 Patricia Ruiz-Limón1,2,3
Patricia Ruiz-Limón1,2,3 Natalia Mena-Vázquez1,4*
Natalia Mena-Vázquez1,4* Isabel Moreno-Indias1,2,3Jose Manuel Lisbona-Montañez1,4,5Arkaitz Mucientes1,4Sara Manrique-Arija1,4,5Rocío Redondo-Rodriguez1,4Laura Cano-García1,4
Isabel Moreno-Indias1,2,3Jose Manuel Lisbona-Montañez1,4,5Arkaitz Mucientes1,4Sara Manrique-Arija1,4,5Rocío Redondo-Rodriguez1,4Laura Cano-García1,4 Francisco J. Tinahones1,2,3,5Antonio Fernández-Nebro1,4,5
Francisco J. Tinahones1,2,3,5Antonio Fernández-Nebro1,4,5- 1The Biomedical Research Institute of Malaga and Platform in Nanomedicine (IBIMA BIONAND Platform), Málaga, Spain
- 2Unidad de Gestión Clínica de Endocrinología y Nutrición, Hospital Universitario Virgen de la Victoria, Málaga, Spain
- 3CIBER Fisiopatología de la Obesidad y Nutrición (CIBEROBN), Instituto de Salud Carlos III, Madrid, Spain
- 4UGC de Reumatología, Hospital Regional Universitario de Málaga, Málaga, Spain
- 5Departamento de Medicina. Universidad de Málaga, Málaga, Spain
Background: Difficult-to-treat rheumatoid arthritis (D2T RA) refers to a subset of patients who fail to achieve adequate disease control after the use of two or more biological or targeted synthetic disease-modifying antirheumatic drugs (b/tsDMARDs) with different mechanisms of action, while maintaining active inflammatory disease. This presents a therapeutic challenge and highlights the need to explore contributing factors such as the potential role of the gut microbiota. Therefore, the aim of this study was to analyze the gut microbiota and inflammation in patients with D2T RA in comparison to patients with easy-to-treat RA (E2T RA).
Objective: To analyze the gut microbiota and inflammation in patients with D2T RA.
Methods: We performed an observational study of a prospective cohort between 2007 and 2011 and analyzed the gut microbiota. In 2022, we identified 2 extreme patient phenotypes: (1) D2T RA, which was defined as failure of ≥2 biological or targeted synthetic disease-modifying antirheumatic drugs (b/tsDMARDs) (with different mechanisms of action) plus signs of active disease; and (2) easy-to-treat RA (E2T RA), i.e., stable disease managed with a single treatment. The gut microbiota was analyzed using 16S rRNA gene sequencing; bioinformatics analysis was performed using QIIME2, and its functionality was inferred through PICRUSt. We recorded data on clinical findings, inflammation, and cytokines. A Cox multivariate analysis was performed to identify factors related to D2T RA.
Results: The study population comprised 39 patients: 13 (33%) with D2T RA and 26 (66%) with E2T RA. The families Lachnospiraceae and Pasteurellaceae, and their genera Coprococcus and Haemophilus were more abundant in E2T RA patients, while the genus Megasphaera was more abundant in D2T RA patients. The Firmicutes/Bacteroidetes ratio decreased in D2T RA patients. The metabolic profile of the gut microbiota was characterized by differences in Degradation/Utilization/Assimilation pathway and the Biosynthesis pathway. The factors associated with D2T RA were inflammatory activity according to DAS28-ESR (HR, 2.649; p = 0.013), prednisone (HR, 3.794; p = 0.008), and the Firmicutes/Bacteroidetes ratio (HR, 0.288; p = 0.033).
Conclusion: The composition of the gut microbiota of patients with D2T RA differed from that of E2T RA patients, as did the metabolic pathways.
Introduction
Rheumatoid arthritis (RA) is an immune-mediated chronic inflammatory disease characterized by involvement of the joints and other tissues. It causes pain, stiffness, and loss of mobility. Although there is no cure for RA, affected patients can be treated with a combination of conventional synthetic disease-modifying antirheumatic drugs (scDMARDs), biological DMARDs (bDMARDs), and targeted synthetic DMARDs (tsDMARDs) (1). Despite this therapeutic arsenal, between 15 and 30% of patients with RA have disease that is difficult to treat (D2T RA) and do not achieve remission or low disease activity (2).
According to the “European Alliance of Associations for Rheumatology” (EULAR) (3), patients with RA are considered D2T if at least 2 biological or targeted synthetic disease-modifying antirheumatic drugs (b/tsDMARDs) (with different mechanisms of action) have failed after previous failure of a csDMARD (unless contraindicated). Furthermore, the patient must have signs of active/progressive disease in which management of signs and/or symptoms is problematic for the rheumatologist and/or doctor.
Various studies have attempted to identify factors associated with a poor response to biologics in RA (4–7). Some of these factors include, once poor adherence and inadequate dosing have been excluded, higher autoantibody levels (6), a greater number of comorbid conditions (4, 6, 7), and more marked inflammatory activity at initiation of therapy (5–7). However, other studies have shown that patients with marked inflammatory activity can respond favorably to bDMARDs (6).
While the etiology of RA is not fully clear, it has been suggested that the disease results from the interaction between genetic and environmental factors (8). In recent years, several studies have focused on the gut microbiota as a major pathogenic factor in RA (9). Many studies have suggested that the degree of dysbiosis differs between patients with RA and controls and that microbial diversity is poorer in patients with RA than in controls. Similarly, intestinal dysbiosis and specific uncommon and harmful bacterial lineages have been associated with continuous high inflammatory activity or with the presence of factors affecting the severity of RA (9–12). Data on the effect of DMARDs on the gut microbiota in RA are limited (13), and no studies to date have specifically evaluated the gut microbiota of patients with D2T. In addition, no evidence is available on whether there is an association between continuously high inflammatory activity and high levels of proinflammatory cytokines in patients with D2T RA. Therefore, the primary objective of the present study was to compare the gut microbiota, cumulative inflammatory activity, and other clinical characteristics between patients with D2T RA and patients who respond well to therapy in order to identify microbial profiles and other factors associated with D2T RA.
Methods
Design, data source, and scope
The data for this controlled cross-sectional study came from a prospective cohort of incident cases recruited between 2007 and 2011 in the Department of Rheumatology, Hospital Universitario Regional de Málaga, Málaga, Spain (9). All the patients were aged ≥18 years, fulfilled the 2010 criteria of the American College of Rheumatology/European League Against Rheumatism for RA (14), and had been diagnosed and treated for the first time during the 12 months after onset of their disease. All participants provided their written informed consent before inclusion. The study was conducted according to the principles of the Declaration of Helsinki, and the study protocol was approved by the Ethics Committee of Málaga (Project identification code 4/2016, P19).
Participants and study protocol
Since the creation of the prospective cohort (2007–2011), all patients have been followed up at the outpatient clinic every 3–6 months by a rheumatologist using a systematic clinical data collection protocol. The data collected included inflammatory activity and physical function throughout follow-up.
During 2016–2018, all the patients in the cohort consented to a relevant modification to the protocol aimed at new, broader study objectives that enabled, among other options, the present study. Peripheral venous blood samples were collected after overnight fast, and fecal samples were refrigerated immediately and transported to the laboratory, where they were stored at −80°C for subsequent analysis. The date of this visit was the index date.
At the last visit in 2022 (final visit in the present study), we identified 2 groups of patients with extreme RA phenotypes: (1) a group comprising patients with difficult-to-treat RA (D2T RA); and (2) a group of easy-to-treat RA (E2T RA) patients at a 2:1 ratio, matched by age, sex, and time since diagnosis.
D2T RA was defined according to the EULAR criteria for D2T RA, as follows: failure of ≥2 biological or targeted synthetic disease-modifying antirheumatic drugs (b/tsDMARDs) (with different mechanisms of action) after failure of a csDMARD (unless contraindicated); signs suggestive of active/progressive disease; and management of signs and/or symptoms perceived as problematic by the rheumatologist and/or the patient (3). E2T RA was defined as treatment throughout follow-up with a single csDMARD and neither active nor progressive disease. Following the EULAR recommendations (3), active/progressive disease was defined as ≥1 of the following: at least moderate disease activity (according to validated composite measures including 28-joint Disease Activity Score for Rheumatoid Arthritis with erythrocyte sedimentation rate [DAS28-ESR] >3.2), signs and/or symptoms suggestive of active disease, inability to taper glucocorticoid treatment (below 7.5 mg/day prednisone or equivalent), rapid radiographic progression, and symptoms that diminish quality of life.
Outcome measures
On the index date, we collected demographic, clinical, and treatment-related data, including comorbid conditions associated with traditional cardiovascular risk factors (smoking, obesity, arterial hypertension, diabetes mellitus, history of cardiovascular disease, and sedentary lifestyle).
Similarly, on the index date, we evaluated inflammatory activity at the visit and calculated the cumulative activity. Activity was estimated as an arithmetic mean of all the values collected regularly since diagnosis (time-averaged disease activity). Inflammatory activity was measured using the DAS28-ESR (range, 0–9.4) (15). A DAS28-ESR value >3.2 was considered high and ≤3.2 was considered low. The erythrocyte sedimentation rate (ESR; mm/h) was measured. High-sensitivity C-reactive protein (hsCRP; mg/L) was measured for all participants using nephelometry (MMAGE-Immunochemistry Systems, Beckman Coulter, Brea, CA, United States). Physical function on the index date was assessed (average value) using the Health Assessment Questionnaire (HAQ).
