 Mateusz Szczupak1
Mateusz Szczupak1 Jacek Kobak2*Anna Wiśniewska3
Jacek Kobak2*Anna Wiśniewska3 Justyna Kosydar-Bochenek4Arkadiusz Jamro5
Justyna Kosydar-Bochenek4Arkadiusz Jamro5 Sabina Krupa-Nurcek6
Sabina Krupa-Nurcek6- 1Department of Anesthesiology and Intensive Care, Copernicus Hospital, Gdańsk, Poland
- 2Department of Otolaryngology, Faculty of Medicine, Medical University of Gdańsk, Gdańsk, Poland
- 3Department of Neurology, Copernicus Hospital, Gdańsk, Poland
- 4Institute of Health Sciences, College of Medical Sciences of the University of Rzeszow, Rzeszów, Poland
- 5Student at Institute of Medical Sciences, Medical College of Rzeszów University, Rzeszów, Poland
- 6Department of Surgery, Institute of Medical Sciences, Medical College of Rzeszów University, Rzeszów, Poland
Opsoclonus-myoclonus syndrome (OMS) is a rare neurological inflammatory disease of paraneoplastic, parainfectious or idiopathic origin. It is manifested by the occurrence of opsoclonus, myoclonus, ataxia, as well as behavioral and sleep disorders. The incidence is estimated at 1/5,000,000 people. This syndrome is usually immune-mediated and may be the first manifestation of cancer as a paraneoplastic syndrome, most often occurring in the course of breast, ovarian or lung cancer. Here we show a case of a 20-year-old woman with symptomatic opsoclonus-myoclonus syndrome in the course of teratoma. A brief review of the literature was conducted to determine the diagnostic route and treatment of this rare condition. As a result, it has been shown that the only method of treatment for OMS syndrome is the removal of the neoplastic lesion.
Highlights
• In the available literature, no other way of treating OMS syndrome has been found other than surgical treatment of tumor removal.
• Untreated OMS can cause sleep and behavioral disorders, which in turn can contribute to the development of complications from the nervous system and the need for treatment in a psychiatric clinic.
Introduction
Opsoclonus-myoclonus syndrome (OMS) is a rare set of disease symptoms, usually immune-mediated, whose symptomatology consists of: opsoclonus (rapid, multidirectional, combined eye movements), myoclonus (sudden jerking movements involving the axial and limb muscles), ataxia (limb and axial of varying severity), sleep disturbances, irritability and other behavioral changes (1, 2). This syndrome was first described in the literature by the Austrian pediatric neurologist and neurobiologist Marcel Kinsobourn in 1962. In his work entitled “Myoclonic encephalopathy of infants,” he presented six cases of children aged 6–20 months who developed myoclonus generating ataxia and opsocloni (3). According to the literature, the term opsocloni was first introduced into medical nomenclature in 1913 by the Polish neurologist Professor Kazimierz Orzechowski (4). In 1927, the researcher linked opsocloni to myoclonus (1, 5). In the same year, American scientists Harvey Cushing and Simeon Wolbach described the relationship between opsocloni and myocloni and fetal sympathetic neuroma in children (6).
The aim of this publication was to present the case of a 20-year-old woman who was admitted to the neurology department due to rapid, multidirectional and combined eye movement accompanied by myoclonus and irritability. The symptoms appeared suddenly, and the diagnostic procedure during the stay in the hospital emergency department did not allow to determine their cause. This prompted the team of doctors caring for the patient to be admitted and further diagnosed as part of the neurology department of the Copernicus Hospital. The authors of this manuscript have reviewed the literature to determine the management and treatment of a patient with this syndrome.
Materials and methods
In order to write this manuscript, the articles available in the PubMed, Google Scholar and Mendeley search engines were reviewed. Keywords such as opsoclonus-myoclonus syndrome, teratoma, ataxia, and multidirectional nystagmus were used. Out of 45 review articles and articles presenting OMS cases found and analyzed, those were selected which, in the opinion of the authors, referred to the subject of this manuscript and constituted a valuable source of information. Those that duplicated the pathophysiology of opsoclonus-myoclonus syndrome or referred to diseases that were not directly related to the topic were excluded from the discussion. The article cites 28 publications and scientific reports. The case of a 20-year-old female patient who was hospitalized due to symptoms in the Department of Neurology of the Copernicus Hospital, Nicolaus Copernicus Hospital in Gdańsk was also presented.
