 Zixuan Zeng
Zixuan Zeng Zhanghong Lu2†
Zhanghong Lu2† Yong Gan
Yong Gan Lei Huang
Lei Huang- 1Department of Psychiatry, Tongji Hospital, School of Medicine, Tongji University, Shanghai, China
- 2Teaching Office, Renmin Hospital of Wuhan University, Wuhan, China
- 3School of Medicine, Tongji University, Shanghai, China
- 4Department of Social Medicine and Health Management, School of Public Health, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, China
- 5Shanghai Yangpu District Mental Health Center, Shanghai, China
- 6Department of Medical Education, Tongji Hospital, School of Medicine, Tongji University, Shanghai, China
Introduction: Shortage and high turnover intention rate of physicians are concerning problems in China. Professional identity has been shown as an influential factor for physicians’ turnover intention. Enhancing physicians’ professional identity in their early phase of career, standardized residency training program (SRTP), may help reduce the turnover rate. This study aimed to investigate the current status of professional identity and explore its associated psychosocial factors among Chinese SRTP trainees, hoping to provide evidence in strengthening the available medical human resources in China.
Methods: The final sample was comprised of 2,267 Chinese SRTP trainees in this cross-sectional survey conducted from 9 March to 20 March in 2023. Descriptive statistics were calculated. Bivariate analyses and hierarchical multiple linear regression were used to analyze potential associated factors of Chinese SRTP trainees’ professional identity.
Results: The average score of respondents’ professional identity was 47.68 (standard deviation, SD = 8.61). Results from hierarchical multiple linear regression analysis showed that being married (β = 0.066, p < 0.01), having work experience before SRTP (β = 0.036, p < 0.05), being satisfied with annual income (β = 0.062, p < 0.01), psychological distress (β = −0.144, p < 0.001), depersonalization (β = −0.053, p < 0.05), emotional exhaustion (β = −0.380, p < 0.001) and resilience (β = 0.169, p < 0.001) were associated with professional identity (F = 114.301, p < 0.001). All associated factors can explain 41.1% of the variance in professional identity, and individual psychological variables make up a substantial portion (28.6%) of this influence.
Discussion: Individual psychological variables are strongly associated with professional identity. Helping SRTP trainees reduce psychological distress, alleviate burnout and enhance resilience may be effective ways to promote the formation of their professional identity.
Introduction
The shortage of physicians has become a pressing challenge on a global scale (1, 2). Escalated healthcare demands, pronounced attrition rates among physicians, and a diminished influx of graduates entering the medical profession have intensified this predicament worldwide (3, 4). In China, there were only 3.04 physicians per 1,000 population in 2022, relatively low compared to many developed countries (5). Physician turnover intention rates range from 10 to 55% (6, 7). More strikingly, almost half (48%) physicians have reported turnover intention since standardized residency training program (SRTP) (8). The cost of physician turnover can be disruptive. It not only exacerbates the scarcity of healthcare personnel, but also impacts the advancement of the medical profession. Research has demonstrated that professional identity is one of the vital influential factors on physicians’ turnover intention, and a stronger professional identity corresponds to a lower inclination to turnover (9, 10).
Based on psychological or cognitive identity theories, identities are considered as cognitive mental representations that reflect an external reality (11). From this standpoint, individuals define who they are (which social group they belong to) through processes of identification, internalisation and comparison within and across social categories (12). These representations are invisible but their content can be discovered by experimental design, structured interviews or questionnaires (13). For physicians, professional identity refers to the self-perception, sense of belonging and identification with the medical profession, which lead them to think, act and feel like a physician (14). Physicians with a strong professional identity tend to have a sense of pride, purpose and dedication to their medical profession, leading to more engagement, satisfaction and fulfillment in their work. Studies have shown that higher levels of professional identity exerts a positive influence on various aspects of personal and occupational development, including the pursuit of advanced medical abilities, stronger sense of responsibilities, discovery of meaning in work, better mental health status, more job satisfaction and less turnover intention (15–17).
Psychological or cognitive identity theories posit that professional identity develops over time and can be influenced by social interactions, though it remains relatively stable (12). The standardized residency training program (SRTP) is a stage when trainees transition form learners into independent physicians (18, 19). Since the sense of professional identity formed in the early clinical practice has a profound influence on their future career path, SRTP is the key phase to improve their professional identity (20, 21). By reinforcing professional identity, it is beneficial for SRTP trainees to form a congruent professional image with their medical vocation. Meanwhile, SRTP trainees are motivated to achieve comprehensive development in professional competence, ethical standards and patient care, thereby preparing them for future independent clinical practice. In order to improve physicians’ professional identity early in this phase, it is essential to investigate and explore the current status and relevant factors of professional identity among SRTP trainees.
Literature has shown that physicians’ professional identity can be affected by demographics and psychosocial factors (22, 23). Physicians with different races, religions, ethnicities, educational backgrounds and socioeconomic statuses reported different levels of professional identity (24, 25). Work-related and individual psychological variables are two significant psychosocial aspects that can influence professional identity (26, 27). Work situations, such as doctor-patient relationships, work experience, work intensity, input and payback, can significantly impact professional identity (28–30). Psychological distress and burnout are prevalent psychological issues among SRTP trainees (31). They have been shown to diminish professional identity and increase the likelihood of turnover (32). Besides, as one of fundamental components of psychological capital, resilience may facilitate their professional identity (33).
To our knowledge, there is a paucity of research investigating the Chinese SRTP trainees’ professional identity nationwide. Despite recognizing the significant impact of psychosocial factors on the formation of professional identity, the specific relationship between them still remains unclear among Chinese SRTP trainees. Therefore, we conducted a cross-sectional survey among this vulnerable population. The aims of this study are: firstly, to provide an overview of the current status of professional identity among Chinese SRTP trainees; secondly, to investigate the relationship between professional identity and psychosocial factors, particularly work-related and individual psychological variables. We anticipate that this knowledge will make a valuable contribution towards enhancing the efficacy of professional identity formation programs and interventions for SRTP trainees. This, in turn, will foster their personal growth, facilitate a smooth transition into the medical profession, and ultimately strengthen the available medical human resources in China.
Methods
Study design
We conducted a cross-sectional survey in China mainland from 9 March to 20 March in 2023. Participants in this survey were SRTP trainees in China mainland. The study protocol was approved by the Tongji Hospital of Tongji University Ethics Committee (Registration Number K-W-2023-002).
