 Sung-Heui Bae
Sung-Heui Bae- College of Nursing, Graduate Program in System Health Science and Engineering, Ewha Womans University, Seoul, Republic of Korea
Objectives: High nurse turnover during nursing shortages can contribute to missed nursing care. This study investigated the prevalence of missed nursing care and how nurse turnover affects missed nursing care.
Methods: A cross-sectional design was adopted to collect data from a convenience sample of nurses working in general hospitals in South Korea. Six-month turnover rates (0%, 1–14%, 15–22%, and 23–50%) and 24 missed nursing care activities were measured. A multivariate regression analysis was performed to examine the relationship between nurse turnover and missed nursing care, after controlling for nurse and work-related characteristics.
Results: The final sample was 264 nurses. The mean six-month turnover rate was 15.49%. Seven activities (turning patient every 2 h, attending interdisciplinary care conference, ambulation, patient bathing/skin care, emotional support, mouth care, full documentation) had a missed care prevalence of 30% or higher. Nurses in units with moderate turnover rates (15 and 22%) reported more missed nursing care than those in units with zero turnover.
Conclusion: Nurse turnover increases missed nursing care, highlighting the adverse effects of nurse turnover on care processes. Consequently, hospitals and governments should implement policy changes and strategies to prevent nurse turnover.
Introduction
Missed nursing care—the omission of the required care by nurses (1)—can be partial, complete, or delayed. When time is limited, nurses may simultaneously provide multiple types of care while omitting others (2). A review reported that at least 75% of nurses missed care (3). Missed nursing care is more likely in work environments with fewer resources, such as those with poor staffing levels (4–6). When nurses care for several patients, they are more likely to miss the necessary care activities as compared to their counterparts. Moreover, patient characteristics such as turnover and acuity are associated with increased missed nursing care (5).
Missed nursing care affects nurses’ job outcomes and patient outcomes. Higher levels of missed nursing care are related to lower job satisfaction and a greater intent to leave (2). When nurses encounter situations in which some required care was omitted, they may experience inner conflicts with professional standards (7), which can lead to job dissatisfaction (2). Further, they may want to leave their positions. Missed nursing care affects patient mortality (8), safety (2, 9), and patients’ satisfaction/dissatisfaction (10), thereby undermining the quality of patient care.
Male and female nurses report different levels of missed nursing care (11). Further, nurses with more work experience perceive higher levels of missed care than those with less work experience (11). Nurses’ workload (12, 13), overtime work (14) and inadequate staffing perceived by nurses (2, 15) also contribute to missed nursing care. Perceived staffing adequacy by both patients and nurses is negatively associated with missed nursing care, specifically concerning communication (16). A systematic review revealed that lower nurse staffing levels are associated with missed nursing care (3, 17). Hospital size and unit type are also associated with missed nursing care (2), and staffing levels might negatively affect nurses’ health and lead to missed nursing care (18). A previous study identified a correlation between presenteeism and missed nursing care, highlighting its significant impact of on quality of care (19). A recent study found a negative relationship between work environment and missed nursing care (14, 20). Further, a favorable nurse practice environment was related to a lower frequency of missed nursing care (21). Team work is another critical factor contributing to missed nursing care (22).
In South Korea, the nurse turnover rate was 12.4%, while that of newly licensed registered nurses was 42.7% (23). A recent study in South Korea (2) reported that nurses, on average, missing 8.9 of 24 nursing activities with 10 activities exhibiting a prevalence of missed care of 50% of higher (3). Such high nurse turnover can lead to longer working hours and a higher nurse-patient ratio. Consequently, nurses may want to leave their positions, perpetuating a nursing shortage-turnover cycle. Nurses working in units with high turnover rates could experience frequent adjustments and spend more time supervising new staff members (24). They may also need to care for more patients (25), potentially leading to teamwork deterioration (22) and difficulty in complying with patient safety guideline (21), resulting in frequently missed nursing care. Despite the apparent relationship between high turnover and missed nursing care, the relationship between nurse turnover and missed nursing care has received scant research attention. It is crucial to examine the relationship between nurse turnover and missed nursing care to elucidate the underlying mechanism of the impact of nurse turnover on care process.
Aims
This study investigated the prevalence of missed nursing care and how nurse turnover affects missed nursing care. The findings provide information about the impact of nurse turnover on the care processes, which informs policies and strategies to prevent nurse turnover and missed nursing care.
Methods
Study design, sample, and data collection
This cross-sectional study examined the prevalence of missed nursing care and how nurse turnover affects missed nursing care. Convenience sampling was used to collect data from nurses working in medical and surgical nursing units of acute care hospitals. Data were collected between July and September 2022. Only nurses who provided direct nursing care and worked in the current unit for at least 6 months were included.
