 Ailing Zhu1†
Ailing Zhu1† Yangchun Wang
Yangchun Wang Xin Yao
Xin Yao Junjun Liu
Junjun Liu
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Med., 03 February 2025
Sec. Pulmonary Medicine
Volume 12 - 2025 | https://doi.org/10.3389/fmed.2025.1477388
Background: Despite chronic obstructive pulmonary disease’s (COPD)'s prevalence in the general populace, its incidence in heart failure (HF) patients is understudied. This study aimed to assess COPD prevalence and clinical associations in Chinese HF patients.
Methods: From the Chinese Heart Failure Study, demographic and clinical details of 2008 HF patients were analyzed. Divided into 233 COPD cases and 1775 non-COPD controls, a multivariable logistic regression identified factors linked to COPD onset in HF, with thorough examination of intergroup clinical differences.
Results: The incidence of COPD in HF individuals was 11.60% (233/2008). The COPD subgroup featured a higher ratio of individuals over 60 and males, alongside lower systolic blood pressure (SBP), body mass index (BMI), higher Charlson Comorbidity Index (CCI) scores, and increased PaCO₂ levels (p < 0.05). Type II respiratory failure and right ventricular dysfunction (RVD) were more prevalent in the COPD subgroup (p < 0.001). Binary logistic regression, after adjustments, indicated positive associations between COPD and age over 60 (OR = 3.831, 95%CI: 1.085–13.526, p = 0.037), male sex (OR = 1.587, 95%CI: 1.032–2.441, p = 0.036), higher CCI (OR = 2.214, 95%CI: 1.796–2.729, p < 0.001), elevated PaCO2 (OR = 1.035, 95%CI: 1.015–1.055, p < 0.001), and RVD (OR = 0.605, 95%CI: 0.119–3.063, p = 0.544). Inversely, higher SBP (OR = 0.990, 95%CI: 0.982–0.998, p = 0.020) and log (triglycerides) (OR = 0.183, 95%CI: 0.064–0.552, p = 0.002) were negatively correlated with COPD in HF patients.
Conclusion: In a large cohort of Chinese Heart Failure (HF) patients, our study revealed a notable COPD prevalence. Key risk factors included age, sex, elevated PaCO2, CCI score, and right heart failure, while higher SBP and triglyceride levels offered protection. These insights lay groundwork for probing disease mechanisms and therapeutic approaches.
Chronic Obstructive Pulmonary Disease (COPD) is the fourth-leading cause of mortality worldwide, contributing significantly to the rising social and economic burden (1, 2). Global estimates of the number of people with COPD aged 30–79 years old are 391.9 million, based on the Global Initiative for Chronic Obstructive Lung Disease (GOLD) criteria (3). Approximately 99.9 million people in China are affected by a prevalence rate of 8.6% of spirometry-defined COPD (4). COPD frequently coexists with cardiovascular diseases, leading to more severe outcomes than either condition alone (5, 6). The three most common cardiac comorbidities of COPD are heart failure, ischemic heart disease, and atrial fibrillation (7). Both COPD and HF are linked to increased mortality, increased healthcare expenses, and there is a pressing need for better treatment approaches.
The association between COPD and HF has significant systemic implications, characterized by a chronic and progressive course that impairs exercise tolerance (8). Emerging research points to modifications in vascular molecular processes as potential initiators of pulmonary emphysema, with a particular emphasis on the significance of the NO-sGC-cGMP axis. This pathway is now recognized as a key player in both the pathophysiology of the condition and its inherent restorative capabilities (9). Several significant risk factors for COPD have been found, including male gender, smoking, body mass index (BMI), biomass exposure, and occupational exposure to dust or smoke (2, 3). Risk factors for COPD and HF are similar and include low-grade systemic inflammation, smoking, and advanced age (7). Despite this, there has been limited research on identifying biomarkers associated with COPD, particularly in HF patients. There is a lot of data to support the theory that dyslipidemia contributes significantly to the development of COPD (10). In an Indian population study, components of metabolic syndrome (MetS) such as BMI, systolic blood pressure (SBP), triglycerides (TG), high-density lipoprotein (HDL) cholesterol, and fasting blood glucose (FBG) were significantly correlated with COPD (11). Further research has also shown that people with MetS have higher odds of high blood pressure (BP), high TG, poor HDL cholesterol, abdominal obesity, and other COPD risk factors (12, 13). Few studies have focused on lipids as biomarkers for COPD in HF patients.
Most COPD incidence studies emphasize age, sex, smoking, and BMI, rarely addressing blood counts, biochemistry, and blood gas analysis impacts. And there is a dearth of epidemiological data on the risk factors for COPD in HF patients, particularly among the Chinese population. The principal objectives of this study were twofold: firstly, to ascertain the prevalence of COPD in HF inpatients; and secondly, to evaluate the relationship between COPD and HF in Chinese individuals, encompassing demographic characteristics, biochemical indicators, CCI scores, and other pertinent factors. By elucidating these relationships, we aim to inform and enhance the development of more targeted therapeutic strategies for patients with coexisting COPD and HF.