We recorded the presence of autoantibodies and their titers, as follows: rheumatoid factor (positive if >10 IU/mL) and anti–citrullinated peptide antibody (positive if >20 IU/mL), as well as the presence or absence of radiologic erosions. We recorded all csDMARDs, such as methotrexate, leflunomide, and sulfasalazine, and bDMARDs, such as tumor necrosis factor inhibitors (anti-TNF), tocilizumab, abatacept, and rituximab. We also included tsDMARDs, such as the Janus kinase inhibitors (JAKi) tofacitinib and baricitinib, and glucocorticoids. Adherence to the Mediterranean diet was evaluated using a validated questionnaire in which adherence was defined as a score of >9 out of 14 (16).
Plasma levels of interleukins, human growth factors, and lipoproteins
Inflammatory mediators such as TNF-α, IL-1β, and IL-6 in plasma were quantified using enzyme-linked immunosorbent assay (ELISA) Quantiglo kits (R&D Systems Inc., Minneapolis, United States) according to the manufacturer’s instructions. Plasma levels of insulin-like growth factor I were analyzed using ELISA (Mediagnost GmbH., Tuebingen, Germany). Malondialdehyde-oxidized low-density lipoprotein (LDL) was also measured in plasma using an ELISA kit (Biomedica GmbH., Vienna, Austria).
Gut microbiota analysis
DNA was extracted using the QIAamp DNA Stool Mini Kit (Qiagen, Hilden, Germany) according to the manufacturer’s instructions. The concentration and purity of DNA were determined using a Nanodrop spectrophotometer (Nanodrop Technologies, Wilmington, DE, United States). Ribosomal 16S RNA (16S rRNA) gene sequences were amplified from DNA using the Ion 16S Metagenomics Kit (Thermo Fisher Scientific, Waltham, MA, United States). The kit includes 2 primer sets (V2-4-8 and V3–6, 7–9) that selectively amplify the corresponding hypervariable regions of the 16S region in bacteria. Libraries were built with the Ion Plus Fragment Library kit (Thermo Fisher Scientific). Barcodes were added to each sample using the Ion Xpress™ Barcode Adapters kit (Thermo Fisher Scientific). Emulsion PCR and sequencing of the amplicon libraries were performed on an Ion 530 chip (Ion 530™ Chip Kit) using the Ion Chef System and Ion Torrent S5™ system (Ion 510™/520™/530™ Kit-Chef, Thermo Fisher Scientific), respectively, according to the manufacturer’s instructions.
Bioinformatic analysis
Base calling and run demultiplexing were performed using Torrent Suite™ Server software (Thermo Fisher Scientific), version 5.4.0, with default parameters for targeted sequencing of 16S (bead loading ≤30, key signal ≤30, and usable sequences ≤30). Quality sequences were further translated into amplicon sequence variants (ASVs) using DADA2 with adapted parameters for Ion Torrent data within the open-source Quantitative Insights into Microbial Ecology software (QIIME2, version 2022.2) (17). Taxonomic assignment was performed through clustering with VSEARCH and the reference base Greengenes version 13_8 at 97% identity. Before analysis, samples with fewer than 1,500 sequences, features with a count sum of less than 10 across all samples, those presented only in one sample, mitochondrial features, and features unidentified at the phylum level were removed in the pre-processing step. Alpha and beta diversities were evaluated using the core-metrics-phylogenetic plugin in QIIME2 after rarefaction to the minimum number of sequences per sample. Alpha diversity was assessed through different indexes, including Pielou-evenness, Faith-PD, observed-features, and Shannon index. Statistically significant differences in alpha diversity between groups were determined by using the Kruskal-Wallis test with a significance level of p = 0.05. The beta diversity was assessed using non-phylogenetic Bray–Curtis dissimilarity index. The structure of the gut microbial community of the different groups was examined using PCoA plots for Bray-Curtis distances. The significance of variations among groups was determined using permutational multivariate analysis of variance (PERMANOVA) with a p-value of 0.05. Linear discriminant analysis (LDA) Effect Size (LEfSe) was used to identify potential biomarker taxa. LEfSe was performed on the online Galaxy web application1 (18), where data were normalized using counts per million (CPM). The nonparametric factorial Kruskal–Wallis sum rank test was used to detect differential abundant features (at genera, family, class, order, and phylum level) within the two groups. As a last step in the LEfSe analysis, LDA was used to determine the effect size of each differentially abundant feature. The differences in microbial relative abundance were considered significant when the LDA < 2 and p < 0.05 (19). The cladogram from the LEfSe method indicates the phylogenetic distribution representing differentially abundant taxonomic groups. The size of each node represents its relative abundance. The Phylogenetic Investigation of Communities by Reconstruction of Unobserved States plugin (PICRUSt2) (20) was used to predict metagenome function within QIIME2 with the DADA2 output. MetaCyc pathways (21) were normalized within QIIME2 and further analyzed using the open-source software STAMP (Statistical Analysis of Metagenomics Profiles) with Welch’s t test option (22).
Statistical analysis
A descriptive analysis of the main outcome measures was performed. Values are expressed as frequencies and percentages or as mean (standard deviation [SD]) or median (interquartile range [IQR]), as applicable. Normality was assessed using the Kolmogorov–Smirnov test. We compared clinical and laboratory characteristics and inflammatory activity between patients with D2T RA and patients with E2T RA using the Pearson χ2 test or the t test, as applicable. A multivariate analysis was performed, as was a Cox regression analysis, to identify factors associated with D2T RA adjusted for disease duration. The variables entered into the models were those that proved to be significant in the bivariate analysis and of clinical interest. Statistical significance was set at p < 0.05. The statistical analyzes were performed using IBM SPSS Statistics for Windows, Version 28 (IBM Corp., Armonk, NY, United States).
Results
We included 39 patients with RA, of whom 13 (33%) were D2T RA and 26 (66%) were E2T RA. Most were women (82%), with a mean (SD) age of 55.1 (11.6) years on the index date. In line with the definitions, at the end of follow-up (final visit), all D2T RA patients had been treated with at least 2 different lines of biologic therapy, whereas E2T RA patients had only received treatment with methotrexate, except for 1 patient who was treated with leflunomide owing to intolerance to methotrexate at 10 mg/wk.
Epidemiological and clinical characteristics and comorbid conditions
Table 1 shows the clinical and epidemiological characteristics of D2T RA patients and E2T RA patients on the index date. Data from both groups were consistent for most of the clinical-epidemiological characteristics and comorbid conditions, except that erosions were more frequent in D2T RA patients than in E2T RA patients (p = 0.021). There were no significant differences in the studied comorbidities related to cardiovascular risk, osteoporosis, fibromyalgia, or depression between the two groups. As for treatment, most D2T RA patients were receiving treatment with an anti-TNF agent on the index date (69.2%) or an IL-6 inhibitor (23.1%) (Table 1).
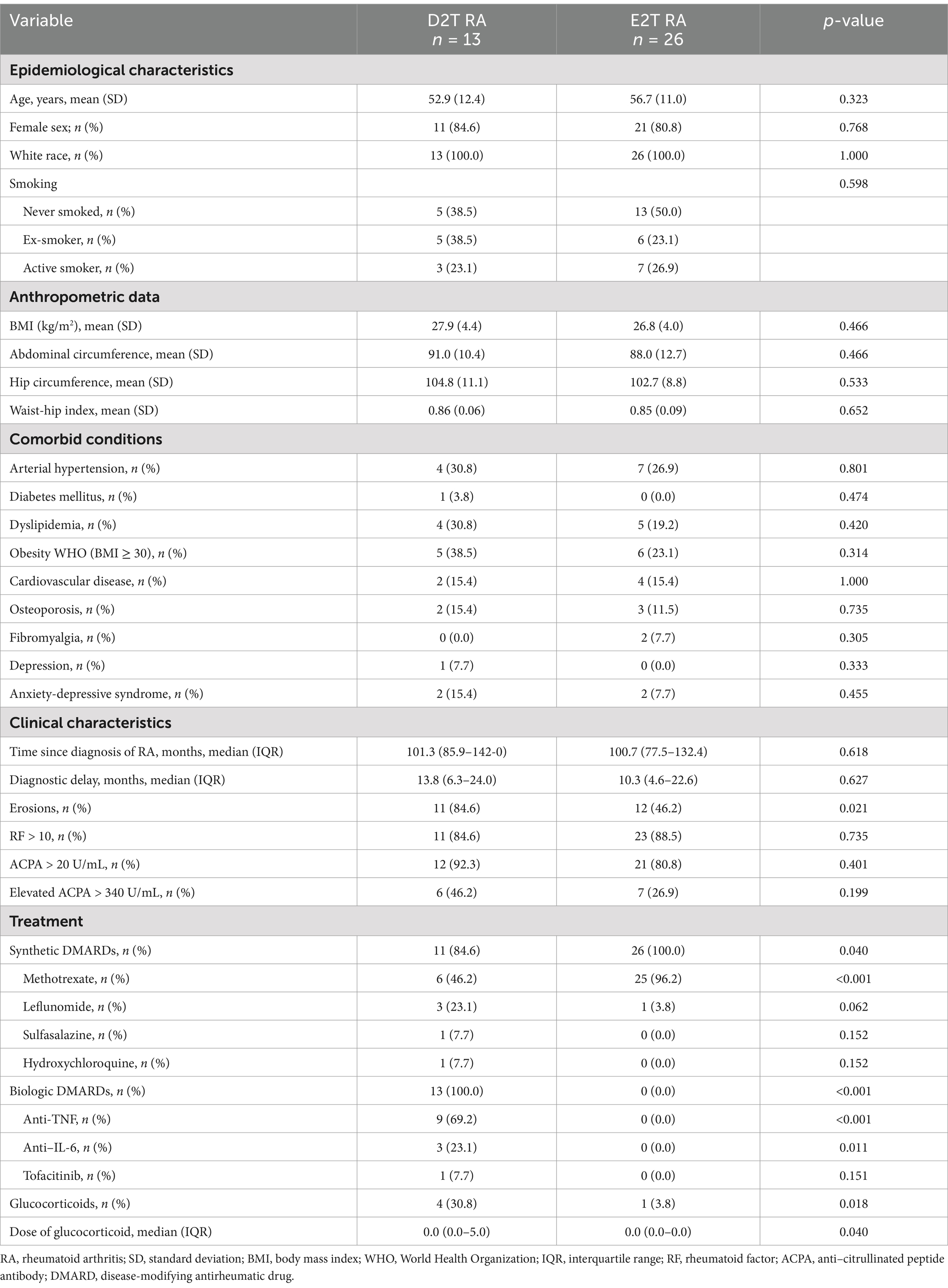
Table 1. Clinical and epidemiological data on the index date.
