 Zhihao Xu
Zhihao Xu Weijian Zhu
Weijian Zhu Sirui Zhou3
Sirui Zhou3 Yi Zhang
Yi Zhang
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
CASE REPORT article
Front. Med. , 13 January 2025
Sec. Infectious Diseases: Pathogenesis and Therapy
Volume 11 - 2024 | https://doi.org/10.3389/fmed.2024.1532282
Aspergillus fumigatus spondylitis is a rare fungal infection, primarily occurring in immunocompromised patients, although cases in immunocompetent individuals have also been reported. While Aspergillus fumigatus is commonly associated with pulmonary infections, it can also cause spondylitis. Patients typically present with back pain, limb numbness, and neurological compression symptoms. Imaging findings often show vertebral destruction, reduced disk height, and paraspinal abscesses, potentially accompanied by characteristic ring-enhancing lesions. MRI findings can help distinguish Aspergillus fumigatus spondylitis from other conditions such as tuberculous spondylitis. This case involves an immunocompetent patient with Aspergillus fumigatus spondylitis, whose non-specific clinical manifestations can easily be confused with other types of spinal infections, leading to a potential misdiagnosis. Diagnosis requires tissue biopsy and microbiological culture. Voriconazole is the first-line antifungal agent, and studies have shown that it improves patient response and survival rates. For patients with significant spinal compression or neurological symptoms, surgical intervention combined with antifungal treatment should be considered if antifungal therapy alone is ineffective. Although Aspergillus fumigatus spondylitis is rare, it can occur in immunocompetent individuals. Early diagnosis through imaging and biopsy is crucial, and a combination of surgery and antifungal therapy can help improve prognosis.
Aspergillus fumigatus is a common opportunistic fungus typically associated with immunocompromised patients. However, spinal infections (Aspergillus fumigatus spondylitis) in immunocompetent individuals are extremely rare, making the diagnostic and therapeutic process challenging. The pathophysiology of fungal spinal infections typically involves the inhalation of fungal spores or hematogenous dissemination leading to damage to the bone structure. Particularly in immunocompetent patients, the mechanisms by which fungi invade the spine remain unclear and may be closely related to the local immune response of the patient, the fungal colonization ability, and other host factors (1). Most case reports in the literature focus on immunocompromised patients, so the documentation of cases in immunocompetent individuals is of significant clinical importance. Recent studies have reported several cases of Aspergillus spondylitis, with imaging findings showing high-signal annular changes around the intervertebral disks, underscoring the importance of early radiological evaluation (2, 3). This case report further demonstrates the rarity of the disease in immunocompetent patients.
A 63-year-old male patient presented with over a month of lower back pain, which gradually progressed to bilateral lower limb pain and numbness. On clinical examination, the patient exhibited restricted lumbar spine mobility with tenderness on palpation of the paraspinal muscles from T12 to L3. Neurological examination revealed no abnormalities. Laboratory findings showed a WBC count of 5.01 × 10^9/L, CRP of 33 mg/L, ESR of 57 mm/hr, PCT of 0.03 ng/mL, and ferritin levels of 442.8 μg/L (Table 1). Tests for tuberculosis, including sputum culture and T-SPOT, were negative, as was screening for HIV.
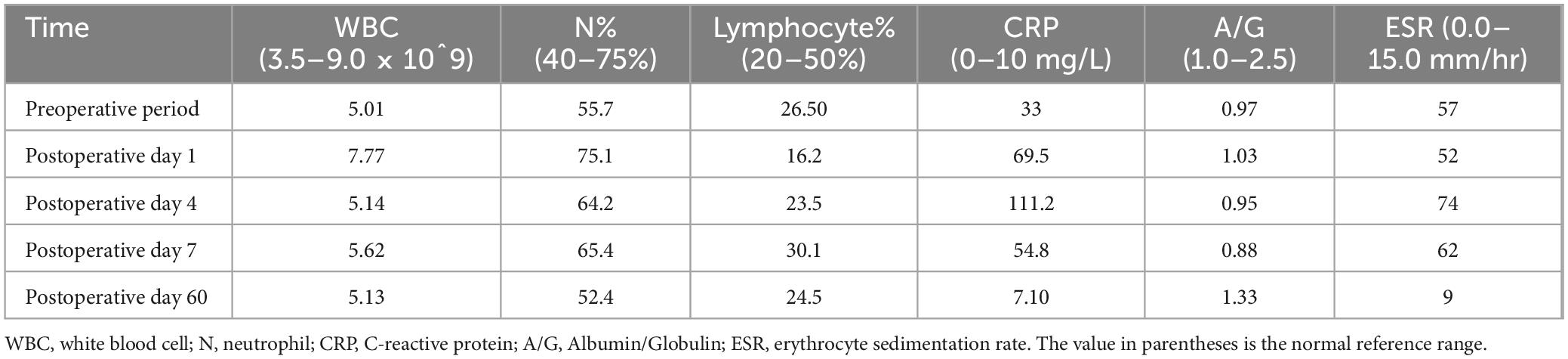
Table 1. Laboratory test values at different stages of the patient.
