
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Med. , 26 September 2024
Sec. Healthcare Professions Education
Volume 11 - 2024 | https://doi.org/10.3389/fmed.2024.1446701
 Ángeles Reyes-Téllez1
Ángeles Reyes-Téllez1 Alberto González-García2*
Alberto González-García2* Adelina Martín-Salvador2
Adelina Martín-Salvador2 María Gázquez-López3
María Gázquez-López3 Encarnación Martínez-García2,4
Encarnación Martínez-García2,4 Inmaculada García-García2
Inmaculada García-García2Advances in healthcare in recent years have resulted in the automation and standardization of healthcare. Consequently, care has become dehumanized. There is a lack of trust from patients toward the health care system, as well as feelings of stress, exhaustion, and fatigue among professionals. The aim of this article is to describe the humanization actions in nursing care, as well as the barriers and facilitating strategies to carry them out. A systematic review of the scientific literature has been carried out following the recommendations of the PRISMA declaration. The search was carried out in the WOS, SCOPUS, CINAHL Complete, MEDLINE (via PubMed), EMBASE and Cochrane Library databases. The keywords used were “humanization of assistance,” “nursing care,” and “nurse–patient relations,” restricting to original studies in English or Spanish, from 2018 to 2022. One author performed the search, selection, and screening of records. Two authors were involved in data extraction, and a third author decided in case of conflict. The systematic review was guided by ethical conduct that respects authorship and reference sources. Of the 744 articles initially identified, 27 were included in this review. Methodological quality was assessed following the STROBE statement or the CASPe and MMAT tools. The main barriers were found to be the lack of training of nurses and their working conditions, as well as the unwillingness of the institutions. Facilitating strategies consisted of solving implementation problems, promoting communication to strengthen nurse–patient relationships and accompaniment by family members. The main interventions are related to the physical environment and have been studied in obstetrics and pediatrics services. Barriers related to training, work situation and lack of institutional involvement are complemented with facilitating strategies that aim to implement the humanized model at a general level.
Advances in healthcare in recent years have led to increased quality, safety and efficiency in health care (1). These results have been achieved through the promotion of specialization of professionals and the development of technologies for the prevention, diagnosis, treatment and rehabilitation of diseases (1, 2). However, technification has also meant automation and standardization of care and fragmentation of work (1). These elements often lead to a decrease in the time spent on direct care. This has led to dehumanization and depersonalization of care, resulting in a lack of trust from patients toward the health care system and feelings of stress, burnout, and fatigue among professionals (1).
Although this conflict persists today, it began to be studied in the last century. The American Rogers and colleagues (3), between 1938 and 1963, researched client-centered care. The term patient-centered medicine was introduced by Balint et al. in 1970 (4), which was to provide care that was not limited exclusively to the management of signs and symptoms (1, 5). Rogers himself qualified his model as client-centered or person-centered care (1, 3), which implied a more holistic perspective where symptoms and illnesses are treated in the context of each person’s unique experiences. Kitwood and Bredin (6) developed a model in 1992, which highlighted the importance of not only considering the physical state of the person in understanding their behavior. They considered equally significant their biography, personality traits and environmental peculiarities.
Subsequently, the concept of Humanization of Care was introduced, based on the model of Margaret Jean Watson (7), an American nurse considered a reference in the defense and application of the Humanization of Care. In 1979 she published her first book, in which she set out her theory, and in 1999, she structured it in the 10 Caring Factors for the Caritas Process or Process of Caring (8). Her theory belongs to the School of Caring, which defends the possibility of improving care by promoting the dimensions of spirituality and culture (9). This new proposal encompasses care for the person, the elements involved in the process and the interactions between them (1).
Today, Bermejo (10) asserts that respect for the human being is more assiduously guaranteed. Different countries have developed policies to recognize humanized care. Nurses are involved in direct care, management, technological manipulation, etc. They may suffer from work overload, so that humanization is neglected (11). This implies dissatisfaction of nurses, but also of patients, who perceive the need for empathetic care (12).
Other review studies have been conducted on the humanization of care and the role of nursing professionals in making it possible. Some focus exclusively on nurses and how their performance influences the humanization of care (13–16), and others include the multidisciplinary healthcare team or institutions (1, 17–19). Generally, they agree on the need for the promotion of education in nursing professionals, provided during university studies, as well as in postgraduate studies (17, 18).
A systematic review published in 2015, in which the participation of nurses as health educators was studied placed the emphasis on communication with the patient and the creation of an interpersonal relationship. It was concluded that it was an essential part of humanization, considering it a decisive factor for better patient recovery, integration with the team and with the family itself (13). Two other more current reviews coincided with this statement. The first was published in 2020 and considered communication as a mediating instrument for the humanization of care and the establishment of a relationship of trust (15). The second one was published in 2021 and aimed to find scientific evidence on humanized care from the perspective of nurses and in hospitalized patients. It was considered an urgent need for health institutions to be able to guarantee accessibility to humanized health services, as they are linked to patient and family satisfaction (16). The importance of communication between health professionals and family members to humanize hospitalization has also been highlighted (11). Finally, a review study published in 2018 (19) showed that the care environment was as important as the humanization knowledge of professionals. The environment is seen as a tool that makes it possible to provide quality care.
Therefore, although there are reviews on similar topics, it is considered relevant to carry out an update, at a global level, of the experiences to date, in order to generate reflection on the existing advances and gaps in the humanization of care. The systematic reviews that explore the interventions used to implement humanization are scarce. Moreover, there are no systematic reviews that report on barriers and facilitating strategies for the implementation of humanization in a structured way. Existing interventions in the literature reviewed are disparate. For this reason, it has been considered pertinent to carry out a systematic review to compile the published evidence on the characteristics of these strategies. The main objective is to know the advances in humanization that have been made in nursing care, at a global level, in the last 5 years. The following secondary objectives are planned: to describe the interventions used to implement humanization, to find out what the barriers are and, in contrast, to list the facilitating strategies for its implementation.
A systematic review of the scientific literature was conducted following the recommendations of the PRISMA 2020 (20) statement, designed primarily to conduct systematic reviews of studies evaluating the effects of health interventions.
The research question was stated following the PICO (21) structure: P - patients perceiving nursing care as well as nurses providing nursing care; I - interventions to provide humanized care; C - comparison of different interventions implemented to provide humanized care; O - the presentation of humanization in nursing care.
The WOS, SCOPUS, CINAHL Complete, MEDLINE (via PubMed), EMBASE and Cochrane Library databases were searched for evidence that met the research objectives. The search for articles was restricted from 1st January 2018 to 31st December 2022. Only articles in English and Spanish were accepted. The search was conducted between February and March 2023. The keywords used were “humanization of assistance,” “nursing care,” and “nurse–patient relations,” following the terms DeCS (Descriptors in Health Sciences) for the formulation of search equations in Spanish, and the MeSH (Medical Subject Headings) thesaurus to extrapolate the search to other languages. The three keywords were combined using the Boolean operator AND. The following search strategies were used in all the databases consulted: Humanization of Assistance (AND) Nursing Care, Humanization of Assistance (AND) Nurse–patient relations. WOS, SCOPUS and Cochrane Library proposed default filters related to topic, title, abstract or keywords. Specifically, WOS proposed default filters related to topic (title, abstract and indexing); and SCOPUS and Cochrane Library applied default filters related to title, abstract and key words. These filters were accepted in our searches, except in Cochrane Library, where the search was only filtered by abstract. Similarly, researchers applied equivalent restrictions in the other three databases consulted: EMBASE was searched by title, abstract and keywords; MEDLINE (via PubMed) was searched by title and abstract; and CINAHL Complete was searched by abstract.
