
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Med. , 25 July 2024
Sec. Rheumatology
Volume 11 - 2024 | https://doi.org/10.3389/fmed.2024.1418995
 Lidia Valencia-MuntalàCarmen Gómez-Vaquero†Laura Berbel-ArcobéDiego BenaventPaola Vidal-Montal
Lidia Valencia-MuntalàCarmen Gómez-Vaquero†Laura Berbel-ArcobéDiego BenaventPaola Vidal-Montal Xavier Juanola
Xavier Juanola Javier Narváez
Javier Narváez Joan M. Nolla*†
Joan M. Nolla*†Introduction: Data on prevalence of fatigue in rheumatoid arthritis (RA) patients in the era of biological treatments remains scarce, with a lack of case-control studies. This study evaluates the prevalence of fatigue in Spanish women over 50 years with RA using the Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-F) scale, explores its association with RA-related variables, and seeks to identify the primary factors influencing fatigue. Ultimately, our objective is to underscore the clinical significance of fatigue as a comorbidity and to advocate for its systematic evaluation in routine clinical practice.
Methods: In a case-control study at a tertiary university hospital, 191 women over 50 years (mean age: 67.5 ± 8.8 years) meeting ACR 2010 criteria for RA and age-matched controls were assessed using the FACIT-F scale, SF-12 questionnaire, and RA-related clinical measures.
Results: Fatigue was significantly more prevalent in the RA group (61%) compared to controls (37%, p < 0.001), with RA patients showing lower mean FACIT-F scores (36.0 ± 10.6 vs. 40.0 ± 0.6, p < 0.001). Correlations were noted between FACIT-F scores and C-reactive protein, DAS28, RAPID3, HAQ, and SF-12 scores. A multivariate analysis was performed and four models generated. The final model, with an R2 of 0.817, indicates that fatigue is significantly influenced by disease activity (RAPID 3) and mental and physical health (SF12) and age, explaining 81.7% of the variance in fatigue.
Conclusion: Fatigue remains significantly prevalent and severe in women over 50 years with RA, strongly linked to disease activity, disability, and diminished quality of life. Systematic fatigue assessment and targeted strategies in clinical settings are essential to address this widespread issue. Future research should explore targeted interventions tailored to this demographic to enhance quality of care.
Rheumatoid arthritis (RA), the most commonly diagnosed systemic autoimmune disease worldwide, manifests as a complex condition with persistent and progressive joint and systemic symptoms, one that significantly elevates the risk of disability and mortality (1). It spans a broad spectrum of manifestations that amplify its overall impact, highlighting the essential need for continuous, integral strategies for disease management.
Recent advances in the treatment of RA have markedly enhanced patient outcomes (2), leading to substantial reductions in disease activity and, in certain instances, achieving remission through the targeting of inflammatory pathways. Concurrently, these improvements in managing RA activity have brought greater awareness to associated comorbidities. Beyond conventional concerns like cardiovascular risks, osteoporosis, and infections, clinical practice (3) is increasingly acknowledging other significant issues, including anxiety, depression, sexual dysfunction, sarcopenia, and fatigue.
Fatigue is a complex phenomenon, multifactorial and multidimensional, lacking a universally accepted definition (4). It is experienced as an overwhelming sense of exhaustion that significantly diminishes an individual’s ability to perform daily activities (5). Recognized worldwide, fatigue can occur as an independent condition or in association with medical procedures and treatments. While it is recognized that patients with RA are more likely to experience fatigue (5–7), data on its prevalence in the era of biological treatments remains relatively sparse, with a lack of case-control studies.
The inherently subjective nature of fatigue, coupled with the challenge of quantifying it, has prompted the creation of various assessment tools (8). Despite these efforts, the establishment of clear guidelines for choosing appropriate instruments for research and clinical practice in rheumatic diseases has been challenging. A thorough review (9) was unable to pinpoint a single scale or instrument as the optimal means for measuring fatigue across different rheumatological conditions.
Common measures for assessing fatigue in RA (10) encompass numeric rating scales, such as the Visual Analogue Scale (VAS), and questionnaires, including, among others, the Bristol Rheumatoid Arthritis Fatigue Multidimensional Questionnaire (BRAF-MDQ), the SF-36 Vitality Domain, the Patient-Reported Outcomes Measurement Information System (PROMIS-29) Fatigue T-score, and the Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-F).
Among all, the FACIT-F scale (11), recognized for its detailed measurement of fatigue in individuals with chronic diseases (9), balances assessments of both physical and emotional well-being. Recently, it has been adopted as a patient-reported outcome in several RA clinical trials (12–14) of JAK inhibitors, emphasizing the value of its psychometric properties.
The exact causes of fatigue in RA are not fully understood (15, 16). Although traditionally associated with inflammation, the persistence of fatigue in many RA patients, despite advancements in anti-inflammatory therapies, underscores both its complexity the need for further investigation.
This study aimed to assess the prevalence of fatigue among a large cohort of elderly Spanish women with RA using the FACIT-F scale. Additionally, we explored the relationship between FACIT-F scores and critical RA-related variables to develop an understanding of the key determinants of this condition. Ultimately, our objective was to approach the clinical relevance of this comorbidity, evaluating the feasibility of incorporating systematic analysis of this condition into routine clinical practice.
This observational case-control study focused on women over 50 with RA, comparing them to age-matched controls. RA patients were diagnosed based on the 2010 ACR criteria and recruited during routine rheumatology visits at a tertiary university hospital. Controls were sourced through three primary methods: accompanying individuals of patients at the rheumatology service, those with non-inflammatory musculoskeletal disorders (mainly soft tissue disorders), and individuals attending the hospital for conditions unrelated to musculoskeletal diseases. We carefully ensured that neither the RA patients nor the control group had any conditions known to cause fatigue, such as cancer, heart or respiratory failure, chronic liver or kidney diseases, or central sensitivity syndromes like fibromyalgia. All participants gave written informed consent, and the local ethics committee approved the study (reference: PR057/20).
• Age
• Body mass index (BMI): BMI is the ratio of human body weight to squared height expressed in kg/m2. It has been categorized as follows: < 18.5 kg/m2 is considered underweight; from 18.5 to 25 kg/m2, normal range; from 25 to 30 mg/m2, overweight; and > 30 kg/m2, obese.
