 Harri Hemilä
Harri Hemilä Elizabeth Chalker
Elizabeth Chalker- 1Department of Public Health, University of Helsinki, Helsinki, Finland
- 2National Centre for Epidemiology and Population Health, Australian National University, Canberra, ACT, Australia
1 Introduction
In empirical studies, sudden termination of high-dose vitamin C has been shown to cause a fall in vitamin C levels to levels below those recorded prior to the high-dose administration (1–4). This phenomenon is called the rebound effect. These studies are old and the vitamin C doses were much less than the dose in the study analyzed in this paper. Unfortunately, there do not seem to be more recent studies, but it seems highly likely that the rebound effect will be observed more strongly with higher doses of vitamin C and with critically ill patients. In certain contexts, the abrupt termination of high-dose vitamin C may dramatically decrease plasma levels and lead to harmful effects on health. The rebound effect was also observed in a guinea pig study, which reported increased mortality after the termination of very high vitamin C doses (5).
Previously we showed that the abrupt termination of 4-day intravenous vitamin C in the LOVIT trial with 862 sepsis patients explained the harm observed in the participants randomized to the vitamin C group (6, 7). After randomization, patients in the vitamin C group were administered vitamin C with a dose of 50 mg/kg body weight every 6 h (16 g/day for an 80 kg person). There was no difference in survival between the trial groups during the 4-day vitamin C administration. However, during days 5 to 7 there was significantly elevated mortality in the vitamin C group with RR = 2.28 (95% CI: 1.24–4.2; vitamin C 33 vs. placebo 15 deaths) (7). After this sharp increase in mortality immediately after the termination of vitamin C, the difference in survival curves leveled off (6, 7). This pattern is consistent with the rebound effect as the cause of the short-term difference between the trial groups.
The CITRIS-ALI trial administered intravenous vitamin C with the same dosage of 50 mg/kg every 6 h for up to 4 days to sepsis patients (8, 9). We showed that there was a statistically significant change in the relationship between the survival curves immediately after the termination of vitamin C in this trial also (10). Vitamin C was significantly beneficial during the 4-day administration, but the benefit sharply disappeared when vitamin C administration was ceased (8, 10). Thus, in these two trials the sudden termination of the 4-day intravenous vitamin C administration caused a substantial short-term change in mortality.
Meta-analyses of large numbers of controlled trials have shown that vitamin C has beneficial effects on unspecified respiratory virus infections (11, 12), and there is also justification that the benefits extend to SARS-CoV-2 infection (13). The COVID A to Z trial of COVID-19 outpatients administered 8 g/day of vitamin C for 10 days (14), and vitamin C increased the rate of recovery by 70% (95% CI 6.8% to 170%, P = 0.025) (15, 16).
A recent study examined the effect of 4-day intravenous vitamin C for COVID-19 patients with a dose of 50 mg/kg every 6 h (17). The patients were also allocated to two groups by the severity of disease: a) patients who were critically ill and b) those who were not critically ill. In the published survival curves of the critically ill patients, visually there is no difference between the vitamin C and control groups during the 4-day vitamin C administration, but there is dramatic divergence soon after the termination of vitamin C. In this paper we analyze the survival curves.
2 Analysis of the survival curves in the trial on vitamin C for COVID-19 patients
The methods of the study on vitamin C and COVID-19 patients have been described previously by Adhikari et al. (17). In brief, two prospectively harmonized randomized clinical trials enrolled critically ill patients receiving organ support in ICU and patients who were not critically ill. The primary outcome was a composite of organ support-free days defined as days alive and free of respiratory and cardiovascular organ support in intensive care up to day 21, and survival to hospital discharge. The range is from −1 (in-hospital death) to 22 for those who survived without needing organ support. The results of the two separate trials were pooled at the end, with 1493 patients assigned to vitamin C and 1097 assigned to the control group.
In their Figure 2C, Adhikari et al. (17) published the survival curves of the critically ill vitamin C and control patients. The follow-up time in the published figure is 90 days which makes it difficult for a reader to detect the substantial divergence between the survival curves during the early follow-up period. Our Figure 1 shows an enlargement of the early period.
