 François Poumeaud1
François Poumeaud1 Marion Jaffrelot2Carlos Gomez-Roca3
Marion Jaffrelot2Carlos Gomez-Roca3 Iphigénie Korakis3Giulia Leonardi3Marine Joly4
Iphigénie Korakis3Giulia Leonardi3Marine Joly4 Julien Mazières5
Julien Mazières5 Rosine Guimbaud2Nadim Fares2,3
Rosine Guimbaud2Nadim Fares2,3 Emily Alouani2,3*
Emily Alouani2,3*- 1Department of Medical Oncology, Oncopole Claudius Regaud, Toulouse, France
- 2Department of Digestive Oncology, Centre Hospitalier Universitaire de Toulouse, Toulouse, France
- 3Clinical Research Unit, Department of Medical Oncology, Oncopole Claudius Regaud, Toulouse, France
- 4Department of Infectiology, Centre Hospitalier Universitaire de Toulouse, Toulouse, France
- 5Department of Thoracic Oncology, Centre Hospitalier Universitaire de Toulouse, Toulouse, France
Selective rearranged during transfection (RET) tyrosine kinase inhibitor, pralsetinib, demonstrated clinical efficacy and was well tolerated in lung and thyroid cancers with RET gene mutations or fusions in clinical trials. While the latter focused on the risk of pneumonitis, there is a lack of data regarding other types of infectious risks associated with pralsetinib. Herein, we report the case of a 53-year-old patient with a CCDC6-RET fusion neuroendocrine tumor, who achieved a partial response with pralsetinib as the fifth-line therapy. Of particular note, during pralsetinib therapy, the clinical course was complicated by five severe infectious events, namely, two oxygen-requiring pneumonias, two distinct spondylodiscitis, and one pneumocystis. Our study highlights the increased risk of any type of opportunistic infectious event with pralsetinib, but not selpercatinib, which is probably caused by off-target JAK1/2 inhibition.
Introduction
The aberrant activation of rearranged during transfection (RET) proto-oncogene is a critical factor of oncogenesis in diverse solid tumors. Germline RET mutations cause multiple endocrine neoplasia type II, leading to the occurrence of medullary thyroid cancers (MTC) and neuroendocrine tumors such as pheochromocytomas (1). Selective RET tyrosine kinase inhibitors demonstrated striking clinical efficacy in lung and thyroid cancers with RET gene mutations or fusion with an overall response rate as high as 70% among treatment-naive patients (2). This theragnostic impact has led to phase I/II basket trials in patients with RET-altered pan-cancers, where RET inhibitors showed significant clinical efficacy, with objective response rate (ORR) varying from 43.9 to 50% (3, 4). There are currently two inhibitors, namely, pralsetinib (BLU-667 or X581238) and selpercatinib (LOXO 292), that are FDA and EMA approved based on ARROW trials and the LIBRETTO-001, for only RET-altered non-small cell lung cancer (NSCLC) and thyroid cancer (5) and locally advanced or metastatic RET fusion-positive solid tumors, respectively. The advent of tumor molecular boards and shifting treatment paradigms toward biomarker-guided tumor-agnostic approaches for the current cancer management will extend the use of such treatments. Indeed, RET testing is currently used in routine in next-generation sequencing (NGS) panels, which identified 2% of RET alterations in various types of cancer, including digestive, breast, ovarian, and head-and-neck cancers (6). It is therefore important to precisely establish the safety profile of these new emerging treatments. There is mounting clinical evidence of severe lung infections associated with pralsetinib, but there is little evidence of other infectious events. Here, we report the first case of multiple severe infections in one patient treated with pralsetinib for RET-rearranged metastatic pancreatic neuroendocrine tumor and provide a narrative review to discuss available clinical evidence on pralsetinib-related infectious toxicities as compared to selpercatinib.