From the registry of hospitals in Korea, 270 general hospitals with 201–1,000 beds in South Korea were invited to participate. Each hospital received information about the current study. Among 270 general hospitals, 35 agreed to participate. An online survey was administered to nurses and nurse managers in these hospitals. In total, 397 nurses and nurse managers in 35 hospitals responded to the online survey. Based on the inclusion criteria in the current study, participants were excluded if they had worked in the current unit for less than 6 months (n = 29), had not worked in medical or surgical units (n = 45), failed to answer more than 70% of the survey questionnaires (n = 26), or were nurse managers (n = 33). The survey focused on missed nursing care of staff nurses who provide direct nursing care, therefore, it excluded nurse managers who do not fit this criterion. Thus, data were analyzed from 264 staff nurses. According to G*Power 3.1.9.4 (26), a minimum sample of 150 participants was required for a multivariate regression analysis with 18 predictors, an effect size of 0.15, a significance level of 0.05, and a power of 0.80. Therefore, the sample size was sufficient.
Measures
Nurse turnover
Nurse turnover was measured using the six-month turnover rates in a nursing unit. Nurse managers provided the number of nurses who left their units between January 1, 2022, and June 30, 2022 (approximately 6 months prior to data collection). The six-month turnover rate was calculated as follows as given below, which was used a previous study (24).
This turnover rate was calculated for nurses working with nurse managers in the same unit. To distinguish low and high levels of nurse turnover, the distribution and levels of turnover were assessed. As a result, the six-month turnover rate was categorized into four groups: zero (0%), low (1–14%), moderate (15–22%), and high (23–50%).
Missed nursing care
The Missed Nursing Care Survey (1) comprising 24 nursing activities measures missed nursing care. The Korean version developed by Cho et al. (2) was used in this study. Nurses reported the frequency of missed nursing care for each activity as rarely (1 point), occasionally (2 points), frequently (3 points), always (4 points), or not applicable. Each nurse responded according to the care activities they missed. The prevalence of missed nursing care was measured considering the number of nurses who responded “occasionally” to “always” (the numerator) and the total number of nurses who responded, excluding “not applicable” responses (the denominator). The mean missed nursing care score was calculated by the averaging nurses’ responses to all 24 activities, excluding those marked as “not applicable.” Kalisch and Williams (1) tested its validity and reliability and reported psychometric standards of this instrument. Cronbach’s alpha of the Korean version of the Missed Nursing Care Survey in Cho’s et al. (2) study was 0.88, while in the current study it was 0.91.
Nurse and work-related characteristics
To examine the impact of nurse turnover on missed nursing care, this study accounted for several confounding variables, including nurse and work-related characteristics. Nurses’ characteristics included sex, age, highest level of nursing education (associate’s degree, bachelor degree, master’s degree or PhD in nursing), and subjective health status (very good, good, fair, poor). Work-related characteristics included work type (three-shift rotation vs. others), work experience in the current hospital, workload, perceived staffing adequacy, type of nursing unit, and hospital size (number of beds).
Workload was measured as the level of performance required for a job (27, 28). It comprised four items that assessed the amount, intensity, and frequency of work on a six-point Likert scale (from “never” to “five or more days a week”). Total scores ranged from 4 to 24. Higher scores indicated higher workload. Cronbach’s alpha in this study was 0.82, indicating good internal consistency.
Perceived staffing adequacy was measured by one item, which is asking nurses’ perception regarding staffing adequacy. It used a four-point Likert scale (very insufficient, insufficient, sufficient, very sufficient).
Data analysis
Data analysis was conducted using (SAS 9.4, Cary, NC, United States). The means and standard deviations of the six-month turnover rates were evaluated and grouped as 0%, 1–14%, 15–22%, and 23–50%. Mean scores for missed nursing care and the prevalence of missed nursing care were calculated. Descriptive statistics for the nurse and work-related characteristics were obtained. Missed nursing care based on participants’ characteristics was evaluated by conducting t-tests and an analysis of variance. A multivariate regression analysis was performed to examine the relationship between nurse turnover and missed nursing care, after controlling for nurse and work-related characteristics. In the multivariate regression analysis, hospital size was divided by 10 for better interpretation. Owing to missing data, the sample sizes per variable varied.
Ethics statement
An appropriate institutional review board approved this study (Approval No. XXX-202205-0005-01). Informed consent was obtained online from all participants. Permissions to use the study instruments were obtained from their respective authors.
