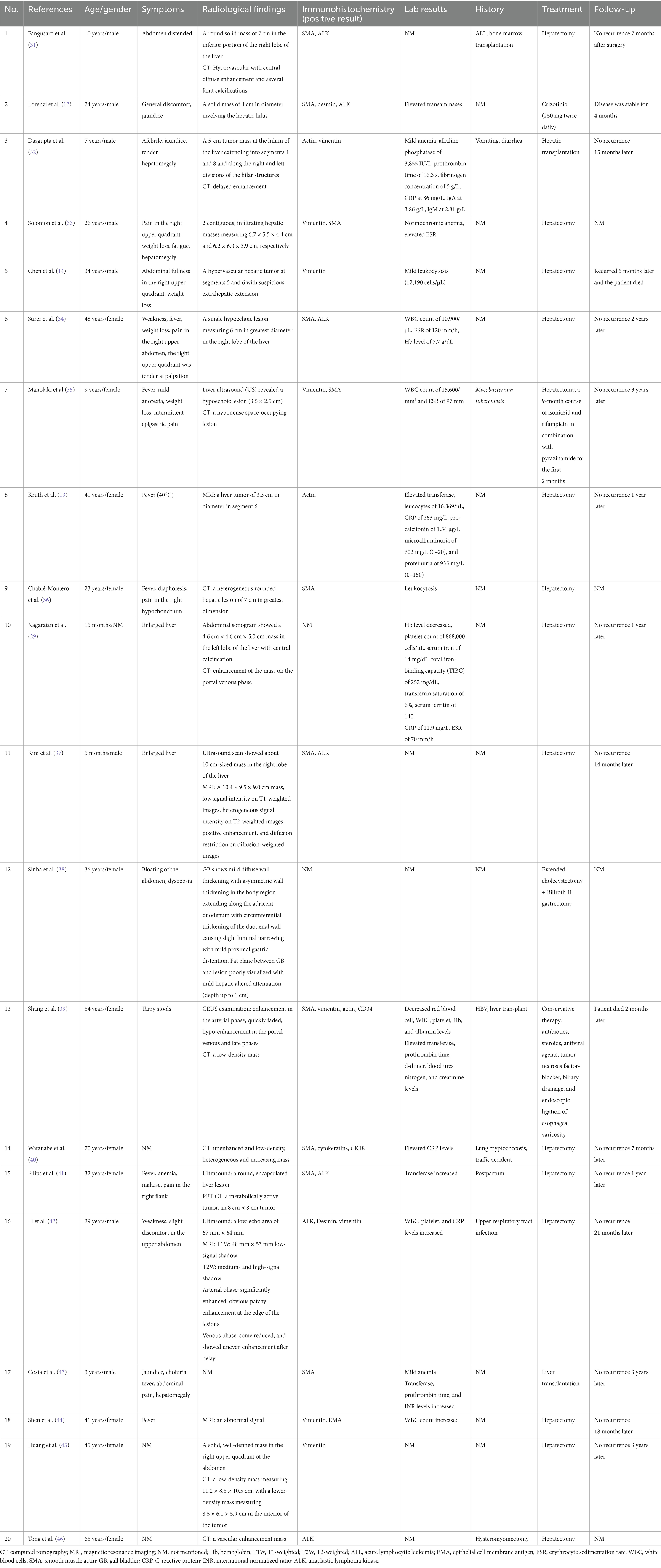
Table 2. Case report.
Surgical resection is the most common and effective treatment for localized parenchymal tumors. In local recurrence cases, a secondary surgical resection may be employed (1). In patients with advanced-stage IMT or distant metastasis, systemic pharmacotherapy might be considered if surgical resection is not feasible (24). Currently, there is no standardized chemotherapy regimen for these cases. The overall response rate (ORR) of methotrexate-vincristine (MTX-V) chemotherapy is approximately 50% (25). Despite the limited evidence regarding the efficacy of chemotherapy in IMT, there are a few studies that suggest that chemotherapy might be useful in certain postoperative scenarios where complete tumor resection is challenging. Hence, ALK tyrosine kinase inhibitors (TKIs), such as crizotinib, ceritinib, alectinib, brigatinib, lorlatinib, and ensartinib, are beneficial for ALK-positive patients (26). In patients with metastatic or recurrent IMTs accompanied by ALK negativity, programmed death 1 (PD-1) and programmed death ligand-1 (PD-L1) inhibitors might exhibit efficacy, as PD-L1 level was enhanced in 80% of such patients (27, 28).
