 Changdong Fei1†
Changdong Fei1† Yan Ma
Yan Ma Yupeng Liu
Yupeng Liu Renzheng Chen
Renzheng Chen
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Med. , 27 June 2024
Sec. Geriatric Medicine
Volume 11 - 2024 | https://doi.org/10.3389/fmed.2024.1393208
This article is part of the Research Topic Pharmacological Therapy in Patients with Arrhythmias View all 6 articles
Background: Patients with atrial fibrillation (AF) who undergo radiofrequency catheter ablation (RFCA) necessitate the administration of antiarrhythmic drugs to prevent early recurrence. The clinical outcomes among these patients may be influenced by varying antiarrhythmic regimens.
Objectives: To identify the risk factors associated with early recurrence and compare the clinical outcomes among different antiarrhythmic regimens in elderly patients with AF following radiofrequency catheter ablation (RFCA) during a 3-month period.
Methods: A retrospective observational study encompassed 420 elderly patients with AF following RFCA. Baseline data were collected during the initial postoperative visit and clinical outcomes were carefully monitored over a 3-month follow-up period. Logistic regression and Cox-proportional hazard regression analyses were performed to investigate the relationship between various antiarrhythmic regimens and the clinical outcomes.
Results: Multivariate logistic regression analysis revealed that age (p = 0.001), left atrial diameter (p < 0.001), left ventricular diameter (p = 0.015), reactive hyperemia index (RHI) (p < 0.001), antiarrhythmic drug (p < 0.001) and hs-cTnI (p = 0.017) were independent risk factors of early recurrence. Furthermore, in cox survival regression analysis model, survival rate of early recurrence in the amiodarone group was higher than in the propafenone group (HR 2.30, 95%CI 1.17–4.53, p = 0.016) and in the sotalol group (HR 3.60, 95%CI 2.17–5.95, p < 0.001). Compared to the amiodarone group, the incidence of liver dysfunction was lower in the dronedarone group (p = 0.046) and the propafenone group (p = 0.021). The incidence of bradyarrhythmia (p = 0.003), QT interval prolongation (p = 0.035) and atrioventricular transmission block (p = 0.021) were higher in the sotalol group than in the amiodarone group.
Conclusion: RHI was identified as an independent risk factor for early recurrence among elderly AF patients after RFCA. Compared to amiodarone, propafenone and sotalol exhibited an elevated risk of early recurrence. Although there was no significant difference in early recurrence between amiodarone and dronedarone, dronedarone emerged as the preferred option due to its lower frequency of adverse drug reactions than amiodarone.
Atrial fibrillation (AF) is the most prevalent cardiac arrhythmia in clinical practice, posing an elevated risk of adverse cardiovascular and cerebrovascular outcomes (1, 2). When AF is accompanied by abnormal haemodynamics, it can lead to platelet activation, structural heart changes, and endothelial dysfunction or damage, ultimately increasing the risk of thrombogenesis (3). Effective management of AF’s abnormal heart rhythm can significantly reduce the occurrence of adverse clinical events (4). Middle-aged and elderly patients constitute the majority of adult patients with AF. Given the aging population and its evolving social structure, this trend will inevitably bring significant health burdens to society (5).
Radiofrequency catheter ablation (RFCA) has firmly established itself as a reliable rhythm control treatment for patients with AF, especially for persistent type with poor drug therapy effect (6). Recent findings have demonstrated that RFCA offers superior therapeutic outcomes compared to traditional antiarrhythmic drug (AAD) therapy alone (7). Moreover, endothelial function plays a crucial role in maintaining vascular homeostasis and preventing thromboembolic phenomena (8). RFCA could restore sinus rhythm and significantly improve vascular endothelial dysfunction caused by flow abnormalities, potentially conferring significant clinical benefits and improved prognosis for AF patients (9, 10).
Notably, patients undergoing RFCA face the risk for fibrillation recurrence. A range of factors, including age, heart size, and other conditions, have been associated with this risk (11, 12). Early recurrence is defined as the onset of atrial arrhythmia (AA) within 3 months after catheter ablation (known as the “blanking period”). In order to improve the effectiveness of RFCA, it is crucial to manage postoperative drug therapy during this critical period. This is because it can significantly impact left atrial (LA) anatomical and electrical remodeling, ultimately reducing the risk of AA recurrence (13). Given the availability of various AAD, different treatment regimens may lead to different outcomes (14).
However, there is currently a limited number of studies focusing on the prognosis of elderly patients with AF following RFCA. For this vulnerable patient population, it is imperative to conduct further analysis on the factors that contribute to early postoperative AF recurrence. Additionally, there is a significant lack of information regarding the efficacy and safety of ADDs in controlling early recurrence. Consequently, we conducted this present retrospective study to provide valuable insights on these pertinent issues and aimed to provide crucial clinical evidence for the prevention of AF among the elderly.
We conducted a retrospective analysis of the clinical data of 420 elderly patients (aged 60 years and above) who had undergone RFCA for paroxysmal AF. These patients were followed up at the outpatient department of the 967th Hospital of Joint Logistics Support Force of Chinese PLA between 2018 and 2023. We excluded patients with histories of myocardial infarction, pulmonary dysfunction, thyroid dysfunction, hematologic disease, severe valvulopathy, severe liver and kidney dysfunction, malignant tumor, and New York Heart Association functional classifications above grade 2. Additionally, we excluded patients with incomplete clinical data, failed operations, or those who were unable to restore sinus rhythm. All patients had their clinical data collected within 1 week before ablation and were followed for a period of 3 months. The diagnosis of AF was based on the 2020 ESC/EACTS Guidelines for Diagnosis and Management of Atrial Fibrillation (15). We obtained written informed consent from all participants. This study conformed to the 1975 Declaration of Helsinki and was approved by the Human Ethics Committee of the 967th Hospital of Joint Logistics Support Force of Chinese PLA.