We included studies on activities to humanize nursing care, published in English or Spanish, from 2018 to 2022 (both included), both quantitative and qualitative. We excluded studies that addressed interventions to humanize care that did not involve nursing staff, as well as those that focused on interventions delivered by nurses that were not related to the humanization of care. Records with limited possibility to provide relevant information or low methodological quality were excluded. We considered low quality articles to be those with less than 50% of the items in the STROBE (22) and CASPe (23) tools, or a negative result in the control questions of the MMAT (24) questionnaire.
One author of this review was responsible for searching, selecting, and screening the records (ART). Two authors were involved in data extraction (AGG, IGG), with a third author deciding in case of conflict between them (AMS).
The assessment of the methodological quality of the articles included in the review was carried out following the standards and criteria of the STROBE (22) statement for descriptive cross-sectional studies, with the CASPe (23) tool for those with a qualitative design and with the MMAT (24) tool for mixed methods studies. A consensus was reached among the authors to relate the total score obtained to the quality of each article. Articles that met less than 50% of the items were considered low quality, between 50 and 75% moderate quality and more than 75% high quality.
The analysis was carried out by peer review by two different authors (MGL, EMG). An intensive reading and detailed analysis of the information described in the studies was carried out with the help of tools to determine the risk of bias (RoB). AHRQ tool (25) was used for the evaluation of cross-sectional studies. A consensus was reached among the authors to relate the total score obtained to the risk of bias of each article. A score from 0 to 4 indicates a high RoB, from 5 to 7 indicates a moderate RoB and from 8 to 11 indicates a low RoB. The JBI checklist (26) was used for qualitative studies. A score from 0 to 4 indicates a high RoB, 5–7 indicates a moderate RoB and 8 to 10 indicates a low RoB. Finally, MMAT (24) tool was used for mixed methods studies. A score less than 50% indicates a high RoB, 50–70% indicates a moderate RoB and 80–100% indicates a low RoB.
This article does not contain any studies with human or animal participants and informed consent is not required.
The initial search of WOS, MEDLINE (via PubMed), SCOPUS, CINAHL Complete, EMBASE and Cochrane Library databases resulted in a total of 744 records (WOS n = 142, MEDLINE (via PubMed) n = 16, SCOPUS n = 409, CINAHL Complete n = 42, EMBASE n = 10, Cochrane Library n = 125). Filtering by inclusion and exclusion criteria resulted in 192. Removing duplicate articles resulted in 170 articles. Articles were screened based on titles and abstracts, resulting in 56 articles from WOS, SCOPUS, and CINAHL Complete. Finally, a complete and exhaustive reading of all articles was carried out to select 27 articles. Two authors participated in the final selection, and there was no disagreement between them regarding the inclusion of studies in this systematic review. No publications were retrieved. They were presented according to the recommendations of the PRISMA 2020 statement (Figure 1). With the research question as a guide, information was extracted from these articles to analyze and interpret them.
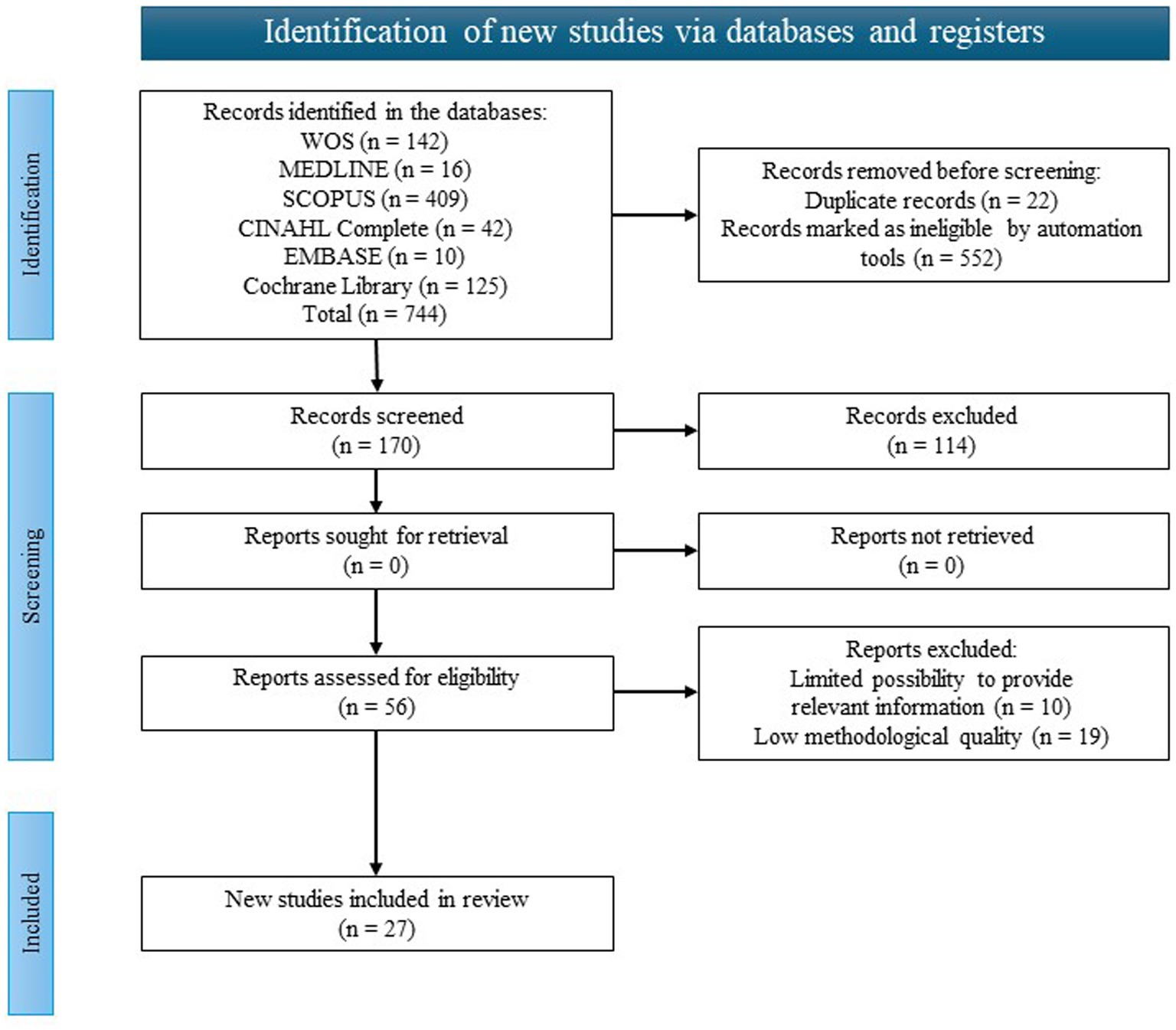
Figure 1. Flow chart.
The 27 selected articles were carefully reviewed and ordered. An analysis was made of the most relevant data, as well as of their study process: methodology, sample, results, conclusions obtained, score achieved and correspondence with their methodological quality and risk of bias (Table 1). The articles were published in six countries: Brazil (27–42), Spain (43–47), Chile (48, 49), Portugal (50), Canada (51), Mexico (52), and Iran (53). It includes 15 qualitative studies (27, 28, 30–33, 35, 37, 38, 40, 41, 44–46, 51, 53), 10 quantitative (29, 34, 36, 39, 42, 43, 47–49, 52) and two mixed (30, 50) which were critically analyzed for inclusion in the study. The topics addressed by the studies are lack of nurse training (29, 31, 37, 42, 50), working conditions (27, 37, 42, 51, 52), institutional unwillingness (27, 29, 37, 38, 42, 51, 52), strategies for solving implementation problems (27–30, 36–38, 41–44, 46, 49, 51–53), promoting communication to strengthen nurse–patient relationships and encouraging patient autonomy (27, 30, 33, 34, 38, 40, 41, 44, 46, 48, 49, 52, 53) and family member accompaniment (28, 29, 31, 34–36, 39).