The recurrence of IMT depends on the tumor location. High recurrence rates are seen in sporadic or severe invasive IMTs or those with incomplete resections. Moreover, the 5-year event-free survival (EFS) and overall survival (OS) rates of IMT were 82.9 and 98.1%, respectively (2, 29). Thus, genetic testing should be performed to clarify the type of gene rearrangement to determine the prognosis. The recurrence rates of extrapulmonary and pulmonary-related IMTs were approximately 25 and 2% (30), respectively, with a metastatic rate of 5% (1). Nevertheless, the recurrence might also be associated with the tumor’s unique anatomic location or histological heterogeneity, which could cause incomplete resection. To date, the recurrence of isolated tumors post complete resection is rare (2). Since it is a malignant tumor, regular follow-up is recommended. This approach can ensure timely treatment in cases of recurrence, thereby improving the survival rate.
In this case, the patient had a history of bone marrow transplantation. The immunosuppressive state might have triggered an inflammatory disease. Since this condition can cause a delay in determining the correct diagnosis and treatment, IMT should be considered in patients with a history of immunosuppression, especially when anti-infective therapies prove ineffective. In addition, a solitary hepatic tumor was identified in this case. Despite diaphragm invasion, we achieved a complete surgical resection. During the postoperative follow-up period, no recurrence was observed. Therefore, patients can benefit from radical surgical resection in cases of localized IMTs. Immunohistochemical analysis revealed that the tumor was ALK-positive. Histological examination revealed that, the tumor comprised spindle cells. These indicators suggest a favorable prognosis.
Conclusion
Hepatic IMT is rare. The rearrangement of the ALK gene might initiate the pathogenesis of IMT. Considering the possibility of IMT, laboratory tests and imaging studies should be analyzed to exclude other diseases. The pathological immunohistochemical examination is the preferred diagnostic criterion. Although the degree of malignancy is generally low, surgical resection is recommended for isolated IMTs due to their potential malignant tendencies. If surgery is unsuccessful in such cases, specific systemic therapies can be selected based on the various gene phenotypes. Additionally, clarifying the types of gene rearrangements may help determine the prognosis. Regular outpatient follow-up is crucial to administer effective and timely treatment in cases of tumor recurrence.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by the Medical Ethics Committee of the Third Affiliated Hospital of Sun Yat-sen University. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
SY: Writing – original draft, Writing – review & editing, Data curation, Investigation. YT: Conceptualization, Project administration, Supervision, Writing – review & editing. ZY: Data curation, Investigation, Methodology, Validation, Writing – original draft. JZ: Conceptualization, Data curation, Investigation, Project administration, Resources, Supervision, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This work was supported by Natural Science Foundation of Guangdong Province (A03411).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Author disclaimer
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, editors, and reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2025.1489399/full#supplementary-material
References
1. Mahajan, P, Casanova, M, Ferrari, A, Fordham, A, Trahair, T, and Venkatramani, R. Inflammatory myofibroblastic tumor: molecular landscape, targeted therapeutics, and remaining challenges. Curr Probl cancer. (2021) 45:100768. doi: 10.1016/j.currproblcancer.2021.100768