Pathophysiology and symptomatology of opsoclonus-myoclonus syndrome
In adults, after excluding structural causes, the most common etiology (60% of cases) of opsoclonus-myoclonus syndrome (OMS) are neoplastic diseases (lung cancer, breast cancer, ovarian teratoma, kidney cell cancers or pancreatic malignant tumors) (7).
The etiopathogenesis of opsoclonus in OMS has still not been clearly understood (6). There are two hypotheses for the development of this syndrome. The first one is associated with the development of opsoclonus with dysinhibition (disinhibition) of the apical nucleus of the cerebellum. Under normal conditions, the nucleus of the cerebellar apex is inhibited by the dorsal part of the cerebellar vermis – in the case of disorders of the inhibition process, it is disinhibited. This theory is confirmed by functional neuroimaging studies. Single photon emission-computed tomography (SPECT) showed dysfunction of the dorsal part of the cerebellar verm, and functional magnetic resonance imaging (fMR) showed excessive bilateral activation of the cerebellar vertex nuclei (1, 8–10).
The second concept of OMS development is associated with immunological determinants and has a paraneoplastic or idiopathic basis. Paraneoplastic etiology occurs at the age of 60–70 years and is usually associated with small cell lung cancer, breast adenoma or ovarian cancer (7, 10–12). In some patients, antibodies against nerve cell surface antigens and neurofilament antigens can be identified (13, 14). As a result of the humoral response, oncogenic antibodies are produced – anti-Ri, -Hu, -Yo, −Ma1, −Ma2, -Ta, -CRMP-5, -CV2, antiamiphysin and neurofilaments. Their presence confirms the paraneoplastic basis of the disease, although the absence does not exclude this cause (1, 2, 7, 10, 11, 15, 16). In the majority of patients with paraneoplastic OMS, the presence of onconeuronal antibodies is not found (1, 11). The exception to this rule are women with OMS and breast or ovarian cancer, who have anti-Ri antibodies directed against the Nova protein, which regulates the function of other proteins involved in synaptic transport in the central nervous system (12, 17).
The idiopathic form of OMS usually affects people aged 30–40 years, and its occurrence is rarely preceded by infection or vaccination (1, 7, 18–20). The humoral immune response is directed against synaptic autoantigens or surface nerve cells, which explains the neuronal dysphyction present in idiopathic OMS (12). This theory is confirmed by Bataller et al., who identified postsynaptic autoantigens such as the bound protein complex in OMS patients. NMDA receptor (16). Similar conclusions were reached by Blaes et al., who discovered antibodies in patients with OMS that bind to the surface of neurons of the granular layer of the cerebellar cortex (21).
Opsoclonus-myoclonus syndrome is sometimes a manifestation of periinfectious encephatomyelitis of bacterial etiology (Borrelia burgdorferi, Mycoplasma pneumoniae) or viral etiology (enteroviruses, Ebstein-Barr virus, cytomegalovirus, West Nile, HIV) (7, 11, 22–25).
In the literature, there are also reports referring to the development of opsoclonus-myoclonus syndrome in the course of diabetic coma, celiac disease, pregnancy, allogeneic bone marrow transplantation, poisoning, drugs such as lithium or amitriptyline, psychoactive substances such as cocaine or toxic compounds such as strychnine or thallium. Sometimes OMS can be a portal effect of craniocerebral trauma, vascular diseases, demyelization diseases or cancers of the central nervous system (10, 11, 22, 23, 26).
In almost 30% of cases, the development of opsoclonus-myoclonus syndrome in adults is preceded by the appearance of parainfluenza symptoms. The most common of these include: non-systemic dizziness, balance disorders, nausea and/or vomiting or visual disturbances (6, 11).