The study population was obtained from an open-source online database of patients with HF in China, accessed via the PhysioNet platform (14). A total of 2008 inpatients were recruited at Zigong Fourth People’s Hospital between December 2016 and June 2019. The research design and database information have been described in detail (15). The study protocol and methodologies were accepted by the Ethics Committee of Zigong Fourth People’s Hospital (approval number: 2020-010). The study adhered to the principles outlined in the Declaration of Helsinki.
Patients admitted to the hospital with a diagnosis of heart failure were enrolled in the study. Electronic healthcare records of consecutive patients diagnosed with HF were reviewed (15). The database included all types of HF—including acute, chronic, left-sided, right-sided, and mixed presentations diagnosed in accordance with the 2016 European Society of Cardiology (ESC) criteria (16).
1. Clinical signs and symptoms of heart failure (HF): fatigue, poor exercise tolerance, delayed recovery after exercise, ankle swelling, and dyspnea, especially orthopnea and nocturnal dyspnea. Clinical indicators of HF include third heart sound (S3 gallop), hepatojugular reflux, high jugular venous pressure, and lateral apical impulse displacement.
2. Biomarker Levels: >35 pg./mL elevated BNP or > 125 pg./mL NT-proBNP.
3. Cardiac Structural/Functional Changes: Objective evidence supporting HF diagnosis.
4. Diagnostic Confirmation: For unclear cases, stress tests or invasive assessment of LV filling pressures confirms HF.
Heart failure can be categorized into left-sided, right-sided, and biventricular types. Left-sided failure includes systolic (reduced ejection fraction) and diastolic (preserved ejection fraction) forms, while right-sided failure often results from left-sided issues or conditions affecting the right ventricle directly, and biventricular failure impacts both ventricles simultaneously (16). We utilized various echocardiographic parameters to group and evaluate heart failure patients, including left ventricular ejection fraction (LVEF), mitral valve flow E/A ratio, tricuspid annular plane systolic excursion (TAPSE), and right ventricular systolic peak velocity (RV S′), among others. However, the source data lacked information on diastolic and systolic heart failure (15). Therefore, our analysis is based on classifications of left heart failure, right heart failure, and global heart failure.
Type II respiratory failure, also known as hypercapnic respiratory failure, is defined by the inability of the respiratory system to adequately eliminate carbon dioxide, resulting in elevated arterial carbon dioxide levels (PaCO2 ≥ 45 mmHg) along with hypoxemia (17).
The fraction of inspired oxygen (FiO2) denotes the proportion of oxygen in the gas mixture that the patient breathes in, typically expressed as a fraction or percentage (18).
Demographics, initial clinical parameters, comorbidities, laboratory results, medicines, and outcomes were the six categories that made up the dataset. A historical case of congestive heart failure, myocardial infarction, dementia, Parkinson’s disease, peripheral vascular disease, cerebrovascular disease, peptic ulcer disease, connective tissue disease, diabetes, hemiplegia, and leukemia were among the comorbidities that were assessed. By reviewing electronic medical records (EMRs) and referencing disease codes rather than the gold standard for lung function, the study population was divided into two groups based on the presence or absence of COPD. Signs of emphysema and alveolar changes were evident on CT scans for the majority of patients, thereby supporting the diagnosis of COPD. The weighted scores of the comorbid conditions listed above were added up to create the Charlson Comorbidity Index (CCI), which considers the number and severity of comorbid diseases, assesses the risk of mortality (19, 41).
Laboratory findings were obtained on the first day of hospital admission, following an eight-hour fast and included the following parameters: serum uric acid, creatinine, glomerular filtration rate (eGFR), cystatin C, hemoglobin, platelet, D-dimer, high-sensitivity troponin, Glutamic-oxaloacetic transaminase (GOT), Gamma-glutamic transferase (GGT), total cholesterol, low-density lipoprotein (LDL) cholesterol, triglycerides, HDL cholesterol, blood pH, and partial pressure of carbon dioxide (PaCO₂).
The statistical software SPSS 26.0 was used for the analyses. The normality of continuous variables was evaluated using the Kolmogorov–Smirnov technique. The means ± standard deviation (SD) of continuous variables with a normal distribution were displayed, and the independent samples T-test was used to compare groups. Log transformation was utilized for variables that exhibit non-normal distributions, helping to normalize the data and stabilize variance for improved statistical analysis. The categorical variables were summed up as percentages and frequencies, and the χ2 test was used to compare groups. Spearman correlation coefficients were used to analyze relationships between biological markers and clinical and demographic variables. To eliminate variables with variance inflation factor (VIF) values greater than five, we ran a VIF screening (19). The factors impacting the development of COPD in the HF population were examined using binary logistic regression analysis, which included variables with a p value <0.05 in the univariate analysis that were highly clinically relevant. Each two-tailed statistical test had a significance level of p < 0.05.