Case report
Herein, we report the case of a 53-year-old man, followed since early 2020 for a grade III, well-differentiated, pancreatic neuroendocrine tumor with synchronous bone, nodal, liver, and lung metastases. His past medical history mainly includes hereditary polyneuropathy (Charcot–Marie–Tooth disease) without clinical invalidity. The patient successively received standard systemic treatments such as gemcitabine-oxaliplatin, capecitabine-temozolomide, carboplatin-etoposide (VP-16), and sunitinib from January 2020 to June 2022. The objective response rate with previous systemic therapy ranged from partial response to stable disease. Oncologic treatments were discontinued for progressive diseases and there was no arrest due to toxicity. Agnostic tumoral NGS (TSO500 panel) performed after progression under sunitinib treatments identified a CCDC6-RET fusion. The patient was enrolled in a tumor-agnostic platform clinical trial and received pralsetinib at a dose of 400 mg/day from 27th September 2022 as the fifth-line treatment. Notably, this patient had neither experienced any infectious events or complications during his oncologic history before pralsetinib initiation nor presented lymphopenia or neutropenia, which would suggest some types of immunosuppression. The patient had no corticosteroid treatment at pralsetinib initiation.
One month after pralsetinib initiation (5 November 2022), he developed symptomatic Pseudomonas aeruginosa bacteremia (wild-type phenotype) complicated with lung septic embolisms and concomitant grade III cervical spondylodiscitis involving the 5th and 6th cervical vertebrae and para-vertebral C2 to C5 abscess. Pralsetinib was immediately discontinued, and the patient was successfully treated with piperacillin-tazobactam and ciprofloxacin antibiotic therapy for 14 days, followed by ciprofloxacin monotherapy for 4 more weeks. Transthoracic echocardiography (TTE) excluded infective endocarditis. Notably, the computational tomodensitometry (CT) performed to diagnose septic embolisms also reported a tumor partial response (PR), according to RECIST (Figure 1). After 3 weeks of ciprofloxacin monotherapy and resuming without pralsetinib (as of 5th December 2022), the patient was diagnosed with a second infectious episode of grade II pneumonia, for which he received 7 days of amoxicillin-clavulanic acid. After 1 month of pralsetinib discontinuation due to these two infectious events, a full CT-scan re-evaluation was performed, which revealed new secondary lesions with pleural effusion, peritoneal carcinosis, and lytic bone lesions. Pralsetinib was then resumed on 23rd December 2022 at a standard dose of 400 mg per day, with rapid clinical benefits. After 3 weeks of reintroduction (12th January 2023), the patient experienced a third infectious episode with grade III pneumonia requiring hospitalization due to grade II neutropenia. This was successfully treated with 7 days of piperacillin-tazobactam. After 1 week of reintroduction, the patient presented with febrile back pain and a 4/5 motor deficit in the right leg. Magnetic resonance imaging (MRI) identified typical spondylodiscitis involving 1st to 3rd lumbar vertebrae. Considering the recurrent infectious events, an extensive infectious immune workout was performed. The vertebral biopsy identified the presence of P. aeruginosa, and the histology did not show the presence of bone tuberculosis or tumor progression. Repeated blood culture (bacterial and fungal) was performed and remained negative, and transesophageal echocardiography (TEO) was normal. Grade I lymphopenia was identified without concomitant neutropenia. Lymphocyte immunophenotyping did not reveal any imbalance between CD4 and CD8 sub-populations, B lymphopenia, and natural killer (NK) deficiency. However, plasmatic protein electrophoresis identified deep hypogammaglobulinemia with specific IgG deficiency without a decrease in IgA and IgM. Broad-spectrum serology, including human immunodeficiency virus (HIV) and hepatitis B and C, was negative. This fourth infectious episode was considered as a grade III lumbar spondylodiscitis, which required 2-week hospitalization, and was successfully treated with tobramycin and ciprofloxacin for 48 h followed by a high dose of piperacilline-tazobactam (16 g per day) and ciprofloxacin for 2 weeks, as well as monotherapy with ciprofloxacin for another 2 months. Pralsetinib was continued at 300 mg, and the patient experienced a new partial response in May 2023. Later, on 15th June 2023, in the context of persistent lymphopenia and febrile hypoxemia, a thoracic CT scan was performed and showed disseminated, poorly delimitated pulmonary lesions, which were first interpreted as disease progression. However, pulmonary secretion was positive for Pneumocystis jirovecii. The final diagnosis was a symptomatic pneumocystis, which was treated with high-dose trimethoprim/sulfamethoxazole. Pralsetinib was discontinued after the fifth episode. Finally, the patient presented with liver progression on 30 June 2023, and pralsetinib was definitively discontinued (Figure 1). The patient died in the palliative care unit in September 2023, 3 years after diagnosis, including 9 months of oncologic clinical treatment with pralsetinib.