However, at the final visit (see Table 2), most of the 13 patients with D2T RA were receiving rituximab (30.8%) or tofacitinib (23.1%) after a mean (SD) of 2.6 (1.3) switches of biologics, with a mean (SD) retention period of 95.8 (56.3) months. In patients with D2T RA, the main reason for switching biological or targeted synthetic disease-modifying antirheumatic drugs (b/tsDMARDs) was loss of efficacy (18/34 treatments used [52%]), followed by insufficient response (11/34 [32%]) and nonserious adverse events (5/34 [14%]).
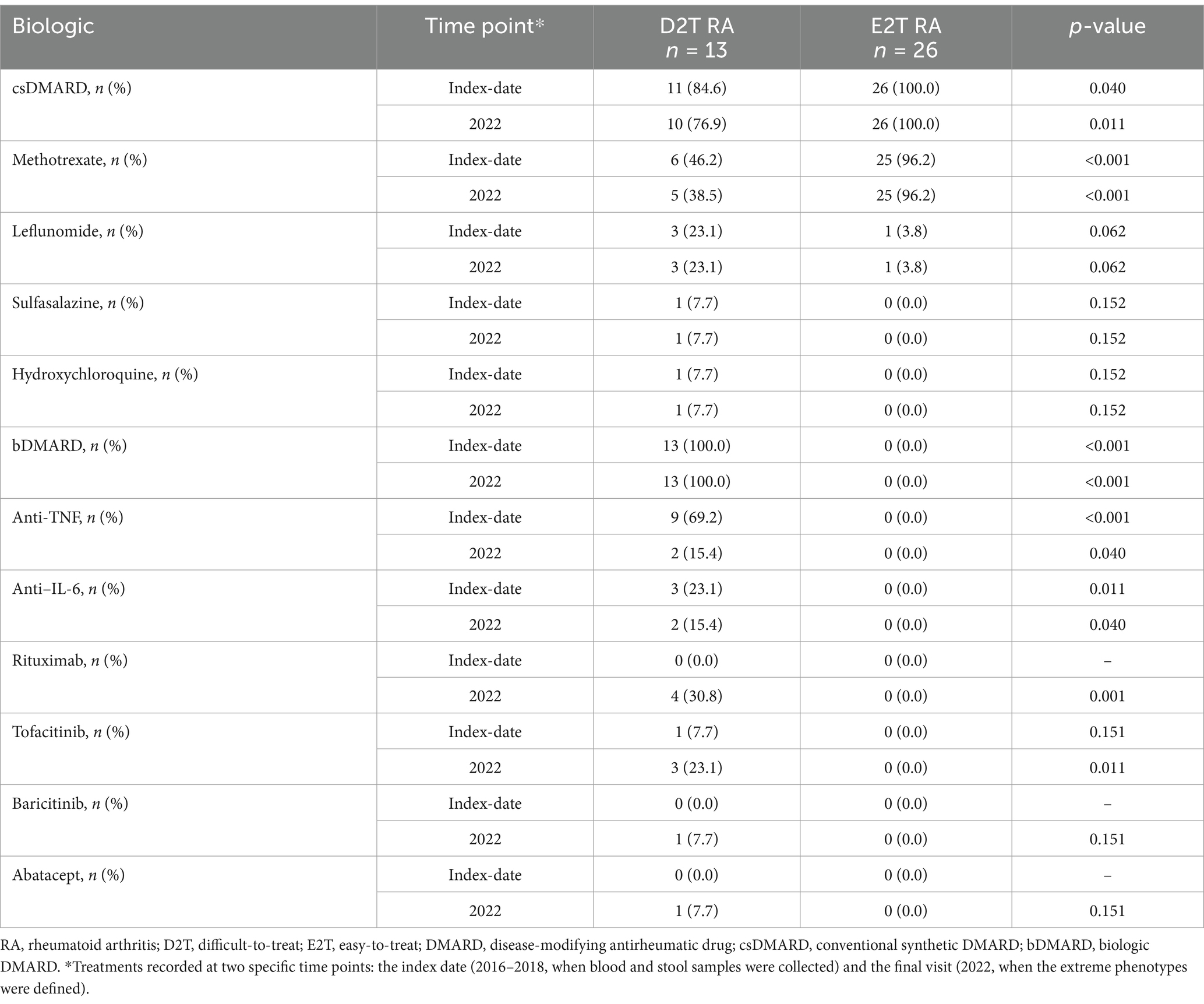
Table 2. Treatments at the index date (2016–2018) and the final visit (2022) in D2T RA and E2T RA patients.
In contrast, as expected, the 26 E2T RA patients maintained the same csDMARDs throughout follow-up. Similarly, a larger number of patients with D2T RA were receiving glucocorticoids on the index date (p = 0.018) and at a higher median dose than the E2T RA patients (p = 0.040).
Study of inflammatory factors and cytokines
Of the 39 patients included, 28 (71.8%) were in remission or with low disease activity at the index date according to their DAS28-ESR values, and 30 (76.9) had maintained an average DAS28-ESR value indicating low activity. D2T RA patients had higher average DAS28-ESR values at the cut-off than the E2T RA patients (Table 3). The same was true of physical functioning according to the HAQ. However, laboratory values were generally similar for both groups, except for some notable differences, such as homocysteine (p = 0.010) and CRP (p = 0.029), which were superior in D2T RA.
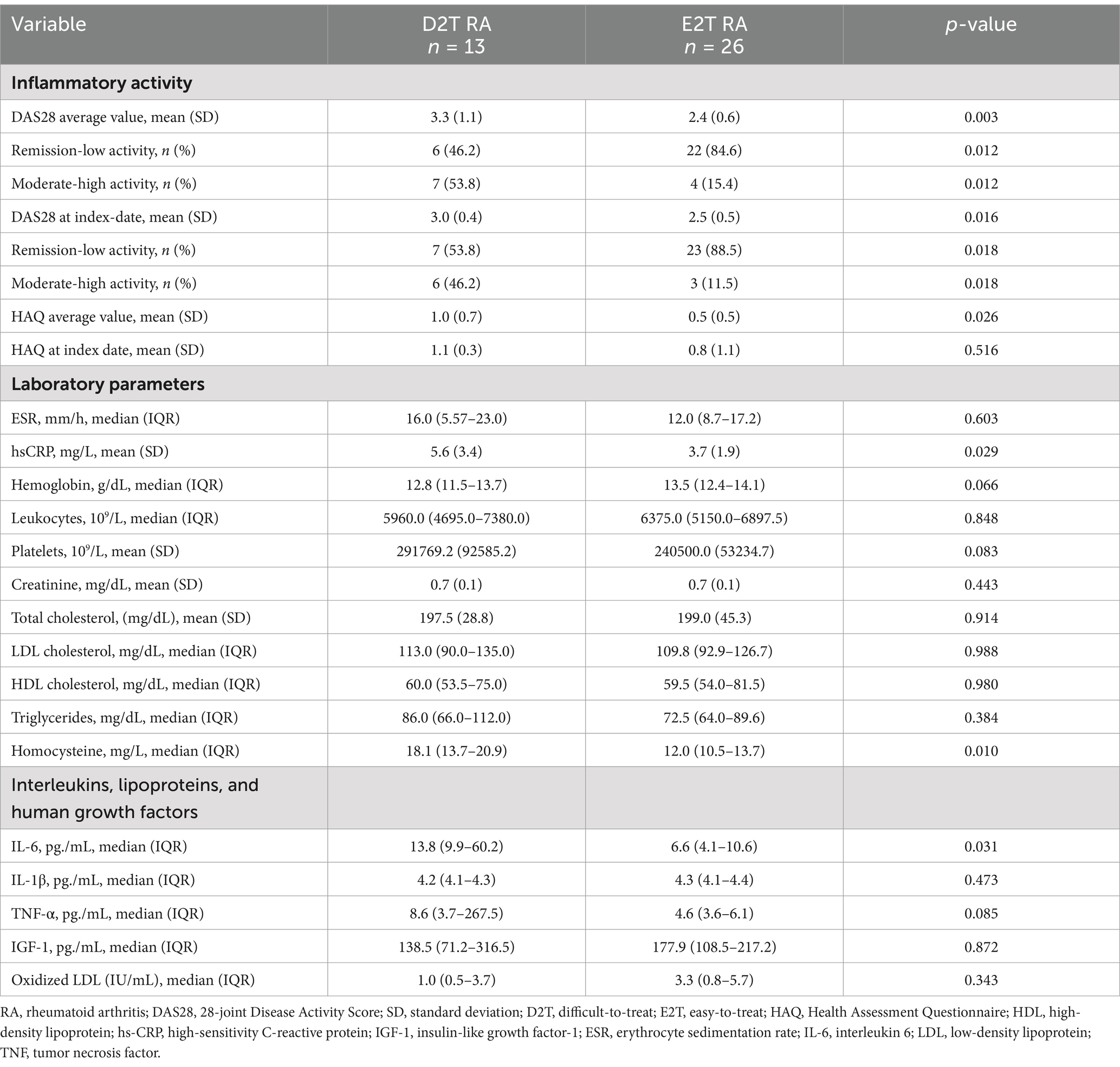
Table 3. Inflammatory factors and cytokines in D2T RA and E2T RA.