All 2008 HF patients were enrolled in the study; 233 of these patients also had concurrent COPD diagnoses, for an overall rate of 11.60%. Table 1 presents a comprehensive comparison of clinical factors and sociodemographic information between the COPD and non-COPD groups. The COPD group exhibited a higher frequency of older males than the non-COPD groups. Additionally, the COPD group showed significantly lower SBP (t = 2.04, p = 0.042) and body mass index (BMI) (t = 2.20, p = 0.028), as well as higher Charlson Comorbidity Index (CCI) scores (t = −12.75, p < 0.001) and inspired oxygen index (t = −3.49, p < 0.001). The incidence of type II respiratory failure (χ2 = 25.51, p < 0.001) and right heart failure (χ2 = 14.421, p = 0.001) was significantly higher in the COPD group. Moreover, our analysis showed higher PaCO2 (t = −3.91, <0.001) and lower log (triglyceride) (t = 3.95, p < 0.001) in the COPD group (Table 1).
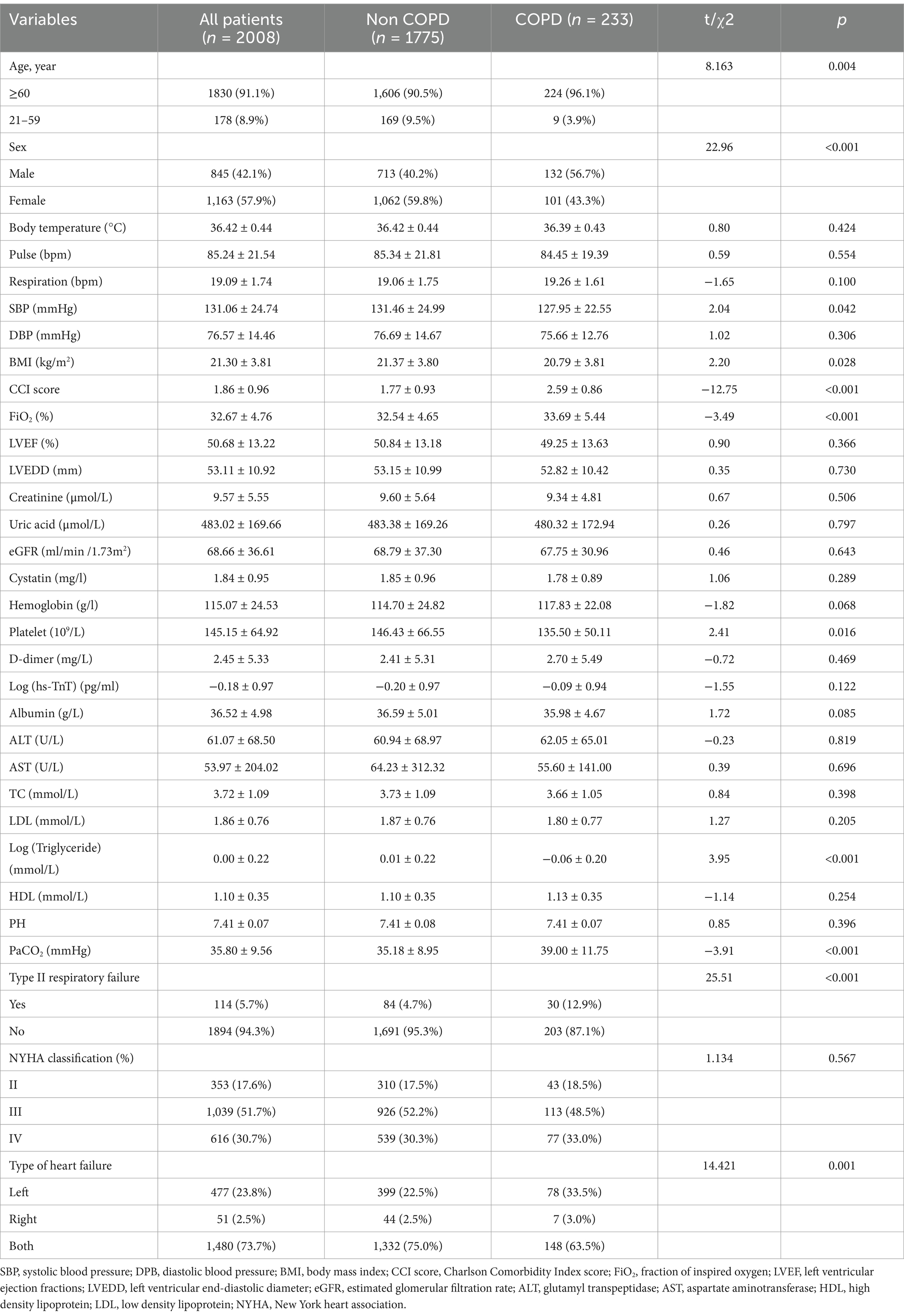
Table 1. Characteristics of HF patients with and without COPD.