In most cases, both opsoclonus and myoclonus are observed from the beginning of the syndrome. Opsocloni can be observed during eye fixation, smooth tracking or convergent eye movementscg. They are also present when the eyelids are closed and during sleep. They require differentiation from “eye flutter” and nystagmus (6). Myoclonus, on the other hand, are sudden arrhythmic, multifocal contractions of the muscles of the limbs, less often of the head, neck or trunk. Myoclonus can occur in certain positions – positional myoclonus or be provoked by movement – kinetic myoclonus. They are most often intensified under the influence of external stimuli and emotional reactions (1, 2, 6, 11). The development of trunk ataxia in the course of OMS, which is a symptom of cerebellar syndrome, is sometimes associated with the development of limb ataxia and dysartia. Both ataxia and myoclonus in about half of patients lead to disability within a month as a result of gait disorders, falls, difficulties in standing and sometimes also sitting (1, 2, 6, 11). Behavioral disorders as a result of encephalopathy associated with opsoclonus-myoclonus syndrome may manifest as confusion, attention deficit, emotional lability or mood disorders (1, 6, 11).
Case presentation
A 20-year-old woman was admitted to the Department of Neurology at the Copernicus Hospital due to increasing balance disorders, inability to walk, dizziness with a feeling of spinning of the environment, a sensation of “jumping” image and difficulty fixing her eyes. In addition, nausea and vomiting occurred. The appearance of symptoms was preceded by severe headache located in the frontal area, with their increasing intensity 3 days before hospitalization. The other neurological symptoms gradually worsened, leading to significant balance difficulties and gait disorders, with maximum intensity on the day before hospital admission. Medical history: patient with polycystic ovary syndrome, insulin resistance, obesity with Body Mass Index 42.4 (BMI 42.4), hypothyroidism, after stabilization surgery and Th4-L1 spondylodesis due to idiopathic juvenile scoliosis in 2016, without a history of previous neurological or psychiatric diseases. Neurological examination at admission to the ward was dominated by severe oculomotor disorders in the form of chaotic, irregular eye movements, intensifying when trying to fix the gaze. In addition, features of the cerebellar syndrome were observed in the form of upper limb dysmetria, trunk ataxia, unsteadiness in the Romberg test, and gait on a wide base. Other symptoms included resting tremor of the limbs and trunk, involuntary movements of the limbs and trunk in the form of myoclonus, and right-sided pyramidal symptoms. To determine the cause of these symptoms, a number of diagnostic tests were carried out. Magnetic resonance imaging of the head described a non-specific small high-signal focus in the cortex of the lower part of the left cerebellar hemisphere. The electroencephalographic (EEG) recording was abnormal – the presence of single sharp wave discharges was found in the frontotemporal and temporal leads, mainly the left ones. In addition, numerous artifacts from eye movement were noted in the frontal leads. The results of laboratory tests were within the reference levels of. No abnormalities were observed in the general examination of cerebrospinal fluid (Table 1). The level of anti-IgM and anti-IgG antibodies to Borrelia burgdorferii in serum and cerebrospinal fluid was negative. Similarly negative was the PCR panel for 14 neuronal infection pathogens (cytomegalovirus, enterovirus, herpes simplex virus type 1, herpes simplex virus type 2, human herpesvirus type 6, human parechovirus, varicella zoster and herpes zoster virus, Escherichia coli K1, Hemophilus influenzae, Listeria monocytogenes, Neisseria meningitidis, Streptococcus agalactiaem Streptococcus pneumoniae, Cryptococcus neoformans/GATTII) and the level of antibodies for atypical encephalitis.