• Tobacco use: We categorized the patient population into three groups based on tobacco use: never smokers, current smokers, and former smokers.
• Physical activity: We categorized the patient population based on their levels of physical activity into four groups: none, sporadic, regular with low intensity, and regular with high intensity.
The FACIT-F scale (11) was employed to measure fatigue levels. This scale includes items rated on a scale from 0 to 4, yielding a total possible score that ranges from 0 to 52, where lower scores signify greater levels of fatigue. While there is no universally accepted cutoff for the presence of fatigue, for the purposes of our study, we pre-established a score below 40 to denote “fatigue” which is in line with the several studies available in the literature (17, 18). Additionally, we have indicated the percentage of patients with a FACIT-F score of < 30, which some authors (19) consider indicative of “significant fatigue.”
We employed the SF-12 questionnaire (20). The SF-12, or Short Form Health Survey, is a 12-item questionnaire designed to measure health-related quality of life. It assesses functional health and well-being from the patient’s perspective. The SF-12 includes two composite scores representing physical and mental health. It is a condensed version of the SF-36 survey, aimed at reducing the burden on respondents while preserving essential health status information. For each participant, two summary scores were calculated: one for physical health and another for mental health. The scores range from 0 to 100, where a higher value indicates a better health-related quality of life.
• Evaluation of RA history: (a) disease duration; (b) positivity of rheumatoid factor (RF), along with their titers; (c) positivity for anti-citrullinated peptide antibodies (ACPA), along with their titers; (d) current treatment (glucocorticoids, conventional disease-modifying antirheumatic drugs, biological disease-modifying antirheumatic drugs, Jak inhibitors).
• Analytical evaluation. We considered the following parameters: (a) albumin levels; (b) erythrocyte sedimentation rate (ESR); (c) C-reactive protein (CRP); and (d) hemoglobin levels. The values corresponding to the last analytical study carried out were considered.
• Evaluation of RA activity using metrological indices. We utilized two indices for this purpose: (a) the Disease Activity Score 28 (DAS28) and (b) the Routine Assessment of Patient Index Data 3 (RAPID3).
(a) DAS28 (21) is a composite index of disease activity comprising tender and swollen joint counts in 28 joints, the Patient’s Global Assessment of Disease Activity and the ESR. The higher the score, the higher the activity level. A value < 2.6 suggests disease remission, a value between ≥ 2.6 and ≤ 3.2 suggests low disease activity, a value > 3.2− ≤ 5.1 suggests moderate disease activity and, finally, a value > 5.1 suggests high disease activity.
(b) RAPID3 (22) is a validated index for measuring disease activity in patients with RA that includes three measures self-reported by the patient: pain, physical function, and global assessment of the disease. The higher the score, the higher the activity level. A value ≤ 3 suggests disease remission, a value between 3.01 and 6 suggests low disease activity, a value between 6.01 and 12 suggests moderate disease activity and a value > 12 suggests high disease activity.
• Evaluation of disability. We used the Health Assessment Questionnaire (HAQ) (23). This questionnaire assesses physical functioning as difficulty performing daily living activities; the score ranges from 0 to 3. The higher the score, the higher the disability level.
To determine the sample size necessary for our case-control study, we utilized the following parameters: a prevalence of fatigue estimated at 50% among cases and 35% among controls, a significance level (alpha) set at 0.05, and a power (1−beta) of 0.8, reflecting an 80% power to detect a significant difference. The ratio of cases to controls was established at 1:1.
The calculations indicated that a sample size of 169 cases and 169 controls, totaling 338 participants, was required to detect a significant difference in fatigue prevalence between the case group (women with RA) and the control group, at the specified significance and power levels.
Data are presented as the mean plus or minus the standard deviation/median and interquartile range for continuous variables and as a number and percentage for categorical variables. Prevalence rates are given as percentages. Continuous variables were tested for normality using the Kolmogorov-Smirnov test. Differences among parametric variables were assessed using ANOVA; for non-parametric variables, we used the U-Mann-Whitney or Kruskal-Wallis tests, when indicated. Differences among categorical variables were evaluated by the chi-squared test.
To assess the relationship between the variables of interest in this study, a correlation analysis using Pearson’s correlation coefficient was conducted. This analysis allowed us to examine linear associations between pairs of variables and determine the strength and direction of these relationships.
A multivariate study by multiple regression including all the variables that correlated with FACT-F plus age, BMI and RA disease duration was used to identify independent factors influencing fatigue.
Table 1 presents the characteristics of the 191 patients with RA included in the study. In the cohort the average age was 67.5 ± 8.8 years, with a mean BMI of 27.9 ± 5.4 kg/m2. The average disease duration among the participants was 16.8 ± 10.3 years. DAS28 scores showed 40.5% in remission and 32% with moderate disease activity, while RAPID3 scores revealed 34% in moderate and another 34% in high disease activity. The HAQ score suggested low disability, and 90% were on DMARDs. FACIT- F and SF-12 scores indicated significant fatigue and reduced quality of life, highlighting the substantial impact of RA on patient well-being.
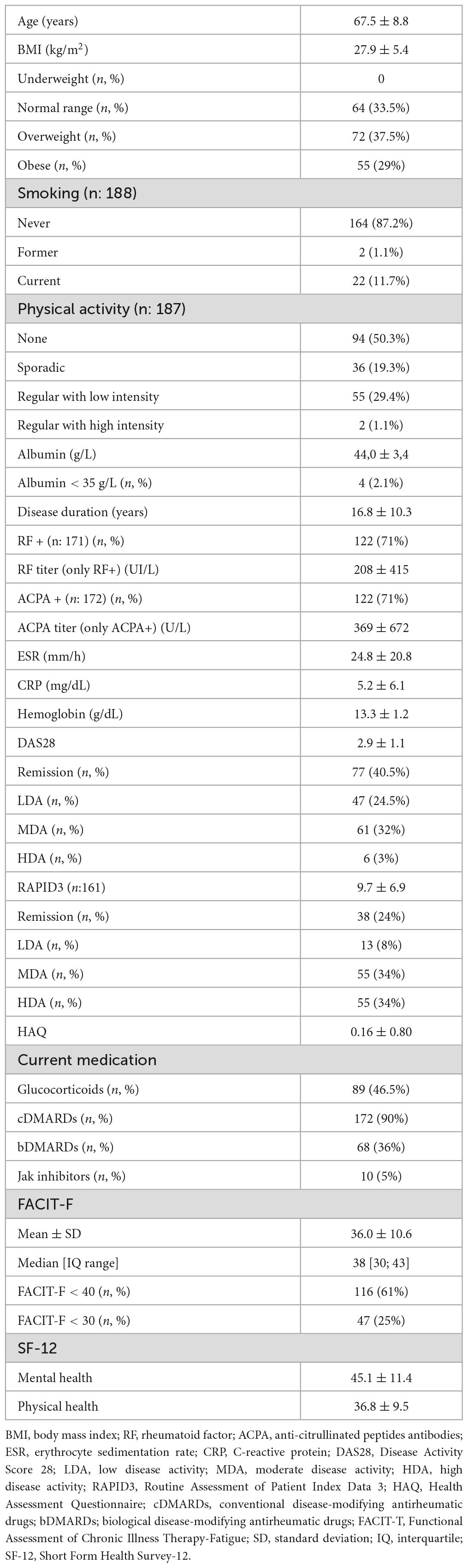
Table 1. Characteristics of the patients with RA (n: 191) included in the study.