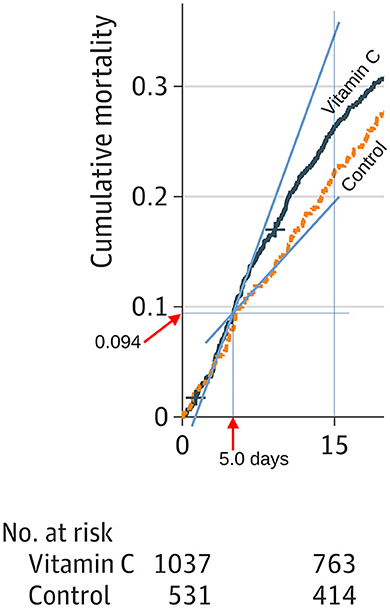
Figure 1. Divergence in the vitamin C and control group survival curves in the trial on vitamin C for COVID-19 patients. We drew the blue lines to estimate the slopes immediately after the termination of vitamin C administration. We measured the distances with a graphics program and determined that the divergence starts at ~5.0 days. The cumulative mortality at the start of the divergence is 0.094. Addition of a separate vitamin C effect for the period 5 to 7.5 days improves the Poisson regression model by χ2 = 6.7 (P = 0.010). See the calculations in the Supplementary material.
We drew guide lines to estimate the time point of the divergence between the two survival curves and determined that to be 5.0 days. The survival proportion at this time point corresponds to a cumulative mortality level of 0.094, which corresponds to 98 patients in the vitamin C group, and 50 participants in the control group. Using these mortality estimates, we calculated the number of patients at risk at day 5: vitamin C 939 and control 481; see the Supplementary material.
Given the published number of patients remaining at day 15 [vitamin C 763; control 414 (17)], we calculated that between days 5 and 15, there were 176 deaths in the vitamin C group and 67 deaths in the control group. These data indicate that in the time range from 5 to 15 days, those in the vitamin C group had 1.35 times the risk of dying than those in the control group (RR = 1.35; 95% CI 1.04–1.74; P = 0.026). This increased mortality occurred directly after the termination of the 4-day intravenous vitamin C.
However, the RR = 1.35 is an underestimate of the immediate harm after the sudden termination of vitamin C. After day 10, the survival curves of the vitamin C and control groups appear equidistant, indicating that the main harm from the abrupt cessation of vitamin C occurred between day 5 and 10; see Supplementary Figures. Therefore, we also estimated the increased risk in mortality in the vitamin C group from the slopes of the blue lines shown in Figure 1. This approach yields RR = 2.5 as the estimate for the increased risk immediately after the termination of vitamin C administration.
As a third approach, we measured the heights of the survival curves at 7.5 days when the divergence started to level off. We calculated that in the time range 5 to 7.5 days there were 56 deaths in the vitamin C group and 13 in the control group, which yields the increased mortality in the vitamin C group soon after the termination of vitamin C as RR = 2.21 (95% CI 1.22–4.0; P = 0.006). This method covers a longer time range than the calculation from the slopes at the intersection, yet the point estimates are consistent and a confidence interval for the estimate can be calculated. Furthermore, addition of a separate vitamin C effect for the period 5 to 7.5 days improves the Poisson regression model by χ2 = 6.7 which corresponds to P = 0.010; see the Supplementary material.
Adhikari et al. (17) reported the effect of 4-day intravenous vitamin C administration on the mortality of COVID-19 patients who were not critically ill in their Figure 3C, and on the primary outcome in Figure 3A. There are no meaningful differences between the groups in either figure.
3 Discussion
In our earlier reanalysis of the LOVIT trial on sepsis patients we found that for the 3 days immediately following the abrupt termination of the 4-day vitamin C administration, mortality in the vitamin C group dramatically increased to RR = 2.28, after which the difference between the survival curves leveled off (6, 7). In the current analysis of the identical 4-day vitamin C administration to critically ill COVID-19 patients, we calculated that immediately after the termination of vitamin C the risk of mortality in the vitamin C group increased to RR = 2.21 which is very close to the estimate for sepsis patients (7). The harm from sudden termination of high-dose vitamin C can be explained by the rebound effect (1–5, 7). Adhikari et al. (17) neglected to mention the previous report (7) even though the vitamin C dosage was identical.
