
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Med., 30 May 2024
Sec. Infectious Diseases: Pathogenesis and Therapy
Volume 11 - 2024 | https://doi.org/10.3389/fmed.2024.1401439
This article is part of the Research TopicEmerging SARS-COV-2 Variants: Genomic Variations, Transmission, Pathogenesis, Clinical Impact and Interventions, Volume IIIView all 26 articles
 Li-Li Liu1,2,3
Li-Li Liu1,2,3 Yu-Wei Liao1,2,3Xiao-Hua Yu1,2,3
Yu-Wei Liao1,2,3Xiao-Hua Yu1,2,3 Ling Rong4Bi-Gui Chen4Gang Chen5Guang-Kuan Zeng1,2,3
Ling Rong4Bi-Gui Chen4Gang Chen5Guang-Kuan Zeng1,2,3 Li-Ye Yang1,2,3*
Li-Ye Yang1,2,3*Objective: To analyze the clinical characteristics and prognostic impacts of SARS-CoV-2 Omicron infection among cancer inpatients during the December 2022 – February 2023 surge, in order to provide scientific evidence for clinical treatment and prevention and control measures.
Methods: A retrospective analysis was conducted on the clinical features, prognosis, and vaccination status of cancer in-patients infected with the Omicron variant during the COVID-19 pandemic of December 2022 – February 2023.
Results: A total of 137 cancer inpatients were included in the study, with a median age of 61 years, and 75 patients (54.74%) were male. The main symptoms were cough (69 cases, 50.36%), expectoration (60 cases, 43.80%), and fever (53 cases, 39.69%). Chest CT examination revealed bilateral pneumonia in 47 cases (34.31%, 47/137) and pleural effusion in 24 cases (17.52%, 24/137). Among the cancer patients, 116 cases (84.67%, 116/137) had solid tumors, and 21 cases (15.33%, 21/137) had hematologic malignancies, with the main types being breast cancer (25 cases, 18.25%) and lung cancer (24 cases, 17.52%). Among the cancer patients, 46 cases (33.58%) were asymptomatic, 81 cases (59.12%) had mild disease, 10 cases (7.30%) had severe infection, and 8 cases (5.84%) died. A total of 91 patients (66.42%) had been vaccinated, with 58 patients (42.34%) receiving three doses. Multivariate analysis showed that cerebral infarction and hypoproteinemia were risk factors for death from COVID-19 infection.
Conclusion: Cancer patients infected with SARS-CoV-2 Omicron typically exhibit mild disease manifestations, but some cancer patients infected with the Omicron variant might progress to severe illness, and even death, necessitating close monitoring and attention during the early stages of infection. Additionally, the presence of cerebral infarction and hypoproteinemia significantly increases the risk of death.
Since the outbreak of the coronavirus (COVID-19) in 2019, the SARS-CoV-2 virus has been raging globally for nearly 3 years, exerting a significant impact on the global economy and bringing unprecedented disease burdens and public health pressures. As of 1 January 2023, the world has reported over 656 million confirmed cases and more than 6.6 million deaths (1). The virus spreads primarily through interpersonal transmission and new variants continue to emerge. The Omicron variant was first detected in South Africa on 9 November 2021, and subsequently rapidly disseminated globally (2). Due to its enhanced transmissibility and immune evasion capabilities (3–5), Omicron easily spreads through human mobility and contact.
Since December 2021, the Omicron strain has locally erupted in Tianjin, Shanghai, and other regions of China. Based on the several rounds of locally transmitted Omicron outbreaks that have occurred in China, the infection rate is high, with low hospitalization rates, lighter disease severity, and lower mortality rates (6–8). The COVID-19 pandemic continues to pose significant challenges worldwide, despite efforts to control its spread and impact. The global control of the COVID-19 pandemic is a multifaceted challenge that demands coordinated efforts, innovative solutions, and collective resilience. Addressing the ongoing challenges, such as vaccine distribution inequities, vaccine hesitancy, emergence of new variants, overwhelmed healthcare systems, and economic repercussions, requires a comprehensive approach that prioritizes equity, collaboration, and evidence-based interventions. By acknowledging these challenges and working together to overcome them, the world can advance toward a future free from the grip of the COVID-19 pandemic (9, 10).
In late 2022, the Chinese government adjusted its prevention and control policies, shifting from a “dynamic zero-COVID” strategy to normalization of epidemic prevention and control measures (11). This resulted in the termination of isolation measures for COVID-19 infected individuals, leading to the first large-scale COVID-19 outbreak in Yangjiang during December 2022 to February 2023. Cancer patients are vulnerable to SARS-CoV-2 infection due to their physical condition and compromised immune system, potentially leading to more severe disease manifestations and poorer prognoses (12, 13). Nevertheless, there is still a lack of extensive research on the effects of the Omicron variant on cancer patients in China (14, 15). Therefore, this study aims to analyze the infection characteristics, outcomes, and vaccination status of this special population during the COVID-19 Omicron pandemic, providing scientific evidence for clinical treatment and prevention and control strategies.
A retrospective analysis was conducted on cancer patients infected with the Omicron variant of SARS-CoV-2 and hospitalized in a tertiary hospital in western Guangdong between 8 December 2022, and 14 February 2023. Adult patients (≥18 years old) diagnosed with cancer and hospitalized were included in the study, including solid tumors, in situ cancers, and hematologic malignancies. Patients with benign tumors or those who had undergone curative surgery without recurrence for 5 years were excluded from the analysis. All patients tested positive for SARS-CoV-2 nucleic acid through real-time reverse transcription polymerase chain reaction (RT-PCR) using nasopharyngeal swab samples. The diagnosis and clinical classification of COVID-19 followed the diagnostic criteria outlined in the “Diagnosis and Treatment Plan for Novel Coronavirus Pneumonia (10th trial edition),” categorizing patients into asymptomatic, mild, moderate, severe, and critical types (16). For a better understanding of clinical features, this study grouped mild and moderate cases as non-severe group, and severe and critical cases as severe group. This study was approved by the Research Ethics Committee of Yangjiang People’s Hospital (No. 20230003).