Results
Characteristics of study variables
In total, data from 264 staff nurses was used in this study. Table 1 presents participants’ demographic and work-related characteristics. Nearly all (97%) participants were women. The mean age of participant was 32.58 (SD = 7.97) years. Approximately half were aged 21–30 years. Approximately 82% of participants had at least a bachelor’s degree, and 154 (66.6%) perceived their subjective health status as fair or poor. More than 90% worked in three-shift rotations. Participants had an average of 7.62 years of work experience in their current hospitals. The mean workload score was 18.05 points (SD = 3.60), and 208 (82.5%) participants reported either very insufficient or insufficient staffing adequacy.
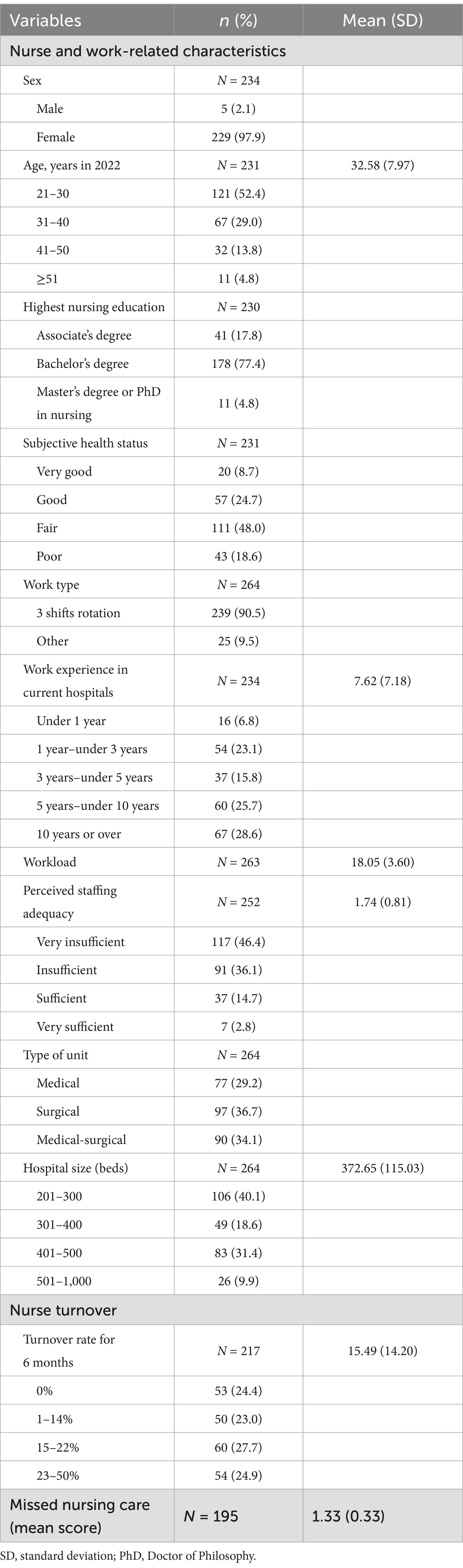
Table 1. General characteristics of the participants and study variables (N = 264).
The mean six-month turnover rate was 15.49% [standard deviation (SD) = 14.2]. Approximately 24% of participants worked in nursing units with a zero turnover rate. Sixty (27.7%) nurses worked in units with a 15–22% turnover rate. The mean score of missed nurse care ranged from 1 to 3 (mean = 1.33, SD = 0.33).
Prevalence and nature of missed nursing care
Table 2 presents the details of missed nursing care. Seven activities had a missed care prevalence of 30% or higher. The top five activities with the highest prevalence were turning the patient every 2 h, attending interdisciplinary care conferences, ambulation, patient bathing/skin care, and emotional support. Seven nursing care activities had a higher proportion of “not applicable”: turning patients every 2 h, attending interdisciplinary care conferences, ambulation, patient bathing/skin care, mouth care, feeding patients, and setting up meals. Ten nursing activities had a missed care prevalence of less than 20%.