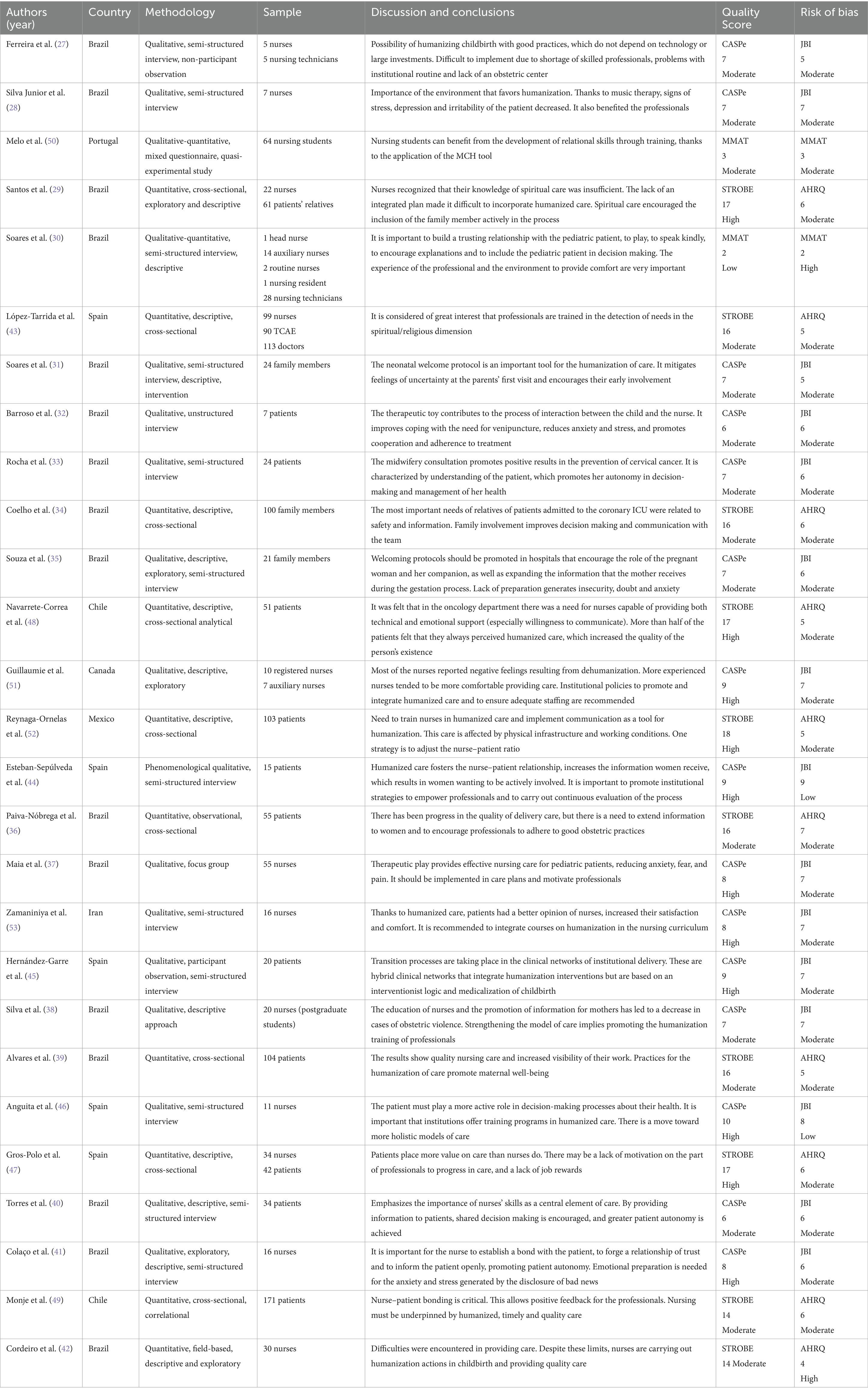
Table 1. Summary of the analysis of the articles included in the review.
Three different tools with different assessment criteria were used to analyze the quality of the studies. The CASPe (23) tool was used for the analysis of qualitative studies. It is a tool with 10 items. Seven studies showed high methodological quality, obtaining scores of eight (37, 51, 53) nine (44, 45, 51) and ten (46). The majority obtained moderate quality with scores of six (33, 40) and seven (27, 28, 31, 33, 35, 38). Quantitative studies were assessed following the STROBE (22) statement. Four of them showed high methodological quality, meeting seventeen (29, 47, 48) or eighteen (52) criteria. The others were considered to be of moderate quality as they met 16 criteria (34, 36, 39, 43), except for Monje et al. (49) and Cordeiro et al. (42), which only met 14. The quality analysis of the mixed studies was performed using the MMAT (24) tool. In the control questions, a positive result was achieved in both, so we continued with the questions according to the study design category. In the first (50), some shortcomings were noted in the rationalization of the rationale for using a mixed approach. It is also felt that the integration of qualitative and quantitative data could be more unified. Its methodological quality is considered to be moderate, meeting 60% of the items. In the second (30), shortcomings have been observed in the explanation of the relevance of the use of mixed methods to answer the research question. The objective data are not presented in an integrated way. It is considered to be of low methodological quality, due to 40% of the criteria. As mentioned before, the risk of bias (RoB) of quantitative studies was measured using the AHRQ (25) tool for cross-sectional studies. All quantitative studies showed a moderate risk of bias (29, 34, 36, 39, 43, 47–49, 52) except for the article by Cordeiro et al. (42), which reported a high risk of bias. The risk of bias of qualitative studies was determined using the JBI (26) checklist. Two studies had a low risk of bias (44, 46), while all others showed a moderate risk of bias (27, 28, 31–33, 35, 37, 38, 40, 41, 45, 51, 53). The mixed methods studies were measured with the MMAT (24). As explained in the quality section, both showed positive results on the control questions. The first article (50) had a moderate risk of bias, whereas the second article (30) a high risk of bias. Although there is a disparity in the quality and risk of bias of the studies, it was decided to include them in this review because they provided relevant information to answer the stated objectives.
The studies included in this review show an intention to change toward more humanized care. In some, a few variations in care are made, in others, major modifications of protocols. Often the actions are directed toward a specific type of care.
Among the most frequent activities are those related to the physical care environment. Examples are the adequacy of light, noise, or temperature. The nursing staff themselves can also provide a supportive environment by grouping all interventions together at one time, making postural changes, using cushions to improve posture, or providing adequate body hydration (30).
Humanization actions in the obstetric setting are among the most studied. The importance of non-invasive techniques (39), non-medicalization of labor and reduction of unnecessary interventions are emphasized (27, 36). Pain relief can be provided through non-pharmacological procedures (early skin-to-skin contact or positions for pain relief), individualization of labor through dialog with the laboring woman, free choice of companion or effective emotional support. Importance is also given to physical measures, such as restricting certain procedures (episiotomy or speeding up labor), favoring the choice of birth position (encouraging upright positions), using rubber balls, massaging, late umbilical cord clamping, promoting breastfeeding, providing a low-stimulation environment, taking warm baths, walking, or promoting music therapy. Similarly, the use of non-invasive tools, such as the partogram, is encouraged for accurate monitoring of labor (27, 36, 42, 45).