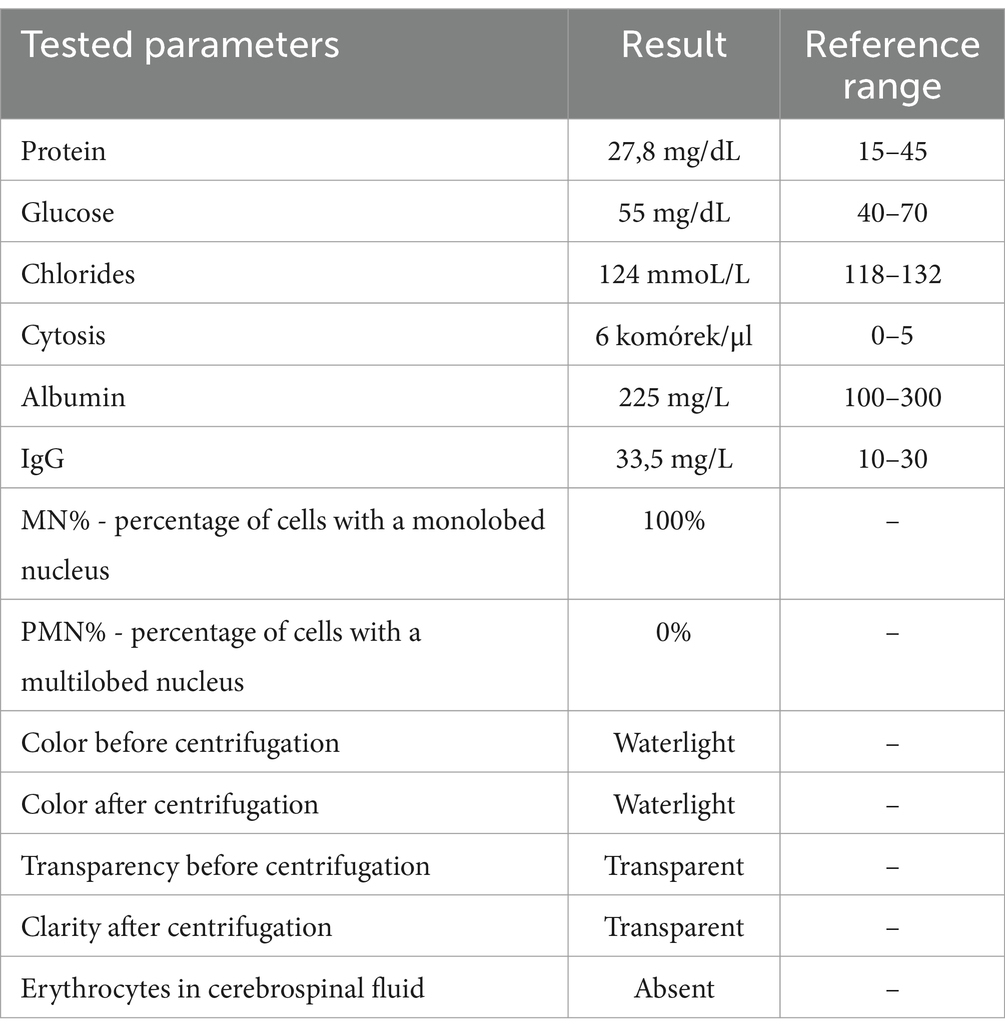
Table 1. Result of the general cerebrospinal fluid examination.
In the course of further diagnostics, computed tomography (CT) of the chest, abdominal cavity and small pelvis was performed, in which a well-demarcated mass in the left ovary measuring 56x77x66 mm suggestive of a teratoma was described from the pathological changes (Figure 1). Transvaginal ultrasonography was performed, which confirmed the presence of a lesion with an ultrasound appearance typical of a teratoma.

Figure 1. Computed tomography of the chest, abdomen and small pelvis with marked pathological mass of the left ovary.
Due to the overall clinical picture suggesting the development of opsoclonus-myoclonus syndrome in the course of teratoma, the team caring for the patient additionally performed immunoblot tests for the presence of onconeuronal and antineuronal antibodies and the ROMA test – negative results were obtained. During hospitalization, after collecting biological material, including blood tests and antibody testing, steroid therapy was administered in the form of an intravenous infusion of methylprednisolone at a total dose of 5.0 grams, followed by prednisone 60 mg once daily for 14 days with a target dose reduction of 5 mg every 5 days. In addition, antiepileptic treatment with levetiracetam was prescribed at a dose of 500 mg twice a day. In response to the identified ovarian mass, the patient was consulted with a gynecologist, and then, in accordance with the planned treatment, underwent laparascopic removal of the teratoma. Histopathological analysis confirmed the presence of a mature teratoma. After surgery, corticosteroids and intravenous immunoglobulins (IVIG) were continued to treat opsoclonus-myoclonus syndrome. After the therapy, a significant improvement in the patient’s condition was observed. The symptoms of opsoclonus and myoclonus were alleviated, cerebellar disorders were significantly reduced, and the patient’s fitness and clinical condition improved. This case highlights the importance of early diagnosis and intervention in opsoclonus-myoclonus syndrome, especially when it occurs in the context of a malignancy such as ovarian teratoma. Prompt diagnosis and treatment can lead to favorable clinical outcomes and significant improvements in patients’ quality of life.