Table 2 shows a comparison between patients with RA and controls. The proportion of patients with fatigue (FACIT-F score < 40) was 61%, significantly higher (p < 0. 001) than observed in the control group (35%). In 47 patients (25%), fatigue was considered significant.
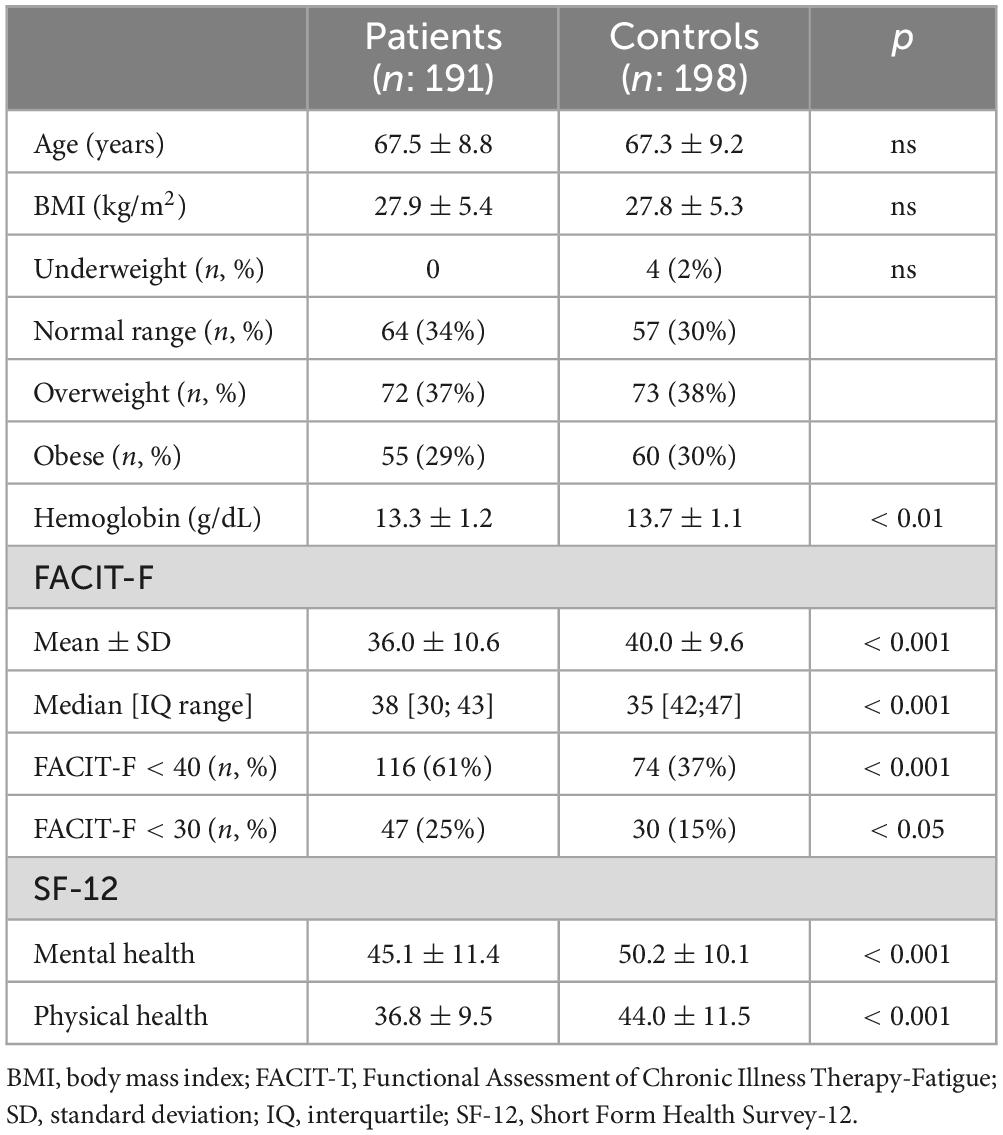
Table 2. Comparison of patients with RA and controls.
Mean value of FACIT-F in RA patients was 36.0 ± 10.6. This value was significantly lower (p < 0.001) than that obtained in the control group (40.0 ± 9.6).
Patients with RA presented a significantly lower values of hemoglobin levels. In addition, the scores of both dominions of SF-12 were significantly lower than in the control group.
Table 3 underline the profound impact of fatigue on disease burden. Patients with RA and fatigue displayed significantly higher disease activity and poorer quality of life compared to those without fatigue. While demographic and clinical characteristics such as age, BMI, disease duration and RF and ACPA positivity were similar across groups, the impact of fatigue was evident in higher disease activity scores and quality of life measurements.