Regarding proinflammatory cytokines, D2T RA patients had higher levels of IL-6 (p = 0.031), and numerically higher levels of TNF-α (p = 0.085). In the case of lipoproteins and human growth factors, the values remained similar in both groups. Additionally, D2T RA patients were similar to those with E2T in their adherence to the Mediterranean diet (69.2% vs. 73.0%; p = 0.901).
Comparison of gut microbiota between groups
There were no differences in any of the alpha diversity measured indexes (Pielou’s evenness, p = 0.121; Faith’s phylogenetic diversity, p = 0.121; observed features, p = 0.318; and Shannon’s diversity, p = 0.101) between E2T RA and D2T RA patients (Figure 1A). While microbiota populations tended to differ based on beta diversity (Bray–Curtis dissimilarity; PERMANOVA, p = 0.089; Figure 1B).
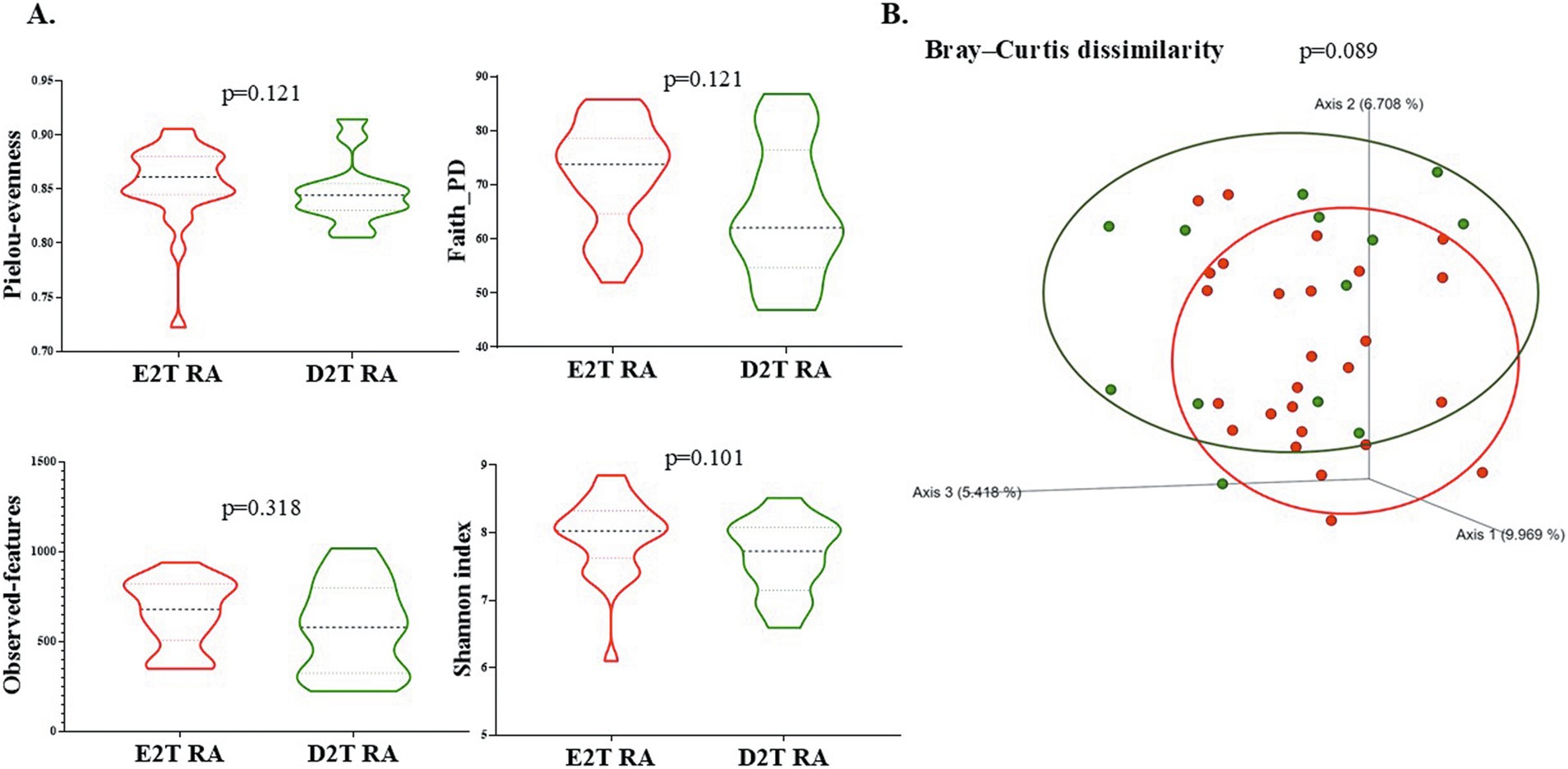
Figure 1. Diversity of gut microbiota between E2T RA and D2T RA patients. (A) Alpha diversity indexes: Pielou-evenness, Faith-PD, Observed features, and the Shannon index were compared between the 2 groups. Values are presented as mean ± SD. (B) Principal coordinates analysis (PCoA) corresponding to the Bray–Curtis dissimilarity index (beta diversity). The statistical analysis used permutational multivariate analysis of variance (PERMANOVA, p < 0.05). Green dots indicate the D2T RA patients; red dots the E2T RA patients. E2T RA, easy-to-treat rheumatoid arthritis; D2T RA, difficult-to-treat rheumatoid arthritis.
At the phylum level, the dominant bacterial phyla were Bacteroidetes, Firmicutes and Proteobacteria, while Actinobacteria, Synergistetes, Lentisphaerae, and Verrucomicrobia accounted for smaller proportions, between 1 and 10%, in both RA groups (Figure 2A). Analysis of the abundance of Bacteroidetes and Firmicutes did not reveal significant differences between E2T RA and D2T RA (p = 0.251 and p = 0.486, respectively; Figure 2B). However, the Firmicutes/Bacteroidetes ratio was lower in the D2T RA patients than in the E2T RA patients (p = 0.011; Figure 2C).
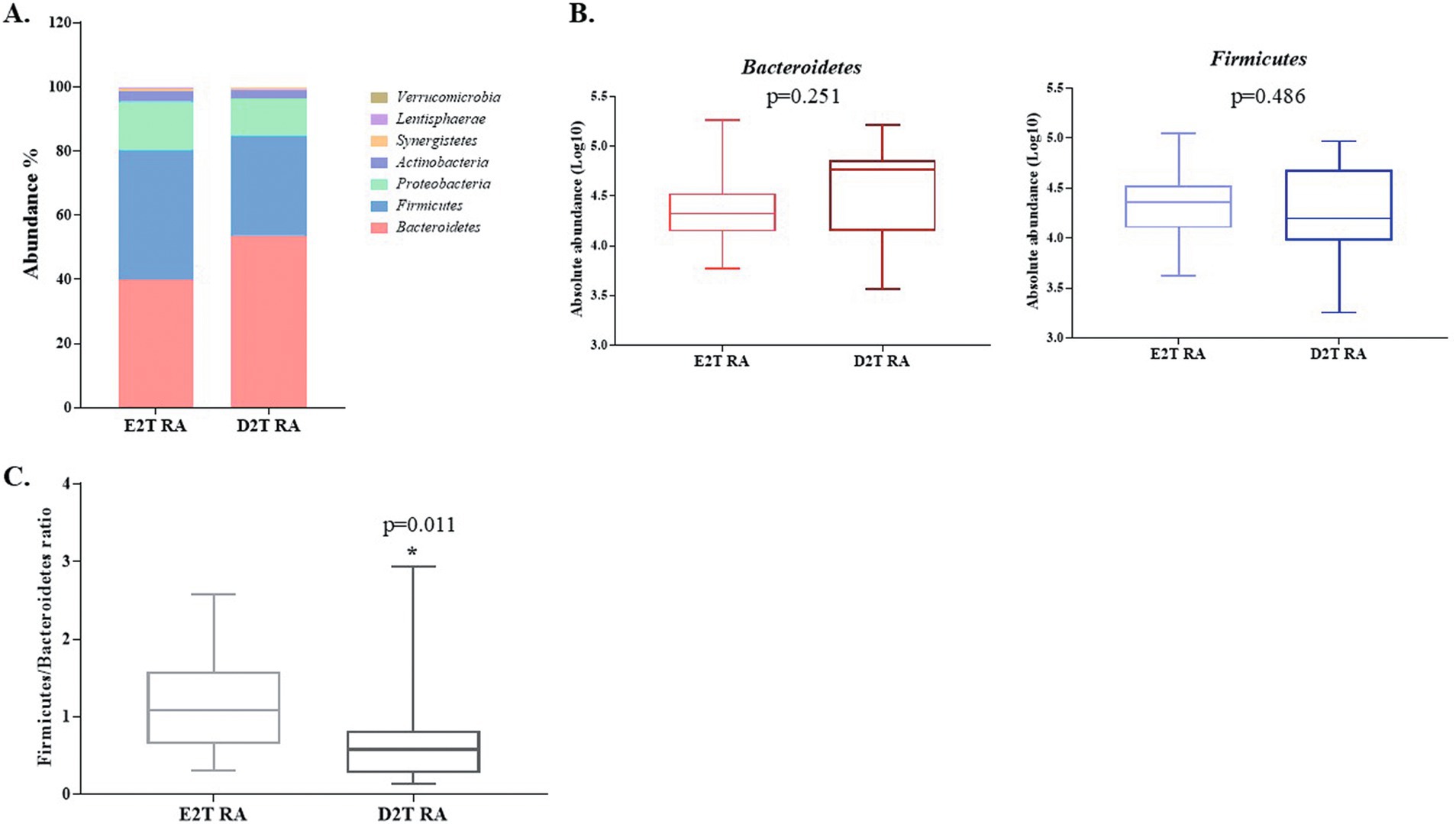
Figure 2. Gut microbiota analysis at the phylum level in E2T RA and D2T RA patients. (A) The distribution of gut microbiota at the phylum level in both RA groups. (B) The absolute abundance in Log10 of the phyla Bacteroidetes and Firmicutes in both RA groups. (C) The Firmicutes/Bacteroidetes ratio. * Indicates significant differences between groups (p < 0.05). E2T RA, easy-to-treat rheumatoid arthritis; D2T RA, difficult-to-treat rheumatoid arthritis.