The study employed binary logistic regression analysis to identify independent determinants of COPD risk in individuals with heart failure. Age, sex, SBP, BMI, CCI score, inspired oxygen index, type II respiratory failure, heart failure type, PaCO2, and triglyceride were among the factors. The results of the analysis showed that the following factors had a positive correlation with COPD: age (OR = 3.831, 95% CI 1.085–13.526, p = 0.037); male sex (OR = 1.587, 95% CI 1.032–2.441, p = 0.036); CCI score (OR = 2.214, 95% CI 1.796–2.729, p < 0.001); PaCO2 (OR = 1.035, 95%CI 1.015–1.055, p < 0.001); the right heart failure (RHF) group (OR = 2.344, 95% CI 1.504–3.653, p < 0.001) (compared to the left heart failure group). On the other hand, in HF patients, higher log (triglyceride) level (OR = 0.183, 95%CI 0.064–0.552, p = 0.002) and high SBP (OR = 0.990, 95%CI: 0.982–0.998, p = 0.020) were found to be negatively correlated with COPD (Table 2).
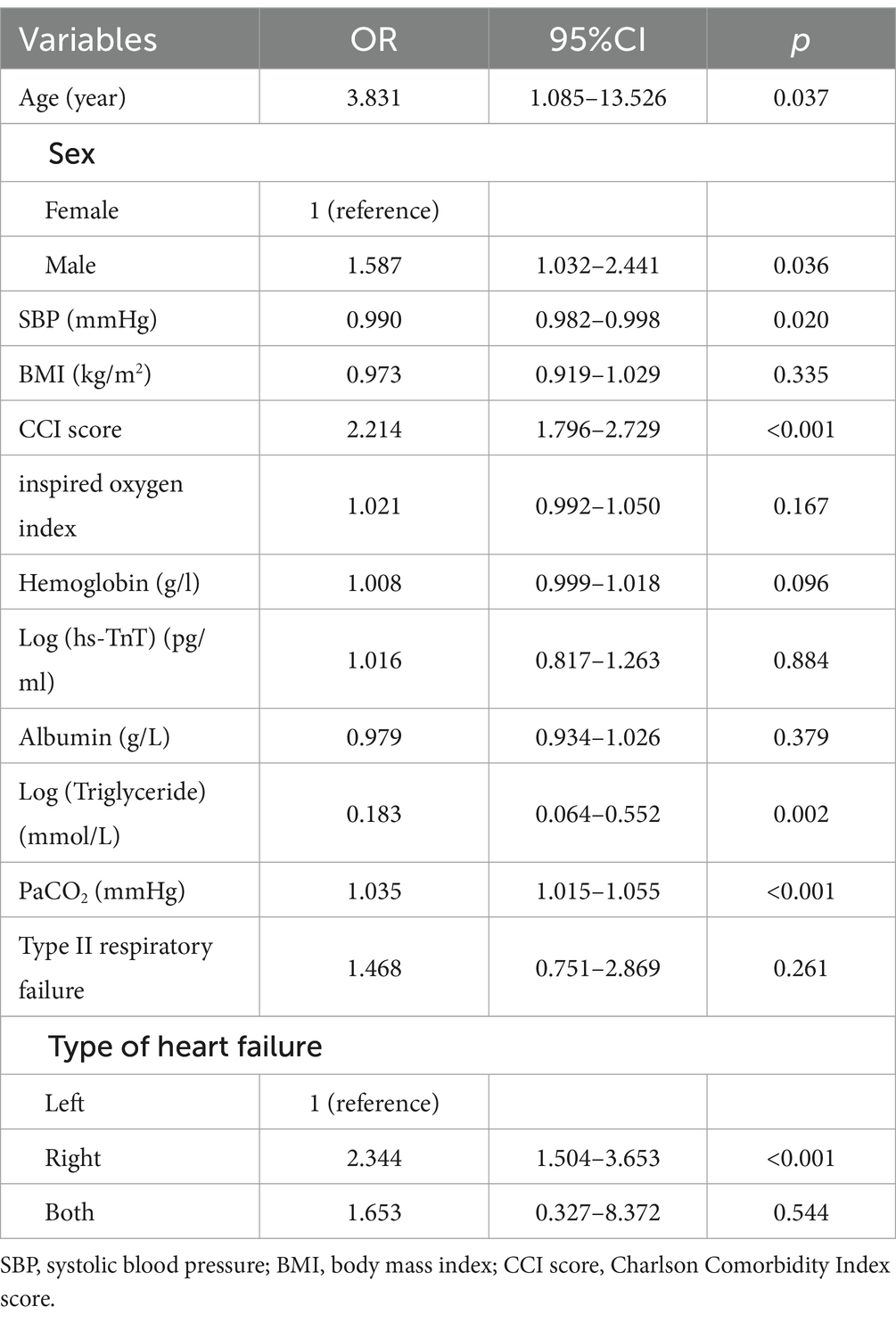
Table 2. Related factors of COPD in patients with HF based on binary logistic regression.