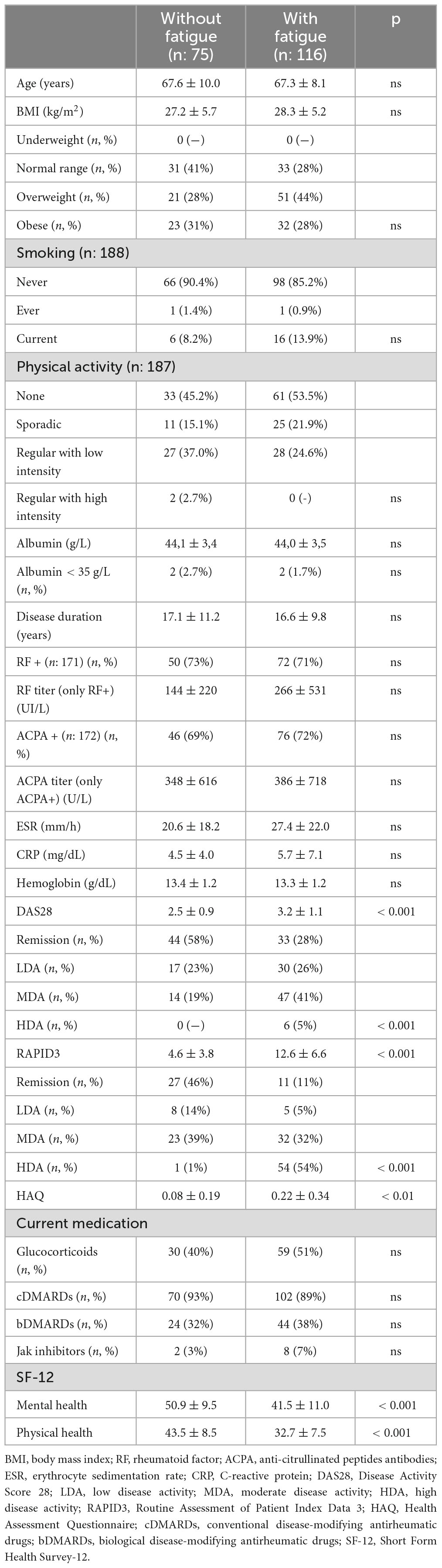
Table 3. Characteristics of the patients with RA and the differences between the ones without and with fatigue.
In RA patients, FACIT-F correlated significantly with clinical and quality of life parameters (Table 4). Negative correlations with CRP, DAS 28, RAPID3 and HAQ highlighted that increased inflammation, disease activity, higher disability and perceived disease severity were associated with greater fatigue. Positive correlations with SF-12 Mental Health and Physical Health demonstrated that lower fatigue levels are associated with better quality of life.
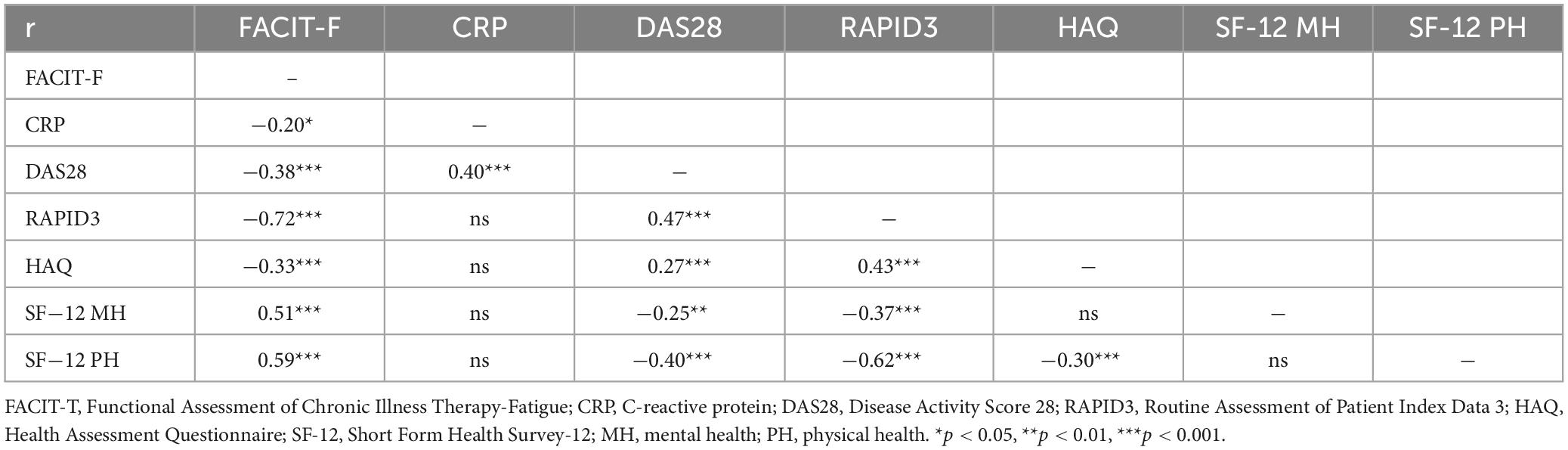
Table 4. Bivariate correlations between FACIT and the rest of variables.
A stepwise multiple regression was conducted to identify factors influencing fatigue measured by FACIT-F, incorporating variables correlated with FACT-F, age, BMI, and RA disease duration. Four models were generated. Model 1 included RAPID 3, showing a significant negative relationship with fatigue (B = −1.159, p < 0.001). Model 2 added SF12 mental showing a significant positive relationship (B = 0.286, p < 0.001). Model 3 included the physical component of SF12. Model 4 added age, with a smaller effect (B = 0.153, p = 0.011). The final model, with an R2 of 0.817, indicates that fatigue is significantly influenced by disease activity (RAPID 3) and mental and physical health (SF12) and age, explaining 81.7% of the variance in fatigue. The coefficients and significance of each variable in the final model are presented in Table 5.