Initial lumbar spine plain radiography performed at an external facility revealed narrowing of the T12-L1 intervertebral space and bony destruction along the adjacent vertebral margins. T1-weighted MRI sequences demonstrated localized low-signal intensity at T12-L1, with poorly visualized intervertebral disks and vertebral margins, alongside a localized defect at the upper margin of the L5 vertebral body. Fluid-sensitive sequences revealed diffuse high-signal intensity at T12-L1, reduced intervertebral disk height, preserved disk morphology, and a localized defect at the superior margin of L5. CT imaging confirmed narrowing of the T12-L1 intervertebral space, irregularities along the vertebral margins, multiple patchy hypodense foci, circumferential thickening of the paravertebral soft tissues, and hypodense lesions at the anterior-superior margin of L5 (Figure 1).

Figure 1. (A) Shows fluid sequence images. (B) Shows the postoperative plain film. (C) Shows the postoperative histopathological examination of the vertebral body and intervertebral disk. Necrosis and granulation tissue formation with inflammatory cell infiltration were seen in the diseased intervertebral disk and adjacent vertebral tissues.
The 63-year-old male patient presents with chronic lower back pain and bilateral lower limb symptoms. From an immunological standpoint, the patient’s white blood cell count (5.01 × 10^9/L) is within normal range, and procalcitonin (PCT) is low (0.03 ng/mL), indicating no acute bacterial infection. However, elevated C-reactive protein (CRP, 33 mg/L), erythrocyte sedimentation rate (ESR, 57 mm/hr), and ferritin (442.8 μg/L) suggest persistent systemic inflammation, possibly linked to chronic infection or immune dysfunction. Tuberculosis and HIV screening results were negative, ruling out major immunosuppressive conditions. Although immune cell counts are normal, the elevated inflammatory markers and clinical presentation raise concerns about potential immune dysfunction, which may affect the patient’s response to infections, including fungal infections. Based on the immune and laboratory results, while no clear immunodeficiency is evident, the patient’s chronic inflammatory response requires attention, as such patients may present with different clinical manifestations and treatment responses when faced with fungal infections.
After obtaining the patient’s informed consent, a CT-guided posterior percutaneous vertebral biopsy was performed to further investigate the underlying cause (see Supplementary File 1). The biopsy samples were subjected to bacterial culture and drug sensitivity testing, which yielded negative results. Based on these findings, the patient was subsequently started on empirical antibiotic therapy, including ceftriaxone 2 g twice daily (BID) and cefoperazone sodium 3 g once daily (QD). However, the patient’s back pain and neurological symptoms did not show significant improvement. Imaging studies revealed high-signal annular changes around the intervertebral disks. Considering the clinical presentation, we continued to favor a diagnosis of fungal spondylitis. To promptly and effectively relieve the patient’s symptoms and improve their condition, the patient underwent posterior lumbar lesion excision, autologous iliac bone grafting, and pedicle screw fixation, after obtaining full informed consent, to restore spinal stability and clear the lesion (see Figure 1). Postoperative fungal tissue culture and Next-Generation Sequencing (NGS) identified Aspergillus fumigatus, while Mycobacterium tuberculosis cultures were negative. Consequently, the treatment regimen was switched to Voriconazole. The initial dose was 400 mg IV for 3 days, followed by 200 mg IV every 12 h for 5 days, after which the patient transitioned to 200 mg orally twice daily. A 1-month course of outpatient antifungal therapy was recommended. Despite treatment, the patient returned 2 months later with persistent low back pain. Follow-up lumbar spine MRI revealed post-T11-L2 internal fixation changes, with abnormal morphology of the L4-L5 vertebrae, showing patchy long T1 and T2 signals in the vertebral bodies and faint long T1 and T2 signals in the adjacent compressed soft tissues (Figure 1). Voriconazole was reinitiated at 200 mg IV every 12 h, and the patient showed symptomatic improvement after another month of treatment, leading to discharge.