Patient medical records and vaccination information were collected, including age, sex, clinical characteristics, cancer types, laboratory test results (complete blood count, serum biochemistry, coagulation assays, and inflammatory markers), and pulmonary imaging findings (CT scans and X-rays). Clinical symptoms and laboratory indices were collected at the time of the first hospital admission test. If data were not available at admission, the most recent test results shortly after admission were used. Information on drug treatments received by hospitalized patients, including antiviral drugs, antibiotics, anticoagulants, and corticosteroids, was also gathered. When necessary, patients will receive oxygen therapy, including low-flow, medium-flow oxygen, high-flow oxygen, non-invasive ventilation, and invasive ventilation with endotracheal intubation. Two outcomes were evaluated: discharge and death. Death was defined as mortality during hospitalization and death within 1 week of discharge due to critical condition and abandonment of treatment.
Data analysis was performed using SPSS 22.0 software. Continuous variables and categorical variables were represented as median, count (n), and percentage (%), while numerical data were described using mean ± standard deviation (x̄ ± s). Group data were analyzed using independent sample t-tests. Multifactor analysis was employed to explore factors influencing mortality in COVID-19 infections, and P < 0.05 was considered statistically significant.
A total of 137 patients were included, with a median age of 61 years (range: 26–95 years), and 51.1% of the patients were over 60 years old, with 54.74% (74/137) being male. The age distribution was mainly concentrated in the middle-aged and elderly stages, with the most patients falling between the ages of 51–70, totaling 75 individuals, accounting for over half (54.8%). Younger patients (18–40 years) and elderly patients (over 80 years) were relatively fewer, accounting for 5.1% (7 cases) and 13.9% (19 cases), respectively. Major symptoms included cough (50.36%, 69/137), expectorations (43.80%, 60/137), and fever (38.69%, 53/137). Some patients also experienced fatigue (20.44%, 28/137), sore throat (16.79%, 23/137), loss of appetite (16.79%, 23/137), dizziness/headache (14.60%, 20/137), and shortness of breath (13.87%, 19/137). Among the 137 patients, 33.58% (46/137) were asymptomatic, 59.12% (81/137) had non-severe symptoms, and 7.30% (10/137) were classified as severe. A total of 54.75% (75/137) of the patients had one or more underlying medical conditions, with hypoalbuminemia (25.55%, 35/137), hypertension (21.90%, 30/137), and anemia (21.17%, 29/137) being the most common. Radiological findings mostly indicated bilateral pneumonia (34.31%, 47/137), with a few cases showing bilateral pleural effusion (13.14%, 18/137) and unilateral pleural effusion (4.38%, 6/137) (Table 1).
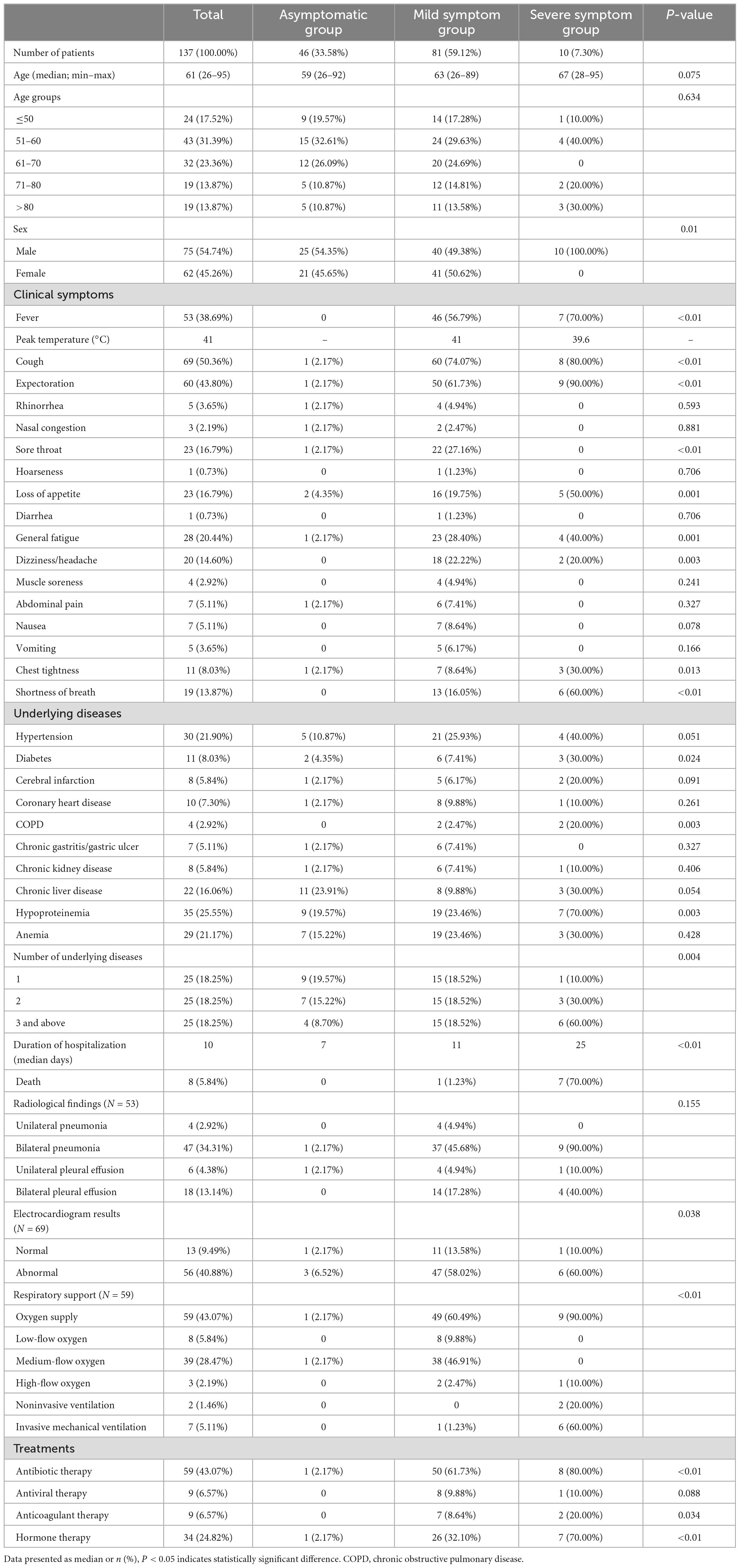
Table 1. Clinical characteristics and laboratory results of COVID-19 in cancer patients.