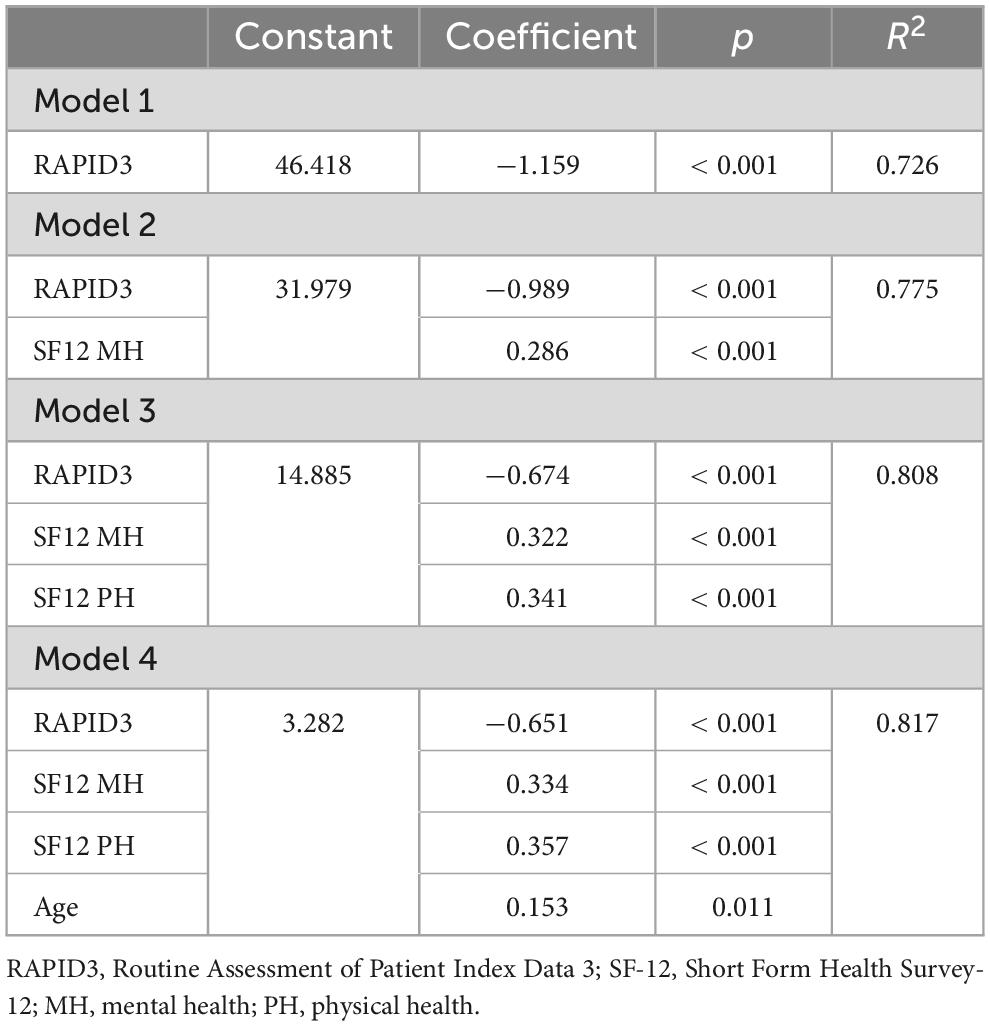
Table 5. Multivariate analysis including all the variables that correlated with FACIT-F plus age, BMI and RA disease duration.
Fatigue is a critical symptom commonly reported across a wide range of conditions, including oncological (24), neurological (25), and renal (26) diseases. Traditionally, the significance of fatigue in rheumatic diseases was underestimated. Nonetheless, the Outcome Measures in Rheumatology (OMERACT) conference in 2002 (27) marked a pivotal moment by formally acknowledging the importance of fatigue in musculoskeletal disorders and its profound effects on patients’ health-related quality of life. Following this, the 2007 OMERACT conference (28) recommended incorporating fatigue measurements in clinical trials for RA whenever possible. Since then, fatigue has been recognized as a key clinical symptom (29) in this inflammatory rheumatic disease and identified as a critical target for therapeutic intervention. Moreover, it is now established that fatigue stands out as a particularly significant symptom for individuals with RA (30), primarily due to its challenging management and substantial impact on all facets of daily life. Despite this recognition, there is no clear recommendation on whether to systematically analyze fatigue in clinical settings.
The estimated prevalence of fatigue in RA varies from 40 to 70% (31) and data on its prevalence in the “biological era” are limited (6, 17, 18, 32, 33). Our data, collected from elderly women with long−standing RA and assessed using the FACIT-F scale, confirm that fatigue remains a significant concern. The observed prevalence (61%) was notably high and significantly higher than in the control population (35%). Additionally, we observed that patients with RA had a mean FACIT-F value that was significantly lower than that of the control group, indicating greater fatigue severity.
The value noted in the control group (40.0 ± 9.6) was only marginally lower compared to that seen (42.7 ± 8.9) in a large sample (n = 1352) of the general German population (mean age: 49.9 ± 17.5 years) (34). This observation, in our opinion, underscores the appropriateness of our control group, especially in light of evidence showing that fatigue levels tend to increase with age in the general population (35).
To date, only three studies have analyzed the prevalence of fatigue in RA patients using the FACIT-F scale (17, 18, 33). Table 6 shows their main characteristics and compares their findings with those of the present study. The previous studies were cross-sectional, did not incorporate control groups, and to varying degrees, included men in their study populations.
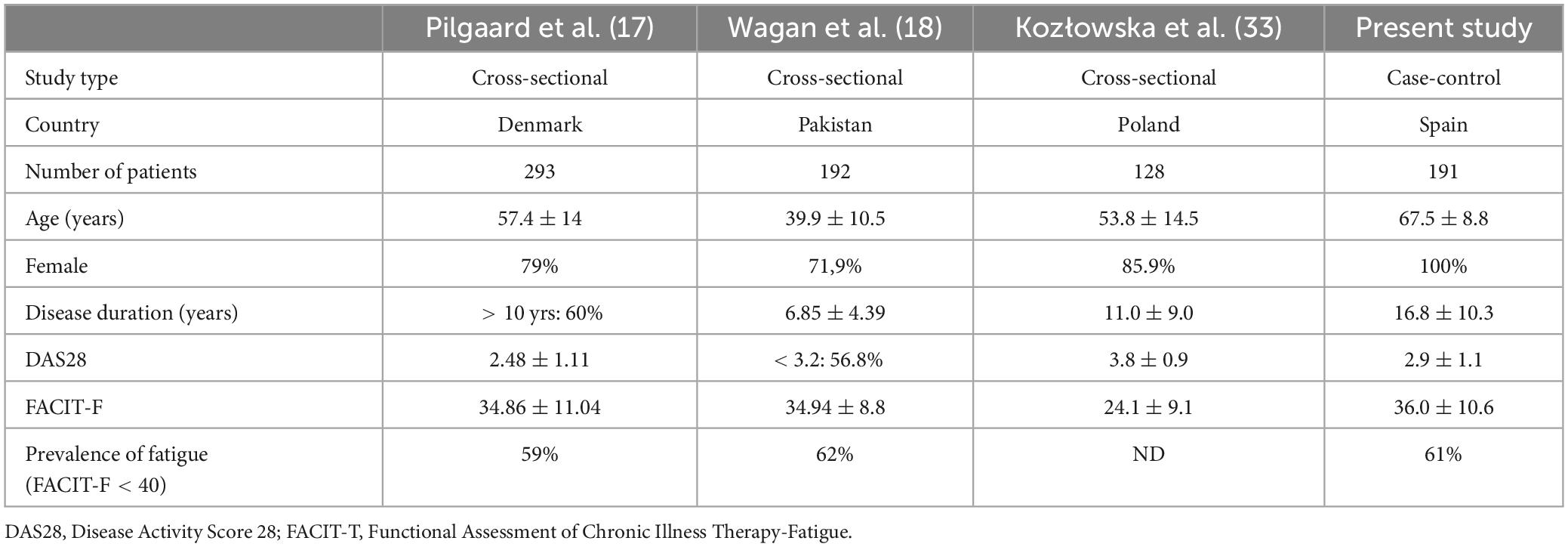
Table 6. Characteristics of studies on fatigue in RA conducted with the FACIT-F scale.
