 Tian Chang
Tian Chang Xieli Ma
Xieli Ma Xun Gong
Xun Gong Congmin Xia
Congmin Xia Quan Jiang
Quan Jiang Rouman Zhang
Rouman Zhang
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
CLINICAL TRIAL article
Front. Med. , 11 November 2024
Sec. Rheumatology
Volume 11 - 2024 | https://doi.org/10.3389/fmed.2024.1454982
This article is part of the Research Topic Rehabilitation and Alternative Medicine in the Healthcare for Chronic Rheumatic Pain Disorders View all 15 articles
Introduction: Rheumatoid arthritis (RA) patients often experience significant hand dysfunction. Yijinjing, a traditional Chinese exercise, has been recognized for its benefits to mind–body health. This study aimed to evaluate the efficacy and safety of Yijinjing in improving hand dysfunction among individuals with RA.
Methods: This research was conducted as a single-center, outcome-blinded, randomized controlled trial. A total of 66 eligible RA participants were randomly assigned in a 1:1 ratio to either the Yijinjing exercise group (YJJG) with sessions conducted three times per week over a 12-week period or the control group (CG), which maintained ordinary activities. Various outcomes were assessed, including the Michigan Hand Outcomes Questionnaire (MHQ), handgrip strength, active range of motion (AROM), RA disease activity, the Health Assessment Questionnaire Disability Index (HAQ-DI), levels of anxiety and depression, and wrist ultrasound, all of which were collected at baseline and the week 12.
Results: At the end of the 12 weeks, the YJJG demonstrated significant improvements in MHQ scores compared to the CG (p < 0.05), alongside enhancements in handgrip strength and AROM, specifically in wrist extension, radial deviation, and metacarpophalangeal flexion (p < 0.05). Wrist ultrasound scores did not exhibit a significant increase in the YJJG, meaning no inflammation aggravation (p > 0.05). Additionally, morning stiffness duration, Disease Activity Score 28-ESR (DAS28-ESR), erythrocyte sedimentation rate (ESR), and C-reactive protein (CRP) levels showed significant improvement in the YJJG (p < 0.05). Both groups reported enhancements in quality of life, as well as reductions in anxiety and depression scores, with the YJJG displaying greater improvements overall (p < 0.05). Importantly, no adverse events or significant abnormalities in vital signs were observed in either group.
Conclusion: Yijinjing exercise may effectively enhance hand function, handgrip strength, and flexibility in RA patients with low disease activity. Furthermore, it appears to improve quality of life and reduce anxiety and depression without exacerbating joint inflammation.
Clinical trial registration: https://clinicaltrials.gov/study/NCT05527158, Identifier NCT05527158.
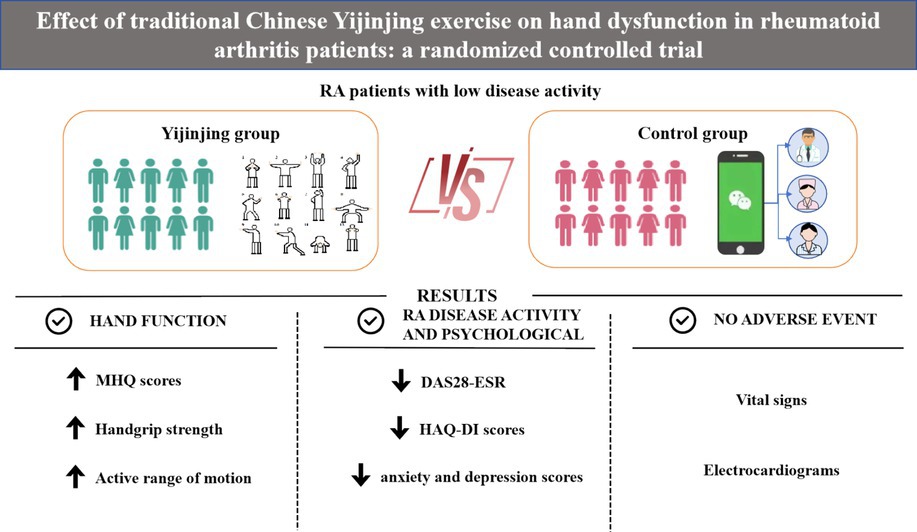
Graphical Abstract.
Rheumatoid arthritis (RA) is a chronic inflammatory disease characterized by severe disability, joint swelling, pain, and stiffness, ultimately leading to joint deformation, distortion, and a diminished quality of life (1). Approximately 0.2–1% of the global population suffers from RA, with a higher prevalence among females (2). The etiology and pathogenesis of RA remain incompletely understood. Pharmacological interventions are typically the first line of treatment. Despite advancements in biologics and disease-modifying antirheumatic drugs (DMARDs), which have significantly improved RA management in recent years, joint dysfunction-particularly in the hands-remains a major clinical challenge (3). Evidence suggests that approximately 70% of RA patients may experience bone erosion within 2 years of diagnosis (4). Furthermore, over 90% of RA cases initially manifest in the wrist and hand (5). Thus, addressing hand dysfunction in RA patients is paramount (6).
Although treat-to-target, patients fail to maintain sustained low disease activity or remission and hand dysfunction continues to plague RA patients. As a result, complementary and alternative medicine treatments for RA, such as acupuncture, physical exercise, and arthritic gloves, are gradually developed and emphasized. In the past few years, strengthening exercises for inflamed joints or flexion exercises against resistance have been questioned due to joint injury or excessive deformity concerns (7). Currently, active exercise is commonly recognized as a safe and effective treatment for RA. Professional rehabilitation guidance can alleviate dysfunction and improve quality of life in RA patients (8, 9). Consistent engagement in exercise received a strong recommendation in the 2022 American College of Rheumatology (ACR) guideline (10). Several meta-analyses have confirmed that exercise can relieve pain, improve somatic function, and enhance quality of life in RA patients, but it is still unclear what kind, how much, and how often they should take (11, 12).
Comparatively few clinical research aimed at hand function training for RA. The Strengthening and Stretching for Rheumatoid Arthritis of the Hand Trial (SARAH), an individually designed, progressive exercise program for the hand and arm, was conducted in a multicenter (n = 17), randomized, double-blind controlled trial (13). This exercise may reduce hand discomfort and strengthen hand function even if RA patients with acute small muscle atrophy and hand abnormalities (4, 14). It is also beneficial for daily life, work, and mood, potentially persisting for 12 months (15, 16). However, it is still unclear whether exercise can generate medium-and long-term benefits. It is necessary to carry out further high-quality research to investigate the benefit of exercise on hand function in RA (17).
Yijinjing is a multi-component and psychosomatic exercise based on traditional Chinese medicine theory. It is easy to learn, convenient, high-security, moderate-intensity, and combines static and dynamic movements with non-invasive external physiotherapy (18). Yi symbolizes change, Jin represents muscles, sinews, bones, and joints, and Jing means methods that integrate the body with mood (19). As a result, it offers a profitable complementary therapy for ameliorating physical function, regulating emotions, and relieving mental stress (20). Yijinjing has primarily focused on motor and cognitive function in stroke sequelae, as well as on osteoarthritis, ankylosing spondylitis, chronic schizophrenia (21, 22). Nevertheless, there are few studies on RA (23). Therefore, we conducted a randomized controlled trial to fill these gaps, with the main goal of improving hand function. We hypothesized that Yijinjing exercise would exert a positive impact on hand function in RA patients.
Participants were recruited from the rheumatology department at Guang’anmen Hospital, China Academy of Chinese Medical Sciences, from February 2022 to December 2022. The subjects met the following criteria: (1) met the 2010 ACR/European League Against Rheumatism (EULAR) classification criteria or the 1987 revised ACR classification criteria; (2) were aged 18–65, regardless of sex; (3) with low disease activity (DAS28-ESR ≤ 32); (4) with joint function in grades I to II and X-ray in stages I to II; (5) with a stable dose of DMARDs, biological agents, or glucocorticoids within 4 weeks prior to screening; (6) all patients were evaluated for hand dysfunction by a professional rheumatologist; and (7) volunteered to participate and cooperated to complete this study. The exclusion criteria were as follows: (1) had Yijinjing exercise experience within the last 3 months; (2) had severe joint deformity (eg. subluxation and severe ulnar deviation) or joint ankylosis; (3) had other diseases affecting limb function, such as trauma, fractures, infections, tumors, or congenital malformations; (4) had complications such as severe cardiovascular, brain, liver, lung, kidney, or hematopoietic system diseases; and (5) had moderate or severe cognitive impairment. All patients signed informed consent prior to baseline assessments for eligibility.