The AAD discontinuation was recommended at least 1 month before the procedure. Sedation was achieved with a combination of midazolam and fentanyl throughout the electrophysiological study and ablation process. Endocardial 3D mapping was conducted using Biosense Webster’s CARTO mapping systems, facilitated by multipolar mapping catheters. For ablation, a 3.5-mm tip externally irrigated ablation catheter was utilized, ensuring a minimum target contact force exceeding 5 g. The ablation targets were determined based on achieving an Ablation Index of at least 400 on the posterior wall and 550 or higher on the anterior, superior, and inferior walls of the left atrium. This approach aimed to create ablation lesions of adequate quality during the wide-area circumferential ablation procedure. Pulmonary vein isolation (PVI) encompassed a comprehensive antral circumferential ablation procedure encompassing the pulmonary veins. The objective was to achieve electrical isolation, which was verified by identifying both entrance and exit block. PVI was further confirmed by the presence of spontaneous potentials or the complete absence of local electrograms, indicating no capture even at high-output pacing. Additional substrate modification, including linear ablation was left to the discretion of the operator and/or the attending physician.
All the data were obtained from standardized clinical electronic medical records, which included comprehensive information such as demographic details, comorbidities, nursing records, laboratory tests, echocardiography, electrocardiography (ECG), treatments, and clinical outcomes. The laboratory tests encompassed a range of assessments including routine blood tests, renal, liver, and thyroid function tests, coagulation profile, myocardial enzymes, electrolytes, and more. Abnormalities in laboratory findings were based on the hospital’s criteria. To assess endothelial function, we employed peripheral arterial tonometry using the EndoPAT2000 device (Itamar Medical, Caesarea, Israel) to measure the reactive hyperemia index (RHI). RHI quantifies the digital hyperemic response and impaired endothelial function was defined as a RHI less than 1.67. We measured these parameters on the day of admission, within 1 week before ablation.
Information about pre-medication were extracted from both electronic and traditional clinical medical records. Following the ablation procedure, all the patients were prescribed a 90-days use of AAD commencing on the day of the ablation (the recommended dosages were as follows: 50 mg/day for propafenone, 80 mg/day for sotalol, 800 mg/day for dronedarone, and 600 mg/day during the initial week, followed by a reduction to 200 mg/day for amiodarone). For safety reasons, the specific choice and dosage of AAD were determined by the attending physician.
Paroxysmal AF was defined as an episode that spontaneously resolves or responds to AADs within 7 days of onset. Patients were prospectively followed for 3 months every 1 week via physician review. Patients were instructed to perform ECG at each visit, and instructed to present for ECG analysis if any symptoms occurred. With the usage of 24-ambulatory electrogram recorder (HCG-801, OMRON HEALTHCARE Co., Ltd.) once a month. The ambulatory electrogram recordings were then reviewed by cardiologists who were unaware of the treatment assignments. These cardiologists evaluated drug usage and the occurrence of AA recurrence. The clinical endpoint was defined as AA recurrence, which was characterized by AA lasting for more than 30 s or AA symptoms persisting during the blanking period (15).
Statistical analyses were carried out using the latest version (27) of the SPSS software. Continuous variables were presented as median [inter quartile range (IQR)] and categorical variables were expressed as n (%). Mann–Whitney U test, Pearson χ2 test or Fisher’s exact test was employed to compare the differences between two groups as appropriate. To identify the risk factors, binary logistic regression models were used. Cox-proportional hazard regression analysis was used to investigate the association between risk factors and clinical endpoint. Variables that were considered clinically relevant or showed a univariate relationship with the outcomes (p < 0.10) were included in the multivariate regression model. To ensure parsimony of the final model, variables for inclusion were carefully chosen according to the number of events available. Odds ratio (OR) or hazard ratio (HR) was employed to determine relationships between risk factors and outcomes. A p-value of less than 0.05 was considered statistically significant.
A total of 420 AF patients who underwent RFCA were enrolled in this study between 2018 and 2023. Among them, there were 87 (20.7%) patients developed an early recurrence and they were divided into patients with early recurrence (n = 87) and patients without early recurrence (n = 333). Baseline characteristics of the two groups were listed in Table 1. Compared to patients without early recurrence, patients with early recurrence showed older age (p < 0.001), larger LA (p < 0.001) and left ventricular (p < 0.001) diameters, and lower ejection fraction (p < 0.001), and lower RHI (p < 0.001). As for blood biomedical tests, high-sensitivity C-reactive protein (hs-CRP) (p < 0.001), d-dimmer (p = 0.011), high-sensitivity cardiac troponin I (hs-cTnI) (p < 0.001), and brain natriuretic peptide (BNP) (p < 0.001) were higher in patients with early recurrence than patients without early recurrence.