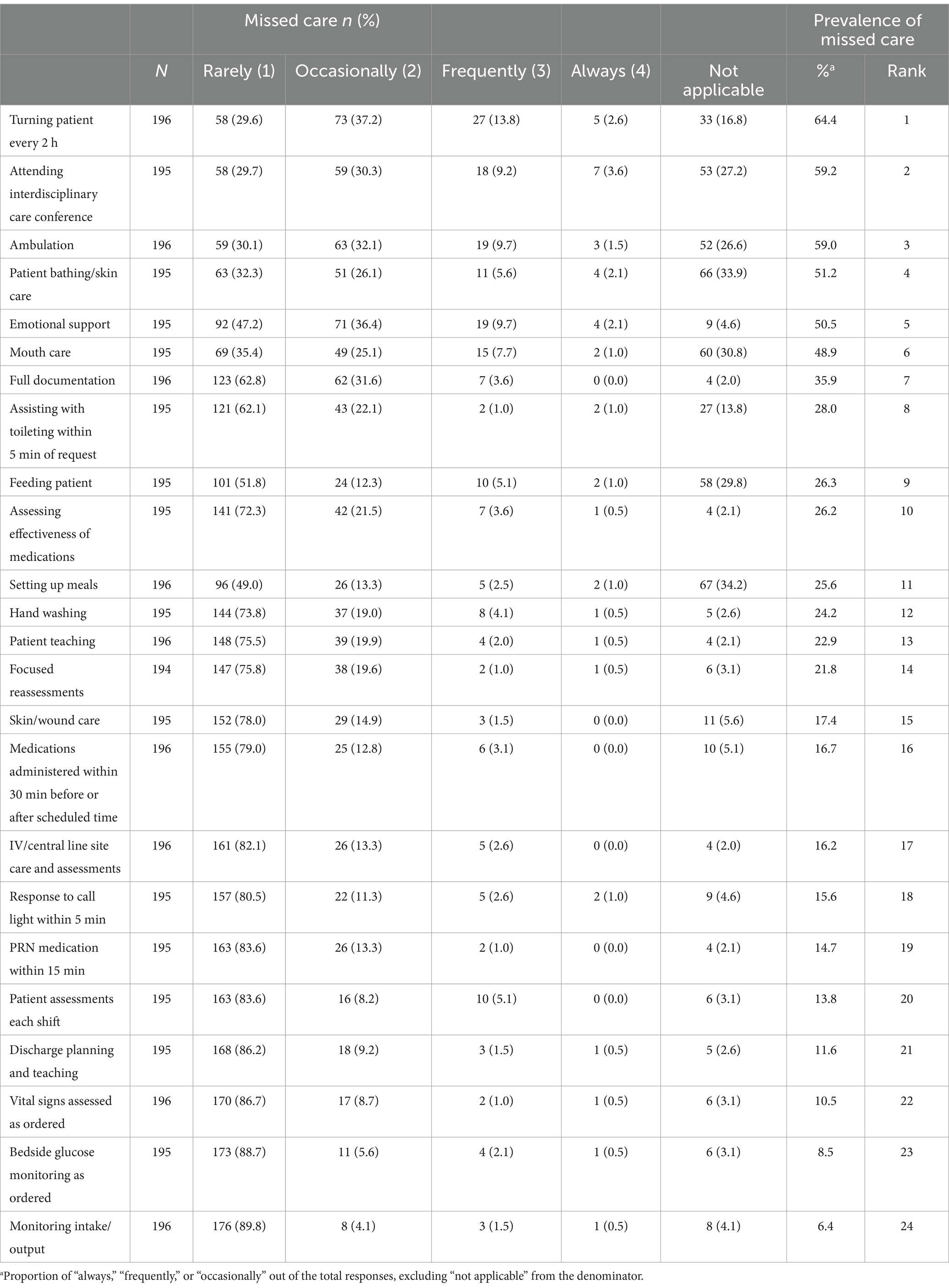
Table 2. Prevalence of missed nursing care and priority rank.
Missed nursing care by participant characteristics
The mean differences in missed nursing care according to participants’ characteristics are presented in Table 3. Missed nursing care among nurses differed according to their age, work type, and hospital size. Younger nurses reported a higher mean score for missed nursing care than did older nurses. Nurses working in three-shift rotations perceived more missed nursing care than those who did not. Nurses working at larger hospitals had higher mean missed care scores than those at smaller hospitals.

Table 3. Missed nursing care by characteristics of participants.
Relationships between nurse turnover and missed care
A multivariate regression analysis was conducted to identify the association between nurse turnover and missed nursing care, controlling for nurse and work-related characteristics (Table 4). Nurses working in units with turnover rates between 15 and 22% reported more missed nursing care [β = 0.160, standard error (SE) = 0.081] than those working in units with a 0% turnover rate. Among nurse and work-related characteristics, subjective health status was a significant predictor of missed nursing care. Compared to nurses reporting poor health conditions, those reporting good or fair health conditions reported less missed nursing care (β = −0.185, SE = 0.082; β = −0.142, SE = 0.070, respectively). Hospital size was positively related to missed nursing care (β = 0.0026, SE = 0.003). The regression model explained 10.3% (adjusted R2 = 0.103, p-value = 0.015) of missed nursing care.