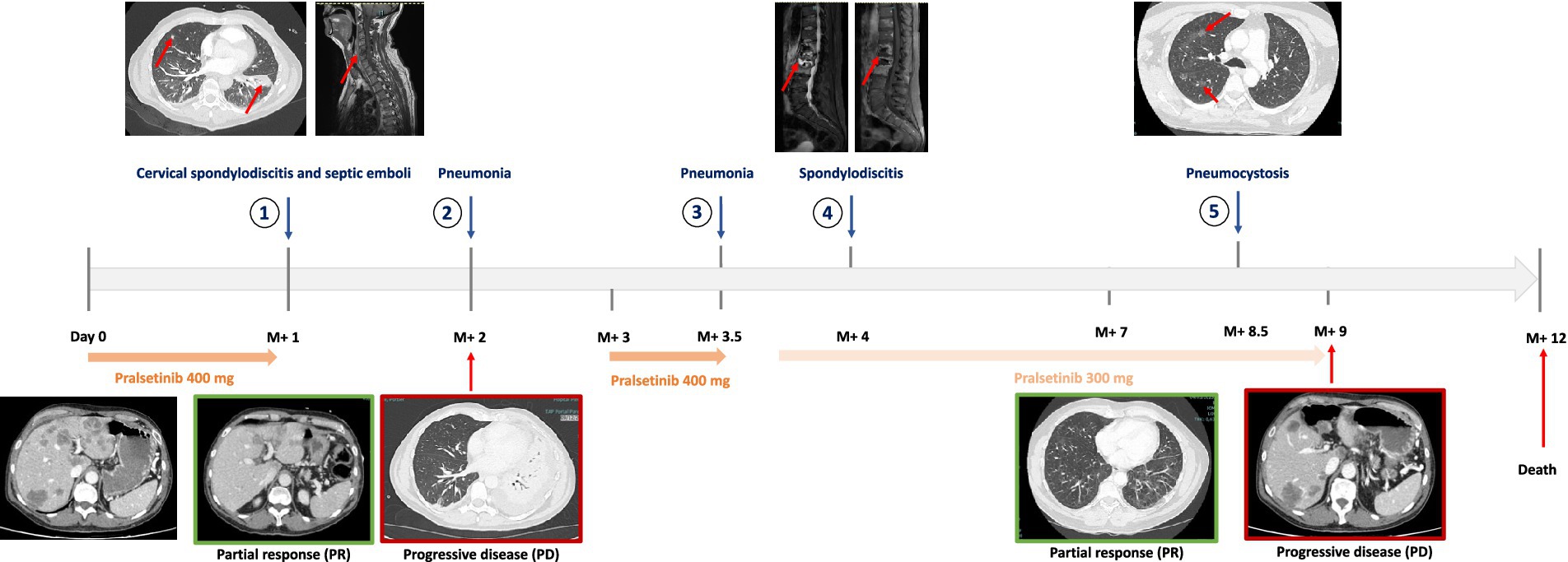
Figure 1. Timeline of infections and therapeutic outcomes. The patient experienced five infectious events under the pralsetinib therapy with oncologic progression during pralsetinib discontinuation. The patient experienced two infectious events at a reduced dose of 300 mg. M+, months since pralsetinib initiation.
Discussion
To the best of our knowledge, we report here the first case of recurrent severe infections characterized by “on/off” episodes under pralsetinib therapy. While clinical trials and most case reports (7–10) focused on the risk of pneumonitis in patients under pralsetinib therapy [grade 3 pneumonia in 3% (2) to 10.7% (11) of patients], our case report and literature review demonstrate the risk of various types of opportunistic infectious events. In some cases, patients treated with pralsetinib presented hematogenous tuberculosis, pulmonary cryptococcosis, one grade V typhlitis, and one grade V sepsis, as shown in Table 1 (7–9, 12, 14). Moreover, it is important to note that these infections can be severe, with 4.1% of fatal events reported by EMA. According to these data, infectious events may be a significant safety issue for patients receiving pralsetinib. Moreover, no risk factor for infection under the pralsetinib therapy has been identified so far.