The average length of hospital stay was 10 days, with a longer duration noted in patients experiencing more severe symptoms. Out of eight patients (5.84%) who passed away, 70% (7/10) had severe cases of COVID-19. Five deaths resulted from respiratory failure and severe pneumonia, while three fatalities were not directly linked to COVID-19.
A total of 84.67% (116/137) of the patients had solid tumors, while 15.33% (21/137) had hematologic malignancies. The most common cancer types were breast cancer (18.25%, 25/137), lung cancer (17.52%, 24/137), colorectal cancer (10.22%, 14/137), nasopharyngeal cancer (8.03%, 11/137), and liver cancer (8.03%, 11/137). Among solid tumor patients, 60.34% (70/116) were in advanced stages of cancer, and 38.79% (45/116) had already metastasized. There was no statistically significant association between cancer type and COVID-19 severity classification (Table 2).
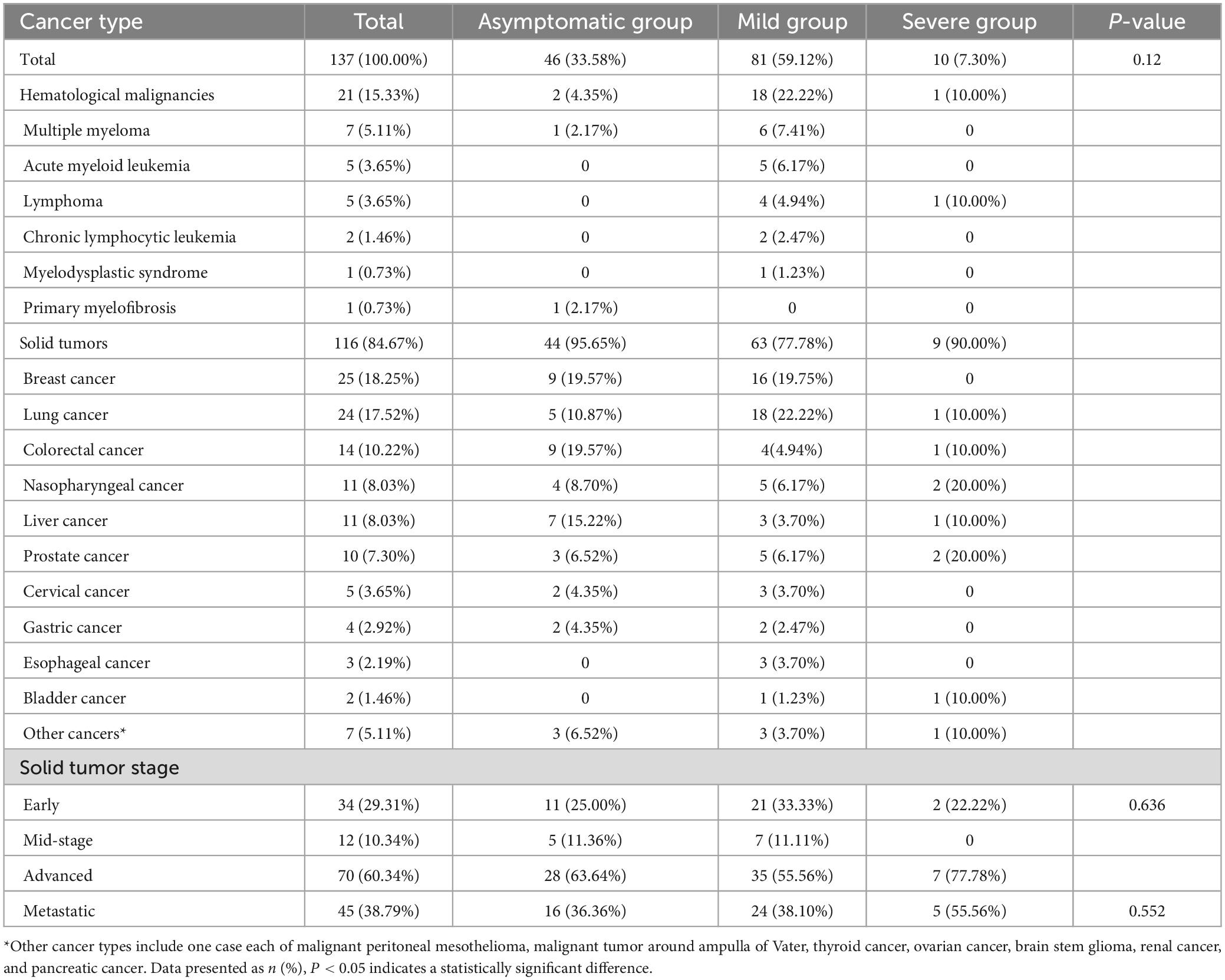
Table 2. Cancer types.
Over 66.42% (91/137) of cancer patients have received the COVID-19 vaccine, with 42.34% (58/137) having received all three doses. The earliest vaccination date was on 26 March 2021, and the latest was on 23 December 2022, with vaccination ages ranging from 25 to 80 years old. A total of 54.95% (50/91) of the vaccines administered were produced by Sinovac Biotech Ltd. There was no significant association found between vaccine administration and the severity of COVID-19 cases. Details of vaccine administration based on COVID-19 severity classification can be found in Table 3.
