
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Med. , 05 July 2024
Sec. Family Medicine and Primary Care
Volume 11 - 2024 | https://doi.org/10.3389/fmed.2024.1399145
This article is part of the Research Topic Updating Long COVID: Mechanisms, Risk Factors, and Treatment View all 21 articles
 Meritxell Carmona-Cervelló1†
Meritxell Carmona-Cervelló1† Brenda Biaani León-Gómez1†
Brenda Biaani León-Gómez1† Rosalia Dacosta-Aguayo1,2
Rosalia Dacosta-Aguayo1,2 Noemí Lamonja-Vicente1,3
Noemí Lamonja-Vicente1,3 Pilar Montero-Alía1,4Gemma Molist1,5
Pilar Montero-Alía1,4Gemma Molist1,5 Aitana Ayet1Carla Chacón1,3Anna Costa-Garrido1Victor M. López-Lifante1,4,6,7Valeria Zamora-Putin1,6
Aitana Ayet1Carla Chacón1,3Anna Costa-Garrido1Victor M. López-Lifante1,4,6,7Valeria Zamora-Putin1,6 Liudmila Liutsko1Rosa García-Sierra1,4,8
Liudmila Liutsko1Rosa García-Sierra1,4,8 Antònia Fornés1
Antònia Fornés1 Eduard Moreno-Gabriel1,4,9
Eduard Moreno-Gabriel1,4,9 Marta Massanella10,11,12
Marta Massanella10,11,12 Jose A. Muñoz-Moreno13,14M. Carmen Rodríguez-Pérez1,4Lourdes Mateu2,11,12,13Anna Prats13
Jose A. Muñoz-Moreno13,14M. Carmen Rodríguez-Pérez1,4Lourdes Mateu2,11,12,13Anna Prats13 Maria Mataró15,16,17Marc Boigues18,19,20
Maria Mataró15,16,17Marc Boigues18,19,20 Bibiana Quirant18,19,20
Bibiana Quirant18,19,20 Julia G. Prado2,10,11
Julia G. Prado2,10,11 Eva Martínez-Cáceres2,18,19
Eva Martínez-Cáceres2,18,19 Concepción Violán1,2,3,7,21*
Concepción Violán1,2,3,7,21* Pere Torán-Monserrat1,2,4,22*
Pere Torán-Monserrat1,2,4,22*  the APC Collaborative Group
the APC Collaborative GroupBackground: The neurological symptoms of Long COVID (LC) and the impact of neuropsychological manifestations on people’s daily lives have been extensively described. Although a large body of literature describes symptoms, validating this with objective measures is important. This study aims to identify and describe the effects of Long COVID on cognition, balance, and the retinal fundus, and determine whether the duration of symptoms influences cognitive impairment.
Methods: This cross-sectional study involved LC volunteers with cognitive complaint from public health centers in northern Barcelona who participated between January 2022 and March 2023. This study collected sociodemographic characteristics, information on substance use, comorbidities, and clinical data related to COVID-19. We measured five cognitive domains using a battery of neuropsychological tests. Balance was assessed through posturography and retinal vascular involvement by retinography.
Results: A total of 166 people with LC and cognitive complaints participated, 80.72% were women and mean age was 49.28 ± 8.39 years. The most common self-reported symptoms were concentration and memory deficit (98.80%), brain fog (82.53%) and insomnia (71.17%). The 68.67% presented cognitive deficit in at least one domain, with executive functions being the most frequent (43.98%). The 51.52% of the participants exhibited a dysfunctional pattern in balance, and 9.2% showed some alteration in the retina. There were no statistically significant differences between cognitive impairment and symptom duration.
Conclusion: Our findings contribute to a more comprehensive understanding of the pathology associated with Long COVID. They highlight the diversity of self-reported symptoms, the presence of abnormal balance patterns, and some cognitive impairment. These findings underscore the necessity of addressing the clinical management of this condition in primary care through follow-up and the pursuit of multidisciplinary and comprehensive treatment.
Most people who became infected with COVID-19 recovered completely, but approximately 3 to 30% might experience a variety of medium-term to long-term effects after the initial illness (1–3). Post COVID-19 condition, also known as Long COVID (LC), it described by the World Health Organization (WHO) as the persistence or emergence of symptoms 3 months after SARS-CoV-2 infection that persist for at least2 months and cannot be explained by an alternative diagnosis (4). LC can affect anyone exposed to the SARS-CoV-2 virus, regardless of the clinical spectrum of the acute illness or age (5).
Some studies posit that SARS-CoV-2 infection may result in endothelial damage through a pro-inflamatory cytokine storm, oxidative stress, coagulation imbalance, and immune cell response, ultimately leading to chronic low-grade inflammation (6, 7). This can caused a non-specific systemic constellation of persistent symptoms involving different organ systems, including neurological, vascular, musculoskeletal, respiratory and others (8). Recent evidence suggest that the most frequent neuropsychological manifestations are fatigue, brain fog, cognitive decline, sleep disturbances, and anxiety (9, 10). Some symptoms may persist for years (11, 12), and it is unclear if they can be established for life (13). The characteristics significantly impact the individual work performance (14), psychosocial well-being and quality of life (15). In addition, it imposes a burden on the health system (16), economy, and social spheres.
Cognitive sequelae are among the most disabling neurological symptoms that affect a high proportion of people with LC. A meta-analysis of LC patients reported that about 32% suffered from brain fog, 28% had memory disturbances, and 22% had attentional difficulties (17). Many studies that evaluated cognition found widespread cognitive impairment (18, 19). Moreover, imaging studies revealed structural and functional changes associated with cognitive assessments scores due to SARS-CoV-2 infection in the brain (20, 21). Additional research effort are needed to understand neurocognitive function in LC by adopting domain-specific assessment tools.
People with LC often experience ontological/vestibular symptoms such as dizziness, vertigo, and tinnitus (22). It appears that the SARS-CoV-2 virus can affect the systems related to balance (23–25). However, current studies are based on subjective methods such as questionnaires or case reports. Alternative, posturographic tests are an objective assessment to measure balance alterations.
Considering the endothelial dysfunction hypothesis, several reports have shown signs of vascular disorders in different organ systems due to COVID-19. The virus can affect the endothelium through the angiotensin-converting enzyme 2 (26) and cause direct damage to the vascular endothelial cells, and it is possible to detect it in the retina. Therefore, retinal examination by retinography, a valuable tool for studying the clinical effects of COVID-19 in vivo.
The persistence and consequences of LC underscore the need to delineate the areas of involvement and associated factors to formulate enhancements in the therapeutic interventions for individuals with this condition. Therefore, it is important to understand how LC affects cognition, balance, and ocular health. This study examines the cognitive, balance and retinal outcomes and explores the relationship between the duration of LC symptoms and the degree of neurocognitive impairment.
This study is part of the Aliança ProHEpiC Cognitiu (APC) project, which aims to characterize the alterations in people with LC. More details regarding the project can be found in the published study protocol (27). This article presents the results of participants with LC and cognitive complaints.
The inclusion criteria were: (a) confirmed diagnosis of LC according to WHO criteria, (b) at least 12 weeks after infection (c) with cognitive complaints and (d) age between 18 and 70 years. The exclusion criteria were: (a) established diagnosis before COVID-19 infection of psychiatric, neurological, neurodevelopmental disorder pathologies known to cause cognitive deficits, (b) inability to perform neuropsychological examination due to literacy or sensory impairment, (c) history of illicit drug use, defined as habitual drug use (more than once a week) for at least 1 year or sporadic use (more than once a month) in the last 5 years, (d) alcohol abuse defined in accordance with the Spanish Ministry of Health risk consumption guidelines (28) (more than 20 gm/day in men or 10 gm/day in women) on a habitual basis for a period longer than 1 year, (e) medical conditions that limit participation and follow-up in the study (e.g., terminal illness).
Clinical and epidemiological characteristics were collected on two visits. During the baseline visit, participants provided sociodemographic information, anthropometric parameters, and vascular risk factors such as substance abuse and comorbidities, and were asked about their COVID-19 experience. Finally, all participants completed a comprehensive neuropsychological assessment. During the second visit, the balance capacity was measured using the posturography test, and eye fundus was explored using retinography (see Figure 1).

Figure 1. Diagram of the study design and the information collected at each visit.
Demographics such as sex (women, man), age labeled as (20–34, 35–44, 45–54, 55–70), educational level (primary, secondary, high School, university degree, specialist or master, doctorate) and job field (medical doctor, nurse, health services, health assistants and others) were collected.
Anthropometric and clinical baseline measures weight (kg), height (cm), body mass index (according to the WHO standards (29)), high blood pressure, high cholesterol, diabetes, tobacco and alcohol consumption and frequency (times per day) were collected.
Diagnosis of SARS-CoV-2 infection variables were collected as date and methods of diagnosis (polymerase chain reaction, rapid antigen test, serology, and symptoms), and severity of symptoms (asymptomatic, mild/moderate, admission to hospital, admission to intensive care unit).