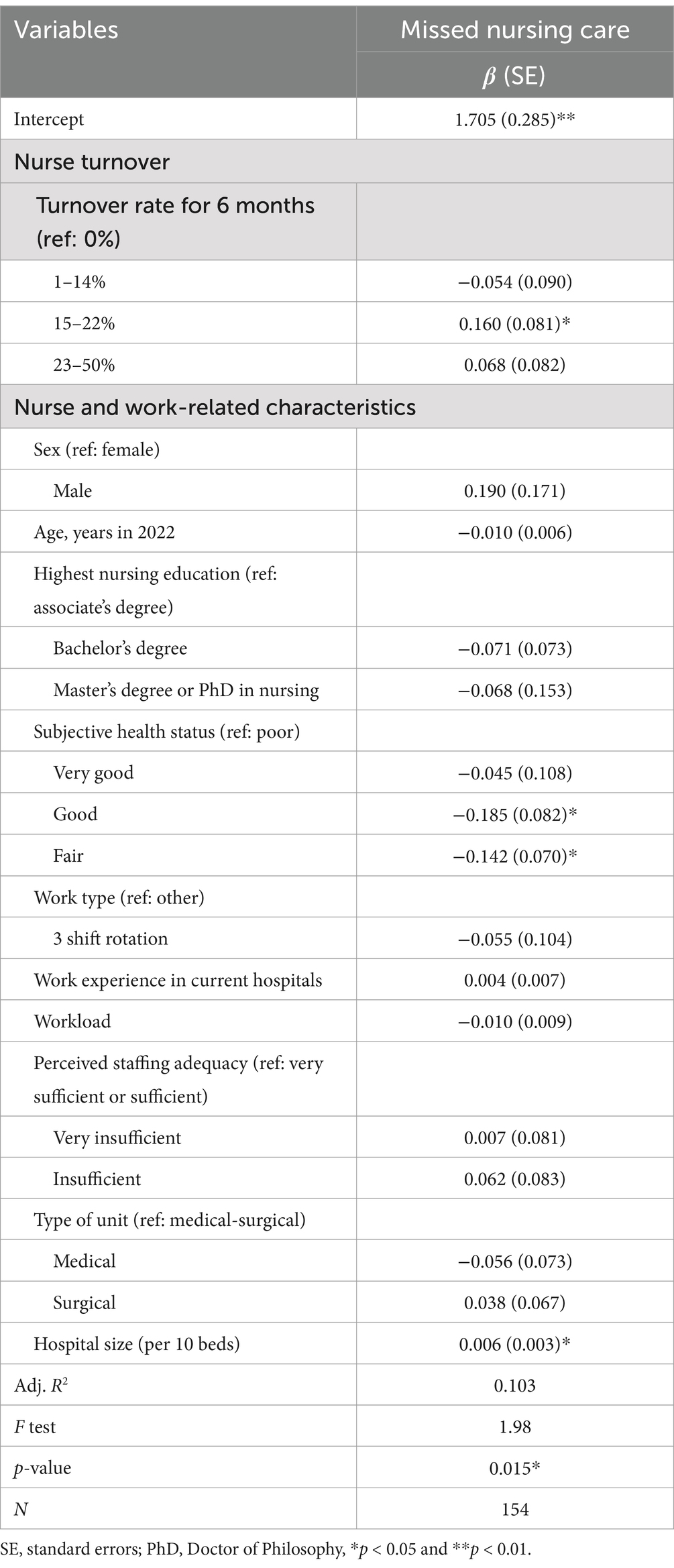
Table 4. Relationships of nurse turnover with missed nursing care.
Discussion
This study examined the prevalence of missed nursing care and how nurse turnover affects missed nursing care. Concerning missed care, 5 out of 24 nursing activities had a prevalence of more than 50%. According to a previous study (2), several activities (turning patients every 2 h, ambulation, patient bathing/skin care, and emotional support) among those five activities also had a high prevalence. However, the number of activities with a prevalence of 50% or more in that previous study (2) was lower in the current study. Patient ambulation was a frequently missed care item, which is consistent findings from a previous review (3). Clinical care, including vital signs, glucose monitoring, and monitoring intake/output, was rarely missed, with glucose monitoring consistently attended to in both the current and previous studies (20).
Nearly 30% of the nurses reported “not applicable” to patient bathing/skin care, mouth care, feeding patients, or setting up meals. Basic care is often provided by informal caregivers (e.g., family members) in South Korea (29). Thus, a response of “not applicable” for missed care in these areas might reflect the care by informal caregivers, not nurses. Only 4.6% of nurses reported that emotional support was “not applicable,” making it the fifth most frequently missed care. This implies that while nurses perceive emotional support as their responsibility, they cannot always provide sufficient support. These findings highlight nurses’ perceptions of their scope of care, which can be influenced by the healthcare delivery system and care culture (2).