This cross-sectional study is the first that we are aware of that estimates the prevalence and clinical correlates of COPD in a sizable sample of HF Chinese patients. Our findings indicate that the prevalence of COPD in this population is 11.60%. The finding is consistent with a previous study (20). Pellicori et al. reported a prevalence range of 10 to 20% for COPD among patients with HF in both observational studies and randomized controlled trials. This discrepancy may suggest that COPD is often underdiagnosed by cardiologists or that HF exerts pulmonary effects that resemble those of COPD, potentially leading to overdiagnosis (21). Our study also discovered that COPD patients with HF had significantly higher CCI scores, and PaCO2, but lower triglycerides and SBP compared to patients with HF alone (p < 0.05). Moreover, the COPD group exhibited an increased rate of right heart failure.
According to our research, males over 60 were more likely than women in the same age group to have COPD, which is consistent with previous research findings (22–27). In China, multiple studies have reported that age is a significant factor in the prevalence of COPD (23–25). Specifically, the risk of COPD doubles for every additional 10 years of age among adults aged 40 and above. Furthermore, the decrease in forced expiratory volume in one second (FEV1) accelerates more significantly in older individuals than in younger individuals (28). The higher incidence of COPD in men is likely related to the higher prevalence of smoking among men, which is a proven independent risk factor for COPD. In addition, higher levels of estrogen in women may offer a protective effect, reducing the incidence of persistent airflow limitation by promoting alveolar regeneration and maintaining alveolar structure (29).
There has not been much research done on the correlation between blood pressure and COPD in heart failure patients. Although hypertension does not directly cause COPD, it may indirectly increase the risk by worsening lung function via systemic inflammation, oxidative stress, vascular issues, and autonomic imbalance (13). In contrast to the findings of an earlier article (11), the present findings indicate a higher frequency of COPD in HF with a lower SBP. However, in the previous study, there was no statistically significant change in SBP between the groups with COPD and those without. A monotonic relationship was found by Rao et al. between SBP and the risk of several cardiovascular endpoints, with COPD patients having the lowest risk at SBP <120 mmHg (30). It’s possible that variations in research populations and endpoints are the cause of the disparity between our findings and those of earlier investigations. To confirm that these results are coherent, more research is needed. These findings imply that, in order to prevent negative consequences, blood pressure in HF patients should be kept within an ideal range.
In our study, patients with HF who had higher CCI scores had an increased chance of developing COPD. These results are in line with earlier research (31, 32). Patients with a higher CCI score exhibited more severe lung function impairment and a higher mMRC score in comparison to those with a lower CCI score (31), all of which are crucial conditions for the development of COPD. The comorbidities observed may share common risk factors, such as systemic inflammation, vascular endothelial dysfunction, and hypoxia, which have all been associated with an increased incidence of COPD and may act as risk factors for its development (33).
It is commonly recognized that dyslipidemia contributes significantly to the advancement of COPD (10). The leading role of lipid metabolism in the lung extends beyond serving as a structural or energy substrate; it is also crucial in the immune defense of the lung (10). In COPD, lipid metabolic pathways and molecules undergo significant changes, which can subsequently influence the functions of specific cells—such as the production of inflammatory mediators, immune regulation, and cell death—thereby contributing to the progression of the disease (34). In our study, low triglyceride levels were identified as a risk factor for COPD (OR = 0.183). However, this finding was not statistically significant in an Indian population (11). This may be attributed to the study focusing on a specific subgroup of heart failure patients who had a poorer nutritional status compared to the general population. Previous studies have consistently demonstrated a positive correlation between a low BMI and the prevalence of COPD. This association has been identified as a potential risk factor for COPD and an independent indicator of poor prognosis (22, 24–27). These patients typically exhibit poorer lung function compared to those with a higher BMI, but similar to our study, this association did not reach statistical significance (10) and warrants further investigation in our specific group.
Correlation analysis in the study shows that the incidence of COPD patients was positively correlated with higher PaCO2 levels. This finding aligns with a previous study (35), which demonstrated that subjects with a higher level of PaCO2 levels had lower FEV1% levels. In individuals with severe COPD, expiratory flow limitation and dynamic lung hyperinflation can lead to increased hypercapnia (36). Higher PaCO2 levels could therefore be a sign of severe COPD. Furthermore, restrictive ventilatory abnormalities, which lower vital capacity by replacing oxygen in the lungs with blood or interstitial fluid and cause hypercapnia, are frequently seen in heart failure patients (37). It is important to ask why COPD patients are more likely than CHF patients to retain CO2. Submissive hypercapnia, an adaptive brain mechanism to conserve breathing effort when recovering normocapnia is difficult or impractical, may be the cause of this phenomenon (38). Moreover, a higher risk of long-term mortality has been linked to a lower PaCO2 level at admission (39). Therefore, maintaining appropriately low levels of CO2 partial pressure is crucial for HF patients.
The findings of this study’s binary logistic regression analysis further showed that, in HF patients, RHF is an independent related factor of COPD. One well-researched COPD consequence is RHF. Pulmonary hypertension (PH) develops in COPD patients as a result of systemic inflammation and chronic hypoxia. PH leads to right ventricular hypertrophy, dilatation and systolic dysfunction (8). Compared to having COPD alone, the combination of COPD and PH is associated with a 70% higher risk of death (40).