This was a 12-week single-center randomized controlled trial in parallel. Sixty-six eligible patients were randomly assigned to receive the Yijinjing exercise (the YJJG group) or usual care control (the CG group) in a 1:1 ratio. The randomization was generated through a random number table by the staff not involved in recruitment and subsequently using sealed envelopes to assign. The outcome assessors were blinded to the allocation. All outcomes were measured at baseline and 12 weeks.
The study protocol, informed consent, and case report forms (CRFs) all met the Helsinki Declaration, and the enrollment, intervention, and measurement schedule adhered to SPIRIT’s requirements. This trial protocol has been registered in ClinicalTrials (NCT05527158) and approved by the Guang’anmen Hospital Research Ethics Committee, Chinese Academy of Chinese Medical Sciences [2022-002-KY-01].
The sample size was calculated by change in the Michigan Hand Outcomes Questionnaire score. Due to the minimal clinically important difference in the MHQ score is 11.0 (24), we assumed a between-group difference of 11.0 points, and a standard deviation of 12.5, with an alpha value of 0.05, and a test power of 90%. Considering a 20% shedding rate, we eventually enrolled at least 66 participants, 33 individuals in each group. The formula is as follows.
We advised patients to maintain regular daily activities but not to initiate any other new exercise. The necessity of physical activity and at-home exercise, daily preventive measures and awareness of RA were emphasized for all participants. All patients sustained stable pharmacological therapy for RA. The CG group received routine joint rehabilitation guidance, such as energy conservation and protection, without additional exercise interventions. We established Wechat group to engage health education and monitor their compliance. The YJJG group underwent Yijinjing exercise three times a week for 12 weeks (Tuesday, Thursday, Saturday, 8:00 p.m. to 9:00 p.m.). Each practice lasted 1 h, including three integral Yijinjing exercises with a five-minute break after each exercise. The Yijinjing, compiled by the State Sports General Administration of China and consisted of 12 operational postures, was recommended as the standard intervention (Figure 1; Table 1). Professional coach with at least 5 years of experience carried out action decomposition teaching before the formal practice started. During the exercise, we paid attention to the patient’s hand function, especially flexion and extension of the wrist and interphalangeal joints. In addition, we concentrated on the center of gravity movement and assisted breathing naturally. The exercise was undertaken in the form of online Tencent meetings. The researchers evaluated the attendance of meetings and instructed patients to keep self-exercise report records. As long as the attendance record was >65% during the 3 months, the experiment was deemed complete (Supplementary Table S1). At later 12 weeks, the patients were not asked to repeat the practice at home in both groups. They can keep practice based on their own preference.
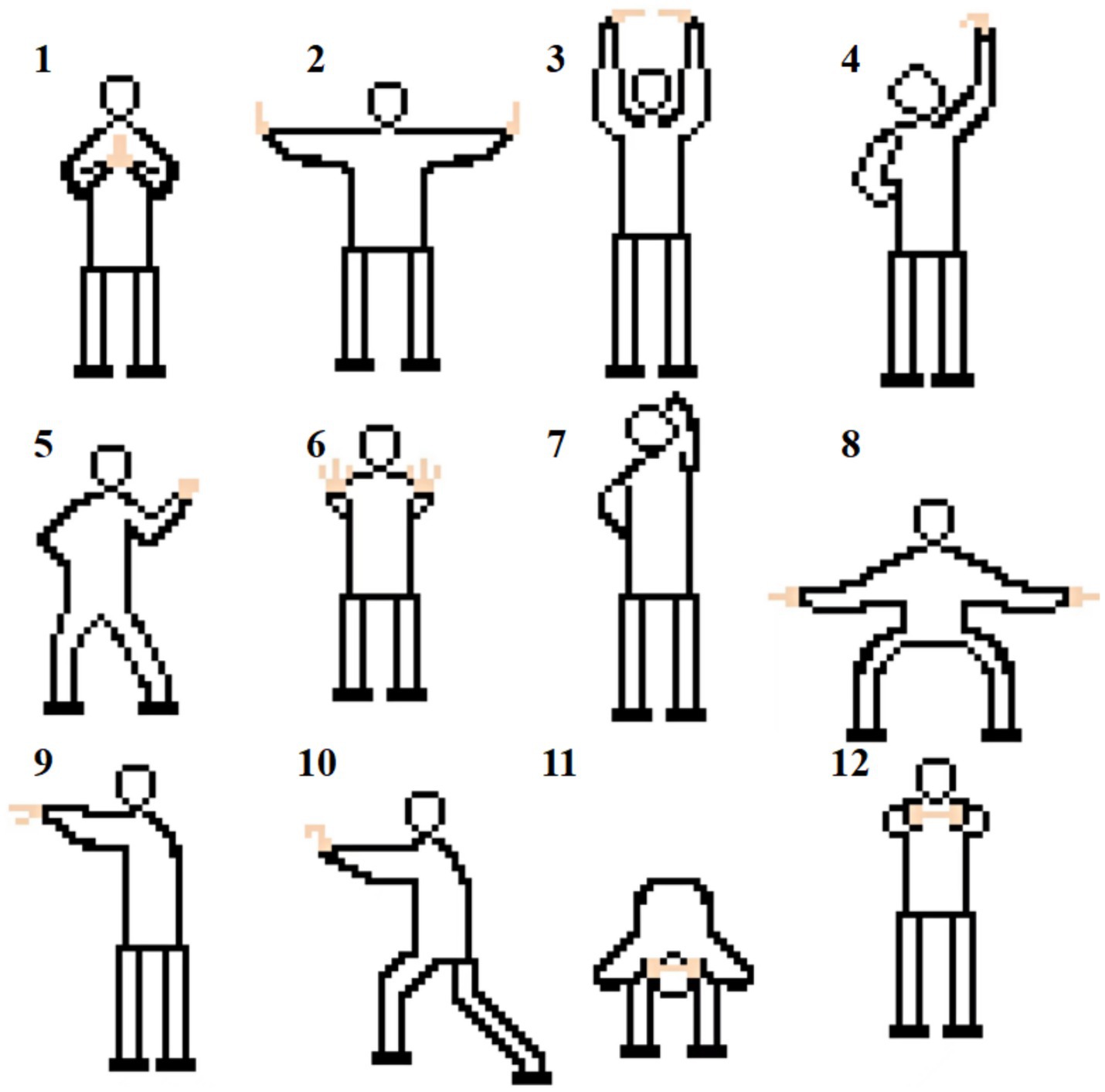
Figure 1. Twelve postures of Yijinjing exercise.
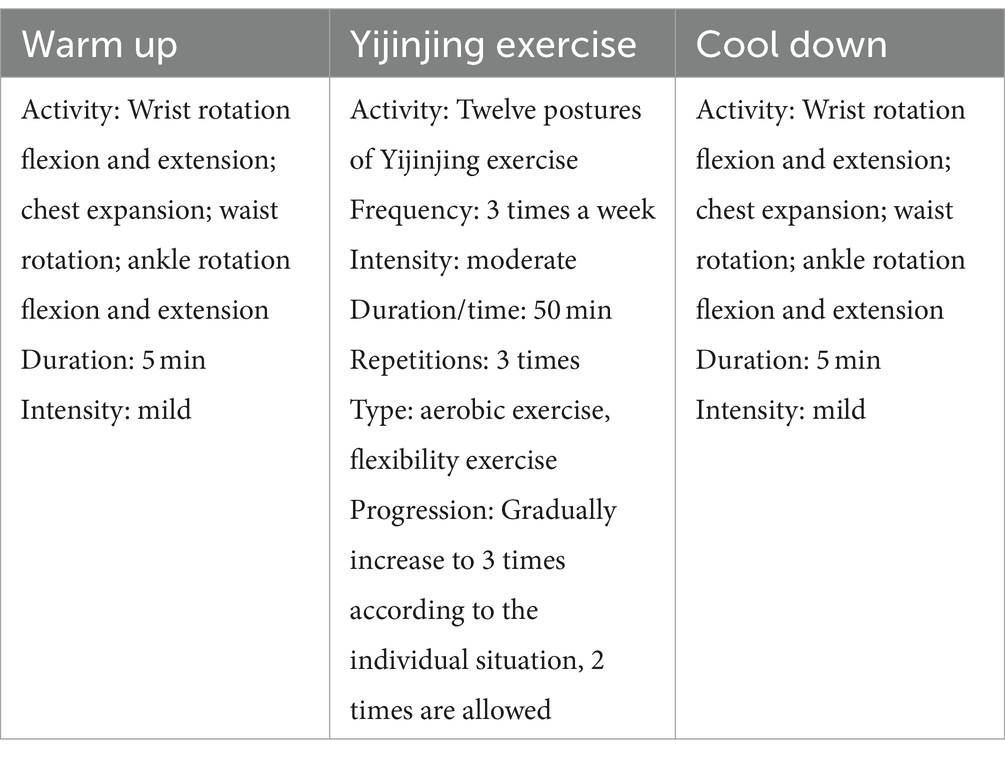
Table 1. Exercise intervention program.