The obtained frequency of fatigue, and the mean FACIT-F value, in our study, was practically the same as in the studies by Pilgaard et al. (17) and Wagan et al. (18), despite differences in patient age and disease duration. In fact, as anticipated, its significantly exceeded the baseline values observed in the three clinical trials (12–14) where fatigue was assessed using this scale. The lowest FACIT-F value was observed in the study by Kozlowska et al. (33), probably because in their cohort the disease activity was clearly higher (mean DAS28: 3.8 ± 0.9).
We observed an inverse relationship between the FACIT-F scores and those of CRP, DAS28, and RAPID3. The relationship was particularly pronounced with the latter parameter, which, to our knowledge, marks the first time it has been associated with fatigue in RA patients. Interestingly, RAPID3, like FACIT-F, is a patient-reported outcome that does not require any clinical or analytical parameters and is solely based on the patient’s perception (36).
The multivariate analysis highlights RAPID 3 as a pivotal predictor of fatigue in RA patients. The significant negative relationship between RAPID 3 scores and fatigue emphasizes that higher levels of patient-reported disability and pain are strongly associated with increased fatigue. The consistent significance of RAPID 3 across various models demonstrates its robustness as a predictor, explaining a substantial portion of the variance in fatigue. This finding suggests that targeting reductions in disease activity could be a key strategy in mitigating fatigue in patients with RA.
The data obtained appear to suggest that the activity of RA exerts a deleterious effect on fatigue levels. Indeed, other researchers (4, 29) have found a positive correlation between fatigue and both the ESR and the DAS28, though not with the ratio of swollen to tender joints, with pain emerging as the predominant factor. This raises the possibility that while disease activity may be associated with fatigue, its contribution may not be significant once adjustments for pain are made.
We have not observed a correlation between disease duration and FACIT scores in our study. Research (5–7) indicates that the relationship between disease duration and fatigue in patients with RA can be variable. Some studies report that fatigue is a prevalent symptom irrespective of how long a patient has been diagnosed with RA, suggesting that fatigue can manifest in both early and long-standing cases.
As expected, we observed that patients with RA, have lower hemoglobin levels compared to the control group. However, no correlation was found between FACIT-F and this analytical parameter. This fact could suggest that hemoglobin doesn’t plays a significative role in the etiopathogenesis of fatigue, when no relevant anemia is found.
Finally, a relationship was identified between FACIT-F scores and both HAQ and SF-12, encompassing both the mental and physical components. These findings underscore the significant impact of fatigue on disability (37) and the resulting deterioration in health-related quality of life (38).
This study presents certain noteworthy limitations. Firstly, the patient cohort consisted exclusively of women. This approach, however, allowed us to focus on an often-underrepresented demographic in RA research (women with advanced age). Secondly, while the study’s single-center nature might raise questions about the generalizability of our findings, we are confident that our cohort reflects the characteristics of patients with long-standing RA typically followed in university hospitals. Thirdly, we have not systematically evaluated depression in our patients, nor have we considered the presence of this condition as an exclusion criterion. It is estimated that depression is twice as common in patients with RA as in the general population (39); additionally, previous research (40) has reported a strong association between depression and high fatigue scores. Fourthly, although we focused heavily on excluding individuals with diseases capable of inducing fatigue from the control group, the fact that some of them were selected during their hospital visits could mean that the frequency of fatigue is somewhat higher than what would have been obtained had the control group been community-based. Fifthly, given the exclusive inclusion of women in this study, our findings do not offer a comparative gender perspective on fatigue in rheumatoid arthritis; future research should aim to include a more diverse gender representation to fully explore this aspect. Sixthly, although we systematically excluded both patients and controls with conditions clearly associated with fatigue, we did not provide a detailed description of the comorbid conditions present in both groups. Seventhly, the study’s design does not allow for the establishment of causal relationships between RA characteristics and the presence of fatigue. Consequently, caution should be applied in the extrapolation of our findings. Broader, longitudinal studies encompassing more diverse populations are needed to validate and expand upon these observations.
Despite its limitations, we believe this study significantly advances the field by employing, for the first time, a case-control design to analyze fatigue frequency in a clinical setting. By using an internationally recognized and validated scale, our research not only underscores the considerable impact of fatigue on a cohort of long-standing RA patients but also reveals that fatigue prevalence significantly exceeds that of the general population. Moreover, the relationships we have identified offer interesting paths for further investigation aimed at unraveling the etiopathogenesis of fatigue in RA.