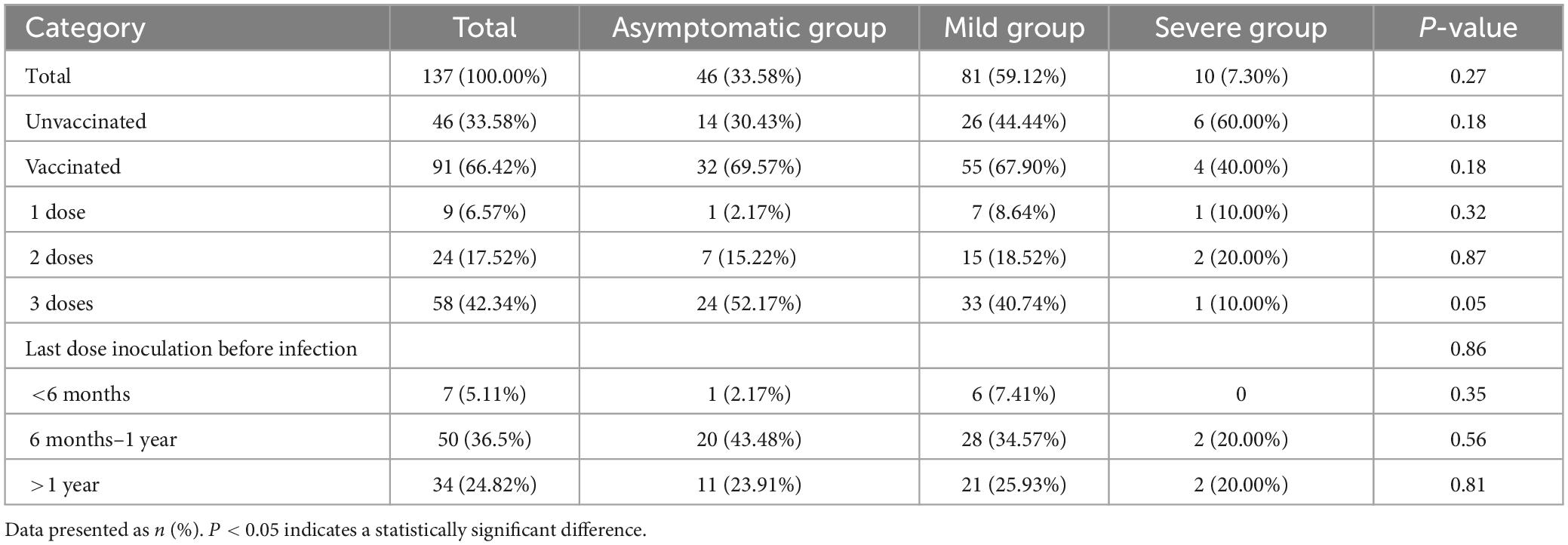
Table 3. COVID-19 vaccination status.
Due to significant variations in blood results among patients with hematologic malignancies, statistical analysis was not deemed meaningful. Therefore, solid tumor patients were divided into two groups based on COVID-19 severity classification: non-severe group including asymptomatic, mild, and moderate cases, and severe group comprising severe and critical cases. In cases of multiple laboratory results, the data from the first hospital admission test were documented. Statistically significant differences were observed in various laboratory parameters between the severe and non-severe groups of COVID-19 patients, including neutrophils (Neu), NLR (neutrophils to lymphocytes ratio), aspartate aminotransferase (AST), urea, creatinine (CR), hydroxybutyrate dehydrogenase (HBDH), lactate dehydrogenase (LDH), C-reactive protein (CRP), interleukin-8 (IL-8), lymphocytes (Lym), total protein (TP), and albumin (ALB). Results of the mentioned parameters were generally higher in the severe group than in the non-severe group of COVID-19 patients, particularly in WBC count, Neu count, and CRP, which are associated with infection and inflammation. On the other hand, levels of RBC and Lym were lower in the severe group compared to the non-severe group, potentially indicating compromised immune function (Table 4).
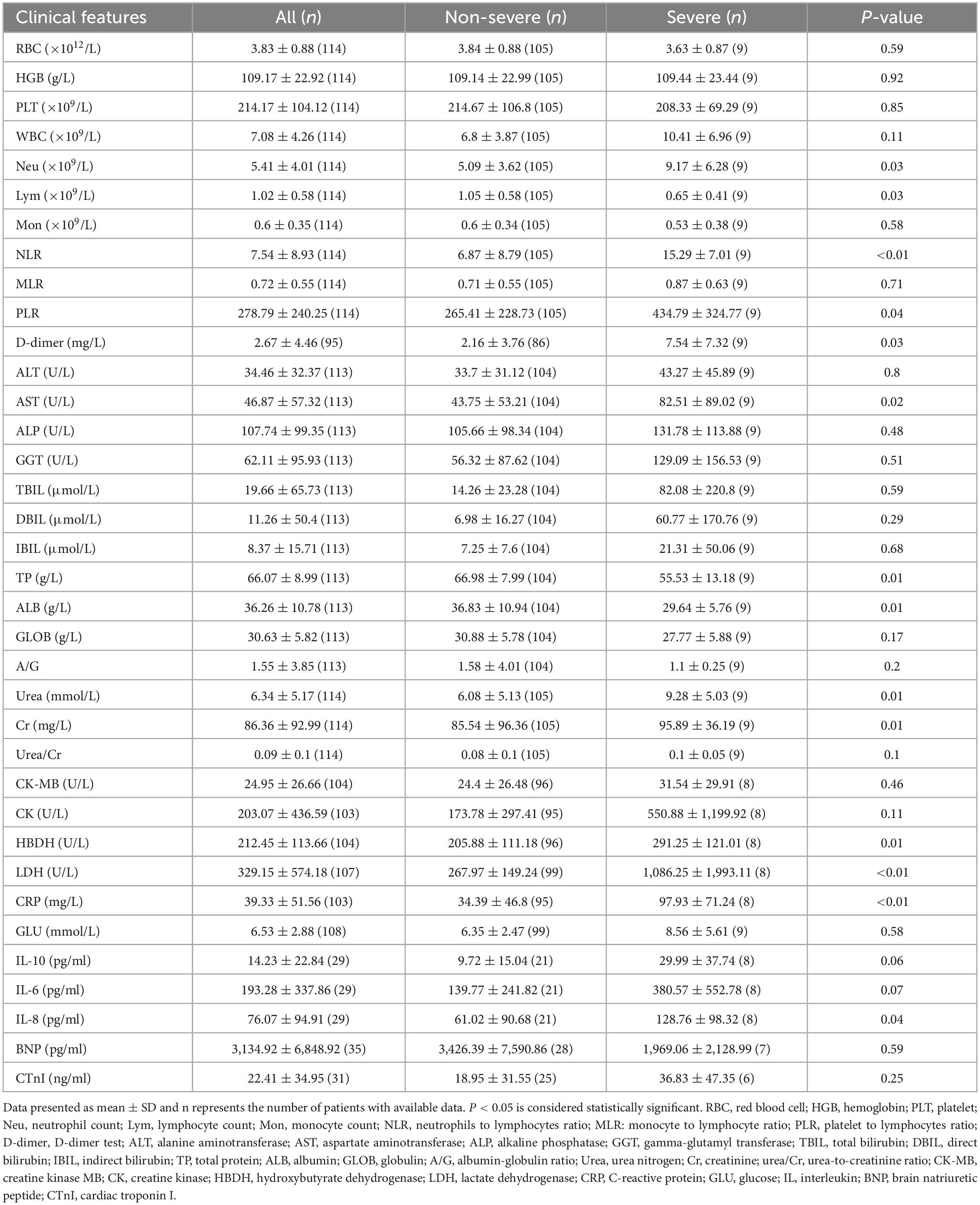
Table 4. Laboratory indices of severe and non-severe solid tumor patients upon hospital admission.