The strength of the current study lies in its dual focus on clinical characteristics and objective blood markers to evaluate factors associated with COPD in HF patients. This comprehensive approach is seldom addressed in studies involving the Chinese population. However, it should be noted that this study is subject to several limitations. First, being a cross-sectional study, the results should only be interpreted as an association rather than causal relationships between COPD and the selected variables. Secondly, the absence of lung function data necessitated the identification of COPD patients based solely on their medical history, which could introduce information bias. Considering that COPD is a multifactorial disease with lung function being a crucial diagnostic criterion, the lack of comprehensive lung function data in our study restricts the depth and precision of our analysis. Finally, in addition to smoking habits, factors like regional air pollution, indoor fuel use in rural areas, malnutrition in certain regions, and a family history of respiratory diseases significantly impact COPD prevalence. These factors, along with disease severity and age stratification, differ from those in Western or urban populations. Our study, however, lacks detailed analyses in these critical areas.
In conclusion, a sizable sample of Chinese HF patients in this study had a significant prevalence of COPD. It was observed that patients with both COPD and HF exhibited lower SBP, reduced triglyceride levels, and elevated PaCO2. Furthermore, it was found that among patients with HF, male sex, age, a greater ACCI, and right heart failure were independent predictors of COPD. Therefore, when treating patients with heart failure, it is important to monitor and manage their blood pressure, address comorbidities, ensure adequate nutritional support, and optimize carbon dioxide excretion to mitigate the risk of developing COPD.
Publicly available datasets were analyzed in this study. This data can be found here: Zhang et al. (15), available at https://doi.org/10.13026/8a9e-w734.
Ethical approval was not required for the study involving humans in accordance with the local legislation and institutional requirements. Written informed consent to participate in this study was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and the institutional requirements.
AZ: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Supervision, Validation, Visualization, Writing – original draft. MH: Data curation, Formal analysis, Investigation, Methodology, Validation, Visualization, Writing – original draft. DG: Project administration, Resources, Supervision, Writing – original draft. XZ: Formal analysis, Methodology, Writing – original draft. JZ: Formal analysis, Methodology, Writing – original draft. YW: Data curation, Formal analysis, Methodology, Writing – original draft. XY: Formal analysis, Validation, Visualization, Writing – review & editing. JL: Formal analysis, Methodology, Validation, Writing – review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors thank the First Affiliated Hospital of Nanjing Medical University for the supports.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. GBD Chronic Respiratory Disease Collaborators. Prevalence and attributable health burden of chronic respiratory diseases, 1990–2017: a systematic analysis for the global burden of disease study 2017. Lancet Respir Med. (2020) 8:585–96. doi: 10.1016/S2213-2600(20)30105-3
2. Agustí, A, Celli, BR, Criner, GJ, Halpin, D, Anzueto, A, Barnes, P, et al. Global initiative for chronic obstructive lung disease 2023 report: GOLD executive summary. Eur Respir J. (2023) 61:2300239. doi: 10.1183/13993003.00239-2023
3. Adeloye, D, Song, P, Zhu, Y, Campbell, H, Sheikh, A, and Rudan, I. NIHR RESPIRE global respiratory health unit. Global, regional, and national prevalence of, and risk factors for, chronic obstructive pulmonary disease (COPD) in 2019: a systematic review and modelling analysis. Lancet. Respir Med. (2022) 10:447–58. doi: 10.1016/S2213-2600(21)00511-7
4. Wang, C, Xu, J, Yang, L, Xu, Y, Zhang, X, Bai, C, et al. Prevalence and risk factors of chronic obstructive pulmonary disease in China (the China pulmonary health [CPH] study): a national cross-sectional study. Lancet. (2018) 391:1706–17. doi: 10.1016/S0140-6736(18)30841-9
5. Rabe, KF, Hurst, JR, and Suissa, S. Cardiovascular disease and COPD: dangerous liaisons? Eur Respir Rev. (2018) 27:180057. doi: 10.1183/16000617.0057-2018