In conclusion, our findings highlight the persistent nature of fatigue in RA, demonstrating its substantial prevalence and intensity, which notably surpasses that within the general population and aligns closely with prior research, despite varying patient demographics and disease durations. Fatigue appears to be linked to disease activity, as well as with the disability and the impairment of health-related quality of life that RA entails. Given its clinical impact, in the clinical setting, it seems imperative to systematically include fatigue assessments in patient evaluations and to devise strategies aimed at minimizing the significance of this issue.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by the CEI IDIBELL-Bellvitge University Hospital. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
LV-M: Conceptualization, Data curation, Investigation, Methodology, Writing−original draft, Writing−review and editing. CG-V: Conceptualization, Formal analysis, Investigation, Methodology, Supervision, Validation, Visualization, Writing−original draft, Writing−review and editing. LB-A: Investigation, Writing−original draft, Writing−review and editing. DB: Formal analysis, Investigation, Methodology, Writing−original draft, Writing−review and editing. PV-M: Investigation, Writing−original draft, Writing−review and editing. XJ: Investigation, Writing−original draft, Writing−review and editing. JN: Investigation, Writing−original draft, Writing−review and editing. JMN: Conceptualization, Formal analysis, Investigation, Methodology, Project administration, Supervision, Validation, Visualization, Writing−original draft, Writing−review and editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
We would thank the Spanish Foundation of Rheumatology for providing editorial assistance during the preparation of the manuscript [FERBT2023]. We would also thank CERCA programme/Generalitat de Catalunya for institutional support.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Di Matteo A, Bathon J, Emery P. Rheumatoid arthritis. Lancet. (2023) 402:2019–33. doi: 10.1016/S0140-6736(23)00758-8
2. Sparks J, Harrold L, Simon T, Wittstock K, Kelly S, Lozenski K, et al. Comparative effectiveness of treatments for rheumatoid arthritis in clinical practice: A systematic review. Semin Arthritis Rheum. (2023) 62:152249. doi: 10.1016/j.semarthrit.2022.152249
3. Espinoza G, Maldonado G, Narvaez J, Guerrero R, Citera G, Rios C. Beyond rheumatoid arthritis evaluation: What are we missing? Open Access Rheumatol Res Rev. (2021) 13:45–55. doi: 10.2147/OARRR.S278727
4. Tiesinga L, Dassen T, Halfens R. Fatigue: A summary of the definitions, dimensions, and indicators. Nurs Diagn. (1996) 7:51–62. doi: 10.1111/j.1744-618x.1996.tb00293.x
5. Seifert O, Baerwald C. Impact of fatigue on rheumatic diseases. Best Pract Res Clin Rheumatol. (2019) 33:101435. doi: 10.1016/j.berh.2019.101435
6. Katz P. Fatigue in rheumatoid arthritis. Curr Rheumatol Rep. (2017) 19:25. doi: 10.1007/s11926-017-0642-7
7. Ifesemen O, McWilliams D, Norton S, Kiely P, Young A, Walsh D. Fatigue in early rheumatoid arthritis: Data from the early rheumatoid arthritis network. Rheumatology. (2022) 61:3737–45. doi: 10.1093/rheumatology/keab947
8. Dures E, Farisoğulları B, Santos E, Molto A, Feldthusen C, Harris C, et al. 2023 EULAR recommendations for the management of fatigue in people with inflammatory rheumatic and musculoskeletal diseases. Ann Rheum Dis. (2023): doi: 10.1136/ard-2023-224514
9. Elera-Fitzcarrald C, Rocha J, Burgos P, Ugarte-Gil M, Petri M, Alarcón G. Measures of fatigue in patients with rheumatic diseases: A critical review. Arthritis Care Res. (2020) 72:369–409. doi: 10.1002/acr.24246
10. Pope J. Management of fatigue in rheumatoid arthritis. RMD Open. (2020) 6:e001084. doi: 10.1136/rmdopen-2019-001084
11. Webster K, Cella D, Yost K. The functional assessment of chronic illness therapy (FACIT) measurement system: Properties, applications, and interpretation. Health Q Life Outcomes. (2003) 1:79.
12. Genovese M, Kalunian K, Gottenberg J, Mozaffarian N, Bartok B, Matzkies F, et al. Effect of Filgotinib vs placebo on clinical response in patients with moderate to severe rheumatoid arthritis refractory to disease-modifying antirheumatic drug therapy: The FINCH 2 randomized clinical trial. JAMA. (2019) 322:315–25. doi: 10.1001/jama.2019.9055
13. Bartlett S, Bingham C, van Vollenhoven R, Murray C, Gruben D, Gold D, et al. The impact of tofacitinib on fatigue, sleep, and health-related quality of life in patients with rheumatoid arthritis: A post hoc analysis of data from Phase 3 trials. Arthritis Res Ther. (2022) 24:83. doi: 10.1186/s13075-022-02724-x
14. Strand V, Tundia N, Bergman M, Ostor A, Durez P, Song I, et al. Upadacitinib improves patient-reported outcomes vs placebo or adalimumab in patients with rheumatoid arthritis: Results from SELECT-COMPARE. Rheumatology. (2021) 60:5583–94. doi: 10.1093/rheumatology/keab158
15. Beckers E, Hermans K, Van Tubergen A, Boonen A. Fatigue in patients with rheumatic and musculoskeletal diseases: A scoping review on definitions, measurement instruments, determinants, consequences, and interventions. RMD Open. (2023) 9:e003056. doi: 10.1136/rmdopen-2020-001056
16. Tanaka Y, Ikeda K, Kaneko Y, Ishiguro N, Takeuchi T. Why does malaise/fatigue occur? Underlying mechanisms and potential relevance to treatments in rheumatoid arthritis. Expert Rev Clin Immunol. (2024) 15:1–15. doi: 10.1080/1744666X.2024.2306220
17. Pilgaard T, Hagelund L, Stallknecht S, Jensen H, Esbensen B. Severity of fatigue in people with rheumatoid arthritis, psoriatic arthritis, and spondyloarthritis – Results of a cross-sectional study. PLoS One. (2019) 14:e0218831. doi: 10.1371/journal.pone.0218831
18. Wagan A, Raheem A, Bhatti A, Zafar T. Fatigue assessment by FACIT-F scale in Pakistani cohort with rheumatoid arthritis (FAF-RA) study. Pak J Med Sci. (2021) 37:1025–30. doi: 10.12669/pjms.37.4.3602
19. Corominas H, Alegre C, Narváez J, Fernández-Cid C, Torrente-Segarra V, Gómez M, et al. Correlation of fatigue with other disease-related and psychosocial factors in patients with rheumatoid arthritis treated with tocilizumab: ACT-AXIS study. Medicine. (2019) 98:26. doi: 10.1097/MD.0000000000015947
20. Ware J, Kosinski M, Keller S. A 12-item short-form health survey: Construction of scales and preliminary tests of reliability and validity. Med Care. (1996) 34:220–33. doi: 10.1097/00005650-199603000-00003
21. Mäkinen H, Kautiainen H, Hannonen P, Möttönen T, Korpela M, Leirisalo-Repo M, et al. Disease activity score 28 as an instrument to measure disease activity in patients with early rheumatoid arthritis. J Rheumatol. (2007) 34:1987–91.