Convenience sampling was used to collect data. The questionnaire was created at an online survey system.1 The link of questionnaire was disseminated to SRTP trainees through managers of SRTP from different provinces and municipalities in China via WeChat group (a widely used social media). After receiving the link, SRTP managers forwarded it to SRTP trainees in their units. All respondents were required to read the participant information sheet and sign an consent form before commencing the questionnaire. In total, 2,364 respondents completed the questionnaire. Those who spent less than 3 min filling the questionnaire were excluded. Finally, 2,267 respondents were enrolled into the analyses, with a validity rate of 95.9%.
Sample size was calculated based on a previous study using the same instrument to measure professional identity of general practitioners (GPs) in China with the average score and standard deviation being 51.23 and 7.06, respectively (34). To set an allowable error of 0.5 and a significance level (α) of 0.05, the minimum sample size of 766 was required. The actual sample size was nearly twice more than the required one, thus, it is sufficient for analysis.
Data collection and quality control
The questionnaire was designed based on literature review and group discussion. The first section collected socio-demographic information. The second section consisted of work-related questions. The third section contained some individual psychological measurement. To improve the quality of questionnaire, a pilot study was conducted by asking 20 SRTP trainees from a particular hospital to complete questionnaires. Based on their feedback, we made adjustments to the questionnaire and implemented a minimum answering time of 3 min as an exclusive criterion. In the process of filling out the questionnaire, all questions were mandatory and participants could terminate at any time. Once all data were collected, two specialized investigators extracted the data from the website database to ensure accuracy.
Questionnaire measurement
Professional identity
The professional identity scale was used to assess SRTP trainees’ professional identity (35). It is derived from the Japanese Nurse’s Career Identity Scale (NCIS), which was developed by researchers at the University of Tokyo and widely used in Japan (36, 37). It consisted of 21 items across seven dimensions: “Sense of Grasp,” “Sense of Consistency,” “Sense of Meaning,” “Self-Efficacy,” “Self-Determination,” “Organizational Influence” and “Patient Influence.” The Cronbach’s α for the total scale and each sub-scale ranges from 0.765 to 0.862. In 2010, Zhao et al. translated and validated the scale for measurement of professional identity of nurses in China (38). Subsequently, Wu further simplified and revised the scale to a 13-item version, making it suitable for both Chinese nurses and physicians in 2012 (35). For instance, the item “Nursing work suits me” was adjusted to “Healthcare work suits me.” The Cronbach’s α for this revised scale was 0.910. In this study, we utilized the 13-item professional identity scale by Wu, with each item rated on a 5-point Likert scale ranging from 1 (very disagree) to 5 (very agree) (35). The total scores range from 13 to 65 and a higher score indicates a stronger sense of professional identity. For the present sample, the Cronbach’s α coefficients and KMO value of this scale were 0.904 and 0.914. Bartlett’s test of sphericity was significant (χ2 (78) = 15, 568.674, p < 0.001). Contents of the scale are presented in Supplementary Table S1.
Influential factors
Demographic characteristics
Demographics included age (continuous variable, years), gender (male or female), marital status (unmarried/divorced or married/cohabitation), region of work (eastern China, central China or western China), highest education level before SRTP (Bachelor’s degree, Master’s degree or Doctoral degree).
Work-related variables
Work-related variables included work experience before SRTP (yes or no), years in SRTP (1st, 2nd, or 3rd year), weekly working hours (≥48 h or <48 h), satisfaction with annual income (unsatisfied, neutral, or satisfied) and occupational pressure (low, intermediate or high).
Individual psychological variables
Psychological distress was screened by the Patient Health Questionnaire-4 (PHQ-4) which included two subscales: PHQ-2 for depression and GAD-2 for anxiety (39). Each contained two items to assess the frequency (from 0 = not at all to 3 = nearly every day) of depressive or anxious symptoms in the last two weeks. Possible total score of PHQ-4 varied from 0 to 12, with higher scores representing more psychological distress. The Cronbach’s α coefficient for PHQ-4 was 0.925.
Burnout was measured using the 2-item version of the Maslach Burnout Inventory (MBI-2), whose items were “I feel burned out from my work” (EE, emotional exhaustion) and “I’ve become more callous toward people since I took this job” (DP, depersonalization). Each item was rated with a 7-point Likert scale ranging from 0 (never) to 6 (every day), with higher scores reflecting greater EE or DP. EE and DP were evaluated separately throughout analyses. West et al. developed this scale and demonstrated its effectiveness in screening the burnout among medical professionals (40).
Resilience was measured by the Connor Davidson Resilience Scale (CD-RISC-2) (41). The CD-RISC-2 included “able to adapt to change” and “tend to bounce back after illness or hardship.” And they were assessed on a 5-point Likert scale ranging from 0 (not true at all) to 4 (true nearly all the time). Total score ranged from 0 to 8, higher suggesting more resilient. In the present study, the Cronbach’s α was 0.806.
Statistical analysis
Descriptive statistics were calculated. Two independent sample t-test or one-way ANOVA were used to test the statistical differences in professional identity scores across different subgroups. Pearson’s correlation was used to assess the degree of correlation between age, resilience, psychological distress, burnout (depersonalization and emotion exhaustion) and professional identity scores. Hierarchical multiple linear regression was conducted to examine the associations between selected variables and professional identity. In the first and second blocks, socio-demographics and work-related variables were entered, respectively. In the subsequent three blocks, individual psychological variables including psychological distress, burnout (depersonalization and emotion exhaustion) and resilience were entered in the model subsequently. P values less than 0.05 were considered statistically significant. SPSS version 25.0 (IBM Corporation, Armonk, NY, United States) was used for analysis.
Results
Tables 1, 2 presents the characteristics of respondents. A final sample of 2, 267 respondents were enrolled. 1, 241 (54.74%) were female, and the average age was 26.68 ± 2.97. 23.51, 48.39, and 28.10% worked in western, central and eastern China and the majority (79.44%) were unmarried. More than nine tenths (91.13%) of respondents had a bachelor’s degree, and 52.67% had work experience before SRTP. The proportion of SRTP trainees at the 1st, 2nd and 3rd year were 34.58, 31.36 and 34.06%. Few (10.63%) were satisfied with their annual income. Approximately half (51.35%) worked more than 48 h a week, and over three quarters (75.25%) reported high occupational pressure. The average score for respondents’ professional identity scale was 47.68 (SD = 8.61). The respondents gave a rating score of 4.41 ± 3.34, 2.42 ± 1.95, 2.68 ± 1.96, and 4.72 ± 1.61 for psychological distress, depersonalization, emotion exhaustion and resilience, respectively.