The Michigan Hand Outcomes Questionnaire (MHQ) consists of 37 questions divided into the following six categories: (1) overall hand function; (2) activities of daily living; (3) work performance; (4) pain; (5) esthetics; and (6) patient satisfaction with hand function, measured individually for the left and right hands (25). The MHQ scale was chosen as the primary outcome due to its comprehensive assessment of hand function. It is an extensively used hand-specific outcome tool in clinical chronic hand illnesses with strong reliability and validity (26). It is designed to capture the patient’s subjective experience of their hand condition, which is crucial in evaluating the impact of treatments on daily life and quality of life. Furthermore, the MHQ allows for separate evaluation of the left and right hand, which is particularly beneficial in conditions where hand dominance and asymmetry in disease severity.
Handgrip strength can reflect hand strength. The use of electronic grippers is more sensitive and easier for patients with weaker grip strength (27). Hence, an electronic gripper (CAMRY, TXUT-013, Guang dong, China) was used to assess handgrip strength (kg). The subjects grabbed with the highest possible force while not suffering any pain or discomfort when seated, with their shoulders not twisted, their elbows bent at a 90-degree angle, and their forearms in a neutral position (28). It was carried out three times with an interval of 15 s, and set the average as the final result. One measurement was acceptable for those with visibly painful joints (6).
The active range of motion (AROM) reflects hand flexibility. Reduced hand ROM is closely related to patient functional disability (29). We used a protractor to judge the AROM. First, we determined the joint and fixed axis and then rotated the moving axis relative to the zero-degree position to calculate the wrist flexion, extension, ulnar deviation, radial deviation, MCP flexion, and PIP flexion angles. The subjects must use their muscular power to move.
The duration (in minutes) of morning stiffness was gauged by the patients’ self-reports. The visual analog scale (VAS) indicated the pain in RA, with 0 signifying “no pain” and 10 signifying “the worst intolerable pain” (30). We evaluated the number of swollen, painful, and deformed joints among the 28 peripheral joints. Rheumatoid factor (RF), the erythrocyte sedimentation rate (ESR), and C-reactive protein (CRP) were detected and recorded. Thus, we assessed RA disease activity using the internationally recognized DAS28-ESR.
The Health Assessment Questionnaire Disability Index (HAQ-DI) has been thoroughly validated and measured in RA (31). The scale contains 20 questions about daily activities such as dressing, grooming, arising, eating, walking, maintaining hygiene, reaching and gripping (32).
The self-rating depression scale (SDS) was used to measure the severity of depression; higher scores reflect symptom severity (33). The self-rating anxiety scale (SAS) mainly consists of 20 items to assess the intensity of anxiety.
Two professionally trained musculoskeletal ultrasound physicians evaluated the conditions of synovitis, tenosynovitis, and bone erosion on the wrist joint. According to the European League against Rheumatism-Rheumatology Outcome Measurement (EULAR-OMERACT) score (34), synovitis, tenosynovitis, and bone erosion of the same wrist joint were graded at baseline and 12 weeks.
Electrocardiograms (ECGs) were performed, along with the individuals’ vital signs (blood pressure, respiration, heart rate, and pulse), and adverse events were recorded.
SPSS 26.0 statistical software (IBM. US) was used for data analysis, and p < 0.05 was considered to indicate statistical significance. Continuous variables are described as the means ± standard deviations for normally distributed data or medians (25, 75%) for non-normally distributed data, while categorical data are expressed as frequencies and percentages. For differences between groups, an independent sample T-test (normal, homogeneity of variance) or Wilcoxon Mann–Whitney test (non-normal, heterogeneity of variance) was used for continuous data, while the Chi-square test or Fisher’ s exact test was used for categorical data and grade data. Time differences (baseline, 12 weeks) were defined as intra-subject, and the presence or absence of Yijinjing exercise was defined as between-subject factor. In terms of intra-group comparisons, the paired-sample t-test or Wilcoxon Mann–Whitney test (non-normal) was used for the continuous data, while the McNemar test or the McNemar-Bowker test was used for the categorical data.
One hundred twenty patients were screened for eligibility and 66 patients were eventually randomized. Six subjects dropped out due to loss to follow up, and 60 subjects finally completed the trial (YJJG: n = 30, CG: n = 30). The entire trial flow diagram is shown in Figure 2. 95% of subjects were female, and the mean ages were 54.80 ± 8.50 and 51.63 ± 10.63 years, respectively, which is consistent with the prevalence of RA in middle-aged and elderly females. At baseline, they were comparable between the two groups in terms of age, sex, height, weight, MHQ score, handgrip strength, AROM, RA disease activity (DAS28-ESR), ECG, and so on (p > 0.05). The medical treatment history for RA over the past 3 months was similar between the two groups. The DAS28-ESR of both groups was <3.2, and the disease activity was relatively stable (Table 2).
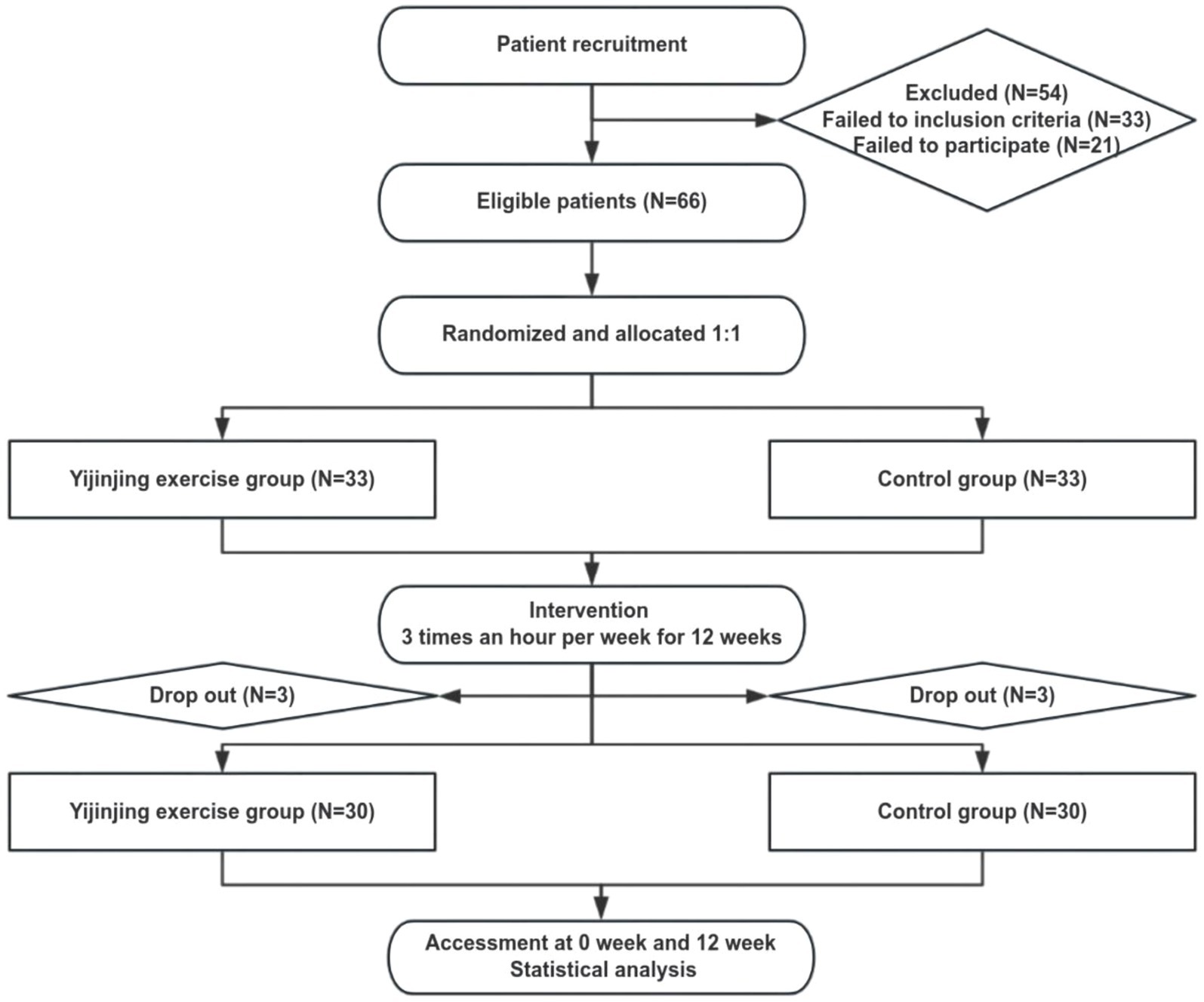
Figure 2. Participant flow diagram.