The patient described underwent surgical removal of the tumor following their diagnosis. In the days after the surgery, we observed a gradual clinical improvement and resolution of the OMS symptoms. Currently, the patient remains under continuous medical care and is asymptomatic.
Discussion
Opsoclonus-myoclonus syndrome (OMS) is a rare but complex neurological condition that can occur in both children and adults. This manuscript analyzes a variety of etiologies of OMS, including cancer, infective, and autoimmune causes. The results of the study support the literature that OMS often accompanies cancers such as ovarian teratoma, which has been extensively reported in the study by Battaller et al., where links between OMS and cancer have been identified, and by Miraclin et al., who have highlighted the complexity of cases involving teraatoms and NMDAR antibodies (7, 22). As in the work of Kinsbourne and Pohl et al., our study reveals that OMS, although less common in adults, tends to occur late in life, which often leads to delays in diagnosis and treatment (3, 5). Kranick et al. emphasize that the symptoms of OMS can be varied and ambiguous, which can cause difficulties in diagnosis and lead to misdiagnoses (26). It is also worth noting that the analysis of antibodies directed against neuronal surface antigens provides valuable information on the pathogenesis of OMS. The results of our observations are consistent with the findings of Sabater et al. and Armangué et al., who showed that the presence of these antibodies may be associated with immune-determined cases of OMS. Faster identification of these markers could lead to better diagnosis and more effective treatment of patients (13, 14).
Table 2 presents additional cases of OMS reported in the literature. The comparative characteristics included gender, age at diagnosis, methods of diagnosis, presence and types of identified antibodies, predominant symptoms, clinical diagnoses leading to OMS and treatments used.
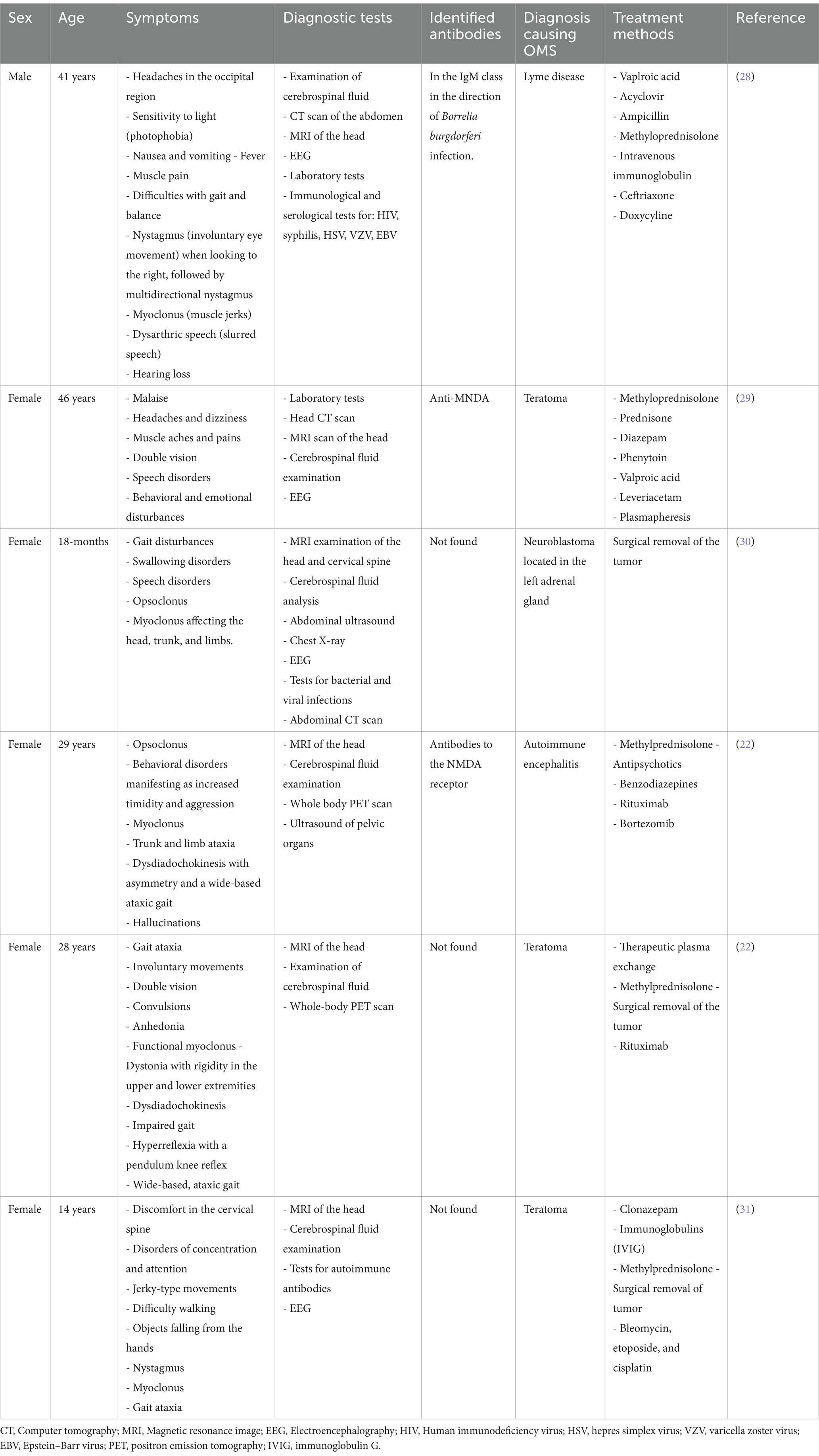
Table 2. A selection of documented cases of Ospoclone-myoclonus syndrome found in the literature, along with their specific characteristics.
Conclusion
Although opsoclonus-myoclonus syndrome is a rare disease, it requires appropriate and applied treatment aimed at the etiology. In idiopathic and paraneoplastic cases, treatment and its results are relatively difficult to evaluate and compare. This is due to the high variability of the drugs used, as well as the number of patients. Currently, commonly used therapeutic options include: corticosteroid therapy, intravenous immunoglobulin administration