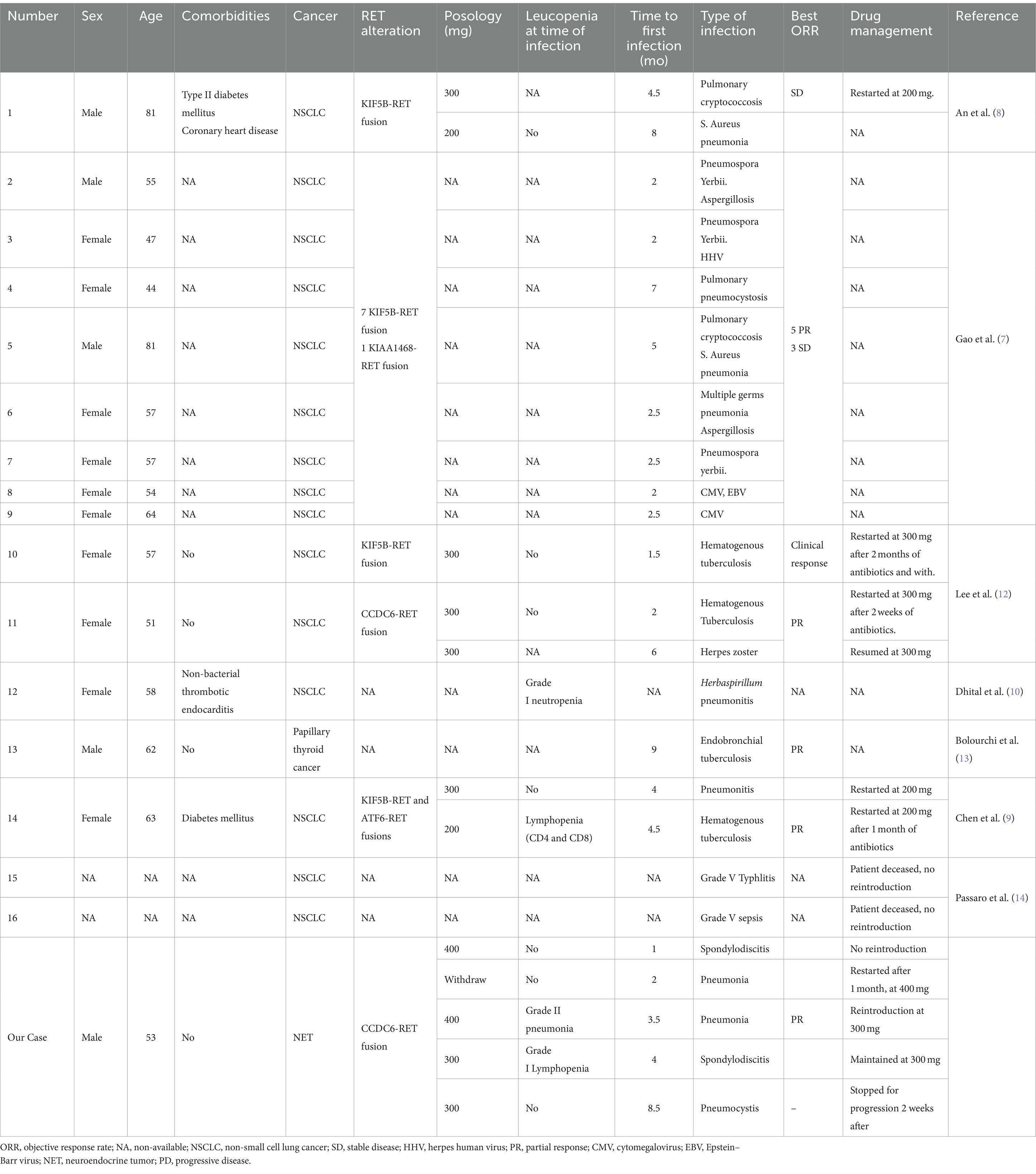
Table 1. Literature review of opportunistic infections reported with pralsetinib.
Another concern is the possible uncertainty between tumor progression and pralsetinib-associated infections. A retrospective study analyzed the occurrence of invasive pulmonary mycosis in patients with NSCLC, and among the 13 patients diagnosed with pulmonary mycosis, 62% of patients were initially misdiagnosed as metastatic or recurrent lung cancer (15). Considering the high incidence of infectious pulmonary events occurring in patients treated with pralsetinib, confusion between pulmonary progression and infectious adverse events might occur, as it was the case for our patient, and must be taken into account.