Aspergillus spondylitis clinically manifests mainly as back pain and can cause numbness and pain in the limbs and other nerve compression symptoms. Its clinical manifestations are not specific. On lumbar spine MRI, vertebral body destruction, decreased disk height, and paravertebral abscess are mostly seen, and the vertebral body is the most common site of infection (4). Furthermore, Aspergillus spondylitis shows an annular high signal around the intervertebral disks on fluid sequences (Figure 1), which may be a more specific imaging feature of Aspergillus spondylitis. This sign is specific in infectious spondylitis, where pyogenic spondylitis tends to show intervertebral disk destruction with diffuse high signal in the vertebral body on the fluid sequences, and tuberculous spondylitis tends to show small intrabody abscesses, sublimated diffusion of the vertebral body in the anterior part of the vertebral body, and gross destruction of the vertebral body (4). Unfortunately, this sign has not been specifically reported in previous reports, but similar signs have been observed (5–7). However, paravertebral abscesses involving multiple vertebrae in a row can be easily confused with tuberculous spondylitis, making the diagnosis challenging (5–7). At the same time, this sign warrants a large-scale search for cases for a controlled clinical study, intending to differentiate it from tuberculosis better and increase clinicians’ attention to Aspergillus infections. Although the probability of Aspergillus spondylitis occurring in immunocompetent individuals is extremely low, an annular high signal around the intervertebral disks on fluid sequences should be a cause for concern and supplemented with antibiotic therapy to further the diagnosis. Early diagnosis can help to alleviate the patient’s pain and reduce the symptoms of nerve compression to improve the long-term prognosis (4).
The most reliable diagnostic methods for Aspergillus spondylitis are histopathologic examination and tissue bacterial culture (8). When inflammatory indicators and imaging tests suggest Aspergillus spondylitis, puncture biopsy with empirical antibiotic therapy should be performed as early as possible. In addition, blood cultures should be actively performed, and although the positive rate of blood cultures is low, the positive results can still guide the choice of antibiotics. According to the latest guidelines for managing Aspergillus, Voriconazole is recommended as the optimal treatment for Aspergillus spondylitis (9). The study showed that using Voriconazole in patients with invasive Aspergillus infection was associated with better response and survival, leading to less serious side effects (10, 11). Conservative antifungal therapy is ineffective when there is epidural abscess formation at the site of spinal infection, spinal cord compression, spinal instability, and the onset of neurologic symptoms. At this point, surgical combination antifungal therapy should be considered.
However, despite these advances in treatment, there remains a significant gap in the literature regarding the optimal management strategies for Aspergillus spondylitis, particularly in immunocompetent patients (Table 2). Further investigation into the role of combined surgical and antifungal therapy in cases with spinal cord compression or epidural abscesses is urgently needed. Moreover, while the pathogenesis of Aspergillus spondylitis is still not fully understood, it is likely that the infection may arise from either direct inoculation following trauma or hematogenous spread from distant sites of infection (3). This suggests that Aspergillus species may exploit specific host vulnerabilities, such as impaired immune responses, making it critical to identify common risk factors such as diabetes, malignancy, or recent surgical interventions, which may predispose individuals to fungal infections.