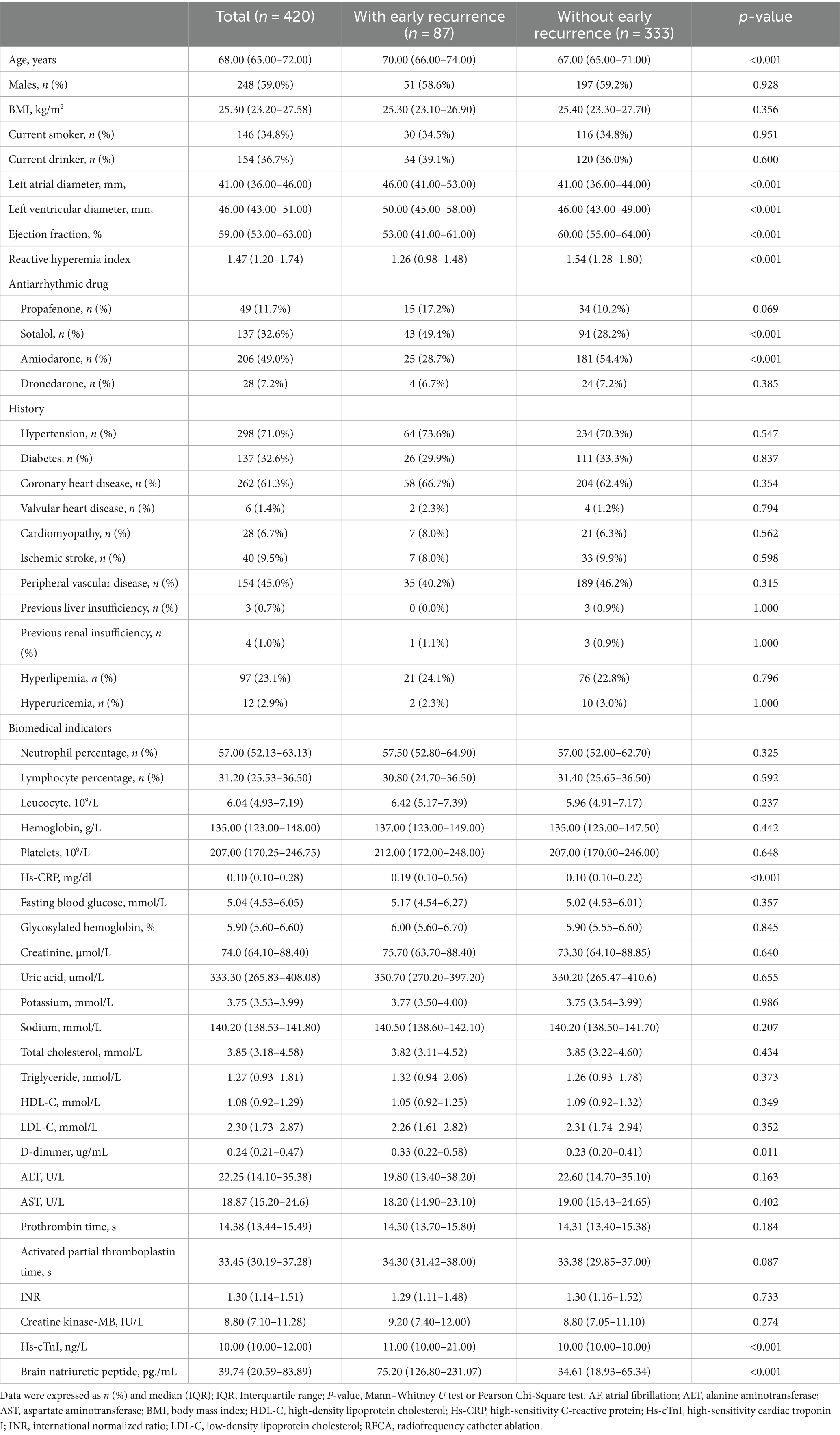
Table 1. Baseline characteristics of elderly AF patients after RFCA.
We performed binary logistic regression models to find the risk factors of early recurrence. After calibration analysis, multivariate model showed that age (p = 0.001), LA diameter (p < 0.001), left ventricular diameter (p = 0.015), RHI (p < 0.001), AAD regimen (p < 0.001) and hs-cTnI (p = 0.017) were independent risk factors that affected the clinical outcome (Table 2).
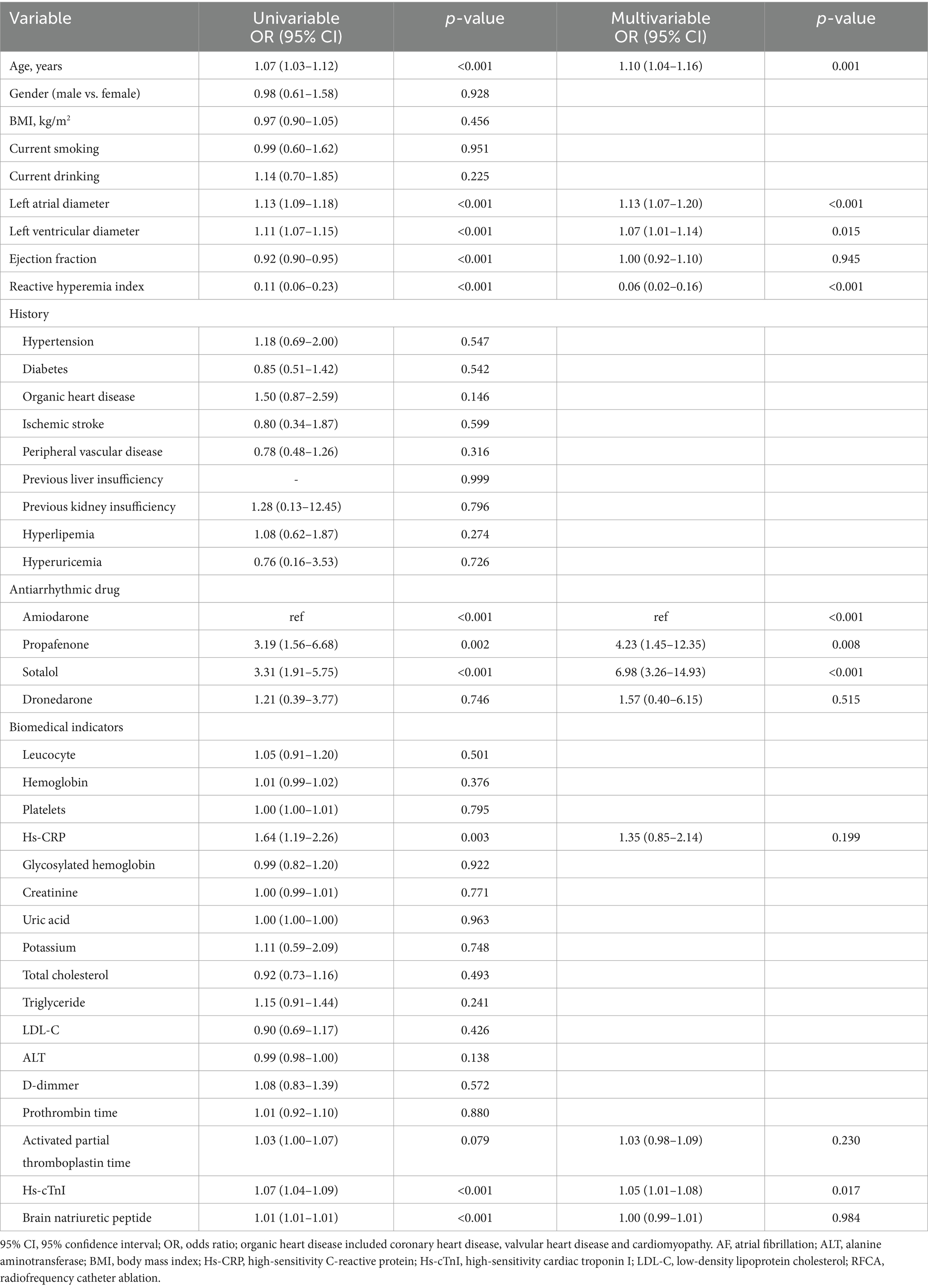
Table 2. Risk factors of early recurrence in elderly AF patients after RFCA.