In the case of our patient, it is also important to note that the continuation of pralsetinib, even at lower doses, is associated with the onset of new infectious events (7, 9, 12).
A rapid clinical and imaging response followed by multisite relapse after the discontinuation of pralsetinib, but with an objective response at reintroduction, confirms the nature of a RET oncologic tumor in our patient. This exposure–response relationship was also observed in patients with RET fusion thyroid cancer treated with pralsetinib, in which patients with the highest plasmatic concentrations had the longest PFS duration, but this benefit was not observed in patients with NSCLC (16). Patients who initiated pralsetinib at 400 mg as opposed to 300 mg or less—both in NSCLC or thyroid cancers—also experienced the longest progression‐free survival (PFS) duration. The same study also reported a significantly increased risk of developing grade III or higher pneumonia and lymphopenia due to increased exposure to pralsetinib (16). This observation is partially consistent with the history of our patient, in whom most opportunistic infections occurred while receiving 400 mg/day of pralsetinib. However, after an infectious adverse event, the timing and resuming dose of pralsetinib remain unknown and dependent on local expertise.
Considering these numerous infectious events, we first hypothesized the possibility of a class effect common to all RET inhibitors. However, no severe infections were reported with selpercatinib in clinical trials nor found in the French Pharmacovigilance Registry that we consulted in February 2024. It seems therefore unlikely that the high incidence of infectious events observed with pralsetinib is linked to a class effect of RET inhibitors. Our next hypothesis was an association with an off-target effect of pralsetinib. Indeed, while selpercatinib and pralsetinib share common off-target effects on VEGF1-3 and FGFR1-3 (5), selpercatinib specifically inhibits aurora kinase B, while pralsetinib has specific off-target inhibition on JAK1/2, DDR1, FLT3, PDGFRb, TRKA, and TRKC (5, 17). Among them, the JAK-mediated intracellular signaling pathways play a crucial role in immunoregulation and host defense. It is well established that for autoimmune diseases or cancers, JAK inhibitors are associated with an increased frequency of infection (18–20). Pralsetinib may therefore predispose patients to infections as a result of their off-target effects on JAK1/2. In vitro, pralsetinib has proven to have a highly specific inhibition on JAK1 and, to a lesser extent, JAK2, with a respective 16-fold and 136-fold shift increase in Ic50 as compared to RET Ic50 (17). In vitro, pralsetinib inhibition of JAK2 decreased STAT-5 phosphorylation (5). Physiologically, the RET pathway is intercrossed with the JAK/STAT pathway, and in addition to JAK1/2 off-target inhibition, RET inhibition by pralsetinib can lead to a decrease in JAK/STAT activation (21) (Figure 2). However, this pathway does not appear to be the most relevant, considering the low frequency of infectious events observed in other RET inhibitors. Considering the key role of the JAK/STAT pathway in innate immunity, immune tolerance (22), cytokine cascade, and interferon gamma response (23), we can hypothesize that a spectrum of pralsetinib infections might be related to the off-target inhibition of the JAK/STAT pathway.

Figure 2. Pralsetinib off-target effect on JAK1/2 and infectious adverse events. The left panel is represented the pralsetinib therapeutic pathway. The right panel is presented pralsetinib’s off-target effect on the JAK/STAT signaling pathway. The common infections associated with JAK/STAT inhibition are viral infections, intracellular bacterial infections, recurrent pneumonia, and candida infections. We hypothesize that this off-target inhibition is involved in recurrent infectious events under pralsetinib treatment.
Finally, there were no iatrogenic or confounding risk factors that could have interfered with the pralsetinib treatment. Notably, Charcot–Marie–Tooth disease affecting our patient is not associated with immunosuppression or recurrent infectious events.