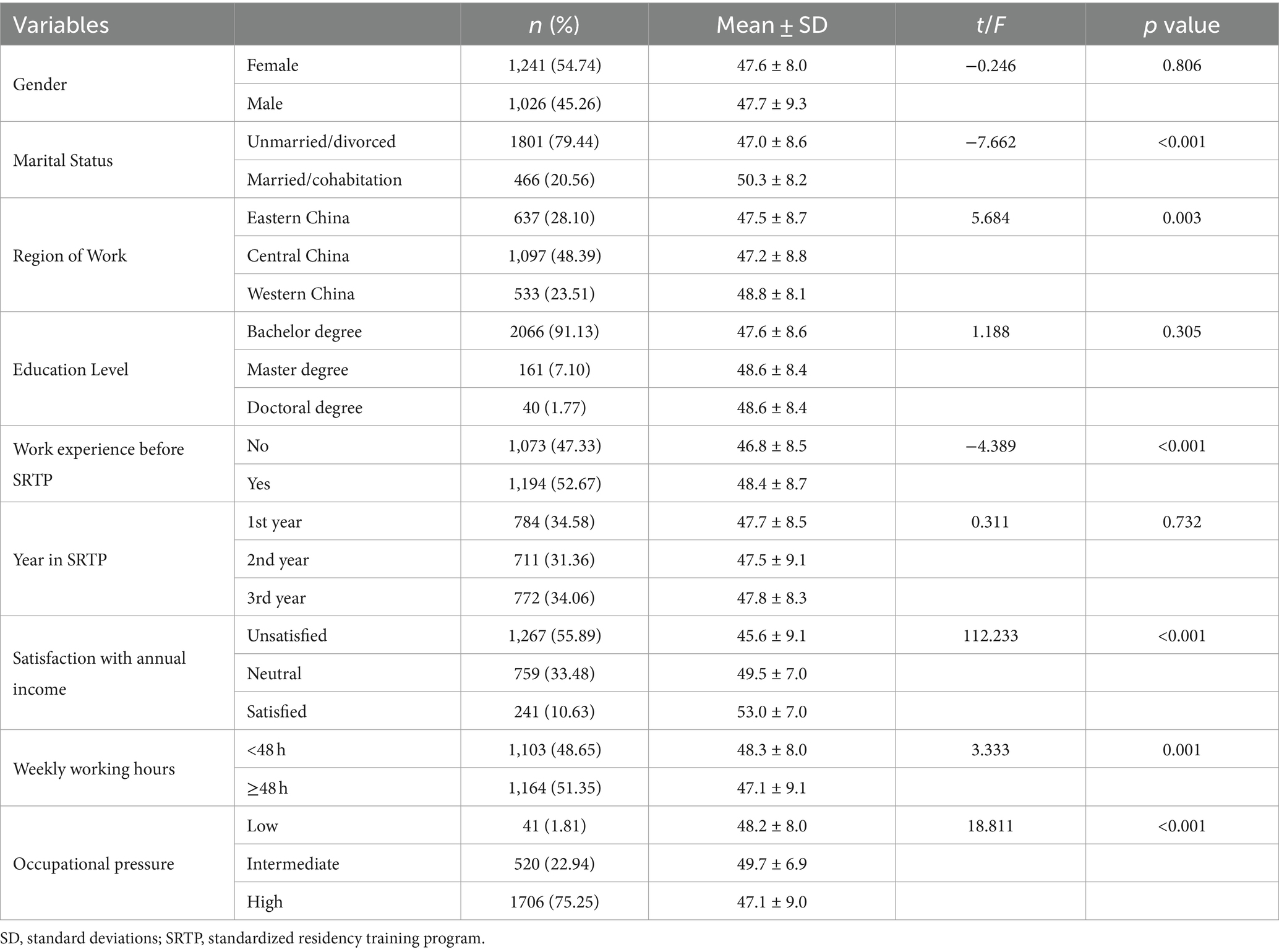
Table 1. Descriptive statistics for categorical variables and associations with professional identity.
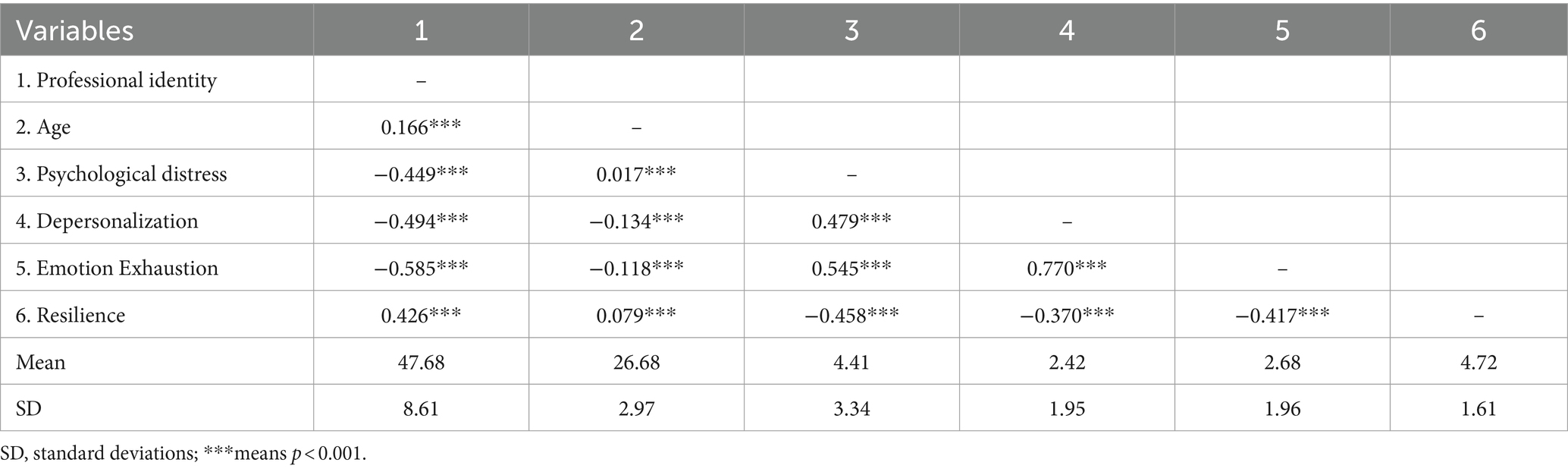
Table 2. Correlation coefficients of continuous variables and professional identity.