and plasmapheresis (11). Patients with parainfectious OMS have a favorable prognosis and achieve full recovery (20, 27). In the case of patients in whom the etiological factor of the syndrome is tumors, treatment is based on resection of the lesion, which contributes to the improvement of the patient’s clinical condition. Our report highlights the need for prospective studies to better understand the pathogenesis of OMS and to identify potential biomarkers. Understanding the molecular mechanisms underlying OMS could lead to the development of new therapeutic strategies. Proper management of patients with OMS requires collaboration between neurologists, oncologists, surgeons, and immunologists. A multidisciplinary approach is essential to optimize the diagnosis, treatment and monitoring of patients with this rare condition. Increasing awareness of OMS among professionals is key to enabling faster and accurate diagnosis. Education and training materials can help identify the symptoms of OMS and refer patients to appropriate specialists. Patients with OMS should undergo long-term monitoring to assess neurological complications and the effectiveness of therapy. Regular check-ups and psychological support can significantly improve the quality of life of these patients.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Okręgowa Izba Lekarska KB – 6/24. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin because this was retrospective research - case study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
MS: Formal analysis, Resources, Writing – original draft, Conceptualization, Methodology. JK: Conceptualization, Formal analysis, Methodology, Writing – original draft. AW: Conceptualization, Formal analysis, Methodology, Writing – original draft. JK-B: Formal analysis, Writing – original draft, Supervision. AJ: Writing – original draft, Methodology. SK-N: Formal analysis, Supervision, Writing – original draft, Resources.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Sahu, JK, and Prasad, K. The opsoclonus–myoclonus syndrome. Pract Neurol. (2011) 11:160–6. doi: 10.1136/practneurol-2011-000017
2. Groiss, SJ, Siebler, M, and Schnitzler, A. Full recovery of adult onset opsoclonus myoclonus syndrome after early immunotherapy: a case report. Mov Disord. (2011) 26:1805–7. doi: 10.1002/mds.23854
3. Kinsbourne, M. Myoclonic encephalopathy of infants. J Neurol Neurosurg Psychiatry. (1962) 25:271–6. doi: 10.1136/jnnp.25.3.271
4. Orzechowski, K. De 1’ataxie dysmetrique des yeux: remarques sur 1’ataxie des yeux dite myoclonique (opsoclonie, opsochorie). J Psychol Neurol. (1927) 35:1–18.