Conclusion
In addition to pneumonia, recurrent and serious infectious adverse events appear to be of concern under the pralsetinib therapy but not reported with selpercatinib. These infections might be wrongly interpreted as disease progression, despite the clinical activity of pralsetinib, and could be related to specific off-target inhibition of the JAK1/2 pathway. Early detection and timely application of anti-infective drugs are key to treatment. Further studies are needed to provide proper guidelines to physicians for managing infectious adverse events under pralsetinib therapy.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
FP: Conceptualization, Investigation, Methodology, Supervision, Validation, Writing – original draft, Writing – review & editing. MJa: Investigation, Writing – review & editing. CG-R: Data curation, Investigation, Supervision, Writing – original draft. IK: Writing – review & editing. GL: Writing – review & editing. MJo: Writing – review & editing. JM: Writing – review & editing, Investigation. RG: Writing – review & editing. NF: Writing – review & editing, Investigation, Methodology, Supervision. EA: Investigation, Methodology, Supervision, Writing – review & editing, Conceptualization, Data curation, Formal analysis, Funding acquisition, Project administration, Resources, Software, Validation, Visualization, Writing – original draft.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Murakumo, Y, Jijiwa, M, Asai, N, Ichihara, M, and Takahashi, M. RET and neuroendocrine tumors. Pituitary. (2006) 9:179–92. doi: 10.1007/s11102-006-0263-4
2. Gainor, JF, Curigliano, G, Kim, D-W, Lee, DH, Besse, B, Baik, CS, et al. Pralsetinib for RET fusion-positive non-small-cell lung cancer (ARROW): a multi-cohort, open-label, phase 1/2 study. Lancet Oncol. (2021) 22:959–69. doi: 10.1016/S1470-2045(21)00247-3
3. Subbiah, V, Wolf, J, Konda, B, Kang, H, Spira, A, Weiss, J, et al. Tumour-agnostic efficacy and safety of selpercatinib in patients with RET fusion-positive solid tumours other than lung or thyroid tumours (LIBRETTO-001): a phase 1/2, open-label, basket trial. Lancet Oncol. (2022) 23:1261–73. doi: 10.1016/S1470-2045(22)00541-1
4. Subbiah, V, Hu, MI-N, Gainor, JF, Mansfield, AS, Alonso, G, Taylor, MH, et al. Clinical activity of the RET inhibitor pralsetinib (BLU-667) in patients with RET fusion+ solid tumors. JCO. (2020) 38:109. doi: 10.1200/JCO.2020.38.15_suppl.109
5. FDAC for DE . FDA approves pralsetinib for non-small cell lung cancer with RET gene fusions. FDA. (2023). Available at: https://www.fda.gov/drugs/drug-approvals-and-databases/fda-approves-pralsetinib-non-small-cell-lung-cancer-ret-gene-fusions
6. Kato, S, Subbiah, V, Marchlik, E, Elkin, SK, Carter, JL, and Kurzrock, R. RET aberrations in diverse cancers: next-generation sequencing of 4,871 patients. Clin Cancer Res. (2017) 23:1988–97. doi: 10.1158/1078-0432.CCR-16-1679
7. Gao, M, Zhang, X, Yan, H, Sun, D, Yang, X, Yuan, F, et al. Pralsetinib-associated pneumonia in RET fusion-positive non-small cell lung cancer. Support Care Cancer. (2023) 31:671. doi: 10.1007/s00520-023-08125-3
8. An, L, Chen, P, Wang, J, Qin, X, Liu, T, Gao, Y, et al. Case report: recurrent lung infections following treatment with pralsetinib for an elderly patient with RET-fusion positive NSCLC. Front Oncol. (2022) 12:1024365. doi: 10.3389/fonc.2022.1024365
9. Chen, Y, Wu, Y, Shao, Z, Ren, F, Jiao, W, and Wu, S. RET fusion-positive non-small cell lung cancer complicated with disseminated hematogenous tuberculosis during first-line Pralsetinib treatment: A case report. (2023). doi: 10.21203/rs.3.rs-2759236/v1
10. Dhital, R, Paudel, A, Bohra, N, and Shin, AK. Herbaspirillum infection in humans: a case report and review of literature. Case Rep Infect Dis. (2020) 2020:1–6. doi: 10.1155/2020/9545243