LC symptoms self-reported and duration were collected, labeled as (a) non-cognitive neurological symptoms: migraine, cephalalgia, non-specific polyneuropathy, myopathy, neuralgia and neuritis, cutaneous sensitivity alteration, cutaneous paresthesia, other cutaneous sensitivities, non-specific cutaneous sensitivity, altered consciousness, vertigo and dizziness and non-specific insomnia; (b) cognitive neurological symptoms: nonspecific disorientation, retrograde amnesia, other amnesia, other cognitive, dyslexia and symbolic disturbances, brain fog and lack of concentration and memory; (c) no neurological symptoms: cardiologic, skin, digestive, general, ocular, otorhinolaryngology, pulmonary, rheumatic, urologic and hormonal (see Appendix 1).
We collected variables related to the treatment of LC symptoms, categorized in pharmacological (antidepressants, anxiolytics, others) or non-pharmacological (cognitive training, yoga, reiki, acupuncture, bach flowers, prescribed physical exercise, others).
All participants underwent a comprehensive neuropsychological battery conducted by a certified neuropsychologist. Five cognitive domains were evaluated: (a) executive functions (b) attention and processing speed, (c) memory, (d) visuospatial and visuoconstructive functions, and (e) language (see Table 1). The tests were selected based on expert consensus and considering the recommendations of the NeuroCOVID International Neuropsychology Taskforce (30). The participants’ raw test scores were standardized to Z-scores based on their age and years of education. The Z-scores range from −3 to 3, with 0 representing the mean. The Z-score indicate the extent to which a raw score deviates from the mean in standard deviation units.
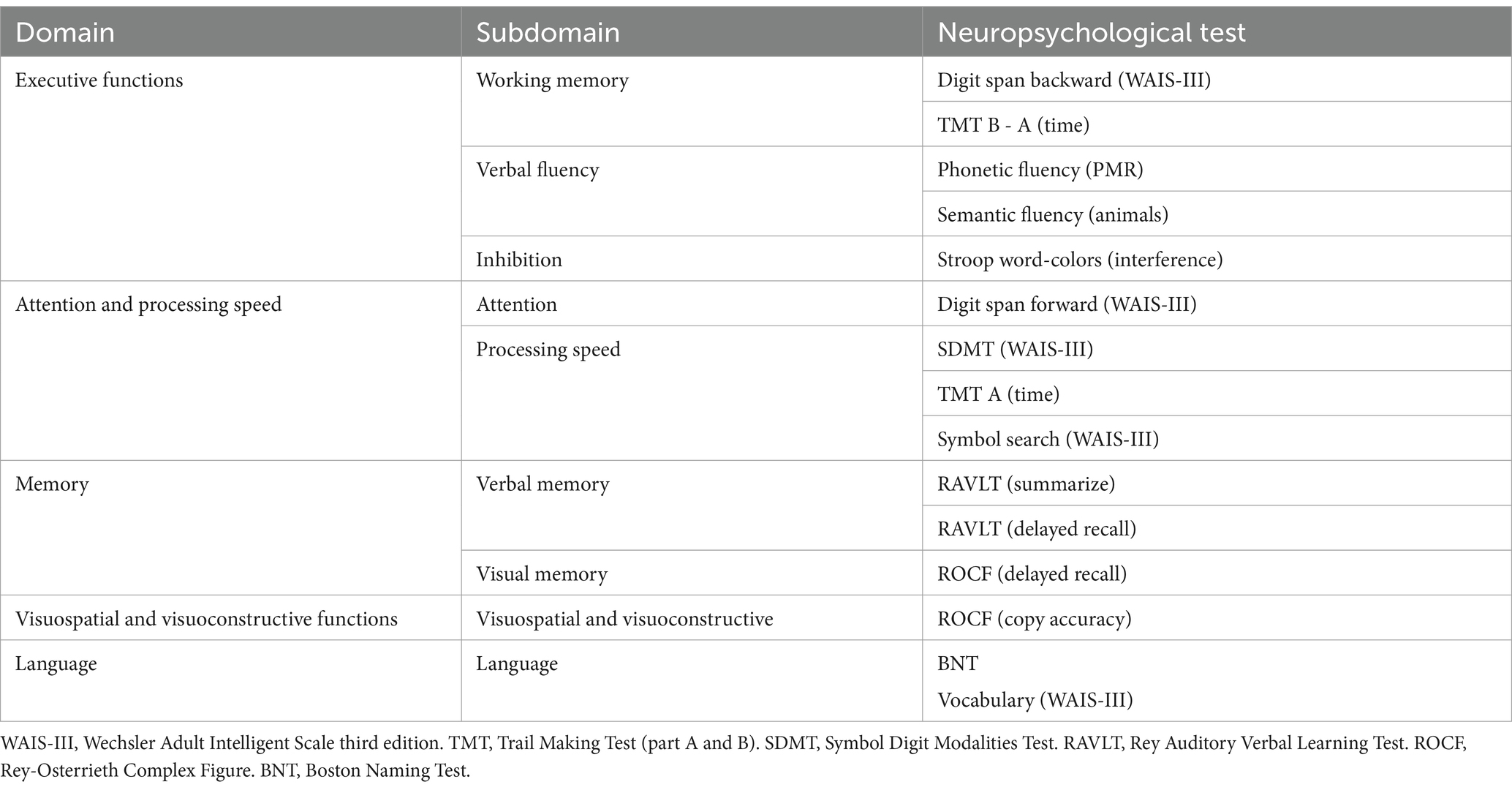
Table 1. Description of cognitive domains assessed and neuropsychological tests administered.
The tests used to evaluate the subdomains of executive functions were the time difference between parts B and A of the Trail Making Test (TMT) (31, 32) and the Digit Span Backward subtest from the Wechsler Adult Intelligent Scale (WAIS-III) (33) for the working memory. The verbal fluency was assessed by the number of words beginning with the letters P, M and R and the category “animals” (31, 34) recalled in one minute. The interference score of the Stroop test color-words was calculated as a measure of cognitive inhibitory control (35). The Digit Span Forward subtest (WAIS-III) was administered to measure attention (33). Visual scanning and motor speed were assessed by part A of the TMT (31, 32), Symbol Digit Modalities Test (SDMT) and Symbol Search from the WAIS-III (33). We used the Spanish version of Rey’s Auditory Verbal Test (RAVLT) (36) for verbal memory and visual memory was evaluated with the 30-min delayed recall test from the Rey-Osterrieth Complex Figure Test (ROCF) (31, 37). The copy accuracy of the ROCF was used to assess visuospatial and visuoconstructive abilities. The Spanish short version (15-items) of the Boston Naming Test (BNT) (38) and vocabulary subtest from the WAIS-III (33) were used to evaluate language.
For posturography, a dynamometric platform (Dinascan/IBVP600) was used to evaluate gait, gait speed and balance by a trained technician. The Romberg’s test (ROA, ROC, RGA, RGC) was used to evaluate postural control with more than two repetitions in each test. Each parameter expresses the percentage value of the variation with respect to the normality. Relation with different types of Romberg’s test automatically provided three indices (somatosensory, vestibular, and visual). The information from the indexes has been used to establish equilibrium patterns following an expert clinical consensus. For detailed information see Appendix 2.
To assess the eye fundus, a Topcon (TRC-NW8) with a non-mydriatic retinal camera was used by a trained technician to obtain entire central, nasal, and temporal retina images from both eyes. The images were anonymized and placed in the same position on the screen with a 16.2-megapixel resolution and a 45° field of view. High-quality control was applied to detect and eliminate images with poor resolution. A trained medical doctor conducted clinical image analysis manually; cases with detected abnormalities were referred to an ophthalmologist.
Categorical variables were described by each frequency and percentage. Continuous variables were described by mean, standard deviation and range. Descriptive analysis was used to characterize the sample sociodemographically and clinically. According to Frascati Criteria (39), an international consensus that has proved usefulness and reliability in another infection research field (40), we considered a cognitive deficit if one of the subtests was below −1.5 SD or if two subtests of the same cognitive domain were − 1 SD below the mean. Participants were classified as cognitively impaired if they had a deficit in at least two cognitive domains.
Subjects were classified into two groups according to the duration of the three symptoms previously defined: (a) 1st group (G1) = 1 to 25 months of symptomatology and (b) 2nd group (G2) = 26 to 36 months symptomatology. Post-hoc analysis was carried out to compare the basal characteristics of G1 and G2 groups. Normality distribution of the data was tested with a Shapiro–Wilk test prior to each analysis. Time differences in demographic characteristics were analyzed as follows: independent 2-sample t-tests for normally distributed continuous variables, Mann–Whitney U-test for non-normally distributed continuous variables, and chi-square tests for categorical variables. All tests were two-sided, and a statistical probability of p < 0.05 was considered significant. Statistical analyses were performed using STATA Statistical Software (version 15.0; Statistical software for data science).
A total of 182 participants were invited to participate in the study, 13 (7.14%) were excluded because they had a previous diagnosis associated with some type of cognitive impairment (attention deficit hyperactivity disorder, low intelligence quotient, previous stroke, language barrier and possibility of malingering) and three (1.64%) decided to abandon the study for different reasons (lack of availability and inability to contact).
Table 2 shows the sociodemographic characteristics of the 166 participants with LC and cognitive complaints included in the study. The 80.72% of the sample were women, with a median age of 49.28 years ±8.39 (range 25.5–69.8), and 39.76% had a job in the health services.