In their introduction to the report, Adhikari et al. (17) stated that two clinical trials (18, 19) had not demonstrated any benefit from vitamin C to sepsis patients. However, Adhikari did not refer to a Korean cohort study which found that the combination of vitamin C and hydrocortisone behaved differently from vitamin C alone, in that vitamin C alone appeared beneficial but the combination did not (20). Although we need to be cautious about treatment effects estimated in observational studies, the Korean findings question the validity of the vitamin C and hydrocortisone combination trials to which Adhikari referred (18, 19). To truly examine the effects of vitamin C, the only difference between the treatment groups should be vitamin C alone, and not combinations with other substances (21).
Furthermore, Adhikari et al. (17) did not justify the choice of 4-day vitamin C administration. Vitamin C levels are low in critically ill patients, which may reflect increased consumption of the vitamin in the system (6, 22). In Adhikari's Figure 2A, about 70% of patients had “organ support-free days” for 17 days or less. Given the 21-day follow-up, this indicates that these patients had organ support for 4 days or more. Thus, about 70% of patients had ongoing organ support after the abrupt termination of the 4-day vitamin C. When there is ongoing increased consumption of vitamin C in the system, the rebound effect may be particularly pronounced, yet this issue was not considered (17). Adhikari's results with the short 4-day administration do not contradict the findings of meta-analyses in which vitamin C shortened ICU stay by 7.8% (22) and the duration of mechanical ventilation by 25% (23).
Although Adhikari et al. (17) studied COVID-19 patients, they did not refer to the COVID A to Z trial (14), which found a 70% increase in the recovery rate of outpatient cases of COVID-19 patients when administering 8 g/day vitamin C for 10 days (15). Furthermore, the quantile treatment effect approach indicated that there was no evidence of benefit for patients who suffered from COVID-19 for less than a week, whereas 4-week symptoms were shortened by about 2 weeks (15, 16).
Adhikari et al. (17) did not consider potential explanations for the conflicting findings: benefit in the COVID A to Z trial but lack of benefit in their study with not-critically ill COVID-19 patients. One potential explanation is the short duration of treatment in their trial (4 days vs. 10 days in the COVID A to Z trial). A second potential explanation is the chosen primary outcome. Adhikari et al. (17) decided on a primary outcome focused on the duration of organ support in the ICU, but such an outcome can be insensitive for patients who are less ill. In fact, the median for the composite primary outcome was 22 days (i.e., maximum) in both groups of the patients who were not critically ill. In contrast, in the COVID A to Z trial, the primary outcome was the duration of symptoms which is a much more sensitive measure.
Cases of scurvy have been reported in critically ill patients and there are numerous reports of patients suffering from scurvy even in Western hospitals (24–37). A few critically ill patients have died of scurvy (38–42). We are concerned that vitamin C may be widely discouraged from use in critically ill patients on the basis of harm caused by the abrupt termination of vitamin C, without any indication that ongoing vitamin C administration is harmful (6, 7, 17). Very low vitamin C levels have been reported in COVID-19 patients (13, 43, 44). Furthermore, scurvy and COVID-19 can co-exist (45).
The efficacy of vitamin C for patients with COVID-19 remains uncertain. However, the Adhikari et al. (17) trial should not be considered as a counterargument to giving vitamin C to COVID-19 patients. Instead, all three trials that terminated 4-day vitamin C administration abruptly (6, 8, 9, 17), provide evidence that vitamin C should not be abruptly stopped if the patients are still critically ill. Given that scurvy is a serious and potentially life-threatening disease, it is not ethical to withhold vitamin C from patients who have very low vitamin C levels (7, 36). Nevertheless, further research of the rebound effect is needed to monitor plasma vitamin C levels in contexts that do not compromise the safety of patients.