There were a total of 8 cancer patients who died, spanning a wide age range from 28 to 95 years, all of whom were male. The shortest hospitalization period among these patients was 1 day, while the longest was 58 days. The types of cancer varied and included prostate cancer, bladder cancer, lymphoma, nasopharyngeal cancer, brainstem glioma, liver cancer, and lung cancer, predominantly in advanced stages. Based on COVID-19 severity classification, seven of the deceased cases were critical, while one was mild, and a total of five patients required endotracheal intubation and mechanical ventilation assistance for breathing. All patients had other comorbidities and health issues, with COVID-19 infection being a significant contributing factor to their deaths (Supplementary Table 1).
In the linear regression model exploring risk factors for COVID-19 mortality, individuals with cerebral infarction and hypoalbuminemia have a significantly elevated risk of death (Table 5).
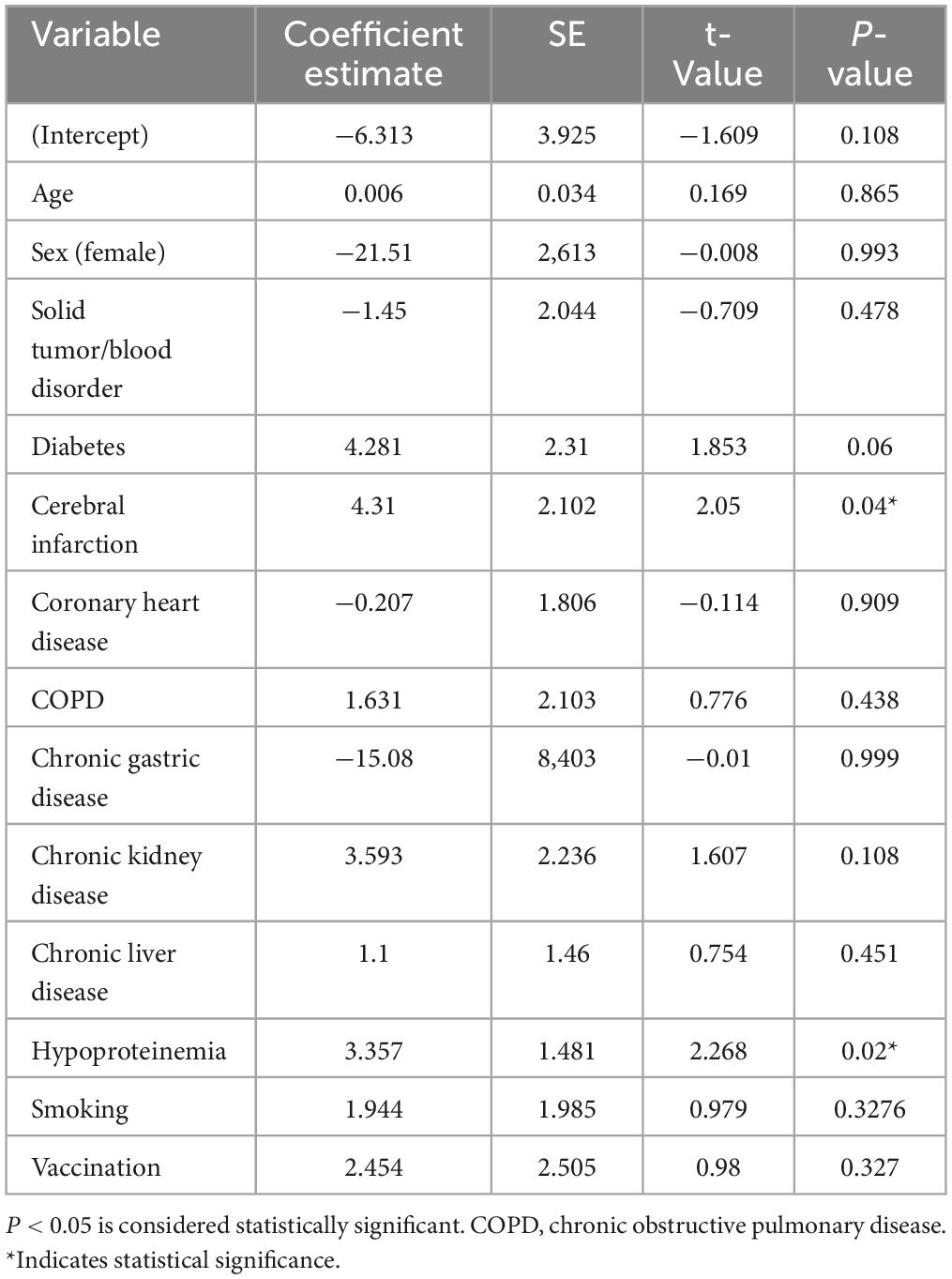
Table 5. Analysis of risk factors for COVID-19 mortality.
Since the outbreak of the COVID-19 pandemic at the end of 2019, the China government has implemented a dynamic Zero COVID-19 strategy, this policy entails swiftly dealing with each discovered local confirmed case, extinguishing the infection promptly to eradicate the transmission chain entirely—a strategy commonly known as achieving zero cases (11). Since December 2019, a series of domestic outbreaks has occurred in the country. Whenever confirmed cases emerge, strict control measures are implemented at their activity venues and residences. Multiple rounds of nucleic acid testing are conducted, and only locations free from epidemic risks are unsealed, aligning with the overarching strategy for COVID-19 epidemic prevention and control. This comprehensive approach encompasses three key elements: timely and proactive identification of infection sources, swift implementation of public health and social intervention measures to trace and manage close contacts, and effective patient treatment. While China’s “Dynamic Zero” epidemic prevention policy has yielded significant results in epidemic control, the localized closed control measures have led to factory shutdowns and logistical disruptions, exerting a noticeable adverse impact on economic operations (17). In order to better cope with virus mutations and changes in the epidemic situation, by the end of 2022, significant adjustments were made to epidemic prevention and control policies in China, including reducing lockdown durations, optimizing isolation methods, relaxing entry policies, and enhancing vaccine coverage (18). The number of domestic SARS-CoV-2 infections has significantly increased, marking the country’s first nationwide COVID-19 pandemic, as well as the first large-scale local outbreak in the Yangjiang region. Monitoring data from the Chinese Center for Disease Control and Prevention shows that since 9 December 2022, a nationwide pandemic of COVID-19 infections has emerged, with the number of positive cases peaking on December 22 (6.94 million) before gradually declining. During this pandemic, the predominant strains across the country are the BA.5.2 and BF.7 variants of the Omicron mutant (19).