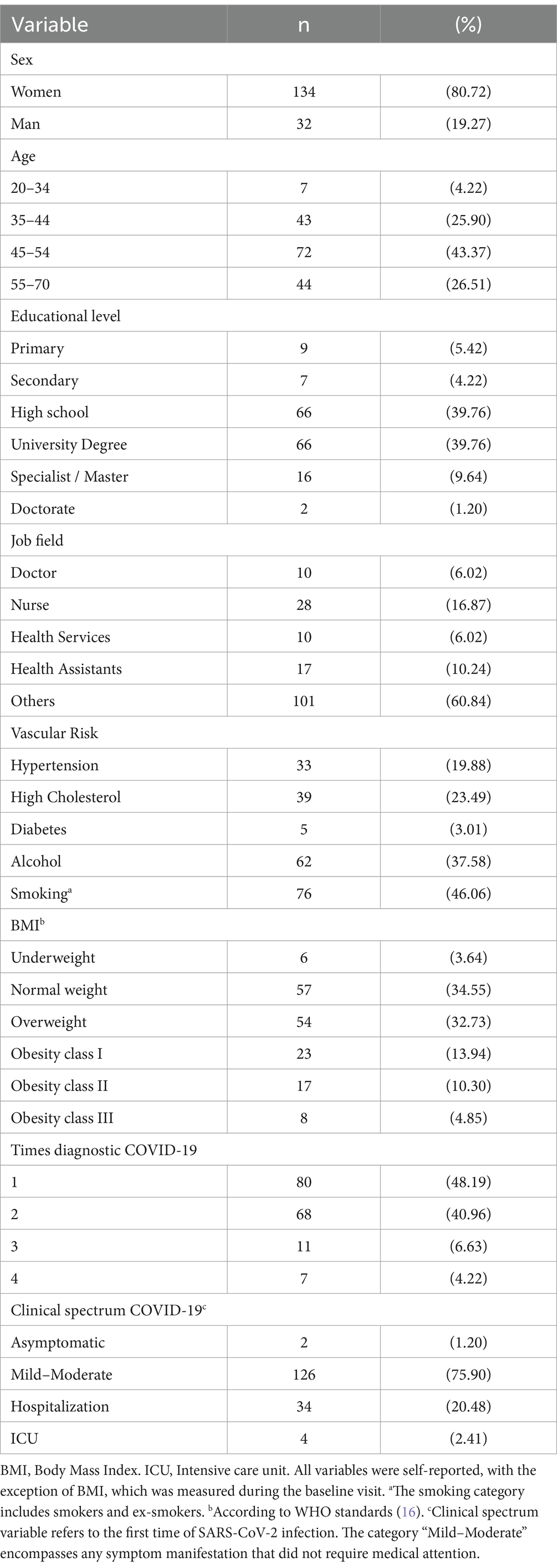
Table 2. Descriptive of the main characteristics of participants who present LC with cognitive complaints (n = 166).
Most participants (75.90%) had mild or moderate COVID-19 symptoms during their first infection, and more than half (51.81%) experienced reinfection. The most common neurological symptom reported was insomnia (71.17%), vertigo and dizziness (67.07%). All of them reported cognitive impairment, especially lack of concentration and memory (98.80%), followed by brain fog (82.53%). Almost the entirety of the sample exhibited some general symptoms, with asthenia being the most prevalent (42.11%) and musculoskeletal symptoms such as myalgia (70.12%). Some clinical variables had missing values: non-cognitive neurological symptoms (1.38%), cognitive neurological symptoms (1.03%), and no neurological symptoms (2.23%). Table 3 and Appendix 3 show the details of the symptoms reported by participants with LC.
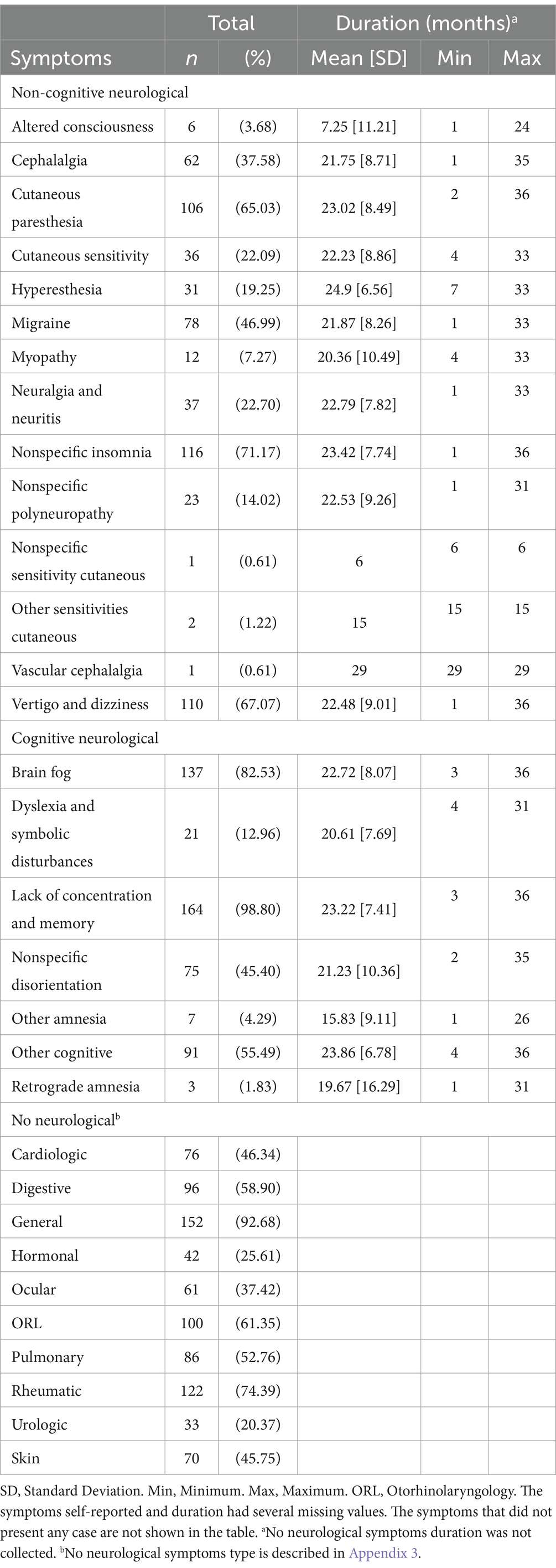
Table 3. Symptoms self-reported and months duration at the time of assessment (n = 166).
Using the Frascati criteria (39) to assess the neuropsychological test battery results, we found that 52 participants (31.33%) in the sample were classified as cognitively intact, while 114 (68.67%) had a cognitive deficit in at least one domain. A total of 31.93% presented cognitive impairment with two or more domains affected (Table 4). The most frequently impaired cognitive domain was executive function (43.98%), followed by attention and processing speed (36.75%), and memory (28.31%) (Table 5). No significant associations were identified between the descriptive variables and cognitive impairment.
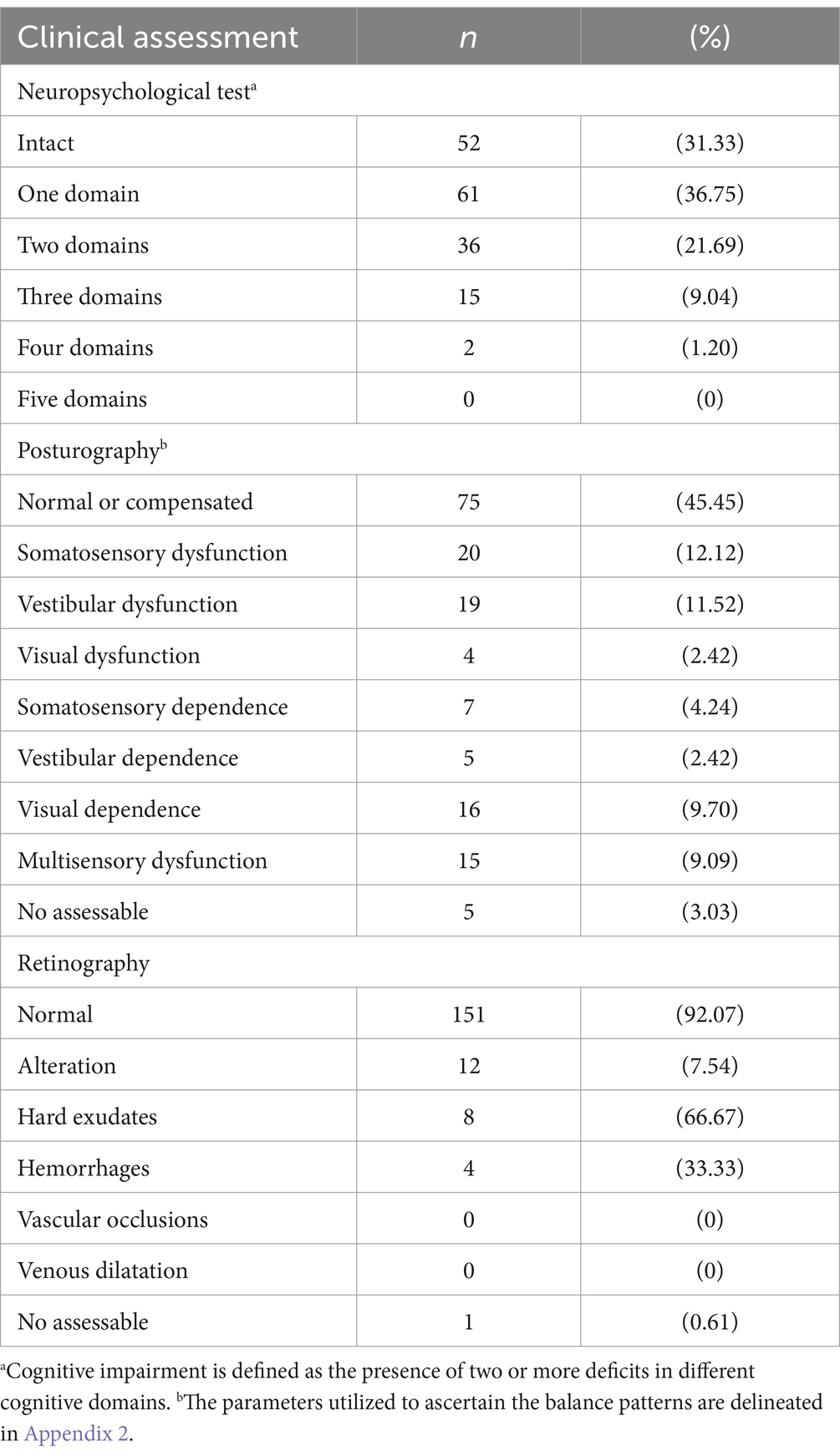
Table 4. Results of neuropsychological test, posturography, and retinography in people suffering from LC (n = 166).