The differences in mean scores of professional identity among subgroups are presented in Table 1. There were significant differences in SRTP trainees’ professional identity across marital status, region of work, work experience before SRTP, satisfaction with annual income, weekly working hours and occupational pressure. Specifically, Those who were married/cohabitation (t = −7.662, p < 0.001), worked in western China (F = 5.684, p = 0.003), had work experience before SRTP (t = −4.389, p < 0.001), were more satisfied with annual income (F = 112.233, p < 0.001), worked less than 48 h per week (t = 3.333, p = 0.001) and had more occupational pressure (F = 18.811, p < 0.001) reported a stronger sense of professional identity. However, no significant differences were detected in professional identity of SRTP trainees by gender, education and year in SRTP (all Ps >0.05). In Table 2, professional identity was significantly associated with age, psychological distress, depersonalization, emotion exhaustion and resilience (r = 0.166, −0.449, −0.494, −0.585 and 0.426, all Ps < 0.001).
Table 3 demonstrates the results of the hierarchical multiple linear regression analysis. Marital status, work experience before SRTP, satisfaction with annual income, occupational pressure, psychological distress, depersonalization, emotion exhaustion and resilience were significantly associated with professional identity in the final model with an adjusted R2 value of 0.411. Specifically, being married (β = 0.066, p < 0.01), having work experience before SRTP (β = 0.036, p < 0.05), being satisfied with annual income (β = 0.062, p < 0.01), and higher level of resilience (β = 0.169, p < 0.001) were associated with a stronger sense of professional identity. Conversely, higher level of psychological distress (β = −0.144, p < 0.001), depersonalization (β = −0.053, p < 0.05) and emotion exhaustion (β = −0.380, p < 0.001) were associated with a weaker sense of professional identity (F = 114.301, p < 0.001). Notably, compared with intermediate occupational pressure, low occupational pressure was associated with lower scores of professional identity (β = −0.031, p < 0.05) and high occupational pressure was associated with higher scores (β = 0.047, p < 0.05). There was no significant multicollinearity among the variables within the model, as all of the variance inflation factors (VIF) were less than 3. Socio-demographics, work-related variables and individual psychological variables explained 3.5, 9.0, and 28.6% of the variance in professional identity, respectively. Among individual psychological variables, psychological distress, burnout and resilience explained 13.7, 12.9 and 2.0% of the variance in professional identity, respectively.
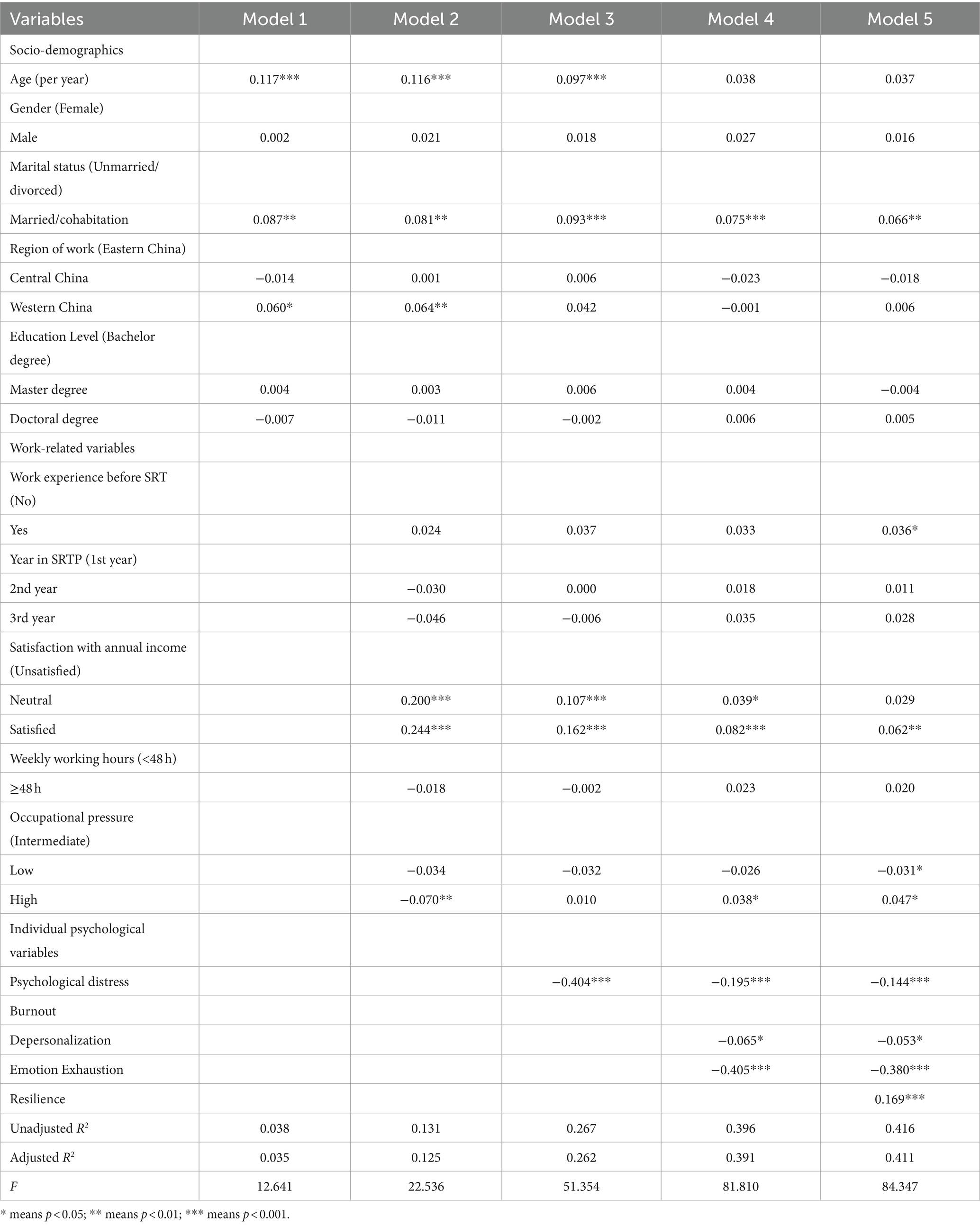
Table 3. Hierarchical multiple linear regression of professional identity.
Discussion
In this study, the average mean score of professional identity among Chinese SRTP trainees was 47.68 (SD = 8.61). When comparing our results to previous studies conducted on Chinese general practitioners (34), public hospital healthcare workers (35), and blood transfusion physicians (42) using the same measurement, we observe a relatively lower mean score of professional identity among SRTP trainees. Possible explanations for the disparities could be the insufficient experience and role ambiguity. First, SRTP trainees are at the early stages of their medical careers, still navigating the transition from medical school to clinical practice. Lack of experience may impact their confidence in professional roles, as they have less exposure to complex medical scenarios compared to the senior physicians (43). Second, as SRTP involves rotations across various medical settings, trainees may still be in the process of exploring different specialties and determining specific professional goals (44). This lack of role clarity could contribute to a lower level of professional identity (45).