Since the discovery of the COVID-19 Omicron variant in South Africa in November 2021, it has rapidly spread globally due to its high transmissibility and immune evasion capabilities (2–5). In early 2022, the Omicron strain began to emerge in localized areas in China, with studies in Macau and Shanghai indicating that individuals infected with the Omicron variant may experience relatively mild symptoms and could potentially present with more asymptomatic infections (8, 19).
According to previous research reports, cancer patients are considered a high-risk group for COVID-19, with a higher risk of infection, increased susceptibility to severe illness, and higher mortality rates (20, 21). Various risk factors are associated with the severity of COVID-19 in cancer patients, including age, underlying health conditions, and cancer types (22, 23). In this study, the male-to-female ratio of cancer patients was 1.2:1, with 82.48% (113/137) of patients over the age of 50, 33.58% (46/137) being asymptomatic carriers, 59.12% (81/137) having mild symptoms, and 7.30% (10/137) in critical condition. Out of the total patients, eight died, with seven being severe/critical COVID-19 cases, of which five deaths were due to respiratory failure, severe pneumonia, and thee deaths were not directly attributed to COVID-19. Our study found a mortality rate of 5.84% (8/137) in cancer patients with COVID-19 infection, while the mortality rate in the severe/critical COVID-19 group was 70% (7/10). Additionally, this study found that cancer patients with conditions such as stroke and hypoalbuminemia may face significantly higher mortality risks. Consistent with the findings of Lee, Sun, and other scholars, for cancer patients, especially those with multiple comorbidities, Omicron infection may still lead to serious outcomes (24, 25). Previous research has indicated that patients with hematologic cancers may be at a higher risk of severe COVID-19 due to immune system alterations in blood cell function compared to non-hematologic cancer patients (26). However, due to the small sample size in this study, there was insufficient data to explore the relationship between the type of cancer and the severity of COVID-19.
In our study, the clinical manifestations of cancer patients combined with COVID-19 infection were similar to the general population, primarily presenting symptoms such as cough, sputum production, and fever (6, 7, 12). However, significant differences were observed in laboratory tests between cancer patients with severe COVID-19 infection and non-severe cases. Specifically, levels of indicators such as Neu, AST, Urea, CR, HBDH, LDH, CRP, and IL-8 were elevated in severe patients, while levels of indicators like LY, TP, and ALB were decreased. These differences may be related to the severity of the patient’s illness and any comorbidities (27). For cancer patients with concurrent COVID-19 infection, close monitoring of their condition and implementation of effective treatment measures are crucial to reduce the incidence and mortality rates of severe cases. Additionally, preventive measures are also essential to decrease the risk of infection.
Vaccination in China primarily consists of inactivated vaccines, adenovirus vector vaccines, and recombinant subunit protein vaccines, with a higher proportion of individuals receiving inactivated vaccines. Over 90% of Chinese citizens have completed the two doses of inactivated COVID-19 vaccines produced by Sinovac Biotech and China National Pharmaceutical Group (28), with no significant differences observed between different vaccine types (29, 30). In this study, 66.42% (91/137) of cancer patients had been vaccinated against COVID-19, although the protective effect of the vaccine was not significant, likely due to the small sample size. While vaccination may not provide optimal protection against the Omicron variant, it can reduce the likelihood of severe illness and death compared to unvaccinated individuals (31, 32). From the perspective of Chinese society, the COVID-19 vaccination program is still considered effective and cost-effective (28, 33), therefore, routine and booster doses of inactivated virus vaccines are necessary (34–36).
As the first comprehensive reopening after the COVID-19 pandemic in China, the mortality rate among cancer patients, a special high-risk group, has significantly decreased compared to previous reports, but still remains higher than the general population (37–39). Due to the shortage of hospital beds during the initial COVID-19 outbreak in the region, hospitals admitted only more severe cases, while many asymptomatic or mildly symptomatic cancer patients chose to self-isolate at home, waiting for improvement before receiving relevant treatment. In reality, the mortality rate among cancer patients with concurrent COVID-19 infection is lower (40). According to the announcement by the World Health Organization on 5 May 2023, the COVID-19 pandemic no longer constitutes a “Public Health Emergency of International Concern.” However, due to the continued variation of the novel coronavirus and the risk of reinfection (5, 41), effective epidemic prevention and control measures still need to be implemented, along with active virus research and treatment efforts.
In our study, we acknowledge certain limitations. Primarily, our sample was restricted to cancer patients from a single hospital in the Yangjiang region, thus limiting the generalizability of our findings regarding the prevalence of COVID-19 infection among cancer patients. Secondly, the lack of data from some laboratory tests and clinical records may lead to biased data interpretation. Therefore, for a more scientifically sound analysis, it is important to include a larger sample size and conduct longer follow-ups to comprehensively understand the impact of SARS-CoV-2 on cancer patients’ outcomes.
The original contributions presented in this study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
The studies involving humans were approved by the Research Ethics Committee of Yangjiang People’s Hospital (No. 20230003). The studies were conducted in accordance with the local legislation and institutional requirements. The ethics committee/institutional review board waived the requirement of written informed consent for participation from the participants or the participants’ legal guardians/next of kin because this study was retrospective, and there is no identifiable data in this article.