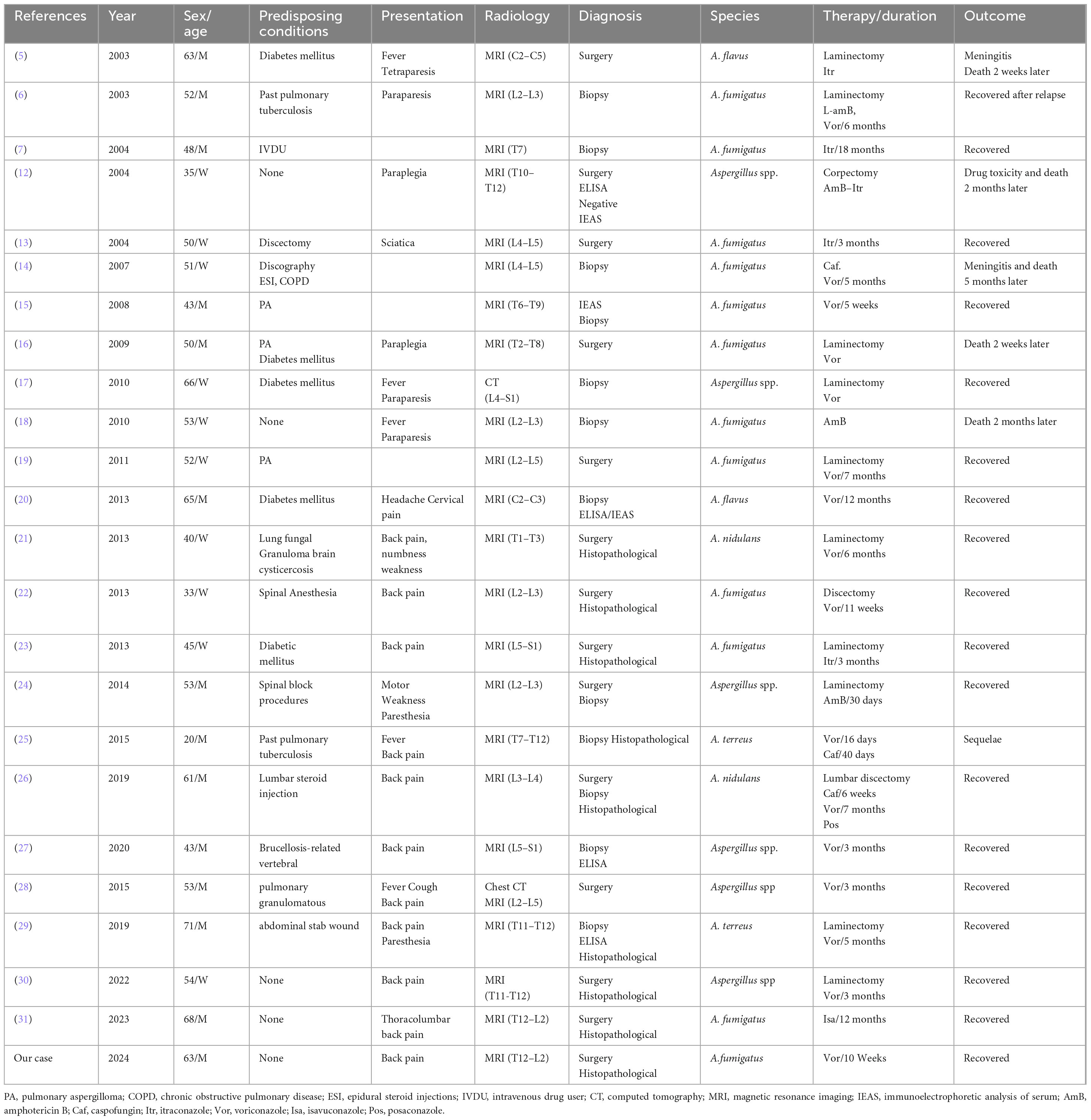
Table 2. Clinical characteristics of Aspergillus spondylitis (AS) in immunocompetent (IC) patients.
In conclusion, reporting cases of Aspergillus spondylitis is of paramount importance to raise awareness among clinicians, particularly in atypical cases or those involving immunocompetent patients. The case we present highlights the need for further research into the pathogenesis, diagnostic markers, and treatment strategies for Aspergillus spondylitis. Establishing more robust clinical guidelines will improve early recognition, treatment outcomes, and overall prognosis for patients affected by this rare but serious infection.
Aspergillus fumigatus spondylitis also needs to be considered as a possibility of mycobacterial spondylitis in the presence of normal immune function and a history of no risk factors, and prompt diagnosis and treatment can help improve the patient’s prognosis.
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found in this article/Supplementary material.
The studies involving humans were approved by the Ethics Committee of Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
ZX: Data curation, Writing – original draft. WZ: Data curation, Writing – original draft. SZ: Data curation, Writing – review and editing. YZ: Data curation, Resources, Writing – review and editing. QX: Data curation, Writing – review and editing. YiZ: Data curation, Resources, Supervision, Writing – original draft.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
YZ employed by KadWise Co.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors declare that no Generative AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2024.1532282/full#supplementary-material
1. Koutserimpas C, Chamakioti I, Raptis K, Alpantaki K, Vrioni GA-O, Samonis G. Osseous infections caused by Aspergillus species. Diagnostics (Basel). (2022) 12:201. doi: 10.3390/Diagnostics12010201
2. Dai G, Wang T, Yin C, Sun Y, Xu D, Wang Z, et al. Aspergillus spondylitis: Case series and literature review. BMC Musculoskelet Disord. (2020) 21:572. doi: 10.1186/s12891-020-03582-x
3. Koutserimpas C, Chamakioti I, Naoum S, Raptis K, Alpantaki K, Kofteridis DP, et al. Spondylodiscitis caused by Aspergillus species. Diagnostics (Basel) (2021) 11:1899. doi: 10.3390/Diagnostics11101899
4. Zhu W, Zhou S, Zhang J, Li L, Liu P, Xiong W. Differentiation of native vertebral osteomyelitis: A comprehensive review of imaging techniques and future applications. Med Sci Monit (2024) 30:e943168. doi: 10.12659/msm.943168
5. Chi CY, Fung CP, Liu CY. Aspergillus flavus epidural abscess and osteomyelitis in a diabetic patient. J Microbiol Immunol Infect. (2003) 36:145–8.