11. Zheng, X, Fang, M, Fan, Y, Sun, Y, Sun, M, Yang, A, et al. Efficacy and safety of pralsetinib in Chinese advanced RET-mutant medullary thyroid cancer patients. Endocr Relat Cancer. (2024):e230134. doi: 10.1530/ERC-23-0134
12. Lee, Y-P, Jeong, B-H, Eun, Y, Kang, C-I, Park, S, Jung, HA, et al. Extrapulmonary tuberculosis in patients with RET fusion-positive non-small cell lung cancer treated with pralsetinib: a Korean single-Centre compassionate use experience. Eur J Cancer. (2021) 159:167–73. doi: 10.1016/j.ejca.2021.09.037
13. Bolourchi, S, and Julka, K. A CASE of ENDOBRONCHIAL tuberculosis in a patient on PRALSETINIB therapy. Chest. (2023) 164:A4542. doi: 10.1016/j.chest.2023.07.2945
14. Passaro, A, Russo, GL, Passiglia, F, D’Arcangelo, M, Sbrana, A, Russano, M, et al. Pralsetinib in RET fusion-positive non-small-cell lung cancer: a real-world data (RWD) analysis from the Italian expanded access program (EAP). Lung Cancer. (2022) 174:118–24. doi: 10.1016/j.lungcan.2022.11.005
15. Park, M, Ho, DY, Wakelee, HA, and Neal, JW. Opportunistic invasive fungal infections mimicking progression of non-small-cell lung Cancer. Clin Lung Cancer. (2021) 22:e193–200. doi: 10.1016/j.cllc.2020.10.001
16. Kassir, N, McDougall, D, Kuruvilla, D, Kim, S, Kumar, S, Rahman, A, et al. Exposure-response relationships for Pralsetinib in patients with RET-altered thyroid Cancer or RET fusion-positive non-small cell lung Cancer. J Clin Pharmacol. (2024) 64:685–96. doi: 10.1002/jcph.2409
17. Subbiah, V, Gainor, JF, Rahal, R, Brubaker, JD, Kim, JL, Maynard, M, et al. Precision targeted therapy with BLU-667 for RET-driven cancers. Cancer Discov. (2018) 8:836–49. doi: 10.1158/2159-8290.CD-18-0338
18. Winthrop, K, Isaacs, J, Calabrese, L, Mittal, D, Desai, S, Barry, J, et al. Opportunistic infections associated with Janus kinase inhibitor treatment for rheumatoid arthritis: a structured literature review. Semin Arthritis Rheum. (2023) 58:152120. doi: 10.1016/j.semarthrit.2022.152120
19. Adas, MA, Alveyn, E, Cook, E, Dey, M, Galloway, JB, and Bechman, K. The infection risks of JAK inhibition. Expert Rev Clin Immunol. (2022) 18:253–61. doi: 10.1080/1744666X.2022.2014323
20. Alves, C, Penedones, A, Mendes, D, and Marques, FB. The risk of infections associated with JAK inhibitors in rheumatoid arthritis: a systematic review and network Meta-analysis. J Clin Rheumatol. (2022) 28:e407–14. doi: 10.1097/RHU.0000000000001749
21. Mastrodomenico, L, Piombino, C, Riccò, B, Barbieri, E, Venturelli, M, Piacentini, F, et al. Personalized systemic therapies in hereditary Cancer syndromes. Genes. (2023) 14:684. doi: 10.3390/genes14030684
22. Hu, Q, Bian, Q, Rong, D, Wang, L, Song, J, Huang, H-S, et al. JAK/STAT pathway: extracellular signals, diseases, immunity, and therapeutic regimens. Front Bioeng Biotechnol. (2023) 11:1110765. doi: 10.3389/fbioe.2023.1110765
Keywords: pralsetinib, RET inhibitor, infection, JAK/STAT, case report
Citation: Poumeaud F, Jaffrelot M, Gomez-Roca C, Korakis I, Leonardi G, Joly M, Mazières J, Guimbaud R, Fares N and Alouani E (2024) A double-edged sword: unusual multiple severe infections with pralsetinib: a case report and literature review. Front. Med. 11:1402902. doi: 10.3389/fmed.2024.1402902
Edited by:
Dharmendra Kumar Yadav, Gachon University, Republic of KoreaReviewed by:
Apurva Patel, Gujarat Cancer & Research Institute, IndiaCaio Abner Leite, Beneficência Portuguesa de São Paulo, Brazil
Copyright © 2024 Poumeaud, Jaffrelot, Gomez-Roca, Korakis, Leonardi, Joly, Mazières, Guimbaud, Fares and Alouani. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Emily Alouani, YWxvdWFuaS5lQGNodS10b3Vsb3VzZS5mcg==