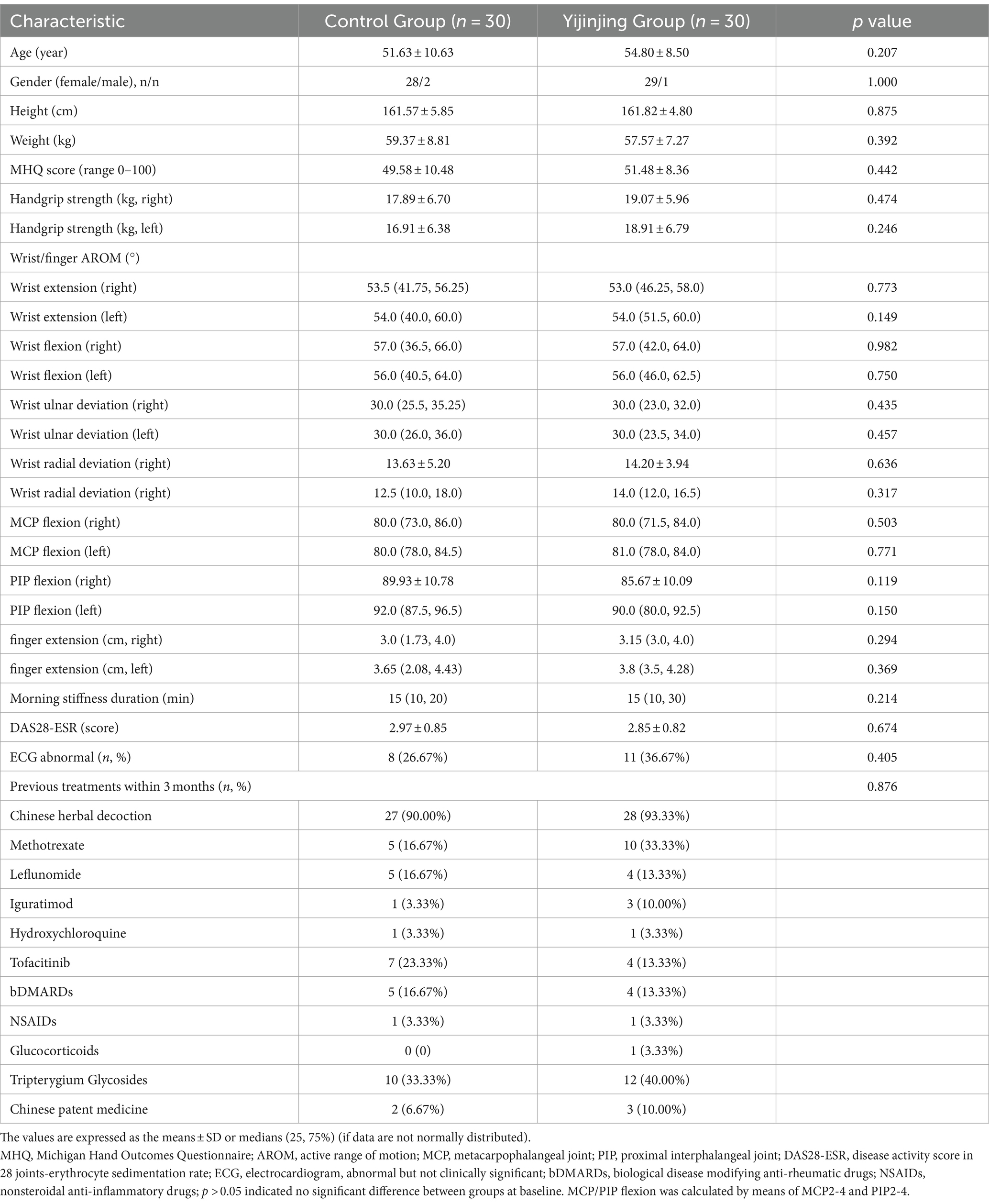
Table 2. Baseline characteristics of participants.
Hand function including the MHQ score, handgrip strength, and AROM, was definitely ameliorated in the YJJG group compared with the CG group at 12 weeks. Not only in MHQ total score, but also six MHQ sub-scales, the YJJG group performed better than the CG group, which is clinically significant (p < 0.05). In terms of handgrip strength, there was an increase more than 1.0 kg for both the left and right hands in YJJG group (p < 0.05), while the CG group did not significantly improve compared with baseline (p > 0.05). Additionally, in the YJJG, all measures of AROM significantly increased by 6–10° (p < 0.05), whereas in the CG, the increase ranged from 1 to 4° compared with baseline. Wrist extension, wrist radial deviation, and MCP flexion in the YJJG group were greater than those in the CG (p < 0.05), but no significant changes in PIP flexion, wrist ulnar deviation, and left wrist flexion were observed between the two groups (p > 0.05). The wrist ultrasound score showed a slight decrease in the YJJG and a mild increase in the CG at 12 weeks with no statistical significance (p > 0.05). Additionally, the Yijinjing exercise did not exacerbate bone erosion and inflammation (Table 3).
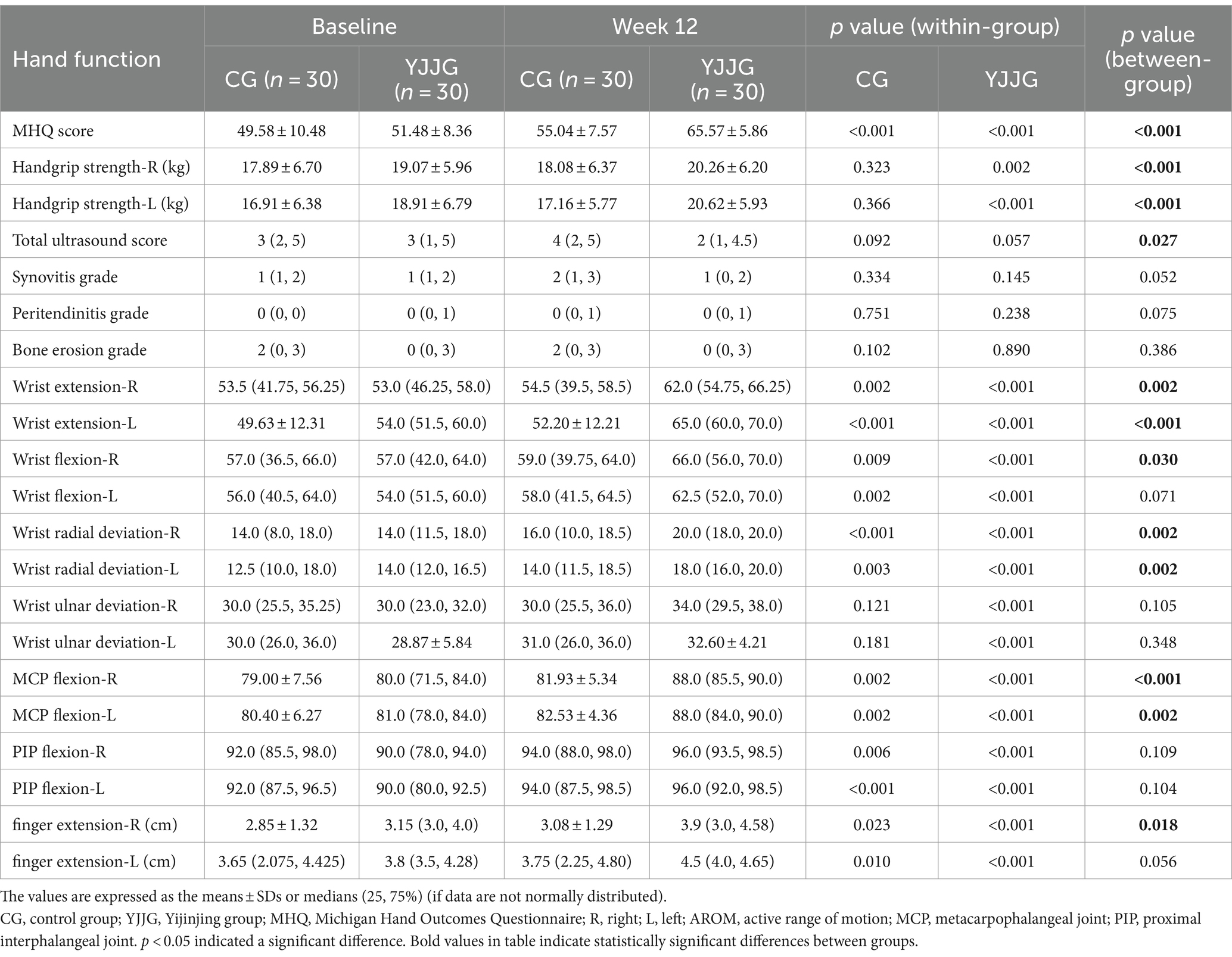
Table 3. Effect of Yijinjing on hand function.