6. Stratov I, Korman TM, Johnson PD. Management of Aspergillus osteomyelitis: Report of failure of liposomal amphotericin B and response to voriconazole in an immunocompetent host and literature review. Eur J Clin Microbiol Infect Dis. (2003) 22:277–83. doi: 10.1007/s10096-003-0909-3
7. Salloum A, Rao S, Havasi A, Miljkovic G, Amoateng-Adjepong Y. Aspergillus Rib and vertebral osteomyelitis in a former intravenous drug user. Am J Med. (2004) 116:208–9. doi: 10.1016/j.amjmed.2003.05.006
8. Wu CJ, Liu WL, Lai CC, Chao CM, Ko WC, Wang HC, et al. Multicenter study of azole-resistant Aspergillus fumigatus clinical isolates, Taiwan. Emerg Infect Dis. (2020) 26:804–6. doi: 10.3201/eid2604.190840
9. Patterson TF, Thompson GR III, Denning DW, Fishman JA, Hadley S, Herbrecht R, et al. Practice guidelines for the diagnosis and management of aspergillosis: 2016 update by the infectious diseases society of America. Clin Infect Dis. (2016) 63:e1–60. doi: 10.1093/cid/ciw326
10. Herbrecht R, Patterson TF, Slavin MA, Marchetti O, Maertens J, Johnson EM, et al. Application of the 2008 definitions for invasive fungal diseases to the trial comparing voriconazole versus amphotericin B for therapy of invasive aspergillosis: A collaborative study of the mycoses study group (Msg 05) and the European Organization for Research and Treatment of Cancer Infectious Diseases Group. Clin Infect Dis. (2015) 60:713–20. doi: 10.1093/cid/ciu911
11. Herbrecht R, Denning DW, Patterson TF, Bennett JE, Greene RE, Oestmann JW, et al. Voriconazole versus amphotericin B for primary therapy of invasive aspergillosis. N Engl J Med. (2002) 347:408–15. doi: 10.1056/NEJMoa020191
12. Vaishya S, Sharma MS. Spinal Aspergillus vertebral osteomyelitis with extradural abscess: Case report and review of literature. Surg Neurol. (2004) 61:551–5; discussion 5. doi: 10.1016/j.surneu.2003.06.005
13. Lenzi J, Agrillo A, Santoro A, Marotta N, Cantore GP. Postoperative spondylodiscitis from Aspergillus fumigatus in immunocompetent subjects. J Neurosurg Sci. (2004) 48:81–5; discussion 5.
14. Kolbe AB, McKinney AM, Kendi AT, Misselt D. Aspergillus meningitis and discitis from low-back procedures in an immunocompetent patient. Acta Radiol (Stockholm, Sweden : 1987). (2007) 48:687–9. doi: 10.1080/02841850701342153
15. Domergue V, Orlandini V, Begueret H, Couprie B, Huerre M, Tunon de Lara M, et al. [Cutaneous, pulmonary and bone aspergillosis in a patient presumed immunocompetent presenting subacute cutaneous lupus erythematosus]. Ann Dermatol Venereol. (2008) 135:217–21. doi: 10.1016/j.annder.2007.04.009
16. Tew CW, Han FC, Jureen R, Tey BH. Aspergillus vertebral osteomyelitis and epidural abscess. Singapore Med J. (2009) 50:e151–4.