2. Casanova, M, Brennan, B, Alaggio, R, Kelsey, A, Orbach, D, van Noesel, MM, et al. Inflammatory myofibroblastic tumor: the experience of the European pediatric Soft Tissue Sarcoma Study Group (EpSSG). Eur J Cancer. (2020) 127:123–9. doi: 10.1016/j.ejca.2019.12.021
3. Chmiel, P, Słowikowska, A, Banaszek, Ł, Szumera-Ciećkiewicz, A, Szostakowski, B, Spałek, MJ, et al. Inflammatory myofibroblastic tumor from molecular diagnostics to current treatment. Oncol Res. (2024) 32:1141–62. doi: 10.32604/or.2024.050350
4. Parker, NC, Singanallur, P, Faiek, S, Gao, J, and White, P. Inflammatory myofibroblastic tumor after receiving treatment for non-small cell carcinoma. Cureus. (2024) 16:e59359. doi: 10.7759/cureus.59359
5. Sbaraglia, M, Bellan, E, and Dei Tos, AP. The 2020 WHO classification of soft tissue tumours: news and perspectives. Pathologica. (2020) 113:70–84. doi: 10.32074/1591-951X-213
6. Antonescu, CR, Suurmeijer, AJH, Zhang, L, Sung, Y-S, Jungbluth, AA, Travis, WD, et al. Molecular characterization of inflammatory myofibroblastic tumors with frequent ALK and ROS1 gene fusions and rare novel RET rearrangement. Am J Surg Pathol. (2015) 39:957–67. doi: 10.1097/PAS.0000000000000404
7. Honda, K, Kadowaki, S, Kato, K, Hanai, N, Hasegawa, Y, Yatabe, Y, et al. Durable response to the ALK inhibitor alectinib in inflammatory myofibroblastic tumor of the head and neck with a novel SQSTM1-ALK fusion: a case report. Investig New Drugs. (2019) 37:791–5. doi: 10.1007/s10637-019-00742-2
8. Yamamoto, H, Nozaki, Y, Kohashi, K, Kinoshita, I, and Oda, Y. Diagnostic utility of pan-Trk immunohistochemistry for inflammatory myofibroblastic tumours. Histopathology. (2020) 76:774–8. doi: 10.1111/his.14010
9. Pulford, K, Morris, SW, and Turturro, F. Anaplastic lymphoma kinase proteins in growth control and cancer. J Cell Physiol. (2004) 199:330–58. doi: 10.1002/jcp.10472
10. Hornick, JL, Sholl, LM, Dal Cin, P, Childress, MA, and Lovly, CM. Expression of ROS1 predicts ROS1 gene rearrangement in inflammatory myofibroblastic tumors. Mod Pathol. (2015) 28:732–9. doi: 10.1038/modpathol.2014.165
11. Yamamoto, H, Yoshida, A, Taguchi, K, Kohashi, K, Hatanaka, Y, Yamashita, A, et al. ALK, ROS1 and NTRK3 gene rearrangements in inflammatory myofibroblastic tumours. Histopathology. (2016) 69:72–83. doi: 10.1111/his.12910
12. Lorenzi, L, Cigognetti, M, Medicina, D, Pellegrini, V, Balzarini, P, Cestari, R, et al. ALK-positive inflammatory myofibroblastic tumor of the abdomen with widespread microscopic multifocality. Int J Surg Pathol. (2014) 22:640–4. doi: 10.1177/1066896914525232
13. Kruth, J, Michaely, H, Trunk, M, Niedergethmann, M, Rupf, A-K, Krämer, BK, et al. A rare case of fever of unknown origin: inflammatory myofibroblastic tumor of the liver. Case report and review of the literature. Acta Gastroenterol Belg. (2012) 75:448–53.
14. Chen, S-T, and Lee, J-C. An inflammatory myofibroblastic tumor in liver with ALK and RANBP2 gene rearrangement: combination of distinct morphologic, immunohistochemical, and genetic features. Hum Pathol. (2008) 39:1854–8. doi: 10.1016/j.humpath.2008.04.016
15. Ma, Z, Hill, DA, Collins, MH, Morris, SW, Sumegi, J, Zhou, M, et al. Fusion of ALK to the ran-binding protein 2 (RANBP2) gene in inflammatory myofibroblastic tumor. Genes Chromosomes Cancer. (2003) 37:98–105. doi: 10.1002/gcc.10177
16. Patel, AS, Murphy, KM, Hawkins, AL, Cohen, JS, Long, PP, Perlman, EJ, et al. RANBP2 and CLTC are involved in ALK rearrangements in inflammatory myofibroblastic tumors. Cancer Genet Cytogenet. (2007) 176:107–14. doi: 10.1016/j.cancergencyto.2007.04.004
17. Greenson, JK. Gastrointestinal stromal tumors and other mesenchymal lesions of the gut. Mod Pathol. (2003) 16:366–75. doi: 10.1097/01.MP.0000062860.60390.C7