Similarly, actions to humanize the care of pediatric patients are explored. They need affection and reassurance as part of care, which can be more humanized if nurses include playing, talking with kindness and providing both information and explanation of procedures (30). A good example is the use of dolls in therapeutic play as mediators to facilitate care. It promotes adherence to treatment and children’s cooperation because they understand the process better. This reduces the anxiety and stress they feel, and promotes resilience (32, 37). Distraction strategies such as videos, books, toys, and songs are also used while the techniques are being carried out. With these actions, the hospital routine is transformed into a more familiar experience, so that they have fun in a context of normality (37).
Despite the activities undertaken to achieve the humanization of care, many of the articles analyzed in this review report difficulties in implementation. Barriers related to nursing staff knowledge are noted (29, 31, 37, 42, 50). The importance of such knowledge was described in research comparing the relational skills of students who had received training in humanized care and those who had not, which concluded that there was a need to implement methodological teaching that fosters the skills to provide complex humanized care (50). This problem was also noted in a study on therapeutic play (37). The training deficit is a drawback that continues throughout specialization and professional practice. In several studies on humanization in delivery care, professionals were poorly prepared, had insufficient knowledge of procedures, or were demotivated (29, 37, 42). This motivation influenced the quality of care, as the willingness to perform care is as important as training (31). In addition, the work of the nurse is often undervalued (31). In one study it was found that patients and nurses perceived care differently, with patients rating the care higher (47).
Similarly, the work situation of nurses resulted in difficulties in providing humanized care. Nurses reported having few professionals and, in addition, staff turnover was low. Therefore, patient care time was more limited (27, 37, 42, 51, 52). In a study on nurse empowerment, nurses themselves recommended increasing staff recruitment, considering lack of time a problem, in addition to inadequate remuneration (51). In another study on spiritual care for critically ill patients, nurses reported lack of time as a barrier (29). Sometimes this lack of time was not due to the need for more staff, but to the amount of administrative tasks that nurses had to perform, which reduced direct care and nurses reported feeling ‘burnt out’ (27, 37, 51). The emotional health of workers was also found to be influenced by negative feelings resulting from the dehumanization of care, such as frustration, anger or diminished empowerment (51). This dehumanization was reported by patients, who, in a study on the evaluation of nurses’ humane care, rated nursing techniques higher and considered humanized care less common (52).
Other aspects described in the studies were problems related to the unwillingness of institutions to implement humanized care. Thus, some studies point out that management support is needed to solve the problem of the physical structure, which was considered inconsistent with the humanization policy, as well as to address the lack of material resources and the need for training of nurses. At other times, it was the lack of an integrated plan for daily care that affected the possibility of incorporating humanized care (27, 29, 37, 42, 51, 53). Practical examples included prioritizing other activities over the humanization of care during labor, not providing the mother with the necessary privacy or not allowing her to choose her companion (27). In a study on the same topic, some women reported a lack of clarity and completeness in the guidelines provided to them (38), although in another study they rated the availability of resources during labor as positive (44).
A large proportion of these were aimed at addressing the lack of training of nurses. Among the possible solutions, several studies proposed that there should be a qualified humanized care professional dedicated exclusively to this task (27, 29), although a majority of studies advocated encouraging the training of all nurses (36, 38, 43, 44, 52).
It has been observed that more experienced nurses tended to be more comfortable providing humanized care, as they were more familiar with the technical aspects and had experience with a variety of situations (29, 30, 51). It is proposed that humanization training should begin in undergraduate studies, integrating courses into the nursing curriculum (38, 53). The importance of continuing with postgraduate training has been highlighted (38, 42). Among the contents of this training, communication with the patient (41, 46) and the professionals’ ability to cope have been mentioned (46). Actions that allow positive feedback on the activities that are carried out are contemplated (28, 37, 49).
An essential skill of the nurse is the ability to communicate, considered the key tool to achieve the humanization of care (48, 52, 53). This was observed in a study on the needs of family members of critically ill patients in which communication and support received, even in situations of little clinical progress, were predictors of satisfaction (34). The more information nurses provide, the more confident the person being cared for feels, increasing their trust in the professional (44). It favors the creation of a bond between nurse and patient, which helps to minimize their anxiety, fear, insecurity and doubts (38, 41). Likewise, patients perceive that professionals invest time in them (49).
Adequate communication allows people to have more autonomy in decision-making and to participate in managing their own health, adopting a more active role (30, 33, 46). The patient must have maximum information and be involved in the process (40). One tool to promote this autonomy is the implementation of continuing education strategies (41). Several examples are noted in obstetric studies describing the importance of promoting maternal empowerment (27, 44). The provision of information should begin in prenatal care and continue through the postpartum period, in order to restore the mother’s agency (27, 35, 36, 39). There is also a need to encourage the autonomy of the companion, as this has been found to reduce the practice of intervention (35). Similarly, there are benefits to including a companion or other family members in care (36, 39). This has been shown in studies on the individual distress of patients with COVID-19 hospitalized in ICU, which was worse when unaccompanied by their relatives (28). Those relatives who actively cooperated in the care process felt empowered, had better communication with the professional team and felt less fear and hesitation at discharge (29, 31, 34).
The involvement of institutions is considered an essential facilitator for the promotion of humanized care. The importance of providing humanized spaces and training professionals is highlighted. Even so, different studies have shown the need for the administration to invest more resources in these aspects and to improve the management of existing infrastructures (28, 37, 46). The need for greater recognition is also projected, due to the fact that humanized care is sometimes not reflected, although it takes time and results in benefits for patients (47). The need to implement all these actions at a general level is projected, so that these processes can be carried out, valued and disseminated at the hospital level. In this way, the humanization of care would be more homogeneous in all services and would not depend on the individual changes made in each one (31, 33, 35, 37, 41, 44, 51). A summary of the different barriers and facilitators identified are presented in Table 2.
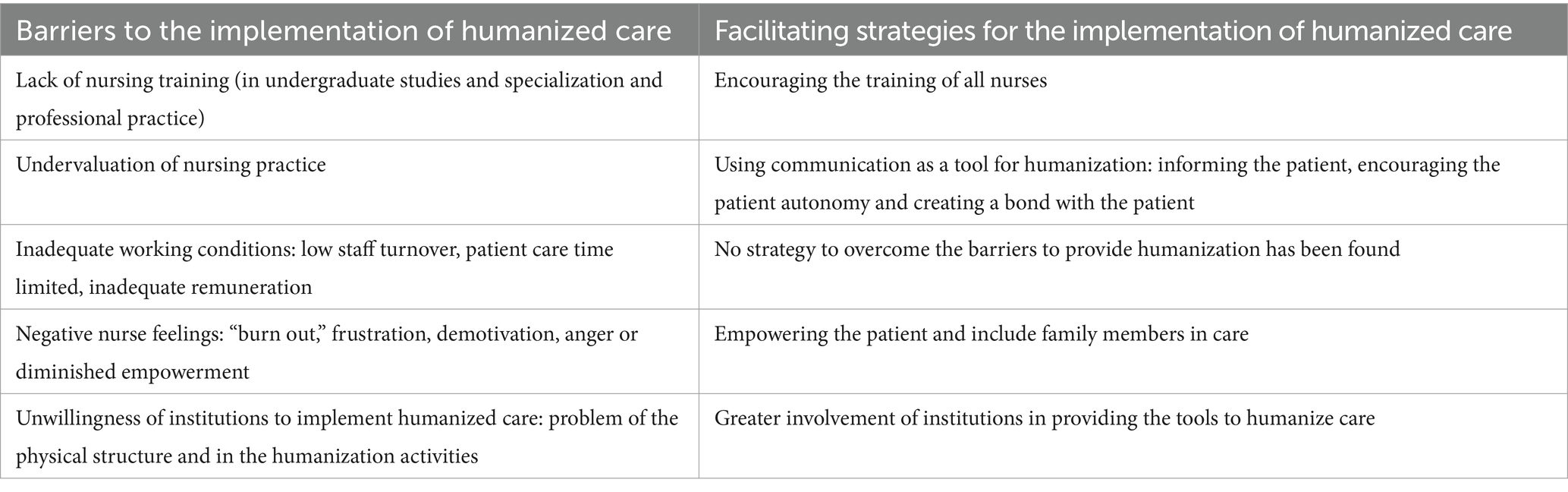
Table 2. Barriers and strategies identified.