According to the social-cognitive approach by Berzonsky, professional identity is influenced by cognitive processes such as reflection, evaluation and regulation in identity construction, and associated with some social relationships and environments (11). Consistent with this theory, findings are that professional identity is significantly associated with social factors including marriage, work experience, annual income, occupational pressure, and psychological factors including psychological distress, depersonalization, emotional exhaustion and resilience, all of which may affect cognitive process.
Being married, having working experience before SRTP, being satisfied with income were positive associated factors of SRTP trainees’ professional identity. Firstly, marriage may provide them with a sense of stability, emotional support and belonging, which in turn motivates them to work diligently and enhances their professional identity (46). Secondly, trainees with previous working experience were likely to possess a better understanding of their chosen career path, have enhanced professional skills, and thus exhibit a stronger professional identity (43). Thirdly, satisfaction with income was found to have a positive influence on professional identity. But it was noticeable that 55.89% of SRTP trainees in our study were unsatisfied with their annual income, consistent with the findings of our earlier investigation among SRTP trainees in Shanghai (47). In fact, SRTP trainees in China undertook significant workload within the hospital setting, yet they continued to face financial constraints (48). The discrepancy between demanding responsibilities and low income can have negative implications for their professional identity (49). Therefore, supporting trainees with adequate financial security enables them to dedicate themselves fully to their professional roles and pursue their aspirations.
Notably, in the univariable analysis, SRTP trainees with “intermediate occupational pressure” had the highest professional identity score. However, in the multivariable analysis, the score of “intermediate occupational pressure” was higher than that of “low occupational pressure,” lower than that of “high occupational pressure.” These results both indicated that moderate work stress might benefit the formation and development of professional identity. A plausible explanation could be that resident physicians who set higher self-expectations in their work and exhibit greater work engagement may have higher stress level, which will meantime promote professional identity formation (34). But the inconsistency between univariable and multivariable analyses may be due to interaction effects between influencing factors. Future research is needed to delve into the interactions between occupational pressure, individual psychological factors and professional identity. Besides, since we assessed occupational pressure using subjective self-assessment through a three-category stress rating rather than utilizing validated and standardized scales specifically designed to measure stress, this finding should be interpreted with caution.
Psychological distress was significantly negatively associated with professional identity among Chinese SRTP trainees, in accordance with the findings reported by Adisaputri et al. (50). A reason for this might be that SRTP trainees with more psychological distress may harbor more negative self-evaluations such as feeling inadequate or incompetent. These negative self-perceptions can hinder the development and maintenance of their professional identity (51). Another possible interpretation is that higher levels of psychological distress often coincide with reduced work enthusiasm and engagement (52). SRTP trainees with depression and anxiety may struggle to sustain their passion for work and become disengaged from their professional roles, ultimately resulting in a weakened sense of professional identity (51). Furthermore, compromised mental health among SRTP trainees can lead to adverse medical outcomes, such as medical errors or lower-quality care (53). As professional identity is closely intertwined with the delivery of high-quality care and feelings of fulfillment in their role as caregivers, psychological distress could exert a detrimental impact on professional identity (54). In light of this, psychological support for trainees can be enhanced by offering peer support programs that foster a sense of belonging and one-on-one counseling sessions that provide personalized assistance (55).
As crucial components of the burnout syndrome, higher levels of emotional exhaustion or depersonalization was significantly associated with lower levels of professional identity among SRTP trainees. This has been evidenced among Portugal healthcare workers (56), Chinese emergency physicians (57) and primary health workers (58). Several plausible explanations can account for these results. Firstly, emotional exhaustion induces fatigue and diminish emotional engagement, making it more challenging for trainees to experience fulfillment and satisfaction in their professional roles, which are crucial components of professional identity (59). Moreover, trainees with elevated emotional exhaustion may have less empathy and compassion towards patients and become disillusioned with their profession (60). This may prompt them to question their career choices and contemplate alternative paths, potentially leading to a weakened sense of professional identity and even increasing the likelihood of turnover (8). When depersonalization occurs, where SRTP trainees display cynicism or treat patients as objects rather than individuals with unique needs, it creates a barrier to effective communication and trust between doctor and patient. Given that professional identity is closely linked to the ability to establish meaningful connections with patients and deliver patient-centered care, depersonalization serves as an impediment to develop professional identity (61). Balint Group, developed by Michael and Enid Balint in the 1950s, is a highly recommended activity to be held regularly to prevent burnout, process identity information and deal with identity conflicts (62, 63). It provides resident physicians with a safe, confidential and non-judgmental space to fully share their thoughts, confusions and emotions about a particular clinical dilemma, encouraging individuals to explore their professional beliefs, values, and goals, which may not be highlighted in daily clinical practices and regular training curricula (64).
Resilience was found to be a positive association of professional identity, concurring with the former results (65). Resilience can enable physicians to adapt, cope and bounce back from challenges, setbacks, and stressors (66). SRTP trainees may generally encounter various stressors such as limited clinical skills, financial constraints, demanding academic workload, family responsibilities, and fierce job competition (48). Resilience thus helps them to overcome these challenges that lead to identity conflicts. For SRTP educators, they can integrate narrative medicine (NM) into the SRTP medical education. NM is a scientifically validated, effective educational intervention that has been shown to increase physicians’ resilience, empathy, affinity, professionalism (67, 68). It can facilitate professional identity by guiding SRTP trainees in self-exploration, fostering critical thinking, promoting reflective learning and increasing understanding of patients (69). However, it is rarely applied among Chinese SRTP trainees.
To our knowledge, this study represents one of the earliest investigations into the status of professional identity and its associated factors among Chinese SRTP trainees. Additionally, the study offers insights into the psychosocial factors that may impact the professional identity of SRTP trainees, thereby providing evidence to support the implementation of tailored interventions for cultivating their professional identity. However, this study has several limitations. Firstly, being a cross-sectional study, it is limited in establishing causal relationships between variables. Secondly, the online data collection through self-filled questionnaires may introduce response biases, as participants who were more enthusiastic and optimistic about their work might be more likely to complete the questionnaire. Thirdly, validated and standardized scales of occupational pressure should be used to explore its relationship with professional identity and the potential interactions with other psychological factors. Future research should consider implementing a longitudinal design to examine the dynamic nature of professional identity over time and explore the temporal relationship between psychosocial factors and professional identity among SRTP trainees.