6. Almagro, P, Boixeda, R, Diez-Manglano, J, Gómez-Antúnez, M, López-García, F, and Recio, J. Insights into chronic obstructive pulmonary disease as critical risk factor for cardiovascular disease. Int J Chron Obstruct Pulmon Dis. (2020) 15:755–64. doi: 10.2147/COPD.S238214
7. Roversi, S, Fabbri, LM, Sin, DD, Hawkins, NM, and Agustí, A. Chronic obstructive pulmonary disease and cardiac diseases. An urgent need or integrated care. Am J Respir Crit Care Med. (2016) 194:1319–36. doi: 10.1164/rccm.201604-0690SO
8. Horodinschi, RN, Bratu, OG, Dediu, GN, Pantea Stoian, A, Motofei, I, and Diaconu, CC. Heart failure and chronic obstructive pulmonary disease: a review. Acta Cardiol. (2020) 75:97–104. doi: 10.1080/00015385.2018.1559485
9. Karnati, S, Seimetz, M, Kleefeldt, F, Sonawane, A, Madhusudhan, T, Bachhuka, A, et al. Chronic obstructive pulmonary disease and the cardiovascular system: vascular repair and regeneration as a therapeutic target. Front Cardiovasc Med. (2021) 8:649512. doi: 10.3389/fcvm.2021.649512
10. Kotlyarov, S, and Kotlyarova, A. Molecular mechanisms of lipid metabolism disorders in infectious exacerbations of chronic obstructive pulmonary disease. Int J Mol Sci. (2021) 22:7634. doi: 10.3390/ijms22147634
11. Acharyya, A, Shahjahan, MD, Mesbah, FB, Dey, SK, and Ali, L. Association of metabolic syndrome with chronic obstructive pulmonary disease in an Indian population. Lung India. (2016) 33:385–90. doi: 10.4103/0970-2113.184871
12. Mahato, B, Nigoskar, S, Lakshmi, LJ, and Zephy, D. Glycemic profile and lipid profile in chronic obstructive pulmonary disease (COPD) patients with and without metabolic syndrome. Cureus. (2024) 16:e58921. doi: 10.7759/cureus.58921
13. Chen, W, Thomas, J, Sadatsafavi, M, and FitzGerald, JM. Risk of cardiovascular comorbidity in patients with chronic obstructive pulmonary disease: a systematic review and meta-analysis. Lancet Respir Med. (2015) 3:631–9. doi: 10.1016/S2213-2600(15)00241-6
14. Goldberger, AL, Amaral, LA, Glass, L, Hausdorf, JM, Ivanov, PC, Mark, RG, et al. PhysioBank, PhysioToolkit, and PhysioNet: components of a new research resource for complex physiologic signals. Circulation. (2000) 101:E215–20. doi: 10.1161/01.CIR.101.23.e215
15. Zhang, Z, Cao, L, Zhao, Y, Xu, Z, Chen, R, Lv, L, et al. Hospitalized patients with heart failure: integrating electronic healthcare records and external outcome data (version 1.2). PhysioNet. (2020):101, e215–e220. doi: 10.13026/8a9e-w734
16. Ponikowski, P, Voors, AA, Anker, SD, Bueno, H, Cleland, JG, Coats, AJ, et al. 2016 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure: the task force for the diagnosis and treatment of acute and chronic heart failure of the european society of cardiology (ESC). Eur J Heart Fail. (2016) 18:891–975. doi: 10.1002/ejhf.592
17. Lamba, TS, Sharara, RS, Singh, AC, and Balaan, M. Pathophysiology and classification of respiratory failure. Crit Care Nurs Q. (2016) 39:85–93. doi: 10.1097/CNQ.0000000000000102
18. Klitgaard, TL, Schjørring, OL, Nielsen, FM, Meyhoff, CS, Perner, A, Wetterslev, J, et al. Higher versus lower fractions of inspired oxygen or targets of arterial oxygenation for adults admitted to the intensive care unit. Cochrane Database Syst Rev. (2023) 2023:CD012631. doi: 10.1002/14651858.CD012631.pub3
19. Hsieh, FY, Lavori, PW, Cohen, HJ, and Feussner, JR. An overview of variance inflation factors for sample-size calculation. Eval Health Prof. (2003) 26:239–57. doi: 10.1177/0163278703255230
20. Pellicori, P, Cleland, JG, and Clark, AL. Chronic obstructive pulmonary disease and heart failure: a breathless conspiracy. Cardiol Clin. (2022) 40:171–82. doi: 10.1016/j.ccl.2021.12.005
21. Pellicori, P, Salekin, D, Pan, D, and Clark, AL. This patient is not breathing properly: is this COPD, heart failure, or neither? Expert Rev Cardiovasc Ther. (2017) 15:389–96. doi: 10.1080/14779072.2017.1317592
22. Wang, Z, Li, Y, Lin, J, Huang, J, Zhang, Q, Wang, F, et al. Prevalence, risk factors, and mortality of COPD in young people in the USA: results from a population-based retrospective cohort. BMJ Open Respir Res. (2023) 10:e001550. doi: 10.1136/bmjresp-2022-001550
23. Haque, MA, Salwa, M, Islam, MT, Sultana, S, Rahman, F, Ahmed, S, et al. Prevalence of chronic obstructive pulmonary disease (COPD) among rural population: a national survey in Bangladesh. Lung India. (2022) 39:537–44. doi: 10.4103/lungindia.lungindia_300_22