The aim of this systematic review was to learn about the advances in humanization that have been made in nursing care, at a global level, in the last 5 years. Although there were systematic reviews already published on this same subject, the secondary objectives proposed here differ from those published previously, so the knowledge provided is considered of great relevance. This systematic review has highlighted the importance of humanizing care and demonstrates the efforts of health services and professionals to achieve this. Most of the studies highlight the importance of institutions in promoting change.
The importance of the interventions used to humanize care, both in terms of changes in the environment and in the way in which they are carried out, is discussed. The importance of such interventions is reiterated in the literature. Most research does not explicitly emphasize their characteristics or lumps them together with change strategies.
Despite their importance, only one study has been included in this systematic review focusing on the influence of the physical environment in which care is perceived (30). Even so, the results obtained coincide with the contributions to promoting the well-being of pediatric patients listed in a review conducted in 2014 (19) that aimed to analyze strategies to humanize the care of hospitalized children. Leisure practices such as toys, music and reading were found to minimize the stress of hospitalization and produce a calming effect. Children were encouraged to participate in the decoration of healthcare facilities in order to humanize the environment. Subsequent research has followed the same line, as is the case of the research study included in the present review (30). Others placed greater importance on the actions of healthcare staff, as is the case of research on the perception of the companion of the child in hospital in a pediatric intensive care unit, published in 2017. A greater perception of humanized care was associated with healthcare workers being actively involved in the care (54).
Most of the studies included in this review have been conducted mainly in obstetrics (26, 33, 36, 39, 42, 45) or pediatric services (30, 32, 37), detailing interventions focused on fostering more humanized care. One study on gynecological reception stands out, in which it was argued that dialog facilitated the process of humanization (33). This consists of receiving the person with an attitude of closeness in which dialog is essential. This was agreed in a review of 2020 (11) which aimed to understand the behavior of nurses in implementing hospital humanization and another review on the challenges of nursing for universal health coverage, published in 2016 (14). The latter revealed that a greater welcome was achieved in those units that had been carrying out this action for longer, in which patient access to the unit was encouraged and in which multidisciplinary team meetings were held to evaluate the services.
Many studies that form part of this review agree that the lack of training of nurses is one of the main barriers to being able to provide humanized care (29, 31, 37, 42, 50). They refer to the existence of this problem from undergraduate training, although they do not go into too much depth. However, in an integrative review of the literature published in 2020 (15), they reflect on how unprepared students feel. They consider that there is a need to supplement the knowledge provided theoretically with occasional seminars and lectures. These findings are in line with those of an earlier review from 2012 (18). It states that including a humanization strand in an isolated course is insufficient to achieve significant changes. Along the same lines are the results of a 2018 research study (17). It confirms the fact that there is no university policy to raise students’ awareness of humanization. Additionally, postgraduate training does not address this training deficit. As a result, nurses feel underprepared, which leads to demotivation and a decrease in the quality of care (31). The results of a 2016 systematic review (14), conducted with the aim of identifying nursing objectives for universal health coverage, also coincide with the above. It reiterates the need to train nurses and all professionals in humanization. A 2021 systematic review, which investigated nurses “and patients” perspectives on humanized care (16), concluded that care recipients perceived limitations in care due to lack of social skills, selflessness and low compassion in the face of suffering. These competencies of professionals were assessed to a greater extent in studies that investigated the patients’ point of view (1).
The articles agree that a major barrier to care is the working conditions in which nurses provide care. Limited care time results in dehumanization, which is related to insufficient staffing and management (27, 37, 42, 51, 52). Different research corroborates the findings of the present systematic review on the influence of nurses’ working conditions on humanization (1, 11, 15, 17, 19). Understaffing is related to increased demand for care, which results in work overload, little time to provide humanized care, intense work routine and increased bureaucratic demands. This is associated with increased stress and job dissatisfaction (1, 11). All of this influence patients’ views of nurses, who consider humanized care less common than the performance of techniques (52).
The importance of management involvement is underlined. The training provided to practicing professionals is considered insufficient (29, 37, 42, 51, 52). Other publications also relate this aspect to involvement in the well-being of professionals (e.g., offering psychological support), although there is currently a gap in this area (1, 19). The low willingness observed on the part of the institutions in this study coincides with that obtained in other reviews. As in the present systematic review, an integrative literature review from 2022 (55) found barriers related to the lack of institutional support. This review investigated the role of nurses with patients who are experiencing maltreatment. Nurses felt that it was important to create opportunities to address barriers related to work overload, lack of professional preparation to identify cases and non-recognition of violence as a health problem. This led to feelings of helplessness and insecurity among nurses.
Infrastructure-related barriers were closely linked to difficulty in accessing services, which negatively affected patients’ confidence and influenced the possibility of creating a therapeutic bond with professionals (1, 13–15, 19). A Brazilian systematic review published in 2015 (13) evaluated the involvement of the nurse as a health educator and primary care provider. It reflected institutional barriers influencing humanization, which were consistent with the results of this study, including physical structure, deficiencies in protocols and organizational shortcomings. Other barriers included long waits or delays, both for consultations and examinations, and deficiencies in routines, center rules and equipment (13).
As a solution to the lack of training in humanization observed in most of the articles, its promotion is proposed as a facilitating strategy. The experience of nurses was related to a more favorable situation for providing humanized care (29, 30, 51), so one strategy was to provide nurses with knowledge to help them in dealing with different situations. In the literature consulted, it has been observed that many of the interventions to promote training are aimed at undergraduate studies. The focus is on learning techniques based on participatory and reflective methods, which encourage student autonomy and teamwork. To achieve this, practical humanization activities and teacher involvement are advocated (14, 15, 18). Of particular note is a 2012 critical review on the teaching of humanization of care in undergraduate programs, in which different Brazilian publications were analyzed (18). It includes teaching strategies such as dramatic games, socio-drama, role-playing, debate, simulations and discussion of films. Emphasis is placed on students being able to reflect on their feelings and limitations (18). Jean Watson stated that those who fail to recognize their own feelings will find it difficult to understand another person’s feelings, so this reflective practice is part of the professionalization of nurses (15). On the other hand, there is a need for continuing postgraduate education of nurses. Institutions have a responsibility to implement the competencies of professionals in humanization, offering specific training in this area, as well as to promote the understanding and participation of professionals and patients (13, 14, 16).