Conclusion
This study indicates that individual psychological factors, namely psychological distress, burnout and resilience may have a substantial influence on professional identity, explaining 28.9% of the variance. Specifically, higher levels of psychological distress and burnout are associated with weaker senses of professional identity. Instead, more resilience may promote professional identity. It is imperative for managers and educators to develop tailored interventions and measures to help SRTP trainees reduce psychological distress, alleviate burnout and enhance resilience, which will help promote professional identity and thereby reduce the turnover rates and strengthen the available medical human resources in China.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Tongji Hospital of Tongji University Institutional Review Board. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
ZZ: Data curation, Investigation, Methodology, Writing – original draft, Writing – review & editing. ZL: Investigation, Supervision, Writing – original draft, Writing – review & editing. XZ: Conceptualization, Data curation, Formal analysis, Methodology, Writing – original draft. YG: Writing – review & editing. JJ: Data curation, Formal analysis, Investigation, Writing – original draft. YC: Funding acquisition, Investigation, Supervision, Writing – review & editing. LH: Funding acquisition, Investigation, Methodology, Project administration, Resources, Supervision, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This work was supported by grants from Shanghai Pujiang Program (2020PJC097), Key Projects of the Ministry of Education in 2019 under “The 13th Five-Year Plan” for National Educational Science (DIA190409), Shanghai Yangpu District Medical Key Discipline Community Mental Health Prevention and Treatment (22YPZB11).
Acknowledgments
The authors gratefully thank all the resident physicians who generously shared their time to participate in this study.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2024.1413126/full#supplementary-material
Footnotes
References
1. Kirch, DG, and Petelle, K. Addressing the physician shortage: the peril of ignoring demography. JAMA. (2017) 317:1947–8. doi: 10.1001/jama.2017.2714
2. Wu, Q, Zhao, L, and Ye, XC. Shortage of healthcare professionals in China. BMJ. (2016) 354:i4860. doi: 10.1136/bmj.i4860
3. Lien, SS, Kosik, RO, Fan, AP, Huang, L, Zhao, X, Chang, X, et al. 10-year trends in the production and attrition of Chinese medical graduates: an analysis of nationwide data. Lancet. (2016) 388:S11. doi: 10.1016/S0140-6736(16)31938-9
4. Rimmer, A . Physician shortage worsened by cuts in job ads and lack of trainees, colleges warn. BMJ. (2019) 367:l6011. doi: 10.1136/bmj.l6011
5. National Health Commission . Accessed 25 August 2022. Available at: health.people.com.cn/n1/2022/0825/c14739-32511370.html.
6. Hou, H, Pei, Y, Yang, Y, Lu, L, Yan, W, Gao, X, et al. Factors associated with turnover intention among healthcare workers during the coronavirus disease 2019 (COVID-19) pandemic in China. Risk Manag Healthc Policy. (2021) 14:4953–65. doi: 10.2147/RMHP.S318106
7. Yan, S, Shen, X, Wang, R, Luo, Z, Han, X, Gan, Y, et al. The prevalence of turnover intention and influencing factors among emergency physicians: a national observation. Hum Resour Health. (2021) 19:149. doi: 10.1186/s12960-021-00688-8
8. Sun, X, Zhang, M, Lu, Z, Zhang, Z, Zheng, JC, Cheng, L, et al. Turnover intention and related factors among resident physicians in China under the standardised residency training programme: a cross-sectional survey. BMJ Open. (2022) 12:e061922. doi: 10.1136/bmjopen-2022-061922
9. Feng, J, Sang, W, Lei, Z, Qu, G, Li, X, Ferrier, A, et al. The impact of burnout on turnover intention among Chinese general practitioners: the mediating effect of job satisfaction and the moderating effect of professional identity. Int J Soc Psychiatry. (2023) 69:705–13. doi: 10.1177/00207640221133939
10. Yang, X, Gao, L, Zhang, S, Zhang, L, Zhang, L, Zhou, S, et al. The professional identity and career attitude of Chinese medical students during the COVID-19 pandemic: a cross-sectional survey in China. Front Psych. (2022) 13:774467. doi: 10.3389/fpsyt.2022.774467
11. Berzonsky, M . A social-cognitive perspective on identity construction In: S Schwartz, K Luyckx, and VL Vignoles, editors. Handbook of identity theory and research, vol. 1, 2: Springer (2011). 55–76.
12. Sawatsky, AP, and Monrouxe, LV. When I say … identity. Med Educ. (2023) 57:303–4. doi: 10.1111/medu.15027
13. Liao, KC, Ajjawi, R, Peng, CH, Jenq, CC, and Monrouxe, LV. Striving to thrive or striving to survive: professional identity constructions of medical trainees in clinical assessment activities. Med Educ. (2023) 57:1102–16. doi: 10.1111/medu.15152
14. Cruess, RL, Cruess, SR, Boudreau, JD, Snell, L, and Steinert, Y. Reframing medical education to support professional identity formation. Acad Med. (2014) 89:1446–51. doi: 10.1097/ACM.0000000000000427
15. Chandran, L, Iuli, RJ, Strano-Paul, L, and Post, SG. Developing “a way of being”: deliberate approaches to professional identity formation in medical education. Acad Psychiatry. (2019) 43:521–7. doi: 10.1007/s40596-019-01048-4
16. Zhang, T, Feng, J, Jiang, H, Shen, X, Pu, B, and Gan, Y. Association of professional identity, job satisfaction and burnout with turnover intention among general practitioners in China: evidence from a national survey. BMC Health Serv Res. (2021) 21:382. doi: 10.1186/s12913-021-06322-6
17. Cullum, RJ, Shaughnessy, A, Mayat, NY, and Brown, ME. Identity in lockdown: supporting primary care professional identity development in the COVID-19 generation. Educ Prim Care. (2020) 31:200–4. doi: 10.1080/14739879.2020.1779616
18. Zhu, J, Li, W, and Chen, L. Doctors in China: improving quality through modernisation of residency education. Lancet. (2016) 388:1922–9. doi: 10.1016/S0140-6736(16)00582-1
19. Gordon, L, Jindal-Snape, D, Morrison, J, Muldoon, J, Needham, G, Siebert, S, et al. Multiple and multidimensional transitions from trainee to trained doctor: a qualitative longitudinal study in the UK. BMJ Open. (2017) 7:e018583. doi: 10.1136/bmjopen-2017-018583