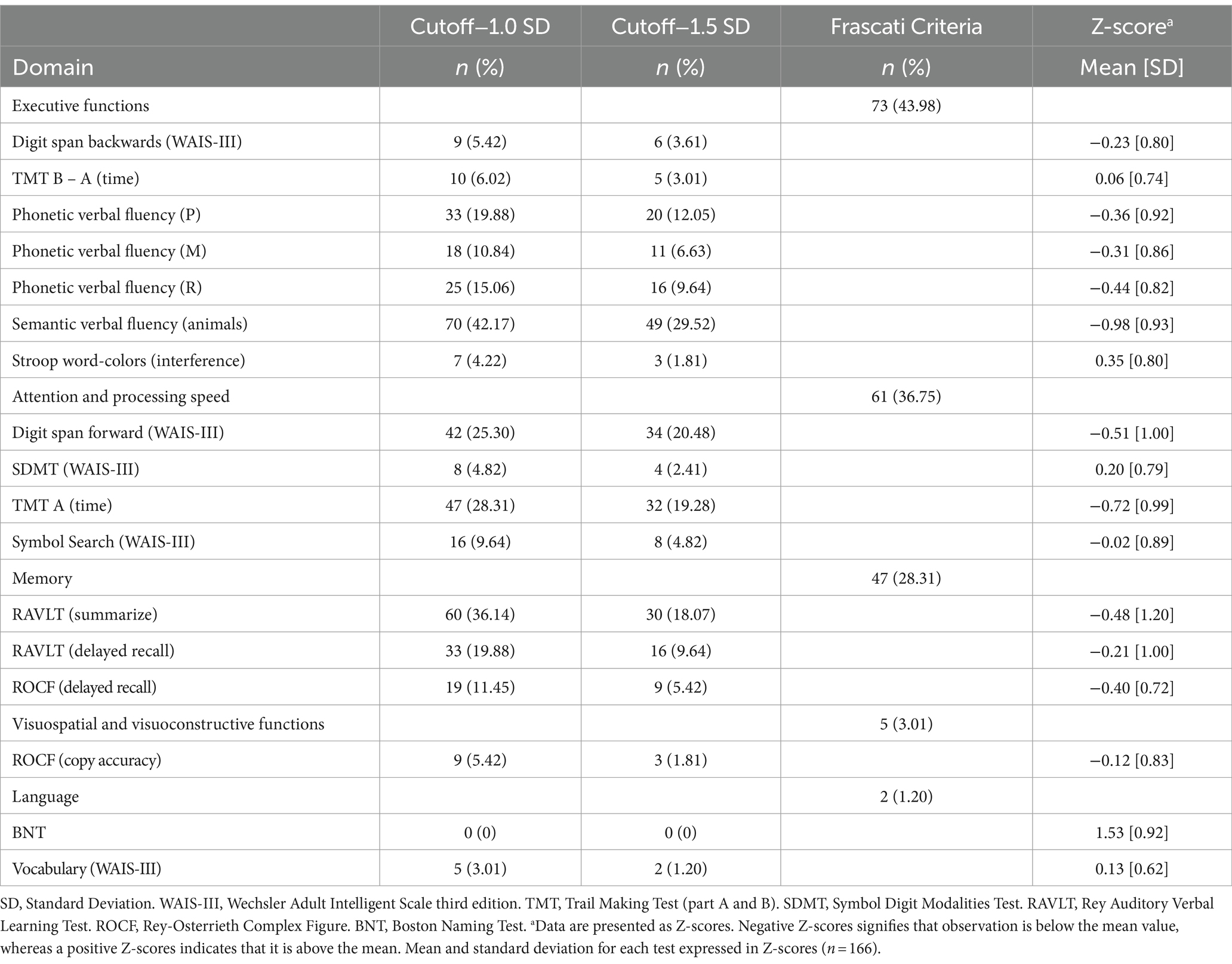
Table 5. Percentage for each test according to −1.0 SD and − 1.5 SD and Frascati Criteria.
The posturography test shows that 75 (45.45%) participants present a normal or compensated pattern. The more frequent patterns were somatosensory dysfunction (12.12%) and vestibular dysfunction (11.52%). Five people (3.03%) could not be evaluated because they were too exhausted to finish the test (Table 4). No significant associations were identified between the descriptive variables and balance patterns.
The 92.07% of individuals did not manifest any type of alteration in the retinography, 12 participants (7.54%) had visible affection in the ocular fundus (Table 4). The alteration found in at least one of the eyes was hard exudates (4.88%) and hemorrhages (2.44%). No significant associations were identified between the descriptive variables and retinal alterations.
Subjects were divided into two groups (G1 and G2) according to the duration of the most predominant cognitive symptoms reported: (a) lack of Concentration and Memory (C&M), (b) Brain Fog (BF) and (c) Nonspecific Disorientation (ND). There were no significant differences in demographic, anthropometric and clinical variables between these groups (see Appendix 4). Figure 2 shows the frequency of cognitive domain deficit by symptom duration. In the executive function domain, the group with a shorter duration of the three symptoms had better scores, with only the ND symptom showing a statistically significant difference (G1 = 37.50% vs. G2 = 61.76%, p = 0.037). There were no significant differences between the groups in terms of the remaining symptoms and domains.
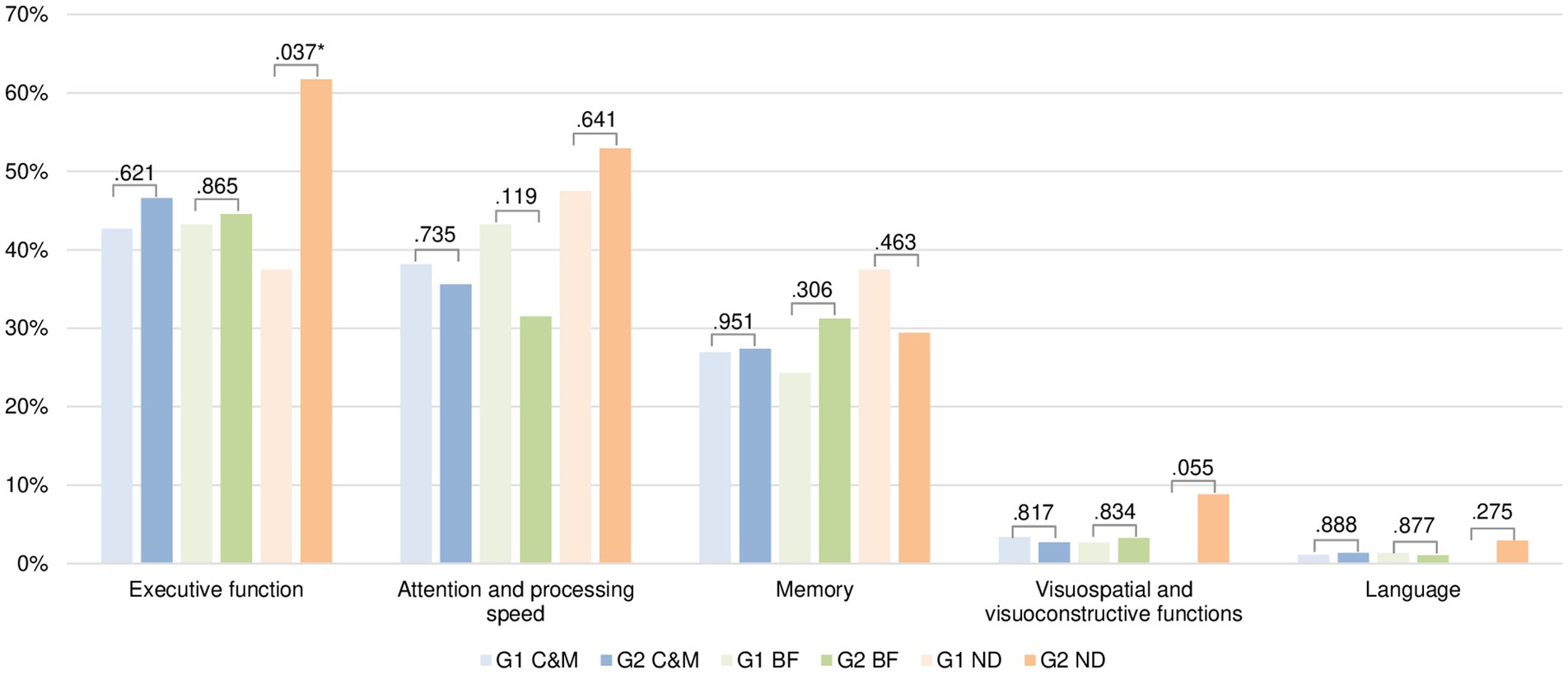
Figure 2. Differences between duration of cognitive symptoms self-reported (lack of concentration and memory, brain fog and nonspecific disorientation) and cognitive deficit by domain (n = 166).C&M, lack of Concentration and Memory. BF, Brain Fog. ND, Nonspecific Disorientation. Note: Symptom duration was divided into two groups: G1 (1 to 25 months) and G2 (26 to 36 months). The Figure shows the p-value of Chi-square analysis. We selected the most prevalent cognitive symptoms in our sample excluding the “Other cognitive symptoms” because it grouped more than one symptom.