Additionally, we performed LEfSe to identify changes in the gut microbiota between E2T RA and D2T RA patients. This analysis revealed an enrichment in the phylum Bacteroidetes and in the genus Megasphaera in the D2T RA group. In contrast, the E2T RA group exhibited a greater abundance of the phylum Proteobacteria, the family Pasteurellaceae and its genus Haemophilus, and the family Lachnospiraceae and its genus Coprococcus (LDA > 2; p < 0.05; Figure 3).
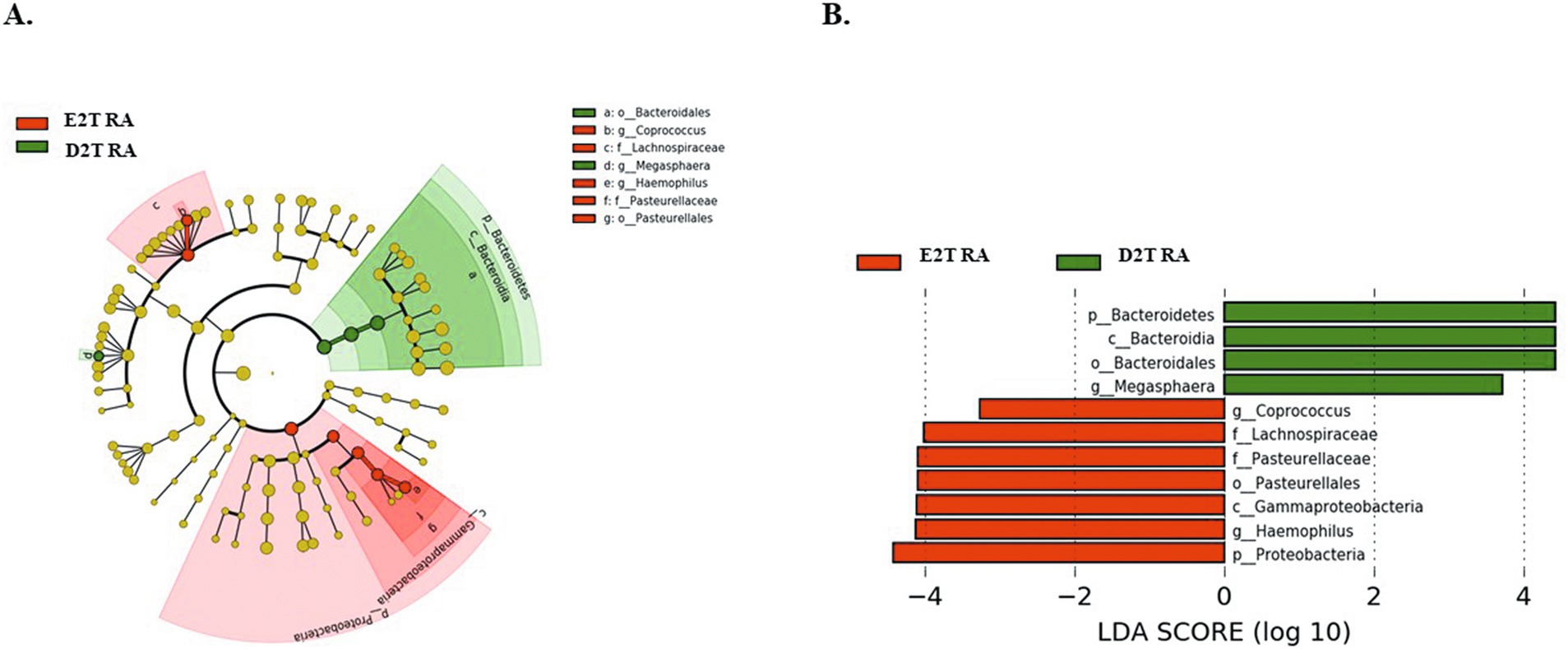
Figure 3. (A) Cladogram and (B) linear discriminant analysis (LDA) scores were used to determine differences in the abundance of microbes in E2T RA and D2T RA patients. LDA > 2; p < 0.05. E2T RA, easy-to-treat rheumatoid arthritis; D2T RA, difficult-to-treat rheumatoid arthritis.
Predicted metabolic profiles of gut microbiota
Metacyc pathway analysis was performed using PiCRUSt2 to increase our understanding of the role of gut microbiota in each of the groups studied. A Kruskal-Wallis analysis showed that 19 pathways differed between the groups (p < 0.05). The main pathways affected belonged to Degradation/Utilization/Assimilation pathways and Biosynthesis. In D2T RA patients, increased values were reported for the thiamine diphosphate salvage II pathway (PWY-6897) and the carbohydrate degradation pathway (PWY-6507). Increased values were also reported for E2T RA patients in the remaining pathways, some of which are involved in peptidoglycan biosynthesis and generation of precursor metabolites and energy (PWY0-1586 and REDCITCYC, respectively), and most of which are involved in degradation, specifically, aromatic compound (PWY-6185, PWY-5417, PWY-5431, PWY-7002, PWY5F9-12), toluene degradation (PWY-5178 and PWY-5181), fatty acid and lipid degradation (PWY-6946 and LIPASYN-PWY), carbohydrate degradation (PWY-7644), secondary metabolite degradation (PWY-6507), and nucleoside and nucleotide degradation (PWY-6353) (Figure 4).
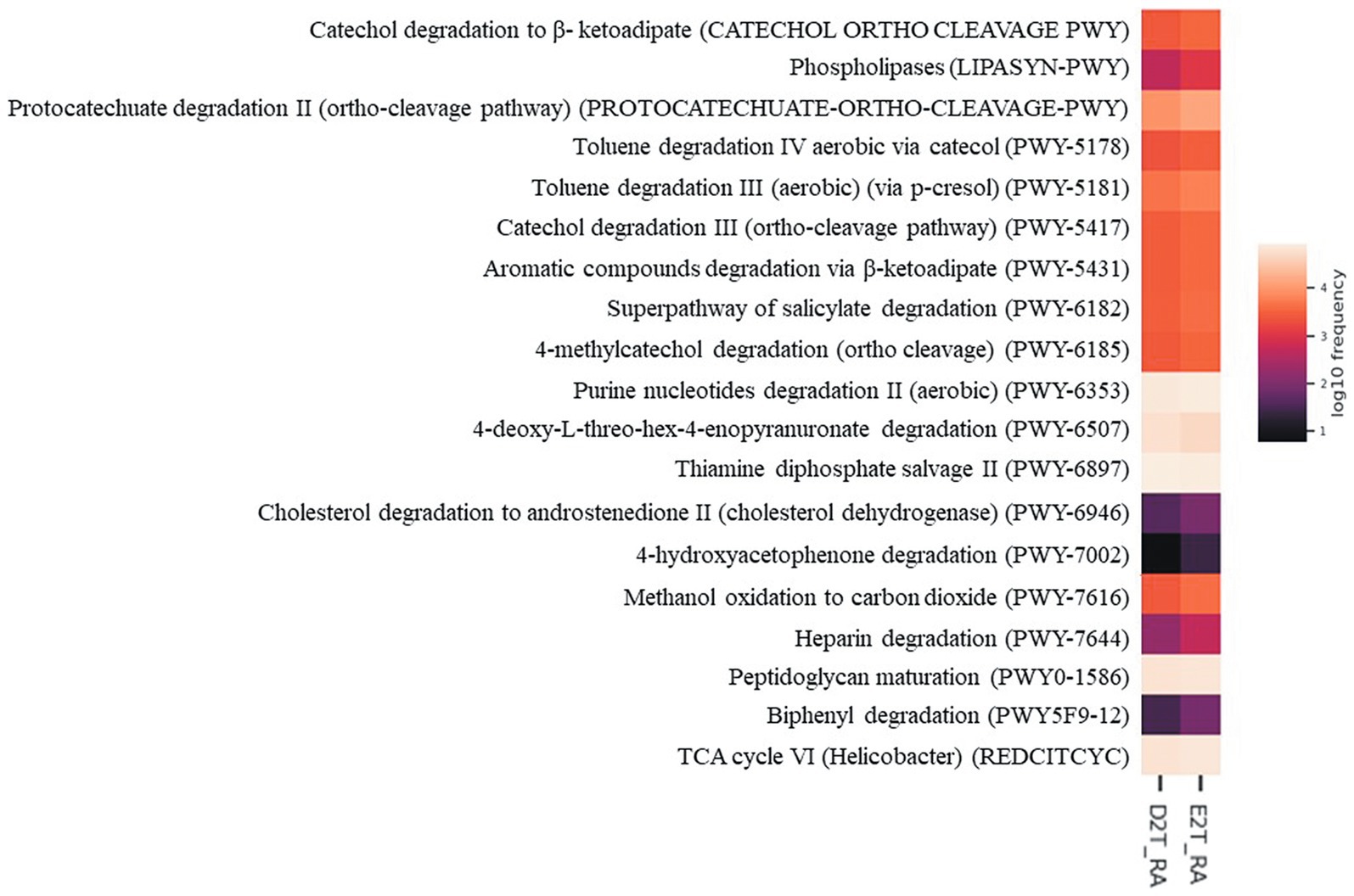
Figure 4. Predictive metabolic pathways by PICRUSt2. Heatmap of differentially abundant Metacyc pathways identified in the study groups (E2T RA and D2T RA patients). The values of color in the heatmap represent the normalized relative abundance of Metacyc pathways. Kruskal-Wallis test, p < 0.05. E2T RA, easy-to-treat rheumatoid arthritis; D2T RA, difficult-to-treat rheumatoid arthritis.