17. B NN, Kini U, Alexander B. Vertebral osteomyelitis with a rare etiology diagnosed by fine-needle aspiration cytology. Diagn Cytopathol. (2010) 38:360–3. doi: 10.1002/dc.21212
18. Ranjan R, Mishra S, Ranjan S. Aspergillus vertebral osteomyelitis in an immunocompetent person. Neurol India. (2010) 58:806–8. doi: 10.4103/0028-3886.72196
19. Studemeister A, Stevens DA. Aspergillus vertebral osteomyelitis in immunocompetent hosts: Role of triazole antifungal therapy. Clin Infect Dis. (2011) 52:e1–6. doi: 10.1093/cid/ciq039
20. Nicolle A, de la Blanchardière A, Bonhomme J, Hamon M, Leclercq R, Hitier M. Aspergillus vertebral osteomyelitis in immunocompetent subjects: Case report and review of the literature. Infection. (2013) 41:833–40. doi: 10.1007/s15010-013-0463-6
21. Jiang Z, Wang Y, Jiang Y, Xu Y, Meng B. Vertebral osteomyelitis and epidural abscess due to aspergillusnidulans resulting in spinal cord compression: Case report and literature review. J Int Med Res. (2013) 41:502–10. doi: 10.1177/0300060513476432
22. Shashidhar N, Tripathy SK, Balasubramanian S, Dhanakodi N, Venkataramaiah S. Aspergillus spondylodiscitis in an immunocompetent patient following spinal anesthesia. Orthopaedic Surg. (2014) 6:72–7. doi: 10.1111/os.12091
23. Raj KA, Srinivasamurthy BC, Nagarajan K, Sinduja MG. A rare case of spontaneous aspergillusspondylodiscitis with epidural abscess in a 45-year-old immunocompetent female. J Cranioverteb Junct Spine. (2013) 4:82–4. doi: 10.4103/0974-8237.128538
24. Yoon KW, Kim YJ. Lumbar Aspergillus osteomyelitis mimicking pyogenic osteomyelitis in an immunocompetent adult. Br J Neurosurg. (2015) 29:277–9. doi: 10.3109/02688697.2014.957648
25. Comacle P, Le Govic Y, Hoche-Delchet C, Sandrini J, Aguilar C, Bouyer B, et al. Spondylodiscitis due to aspergillusterreus in an immunocompetent host: Case report and literature review. Mycopathologia. (2016) 181:575–81. doi: 10.1007/s11046-016-0007-6
26. Lyons MK, Neal MT, Patel NP, Vikram HR. Progressive back pain due to Aspergillus Nidulans vertebral osteomyelitis in an immunocompetent patient: Surgical and antifungal management. Case Rep Orthopedics. (2019) 2019:4268468. doi: 10.1155/2019/4268468
27. Aydın Ö, Bektaş B, Aslan A, Yıldırım AN, Arslan F. Voriconazole-treated aspergillusvertebral osteomyelitis in an immunocompetent patient. J Orthopaedic Sci. (2023) 28:710–2. doi: 10.1016/j.jos.2020.09.003
28. Li Y, Cen Y, Luo Y, Zhu Z, Min S, Chen X. Aspergillus vertebral osteomyelitis complicating pulmonary granuloma in an immunocompetent adult. Med Principles Pract. (2016) 25:394–6. doi: 10.1159/000443310
29. Takagi Y, Yamada H, Ebara H, Hayashi H, Kidani S, Okamoto S, et al. AspergillusTerreus spondylodiscitis following an abdominal stab wound: A case report. J Med Case Rep. (2019) 13:172. doi: 10.1186/s13256-019-2109-5
30. Rashid MH, Hossain MN, Ahmed N, Kazi R, Ferini G, Palmisciano P, et al. Aspergillus spinal epidural abscess: A case report and review of the literature. J Cranioverteb Junct Spine. (2022) 13:204–11. doi: 10.4103/jcvjs.jcvjs_35_22
Keywords: Aspergillus fumigatus, Aspergillus, infectious spondylitis, immunocompetent, clinical features
Citation: Xu Z, Zhu W, Zhou S, Zhao Y, Xiang Q and Zhang Y (2025) Aspergillus fumigatus spondylitis in an immunocompetent patient with annular high signal around the intervertebral disks: a case report and literature review. Front. Med. 11:1532282. doi: 10.3389/fmed.2024.1532282
Received: 26 November 2024; Accepted: 24 December 2024;
Published: 13 January 2025.
Edited by:
Sam Donta, Falmouth Hospital, United StatesReviewed by:
Christos Koutserimpas, Hôpital de la Croix-Rousse, FranceCopyright © 2025 Xu, Zhu, Zhou, Zhao, Xiang and Zhang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yi Zhang, MTc2NzExMTQ1NDdAMTYzLmNvbQ==
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.