20. Littlewood, S, Ypinazar, V, Margolis, SA, Scherpbier, A, Spencer, J, and Dornan, T. Early practical experience and the social responsiveness of clinical education: systematic review. BMJ. (2005) 331:387–91. doi: 10.1136/bmj.331.7513.387
21. Chen, L, and Hubinette, MM. Exploring the role of classroom-based learning in professional identity formation of family practice residents using the experiences, trajectories, and reifications framework. Med Teach. (2017) 39:876–82. doi: 10.1080/0142159X.2017.1317729
22. Holden, M, Buck, E, Clark, M, Szauter, K, and Trumble, J. Professional identity formation in medical education: the convergence of multiple domains. HEC Forum. (2012) 24:245–55. doi: 10.1007/s10730-012-9197-6
23. Mao, A, Lu, SE, Lin, Y, and He, M. A scoping review on the influencing factors and development process of professional identity among nursing students and nurses. J Prof Nurs. (2021) 37:391–8. doi: 10.1016/j.profnurs.2020.04.018
24. Frost, HD, and Regehr, G. "I am a doctor": negotiating the discourses of standardization and diversity in professional identity construction. Acad Med. (2013) 88:1570–7. doi: 10.1097/ACM.0b013e3182a34b05
25. Matsui, T, Sato, M, Kato, Y, and Nishigori, H. Professional identity formation of female doctors in Japan-gap between the married and unmarried. BMC Med Educ. (2019) 19:55. doi: 10.1186/s12909-019-1479-0
26. Monrouxe, LV, Bullock, A, Tseng, HM, and Wells, SE. Association of professional identity, gender, team understanding, anxiety and workplace learning alignment with burnout in junior doctors: a longitudinal cohort study. BMJ Open. (2017) 7:e017942. doi: 10.1136/bmjopen-2017-017942
27. Mikkola, L, Suutala, E, and Parviainen, H. Social support in the workplace for physicians in specialization training. Med Educ Online. (2018) 23:1435114. doi: 10.1080/10872981.2018.1435114
28. Tang, L, and Guan, M. Rise of health consumerism in China and its effects on Physicians' professional identity and the physician-patient relationship and communication. Health Commun. (2018) 33:636–42. doi: 10.1080/10410236.2017.1290015
29. Wang, G, Shi, X, Ma, D, Li, C, and Yin, A. Relationship between professional identity and social support among general practitioners in Shandong province. China J Publ Health. (2016) 32:818–20. doi: 10.11847/zgggws2016-32-06-25
30. Passi, V, and Johnson, N. The impact of positive doctor role modeling. Med Teach. (2016) 38:1139–45. doi: 10.3109/0142159X.2016.1170780
31. Mata, DA, Ramos, MA, Bansal, N, Khan, R, Guille, C, Di Angelantonio, E, et al. Prevalence of depression and depressive symptoms among resident physicians: a systematic review and Meta-analysis. JAMA. (2015) 314:2373–83. doi: 10.1001/jama.2015.15845
32. Yousef, S, Athamneh, M, Masuadi, E, Ahmad, H, Loney, T, Moselhy, HF, et al. Association between depression and factors affecting career choice among Jordanian nursing students. Front Public Health. (2017) 5:311. doi: 10.3389/fpubh.2017.00311
33. Wald, HS . Professional identity (trans)formation in medical education: reflection, relationship, resilience. Acad Med. (2015) 90:701–6. doi: 10.1097/ACM.0000000000000731
34. Li, L, Gan, Y, Yang, Y, Jiang, H, Lu, K, Zhou, X, et al. Analysis on professional identity and related factors among Chinese general practitioners: a National Cross-sectional Study. BMC Fam Pract. (2020) 21:80. doi: 10.1186/s12875-020-01155-4
35. Wu, H . Public hospital medical workers' professional identity research Southwestern University of Finance and Economics (2012).
36. Takemura, Y . The measurements of career identity of nurses and unlicensed assistants at long-term care units. Iryo to Syakai. (2005) 14:83–98. doi: 10.4091/iken.14.4_83
37. Yamagishi, M, Kobayashi, T, and Nakamura, Y. Effects of web-based career identity training for stress management among Japanese nurses: a randomized control trial. J Occup Health. (2008) 50:191–3. doi: 10.1539/joh.l7086
38. Zhao, H, Lu, T, Zhang, C, Deng, F, Zheng, J, and Da, X. Testing for reliability and validity of Chinese version of the Nurse's career identity scale. Chin Nurs Manag. (2010) 10:49–51. doi: 10.3969/j.issn.1672-1756.2010.11.018
39. Löwe, B, Wahl, I, Rose, M, Spitzer, C, Glaesmer, H, Wingenfeld, K, et al. A 4-item measure of depression and anxiety: validation and standardization of the patient health Questionnaire-4 (PHQ-4) in the general population. J Affect Disord. (2010) 122:86–95. doi: 10.1016/j.jad.2009.06.019
40. West, CP, Dyrbye, LN, Sloan, JA, and Shanafelt, TD. Single item measures of emotional exhaustion and depersonalization are useful for assessing burnout in medical professionals. J Gen Intern Med. (2009) 24:1318–21. doi: 10.1007/s11606-009-1129-z
41. Vaishnavi, S, Connor, K, and Davidson, JR. An abbreviated version of the Connor-Davidson resilience scale (CD-RISC), the CD-RISC2: psychometric properties and applications in psychopharmacological trials. Psychiatry Res. (2007) 152:293–7. doi: 10.1016/j.psychres.2007.01.006
42. Shi, Y, Zhang, T, and Du, C. A survey on professional identity and job satisfaction of blood transfusion physicians and its influencing factors in Tianjin. Chinese J Blood Transf. (2022) 35:667–71. doi: 10.13303/j.cjbt.issn.1004-549x.2022.06.020
43. Bloom, TJ, Smith, JD, and Rich, W. Impact of pre-pharmacy work experience on development of professional identity in student pharmacists. Am J Pharm Educ. (2017) 81:6141. doi: 10.5688/ajpe6141
44. Yu, C, and Zong, Z. Professional Socialization in Transition:Margins and Conflicts in the Professional Interactions of Residency Training. Soc Stud. (2023) 38:45–67.
45. O’Rourke, MW . A situation-specific theory about professional role identity formation as related to role clarity and nurse work engagement. Situation Specific Theories: Development, Utilization, and Evaluation in Nursing (2021): 211–230
46. Bai, J, He, L, Huang, L, Liu, X, and Pu, C. Analysis of the status of family Doctors' professional identity in Chongqing and its influencing factors. Chin Health Serv Manag. (2022) 39:396–400.