Sotalol was more used in patients with early recurrence (p < 0.001) while amiodarone was more used in patients without early recurrence (p < 0.001). Compared to patients without early recurrence, there seemed to be more propafenone usage in patients with early recurrence but the difference did not reach statistical significance. To investigate the effect of AAD regimen on clinical outcomes, we employed cox-proportional hazard regression model to compare early recurrence in the 3-month follow-up between the different groups. These patients were classified into four groups according to AAD application after RFCA. We observed that the survival rate of early recurrence in the amiodarone group was higher than in the propafenone group (HR 2.30, 95%CI 1.17–4.53, p = 0.016) and in the sotalol group (HR 3.60, 95%CI 2.17–5.95, p < 0.001). Besides, there was no difference of the survival rate of early recurrence between the amiodarone group and the dronedarone group (HR 1.43, 95%CI 0.49–4.17, p = 0.509) (Figure 1).

Figure 1. Event-free survival for early recurrence in elderly patients with AF after RFCA.
Moreover, we analyzed the occurrence of adverse reactions to different AAD regimens after RFCA. Compared to the amiodarone group, the incidence of liver dysfunction was lower in the dronedarone group (p = 0.046) and the propafenone group (p = 0.021). The incidence of rash/skin irritation was lower the propafenone group than in the amiodarone group (p = 0.036). Although the incidence of thyroid dysfunction was significantly lower in the sotalol group (p = 0.036), the incidence of bradyarrhythmia (p = 0.003), QT interval prolongation (p = 0.035) and atrioventricular transmission block (p = 0.021) were significantly increased than in the amiodarone group (Table 3).
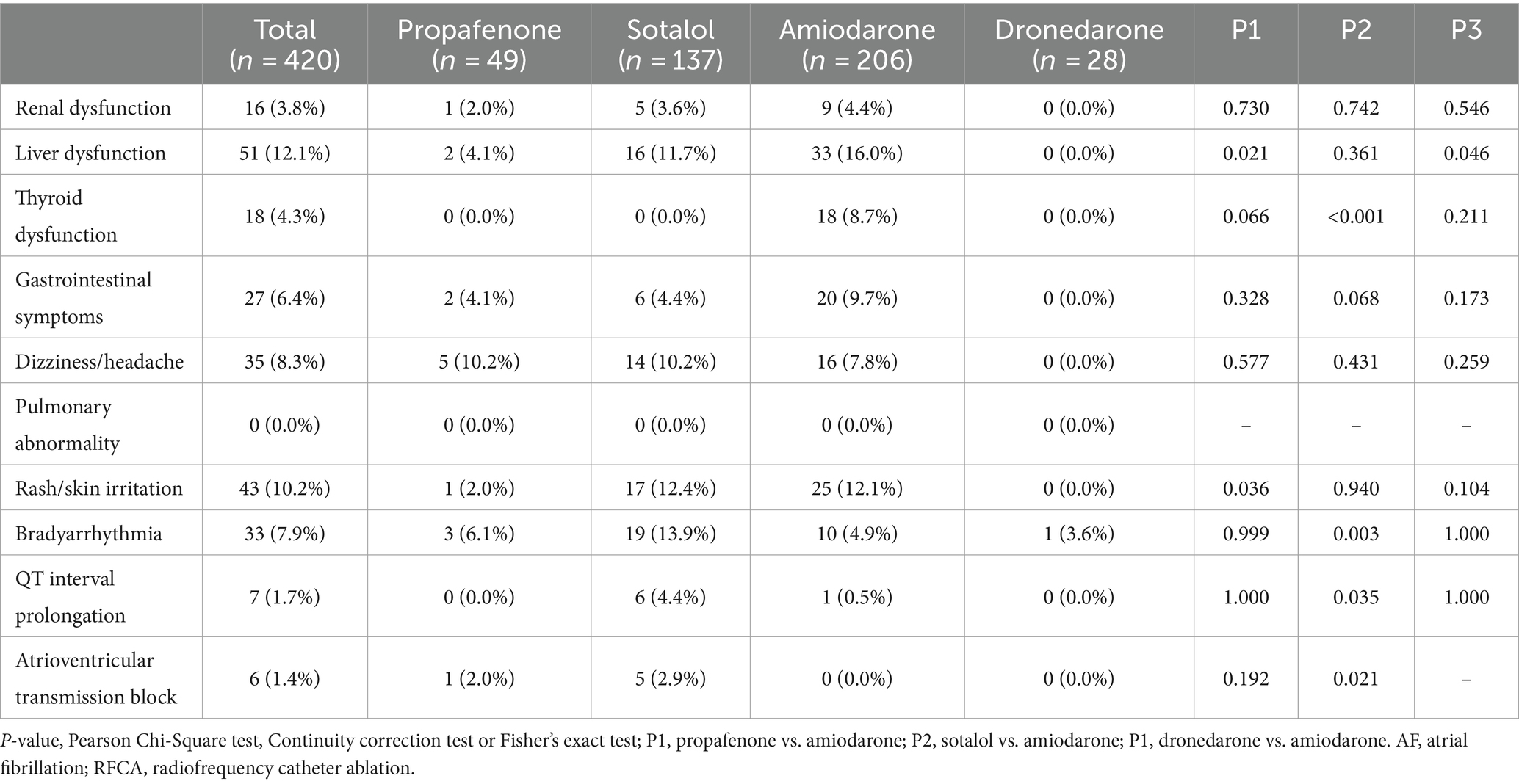
Table 3. Adverse reactions to antiarrhythmic drugs of aged AF patients after RFCA.