In the APC cohort of people with LC and cognitive complaints, the three most common self-reported symptoms were concentration and memory deficit, asthenia, fatigue. More than 60% presented a cognitive deficit in at least one domain, being the executive functions the most impaired. Additionally, more than half of the participants presented a dysfunctional pattern in balance; and the 9% presented a fundus retina alteration.
The demographic profile of our cohort study is similar to other studies (1, 41). According to several studies, women are more susceptible to developing LC (42, 43). Some papers propose that this may be due to a different expression of angiotensin-converting enzyme 2 (ACE-2) or transmembrane protease serine 2 (TMPRSS2) receptors, or to lower production of proinflammatory cytokines such as interleukin-6 (IL-6) in women after a viral infection (44, 45). The greater frequency of women’s participation in health-related studies may be attributed to various factors, including their tendency to care more for their health. Most people in our study had a mild or moderate clinical course of SARS-CoV-2 infection. Thus, the data from our study corroborate previous research that the morbidity associated with prolonged COVID-19 is not related to the severity of the initial infection (5, 46, 47). In our sample, the most predominant complaints were lack of concentration and memory, asthenia, fatigue, brain fog, insomnia, myalgia, vertigo and dizziness. These findings are consistent with the current literature (48, 49). It is important to consider that high percentage of health professionals in our cohort could be influence a higher detection and reporting of symptoms.
Our results show that many patients in the sample demonstrated cognitive deficits in at least one domain. This overall result supports subjective cognitive complaints with objective neuropsychological measurements. Several articles assess cognitive functioning in people with LC, and most point to lower functioning compared to healthy subjects (17, 19, 50). In our study, patients showed impairments in several cognitive domains, including executive functions, attention, speed processing, and memory. These findings are in line with recent reviews (8, 49, 51). Linguistic and visuospatial abilities appear to be more preserved, whereas memory, executive function and attention seem to be the most affected capacities in these patients (52–54). This may be because attention, memory, and executive functions are high-level cognitive processes that integrate multiple brain regions. In contrast, language and visuospatial skills are more specific modular functions that are localized to specific brain areas. Considering that, COVID-19 affects the central nervous system (CNS), several hypotheses that try to explain the cognitive impairment. The immune response induced by the SARS-CoV-2 infection resulted in inflammation of CNS through systemic chemokines and other possible mechanisms (55). Persistent elevation of cytokines, chemokines and reactive microglia in cerebrospinal fluid can dysregulate multiple neural cell types. Such as altering homeostasis and plasticity (56), impairing neurogenesis (57) and inducing neurotoxic reactivity (58), all of which can affect neural circuit function and thus cognition (59).
To our knowledge, this is the first study to examine differences in cognitive impairment in relation to the duration of cognitive symptoms such as lack of concentration and memory, brain fog, and non-specific disorientation. It should be noted that most of the comparisons were not significant, making it difficult to draw conclusions. In the domain of executive functions, it seems that more time with the symptoms (lack of concentration and memory, brain fog and non-specific disorientation) is related to greater deficits. Nevertheless, there is some dispersion in the results for the other domains. This may be because it behaves differently depending on each symptom and cognitive domain. These discrepancies may also be caused by the intervention of other factors that have not been considered, such as comorbidities, severity of LC symptoms, and cognitive reserve. Thus, the results are inconclusive; therefore, we cannot assume that the persistence of symptomatology affects the progression of cognitive deficits. According to the PHOSP-COVID research group (60), a small improvement was found at 1 year, indicating that part of this deficit was not pre-existing and is potentially modifiable; however, some persisted after 1 year in susceptible individuals. In contrast, other studies showed a lower rate of improvement after 2 years of follow-up (61).
Results of the posturography test showed a wide variety of patterns in our sample, with the most predominant being somatosensory and vestibular dysfunction. These results cannot be strictly attributed to LC due to limited evidence in the literature. Even so, Yilmaz et al. (62) proved that balance in patients undergoing COVID-19 was impaired compared to healthy individuals. The mechanisms for reduced postural control remain unclear. It is not known whether the virus causes dysfunction of the vestibular system or whether such dysfunction is the result of an infectious process within the neural structures (25). Our findings suggest that the dysfunction is not due to a specific system; but is a more generalized affectation in the different systems involved in balance. The results obtained in the study by Gervasoni et al. (63) suggest the LC balance test performances were away from normality when integrating vision, somatosensory and vestibular information. It is therefore postulated that the alterations induced by SARS-CoV-2 infection result in a failure to integrate the various sensory inputs. Nevertheless, more specific complementary tests, such as nerve conduction, nuclear resonance, sensory, and organizational tests, are required to corroborate this hypothesis.
Retinal vascular involvement following SARS-CoV-2 infection has been little studied. Nevertheless, some studies indicate that SARS-CoV-2 infection causes retinal manifestations. Vavvas et al. (64) reported that the diameter of arteries and vessels in the retina was larger in patients with COVID-19 than in healthy individuals. This could be because when the inflammatory response begins, blood supply increases and vasodilation occurs (65). Some of the fundus findings in people with recent COVID-19 infection included retinitis patches, hard exudates, cotton wool spots, and superficial hemorrhages (66, 67). In a longitudinal study conducted by Invernizzi et al. (68), they found that most of the retinal vasculature alterations regress with time after acute COVID-19. However, those who suffer from severe COVID-19 may have long-lasting retinal vessel dilation persisting. In absence of previous information, we cannot be sure that the retinal lesions are due to SARS-CoV-2. There are also no studies on the prevalence of retinal vascular lesions in the general population. Although some retinal damage has been reported in the literature, the percentage of retinal damage observed in our sample is low, suggesting that retinography may not be a sensitive instrument for detecting the type of lesions produced by SARS-CoV-2. Therefore, it may be more advisable to use other techniques such as optical coherence tomography (69).
The study’s strengths include extensive follow-up of a population with a newly established disease. Our study uses various infrequent assessments such as posturography and retinography, and extensive battery of neurocognitive tests adopting domain-specific assessment tools to provide comprehensive monitoring. Furthermore, we have endeavored to collect all the symptoms reviewed in the literature and their duration, which may aid in the delimitation of the clinical spectrum.
However, our study has several limitations. First, the limited sample size may make it difficult to find significant relationships in the data. Second, there may be a sampling bias considering that most volunteers may have wanted to participate in the study because they had considerable impairment. Third, it should be noted that the measurement of clinical symptoms depended on the participants’ recall accuracy. Lastly, the lack of a control group without LC makes it challenging to definitively attribute the observed effects to LC specifically. For this reason, future lines of research should include a control group in each clinical test. It would also be interesting to re-evaluate the same sample after some time to see the progression of the conditions.
This study describes retinal, balance and cognition status in individuals with LC and cognitive complaints. It provides a framework for addressing patient and family expectations regarding their anticipated health. It also provides a better understanding of the LC syndrome and facilitates awareness of the importance of clinical management in primary care. It is important to maintain and increase the sensitivity of the health system around this pathology, both at the level of health professionals and managers and the general population. Knowing the health status of these individuals can help healthcare professionals distinguish LC symptoms from pre-existing conditions, helping to formalize diagnosis and treatment. Considering that, the majority in our sample present a cognitive deficit, it is convenient to monitor the progression of cognitive deterioration. As well as implementing, a pattern of postural balance exercises as rehabilitation training for vestibular problems. From this perspective, the main objective of clinicians and researchers is to create interventions that promote cognitive stimulation and balance training. Also, that ophthalmologists or retina specialists make a proper diagnosis and, if necessary, implement a personalized treatment plan. In conclusion, it is important to follow up with these patients to control their affectations and to find an adequate multidisciplinary treatment that contemplates physical and psychological aspects.