47. Huang, L, Caspari, JH, Sun, X, Thai, J, Li, Y, Chen, FZ, et al. Risk and protective factors for burnout among physicians from standardized residency training programs in Shanghai: a cross-sectional study. BMC Health Serv Res. (2020) 20:965. doi: 10.1186/s12913-020-05816-z
48. Levey, RE . Sources of stress for residents and recommendations for programs to assist them. Acad Med. (2001) 76:142–50. doi: 10.1097/00001888-200102000-00010
49. Siegrist, J, Starke, D, Chandola, T, Godin, I, Marmot, M, Niedhammer, I, et al. The measurement of effort-reward imbalance at work: European comparisons. Soc Sci Med. (2004) 58:1483–99. doi: 10.1016/S0277-9536(03)00351-4
50. Adisaputri, G, and Ungar, M. Shifting professional identity among Indonesian medical practitioners during the COVID-19 pandemic. Qual Health Res. (2023) 33:400–11. doi: 10.1177/10497323231159614
51. Chang, YC, Xiao, X, Nkambule, N, Ngerng, R, Bullock, A, and Monrouxe, LV. Exploring emergency physicians' professional identities: a Q-method study. Adv Health Sci Educ Theory Pract. (2021) 26:117–38. doi: 10.1007/s10459-020-09973-y
52. Jiang, M, Shao, X, Rao, S, Ling, Y, Pi, Z, Shao, Y, et al. Emotional state of Chinese healthcare workers during COVID-19 pandemic. Front Psychol. (2022) 13:854815. doi: 10.3389/fpsyg.2022.854815
53. Crijns, TJ, Kortlever, J, Guitton, TG, Ring, D, and Barron, GC. Symptoms of burnout among surgeons are correlated with a higher incidence of perceived medical errors. HSS J. (2020) 16:305–10. doi: 10.1007/s11420-019-09727-6
54. Fitzgerald, A . Professional identity: a concept analysis. Nurs Forum. (2020) 55:447–72. doi: 10.1111/nuf.12450
55. Talisman, N, Harazduk, N, Rush, C, Graves, K, and Haramati, A. The impact of mind-body medicine facilitation on affirming and enhancing professional identity in health care professions faculty. Acad Med. (2015) 90:780–4. doi: 10.1097/ACM.0000000000000720
56. Correia, I, and Almeida, AE. Organizational justice, professional identification, empathy, and meaningful work during COVID-19 pandemic: are they burnout protectors in physicians and nurses. Front Psychol. (2020) 11:566139. doi: 10.3389/fpsyg.2020.566139
57. Feng, X, Wang, Y, Jia, P, Wang, Y, Guan, Z, and Meng, K. Associations between professional identity and turnover intent in prehospital emergency physicians: the mediating effect of burnout. Front Public Health. (2022) 10:1034925. doi: 10.3389/fpubh.2022.1034925
58. Yang, D, Fang, G, Fu, D, Hong, M, Wang, H, Chen, Y, et al. Impact of work-family support on job burnout among primary health workers and the mediating role of career identity: a cross-sectional study. Front Public Health. (2023) 11:1115792. doi: 10.3389/fpubh.2023.1115792
59. Liu, H, Zou, HY, Wang, HJ, Xu, X, and Liao, JQ. Do emotional labour strategies influence emotional exhaustion and professional identity or vice versa? Evidence from new nurses. J Adv Nurs. (2020) 76:577–87. doi: 10.1111/jan.14266
60. Wu, LX, Qi, L, and Li, Y. Challenges faced by young Chinese doctors. Lancet. (2016) 387:1617. doi: 10.1016/S0140-6736(16)30202-1
61. Kline, CC, Park, SE, Godolphin, WJ, and Towle, A. Professional identity formation: a role for patients as mentors. Acad Med. (2020) 95:1578–86. doi: 10.1097/ACM.0000000000003561
62. Balint, M . The doctor, his patient, and the illness. Lancet. (1955) 265:683–8. doi: 10.1016/s0140-6736(55)91061-8
63. Huang, L, Harsh, J, Cui, H, Wu, J, Thai, J, Zhang, X, et al. A randomized controlled trial of Balint groups to prevent burnout among residents in China. Front Psych. (2019) 10:957. doi: 10.3389/fpsyt.2019.00957
64. Antoun, J, Khater, B, Itani, H, Naous, J, and Romani, M. Effectiveness of a modified Balint group process on empathy and psychological skills employing Kirkpatrick's evaluation framework. PeerJ. (2023) 11:e15279. doi: 10.7717/peerj.15279
65. Cui, Q, Liu, L, Hao, Z, Li, M, Liu, C, Chenxin, Y, et al. Research on the influencing factors of fatigue and professional identity among CDC workers in China: an online cross-sectional study. BMJ Open. (2022) 12:e058762. doi: 10.1136/bmjopen-2021-058762
66. Connor, KM, and Davidson, JR. Development of a new resilience scale: the Connor-Davidson resilience scale (CD-RISC). Depress Anxiety. (2003) 18:76–82. doi: 10.1002/da.10113
67. Remein, CD, Childs, E, Pasco, JC, Trinquart, L, Flynn, DB, Wingerter, SL, et al. Content and outcomes of narrative medicine programmes: a systematic review of the literature through 2019. BMJ Open. (2020) 10:e031568. doi: 10.1136/bmjopen-2019-031568
68. Florijn, BW . Narrative medicine: thinking with stories during the plague. Am J Med. (2020) 133:1003–4. doi: 10.1016/j.amjmed.2020.02.035
Keywords: China, influential factors, physicians, professional identity, standardized residency training program
Citation: Zeng Z, Lu Z, Zeng X, Gan Y, Jiang J, Chen Y and Huang L (2024) Professional identity and its associated psychosocial factors among physicians from standardized residency training programs in China: a national cross-sectional study. Front. Med. 11:1413126. doi: 10.3389/fmed.2024.1413126
Edited by:
Adam Sawatsky, Mayo Clinic, United StatesReviewed by:
Ana L. S. Da Silva, Swansea University Medical School, United KingdomYaxin Zhu, China Medical University, China
Copyright © 2024 Zeng, Lu, Zeng, Gan, Jiang, Chen and Huang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: You Chen, eWFuZ3B1Y3lAMTYzLmNvbQ==; Lei Huang, aHVhbmdsZWlAdG9uZ2ppLmVkdS5jbg==
†These authors have contributed equally to this work