L-LL: Investigation, Methodology, Validation, Writing – original draft. Y-WL: Software, Writing – original draft. X-HY: Data curation, Methodology, Validation, Writing – original draft. LR: Validation, Writing – original draft. B-GC: Investigation, Writing – original draft. GC: Validation, Writing – review & editing. G-KZ: Investigation, Writing – review & editing. L-YY: Conceptualization, Funding acquisition, Resources, Supervision, Writing – original draft, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This study was supported by the High Level Development Plan of People’s Hospital of Yangjiang (grant no. 2021007), the Research Plan of Hygiene and Health Bureau of Yangjiang (no. 2023032), and the High Level and Key Health Research Plan of Yangjiang (no. 2023001). The funder had no role in the study’s design, data interpretation, and manuscript writing.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2024.1401439/full#supplementary-material
2. World Health Organization. Enhancing response to omicron SARS-CoV-2 variant: Technical brief and priority actions for member states. [EB/OL]. Geneva: World Health Organization (2022).
3. Pulliam JRC, van Schalkwyk C, Govender N, von Gottberg A, Cohen C, Groome MJ, et al. Increased risk of SARS-CoV-2 reinfection associated with emergence of Omicron in South Africa. Science. (2022) 376:e4947. doi: 10.1126/science.abn4947
4. Kontopodis E, Pierros V, Stravopodis DJ, Tsangaris GT. Prediction of SARS-CoV-2 omicron variant immunogenicity, immune escape and pathogenicity, through the analysis of spike protein-specific core unique peptides. Vaccines (Basel). (2022) 10:357. doi: 10.3390/vaccines10030357
5. Reynolds CJ, Pade C, Gibbons JM, Otter AD, Lin KM, Muñoz Sandoval D, et al. Immune boosting by B.1.1.529 (omicron) depends on previous SARS-CoV-2 exposure. Science. (2022) 377:e1841. doi: 10.1126/science.abq1841
6. Ren Y, Shi L, Xie Y, Wang C, Zhang W, Wang F, et al. Course and clinical severity of the SARS-CoV-2 omicron variant infection in Tianjin, China. Medicine (Baltimore). (2023) 102:e34669. doi: 10.1097/MD.0000000000034669
7. Zhang H, Weng Z, Zheng Y, Zheng M, Chen W, He H, et al. Epidemiological and clinical features of SARS-CoV-2 omicron variant infection in Quanzhou, Fujian province: A retrospective study. Sci Rep. (2023) 13:22152. doi: 10.1038/s41598-023-49098-x
8. Wang B, Yu Y, Yu Y, Wang N, Chen F, Jiang B, et al. Clinical features and outcomes of hospitalized patients with COVID-19 during the omicron wave in Shanghai, China. J Infect. (2023) 86:e27–9. doi: 10.1016/j.jinf.2022.08.001
9. Perez Perez GI, Talebi Bezmin Abadi A. Ongoing challenges faced in the global control of COVID-19 pandemic. Arch Med Res. (2020) 51:574–6. doi: 10.1016/j.arcmed.2020.04.016
10. Saqr M, Wasson B. COVID-19: Lost opportunities and lessons for the future. Int J Health Sci (Qassim). (2020) 14:4–6.
11. Xiao H, Liu F, Unger JM. Dynamic zero-COVID policy and healthcare utilization patterns in China during the Shanghai COVID-19 Omicron outbreak. Commun Med (Lond). (2023) 3:143. doi: 10.1038/s43856-023-00375-w
12. Liang W, Guan W, Chen R, Wang W, Li J, Xu K, et al. Cancer patients in SARS-CoV-2 infection: A nationwide analysis in China. Lancet Oncol. (2020) 21:335–7. doi: 10.1016/S1470-2045(20)30096-6
13. Kuderer NM, Choueiri TK, Shah DP, Shyr Y, Rubinstein SM, Rivera DR, et al. Clinical impact of COVID-19 on patients with cancer (CCC19): A cohort study. Lancet. (2020) 395:1907–18. doi: 10.1016/S0140-6736(20)31187-9
14. Zhang M, Cao L, Zhang L, Li X, Chen S, Zhang Y. SARS-CoV-2 reinfection with omicron variant in Shaanxi province, China: December 2022 to February 2023. BMC Public Health. (2024) 24:496. doi: 10.1186/s12889-024-17902-6
15. Cheong HH, Sio FI, Chan CC, Neng SI, Sam IP, Cheang T, et al. Clinical characteristics of COVID-19 patients infected by the omicron variants in Macao, China: A cross-sectional study. Health Sci Rep. (2023) 6:e1361. doi: 10.1002/hsr2.1361
16. National Health Commission of the People’s Republic of China. Novel coronavirus infection diagnosis and treatment protocol (trail version 10). Beijing: National Health Commission of the People’s Republic of China (2023).
17. Guan WJ, Zhong NS. Strategies for reopening in the forthcoming COVID-19 era in China. Natl Sci Rev. (2022) 9:nwac054. doi: 10.1093/nsr/nwac054
18. The Central Commission for Discipline Inspection of the Communist Party of China. The introduction of new ten optimization measures to better adapt to the new situation of epidemic prevention and control and the new characteristics of the virus. (2022). Available online at: https://www.ccdi.gov.cn/yaowenn/202212/t20221208_235499.html (accessed January 20, 2023).