22. Pincus T, Bergman M, Yazici Y, Hines P, Raghupathi K, Maclean R. An index of only patient-reported outcome measures, routine assessment of patient index data 3 (RAPID3) in two abatacept clinical trials: Similar results to disease activity score (DAS28) and other RAPID indices that include physician-reported measures. Rheumatology. (2008) 47:345–9. doi: 10.1093/rheumatology/kem293
23. Esteve-Vives J, Batlle-Gualda E, Reig A. Spanish version of the health assessment questionnaire: Reliability, validity, and transcultural equivalency. J Rheumatol. (1993) 20:2116–22.
24. Zeinali N, Youn N, Albashayreh A, Fan W, Gilbertson White S. machine learning approaches to predict symptoms in people with cancer: Systematic review. JMIR Cancer. (2024) 10:e52322. doi: 10.2196/52322
25. Zhan J, Zhang P, Wen H, Wang Y, Yan X, Zhan L, et al. Global prevalence estimates of poststroke fatigue: A systematic review and meta-analysis. Int J Stroke. (2023) 18:1040–50.
26. Wilund K, Thompson S, Viana J, Wang A. Physical activity and health in chronic kidney disease. Contribut Nephrol. (2021) 199:43–55. doi: 10.1159/000517696
27. Kirwan J, Heiberg T, Hewlett S, Hughes R, Kvien T, Ahlmèn M, et al. Outcomes from the patient perspective workshop at OMERACT 6. J Rheumatol. (2003) 30:868–72.
28. Kirwan J, Minnock P, Adebajo A, Bresnihan B, Choy E, de Wit M, et al. Patient perspective: Fatigue as a recommended patient centered outcome measure in rheumatoid arthritis. J Rheumatol. (2007) 34:1174–7.
29. Chmielewski G, Majewski M, Kuna J, Mikiewicz M, Krajewska-Włodarczyk M. Fatigue in inflammatory joint diseases. Int J Mol Sci. (2023) 24:12040. doi: 10.3390/ijms241512040
30. Primdahl J, Hegelund A, Lorenzen A, Loeppenthin K, Dures E, Appel Esbensen B. The Experience of people with rheumatoid arthritis living with fatigue: A qualitative metasynthesis. BMJ Open. (2019) 9:e024338. doi: 10.1136/bmjopen-2018-024338
31. Katz P. Causes and consequences of fatigue in rheumatoid arthritis. Curr Opin Rheumatol. (2017) 29:269–76. doi: 10.1097/BOR.0000000000000376
32. Overman C, Kool M, Da Silva J, Geenen R. The prevalence of severe fatigue in rheumatic diseases: An international study. Clin Rheumatol. (2016) 35:409–15. doi: 10.1007/s10067-015-3035-6
33. Kozłowska K, Formanowicz D, Bączyk G. The link between the demographic and clinical factors and fatigue symptoms among rheumatoid arthritis patients. Int J Environ Res Public Health. (2022) 19:14681. doi: 10.3390/ijerph192214681
34. Montan I, Löwe B, Cella D, Mehnert A, Hinz A. General population norms for the functional assessment of chronic illness therapy (FACIT)-fatigue scale. Value Health. (2018) 21:1313–21. doi: 10.1016/j.jval.2018.03.013
35. Watt T, Groenvold M, Bjorner J, Noerholm V, Rasmussen N, Bech P. Fatigue in the Danish general population: Influence of sociodemographic factors and disease. J Epidemiol Commun Health. (2000) 54:827–33. doi: 10.1136/jech.54.11.827
36. Pincus T, Yazici Y, Bergman M. RAPID3, an index to assess and monitor patients with rheumatoid arthritis, without formal joint counts: Similar results to DAS28 and CDAI in clinical trials and clinical care. Rheum Dis Clin North Am. (2009) 35:773–778,viii. doi: 10.1016/j.rdc.2009.10.008
37. Fazaa A, Boussaa H, Ouenniche K, Miladi S, Makhlouf Y, Belhadj S, et al. Baseline predictors of fatigue and persistent fatigue in rheumatoid arthritis: A longitudinal observational study. Musculoskelet Care. (2023) 21:1068–74. doi: 10.1002/msc.1787
38. Santos E, Duarte C, da Silva J, Ferreira R. The impact of fatigue in rheumatoid arthritis and the challenges of its assessment. Rheumatology. (2019) 58:v3–9. doi: 10.1093/rheumatology/kez351
39. Lwin M, Serhal L, Holroyd C, Edwards C. Rheumatoid arthritis: The impact of mental health on disease: A narrative review. Rheumatol Ther. (2020) 7:457–71. doi: 10.1007/s40744-020-00217-4
Keywords: fatigue, rheumatoid arthritis, FACIT-F scale, comorbidity, case-control study
Citation: Valencia-Muntalà L, Gómez-Vaquero C, Berbel-Arcobé L, Benavent D, Vidal-Montal P, Juanola X, Narváez J and Nolla JM (2024) Assessing fatigue in women over 50 years with rheumatoid arthritis: a comprehensive case-control study using the FACIT-F scale. Front. Med. 11:1418995. doi: 10.3389/fmed.2024.1418995
Received: 17 April 2024; Accepted: 08 July 2024;
Published: 25 July 2024.
Edited by:
Rubén Queiro, Foundation for Biosanitary Research and Innovation of the Principality of Asturias (FINBA), SpainReviewed by:
Jose Pinto-Tasende, A Coruña University Hospital Complex (CHUAC), SpainCopyright © 2024 Valencia-Muntalà, Gómez-Vaquero, Berbel-Arcobé, Benavent, Vidal-Montal, Juanola, Narváez and Nolla. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Joan M. Nolla, am0ubm9sbGFAYmVsbHZpdGdlaG9zcGl0YWwuY2F0
†These authors have contributed equally to this work and share senior authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.