The original contributions presented in the study are included in the article or the Supplementary material, further inquiries can be directed to the corresponding authors.
The ethics committee of the Foundation University Institute for Primary Health Care Research Jordi Gol I Gurina (IDIAPJGol) has approved the study protocol (ref. 21/220-P). This study adheres to guidelines established in the Declaration of Helsinki. All participants recruited were fully informed about study and signed informed consent to participate. They consented to use their collected data for research and agreed to the applicable regulations, privacy policies, and terms of use. Participant data has been anonymized according to a numerical coding system and stored securely in the REDCap database.
MC-C: Formal analysis, Writing – original draft, Writing – review & editing, Data curation, Validation, Visualization. BL-G: Data curation, Formal analysis, Writing – original draft, Writing – review & editing, Validation, Visualization. RD-A: Writing – review & editing, Investigation, Visualization. NL-V: Writing – review & editing, Investigation, Funding acquisition, Resources, Visualization. PM-A: Writing – review & editing, Investigation, Visualization. GM: Formal analysis, Visualization, Writing – review & editing, Data curation. AA: Writing – review & editing, Investigation, Visualization. CC: Writing – review & editing, Investigation, Funding acquisition, Resources, Visualization. AC-G: Formal analysis, Writing – review & editing, Data curation, Visualization. VL-L: Writing – review & editing, Investigation, Visualization. VZ-P: Writing – review & editing, Investigation, Visualization. LL: Writing – review & editing, Methodology, Visualization. RG-S: Writing – review & editing, Methodology, Funding acquisition, Resources, Software, Visualization. AF: Writing – review & editing, Investigation, Visualization. EM-G: Writing – review & editing, Methodology, Visualization. MMas: Writing – review & editing, Funding acquisition, Project administration, Resources, Supervision, Visualization. JM-M: Writing – review & editing, Methodology, Visualization. MR-P: Writing – review & editing, Investigation, Visualization. LM: Writing – review & editing, Investigation, Funding acquisition, Resources, Visualization. AP: Writing – review & editing, Methodology, Visualization. MMat: Writing – review & editing, Methodology, Visualization. MB: Writing – review & editing, Investigation, Visualization. BQ: Writing – review & editing, Investigation, Visualization. JP: Supervision, Writing – review & editing, Funding acquisition, Project administration, Resources, Visualization. EM-C: Supervision, Writing – review & editing, Funding acquisition, Project administration, Resources, Visualization. CV: Conceptualization, Supervision, Writing – original draft, Writing – review & editing, Funding acquisition, Project administration, Resources, Visualization. PT-M: Conceptualization, Supervision, Writing – original draft, Writing – review & editing, Funding acquisition, Project administration, Resources, Visualization.
Aitana Ayet, Sandra Banderas, Laia Bernard, Jofre Bielsa-Pascual, Marc Boigues, Meritxell Carmona-Cervelló, Lucía A. Carrasco-Ribelles, Carla Chacón, Anna Costa-Garrido, Galadriel Diez Fadrique, Rosalía Dacosta-Aguayo, Antònia Fornés, Rosa García-Sierra, Eulàlia Grau, Noemí Lamonja-Vicente, Brenda B. León-Gómez, Liudmila Liutsko, Gemma Lladós, Cristina López, Víctor M. López-Lifante, Cora Loste, Marta Massanella, Maria Mataró, Lourdes Mateu, Eva Martínez-Cáceres, Gemma Molist, Pilar Montero-Alía, Eduard Moreno-Gabriel, Francisco Muñoz-López, Jose A. Muñoz-Moreno, Maria Nevot, Alba Pachón, Ruth Peña, Raul Pérez-Caballero, Julia G. Prado, Anna Prats, Josep Puig, Bibiana Quirant, Gabriel F. Rodriguez-Lozano, M. Carmen Rodríguez-Pérez, Sandra Sánchez-Vallespín, Jose Ramón Santos, Pere Torán-Monserrat, Macedonia Trigueros, Concepció Violán, and Valeria Zamora-Putin.
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This research was funded by grant number SLT0020/6_14 and in the call for grants corresponding to the year 2021 of the Strategic Plan for Research and Innovation in Health (PERIS) 2016–2020, category Research projects oriented to primary care, with file code SLT0021/000055 of Departament de Salut, Generalitat de Catalunya. Besides, MMat is supported by ICREA Academia program.
This project would not have been possible without the generous contribution and effort of the participants. The authors also express their gratitude to the Management Department, Primary Care Directorate, and the Directorate of the Clinical Laboratory of Metropolitan North for providing the necessary resources and support for the project.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2024.1399145/full#supplementary-material
1. Ballering, AV, van Zon, SKR, Olde Hartman, TC, and Rosmalen, JGMLifelines Corona Research Initiative. Persistence of somatic symptoms after COVID-19 in the Netherlands: an observational cohort study. Lancet. (2022) 400:452–61. doi: 10.1016/S0140-6736(22)01214-4
2. Perlis, RH, Santillana, M, Ognyanova, K, Safarpour, A, Lunz Trujillo, K, Simonson, MD, et al. Prevalence and correlates of long COVID symptoms among US adults. JAMA Netw Open. (2022) 5:E2238804. doi: 10.1001/jamanetworkopen.2022.38804
3. Bowe, B, Xie, Y, and Al-Aly, Z. Postacute sequelae of COVID-19 at 2 years. Nat Med. (2023) 29:2347–57. doi: 10.1038/s41591-023-02521-2
4. World Health Organization. A clinical case definition of post COVID-19 condition by a Delphi consensus. (2021). Available at: https://www.who.int/publications/i/item/WHO-2019-nCoV-Post_COVID-19_condition-Clinical_case_definition-2021.1 (Accessed October 26, 2022).
5. FAIR Health. Patients diagnosed with post-COVID conditions. An analysis of private healthcare claims using the official ICD-10 diagnostic code. Radiological Society of North America Inc. Diagnosed with Post-COVID Conditions - A FAIR Health White Paper. (2022). Available at: https://s3.amazonaws.com/media2.fairhealth.org/whitepaper/asset/Patients (Accessed June 10, 2023).
6. Charfeddine, S, Ibn Hadj Amor, H, Jdidi, J, Torjmen, S, Kraiem, S, Hammami, R, et al. Long COVID 19 syndrome: is it related to microcirculation and endothelial dysfunction? Insights from TUN-EndCOV study. Front Cardiovasc Med. (2021) 8:1–8. doi: 10.3389/fcvm.2021.745758
7. Poyatos, P, Luque, N, Sabater, G, Eizaguirre, S, Bonnin, M, Orriols, R, et al. Endothelial dysfunction and cardiovascular risk in post-COVID-19 patients after 6- and 12-months SARS-CoV-2 infection. Infection. (2024). doi: 10.1007/s15010-024-02173-5
8. Kubota, T, Kuroda, N, and Sone, D. Neuropsychiatric aspects of long COVID: a comprehensive review. Psychiatry Clin Neurosci. (2023) 77:84–93. doi: 10.1111/pcn.13508
9. Premraj, L, Kannapadi, NV, Briggs, J, Seal, SM, Battaglini, D, Fanning, J, et al. Mid and long-term neurological and neuropsychiatric manifestations of post-COVID-19 syndrome: a meta-analysis. J Neurol Sci. (2022) 434:120162. doi: 10.1016/j.jns.2022.120162