Author contributions
HH: Conceptualization, Methodology, Visualization, Writing—original draft, Writing—review & editing. EC: Data curation, Methodology, Validation, Writing—review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Acknowledgments
An earlier version of this comment was published in Pubpeer (46). We contacted the authors and requested primary data for more exact analysis, but we have not received the data.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2024.1391346/full#supplementary-material
References
1. Spero LM, Anderson TW. Ascorbic acid and common colds. Br Med J. (1973) 4:354. doi: 10.1136/bmj.4.5888.354-b
2. Tsao CS, Salimi SL. Evidence of rebound effect with ascorbic acid. Med Hypotheses. (1984) 13:303–10. doi: 10.1016/0306-9877(84)90163-4
3. Omaye ST, Skala JH, Jacob RA. Plasma ascorbic acid in adult males: effects of depletion and supplementation. Am J Clin Nutr. (1986) 44:257–64. doi: 10.1093/ajcn/44.2.257
4. Omaye ST, Skala JH, Jacob RA. Rebound effect with ascorbic acid in adult males. Am J Clin Nutr. (1988) 48:379–80. doi: 10.1093/ajcn/48.2.379
5. Gordonoff T. Can water-soluble vitamins be over-dosed? Research on vitamin C [In German, translation available]. Schweiz Med Wochenschr. (1960) 90:726–9. doi: 10.5281/zenodo.11066294
6. Lamontagne F, Masse MH, Menard J, Sprague S, Pinto R, Heyland DK, et al. Intravenous vitamin C in adults with sepsis in the intensive care unit. N Engl J Med. (2022) 386:2387–98. doi: 10.1056/nejmoa2200644
7. Hemilä H, Chalker E. Abrupt termination of vitamin C from ICU patients may increase mortality: secondary analysis of the LOVIT trial. Eur J Clin Nutr. (2023) 77:490–4. doi: 10.1038/s41430-022-01254-8
8. Fowler AA, Truwit JD, Hite RD, Morris PE, DeWilde C, Priday A, et al. Effect of vitamin C infusion on organ failure and biomarkers of inflammation and vascular injury in patients with sepsis and severe acute respiratory failure: the CITRIS-ALI randomized clinical trial. JAMA. (2019) 322:1261–70. doi: 10.1001/jama.2019.11825
9. de Grooth HJ, Elbers PWG, Vincent JL, Fowler AA, Fisher BJ, Kashiouris MG. Vitamin C for sepsis and acute respiratory failure [discussion]. JAMA. (2020) 323:792–3. doi: 10.1001/jama.2019.21981
10. Hemilä H, Chalker E. Reanalysis of the effect of vitamin C on mortality in the CITRIS-ALI trial: important findings dismissed in the trial report. Front Med. (2020) 7:590853. doi: 10.3389/fmed.2020.590853
11. Hemilä H, Chalker E. Vitamin C for preventing and treating the common cold. Cochrane Database Syst Rev. (2013) 31:CD000980. doi: 10.1002/14651858.CD000980.pub4
12. Hemilä H, Chalker E. Vitamin C reduces the severity of common colds: a meta-analysis. BMC Public Health. (2023) 23:2468. doi: 10.1186/s12889-023-17229-8
13. Hemilä H, de Man AME. Vitamin C and COVID-19. Front Med. (2021) 7:559811. doi: 10.3389/fmed.2020.559811
14. Thomas S, Patel D, Bittel B, Wolski K, Wang Q, Kumar A, et al. Effect of high-dose zinc and ascorbic acid supplementation vs usual care on symptom length and reduction among ambulatory patients with SARSCoV-2 infection: the COVID A to Z randomized clinical trial. JAMA Netw Open. (2021) 4:e210369. doi: 10.1001/jamanetworkopen.2021.0369
15. Hemilä H, Carr A, Chalker E. Vitamin C may increase the recovery rate of outpatient cases of SARS-CoV-2 infection by 70%: reanalysis of the COVID A to Z randomized clinical trial. Front Immunol. (2021) 12:674681. doi: 10.3389/fimmu.2021.674681
16. Hemilä H, Chalker E. Bias against vitamin C in mainstream medicine: examples from trials of vitamin C for infections. Life. (2022) 12:62. doi: 10.3390/life12010062
17. Adhikari NKJ, Hashmi M, Tirupakuzhi Vijayaraghavan BK, Haniffa R, Beane A, et al. Intravenous vitamin C for patients hospitalized with COVID-19: two harmonized randomized clinical trials. JAMA. (2023) 330:1745–59. doi: 10.1001/jama.2023.21407