This observational retrospective study of 420 consecutive subjects firstly showed RHI was an independent risk factor of early recurrence in elderly patients with AF after RFCA. Different AAD regimens affected the clinical outcomes between of these patients. We found that amiodarone and dronedarone significantly reduced the risk of early recurrence after RFCA than propafenone and sotalol. Moreover, we supposed that dronedarone may be a better option because of its lower incidence of adverse drug reactions compared to amiodarone in elderly patients.
Atrial fibrillation is the most frequently encountered sustained tachyarrhythmia in clinical practice (16). RFCA has emerged as the most effective method for treating AF recently and it is the preferred choice to control cardiac rhythm in patients with drug-refractory symptomatic AF and tachycardia cardiomyopathy AF (17, 18). However, postoperative recurrence remains a significant challenge. Early postoperative recurrence of RFCA refers to any AA lasting ≥30s within 3 months after ablation (19, 20). Effective prediction of early recurrence can guide timely intervention and prevent long-term recurrence, ultimately improving patient outcomes (21). Multiple factors have been reported could affect recurrence after RFCA, including age, gender, baseline cardiac function, and heart size (11, 12, 22). Even rare factors like anxiety have been demonstrated to be linked with it (23). Besides, other factors such as estimated glomerular filtration rate, BNP, soluble tumorigenic inhibition 2 and serum cholesterol have also been demonstrated associated with AF recurrence post-ablation (24–27). Our results were basically consistent with previous findings. However, we employed a non-invasive, highly reproducible method refereed as RHI to assess endothelial function in our study, and found RHI served as an independent risk factor for AF recurrence after ablation which exhibiting good predictive efficacy. This added information to the effective prediction of postoperative AF early recurrence.
Endothelial function is crucial for physiological activities. Patients with AF exhibit significantly reduced endothelial function compared to those with normal sinus rhythm, which is associated with adverse cardiovascular outcomes (28, 29). Moreover, AF triggers the elevation of c-reactive protein and cytokines, exerting a proinflammatory effect on endothelial cells, potentially leading to endothelial dysfunction (30). Additionally, patients with AF are generally older and often have other co-morbidities such as hypertension and diabetes, all of which could cause endothelial damage (31). Impaired endothelial function can also lead to abnormal hemodynamic changes, exacerbating or inducing AF, potentially perpetuating a vicious cycle leading to worse endothelial dysfunction and persistent AF (32). However, endothelial dysfunction can be reversed through various interventions, including dietary modifications, exercise, and drug administration (33). This present study confirmed the potential association between endothelial function and AF early recurrence after RFCA. Previous study has pointed out that assessing endothelial function (RHI) could enable risk stratification for cardiovascular events following AF ablation (34). Our results further emphasized the importance of assessing endothelial function prior to ablation procedures.
The application of AAD during the blanking period after ablation can promote the reversal of electrical remodeling in the atrium and stabilize the heart toward stable sinus rhythm without arrhythmia recurrence (35). This approach is suggested to not only effectively minimize the risk of recurrent AA but also to prevent late recurrences (36). However, other study pointed that AAD usage did not lead to improved clinical outcomes in the later stages (37). Given the high cost and potential postprocedural complications of repeat ablation, promoting sinus rhythm post-ablation through the administration of AAD is still essential. However, consensus is lacking regarding the optimal selection, dosage, and duration of AAD treatment after ablation due to existing AADs have limited safety and effectiveness (15, 38). Additionally, elderly patients account for a higher incidence rate of AF (5, 39). Currently, there is still limited information available on the optimal ADD treatment regimen for this special population following RFCA. Study have demonstrated class III antiarrhythmic drugs exhibiting a more pronounced effect (40). As a multi-ion channel blocker AAD, amiodarone is currently the most widely utilized AAD for the maintenance of sinus rhythm. It also plays a role in controlling atrial inflammation and correcting cardiac autonomic nervous dysfunction (41–43). Similar to our results, compared to propafenone and sotalol, it was more effective in maintaining sinus rhythm (41, 44).
However, it is crucial to remain vigilant about the potential side effects of prolonged AAD usage especially in elderly patients. Amiodarone’s long half-life and tissue accumulation can potentially lead to multiple adverse drug reactions with prolonged use (40). Sotalol has a high risk of cardiotoxicity (44). Besides, more arrhythmias occurred when sotalol was maintained at 80 mg/d within 3 months after RFCA in our study. Dronedarone, a benzofuran derivative, exhibits electrophysiological characteristics belonging to all four Vaughan-Williams classes. It lacks the iodine moiety and has a methane sulfonyl group that reduces its lipophilicity and tissue accumulation potential. Thus, it held favorable safety profile of dronedarone in patients with AF and its lower risk of amiodarone-like organ toxicity (45). However, dronedarone showed lower efficacy in maintaining sinus rhythm in AF patients after electrical cardioversion compared to amiodarone (46). Our findings indicated that dronedarone exhibited comparable efficacy to amiodarone in controlling early recurrence after ablation in elderly patients with AF. However, dronedarone demonstrated a lower incidence of adverse events, suggesting that it could be a preferential choice. The disparity could be attributed to differences in the patient population included, and further confirmation is required in the future.