On the other hand, the importance of communication as a fundamental tool for humanization (30, 33, 46) as presented in the results of this study is consistent with a large body of research (1, 11, 13, 15, 16). It was observed that when patients’ preferences and needs were considered, their satisfaction, empowerment, quality of life and improved treatment outcomes were increased (1, 15, 16). The results of this study are consistent with those of an integrative review published in 2022 (55). In this review, the performance of nurses in family health strategies with abused children was investigated. The importance of forming a bond with pediatric patients, in order to obtain details, could break the cycle of violence. All this is directly related to the provision of information to patients, so that they can be involved in the process and their autonomy in decision-making is promoted (30, 33, 40, 41, 46). Specifically in interventions carried out in obstetric services, decision-making during childbirth is related to the empowerment of the mother, in order to promote her protagonism (27, 44). The same conclusions are observed in a systematic review about the nursing perspective of the humanized care of the neonate and family published in 2021 (56). It is argued that professionals should be actively involved in humanized care. In addition, the patient and family should be included in decision making, even being able to discuss the daily care plan and the expected outcomes. As a result, care becomes safer and more efficient.
This systematic review highlights the benefits for patients of including family members or companions in care (28, 29, 31, 34). This information coincides with that published in a review on training guidelines for humanized care, carried out in 2020 (15). It shows that the presence of family members is an element that favors the physical and emotional recovery of the person being cared for. It has been proposed that the family be included in undergraduate programs so that nursing students acquire skills to work with them and value their importance.
It has been mentioned previously that the lack of institutional involvement is a barrier to the implementation of humanized care. Reversing this becomes a facilitating strategy. It is possible to improve the infrastructure to favor humanization and to optimize the use of existing resources for this purpose (28, 37). It is also considered a step forward to offer training programs in humanized care and non-technical competencies (46). Another measure considered necessary is the recognition of the humanization activities carried out by nurses (47). This can be achieved through the promotion of institutional strategies, as well as the implementation of good clinical practices, care plans and welcome protocols. Subsequent assessment of these processes is essential for ongoing evaluation and dissemination of research in the fields of knowledge (31, 33, 35, 37, 41, 44, 51). The literature also stresses the importance of implementing institutional policies governed by quality indicators, which should correspond to international standards of humanization, as well as making research-based changes and applying tools and models to improve care (14, 16).
Finally, it is significant to underline the scarce information that has been found on humanization facilitating strategies related to the work situation of nurses. This review presents strategies to overcome barriers related to the lack of training of nurses or the unwillingness of institutions to implement humanized care. However, there are no strategies that correspond to the barrier of the work situation in which nurses carry out their profession. There is no discussion of possible solutions to the lack of time and staff available to provide care, the inadequate remuneration of nurses or the number of administrative tasks that reduce direct care. However, recognition of the humanization activities they perform is raised (47). There is a big difference between the projection of the future to solve other barriers and the scarcity of this same aspect that has been found in relation to the employment situation of nurses. In contrast, the literature consulted suggests measures such as improving the working conditions of professionals and the relationships between all those involved in the care process (19). To this end, it is important to have a suitable environment that fosters interpersonal relationships and provides welcoming care (1, 19).
This systematic review has some limitations that need to be highlighted. Firstly, the location of the studies that have been analyzed. Most of them have been located in Brazil, which implies that the social and political reality of this country has a greater weight in the vision of humanization provided by this study. Therefore, extrapolation of these results to other geographical areas and socio-cultural environments may be difficult. This limitation may be related to the quantity, quality and impact of the research selected for this review, which does not include gray literature in the search. In this sense, some humanization actions implemented are not subsequently published. Therefore, it would be necessary to complement the information obtained with protocols of each service and with actions included in institutional humanization plans, for example. Secondly, although all the research included in this review studies the humanization work of nursing professionals, some of them also include other professionals such as nursing technicians, auxiliary nursing care technicians or doctors, or nursing students. Nurses perform different tasks and have different levels of competencies depending on the country in which they practice their profession, delegating or taking over delegated actions from other professionals. Thirdly, even though, the studies included in this review have disparate quality criteria. In our systematic review we have included studies that had sufficient quality; therefore, the conclusions of our study do not reflect the individual value of each article. Nonetheless, it is possible that some of the information in these studies was biased or incomplete. Fourth, the search was limited to articles published in English or Spanish, so it is possible that publications in other languages could have met the inclusion criteria and provided relevant information. Finally, it is noted that most of the articles analyzed used a qualitative approach, so the results obtained cannot be extrapolated to the general population.
This review shows the reality of the humanization of care today. The results obtained are not extrapolable to a global level for the reasons mentioned above, although they provide important data on the degree of implementation of humanization. It is considered that in the future it would be pertinent to continue to expand knowledge on this subject. Knowing the perspectives of professionals, patients and relatives provides a richer and deeper vision of the situation, as it encompasses a large part of the factors that influence the care process. It is especially important to know what patients think, since they are the main recipients of care, and it is a way of ensuring that they continue to be protagonists in their vital processes.
Different interventions have been described to implement humanized care, often targeting a specific type of care. Many of them relate to the environment in which care is provided. Of particular note are those implemented in the field of obstetrics, which are based on dialog and encouragement of patient autonomy, as well as changes in nursing care processes to reduce unnecessary interventions, use less invasive tools and promote physical measures. Interventions in pediatric services that promote information and distraction strategies for painful processes are also highlighted. The barriers encountered have been the lack of training of nursing professionals, the work situation of nursing professionals, with few staff and therefore little time dedicated to humanized care, which generates negative feelings in the professionals, as well as the low willingness of the institutions to change this situation. The facilitating strategies for humanized care are related to the promotion of nurse training, the use of communication as an indispensable tool to achieve patient autonomy in decision-making, the promotion of family accompaniment and greater involvement of the institutions to evolve toward a model of humanized care at a general level.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
ÁR-T: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Validation, Visualization, Writing – original draft, Writing – review & editing, Funding acquisition, Software. AG-G: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Validation, Visualization, Writing – original draft, Writing – review & editing, Supervision. AM-S: Methodology, Resources, Validation, Visualization, Writing – review & editing. MG-L: Methodology, Resources, Validation, Visualization, Writing – review & editing. EM-G: Methodology, Resources, Validation, Visualization, Writing – review & editing. IG-G: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This work was supported by the Consejo General de Enfermería, “Programa de ayudas a doctorandos y realización de tesis CGE 2023-24” [grant number AYD219_2023].
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Busch, IM, Moretti, F, Travaini, G, Wu, AW, and Rimondini, M. Humanization of care: key elements identified by patients, caregivers, and healthcare providers. A systematic review. Patient. (2019) 12:461–74. doi: 10.1007/s40271-019-00370-1
2. Consejería de salud y familias. Plan de Humanización del Sistema Sanitario Público de Andalucía. Sevilla (2021). Available at: https://www.juntadeandalucia.es/export/drupaljda/Plan%20Humanizaci%C3%B3n%20SSPA_v12042021.pdf (Accessed November 17, 2023).
3. Méndez-López, M. Carl Rogers y Martin Buber: las actitudes del terapeuta centrado en la persona y la relación “yo-tú” en psicoterapia. Apunt Psic. (2014) 32:171–80. doi: 10.55414/ezxj9k69
6. Vila-Miravent, J, Villar, F, Celdrán, M, and Fernández, E. El modelo de la atención centrada en la persona: análisis descriptivo de una muestra de personas mayores con demencia en centros residenciales. Aloma. (2012) 30:109–117180.