After 12 weeks of Yijinjing exercise, the VAS score, morning stiffness duration, number of tender joints, number of swollen joints, and DAS28-ESR in the YJJG group were significantly different from baseline (p < 0.05). However, there was no significant decrease in RF, ESR, and CRP (p > 0.05). No evidence of within-group differences in the CG was found, except for the VAS score and morning stiffness minutes (p < 0.05). Compared with the CG, the VAS score, morning stiffness minutes, DAS28-ESR, ESR, and CRP in the YJJG group significantly improved (p < 0.05). More importantly, the disease activity in the YJJG turned into remission (Table 4).
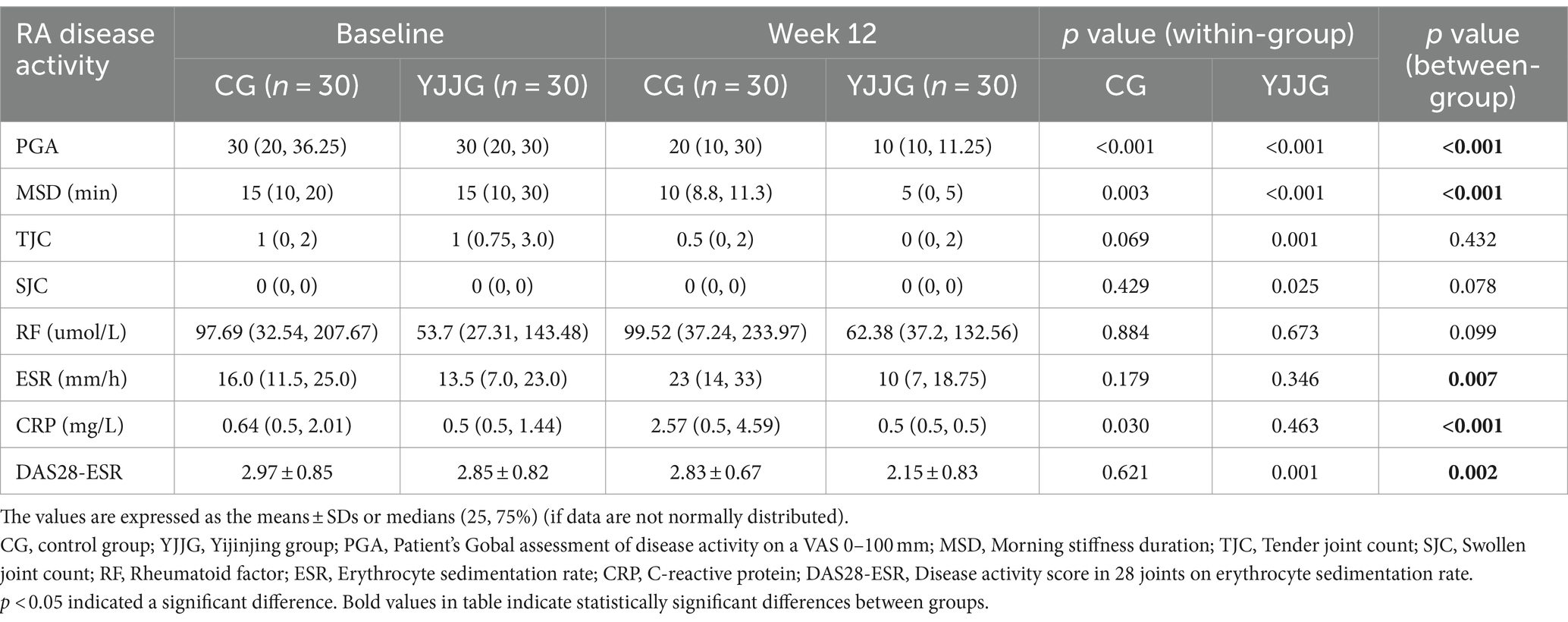
Table 4. Effect of Yijinjing on RA disease activity.
Regarding dysfunction in daily activities, we observed a decline in HAQ-DI scores in both groups compared to baseline, with the YJJG showing superior improvement (p < 0.05). In terms of mental condition, the reductions in anxiety and depression scores from baseline to week 12 were significant (p < 0.05). Furthermore, no serious adverse events were reported in either the YJJG or the CG, indicating that the YJJG was as safe as the CG (Table 5).
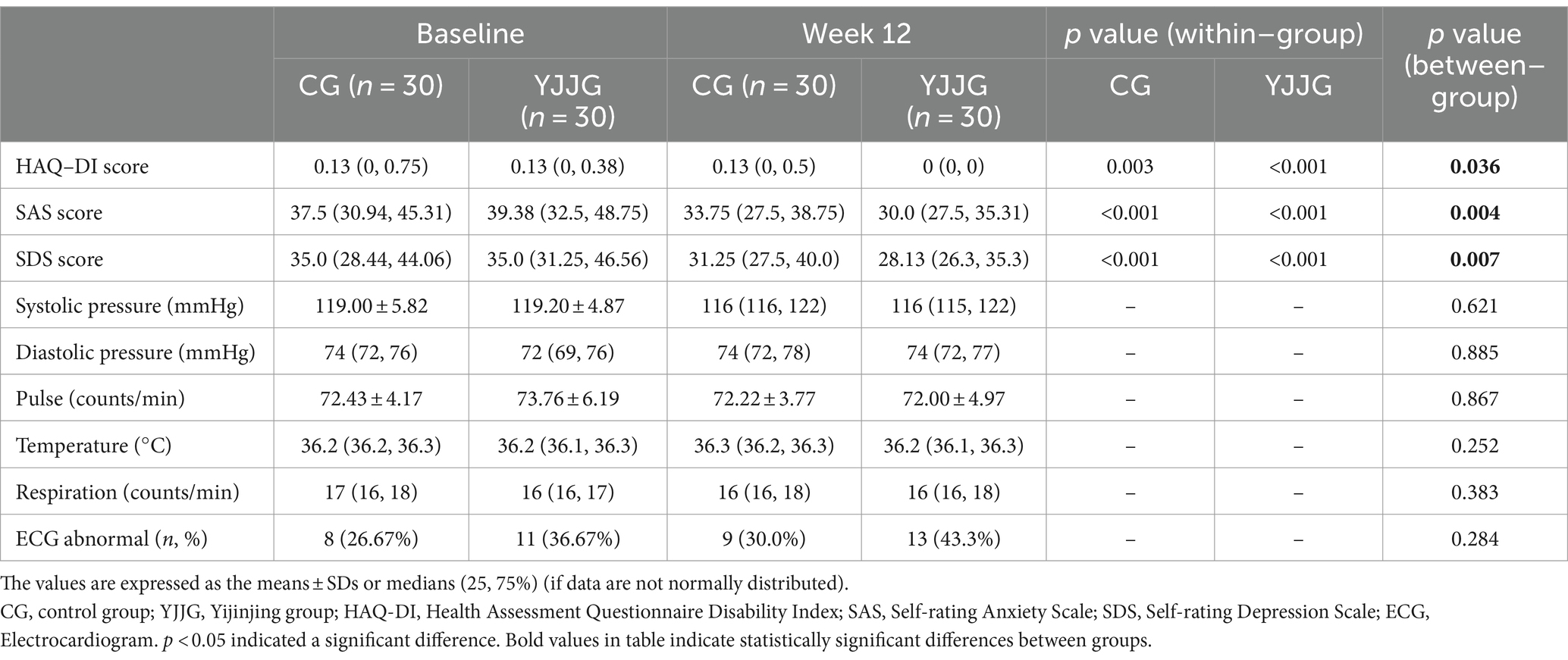
Table 5. Effect of Yijinjing on function, mental health and safety.
In 2022, the ACR recommended hand exercises to improve mobility and strength, with low certainty evidence suggesting that mind–body exercise can improve physical function. As far as we know, this is the first randomized controlled trial aimed to evaluate the effect of Yijinjing on hand dysfunction in patients with rheumatoid arthritis (RA). It showed an improvement in hand function and enhanced handgrip strength and flexibility (active range of motion) in RA patients with low disease activity with a potential to ameliorate quality of life and alleviate anxiety and depression.