5. Pohl, KR, Pritchard, J, and Wilson, J. Neurological sequelae of the dancing eye syndrome. Eur J Pediatr. (1996) 155:237–44. doi: 10.1007/BF01953945
6. Koziorowska-Gawron, E, Koszewicz, M, Bladowska, J, Ejma, M, and Budrewicz, S. Opsoclonus-myoclonus syndrome with severe clinical course and beneficial outcome: A case report. Medicine (Baltimore) (2021) 100:e25261. doi: 10.1097/MD.0000000000025
7. Bataller, L, Graus, F, Saiz, A, and Vilchez, JJSpanish Opsoclonus-Myoclonus Study Group. Clinical outcome in adult onset idiopathic or paraneoplastic opsoclonus-myoclonus. Brain. (2001) 124:437–43. doi: 10.1093/brain/124.2.437
8. Wong, AM, Musallam, S, Tomlinson, RD, Shannon, P, and Sharpe, JA. Opsoclonus in three dimensions: oculographic, neuropathologic and modelling correlates. J Neurol Sci. (2001) 189:71–81. doi: 10.1016/s0022-510x(01)00564-0
9. Zee, DS, and Robinson, DA. A hypothetical explanation of saccadic oscillations. Ann Neurol. (1979) 5:405–14. doi: 10.1002/ana.410050502
11. Klaas, JP, Ahlskog, JE, Pittock, SJ, Matsumoto, JY, Aksamit, AJ, Bartleson, JD, et al. Adult-onset opsoclonus-myoclonus syndrome. Arch Neurol. (2012) 69:1598–607. doi: 10.1001/archneurol.2012.1173
12. Panzer, J, and Dalmau, J. Movement disorders in paraneoplastic and autoimmune disease. Curr Opin Neurol. (2011) 24:346–53. doi: 10.1097/WCO.0b013e328347b307
13. Sabater, L, Xifró, X, Saiz, A, Alberch, J, and Graus, F. Analysis of antibodies to neuronal surface antigens in adult opsoclonus-myoclonus. J Neuroimmunol. (2008) 196:188–91. doi: 10.1016/j.jneuroim.2008.03.013
14. Armangué, T, Sabater, L, Torres-Vega, E, Martínez-Hernández, E, Ariño, H, Petit-Pedrol, M, et al. Clinical and immunological features of Opsoclonus-myoclonus syndrome in the era of neuronal cell surface antibodies. JAMA Neurol. (2016) 73:417–24. doi: 10.1001/jamaneurol.2015.4607
15. Lewis, MA, Hartmann, LC, Lachance, DH, and Jimenez, RE. Opsoclonus as a suspected paraneoplastic syndrome of endometrial cancer. Rare Tumors. (2010) 2:e42:115–6. doi: 10.4081/rt.2010.e42
16. Bataller, L, Rosenfeld, MR, Graus, F, Vilchez, JJ, Cheung, NK, and Dalmau, J. Autoantigen diversity in the opsoclonus-myoclonus syndrome. Ann Neurol. (2003) 53:347–53. doi: 10.1002/ana.10462
17. Buckanovich, RJ, Yang, YY, and Darnell, RB. The onconeural antigen Nova-1 is a neuron-specific RNA-binding protein, the activity of which is inhibited by paraneoplastic antibodies. J Neurosci. (1996) 16:1114–22. doi: 10.1523/JNEUROSCI.16-03-01114.1996
18. Wong, A. An update on opsoclonus. Curr Opin Neurol. (2007) 20:25–31. doi: 10.1097/WCO.0b013e3280126b51
19. Lapenna, F, Lochi, L, de Mari, M, Iliceto, G, and Lamberti, P. Post-vaccinic opsoclonus-myoclonus syndrome: a case report. Parkinsonism Relat Disord. (2000) 6:241–2. doi: 10.1016/s1353-8020(00)00020-1
20. Dassan, P, Clarke, C, and Sharp, DJ. A case of poststreptococcal opsoclonus-myoclonus syndrome. Mov Disord. (2007) 22:1490–1. doi: 10.1002/mds.21513