7. Instituto de Salud Carlos III. El futuro de la investigación en cuidados desde la perspectiva de seis enfermeras Honoris Causa. Madrid: Unidad de investigación en cuidados y servicios de salud (2021). Available at: https://www.isciii.es/QuienesSomos/CentrosPropios/INVESTEN/SiteAssets/Paginas/Encuentros/El%20futuro%20de%20la%20investigacio%CC%81n%20en%20cuidados%20desde%20la%20perspectiva%20de%20SEIS%20ENFERMERAS%20Honoris%20Causa.pdf (Accessed March 13, 2023).
8. Urra, ME, Jana, AA, and García, MV. Algunos aspectos esenciales del pensamiento de Jean Watson y su teoría de cuidados transpersonales. Cienc Enferm. (2011) 17:11–22. doi: 10.4067/S0717-95532011000300002
9. Izquierdo-Machín, E. Enfermería: Teoría de Jean Watson y la inteligencia emocional, una visión humana. Rev Cubana Enferm. (2015) 31.
10. Carlosama, DM, Villota, NG, Benavides, VK, Villalobos, FH, Hernández, EL, and Matabanchoy Tulcan, SM. Humanización de los servicios de salud en Iberoamérica: una revisión sistemática de la literatura. Pers Bioet. (2019) 23:245–62. doi: 10.5294/pebi.2019.23.2.6
11. Silva, JNB, Gomes, ACMS, Guedes, HCS, Lima, EAP, Januário, DC, and Santos, M. Behavior of nursing professionals and the implementation of hospital humanization policy. Rev Pesqui. (2020) 12:471–8. doi: 10.9789/2175-5361.rpcfo.v12.8527
12. Troncoso, MP, and Suazo, SV. Cuidado humanizado: un desafío para las enfermeras en los servicios hospitalarios. Acta Paul Enferm. (2007) 20:499–503. doi: 10.1590/S0103-21002007000400019
13. Silveira, RE, and Contim, D. Health education and humanized practice of nursing at intensive care units: bibliometric study. Rev Pesqui. (2015) 7:2113–22. doi: 10.9789/2175-5361.2015.v7i1.2113-2122
14. Schveitzer, MC, Zoboli, EL, and Vieira, MM. Nursing challenges for universal health coverage: a systematic review. Rev Lat Am Enfermagem. (2016) 24:e2676. doi: 10.1590/1518-8345.0933.2676
15. Diaz-Rodríguez, M, Alcántara-Rubio, L, Aguilar-Garcia, D, Puertas-Cristobal, E, and Cano-Valero, M. Orientaciones formativas para un cuidado humanizado en enfermería: una revisión integrativa de la literatura. Enf Global. (2020) 19:640–72.
16. Meneses-La-Riva, ME, Suyo-Vega, JA, and Fernández-Bedoya, VH. Humanized care from the nurse-patient perspective in a hospital setting: a systematic review of experiences disclosed in Spanish and Portuguese scientific articles. Front Public Health. (2021) 9:737506. doi: 10.3389/fpubh.2021.737506
17. Santos, BM, Silva, RMCRA, Pereira, ER, Joaquim, FL, and Goés, TRP. Nursing students’ perception about humanized care: an integrative review. Rev Bras Enferm. (2017) 71:2800–7. doi: 10.1590/0034-7167-2017-0845
18. Casate, JC, and Corrêa, AK. The humanization of care in the education of health professionals in undergraduate courses. Rev Esc Enferm USP. (2012) 46:219–26. doi: 10.1590/s0080-62342012000100029
19. Ribeiro, JP, Gomes, GC, and Thofehrn, MB. Health facility environment as humanization strategy care in the pediatric unit: systematic review. Rev Esc Enferm USP. (2014) 48:530–9. doi: 10.1590/s0080-623420140000300020
20. Page, MJ, McKenzie, JE, Bossuyt, PM, Boutron, I, Hoffmann, TC, Mulrow, CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. (2021) 372:n71. doi: 10.1136/bmj.n71
21. Eriksen, MB, and Frandsen, TF. The impact of patient, intervention, comparison, outcome (PICO) as a search strategy tool on literature search quality: a systematic review. J Med Libr Assoc. (2018) 106:420–31. doi: 10.5195/jmla.2018.345
22. von Elm, E, Altman, DG, Egger, M, Pocock, SJ, Gøtzsche, PC, Vandenbroucke, JP, et al. Declaración de la Iniciativa STROBE (strengthening the reporting of observational studies in epidemiology): directrices Para la comunicación de estudios observacionales. Gac Sanit. (2008) 22:144–50. doi: 10.1157/13119325
23. Cano-Arana, A, González-Gil, T, and Cabello-López, JB. Por CASPe. Plantilla para ayudarte a entender un estudio cualitativo In: CASPe. Guías CASPe de Lectura Crítica de la Literatura Médica. Alicante: CASPe (2010). Cuaderno III). 3–8.
24. Hong, QN, Pluye, P, Fàbregues, S, Bartlett, G, Boardman, F, Cargo, M, et al. Mixed methods appraisal tool (MMAT), version 2018. Registration of copyright (#1148552). Canadian Intellectual Property Office, Industry Canada. (2018).
25. Rostom, A, Dubé, C, Cranney, A, Saloojee, N, Sy, R, Garritty, C, et al. Quality assessment forms. Rockville, MD: Agency for Healthcare Research and Quality (2014) Appendix D. 2004 Sep. (Evidence Reports/Technology assessments, No. 104.
26. JBI Checklist. JBI Checklist: Joanna Briggs Institute (JBI) Critical Appraisal Checklist for Qualitative Research (JBI Manual for Evidence synthesis. Appendix 2.1). (2017). Available at: https://wiki.joannabriggs.org/display/MANUAL/Appendix+2.1%3A+JBI+Critical+Appraisal+Checklist+for+Qualitative+Research.