Factors associated with D2T RA patients
Table 4 shows the results of the Cox multivariate analysis (DV: D2T RA), in which 39 patients with RA were included over a mean (SD) follow-up of 103.8 (37.8) months. A total of 13/39 patients had D2T RA. The multivariate analysis showed that the Firmicutes/Bacteroidetes ratio was associated with a reduced risk of D2T RA (HR, 0.288; 95% CI, 0.092–0.907; p = 0.033), whereas the variables associated with a greater probability of D2T RA were greater average inflammatory activity according to the DAS28-ESR (HR, 2.649; 95% CI, 1.225–5.732; p = 0.013) and treatment with prednisone on the index date (HR, 3.794; 95% CI, 1.098–10.990; p = 0.008). Thus, for each 0.1-point increase in the Firmicutes/Bacteroidetes ratio, the risk of D2T RA decreased by approximately 71%.
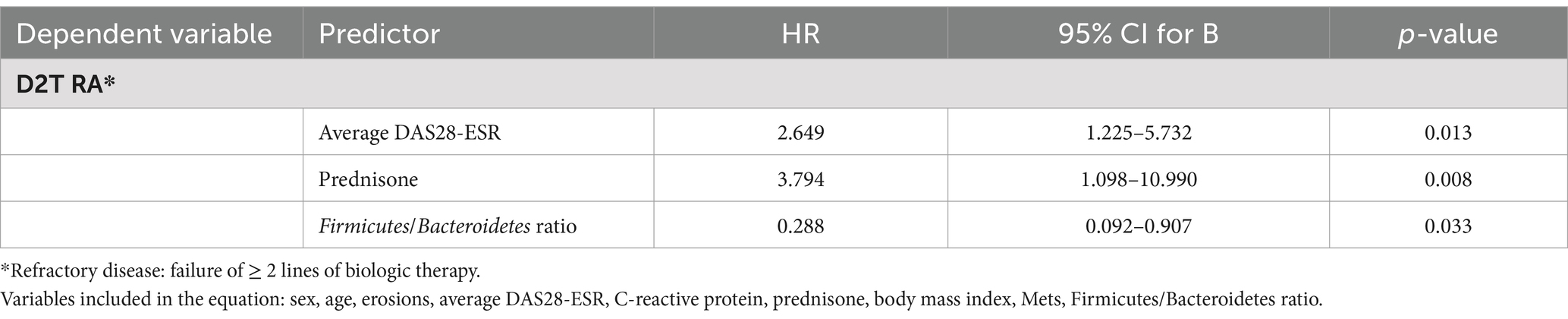
Table 4. Cox regression model of factors for RA patients with refractory disease.
Discussion
Patients with D2T RA continue to display symptoms after several treatment cycles, thus generating a considerable burden in clinical practice (4). Various factors are thought to affect the persistence of signs and symptoms in affected patients, which is rarely caused only by resistance to therapy (2). Today, however, there is little evidence indicating the particular characteristics, mechanisms, and factors associated with D2T RA, thus further hampering patient management (2). In an attempt to address this unmet need, the present study compares the gut microbiota profile, cumulative disease activity, and other severity-related factors between patients with D2T RA and patients with E2T RA in order to identify the intestinal microbiota profile and other factors associated with this major problem. Non-responder patients do not achieve adequate control with any treatment, while D2T RA patients have failed to respond to two or more biologics or targeted synthetic DMARDs, highlighting their clinical profile and the need for tailored therapeutic strategies.
The present study revealed that although gut microbiota populations are characterized by similar features, their abundance differed between the 2 groups. Differences were recorded in the abundance of various features, such as the families Lachnospiraceae and Pasteurellaceae and their respective genera Coprococcus and Haemophilus, which were more abundant in E2T RA patients than in D2T RA patients, in fact Haemophilus is implicated in RA (23). On the other hand, an increase in the abundance of Coprococcus has previously been observed in RA patients after therapy with methotrexate (24) and with sulfasalazine (25). Moreover, the Lachnospiraceae family is a major producer of butyrate (a short-chain fatty acid [SCFA]) which has beneficial effects on RA (26). In addition, a recent study (25) showed a rise in the number of SCFA-producing genera after patients with RA were treated with TNF inhibitors. These observations suggest that alterations in gut microbiota could contribute to the therapeutic effects of bDMARDs. Furthermore, this study found that the genus Megasphaera was more abundant in D2T RA patients. Indeed, this genus has been shown to be positively related to RA with greater abundances (27, 28).
Regarding the phyla Firmicutes and Bacteroidetes, LEfSe revealed enrichment of the phylum Bacteroidetes in the D2T RA group. In this line, we found that the Firmicutes/Bacteroidetes ratio was lower in D2T RA patients than in E2T RA patients. This ratio, although controversial, has been shown to be associated with different diseases; for instance, it is decreased in RA patients (29). Moreover, our multivariate analysis showed that the phylum Bacteroidetes was associated with a greater risk of E2T RA, whereas the phylum Firmicutes acted as a protective factor. The phylum Bacteroidetes was found to be less abundant in treated patients with established RA than in healthy controls (30, 31). In fact, as shown by Zhang et al. (32), levels of the genus Bacteroides were further reduced after treatment with DMARDs, especially methotrexate, which reverses the perturbations of the microbiota typically associated with RA (33, 34). In fact, several studies demonstrated that abundance of Firmicutes was increased while Bacteroidetes was decreased after treatment with methotrexate (32, 35). These changes in levels of Bacteroidetes could be associated with the stage of development of RA and with the response to treatment. Thus, the absence of response in patients with D2T RA could be associated with the increase we observed for the phylum Bacteroidetes. Moreover, in situations that alter intestinal acidity or composition, values for the phylum Firmicutes would decrease, thus leading to an increase in values for acetate- and propionate-producing Bacteroidetes (36, 37). The butyrate deficiency following the decrease in Firmicutes leads to a deficiency in mucin and an increase in intestinal permeability, which in turn induces a chronic inflammatory state (38). Therefore, this could be one of the factors affecting the inadequate response to treatment in patients with RA in our study.
According to the microbial metabolism approach, which was based on the inference of the metabolic pathways taken by the gut microbiota using PICRUSt2, no notable differences were found between the 2 groups studied. However, the main pathways implicated indicate that degradation is a major contributor to the results, including degradation of aromatic compounds (e.g., catechol and toluene, carbohydrates, and fatty acids), which provide energy, and that degradation was more pronounced in E2T RA patients than in D2T RA patients. Likewise, purine metabolism was increased in the E2T RA patients compared to D2T RA patients. The purine pathway plays an important role in intestinal permeability; specifically, purines help maintain a healthy energy balance and contribute to the restoration of the gut barrier (39). The findings reported may provide insight into how gut microbiota composition and metabolic activity differ between patients who respond and do not respond to treatment. This in turn could prove useful for developing targeted therapies and improving our understanding of disease mechanisms.
We also observed that patients with D2T RA had a higher average DAS28-ESR, poorer physical function according to HAQ, and higher values for inflammatory factors such as CRP and IL-6 than patients with E2T RA. Regarding these factors, the multivariate analysis showed a significant association between the average DAS28-ESR value and D2T RA. Several studies have reported that patients with D2T RA are characterized by greater inflammatory activity according to indices such as DAS28, both at initiation of biologics (40, 41) and during switches in biologic therapy over time (42). This finding could be explained by the low rates of response to treatment in patients with greater inflammatory activity (43, 44) and by the difficulty encountered when attempting to reduce very high DAS28 values until remission is achieved. Other factors that could affect higher disease activity indexes in these patients include pain and a more negative global evaluation owing to chronic disease with structural damage that has not been easily controlled. The latter observation could arise from the association between treatment with glucocorticoids and D2T RA revealed by our multivariate analysis. Reducing doses of glucocorticoids to below 5–10 mg/d has proven difficult in patients with D2T RA (4), probably because of the greater inflammatory activity. Moreover, it is worth noting that the concomitant use of glucocorticoids has been associated with severe adverse reactions and interruption of some biologics such as anti-TNF agents and anti–IL-6 agents, mainly owing to infection (45, 46).
Our study has both strengths and limitations. First, we performed a cross-sectional analysis of microbiota and inflammatory cytokines based on a single determination. However, the patients belonged to a prospective RA cohort in which all inflammation- and treatment-related data were collected longitudinally following a predetermined protocol. Second, the sample of patients with D2T RA is small, potentially limiting the possibility of detecting differences between the groups. In order to mitigate this problem, we selected 2 comparators with extreme phenotypes and twice the number of E2T RA patients per case of D2T RA. This approach enabled us to demonstrate significant differences in the main hypotheses proposed. Furthermore, while the definition of D2T RA has varied over time, we used the definition recommended by EULAR (3), which serves as a basis for most published studies. While we acknowledge that including a healthy control group would strengthen our findings, our study primarily focused on comparing D2T and E2T RA patients. Likewise, the higher proportion of female participants in our cohort may introduce confounding factors, such as hormonal influences on disease activity. Additionally, although we did not assess dietary components in detail, we observed that a high percentage of patients in both groups adhered to the Mediterranean diet. Finally, it is important to remember that other factors may affect D2T RA and have not been the object of this study, for example, metabolic differences between conventional synthetic disease-modifying antirheumatic drugs (csDMARDs) and biological or targeted synthetic disease-modifying antirheumatic drugs (b/tsDMARDs) or adherence to treatment. Nevertheless, we identified and described, for the first time, the association between microbiota-related factors and D2T RA by combining these findings with other clinical characteristics.