This study has several limitations. Firstly, despite enrolling patients over nearly six consecutive years, the sample size remained relatively small. Secondly, the study was conducted at a single center, which may have resulted in a limited variety of patients enrolled. Thirdly, there was a notable absence of comprehensive analysis pertaining to the confounding factors encountered during RFCA procedure and subsequent postoperative follow-up period. These factors encompass subtle variations in surgical techniques, individualized differences in disease presentation (specifically COVID-19), disparities in the preoperative cessation period of ADDs, as well as biases in medication selection influenced by the clinician’s clinical experience. All of these could potentially affect the clinical prognosis. Lastly, due to disparities in baseline clinical characteristics that could have biased our results, we attempted to adjust for these differences through a multivariable analysis encompassing a broad range of variables. However, given the absence of a rigorous matching criterion, the findings of this retrospective study should be interpreted with caution.
In summary, the findings of the present analysis revealed that RHI served as an independent predictor of early recurrence in elderly patients with AF after RFCA. Notably, amiodarone and dronedarone were found to be more effective in reducing the risk of early recurrence compared to propafenone and sotalol. Furthermore, we hypothesized that dronedarone might be a preferable choice given its relatively lower incidence of adverse drug reactions compared to amiodarone.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding authors.
The studies involving humans were approved by Human Ethics Committee of the 967th Hospital of Joint Logistics Support Force of Chinese PLA (No. PLA967-GC2023-21). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
CF: Writing – review & editing, Software, Methodology, Investigation, Formal analysis, Data curation. CZ: Writing – review & editing, Software, Methodology, Investigation, Formal analysis, Data curation. YM: Writing – review & editing, Software, Methodology, Investigation, Formal analysis, Data curation. YL: Writing – review & editing, Validation, Resources, Project administration, Funding acquisition. RC: Writing – original draft, Methodology, Conceptualization. HZ: Writing – review & editing, Visualization, Validation, Supervision, Resources, Project administration, Conceptualization.
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This work was supported by grants from the China Red Cross Foundation Medical empowerment public welfare special fund (Grant No. CRCF-YXFN-202201047).
We appreciated all the subjects who participated in the study.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Lippi, G, Sanchis-Gomar, F, and Cervellin, G. Global epidemiology of atrial fibrillation: an increasing epidemic and public health challenge. Int J Stroke. (2021) 16:217–21. doi: 10.1177/1747493019897870
2. King, JB, Azadani, PN, Suksaranjit, P, Bress, AP, Witt, DM, Han, FT, et al. Left atrial fibrosis and risk of cerebrovascular and cardiovascular events in patients with atrial fibrillation. J Am Coll Cardiol. (2017) 70:1311–21. doi: 10.1016/j.jacc.2017.07.758
3. Karim, N, Ho, SY, Nicol, E, Li, W, Zemrak, F, Markides, V, et al. The left atrial appendage in humans: structure, physiology, and pathogenesis. Europace. (2020) 22:5–18. doi: 10.1093/europace/euz212
4. Kirchhof, P, Camm, AJ, Goette, A, Brandes, A, Eckardt, L, Elvan, A, et al. Early rhythm-control therapy in patients with atrial fibrillation. N Engl J Med. (2020) 383:1305–16. doi: 10.1056/NEJMoa2019422
5. Go, AS, Hylek, EM, Phillips, KA, Chang, Y, Henault, LE, Selby, JV, et al. Prevalence of diagnosed atrial fibrillation in adults: national implications for rhythm management and stroke prevention: the AnTicoagulation and risk factors in atrial fibrillation (ATRIA) study. JAMA. (2001) 285:2370–5. doi: 10.1001/jama.285.18.2370
6. Parameswaran, R, Al-Kaisey, AM, and Kalman, JM. Catheter ablation for atrial fibrillation: current indications and evolving technologies. Nat Rev Cardiol. (2021) 18:210–25. doi: 10.1038/s41569-020-00451-x
7. Packer, DL, Mark, DB, Robb, RA, Monahan, KH, Bahnson, TD, Poole, JE, et al. Effect of catheter ablation vs. antiarrhythmic drug therapy on mortality, stroke, bleeding, and cardiac arrest among patients with atrial fibrillation: the CABANA randomized clinical trial. JAMA. (2019) 321:1261–74. doi: 10.1001/jama.2019.0693
8. Corban, MT, Godo, S, Burczak, DR, Noseworthy, PA, Toya, T, Lewis, BR, et al. Coronary endothelial dysfunction is associated with increased risk of incident atrial fibrillation. J Am Heart Assoc. (2020) 9:e014850. doi: 10.1161/JAHA.119.014850
9. Lim, HS, Willoughby, SR, Schultz, C, Chakrabarty, A, Alasady, M, Lau, DH, et al. Successful catheter ablation decreases platelet activation and improves endothelial function in patients with atrial fibrillation. Heart Rhythm. (2014) 11:1912–8. doi: 10.1016/j.hrthm.2014.07.030