In the multivariate analysis, nurses working in units with a moderate turnover rate (15–22%) reported a higher mean score for missed nursing care than those working in units with a zero turnover rate. High turnover may lead to frequent adjustments and more time spent with new staff (24), increasing workload and reducing staffing levels (25). This can increase missed nursing care, hinder teamwork, and disrupt communication and relationships between staff (30). Teamwork is a predictor of missed nursing care (22, 31). Lower levels of teamwork, deteriorated by frequent turnover, can lead to missed nursing care. Moreover, frequent turnover can cause nurses to spend less time adhering to clinical safety guidelines as they need to adjust new staff, potentially increasing incidents of missed nursing care (21).
Thus, this study demonstrated how nurse turnover can affect missed nursing care, emphasizing the importance of preventing nurse turnover. Turnover entails more than just replacing individual nursing staff; it also has a significant impact on care processes such as missed nursing care. Therefore, developing relevant strategies is crucial to prevent turnover among nurses in acute care hospitals. Practical strategies, such as new graduate transition programs (32) and adequate nurse staffing levels that consider the training and adjustment of new nurses, can facilitate their integration (3).
An unexpected finding was that no statistical difference was observed between the units with a turnover rate of 23–50% and those with zero turnover. Perhaps in nursing units with a high turnover rate (23–50%), a significant portion of nursing care might be delegated to patients’ families or informal caregivers. If this is the case, nurses do not consider these delegated nursing care activities within their scope of practice. Thus, they answered “not applicable” instead of missed care, indicating no significant relationship between the higher turnover rate and missed nursing care. Future studies should examine this in depth.
Notably, nurses who reported good health had relatively lower levels of missed nursing care than those with poor health. In previous studies, the main contributing factors to missed nursing care were related to nurses’ working conditions or patient characteristics, such as workload and staffing levels (4–6) and acuity (5), respectively. Managerial strategies and policies promoting nurses’ health and a health work environment (33) should be implemented to prevent missed nursing care. Institutional and governmental regulations could also be implemented.
Workload and perceived staffing adequacy were used as control variables in the relationship between turnover and missed nursing care. In previous studies, these two variables were significant contributing factors (4–6). However, they were not associated with missed nursing care in the current study. Nurse staffing was measured according to the nurses’ perceptions, not the absolute numerical values. Previous studies also used this measure but found a significant association with missed nursing care (2, 16). A previous review found that 14 out of 18 studies reported a significant relationship between low nurse staffing levels and higher levels of missed care (3). This relationship should be investigated in future research.
A recent review found that nurse turnover negatively affected nurse and patient outcomes, although this relationship was partially supported (34). The underlying mechanisms can be explained by care processes such as missed nursing care. In this study, nurse turnover had an adverse effect on missed nursing care, which may have been detrimental to patient safety and care quality. Unnecessary healthcare expenditures can compromise care quality (e.g., prolonged length of stay). Thus, this study elucidates the underlying mechanism of turnover and outcome relationships. Future studies should aim to validate these findings.
Limitations
This study has some limitations. The cross-sectional design limits any causal inferences. Although turnover and missed nursing care dare were sequential, inverse relationships must be considered, such as higher levels of missed nursing care leading to turnover. Longitudinal studies are needed to establish causality. Convenience sampling limits generalizability of the findings to other hospitals in South Korea. Data were collected from general hospitals, and the results may differ in other types of hospitals (e.g., tertiary general hospitals). Additionally, data from self-reported surveys are subject to recall bias and socially desirable response errors. Another limitation is the failure to assess confounding variables such as job satisfaction, income, and work–family conflict. Future studies should employ diverse measurement methods with these confounding variables.
Conclusion
This study investigated the prevalence of missed nursing care and the impact of nurse turnover on missed care. Nurse turnover was associated with missed nursing care, highlighting the adverse effects of nurse turnover on care processes. Nursing shortage is a global concern. Clarifying the adverse effects of nurse turnover could facilitate the development of policies to prevent nurse turnover. Several countries, including South Korea, have developed policies to retain nurses. The current findings inform policy change, further policy development, and strategies to prevent nurse turnover at institutional and national levels.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Ewha Womans University Institutional Review Board. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
S-HB: Conceptualization, Data curation, Formal analysis, Funding acquisition, Project administration, Supervision, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This study was funded by a National Research Foundation of Korea grant funded by the South Korean Government (Ministry of Science and ICT; No. 2021R1F1A1045394).