10. Subramanian, A, Nirantharakumar, K, Hughes, S, Myles, P, Williams, T, Gokhale, KM, et al. Symptoms and risk factors for long COVID in non-hospitalized adults. Nat Med. (2022) 28:1706–14. doi: 10.1038/s41591-022-01909-w
11. Demko, ZO, Yu, T, Mullapudi, SK, Varela Heslin, MG, Dorsey, CA, Payton, CB, et al. Post-acute sequelae of SARS-CoV-2 (PASC) impact quality of life at 6, 12 and 18 months post-infection. medRxiv. (2022) 2022:22278543. doi: 10.1101/2022.08.08.22278543
12. Han, Q, Zheng, B, Daines, L, and Sheikh, A. Long-term sequelae of COVID-19: a systematic review and Meta-analysis of one-year follow-up studies on post-COVID symptoms. Pathogens. (2022) 11:269. doi: 10.3390/pathogens11020269
13. Hartung, TJ, Bahmer, T, Chaplinskaya-Sobol, I, Deckert, J, Endres, M, Franzpötter, K, et al. Predictors of non-recovery from fatigue and cognitive deficits after COVID-19: a prospective, longitudinal, population-based study. eClinicalMedicine. (2024) 69:102456. doi: 10.1016/j.eclinm.2024.102456
14. Davis, HE, Assaf, GS, McCorkell, L, Wei, H, Low, RJ, Re’em, Y, et al. Characterizing long COVID in an international cohort: 7 months of symptoms and their impact. eClinicalMedicine. (2021) 38:101019. doi: 10.1016/J.ECLINM.2021.101019
15. Chatys-Bogacka, Z, Mazurkiewicz, I, Slowik, J, Bociaga-Jasik, M, Dzieza-Grudnik, A, Slowik, A, et al. Brain fog and quality of life at work in non-hospitalized patients after COVID-19. Int J Environ Res Public Health. (2022) 19:12816. doi: 10.3390/ijerph191912816
16. Menges, D, Ballouz, T, Anagnostopoulos, A, Aschmann, HE, Domenghino, A, Fehr, JS, et al. Burden of post-COVID-19 syndrome and implications for healthcare service planning: a population-based cohort study. PLoS One. (2021) 16:e0254523–19. doi: 10.1371/journal.pone.0254523
17. Ceban, F, Ling, S, Lui, LMW, Lee, Y, Gill, H, Teopiz, KM, et al. Fatigue and cognitive impairment in post-COVID-19 syndrome: a systematic review and meta-analysis. Brain Behav Immun. (2022) 101:93–135. doi: 10.1016/j.bbi.2021.12.020
18. Herrera, E, Pérez-Sánchez, MC, San Miguel-Abella, R, Barrenechea, A, Blanco, C, Solares, L, et al. Cognitive impairment in young adults with post COVID-19 syndrome. Sci Rep. (2023) 13:1–9:6378. doi: 10.1038/s41598-023-32939-0
19. Miskowiak, KW, Pedersen, JK, Gunnarsson, DV, Roikjer, TK, Podlekareva, D, Hansen, H, et al. Cognitive impairments among patients in a long-COVID clinic: prevalence, pattern and relation to illness severity, work function and quality of life. J Affect Disord. (2023) 324:162–9. doi: 10.1016/j.jad.2022.12.122
20. Douaud, G, Lee, S, Alfaro-Almagro, F, Arthofer, C, Wang, C, McCarthy, P, et al. SARS-CoV-2 is associated with changes in brain structure in UK biobank. Nature. (2022) 604:697–707. doi: 10.1038/s41586-022-04569-5
21. Díez-Cirarda, M, Yus, M, Gómez-Ruiz, N, Polidura, C, Gil-Martínez, L, Delgado-Alonso, C, et al. Multimodal neuroimaging in post-COVID syndrome and correlation with cognition. Brain. (2022) 146:2142–52. doi: 10.1093/brain/awac384
22. Degen, CV, Mikuteit, M, Niewolik, J, Schröder, D, Vahldiek, K, Mücke, U, et al. Self-reported tinnitus and Vertigo or dizziness in a cohort of adult long COVID patients. Front Neurol. (2022) 13:1–6. doi: 10.3389/fneur.2022.884002
23. Viola, P, Ralli, M, Pisani, D, Malanga, D, Sculco, D, Messina, L, et al. Tinnitus and equilibrium disorders in COVID-19 patients: preliminary results. Eur Arch Otorhinolaryngol. (2021) 278:3725–30. doi: 10.1007/s00405-020-06440-7
24. Özçelik Korkmaz, M, Eğilmez, OK, Özçelik, MA, and Güven, M. Otolaryngological manifestations of hospitalised patients with confirmed COVID-19 infection. Eur Arch Otorhinolaryngol. (2021) 278:1675–85. doi: 10.1007/s00405-020-06396-8
25. Dzięcioł-Anikiej, Z, Dakowicz, A, Dzięcioł, J, Kopko, S, Moskal-Jasińska, D, Gawlikowska-Sroka, A, et al. Balance disorders in people with history of COVID-19 in light of Posturographic tests. J Clin Med. (2023) 12:461. doi: 10.3390/jcm12134461
26. Hikmet, F, Méar, L, Edvinsson, Å, Micke, P, Uhlén, M, and Lindskog, C. The protein expression profile of ACE2 in human tissues. Mol Syst Biol. (2020) 16:e9610–6. doi: 10.15252/msb.20209610
27. Dacosta-Aguayo, R, Lamonja-Vicente, N, Chacon, C, Carrasco-Ribelles, LA, Montero-Alia, P, Costa-Garrido, A, et al. Neurocognitive profile of the post-COVID condition in adults in Catalonia-a mixed method prospective cohort and nested case-control study: study protocol. Vaccine. (2022) 10:849. doi: 10.3390/vaccines10060849
28. Ministerio de Sanidad. Límites de consumo de bajo riesgo de alcohol. Actualización del riesgo relacionado con los niveles de consumo de alcohol, el patrón de consumo y el tipo de bebida. (2020). Available at: https://www.sanidad.gob.es/areas/promocionPrevencion/alcohol/documentosTecnicos/docs/Limites_Consumo_Bajo_Riesgo_Alcohol_Actualizacion.pdf.
29. World Health Organization. A healthy lifestyle - WHO recommendations. (2010). Available at: https://www.who.int/europe/news-room/fact-sheets/item/a-healthy-lifestyle---who-recommendations (Accessed June 24, 2023).
30. Cysique, LA, Łojek, E, Cheung, TCK, Cullen, B, Egbert, AR, Evans, J, et al. Assessment of neurocognitive functions, olfaction, taste, mental, and psychosocial Health in COVID-19 in adults: recommendations for harmonization of research and implications for clinical practice. J Int Neuropsychol Soc. (2022) 28:642–60. doi: 10.1017/S1355617721000862
31. Peña-Casanova, J, Quiñones-Úbeda, S, Gramunt-Fombuena, N, Quintana-Aparicio, M, Aguilar, M, Badenes, D, et al. Spanish multicenter normative studies (NEURONORMA project): norms for verbal fluency tests. Arch Clin Neuropsychol. (2009) 24:395–411. doi: 10.1093/arclin/acp042
32. Tamayo, F, Casals-Coll, M, Sánchez-Benavides, G, Quintana, M, Manero, RM, Rognoni, T, et al. Estudios normativos españoles en población adulta joven (Proyecto NEURONORMA jóvenes): Normas para las pruebas span verbal, span visuoespacial, Letter-Number Sequencing, Trail Making Test y Symbol Digit Modalities Test. Neurologia. (2012) 27:319–29. doi: 10.1016/j.nrl.2011.12.020
33. Wechsler, D . WAIS-iii Escala de Inteligencia de Wechsler para Adultos. Madrid: TEA Ediciones (2001).
34. Casals-Coll, M, Sánchez-Benavides, G, Quintana, M, Manero, RM, Rognoni, T, Calvo, L, et al. Estudios normativos españoles en población adulta joven (proyecto NEURONORMA jóvenes): Normas para los test de fluencia verbal. Neurologia. (2013) 28:33–40. doi: 10.1016/j.nrl.2012.02.010
36. Schmidt, M . Rey auditory and verbal learning test: A handbook. Los Angeles, CA: Western Psychological Services (1996).
37. Palomo, R, Casals-Coll, M, Sánchez-Benavides, G, Quintana, M, Manero, RM, Rognoni, T, et al. Estudios normativos españoles en población adulta joven (proyecto NEURONORMA jóvenes): Normas para las pruebas Rey-Osterrieth Complex Figure (copia y memoria) y Free and Cued Selective Reminding Test. Neurologia. (2013) 28:226–35. doi: 10.1016/j.nrl.2012.03.008
38. Goodglass, H, Kaplan, E, and Barresi, B. Test de Boston para el Diagnóstico de la Afasia. 3rd ed. Madrid: Editorial Médica Panamericana (2001).