10. Okawa, K, Miyoshi, T, Sogo, M, Hara, S, Sudo, Y, Ugawa, S, et al. Improvement in renal and endothelial function after catheter ablation in patients with persistent atrial fibrillation. J Cardiol. (2020) 76:610–7. doi: 10.1016/j.jjcc.2020.07.002
11. Vizzardi, E, Curnis, A, Latini, MG, Salghetti, F, Rocco, E, Lupi, L, et al. Risk factors for atrial fibrillation recurrence: a literature review. J Cardiovasc Med. (2014) 15:235–53. doi: 10.2459/JCM.0b013e328358554b
12. Elliott, AD, Middeldorp, ME, Van Gelder, IC, Albert, CM, and Sanders, P. Epidemiology and modifiable risk factors for atrial fibrillation. Nat Rev Cardiol. (2023) 20:404–17. doi: 10.1038/s41569-022-00820-8
13. Kim, YG, Boo, KY, Choi, JI, Choi, YY, Choi, HY, Roh, SY, et al. Early recurrence is reliable predictor of late recurrence after radiofrequency catheter ablation of atrial fibrillation. JACC Clin Electrophysiol. (2021) 7:343–51. doi: 10.1016/j.jacep.2020.09.029
14. Bray, JJH, Warraich, M, Whitfield, MG, Peter, CU, Baral, R, Ahmad, M, et al. Oral class I and III antiarrhythmic drugs for maintaining sinus rhythm after catheter ablation of atrial fibrillation. Cochrane Database Syst Rev. (2023) 2023:Cd013765. doi: 10.1002/14651858.CD013765.pub2
15. Hindricks, G, Potpara, T, Dagres, N, Arbelo, E, Bax, JJ, Blomström-Lundqvist, C, et al. ESC guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): the task force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) developed with the special contribution of the European heart rhythm association (EHRA) of the ESC. Eur Heart J. (2020) 42:373–498. doi: 10.1093/eurheartj/ehaa612
16. Sagris, M, Vardas, EP, Theofilis, P, Antonopoulos, AS, Oikonomou, E, and Tousoulis, D. Atrial fibrillation: pathogenesis, predisposing factors, and genetics. Int J Mol Sci. (2021) 23:6. doi: 10.3390/ijms23010006
17. Elsayed, M, Abdelfattah, OM, Sayed, A, Prasad, RM, Barakat, AF, Elgendy, IY, et al. Bayesian network meta-analysis comparing cryoablation, radiofrequency ablation, and antiarrhythmic drugs as initial therapies for atrial fibrillation. J Cardiovasc Electrophysiol. (2022) 33:197–208. doi: 10.1111/jce.15308
18. Jame, S, and Barnes, G. Stroke and thromboembolism prevention in atrial fibrillation. Heart. (2020) 106:10–7. doi: 10.1136/heartjnl-2019-314898
19. Miyazaki, S, Taniguchi, H, Nakamura, H, Takagi, T, Iwasawa, J, Hachiya, H, et al. Clinical significance of early recurrence after pulmonary vein antrum isolation in paroxysmal atrial fibrillation – insight into the mechanism. Circ J. (2015) 79:2353–9. doi: 10.1253/circj.CJ-15-0475
20. Badger, TJ, Oakes, RS, Daccarett, M, Burgon, NS, Akoum, N, Fish, EN, et al. Temporal left atrial lesion formation after ablation of atrial fibrillation. Heart Rhythm. (2009) 6:161–8. doi: 10.1016/j.hrthm.2008.10.042
21. Harrison, JL, Jensen, HK, Peel, SA, Chiribiri, A, Grøndal, AK, Bloch, L, et al. Cardiac magnetic resonance and electroanatomical mapping of acute and chronic atrial ablation injury: a histological validation study. Eur Heart J. (2014) 35:1486–95. doi: 10.1093/eurheartj/eht560
22. Peng, Z, Wen-Heng, L, Qing, Z, Pin, S, Shang-Lang, C, Mao-Jing, W, et al. Risk factors for late recurrence in patients with non-valvular atrial fibrillation after radiofrequency catheter ablation. Ann Noninvasive Electrocardiol. (2022) 27:e12924. doi: 10.1111/anec.12924
23. Severino, P, Mariani, MV, Maraone, A, Piro, A, Ceccacci, A, Tarsitani, L, et al. Triggers for atrial fibrillation: the role of anxiety. Cardiol Res Pract. (2019) 2019:1208505. doi: 10.1155/2019/1208505
24. Zheng, J, Zu, D, Cheng, K, Xia, Y, Dong, Y, and Gao, Z. Decreased estimated glomerular filtration rate predicts long-term recurrence after catheter ablation of atrial fibrillation in mild to moderate renal insufficiency. BMC Cardiovasc Disord. (2021) 21:508. doi: 10.1186/s12872-021-02320-y
25. Tan, R, Yu, H, Han, X, Liu, Y, Yang, X, Xia, YL, et al. Circulating soluble suppression of Tumorigenicity 2 predicts recurrence after radiofrequency ablation of persistent atrial fibrillation. Front Cardiovasc Med. (2021) 8:653312. doi: 10.3389/fcvm.2021.653312
26. Carballo, D, Noble, S, Carballo, S, Stirnemann, J, Muller, H, Burri, H, et al. Biomarkers and arrhythmia recurrence following radiofrequency ablation of atrial fibrillation. J Int Med Res. (2018) 46:5183–94. doi: 10.1177/0300060518793807
27. Li, A, Chen, Y, Wang, W, Su, L, and Ling, Z. Association of clinical predictors with recurrence of atrial fibrillation after catheter ablation. Ann Noninvasive Electrocardiol. (2020) 25:e12787. doi: 10.1111/anec.12787
28. Zhang, J, Tan, Q, Lina, W, and Zhaoqian, Z. Endothelial dysfunction predicted cardiovascular events in patients with paroxysmal atrial fibrillation. Saudi Med J. (2022) 43:708–14. doi: 10.15537/smj.2022.43.7.20220214