Acknowledgments
The author acknowledges Suin Kim, Hwasook Myung, and Ju Ree Youn for their assistance with this study.
Conflict of interest
The author declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Kalisch, BJ, and Williams, RA. Development and psychometric testing of a tool to measure missed nursing care. J Nurs Adm. (2009) 39:211–9. doi: 10.1097/NNA.0b013e3181a23cf5
2. Cho, SH, Lee, JY, You, SJ, Song, KJ, and Hong, KJ. Nurse staffing, nurses prioritization, missed care, quality of nursing care, and nurse outcomes. Int J Nurs Pract. (2020) 26:e12803. doi: 10.1111/ijn.12803
3. Griffiths, P, Recio-Saucedo, A, Dall'Ora, C, Briggs, J, Maruotti, A, Meredith, P, et al. The association between nurse staffing and omissions in nursing care: a systematic review. J Adv Nurs. (2018) 74:1474–87. doi: 10.1111/jan.13564
4. Lake, ET, Riman, KA, and Sloane, DM. Improved work environments and staffing lead to less missed nursing care: a panel study. J Nurs Manag. (2020) 28:2157–65. doi: 10.1111/jonm.12970
5. Redfern O.C.Griffiths, P, Maruotti, A, Recio Saucedo, A, and Smith, GBMissed Care Study Group. The association between nurse staffing levels and the timeliness of vital signs monitoring: a retrospective observational study in the UK. BMJ Open. (2019) 9:e032157. doi: 10.1136/bmjopen-2019-032157
6. Simonetti, M, Cerón, C, Galiano, A, Lake, ET, and Aiken, LH. Hospital work environment, nurse staffing and missed care in Chile: a cross-sectional observational study. J Clin Nurs. (2022) 31:2518–29. doi: 10.1111/jocn.16068
7. Bagnasco, A, Timmins, F, de Vries, JMA, Aleo, G, Zanini, M, Catania, G, et al. Understanding and addressing missed care in clinical placements—implications for nursing students and nurse educators. Nurse Educ Today. (2017) 56:1–5. doi: 10.1016/j.nedt.2017.05.015
8. Ball, JE, Bruyneel, L, Aiken, LH, Sermeus, W, Sloane, DM, Rafferty, AM, et al. Post-operative mortality, missed care and nurse staffing in nine countries: a cross-sectional study. Int J Nurs Stud. (2018) 78:10–5. doi: 10.1016/j.ijnurstu.2017.09.003
9. Min, A, Yoon, YS, Hong, HC, and Kim, YM. Association between nurses’ breaks, missed nursing care and patient safety in Korean hospitals. J Nurs Manag. (2020) 28:2266–74. doi: 10.1111/jonm.12831
10. Aiken, LH, Sloane, DM, Ball, J, Bruyneel, L, Rafferty, AM, and Griffiths, P. Patient satisfaction with hospital care and nurses in England: an observational study. BMJ Open. (2018) 8:e019189. doi: 10.1136/bmjopen-2017-019189
11. Chapman, R, Rahman, A, Courtney, M, and Chalmers, C. Impact of teamwork on missed care in four Australian hospitals. J Clin Nurs. (2017) 26:170–81. doi: 10.1111/jocn.13433
12. Srulovici, E, and Drach-Zahavy, A. Nurses’ personal and ward accountability and missed nursing care: a cross-sectional study. Int J Nurs Stud. (2017) 75:163–71. doi: 10.1016/j.ijnurstu.2017.08.003
13. Thomas-Hawkins, C, Flynn, L, and Dillon, J. Registered nurse staffing, workload, and nursing care left undone, and their relationships to patient safety in hemodialysis units. Nephrol Nurs J. (2020) 47:133–42. doi: 10.37526/1526-744X.2020.47.2.133
14. Gurková, E, Mikšová, Z, and Šáteková, L. Missed nursing care in hospital environments during the COVID-19 pandemic. Int Nurs Rev. (2022) 69:175–84. doi: 10.1111/inr.12710
15. Blackman, I, Lye, CY, Darmawan, IGN, Henderson, J, Giles, T, Willis, E, et al. Modeling missed care: implications for evidence-based practice. Worldviews Evid-Based Nurs. (2018) 15:178–88. doi: 10.1111/wvn.12285
16. Cho, SH, Mark, BA, Knafl, G, Chang, HE, and Yoon, HJ. Relationships between nurse staffing and patients’ experiences, and the mediating effects of missed nursing care. J Nurs Scholarsh. (2017) 49:347–55. doi: 10.1111/jnu.12292