Yijinjing can improve hand function in RA patients. Due to successive progressive joint erosion, RA often leads to functional disability, typically resulting in hand dysfunction (35). It showed that MHQ scores moderately correlate with disease activity, in which higher DAS28 scores tended to correlate with lower MHQ scores, indicating worse hand function (36). Our study revealed that most patients with low disease activity or remission were not satisfied with their hand function even without moderate or severe joint pain. The MHQ total and each subscale score indicated that Yijinjing exercise for 12 weeks effectively ameliorated the hand function. This finding was consistent with previous studies (4) in strengthening and stretching for rheumatoid arthritis of the hand (SARAH) exercise. The Yijinjing exercise is highly similar to the SARAH program. For example, the first posture Wei tuo xian chu requires putting your hands together before your chest and maintaining as far as possible 90° wrist extension to exercise the wrist fully. Our study preliminarily showed that Yijinjing exercise effectively improves MHQ hand function in RA patients.
Yijinjing can enhance handgrip strength and flexibility in RA patients. Handgrip strength is critical for assessing hand function and predicting disability and joint impairment in RA (37, 38). The active range of motion (AROM) reflects hand flexibility quantitatively (39). High disease activity, more pain, severe dysfunction, hand disability, and bone erosion in RA patients have been associated with low grip strength (40) and worse AROM (41). For healthy people, the grip strength in a neutral position in the dominant hand was 29.1 kg, with a wrist flexion of 79.7°, a wrist extension of 74.4°, a pronation position ulnar deviation of 32.8° and a radial deviation of 21.1° in Stacy Fan’s study (42). However, for RAs with high disease activity, the grip strength was 11.4 kg (43), with wrist flexion of 38.7°, wrist extension of 35.2°, ulnar deviation of 29.7° and radial deviation of 13.1° (29). In terms of our study, we included 95% RA with low disease activity. The grip strength at baseline was less than 20 kg, which was weaker than healthy individuals but better than RA with high disease activity, showing a similar trend in AROM, which may be related to less pain. Our study revealed that handgrip strength and AROM were significantly greater in the YJJG than CG at 12 weeks, indicating Yijinjing exercise effectively improves hand muscle strength and ameliorates hand flexibility. This finding was consistent with Mark A Williams (4), but due to the different use of grip devices, we did not measure the pinch grip force, which was one of the limitations of our study. The reason about AROM did not reach healthy can be explained as follows. First, this study was carried out in RA patients with constant hand dysfunction. Second, even though the RA is relatively stable, there still exists subclinical synovitis under ultrasound or MRI. In addition, this may be related to insufficient length of intervention. Besides, there is no standard method to measure RA joint mobility. Naoto Ienaga (44) developed a smartphone-based system to assess the AROM of wrist. Whose accuracy was within a clinically usable error range. The Yijinjing exercise contains multiple hand or wrist movements to effectively promote muscular strength and dexterity in hand.
Yijinjing did not increase inflammation in RA patients. As recommended by the EULAR (45), the semi-quantitative grading of musculoskeletal ultrasound is more sensitive for diagnosing subclinical synovitis in wrist and hand (46). This study revealed that subclinical synovitis and tenosynovitis were present in both groups at baseline. Although no significant difference was found between two groups, a gradual improvement was noted in YJJG, indicating that Yijinjing does not exacerbate synovitis and is safe for RA. A prospective intervention study made clear that strengthening exercise is beneficial for enhancing the cross-sectional area of the rectus femoris via ultrasonography (47). In addition, training did not increase blood flow on ultrasound Doppler induced by inflammation, indicating that it had no adverse effect on RA (48). Therefore, it is necessary to introduce ultrasound as an evaluation to monitor the safety of exercise in RA. If the ultrasound score significantly increases, it hints at reducing intensity or stopping temporarily.
The morning stiffness duration, patient global assessment of disease activity, TJC, SJC, RF, CRP, and ESR are associated with RA disease activity. DAS28-ESR < 2.6, as a remission criterion, may be appropriate for most patients in the clinic (49). At 12 weeks the Yijinjing further reduced the disease activity of stable RA, gradually run up to remission, and did not aggravate joint inflammation. The effect of aerobic exercise on the prevention and treatment of RA dysfunction and disease activity has been gradually recognized. A study affirmed that aerobic and resistance exercise improved physical fitness in terms of aerobic capacity, endurance, and strength in older adults with RA (50). Tai Chi is safe for RA patients, but more evidence is needed to improve physical function and pain with active RA (51). Future researchers could attach importance to exercise in ameliorating function with moderate/severe disease activity RA. Exercise not only improved function but also controled inflammation, and the best duration and intensity of exercise should be explored in the future.
Yijinjing is beneficial for mind–body function in RA patients. RA with dysfunction often affects quality of life (52). Depression and anxiety are common comorbidities of RA, with the prevalence of depression varying from 14 to 48% (53), and the prevalence of anxiety was 62.1%, which is even greater than depression (54). Therefore, we should not only control the disease activity but also pay attention to improving quality of life and mental health. It showed that the HAQ-DI in the YJJG as well as anxiety and depression scores were obviously reduced in our study. During the follow-up, most patients said they were willing to exercise, but they were afraid the strenuous exercise would aggravate joint disorder, and they were irritable or depressed in the long term, which not only affected mental health but also further influenced body function. Yijinjing exercise made the patients sweat slightly, relaxed mind and body, and patients were willing to maintain. This study provided a rehabilitation treatment for RA patients with psychosomatic benefits.
Rheumatoid arthritis primarily presents as symmetric joint swelling, pain, and stiffness, most commonly affecting the hands and wrists, and can lead to joint deformity and loss of function. Yijinjing exercise contains a lot of fine hand movements, and acts on muscles, sinews, bones, and joints. It helps promote blood circulation, improve finger flexibility and coordination, and alleviate symptoms such as morning stiffness, localized inflammation, and pain. This contributes to maintain hand function, address motion difficulties caused by arthritis, and enhance the patient’s quality of life. Additionally, Yijinjing exercise can help reduce psychological stress and boost the patient’s confidence in managing the disease. Thus, Yijinjing offers a holistic approach, improving not just hand function but also overall well-being and mental health. It combines gentle movements with meditation and breathing techniques, which may lead to better compliance compared to isolated functional exercises. Moreover, Yijinjing appears to be safe for RA patients, without exacerbating inflammation.
Due to outbreak of COVID-19 epidemic, we choose instruct and monitor practice through online Tencent meetings via virtual mode over the offline face to face. It showed the adherence is acceptable. Online practice breaks the geographical limitations, saving patients expenses and time when seeking face to face care. Additionally, online practice supports simultaneous participation for multiple individuals, which can enhance patient engagement, improve compliance, and boost the effect.
Our study adds the growing literature about the cost-effective and non-toxic interventions to help improve the hand function in RA. However, it suffers from some limitations. First, the participant sample size is low that more data is required from more highly powered studies. Second, our study was only single-blinded because the characteristic of the intervention which means we could not control for non-specific effects. Third, there was no follow-up period, so we have no idea how quickly participants returned to baseline levels of all the study parameters. Besides, our study focused on RA patients with low disease activity. Subsequent research can further explore the effect in RA with medium and high disease activity. Last, our study were lack of an active control group. In the future, further multi-center RCTs should be carried out, and a active control, such as SARAH, could be set up to obtain more evidence.
In conclusion, Yijinjing exercise can improve hand function and enhance handgrip strength and flexibility in RA patients with low disease activity while ameliorating quality of life and alleviating anxiety and depression while safe and not aggravating joint inflammation.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Our study were approved by the Ethics Committee of Guang’anmen Hospital, Chinese Academy of Traditional Chinese Medicine. We did contain identifiable human images. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
TC: Conceptualization, Investigation, Supervision, Writing – original draft, Writing – review & editing. XM: Formal analysis, Writing – original draft, Writing – review & editing. XG: Conceptualization, Supervision, Writing – review & editing. CX: Conceptualization, Supervision, Writing – review & editing. QJ: Conceptualization, Funding acquisition, Supervision, Writing – review & editing. RZ: Conceptualization, Funding acquisition, Supervision, Writing – original draft, Writing – review & editing.
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This study was supported by grants from Guang’anmen Hospital, the China Academy of Chinese Medical Sciences (grant no. 2019s459) and the National Natural Science Foundation of China (82230121). All funders will play no role in the research design, data gathering, analysis, interpretation, or manual writing.