18. Telugu, RB, Prabhu, AJ, Kalappurayil, NB, Mathai, J, Gnanamuthu, BR, and Manipadam, MT. Clinicopathological study of 18 cases of inflammatory myofibroblastic tumors with reference to ALK-1 expression: 5-year experience in a tertiary care center. J Pathol Transl Med. (2017) 51:255–63. doi: 10.4132/jptm.2017.01.12
19. Da, M, Qian, B, Mo, X, Xu, C, Wu, H, Jiang, B, et al. Inflammatory myofibroblastic tumors in children: a clinical retrospective study on 19 cases. Front Pediatr. (2021) 9:543078. doi: 10.3389/fped.2021.543078
20. Elpek, GÖ. Inflammatory myofibroblastic tumor of the liver: a diagnostic challenge. J Clin Transl Hepatol. (2014) 2:53–7. doi: 10.14218/JCTH.2013.00023
21. Zeng, X, Huang, H, Li, J, Peng, J, and Zhang, J. The clinical and radiological characteristics of inflammatory myofibroblastic tumor occurring at unusual sites. Biomed Res Int. (2018) 2018:1–8. doi: 10.1155/2018/5679634
22. Gros, L, Dei Tos, AP, Jones, RL, and Digklia, A. Inflammatory myofibroblastic tumour: state of the art. Cancers. (2022) 14:3662. doi: 10.3390/cancers14153662
23. Yang, X, Miao, R, Yang, H, Chi, T, Jiang, C, Wan, X, et al. Retrospective and comparative study of inflammatory myofibroblastic tumor of the liver. J Gastroenterol Hepatol. (2015) 30:885–90. doi: 10.1111/jgh.12846
24. Tao, Y-L, Wang, Z-J, Han, J-G, and Wei, P. Inflammatory myofibroblastic tumor successfully treated with chemotherapy and nonsteroidals: a case report. World J Gastroenterol. (2012) 18:7100–3. doi: 10.3748/wjg.v18.i47.7100
25. Baldi, GG, Brahmi, M, Lo Vullo, S, Cojocaru, E, Mir, O, Casanova, M, et al. The activity of chemotherapy in inflammatory myofibroblastic tumors: a multicenter, European retrospective case series analysis. Oncologist. (2020) 25:e1777–84. doi: 10.1634/theoncologist.2020-0352
26. Trahair, T, Gifford, AJ, Fordham, A, Mayoh, C, Fadia, M, Lukeis, R, et al. Crizotinib and surgery for long-term disease control in children and adolescents with ALK-positive inflammatory myofibroblastic tumors. JCO Precis Oncol. (2019) 3:1–11. doi: 10.1200/PO.18.00297
27. Du, X, Gao, Y, Zhao, H, Li, B, Xue, W, and Wang, D. Clinicopathological analysis of epithelioid inflammatory myofibroblastic sarcoma. Oncol Lett. (2018) 15:9317–26. doi: 10.3892/ol.2018.8530
28. Cottrell, TR, Duong, AT, Gocke, CD, Xu, H, Ogurtsova, A, Taube, JM, et al. PD-L1 expression in inflammatory myofibroblastic tumors. Mod Pathol. (2018) 31:1155–63. doi: 10.1038/s41379-018-0034-6
29. Nagarajan, S, Jayabose, S, McBride, W, Prasadh, I, Tanjavur, V, Marvin, MR, et al. Inflammatory myofibroblastic tumor of the liver in children. J Pediatr Gastroenterol Nutr. (2013) 57:277–80. doi: 10.1097/MPG.0b013e31829e0b3b
30. López de Sa, A, Pascual, A, Garcia Santos, J, Mendez, R, Bellon, M, Ramirez, M, et al. Inflammatory myofibroblastic tumour of an unusual presentation in the uterine cervix: a case report. World J Surg Oncol. (2021) 19:331. doi: 10.1186/s12957-021-02438-5
31. Fangusaro, J, Klopfenstein, K, Groner, J, Hammond, S, and Altura, RA. Inflammatory myofibroblastic tumor following hematopoietic stem cell transplantation: report of two pediatric cases. Bone Marrow Transplant. (2004) 33:103–7. doi: 10.1038/sj.bmt.1704292
32. Dasgupta, D, Guthrie, A, McClean, P, Davison, S, Luntley, J, Rajwal, S, et al. Liver transplantation for a hilar inflammatory myofibroblastic tumor. Pediatr Transplant. (2004) 8:517–21. doi: 10.1111/j.1399-3046.2004.00206.x
33. Solomon, GJ, Kinkhabwala, MM, and Akhtar, M. Inflammatory myofibroblastic tumor of the liver. Arch Pathol Lab Med. (2006) 130:1548–51. doi: 10.5858/2006-130-1548-IMTOTL
34. Sürer, E, Bozova, S, Gökhan, GA, Gürkan, A, and Elpek, GO. Inflammatory myofibroblastic tumor of the liver: a case report. Turk J Gastroenterol. (2009) 20:129–34.