17. Chaboyer, W, Harbeck, E, Lee, BO, and Grealish, L. Missed nursing care: an overview of reviews. Kaohsiung J Med Sci. (2021) 37:82–91. doi: 10.1002/kjm2.12308
18. Shin, S, Park, JH, and Bae, SH. Nurse staffing and nurse outcomes: a systematic review and meta-analysis. Nurs Outlook. (2018) 66:273–82. doi: 10.1016/j.outlook.2017.12.002
19. Dirgar, E, Berşe, S, Şahin, A, Tosun, B, and Manuel Levya-Moral, J. Presenteeism and missed nursing care: a descriptive, correlational and observational study. BMC Nurs. (2024) 23:652. doi: 10.1186/s12912-024-02253-9
20. Çiriş Yildiz, C, Değirmenci Öz, S, Yilmaz Kuşakli, B, and Korkmaz, I. The relationship between work environment and missed nursing care in nurses: the moderator role of profession self-efficacy. J Patient Saf. (2024) 20:522–7. doi: 10.1097/PTS.0000000000001266
21. Labrague, LJ, Al Sabei, S, AbuAlRub, R, Burney, I, and Al Rawajfah, O. The role of nurses’ adherence to clinical safety guidelines in linking nurse practice environment to missed nursing care. J Nurs Scholarsh. (2024). doi: 10.1111/jnu.13017
22. Kohanová, D, Solgajová, A, and Cubelo, F. The association of teamwork and missed nursing care in acute care setting: a mixed-methods systematic review. J Clin Nurs. (2024) 33:3399–413. doi: 10.1111/jocn.17182
23. Hospital Nurses Association. A survey on hospital nursing staffing 2018. Business report for Hospital Nurses Association. Available at: https://khna.or.kr/home/pds/utilities.php, (Accessed June 14, 2024).
24. Bae, SH, Mark, B, and Fried, B. Impact of nursing unit turnover on patient outcomes in hospitals. J Nurs Scholarsh. (2010) 42:40–9. doi: 10.1111/j.1547-5069.2009.01319.x
25. Park, SH, Boyle, DK, Bergquist-Beringer, S, Staggs, VS, and Dunton, NE. Concurrent and lagged effects of registered nurse turnover and staffing on unit-acquired pressure ulcers. Health Serv Res. (2014) 49:1205–25. doi: 10.1111/1475-6773.12158
26. Faul, F, Erdfelder, E, Lang, AG, and Buchner, A. G*Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods. (2007) 39:175–91. doi: 10.3758/BF03193146
27. Brewer, CS, Kovner, CT, Greene, W, and Cheng, Y. Predictors of RNs’ intent to work and work decisions 1 year later in a U.S. national sample. Int J Nurs Stud. (2009) 46:940–56. doi: 10.1016/j.ijnurstu.2008.02.003
28. Shin, S, Oh, SJ, Kim, J, Lee, I, and Bae, SH. Impact of nurse staffing on intent to leave, job satisfaction, and occupational injuries in Korean hospitals: a cross-sectional study. Nurs Health Sci. (2020) 22:658–66. doi: 10.1111/nhs.12709
29. Cho, SH, Kim, YS, Yeon, KN, You, SJ, and Lee, ID. Effects of increasing nurse staffing on missed nursing care. Int Nurs Rev. (2015) 62:267–74. doi: 10.1111/inr.12173
31. Bragadóttir, H, Kalisch, BJ, and Tryggvadóttir, GB. Correlates and predictors of missed nursing care in hospitals. J Clin Nurs. (2017) 26:1524–34. doi: 10.1111/jocn.13449
32. Rush, KL, Janke, R, Duchscher, JE, Phillips, R, and Kaur, S. Best practices of formal new graduate transition programs: an integrative review. Int J Nurs Stud. (2019) 94:139–58. doi: 10.1016/j.ijnurstu.2019.02.010
33. Min, A, Min, H, and Hong, HC. Work schedule characteristics and fatigue among rotating shift nurses in hospital setting: an integrative review. J Nurs Manag. (2019) 27:884–95. doi: 10.1111/jonm.12756
Keywords: nurse turnover, missed nursing care, administration, acute hospitals, evaluation, quantitative study
Citation: Bae S-H (2025) Association between nurse turnover and missed nursing care in acute care hospitals in South Korea. Front. Med. 11:1448839. doi: 10.3389/fmed.2024.1448839
Edited by:
Kim Walker, University of Aberdeen, United KingdomReviewed by:
Jacopo Fiorini, Policlinico Tor Vergata, ItalyAli Safdari, Hamadan University of Medical Sciences, Iran
Copyright © 2025 Bae. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sung-Heui Bae, c2JhZUBld2hhLmFjLmty