We would like to thank the participating doctors and health professionals at the Department of Rheumatology, Guang’anmen Hospital, Chinese Academy of Traditional Chinese Medicine.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2024.1454982/full#supplementary-material
RA, rheumatoid arthritis; VAS, visual analog scale; HAQ-DI, Health Assessment Questionnaire Disability Index; DMARDs, disease-modifying anti-rheumatic drugs; EULAR, European League Against Rheumatism; SARAH, Strengthening and Stretching for Rheumatoid Arthritis of the Hand Trial; RCT, randomized controlled trial; MHQ, Michigan Hand Outcomes Questionnaire; AROM, active range of motion of joints; SJC, swollen joint count; TJC, tender joint count; SAS, self-rating anxiety scale; SDS, self-rating depression scale; ECG, electrocardiogram; US, ultrasonography; ACR, American College of Rheumatology; CRF, case report form.
1. Sparks, JA. Rheumatoid arthritis. Ann Intern Med. (2019) 170:ITC1–ITC16. doi: 10.7326/AITC201901010
2. Smolen, JS, Aletaha, D, Barton, A, Burmester, GR, Emery, P, Firestein, GS, et al. Rheumatoid arthritis. Nat Rev Dis Primers. (2018) 4:18001. doi: 10.1038/nrdp.2018.1
3. Horsten, NC, Ursum, J, Roorda, LD, van Schaardenburg, D, Dekker, J, and Hoeksma, AF. Prevalence of hand symptoms, impairments and activity limitations in rheumatoid arthritis in relation to disease duration. J Rehabil Med. (2010) 42:916–21. doi: 10.2340/16501977-0619
4. Williams, MA, Williamson, EM, Heine, PJ, Nichols, V, Glover, MJ, Dritsaki, M, et al. Strengthening and stretching for rheumatoid arthritis of the hand (SARAH). A randomised controlled trial and economic evaluation. Health Technol Assess. (2015) 19:1–222. doi: 10.3310/hta19190
5. Bergstra, SA, Murgia, A, Te Velde, AF, and Caljouw, SR. A systematic review into the effectiveness of hand exercise therapy in the treatment of rheumatoid arthritis. Clin Rheumatol. (2014) 33:1539–48. doi: 10.1007/s10067-014-2691-2
6. Rodríguez-Sánchez-Laulhé, P, Luque-Romero, LG, Blanquero, J, Suero-Pineda, A, Biscarri-Carbonero, Á, Barrero-García, FJ, et al. A mobile app using therapeutic exercise and education for self-management in patients with hand rheumatoid arthritis: a randomized controlled trial protocol. Trials. (2020) 21:777. doi: 10.1186/s13063-020-04713-4
7. Filairea, E, and Toumib, H. Reactive oxygen species and exercise on bone metabolism: friend or enemy? Joint Bone Spine. (2012) 79:341–6. doi: 10.1016/j.jbspin.2012.03.007
8. Aletaha, D, Neogi, T, Silman, AJ, Funovits, J, Felson, DT, Bingham, CO, et al. 2010 rheumatoid arthritis classification criteria: an American College of Rheumatology/European League Against Rheumatism collaborative initiative. Ann Rheum Dis. (2010) 69:1580–8. doi: 10.1136/ard.2010.138461
9. Peter, WF, Swart, NM, Meerhoff, GA, and Vliet Vlieland, TPM. Clinical practice guideline for physical therapist Management of People with Rheumatoid Arthritis. Phys Ther. (2021) 101:pzab 127. doi: 10.1093/ptj/pzab127
10. England, BR, Smith, BJ, Baker, NA, Barton, JL, Oatis, CA, Guyatt, G, et al. 2022 American College of Rheumatology Guideline for exercise, rehabilitation, diet, and additional integrative interventions for rheumatoid arthritis. Arthritis Rheumatol. (2023) 75:1299–311. doi: 10.1002/art.42507
11. Hu, H, Xu, A, Gao, C, et al. The effect of physical exercise on rheumatoid arthritis: an overview of systematic reviews and meta-analysis. J Adv Nurs. (2021) 77:506–22. doi: 10.1111/jan.14574
12. Sobue, Y, Kojima, T, Ito, H, Nishida, K, Matsushita, I, Kaneko, Y, et al. Does exercise therapy improve patient-reported outcomes in rheumatoid arthritis? A systematic review and meta-analysis for the update of the 2020 JCR guidelines for the management of rheumatoid arthritis. Mod Rheumatol. (2022) 32:96–104. doi: 10.1080/14397595.2021.1886653
13. Lamb, SE, Williamson, EM, Heine, PJ, Adams, J, Dosanjh, S, Dritsaki, M, et al. Exercises to improve function of the rheumatoid hand (SARAH): a randomised controlled trial. Lancet. (2015) 385:421–9. doi: 10.1016/S0140-6736(14)60998-3
14. Kjeken, I. A tailored hand exercise program improves function of the rheumatoid hand. J Physiother. (2015) 61:96. doi: 10.1016/j.jphys.2015.02.007
15. Nichols, VP, Williamson, E, Toye, F, and Lamb, SE. A longitudinal, qualitative study exploring sustained adherence to a hand exercise programme for rheumatoid arthritis evaluated in the SARAH trial. Disabil Rehabil. (2017) 39:1856–63. doi: 10.1080/09638288.2016.1212111
16. Williamson, E, McConkey, C, Heine, P, Dosanjh, S, Williams, M, and Lamb, SE. Hand exercises for patients with rheumatoid arthritis: an extended follow-up of the SARAH randomised controlled trial. BMJ Open. (2017) 7:e013121. doi: 10.1136/bmjopen-2016-013121
17. Williams, MA, Srikesavan, C, Heine, PJ, Bruce, J, Brosseau, L, Hoxey-Thomas, N, et al. Exercise for rheumatoid arthritis of the hand. Cochrane Database Syst Rev. (2018) 2018:CD003832. doi: 10.1002/14651858.CD003832.pub3
18. Zhang, S, Guo, G, Li, X, Yao, F, Wu, Z, Zhu, Q, et al. The effectiveness of traditional Chinese Yijinjing qigong exercise for the patients with knee osteoarthritis on the pain, dysfunction, and mood disorder: a pilot randomized controlled trial. Front Med. (2022) 8:792436. doi: 10.3389/fmed.2021.792436
19. Chen, Y, Ma, Y, Zhang, Z, Zhang, Y, and Jia, J. The efficacy and safety of Yijinjing exercise in the adjuvant treatment of ankylosing spondylitis: a protocol of randomized controlled trial. Medicine. (2021) 100:e27109. doi: 10.1097/MD.0000000000027109
20. Cheng, Z, Chen, Z, Xie, F, Guan, C, Gu, Y, Wang, R, et al. Efficacy of Yijinjing combined with Tuina for patients with non-specific chronic neck pain: study protocol for a randomized controlled trial. Trials. (2021) 22:586. doi: 10.1186/s13063-021-05557-2
21. Xue, X, Jin, XM, Luo, KL, Liu, XH, Zhang, L, and Hu, J. Effectiveness of Yijinjing on cognitive functions in post-stroke patients with mild cognitive impairment: study protocol for a randomized controlled trial. Trials. (2021) 22:265. doi: 10.1186/s13063-021-05220-w
22. Gao, H, Luo, C, Tu, SJ, Lu, RP, Jiang, LN, Qiao, HJ, et al. The effect of Yijinjing on the cognitive function of patients with chronic schizophrenia. Front Psych. (2021) 12:739364. doi: 10.3389/fpsyt.2021.739364
23. Fang, L. Study on the improvement of the function of affected limbs in patients with rheumatoid arthritis by fitness qigong-Yi Jin Jing. Beijing: Beijing Sport University (2013).