35. Manolaki, N, Vaos, G, Zavras, N, Sbokou, D, Michael, C, and Syriopoulou, V. Inflammatory myofibroblastic tumor of the liver due to Mycobacterium tuberculosis in an immunocompetent girl. Pediatr Surg Int. (2009) 25:451–4. doi: 10.1007/s00383-009-2361-7
36. Chablé-Montero, F, Angeles-Ángeles, A, and Albores-Saavedra, J. Inflammatory myofibroblastic tumor of the liver. Ann Hepatol. (2012) 11:708–9. doi: 10.1016/S1665-2681(19)31447-4
37. Kim, S-H, Cho, YH, and Kim, HY. Two cases of infantile intra-abdominal inflammatory myofibroblastic tumor. Pediatr Gastroenterol Hepatol Nutr. (2014) 17:116–20. doi: 10.5223/pghn.2014.17.2.116
38. Sinha, L, Hasan, A, Singh, AK, Bhadani, PP, Jha, AN, Singh, PK, et al. Inflammatory myofibroblastic tumor involving liver, gallbladder, pylorus & duodenum: a rare case presentation. Int J Surg Case Rep. (2017) 31:27–9. doi: 10.1016/j.ijscr.2016.12.017
39. Shang, J, Wang, Y-Y, Dang, Y, Zhang, X-J, Song, Y, and Ruan, L-T. An inflammatory myofibroblastic tumor in the transplanted liver displaying quick wash-in and wash-out on contrast-enhanced ultrasound: a case report. Medicine. (2017) 96:e9024. doi: 10.1097/MD.0000000000009024
40. Watanabe, J, Yamada, S, Sasaguri, Y, Guo, X, Kurose, N, Kitada, K, et al. A surgical case of inflammatory myofibroblastic tumor of the liver: potentially characteristic gross features. Clin Med Insights Oncol. (2019) 13:1179554919829498. doi: 10.1177/1179554919829498
41. Filips, A, Maurer, MH, Montani, M, Beldi, G, and Lachenmayer, A. Inflammatory myofibroblastic tumor of the liver: a case report and review of literature. World J Hepatol. (2020) 12:170–83. doi: 10.4254/wjh.v12.i4.170
42. Li, Y-Y, Zang, J-F, and Zhang, C. Laparoscopic treatment of inflammatory myofibroblastic tumor in liver: a case report. World J Clin Cases. (2022) 10:11853–60. doi: 10.12998/wjcc.v10.i32.11853
43. Costa, CM, Neto, JS, Benavidez, MR, Vincenzi, R, Roda, K, Oliveira, CMV, et al. Liver transplantation for hilar inflammatory myofibroblastic tumor: case report and review of the literature. Pediatr Transplant. (2023) 27:e14445. doi: 10.1111/petr.14445
44. Shen, L, Yang, Z, Ding, R, Wei, W, and Xu, Y. Hepatic inflammatory myofibroblastic tumor: one case report. Front Surg. (2022) 9:902753. doi: 10.3389/fsurg.2022.902753
45. Huang, K, Zhao, P, Zhao, J, Zhao, P, and Yang, J. A unique case of inflammatory myofibroblastic tumor of the liver manifesting with biloma: a case report. Oncol Lett. (2022) 24:227. doi: 10.3892/ol.2022.13348
Keywords: anaplastic lymphoma kinase (ALK), case report, immunohistochemistry, inflammatory myofibroblastic tumor, liver tumor, MRI
Citation: Yang S, Tang Y, Yuan Z and Zhang J (2025) Inflammatory myofibroblastic tumor in the liver after bone marrow transplantation: case report and literature review. Front. Med. 12:1489399. doi: 10.3389/fmed.2025.1489399
Edited by:
Hiroyuki Nojima, Teikyo University Chiba Medical Center, JapanReviewed by:
Rahul Gupta, Synergy Institute of Medical Sciences, IndiaTiago Siqueira, Albert Einstein Israelite Hospital, Brazil
Copyright © 2025 Yang, Tang, Yuan and Zhang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jianwen Zhang, emhqaWFudzJAbWFpbC5zeXN1LmVkdS5jbg==
†These authors share first authorship