24. Zhang, X, Lei, Z, Wu, Y, Song, Y, Wu, X, Yang, B, et al. Prevalence and risk factors for COPD in an urbanizing rural area in Western China: a cross-sectional study. Int J Chron Obstruct Pulmon Dis. (2023) 18:459–68. doi: 10.2147/COPD.S400213
25. Yan, X, Xu, L, Shi, B, Wang, H, Xu, X, and Xu, G. Epidemiology and risk factors of chronic obstructive pulmonary disease in Suzhou: a population-based cross-sectional study. J Thorac Dis. (2020) 12:5347–56. doi: 10.21037/jtd-20-1616
26. Kanetake, R, Takamatsu, K, Park, K, and Yokoyama, A. Prevalence and risk factors for COPD in subjects with preserved ratio impaired spirometry. BMJ Open Respir Res. (2022) 9:e001298. doi: 10.1136/bmjresp-2022-001298
27. García Castillo, E, Alonso Pérez, T, Peláez, A, Pérez González, P, Soriano, JB, and Ancochea, J. Prevalence of chronic obstructive pulmonary disease in an urban area. changes in COPD ten years on. Int J Chron Obstruct Pulmon Dis. (2022) 17:2431–41. doi: 10.2147/COPD.S377140
28. Kim, SJ, Lee, J, Park, YS, Lee, CH, Yoon, HI, Lee, SM, et al. Age-related annual decline of lung function in patients with COPD. Int J Chron Obstruct Pulmon Dis. (2015) 11:51–60. doi: 10.2147/COPD.S95028
29. Kamil, F, Pinzon, I, and Foreman, MG. Sex and race factors in early-onset COPD. Curr Opin Pulm Med. (2013) 19:140–4. doi: 10.1097/MCP.0b013e32835d903b
30. Rao, S, Nazarzadeh, M, Li, Y, Canoy, D, Mamouei, M, Salimi-Khorshidi, G, et al. Systolic blood pressure, chronic obstructive pulmonary disease and cardiovascular risk. Heart. (2023) 109:1216–22. doi: 10.1136/heartjnl-2023-322431
31. Huang, YL, Mao, B, Mim, J, Li, GH, Zheng, YQ, Wu, LH, et al. The associations between comorbidity and exacerbation risk in patients with chronic obstructive pulmonary disease. Zhonghua Jie He He Hu xi Za Zhi. (2018) 41:349–54. doi: 10.3760/cma.j.issn.1001-0939.2018.05.009
32. Osundolire, S, Goldberg, RJ, and Lapane, KL. Differences in chronic obstructive pulmonary disease among US nursing home residents with heart failure according to sex and type of heart failure. Clin Respir J. (2023) 17:1130–44. doi: 10.1111/crj.13698
33. Smith, MC, and Wrobel, JP. Epidemiology and clinical impact of major comorbidities in patients with COPD. Int J Chron Obstruct Pulmon Dis. (2014) 9:871–88. doi: 10.2147/COPD.S49621
34. Chen, H, Li, Z, Dong, L, Wu, Y, Shen, H, and Chen, Z. Lipid metabolism in chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. (2019) 14:1009–18. doi: 10.2147/COPD.S196210
35. Zhang, X, Miao, X, Ding, K, Wang, J, Hu, B, Hu, X, et al. The relationship of partial pressure of carbon dioxide (PaCO2) with disease severity indicators such as BODE and GOLD in hospitalized COPD patients. Int J Clin Pract. (2022) 2022:4205079–8. doi: 10.1155/2022/4205079
36. Neder, JA, Arbex, FF, Alencar, MC, O’Donnell, CD, Cory, J, Webb, KA, et al. Exercise ventilatory inefficiency in mild to end-stage COPD. Eur Respir J. (2014) 45:377–87. doi: 10.1183/09031936.00135514
37. Agostoni, P, Cattadori, G, Bussotti, M, and Apostolo, A. Cardiopulmonary interaction in heart failure. Pulm Pharmacol Ther. (2007) 20:130–4. doi: 10.1016/j.pupt.2006.03.001
38. Poon, CS, Tin, C, and Song, G. Submissive hypercapnia: why COPD patients are more prone to CO2 retention than heart failure patients. Respir Physiol Neurobiol. (2015) 216:86–93. doi: 10.1016/j.resp.2015.03.001
39. Kato, T, Kasai, T, Suda, S, Sato, A, Ishiwata, S, Yatsu, S, et al. Prognostic effects of arterial carbon dioxide levels in patients hospitalized into the cardiac intensive care unit for acute heart failure. Eur Heart J Acute Cardiovasc Care. (2021) 10:497–502. doi: 10.1093/ehjacc/zuab001.;
40. Cook, DP, Xu, M, Martucci, VL, Annis, JS, Aldrich, MC, Hemnes, AR, et al. Clinical insights into pulmonary hypertension in chronic obstructive pulmonary disease. Pulm Circ. (2022) 12:e12006. doi: 10.1002/pul2.12006
Keywords: COPD, HF, prevalence, clinical correlates, CCI score, lipid metabolism
Citation: Zhu A, Hu M, Ge D, Zhang X, Zhang J, Wang Y, Yao X and Liu J (2025) Prevalence and clinical correlates of chronic obstructive pulmonary disease in heart failure patients: a cross-sectional study in China. Front. Med. 12:1477388. doi: 10.3389/fmed.2025.1477388
Edited by:
Takatoshi Kasai, Juntendo University, JapanReviewed by:
Jun-Jun Yeh, Ditmanson Medical Foundation Chia-Yi Christian Hospital, TaiwanCopyright © 2025 Zhu, Hu, Ge, Zhang, Zhang, Wang, Yao and Liu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xin Yao, eHlhbzE5OThAMTI2LmNvbQ==; Junjun Liu, MzI1NzIzNDhAcXEuY29t
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.