24. Shauver, MJ, and Chung, KC. The minimal clinically important difference of the Michigan hand outcomes questionnaire. J Hand Surg Am. (2009) 34:509–14. doi: 10.1016/j.jhsa.2008.11.001
25. Jayaram, M, Wang, C, Wang, L, and Chung, KC. Validating the Michigan hand outcomes questionnaire in patients with rheumatoid arthritis using Rasch analysis. PLoS One. (2021) 16:e0254984. doi: 10.1371/journal.pone.0254984
26. Chung, KC, Pillsbury, MS, Walters, MR, and Hayward, RA. Reliability and validity testing of the Michigan hand outcomes questionnaire. J Hand Surg. (1998) 23:575–87. doi: 10.1016/S0363-5023(98)80042-7
27. Hogrel, JY. Grip strength measured by high precision dynamometry in healthy subjects from 5 to 80 years. BMC Musculoskelet Disord. (2015) 16:139. doi: 10.1186/s12891-015-0612-4
28. Shiratori, AP, Iop Rda, R, Borges Júnior, NG, Domenech, SC, and Gevaerd Mda, S. Evaluation protocols of hand grip strength in individuals with rheumatoid arthritis: a systematic review. Rev Bras Reumatol. (2014) 54:140–7. doi: 10.1016/j.rbre.2014.03.009
29. Zhang, L, Cao, H, Zhang, Q, Fu, T, Yin, R, Xia, Y, et al. Motion analysis of the wrist joints in Chinese rheumatoid arthritis patients: a cross-sectional study. BMC Musculoskelet Disord. (2018) 19:270. doi: 10.1186/s12891-018-2146-z
30. Massy-Westropp, N, Ahern, M, and Krishnan, J. A visual analogue scale for assessment of the impact of rheumatoid arthritis in the hand: validity and repeatability. J Hand Ther. (2005) 18:30–3. doi: 10.1197/j.jht.2004.10.003
31. Tuominen, R, Möttönen, T, Suominen, C, Vahlberg, T, and Tuominen, S. Relative importance of the functional abilities comprising health assessment questionnaire disability index among rheumatoid arthritis patients. Rheumatol Int. (2010) 30:1477–82. doi: 10.1007/s00296-009-1176-0
32. Carter, JD, Lodhi, AB, Nagda, SR, Ricca, L, Ward, C, Traina, E, et al. Determining rheumatologists' accuracy at assessing functional disability in rheumatoid arthritis patients using the health assessment questionnaire-disability index. J Rheumatol. (2007) 34:958–63.
33. Geng, Y, Gao, T, Zhang, X, Wang, Y, and Zhang, Z. The association between disease duration and mood disorders in rheumatoid arthritis patients. Clin Rheumatol. (2022) 41:661–8. doi: 10.1007/s10067-021-05967-2
34. Terslev, L, Naredo, E, Aegerter, P, Wakefield, RJ, Backhaus, M, Balint, P, et al. Scoring ultrasound synovitis in rheumatoid arthritis: a EULAR-OMERACT ultrasound task force-part 2: reliability and application to multiple joints of a standardised consensus-based scoring system. RMD Open. (2017) 3:e000427. doi: 10.1136/rmdopen-2016-000427
35. Kroon, FPB, Boersma, A, Boonen, A, van Beest, S, Damman, W, van der Heijde, D, et al. Performance of the Michigan hand outcomes questionnaire in hand osteoarthritis. Osteoarthr Cartil. (2018) 26:1627–35. doi: 10.1016/j.joca.2018.07.018
36. Durmus, D, Uzuner, B, Durmaz, Y, Bilgici, A, and Kuru, O. Michigan hand outcomes questionnaire in rheumatoid arthritis patients: relationship with disease activity, quality of life, and handgrip strength. J Back Musculoskelet Rehabil. (2013) 26:467–73. doi: 10.3233/BMR-130408
37. Higgins, SC, Adams, J, and Hughes, R. Measuring hand grip strength in rheumatoid arthritis. Rheumatol Int. (2018) 38:707–14. doi: 10.1007/s00296-018-4024-2
38. Özeri, Z, Çakýt, BD, Taþkýn, S, et al. The relationships among functional impairment, disability and articular damage in rheumatoid hand. J Phys Med Rehabil Sci. (2008) 2:53–8.
39. Yayama, T, Kobayashi, S, Kokubo, Y, Inukai, T, Mizukami, Y, Kubota, M, et al. Motion analysis of the wrist joints in patients with rheumatoid arthritis. Mod Rheumatol. (2007) 17:322–6. doi: 10.3109/s10165-007-0590-y
40. Palamar, D, Er, G, Terlemez, R, Ustun, I, Can, G, and Saridogan, M. Disease activity, handgrip strengths, and hand dexterity in patients with rheumatoid arthritis. Clin Rheumatol. (2017) 36:2201–8. doi: 10.1007/s10067-017-3756-9
41. Navarro-Compán, V, Landewé, R, Provan, SA, et al. Relationship between types of radiographic damage and disability in patients with rheumatoid arthritis in the EURIDISS cohort: a longitudinal study. Rheumatology. (2015) 54:83–90. doi: 10.1093/rheumatology/keu284
42. Fan, S, Cepek, J, Symonette, C, Ross, D, Chinchalkar, S, and Grant, A. Variation of grip strength and wrist range of motion with forearm rotation in healthy young volunteers aged 23 to 30. J Hand Microsurg. (2019) 11:88–93. doi: 10.1055/s-0038-1676134
43. Žura, N, Vukorepa, M, Jurak, I, Perić, P, Botonjić, J, Matijević, A, et al. Decrease in handgrip strength in rheumatoid arthritis (RA): is there a sex-related difference? Rheumatol Int. (2021) 41:1795–802. doi: 10.1007/s00296-021-04959-4
44. Ienaga, N, Fujita, K, Koyama, T, Sasaki, T, Sugiura, Y, and Saito, H. Development and user evaluation of a smartphone-based system to assess range of motion of wrist joint. J Hand Surg Glob Online. (2020) 2:339–42. doi: 10.1016/j.jhsg.2020.09.004
45. Colebatch, AN, Edwards, CJ, Østergaard, M, van der Heijde, D, Balint, PV, D'Agostino, MA, et al. EULAR recommendations for the use of imaging of the joints in the clinical management of rheumatoid arthritis. Ann Rheum Dis. (2013) 72:804–14. doi: 10.1136/annrheumdis-2012-203158
46. Huang, Y, Liu, KJ, Chen, GW, Liu, JF, Mo, FQ, and Xie, YH. Diagnostic value of semi-quantitative grading of musculoskeletal ultrasound in wrist and hand lesions of subclinical synovitis in rheumatoid arthritis. Am J Nucl Med Mol Imaging. (2022) 12:25–32.
47. Sul, B, Lee, KB, Joo, YB, Hong, BY, Kim, JS, Kim, KJ, et al. Twelve weeks of strengthening exercise for patients with rheumatoid arthritis: a prospective intervention study. J Clin Med. (2020) 9:2792. doi: 10.3390/jcm9092792
48. Ellegaard, K, Torp-Pedersen, S, Lund, H, Pedersen, K, Henriksen, M, Danneskiold-Samsøe, B, et al. The effect of isometric exercise of the hand on the synovial blood flow in patients with rheumatoid arthritis measured by color Doppler ultrasound. Rheumatol Int. (2013) 33:65–70. doi: 10.1007/s00296-011-2314-z
49. Ramírez, J, Inciarte-Mundo, J, Cuervo, A, Celis, R, Ruiz-Esquide, V, Castellanos-Moreira, R, et al. Comparable long-term outcomes between DAS28-ESR remission criteria and ACR/EULAR definitions in patients with established rheumatoid arthritis. Clin Rheumatol. (2021) 40:2665–72. doi: 10.1007/s10067-021-05603-z
50. Lange, E, Kucharski, D, Svedlund, S, Svensson, K, Bertholds, G, Gjertsson, I, et al. Effects of aerobic and resistance exercise in older adults with rheumatoid arthritis: a randomized controlled trial. Arthritis Care Res. (2019) 71:61–70. doi: 10.1002/acr.23589
51. Wu, H, Wang, Q, Wen, G, Wu, J, and Wang, Y. The effects of tai chi on physical function and safety in patients with rheumatoid arthritis: a systematic review and meta-analysis. Front Physiol. (2023) 14:1079841. doi: 10.3389/fphys.2023.1079841
52. Rosa-Gonçalves, D, Bernardes, M, and Costa, L. Quality of life and functional capacity in patients with rheumatoid arthritis - cross-sectional study. Reumatol Clin. (2018) 14:360–6. doi: 10.1016/j.reuma.2017.03.002
53. Matcham, F, Rayner, L, and Steer, S. The prevalence of depression in rheumatoid arthritis: a systematic review and meta-analysis. Rheumatology. (2013) 52:2136–48. doi: 10.1093/rheumatology/ket169
Keywords: rheumatoid arthritis, hand function, Yijinjing exercise, randomized controlled trial, Michigan Hand Outcomes Questionnaire
Citation: Chang T, Ma X, Gong X, Xia C, Jiang Q and Zhang R (2024) Effect of traditional Chinese Yijinjing exercise on hand dysfunction in rheumatoid arthritis patients: a randomized controlled trial. Front. Med. 11:1454982. doi: 10.3389/fmed.2024.1454982
Edited by:
Ching-Mao Chang, Taipei Veterans General Hospital, TaiwanReviewed by:
Surabhi Gautam, Emory University, United StatesCopyright © 2024 Chang, Ma, Gong, Xia, Jiang and Zhang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Rouman Zhang, emhhbmdyb3VtYW5AMTI2LmNvbQ==; Quan Jiang, ZG9jdG9yanFAMTI2LmNvbQ==
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.