20. Dai M, Liu D, Liu M, Zhou F, Li G, Chen Z, et al. Patients with cancer appear more vulnerable to SARS-CoV-2: A multicenter study during the COVID-19 outbreak. Cancer Discov. (2020) 10:783–91. doi: 10.1158/2159-8290.CD-20-0422
21. Yang K, Sheng Y, Huang C, Jin Y, Xiong N, Jiang K, et al. Clinical characteristics, outcomes, and risk factors for mortality in patients with cancer and COVID-19 in Hubei, China: A multicentre, retrospective, cohort study. Lancet Oncol. (2020) 21:904–13. doi: 10.1016/S1470-2045(20)30310-7
22. Tian J, Yuan X, Xiao J, Zhong Q, Yang C, Liu B, et al. Clinical characteristics and risk factors associated with COVID-19 disease severity in patients with cancer in Wuhan, China: A multicentre, retrospective, cohort study. Lancet Oncol. (2020) 21:893–903. doi: 10.1016/S1470-2045(20)30309-0
23. Zhou Y, Yang Q, Ye J, Wu X, Hou X, Feng Y, et al. Clinical features and death risk factors in COVID-19 patients with cancer: A retrospective study. BMC Infect Dis. (2021) 21:760. doi: 10.1186/s12879-021-06495-9
24. Lee M, Quinn R, Pradhan K, Fedorov K, Levitz D, Fromowitz A, et al. Impact of COVID-19 on case fatality rate of patients with cancer during the omicron wave. Cancer Cell. (2022) 40:343–5. doi: 10.1016/j.ccell.2022.02.012
25. Sun P, Yang H, Zhao B, Wang Y, Nie M, Huang K, et al. Outcomes of COVID-19 in patients with lymphomas participating in registered clinical trials: A real-world study from China in the omicron outbreak era. Cancer Med. (2023) 12:21148–58. doi: 10.1002/cam4.6678
26. Naimi A, Yashmi I, Jebeleh R, Imani Mofrad M, Azimian Abhar S, Jannesar Y, et al. Comorbidities and mortality rate in COVID-19 patients with hematological malignancies: A systematic review and meta-analysis. J Clin Lab Anal. (2022) 36:e24387. doi: 10.1002/jcla.24387
27. Cao B, Jing X, Liu Y, Wen R, Wang C. Comparison of laboratory parameters in mild vs. severe cases and died vs. survived patients with COVID-19: Systematic review and meta-analysis. J Thorac Dis. (2022) 14:1478–87. doi: 10.21037/jtd-22-345
28. Fu Y, Zhao J, Wei X, Han P, Yang L, Ren T, et al. Effectiveness and cost-effectiveness of inactivated vaccine to address COVID-19 pandemic in China: Evidence from randomized control trials and real-world studies. Front Public Health. (2022) 10:917732. doi: 10.3389/fpubh.2022.917732
29. McMenamin ME, Nealon J, Lin Y, Wong JY, Cheung JK, Lau EHY, et al. Vaccine effectiveness of one, two, and three doses of BNT162b2 and CoronaVac against COVID-19 in Hong Kong: A population-based observational study. Lancet Infect Dis. (2022) 22:1435–43. doi: 10.1016/S1473-3099(22)00345-0
30. Ma C, Sun W, Tang T, Jia M, Liu Y, Wan Y, et al. Effectiveness of adenovirus type 5 vectored and inactivated COVID-19 vaccines against symptomatic COVID-19, COVID-19 pneumonia, and severe COVID-19 caused by the B.1.617.2 (Delta) variant: Evidence from an outbreak in Yunnan, China, 2021. Vaccine. (2022) 40:2869–74. doi: 10.1016/j.vaccine.2022.03.067
31. Puhach O, Adea K, Hulo N, Sattonnet P, Genecand C, Iten A, et al. Infectious viral load in unvaccinated and vaccinated individuals infected with ancestral, delta or omicron SARS-CoV-2. Nat Med. (2022) 28:1491–500. doi: 10.1038/s41591-022-01816-0
32. Lauring AS, Tenforde MW, Chappell JD, Gaglani M, Ginde AA, McNeal T, et al. Clinical severity of, and effectiveness of mRNA vaccines against, covid-19 from omicron, delta, and alpha SARS-CoV-2 variants in the United States: Prospective observational study. BMJ. (2022) 376:e069761. doi: 10.1136/bmj-2021-069761
33. Tran S, Truong TH, Narendran A. Evaluation of COVID-19 vaccine response in patients with cancer: An interim analysis. Eur J Cancer. (2021) 159:259–74. doi: 10.1016/j.ejca.2021.10.013
34. Hu Z, Jin Z, Zhou M, Zhang C, Bao Y, Gao X, et al. CoronaVac and BBIBP-CorV vaccines against SARS-CoV-2 during predominant circulation of Omicron BA.5.2 and BF.7 in China, a retrospective cohort study. J Med Virol. (2023) 95:e29143. doi: 10.1002/jmv.29143
35. Yang Y, Gong X, Yang L, Li J, Zhang J, Wei L, et al. Regular and booster vaccination with inactivated vaccines enhance the neutralizing activity against omicron variant both in the breakthrough infections and vaccinees. J Infect. (2022) 84:579–613. doi: 10.1016/j.jinf.2022.01.004
36. Zeng QL, Lv YJ, Liu XJ, Jiang ZY, Huang S, Li WZ, et al. Clinical characteristics of omicron SARS-CoV-2 variant infection after non-mRNA-based vaccination in China. Front Microbiol. (2022) 13:901826. doi: 10.3389/fmicb.2022.901826
37. da Silva JL, de Souza BSW, de Albuquerque LZ, Aleixo SB, Resende GADS, de Oliveira DGB, et al. Factors influencing COVID-19 mortality among cancer patients: A Brazilian multi-institutional study. PLoS One. (2023) 18:e0295597. doi: 10.1371/journal.pone.0295597
38. Zyoud SH, Koni A, Al-Jabi SW, Amer R, Shakhshir M, Al Subu R, et al. Current global research landscape on COVID-19 and cancer: Bibliometric and visualization analysis. World J Clin Oncol. (2022) 13:835–47. doi: 10.5306/wjco.v13.i10.835
39. Castelo-Branco L, Tsourti Z, Gennatas S, Rogado J, Sekacheva M, Viñal D, et al. COVID-19 in patients with cancer: First report of the ESMO international, registry-based, cohort study (ESMO-CoCARE). ESMO Open. (2022) 7:100499. doi: 10.1016/j.esmoop.2022.100499
40. Liu Y, Zhu W, Wang Z, Yu J, Dong L, Li C, et al. Recent antitumor therapy does not increase Omicron COVID-19 severity in cancer patients: A two-center retrospective study in China. Front Oncol. (2023) 13:1284255. doi: 10.3389/fonc.2023.1284255
Keywords: COVID-19, Omicron, cancer, clinical characteristics, China
Citation: Liu L-L, Liao Y-W, Yu X-H, Rong L, Chen B-G, Chen G, Zeng G-K and Yang L-Y (2024) Clinical characteristics and prognostic factors of COVID-19 infection among cancer patients during the December 2022 – February 2023 Omicron variant outbreak. Front. Med. 11:1401439. doi: 10.3389/fmed.2024.1401439
Received: 15 March 2024; Accepted: 16 May 2024;
Published: 30 May 2024.
Edited by:
Sergio E. Rodriguez, Centers for Disease Control and Prevention (CDC), United StatesReviewed by:
Amin Talebi Bezmin Abadi, Tarbiat Modares University, IranCopyright © 2024 Liu, Liao, Yu, Rong, Chen, Chen, Zeng and Yang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Li-Ye Yang, eWFuZ2xlZXllZUBzaW5hLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.