29. Khan, AA, Thomas, GN, Lip, GYH, and Shantsila, A. Endothelial function in patients with atrial fibrillation. Ann Med. (2020) 52:1–11. doi: 10.1080/07853890.2019.1711158
30. Peller, M, Lodziński, P, Ozierański, K, Tymińska, A, Balsam, P, Kajurek, K, et al. The influence of the atrial fibrillation episode duration on the endothelial function in patients treated with pulmonary veins isolation. Adv Clin Exp Med. (2017) 26:109–13. doi: 10.17219/acem/66995
31. Guazzi, M, Belletti, S, Bianco, E, Lenatti, L, and Guazzi, MD. Endothelial dysfunction and exercise performance in lone atrial fibrillation or associated with hypertension or diabetes: different results with cardioversion. Am J Physiol Heart Circ Physiol. (2006) 291:H921–8. doi: 10.1152/ajpheart.00986.2005
32. Raviele, A, and Ronco, F. Endothelial dysfunction and atrial fibrillation: what is the relationship? J Cardiovasc Electrophysiol. (2011) 22:383–4. doi: 10.1111/j.1540-8167.2010.01954.x
33. Möbius-Winkler, S, Linke, A, Adams, V, Schuler, G, and Erbs, S. How to improve endothelial repair mechanisms: the lifestyle approach. Expert Rev Cardiovasc Ther. (2010) 8:573–80. doi: 10.1586/erc.10.7
34. Okawa, K, Sogo, M, Morimoto, T, Tsushima, R, Sudo, Y, Saito, E, et al. Relationship between endothelial dysfunction and the outcomes after atrial fibrillation ablation. J Am Heart Assoc. (2023) 12:e028482. doi: 10.1161/JAHA.122.028482
35. Xu, B, Peng, F, Tang, W, Du, Y, and Guo, H. Short-term antiarrhythmic drugs after catheter ablation for atrial fibrillation: a Meta-analysis of randomized controlled trials. Ann Pharmacother. (2016) 50:697–705. doi: 10.1177/1060028016653140
36. Leong-Sit, P, Roux, JF, Zado, E, Callans, DJ, Garcia, F, Lin, D, et al. Antiarrhythmics after ablation of atrial fibrillation (5A study): six-month follow-up study. Circ Arrhythm Electrophysiol. (2011) 4:11–4. doi: 10.1161/CIRCEP.110.955393
37. Kaitani, K, Inoue, K, Kobori, A, Nakazawa, Y, Ozawa, T, Kurotobi, T, et al. Efficacy of antiarrhythmic drugs short-term use after catheter ablation for atrial fibrillation (EAST-AF) trial. Eur Heart J. (2016) 37:610–8. doi: 10.1093/eurheartj/ehv501
38. Xu, X, Alida, CT, and Yu, B. Administration of antiarrhythmic drugs to maintain sinus rhythm after catheter ablation for atrial fibrillation: a meta-analysis. Cardiovasc Ther. (2015) 33:242–6. doi: 10.1111/1755-5922.12133
39. Haim, M, Hoshen, M, Reges, O, Rabi, Y, Balicer, R, and Leibowitz, M. Prospective national study of the prevalence, incidence, management and outcome of a large contemporary cohort of patients with incident non-valvular atrial fibrillation. J Am Heart Assoc. (2015) 4:e001486. doi: 10.1161/JAHA.114.001486
40. Huang, R, Lin, J, Gong, K, Chen, L, Fan, L, Zhang, F, et al. Comparison of amiodarone and Propafenone in blanking period after radiofrequency catheter ablation in patients with atrial fibrillation: a propensity score-matched study. Biomed Res Int. (2020) 2020:1835181. doi: 10.1155/2020/1835181
41. Freemantle, N, Lafuente-Lafuente, C, Mitchell, S, Eckert, L, and Reynolds, M. Mixed treatment comparison of dronedarone, amiodarone, sotalol, flecainide, and propafenone, for the management of atrial fibrillation. Europace. (2011) 13:329–45. doi: 10.1093/europace/euq450
42. Ozbakis-Dengiz, G, Halici, Z, Akpinar, E, Cadirci, E, Bilici, D, and Gursan, N. Role of polymorphonuclear leukocyte infiltration in the mechanism of anti-inflammatory effect of amiodarone. Pharmacol Rep. (2007) 59:538–44.
43. Kodama, I, Kamiya, K, and Toyama, J. Amiodarone: ionic and cellular mechanisms of action of the most promising class III agent. Am J Cardiol. (1999) 84:20r–8r. doi: 10.1016/s0002-9149(99)00698-0
44. Piccini, JP, Al-Khatib, SM, Wojdyla, DM, Shaw, LK, Horton, JR, Lokhnygina, Y, et al. Comparison of safety of sotalol versus amiodarone in patients with atrial fibrillation and coronary artery disease. Am J Cardiol. (2014) 114:716–22. doi: 10.1016/j.amjcard.2014.06.004
45. Boriani, G, Blomström-Lundqvist, C, Hohnloser, SH, Bergfeldt, L, Botto, GL, Capucci, A, et al. Safety and efficacy of dronedarone from clinical trials to real-world evidence: implications for its use in atrial fibrillation. Europace. (2019) 21:1764–75. doi: 10.1093/europace/euz193
Keywords: atrial fibrillation, radiofrequency catheter ablation, antiarrhythmic drug, reactive hyperemia index, elderly, clinical outcome
Citation: Fei C, Zhao C, Ma Y, Liu Y, Chen R and Zhang H (2024) Factors influencing early recurrence of atrial fibrillation among elderly patients following radiofrequency catheter ablation and the impact of different antiarrhythmic regimens. Front. Med. 11:1393208. doi: 10.3389/fmed.2024.1393208
Edited by:
Silvio Romano, University of L’Aquila, ItalyReviewed by:
Roberto Coury Pedrosa, Federal University of Rio de Janeiro, BrazilCopyright © 2024 Fei, Zhao, Ma, Liu, Chen and Zhang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hualin Zhang, ZHJhZ29uMTIxOEAxMjYuY29t; Renzheng Chen, NDA2MzQ2MjA1QHFxLmNvbQ==
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.