39. Gates, TM, and Cysique, LA. The chronicity of HIV infection should drive the research strategy of NeuroHIV treatment studies: a critical review. CNS Drugs. (2016) 30:53–69. doi: 10.1007/s40263-015-0302-7
40. Antinori, A, Arendt, G, Becker, JT, Brew, BJ, Byrd, DA, Cherner, M, et al. Updated research nosology for HIV-associated neurocognitive disorders. Neurology. (2007) 69:1789–99. doi: 10.1212/01.WNL.0000287431.88658.8b
41. Carvalho-Schneider, C, Laurent, E, Lemaignen, A, Beaufils, E, Bourbao-Tournois, C, Laribi, S, et al. Follow-up of adults with noncritical COVID-19 two months after symptom onset. Clin Microbiol Infect. (2021) 27:258–63. doi: 10.1016/j.cmi.2020.09.052
42. Sylvester, SV, Rusu, R, Chan, B, Bellows, M, O’Keefe, C, and Nicholson, S. Sex differences in sequelae from COVID-19 infection and in long COVID syndrome: a review. Curr Med Res Opin. (2022) 38:1391–9. doi: 10.1080/03007995.2022.2081454
43. Notarte, KI, de Oliveira, MHS, Peligro, PJ, Velasco, JV, Macaranas, I, Ver, AT, et al. Age, sex and previous comorbidities as risk factors not associated with SARS-CoV-2 infection for long COVID-19: a systematic review and Meta-analysis. J Clin Med. (2022) 11:314. doi: 10.3390/jcm11247314
44. Fernández-de-Las-Peñas, C, Martín-Guerrero, JD, Pellicer-Valero, ÓJ, Navarro-Pardo, E, Gómez-Mayordomo, V, Cuadrado, ML, et al. Female sex is a risk factor associated with long-term post-COVID related-symptoms but not with COVID-19 symptoms: the LONG-COVID-EXP-CM multicenter study. J Clin Med. (2022) 11:413. doi: 10.3390/jcm11020413
45. Torrell, G, Puente, D, Jacques-Aviñó, C, Carrasco-Ribelles, LA, Violán, C, López-Jimenéz, T, et al. Characterisation, symptom pattern and symptom clusters from a retrospective cohort of long COVID patients in primary care in Catalonia. BMC Infect Dis. (2024) 24:954. doi: 10.1186/s12879-023-08954-x
46. Vivaldi, G, Pfeffer, PE, Talaei, M, Basera, TJ, Shaheen, SO, and Martineau, AR. Long-term symptom profiles after COVID-19 vs other acute respiratory infections: an analysis of data from the COVIDENCE UK study. eClinicalMedicine. (2023) 65:102251. doi: 10.1016/j.eclinm.2023.102251
47. Davis, HE, McCorkell, L, Vogel, JM, and Topol, EJ. Long COVID: major findings, mechanisms and recommendations. Nat Rev Microbiol. (2023) 21:133–46. doi: 10.1038/s41579-022-00846-2
48. Pinzon, RT, Wijaya, VO, Al, JA, Nunsio, PN, and Buana, RB. Persistent neurological manifestations in long COVID-19 syndrome: a systematic review and meta-analysis. J Infect Public Health. (2022) 15:856–69. doi: 10.1016/j.jiph.2022.06.013
49. Reiss, AB, Greene, C, Dayaramani, C, Rauchman, SH, Stecker, MM, De Leon, J, et al. Long COVID, the brain, nerves, and cognitive function. Neurol Int. (2023) 15:821–41. doi: 10.3390/neurolint15030052
50. Li, Z, Zhang, Z, Zhang, Z, Wang, Z, and Li, H. Cognitive impairment after long COVID-19: current evidence and perspectives. Front Neurol. (2023) 14:182. doi: 10.3389/fneur.2023.1239182
51. Tavares-Júnior, JWL, de Souza, ACC, Borges, JWP, Oliveira, DN, Siqueira-Neto, JI, Sobreira-Neto, MA, et al. COVID-19 associated cognitive impairment: a systematic review. Cortex. (2022) 152:77–97. doi: 10.1016/j.cortex.2022.04.006
52. Delgado-alonso, C, Valles-salgado, M, Alvarez, AD, Yus, M, Gómez-Ruiz, N, Jorquera, M, et al. Cognitive dysfunction associated with COVID-19: a comprehensive neuropsychological study. J Psychiatr Res. (2022) 150:40–6. doi: 10.1016/j.jpsychires.2022.03.033
53. García-Sánchez, C, Calabria, M, Grunden, N, Pons, C, Arroyo, JA, Gómez-Anson, B, et al. Neuropsychological deficits in patients with cognitive complaints after COVID-19. Brain Behav. (2022) 12:1–11. doi: 10.1002/brb3.2508
54. Voruz, P, Allali, G, Benzakour, L, Nuber-Champier, A, Thomasson, M, Jacot de Alcântara, I, et al. Long COVID neuropsychological deficits after severe, moderate, or mild infection. Clin Transl Neurosci. (2022) 6:9. doi: 10.3390/ctn6020009
55. Fernández-Castañeda, A, Lu, P, Geraghty, AC, Song, E, Lee, MH, Wood, J, et al. Mild respiratory COVID can cause multi-lineage neural cell and myelin dysregulation. Cell. (2022) 185:2452–2468.e16. doi: 10.1016/j.cell.2022.06.008
56. Ribeiro, M, Brigas, HC, Temido-Ferreira, M, Pousinha, PA, Regen, T, Santa, C, et al. Meningeal γδ T cell-derived IL-17 controls synaptic plasticity and short-term memory. Sci Immunol. (2019) 4:5199. doi: 10.1126/sciimmunol.aay5199
57. Soung, AL, Vanderheiden, A, Nordvig, AS, Sissoko, CA, Canoll, P, Mariani, MB, et al. COVID-19 induces CNS cytokine expression and loss of hippocampal neurogenesis. Brain. (2022) 145:4193–201. doi: 10.1093/brain/awac270
58. Guttenplan, KA, Weigel, MK, Prakash, P, Wijewardhane, PR, Hasel, P, Rufen-Blanchette, U, et al. Neurotoxic reactive astrocytes induce cell death via saturated lipids. Nature. (2021) 599:102–7. doi: 10.1038/s41586-021-03960-y
59. Monje, M, and Iwasaki, A. The neurobiology of long COVID. Neuron. (2022) 110:3484–96. doi: 10.1016/j.neuron.2022.10.006
60. Evans, RA, Leavy, OC, Richardson, M, Elneima, O, McAuley, HJC, Shikotra, A, et al. Clinical characteristics with inflammation profiling of long COVID and association with 1-year recovery following hospitalisation in the UK: a prospective observational study. Lancet Respir Med. (2022) 10:761–75. doi: 10.1016/S2213-2600(22)00127-8
61. Mateu, L, Tebe, C, Loste, C, Santos, JR, Lladós, G, López, C, et al. Determinants of the onset and prognosis of the post-COVID-19 condition: a 2-year prospective observational cohort study. Lancet Reg Health Eur. (2023) 33:100724. doi: 10.1016/j.lanepe.2023.100724
62. Yılmaz, O, Mutlu, BÖ, Yaman, H, Bayazıt, D, Demirhan, H, and Bayazıt, YA. Assessment of balance after recovery from Covid-19 disease. Auris Nasus Larynx. (2022) 49:291–8. doi: 10.1016/j.anl.2021.08.011
63. Gervasoni, F, LoMauro, A, Ricci, V, Salce, G, Andreoli, A, Visconti, A, et al. Balance and visual reliance in post-COVID syndrome patients assessed with a robotic system: a multi-sensory integration deficit. Neurol Sci. (2022) 43:85–8. doi: 10.1007/s10072-021-05647-8
64. Vavvas, DG, Sarraf, D, Sadda, SVR, Eliott, D, Ehlers, JP, Waheed, NK, et al. Concerns about the interpretation of OCT and fundus findings in COVID-19 patients in recent lancet publication. Eye. (2020) 34:2153–4. doi: 10.1038/s41433-020-1084-9
65. Yusef, YN, Kazaryan, EE, Andzhelova, DV, and Vorobyova, MV. Ophthalmological manifestations of post-COVID-19 syndrome. Russ Ann Ophthalmol. (2021) 137:331–9. doi: 10.17116/oftalma2021137052331
66. Sen, S, Kannan, NB, Kumar, J, Rajan, RP, Kumar, K, Baliga, G, et al. Retinal manifestations in patients with SARS-CoV-2 infection and pathogenetic implications: a systematic review. Int Ophthalmol. (2022) 42:323–36. doi: 10.1007/s10792-021-01996-7
67. Ayachit, A, Joshi, M, Ayachit, G, Joshi, S, and Shah, P. Presumed post-COVID infection retinitis - clinical and tomographic features of retinitis as a post-COVID syndrome. Ocul Immunol Inflamm. (2023) 31:1117–21. doi: 10.1080/09273948.2022.2060264
68. Invernizzi, A, Schiuma, M, Parrulli, S, Torre, A, Zicarelli, F, Colombo, V, et al. Retinal vessels modifications in acute and post-COVID-19. Sci Rep. (2021) 11:19373. doi: 10.1038/s41598-021-98873-1
Keywords: long COVID, neurological symptoms, neuropsychological assessment, postural balance, retina fundus
Citation: Carmona-Cervelló M, León-Gómez BB, Dacosta-Aguayo R, Lamonja-Vicente N, Montero-Alía P, Molist G, Ayet A, Chacón C, Costa-Garrido A, López-Lifante VM, Zamora-Putin V, Liutsko L, García-Sierra R, Fornés A, Moreno-Gabriel E, Massanella M, Muñoz-Moreno JA, Rodríguez-Pérez MC, Mateu L, Prats A, Mataró M, Boigues M, Quirant B, Prado JG, Martínez-Cáceres E, Violán C and Torán-Monserrat P the APC Collaborative Group (2024) Long COVID: cognitive, balance, and retina manifestations. Front. Med. 11:1399145. doi: 10.3389/fmed.2024.1399145
Edited by:
César Fernández-de-las-Peñas, Rey Juan Carlos University, SpainReviewed by:
Tracy Fischer, Tulane University, United StatesCopyright © 2024 Carmona-Cervelló, León-Gómez, Dacosta-Aguayo, Lamonja-Vicente, Montero-Alía, Molist, Ayet, Chacón, Costa-Garrido, López-Lifante, Zamora-Putin, Liutsko, García-Sierra, Fornés, Moreno-Gabriel, Massanella, Muñoz-Moreno, Rodríguez-Pérez, Mateu, Prats, Mataró, Boigues, Quirant, Prado, Martínez-Cáceres, Violán, Torán-Monserrat and the APC Collaborative Group. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Concepción Violán, Y3Zpb2xhbmYubW4uaWNzQGdlbmNhdC5jYXQ=; Pere Torán-Monserrat, cHRvcmFuLmJubS5pY3NAZ2VuY2F0LmNhdA==
†These authors share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.