Conclusion
This study found that the gut microbiota profile differs between D2T RA and E2T RA patients. Specifically, patients with D2T RA were characterized by enrichment of the phylum Bacteroidetes and the genus Megasphaera, whereas in patients with E2T RA, the phylum Proteobacteria, the family Pasteurellaceae and its genus Haemophilus, and the family Lachnospiraceae and its genus Coprococcus were more abundant. The Firmicutes/Bacteroidetes ratio was lower in patients with D2T RA. In addition, an increase in this ratio was seen to be an independent factor for reduced risk of D2T RA, suggesting that gut dysbiosis plays a role in nonresponse to treatment. Moreover, the above-mentioned metabolic pathway analysis revealed differences in the pathways involved in degradation of aromatic compounds, carbohydrates, and fatty acids between D2T RA and E2T RA patients. Greater inflammatory activity and use of prednisone were associated with D2T RA. The identification of new factors associated with D2T RA is a relevant finding that enhances our knowledge of patients with this disease, which is currently a severe problem with high social and health care costs. A more individualized approach including these factors can improve outcomes and reduce the risk of adverse effects of medication.
Data availability statement
The datasets presented in this article are not readily available because according to the data regulations and ethical considerations, the datasets generated and analyzed during our study cannot be made public due to the fact participants only provided their consent to the original team of investigators for the use of their data, and this information may compromise their consent to participate in the study. Requests to access the datasets should be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by Research Ethics Committee of Hospital Regional Universitario de Málaga (HRUM) (Project identification code 4/2016, P19). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
PR-L: Conceptualization, Investigation, Methodology, Writing – original draft, Writing – review & editing. NM-V: Conceptualization, Investigation, Methodology, Writing – original draft, Writing – review & editing. IM-I: Investigation, Writing – review & editing. JL-M: Investigation, Writing – review & editing. AM: Investigation, Writing – review & editing. SM-A: Investigation, Writing – review & editing. RR-R: Investigation, Writing – review & editing. LC-G: Investigation, Writing – review & editing. FT: Conceptualization, Supervision, Writing – review & editing. AF-N: Conceptualization, Investigation, Supervision, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This work was supported by Instituto Salud Carlos III (grants cofunded by ERDF) (PI18/00824). “Redes de Investigación Cooperativa Orientadas a Resultados en Salud (RICORS), Red de Enfermedades Inflamatorias (REI) (RD21/0002/0037)”: fondos de Next Generation EU, que financian las actuaciones del Mecanismo para la Recuperación y la 4 Resiliencia (MRR). PR-L was supported by a “Miguel Servet” postdoctoral contract (CP22/00096) by the ISCIII-Madrid (Spain) and cofunded by the European Union. IM-I was supported by the “Miguel Servet Type II” program (CPII21/00013) of the ISCIII-Madrid, co-financed by the FEDER. AM was supported by a “Sara Borrell” postdoctoral contract (CD23/00082) by ISCIII and co-funded by the European Union. JL-M was supported by PFIS predoctoral contract (FI23/00084) by ISCIII and co-funded by the European Union.
Acknowledgments
The authors thank the Spanish Foundation of Rheumatology for providing medical writing/editorial assistance during the preparation of the manuscript (FERBT2024). The research groups thanks for its support of the CIBER-IBIMA-Metagenomics platform, especially Pablo Rodríguez and Mª José García-López.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
16S rRNA, Ribosomal 16S RNA; anti-TNF, Tumor necrosis factor inhibitors; ASVs, Amplicon sequence variants; bDMARDs, Biological disease-modifying antirheumatic drugs; DAS28-ESR, 28-joint Disease Activity Score for Rheumatoid Arthritis with erythrocyte sedimentation rate; D2T, Difficult to treat; E2T, Easy to treat; EULAR, European Alliance of Associations for Rheumatology; HAQ, Health Assessment Questionnaire; HDL, High-density lipoprotein; hsCRP, High-sensitivity C-reactive protein; IQR, Interquartile range; LDL, Low-density lipoprotein; LDA, Linear discriminant analysis; LEfSe, Linear discriminant analysis Effect Size; PERMANOVA, Permutational multivariate analysis of variance; PICRUSt2, Phylogenetic Investigation of Communities by Reconstruction of Unobserved States plugin; QIIME2, Quantitative Insights into Microbial Ecology software; RA, Rheumatoid arthritis; scDMARDs, Conventional synthetic disease-modifying antirheumatic drugs; SCFA, Short-chain fatty acid; SD, Standard deviation; STAMP, Statistical Analysis of Metagenomics Profiles; tsDMARDs, Targeted synthetic disease-modifying antirheumatic drugs.
Footnotes
References
1. Mena-Vázquez, N, Ruiz-Limón, P, Moreno-Indias, I, Manrique-Arija, S, Tinahones, FJ, and Fernández-Nebro, A. Expansion of rare and harmful lineages is associated with established rheumatoid arthritis. J Clin Med. (2020) 9:1044. doi: 10.3390/jcm9041044
2. de Hair, MJH, Jacobs, JWG, Schoneveld, JLM, and van Laar, JM. Difficult-to-treat rheumatoid arthritis: an area of unmet clinical need. Rheumatology (Oxford). (2018) 57:1135–44. doi: 10.1093/rheumatology/kex349
3. Nagy, G, Roodenrijs, NMT, Welsing, PMJ, Kedves, M, Hamar, A, van der Goes, MC, et al. EULAR points to consider for the management of difficult-to-treat rheumatoid arthritis. Ann Rheum Dis. (2022) 81:20–33. doi: 10.1136/annrheumdis-2021-220973
4. Roodenrijs, NMT, de Hair, MJH, van der Goes, MC, Jacobs, JWG, Welsing, PMJ, van der Heijde, D, et al. Characteristics of difficult-to-treat rheumatoid arthritis: results of an international survey. Ann Rheum Dis. (2018) 77:1705–9. doi: 10.1136/annrheumdis-2018-213687
5. Yoshii, I, Sawada, N, and Chijiwa, T. Clinical characteristics and variants that predict prognosis of difficult-to-treat rheumatoid arthritis. Rheumatol Int. (2022) 42:1947–54. doi: 10.1007/s00296-022-05124-1
6. Watanabe, R, Hashimoto, M, Murata, K, Murakami, K, Tanaka, M, Ohmura, K, et al. Prevalence and predictive factors of difficult-to-treat rheumatoid arthritis: the KURAMA cohort. Immunol Med. (2022) 45:35–44. doi: 10.1080/25785826.2021.1928383
7. Roodenrijs, NMT, van der Goes, MC, Welsing, PMJ, Tekstra, J, Lafeber, FPJG, Jacobs, JWG, et al. Difficult-to-treat rheumatoid arthritis: contributing factors and burden of disease. Rheumatology (Oxford). (2021) 60:3778–88. doi: 10.1093/rheumatology/keaa860
8. Choy, EH, and Panayi, GS. Cytokine pathways and joint inflammation in rheumatoid arthritis. N Engl J Med. (2001) 344:907–16. doi: 10.1056/NEJM200103223441207
9. Ruiz-Limón, P, Mena-Vázquez, N, Moreno-Indias, I, Manrique-Arija, S, Lisbona-Montañez, JM, Cano-García, L, et al. Collinsella is associated with cumulative inflammatory burden in an established rheumatoid arthritis cohort. Biomed Pharmacother. (2022) 153:113518. doi: 10.1016/j.biopha.2022.113518
10. Chen, J, Wright, K, Davis, JM, Jeraldo, P, Marietta, EV, Murray, J, et al. An expansion of rare lineage intestinal microbes characterizes rheumatoid arthritis. Genome Med. (2016) 8:43. doi: 10.1186/s13073-016-0299-7
11. Gupta, VK, Cunningham, KY, Hur, B, Bakshi, U, Huang, H, Warrington, KJ, et al. Gut microbial determinants of clinically important improvement in patients with rheumatoid arthritis. Genome Med. (2021) 13:149. doi: 10.1186/s13073-021-00957-0
12. Attur, M, Scher, JU, Abramson, SB, and Attur, M. Role of intestinal Dysbiosis and nutrition in rheumatoid arthritis. Cells. (2022) 11:2436. doi: 10.3390/cells11152436
13. Picchianti-Diamanti, A, Panebianco, C, Salemi, S, Sorgi, ML, Di Rosa, R, Tropea, A, et al. Analysis of gut microbiota in rheumatoid arthritis patients: disease-related dysbiosis and modifications induced by etanercept. Int J Mol Sci. (2018) 19:2938. doi: 10.3390/ijms19102938
14. Aletaha, D, Neogi, T, Silman, AJ, Funovits, J, Felson, DT, Bingham, CO 3rd, et al. 2010 rheumatoid arthritis classification criteria: an American College of Rheumatology/European league against rheumatism collaborative initiative. Arthritis Rheum. (2010) 62:2569–81. doi: 10.1002/art.27584
15. Iwamoto, N, Kawakami, A, Fujikawa, K, Aramaki, T, Kawashiri, SY, Tamai, M, et al. Prediction of DAS28-ESR remission at 6 months by baseline variables in patients with rheumatoid arthritis treated with etanercept in Japanese population. Mod Rheumatol. (2009) 19:488–92. doi: 10.3109/s10165-009-0187-8