21. Blaes, F, Fühlhuber, V, Korfei, M, Tschernatsch, M, Behnisch, W, Rostasy, K, et al. Surface-binding autoantibodies to cerebellar neurons in opsoclonus syndrome. Ann Neurol. (2005) 58:313–7. doi: 10.1002/ana.20539
22. Miraclin, AT, Mani, AM, Sivadasan, A, Nair, A, Christina, M, and Gojer, AR. Opsoclonus myoclonus ataxia syndrome, ovarian teratoma and anti-NMDAR antibody: an 'unresolved' mystery. BMJ Neurol Open. (2023) 5:e000414. doi: 10.1136/bmjno-2023-000414
23. Bhatia, P, Heim, J, Cornejo, P, Kane, L, Santiago, J, and Kruer, MC. Opsoclonus-myoclonus-ataxia syndrome in children. J Neurol. (2022) 269:750–757. doi: 10.1007/s00415-021-10536-3
24. Peter, L, Jung, J, Tilikete, C, Ryvlin, P, and Mauguiere, F. Opsoclonus-myoclonus as a manifestation of Lyme disease. J Neurol Neurosurg Psychiatry. (2006) 77:1090–1. doi: 10.1136/jnnp.2006.091728
25. Medrano, V, Royo-Villanova, C, Flores-Ruiz, JJ, Sempere, AP, and de Roda, SMC. Síndrome opsoclono-mioclono parainfeccioso secundario a virus varicela-zóster [Parainfectious opsoclonus-myoclonus syndrome secondary to varicella-zoster virus infection]. Rev Neurol. (2005) 41:507–8. doi: 10.33588/rn.4108.2004616
26. Kranick, SM, Mowry, EM, Colcher, A, Horn, S, and Golbe, LI. Movement disorders and pregnancy: a review of the literature. Mov Disord. (2010) 25:665–71. doi: 10.1002/mds.23071
27. Huber, BM, Strozzi, S, Steinlin, M, Aebi, C, and Fluri, S. Mycoplasma pneumoniae associated opsoclonus-myoclonus syndrome in three cases. Eur J Pediatr. (2010) 169:441–5. doi: 10.1007/s00431-009-1048-3
28. Lino, AMM, Spera, RR, de Campos, FPF, Freitas, CHA, Garcia, MRT, Lopes, LDC, et al. Adult-onset opsoclonus-myoclonus-ataxia syndrome as a manifestation of brazilian Lyme disease-like syndrome: a case report and review of literature. Autops Case Rep. (2014) 4:29–37. doi: 10.4322/acr.2014.005
29. Jasińska-Mikołajczyk, A, Osip, P, Osip-Permoda, A, and Rybakowski, F. Anti-NMDA receptor encephalitis in a patient with ovarian teratoma – case report. Adv Psychiatry Neurol. (2017) 26:246–54. doi: 10.5114/ppn.2017.71277
30. Augustyn, D, Jamroz, E, and Sobol, G. Opsoclonus-myoclonus síndrome associated with neuroblastoma. Neurol Dziec. (2007) 16:65–8.
Keywords: opsoclonus myoclonus, case study, gynecology, patient, teratoma
Citation: Szczupak M, Kobak J, Wiśniewska A, Kosydar-Bochenek J, Jamro A and Krupa-Nurcek S (2025) Opsoclonus-myoclonus syndrome in the course of teratoma: a case report. Front. Med. 11:1519408. doi: 10.3389/fmed.2024.1519408
Edited by:
Cristina Secosan, Victor Babes University of Medicine and Pharmacy, RomaniaReviewed by:
Abhay Kattepur, Sri Devaraj Urs Medical College, IndiaKatarzyna Tomaszewska, Państwowa Akademia Nauk Stosowanych im. ks. B. Markiewicza w Jarosławiu, Poland
Copyright © 2025 Szczupak, Kobak, Wiśniewska, Kosydar-Bochenek, Jamro and Krupa-Nurcek. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jacek Kobak, amFjZWsua29iYWtAZ3VtZWQuZWR1LnBs