27. Ferreira, MC, Monteschio, LVC, Teston, EF, Oliveira, L, Serafim, D, and Marcon, SS. Perceptions of nursing professionals about humanization of childbirth in a hospital environment. Rev Rene. (2019) 20:e41409. doi: 10.15253/2175-6783.20192041409
28. Silva Junior, SV, Machado, AG, Alves, AMRS, Cordeiro, KJS, Barbosa, MB, Teodozio, GC, et al. Humanizing intensive nursing care for people with COVID-19. Rev Rene. (2021) 22:e62584. doi: 10.15253/2175-6783.20212262584
29. Santos, PMD, Rodrigues, KS, Pinheiro, LA, Santana, BS, Ipólito, MZ, and Magro, MCDS. Religious and spiritual support in the conception of nurses and families of critical patients: a cross-sectional study. Rev Esc Enferm USP. (2021) 55:e20200508. doi: 10.1590/1980-220X-REEUSP-2020-0508
30. Soares, PR, Silva, CRLD, and Louro, TQ. Comfort of the child in intensive pediatric therapy: perception of nursing professionals. Rev Bras Enferm. (2020) 73:e20180922. doi: 10.1590/0034-7167-2018-0922
31. Soares, LG, Soares, LG, Decesário, MN, and Higarashi, IH. Perception of families on reception in the neonatal context during an intervention. Rev Pesqui. (2019) 11:147–53. doi: 10.9789/2175-5361.2019.v11i1.147-153
32. Barroso, MCCS, Santos, RSFV, Santos, AEV, Nunes, MDR, and Lucas, EAJCF. Children’s perception of venipuncture through therapeutic toy. Acta Paul Enferm. (2020) 33:e–APE20180296. doi: 10.37689/acta-ape/2020AO0296
33. Rocha, MGL, Linard, AG, Santos, LVF, and Sousa, LB. Embracement in gynecological nursing consultation: women’s perceptions of the family health strategy. Rev Rene. (2018) 19:e3341. doi: 10.15253/2175-6783.2018193341
34. Coelho, AC, Lopes, CT, Lopes, JL, Santos, VB, and Barros, ALBL. Needs of family members of patients in a coronary care unit. Einstein. (2022) 20:eAO6258. doi: 10.31744/einstein_journal/2022AO6258
35. Souza, MAR, Wall, ML, Thuler, ACMC, and Souza, SRRK. Prenatal as a facilitator in the participation of companions during labor and delivery. Rev Pesqui. (2021) 12:197–202. doi: 10.9789/2175-5361.rpcfo.v12.7201
36. Nóbrega, MCP, Silva, MI, Albuquerque, GPM, Lima-Castro, JF, de Mendonça, FW, and de Holanda, VR. Assessment of the quality of natural childbirth care in hospital setting through the Bologna index. Enferm Glob. (2022) 21:356–97. doi: 10.6018/eglobal.487441
37. Maia, EBS, Banca, RO, Rodrigues, S, Pontes, ECD, Sulino, MC, and Lima, RAG. The power of play in pediatric nursing: the perspectives of nurses participating in focal groups. Texto Contexto Enferm. (2022) 31:e20210170. doi: 10.1590/1980-265X-TCE-2021-0170
38. Silva, TM, Sousa, KHJF, Oliveira, ADS, Amorim, FCM, and Almeida, CAPL. Obstetric violence: theme approach in the training of Certifi ed nurse-midwives. Acta Paul Enferm. (2020) 33:eAPE20190146. doi: 10.37689/acta-ape/2020AO01466
39. Alvares, AS, Corrêa, ÁCP, Nakagawa, JTT, Valim, MD, Jamas, MT, and Medeiros, RMK. Hospital obstetric practices and their repercussions on maternal welfare. Rev Esc Enferm. (2020) 54:e03606. doi: 10.1590/S1980-220X2018039003606
40. Torres, DG, Rojas, GTR, Garduño, MDM, and Peres, AM. Professional autonomy for perinatal nurses: social perception of competences gained. Rev Enferm. (2019) 27:e37778. doi: 10.12957/reuerj.2019.37778
41. Colaço, AD, Meirelles, BHS, Heidemann, ITSB, and Villarinho, MV. Care for the person who lives with Hiv/aids in primary health care. Texto Contexto Enferm. (2019) 28:e20170339. doi: 10.1590/1980-265X-TCE-2017-0339
42. Cordeiro, EL, Silva, TM, Silva, LSR, Pimentel, RVT, Veloso, ACF, Cabral, MMO, et al. A humanização na assistência ao parto e ao nascimento. REUOL. (2018) 12:2154–62. doi: 10.5205/1981-8963-v12i8a236334p2154-2162-2018
43. López-Tarrida, AC, Ruiz-Romero, V, and González-Martín, T. Cuidando con sentido: la atención de lo espiritual en la práctica clínica desde la perspectiva del profesional. Rev Esp Salud Publica. (2020) 94:e202001002. doi: 10.4321/s1135-57272020000100024
44. Esteban-Sepúlveda, S, Fabregas-Mitjans, M, Ordobas-Pages, L, Tutusaus-Arderiu, A, Andreica, LE, and Leyva-Moral, JM. The experience of giving birth in a hospital in Spain: humanization versus technification. Enferm Clin. (2022) 32:S14–22. doi: 10.1016/j.enfcle.2021.10.007
45. Hernández-Garre, JM, Maya-Sánchez, B, and Pérez, PE. Etno-obstetricias hospitalarias mixtas: Redes clínicas de transición hacia la humanización asistencial. Cul Cuid. (2020) 58:178–95. doi: 10.14198/cuid.2020.58.16
46. Anguita, MV, Sanjuan-Quiles, Á, Ríos-Risquez, MI, Valenzuela-Anguita, MC, Juliá-Sanchis, R, and Montejano-Lozoya, R. Humanization of healthcare at the emergency department: a qualitative analysis based on nurses’ experiences. Referência. (2019) 4:59–68. doi: 10.12707/RIV19030
47. Gros-Polo, S, Navas-Ferrer, C, and Germán-Bes, C. Percepción de los cuidados visibles e invisibles desde una doble perspectiva en una Unidad de Hemodiálisis. Index Enferm. (2019) 28:174–8.
48. Navarrete-Correa, T, Fonseca-Salamanca, F, and Barría, RM. Humanized care from the perception of oncology patients from southern Chile. Invest Educ Enferm. (2021) 39:e04. doi: 10.17533/udea.iee.v39n2e04
49. Monje, VP, Miranda, CP, Oyarzún, GJ, Seguel, PF, and Flores, GE. Percepción De Cuidado Humanizado De Enfermería Desde La Perspectiva De Usuarios Hospitalizados. Cienc Enferm. (2018) 240:43–52. doi: 10.4067/s0717-95532018000100205
50. Melo, RCCP, Queirós, PJP, Tanaka, LH, Henriques, LVL, and Neves, HL. Nursing students’ relational skills with elders improve through humanitude care methodology. Int J Environ Res Public Health. (2020) 17:8588. doi: 10.3390/ijerph17228588
51. Guillaumie, L, Boiral, O, Desgroseilliers, V, Vonarx, N, and Roy, B. Empowering nurses to provide humanized Care in Canadian Hospital Care Units: a qualitative study. Holist Nurs Pract. (2022) 36:311–26. doi: 10.1097/HNP.0000000000000418
52. Reynaga-Ornelas, L, Díaz-García, NY, González-Flores, AD, Meza-García, CF, and Rodríguez-Medina, RM. Evaluation of caring Behaviours by nurses: a perspective by hospitalized adult persons. Metas Enferm. (2022) 25:5–13. doi: 10.35667/MetasEnf.2022.25.1003081921
53. Zamaniniya, Z, Khademi, M, Toulabi, T, and Zarea, K. The outcomes of humanistic nursing for critical care nurses: a qualitative study. Nurs Midwifery Stud. (2021) 10:114–20. doi: 10.4103/nms.nms_32_19
54. Villa, LLO, Silva, JC, Costa, FR, and Camargo, CL. The perception of the companion of the humanized care in a pediatric intensive care unit. Rev Pesqui. (2017) 9:187–92. doi: 10.9789/2175-5361.2017.v9i1.187-192
55. Souza, JSR, Rodrigues, ASC, Leite, MAC, Moraes, CM, Freitas, PS, and Sawada, NO. The performance of nurses in the family health strategy for children suffering maltreatment: an integrative review. R Pesq Cuid Fundam. (2022) 14:e11360. doi: 10.9789/2175-5361.rpcfo.v14.11360
Keywords: humanization of assistance, nursing care, nurse–patient relations, systematic review, working conditions
Citation: Reyes-Téllez Á, González-García A, Martín-Salvador A, Gázquez-López M, Martínez-García E and García-García I (2024) Humanization of nursing care: a systematic review. Front. Med. 11:1446701. doi: 10.3389/fmed.2024.1446701
Edited by:
Te-Chuan Chen, National Sun Yat-sen University, TaiwanReviewed by:
Chang-Chyi Jenq, Linkou Chang Gung Memorial Hospital, TaiwanCopyright © 2024 Reyes-Téllez, González-García, Martín-Salvador, Gázquez-López, Martínez-García and García-García. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Alberto González-García, YWxiZXJ0b2dvbnphbGV6QHVnci5lcw==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.