16. Krone, W, and Nitschmann, S. Mediterranean diet for primary prevention of cardiovascular diseases: Prevención-con-Dieta-Mediterránea (PREDIMED) study. Internist (Berl). (2014) 55:607–8. doi: 10.1007/s00108-014-3497-7
17. Bolyen, E, Rideout, JR, Dillon, MR, Bokulich, NA, Abnet, CC, Al-Ghalith, GA, et al. Reproducible, interactive, scalable and extensible microbiome data science using QIIME 2. Nat Biotechnol. (2019) 37:852–7. doi: 10.1038/s41587-019-0209-9
18. Blankenberg, D, Von Kuster, G, Coraor, N, Ananda, G, Lazarus, R, Mangan, M, et al. Galaxy: a web-based genome analysis tool for experimentalists. Curr Protoc Mol Biol. (2010) Chapter 19:Unit 19.10.1-21. doi: 10.1002/0471142727.mb1910s89
19. Segata, N, Izard, J, Waldron, L, Gevers, D, Miropolsky, L, Garrett, WS, et al. Metagenomic biomarker discovery and explanation. Genome Biol. (2011) 12:R60. doi: 10.1186/gb-2011-12-6-r60
20. Douglas, GM, Maffei, VJ, Zaneveld, JR, Yurgel, SN, Brown, JR, Taylor, CM, et al. PICRUSt2 for prediction of metagenome functions. Nat Biotechnol. (2020) 38:685–8. doi: 10.1038/s41587-020-0548-6
21. Caspi, R, Billington, R, Keseler, IM, Kothari, A, Krummenacker, M, Midford, PE, et al. The MetaCyc database of metabolic pathways and enzymes - a 2019 update. Nucleic Acids Res. (2020) 48:D445–53. doi: 10.1093/nar/gkz862
22. Parks, DH, Tyson, GW, Hugenholtz, P, and Beiko, RG. STAMP: statistical analysis of taxonomic and functional profiles. Bioinformatics. (2014) 30:3123–4. doi: 10.1093/bioinformatics/btu494
23. Mena-Vázquez, N, Ruiz-Limón, P, Moreno-Indias, I, Manrique-Arija, S, Lisbona-Montañez, JM, Rioja, J, et al. Adiposity is associated with expansion of the genus Dialister in rheumatoid arthritis patients. Biomed Pharmacother. (2023) 160:114388. doi: 10.1016/j.biopha.2023.114388
24. Marazzato, M, Iannuccelli, C, Guzzo, MP, Nencioni, L, Lucchino, B, Radocchia, G, et al. Gut microbiota structure and metabolites, before and after treatment in early rheumatoid arthritis patients: a pilot study. Front Med. (2022) 9:921675. doi: 10.3389/fmed.2022.921675
25. Koh, JH, Lee, EH, Cha, KH, Pan, CH, Kim, D, and Kim, WU. Factors associated with the composition of the gut microbiome in patients with established rheumatoid arthritis and its value for predicting treatment responses. Arthritis Res Ther. (2023) 25:32. doi: 10.1186/s13075-023-03013-x
26. He, J, Chu, Y, Li, J, Meng, Q, Liu, Y, Jin, J, et al. Intestinal butyrate-metabolizing species contribute to autoantibody production and bone erosion in rheumatoid arthritis. Sci Adv. (2022) 8:eabm1511. doi: 10.1126/sciadv.abm1511
27. El Menofy, NG, Ramadan, M, Abdelbary, ER, Ibrahim, HG, Azzam, AI, Ghit, MM, et al. Bacterial compositional shifts of gut microbiomes in patients with rheumatoid arthritis in association with disease activity. Microorganisms. (2022) 10:1820. doi: 10.3390/microorganisms10091820
28. Zhao, Y, Chen, B, Li, S, Yang, L, Zhu, D, Wang, Y, et al. Detection and characterization of bacterial nucleic acids in culture-negative synovial tissue and fluid samples from rheumatoid arthritis or osteoarthritis patients. Sci Rep. (2018) 8:14305. doi: 10.1038/s41598-018-32675-w
29. Kasselman, LJ, Vernice, NA, DeLeon, J, and Reiss, AB. The gut microbiome and elevated cardiovascular risk in obesity and autoimmunity. Atherosclerosis. (2018) 271:203–13. doi: 10.1016/j.atherosclerosis.2018.02.036
30. Chen, Y, Ma, C, Liu, L, He, J, Zhu, C, Zheng, F, et al. Analysis of gut microbiota and metabolites in patients with rheumatoid arthritis and identification of potential biomarkers. Aging (Albany NY). (2021) 13:23689–701. doi: 10.18632/aging.203641
31. Kishikawa, T, Maeda, Y, Nii, T, Motooka, D, Matsumoto, Y, Matsushita, M, et al. Metagenome-wide association study of gut microbiome revealed novel aetiology of rheumatoid arthritis in the Japanese population. Ann Rheum Dis. (2020) 79:103–11. doi: 10.1136/annrheumdis-2019-215743
32. Zhang, X, Zhang, D, Jia, H, Feng, Q, Wang, D, Liang, D, et al. The oral and gut microbiomes are perturbed in rheumatoid arthritis and partly normalized after treatment. Nat Med. (2015) 21:895–905. doi: 10.1038/nm.3914
33. Scher, JU, Nayak, RR, Ubeda, C, Turnbaugh, PJ, and Abramson, SB. Pharmacomicrobiomics in inflammatory arthritis: gut microbiome as modulator of therapeutic response. Nat Rev Rheumatol. (2020) 16:282–92. doi: 10.1038/s41584-020-0395-3
34. Scher, JU, Littman, DR, and Abramson, SB. Microbiome in inflammatory arthritis and human rheumatic diseases. Arthritis Rheumatol (Hoboken, NJ). (2016) 68:35–45. doi: 10.1002/art.39259
35. Artacho, A, Isaac, S, Nayak, R, Flor-Duro, A, Alexander, M, Koo, I, et al. The pretreatment gut microbiome is associated with lack of response to methotrexate in new-onset rheumatoid arthritis. Arthritis Rheumatol. (2021) 73:931–42. doi: 10.1002/art.41622
36. Chakraborti, CK. New-found link between microbiota and obesity. World J Gastrointest Pathophysiol. (2015) 6:110–9. doi: 10.4291/wjgp.v6.i4.110
37. den Besten, G, van Eunen, K, Groen, AK, Venema, K, Reijngoud, DJ, and Bakker, BM. The role of short-chain fatty acids in the interplay between diet, gut microbiota, and host energy metabolism. J Lipid Res. (2013) 54:2325–40. doi: 10.1194/jlr.R036012
38. Tailford, LE, Crost, EH, Kavanaugh, D, and Juge, N. Mucin glycan foraging in the human gut microbiome. Front Genet. (2015) 6:81. doi: 10.3389/fgene.2015.00081
39. Lee, JS, Wang, RX, Goldberg, MS, Clifford, GP, Kao, DJ, and Colgan, SP. Microbiota-sourced purines support wound healing and mucous barrier function. iScience. (2020) 23:101226. doi: 10.1016/j.isci.2020.101226
40. Novella-Navarro, M, Ruiz-Esquide, V, Torres-Ortiz, G, Chacur, CA, Tornero, C, Fernández-Fernández, E, et al. A paradigm of difficult-to-treat rheumatoid arthritis: subtypes and early identification. Clin Exp Rheumatol. (2022) 41:1114–9. doi: 10.55563/clinexprheumatol/7mscci
41. Li, H, Zhu, H, Xu, L, Xue, J, Zhao, Z, Zhong, H, et al. The characteristics and its contributing factors of refractory rheumatoid arthritis, view of the rheumatologists of China: results of a nationwide cross-sectional survey. Clin Rheumatol. (2021) 40:4029–38. doi: 10.1007/s10067-021-05687-7
42. Novella-Navarro, M, Benavent, D, Ruiz-Esquide, V, Tornero, C, Díaz-Almirón, M, Chacur, CA, et al. Predictive model to identify multiple failure to biological therapy in patients with rheumatoid arthritis. Ther Adv Musculoskelet Dis. (2022) 14:1759720X221124028. doi: 10.1177/1759720X221124028
43. Atzeni, F, Bongiovanni, S, Marchesoni, A, Filippini, M, Caporali, R, Gorla, R, et al. Predictors of response to anti-TNF therapy in RA patients with moderate or high DAS28 scores. Joint Bone Spine. (2014) 81:37–40. doi: 10.1016/j.jbspin.2013.04.005
44. Fransen, J, and van Riel, PLCM. The disease activity score and the EULAR response criteria. Rheum Dis Clin N Am. (2009) 35:745–757, vii–viii. doi: 10.1016/j.rdc.2009.10.001
45. Cho, SK, Sakai, R, Nanki, T, Koike, R, Watanabe, K, Yamazaki, H, et al. A comparison of incidence and risk factors for serious adverse events in rheumatoid arthritis patients with etanercept or adalimumab in Korea and Japan. Mod Rheumatol. (2014) 24:572–9. doi: 10.3109/14397595.2013.860695
46. Marchesoni, A, Zaccara, E, Gorla, R, Bazzani, C, Sarzi-Puttini, P, Atzeni, F, et al. TNF-alpha antagonist survival rate in a cohort of rheumatoid arthritis patients observed under conditions of standard clinical practice. Ann N Y Acad Sci. (2009) 1173:837–46. doi: 10.1111/j.1749-6632.2009.04621.x
Keywords: rheumatoid arthritis, gut microbiota, disease modifying antirheumatic drugs, Firmicutes/Bacteroidetes ratio, inflammation
Citation: Ruiz-Limón P, Mena-Vázquez N, Moreno-Indias I, Lisbona-Montañez JM, Mucientes A, Manrique-Arija S, Redondo-Rodriguez R, Cano-García L, Tinahones FJ and Fernández-Nebro A (2025) Gut dysbiosis is associated with difficult-to-treat rheumatoid arthritis. Front. Med. 11:1497756. doi: 10.3389/fmed.2024.1497756
Edited by:
Giuseppe Murdaca, University of Genoa, ItalyReviewed by:
Vinod Kumar Gupta, Mayo Clinic, United StatesFederico Diaz-Gonzalez, University of La Laguna, Spain
Junfeng Jia, Fourth Military Medical University, China
Copyright © 2025 Ruiz-Limón, Mena-Vázquez, Moreno-Indias, Lisbona-Montañez, Mucientes, Manrique-Arija, Redondo-Rodriguez, Cano-García, Tinahones and Fernández-Nebro. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Natalia Mena-Vázquez, bmF0YWxpYW1lbmF2YXpxdWV6QGdtYWlsLmNvbQ==