18. Fujii T, Luethi N, Young PJ, Frei DR, Eastwood GM, French CJ, et al. Effect of vitamin C, hydrocortisone, and thiamine vs hydrocortisone alone on time alive and free of vasopressor support among patients with septic shock: the VITAMINS randomized clinical trial. JAMA. (2020) 323:423–31. doi: 10.1001/jama.2019.22176
19. Sevransky JE, Rothman RE, Hager DN, Bernard GR, Brown SM, Buchman TG, et al. Effect of vitamin C, thiamine, and hydrocortisone on ventilator- and vasopressor-free days in patients with sepsis: the VICTAS randomized clinical trial. JAMA. (2021) 325:742–50. doi: 10.1001/jama.2020.24505
20. Jung SY, Lee MT, Baek MS, Kim WY. Vitamin C for ≥5 days is associated with decreased hospital mortality in sepsis subgroups: a nationwide cohort study. Crit Care. (2022) 26:3. doi: 10.1186/s13054-021-03872-3
21. Hemilä H, Chalker E. Concerns with the revised Japanese recommendation for administering vitamin C to septic patients. J Intensive Care. (2023) 11:52. doi: 10.1186/s40560-023-00702-2
22. Hemilä H, Chalker E. Vitamin C can shorten the length of stay in the ICU: a meta-analysis. Nutrients. (2019) 11:708. doi: 10.3390/nu11040708
23. Hemilä H, Chalker E. Vitamin C may reduce the duration of mechanical ventilation in critically ill patients: a meta-regression analysis. J Intensive Care. (2020) 8:15. doi: 10.1186/s40560-020-0432-y
24. Pichan C, Dhaliwal G, Cusick A, Saint S, Houchens N. Inadequate support. N Engl J Med. (2021) 385:938–44. doi: 10.1056/NEJMcps2108909
25. Baluch A, Landsberg D. Scurvy in the intensive care unit. J Investig Med High Impact Case Rep. (2021) 9:23247096211067970. doi: 10.1177/23247096211067970
26. Gayen SK, Abdelrahman AA, Preston IR, Petit RD, Hill NS. Vitamin C deficiency induced pulmonary arterial hypertension. Chest. (2020) 157:e21–3. doi: 10.1016/j.chest.2019.06.043
27. Penn EH, Olenchock BA, Marston NA. A shocking deficiency. Circulation. (2019) 140:613–7. doi: 10.1161/CIRCULATIONAHA.119.040894
28. Alnaimat S, Oseni A, Yang Y, Melvani V, Aronson A, Harris K, et al. Missing vitamin C: a case of scorbutic cardiac tamponade. JACC Case Rep. (2019) 1:192–6. doi: 10.1016/j.jaccas.2019.07.006
29. Bennett SE, Schmitt WP, Stanford FC, Baron JM. Case 22-2018: a 64-year-old man with progressive leg weakness, recurrent falls, and anemia. N Engl J Med. (2018) 379:282–9. doi: 10.1056/NEJMcpc1802826
30. Abbas F, Ha LD, Sterns R, von Doenhoff L. Reversible right heart failure in scurvy: rediscovery of an old observation. Circ Heart Fail. (2016) 9:e003497. doi: 10.1161/CIRCHEARTFAILURE.116.003497
31. Blanchard MS, Romero JM, Hoang MP. Case records of the Massachusetts General Hospital. Case 1-2014. A 32-year-old man with loss of vision and a rash. N Engl J Med. (2014) 370:159–66. doi: 10.1056/NEJMcpc1214217
32. Kupari M, Rapola J. Reversible pulmonary hypertension associated with vitamin C deficiency. Chest. (2012) 142:225–7. doi: 10.1378/chest.11-1857
33. Holley AD, Osland E, Barnes J, Krishnan A, Fraser JF. Scurvy: historically a plague of the sailor that remains a consideration in the modern intensive care unit. Intern Med J. (2011) 41:283–5. doi: 10.1111/j.1445-5994.2010.02413.x
34. Kieffer P, Thannberger P, Wilhelm JM, Kieffer C, Schneider F. Multiple organ dysfunction dramatically improving with the infusion of vitamin C: more support for the persistence of scurvy in our “welfare” society. Intensive Care Med. (2001) 27:448. doi: 10.1007/s001340000830
35. Meisel JL, McDowell RK. Case 39-1995: a 72-year-old man with exertional dyspnea, fatigue, and extensive ecchymoses and purpuric lesions. N Engl J Med. (1995) 333:1695–702. doi: 10.1056/NEJM199512213332508
36. Hemilä H, de Man AME. Vitamin C deficiency can lead to pulmonary hypertension: a systematic review of case reports. BMC Pulm Med. (2024) 24:140. doi: 10.1186/s12890-024-02941-x
37. Raynaud-Simon A, Cohen-Bittan J, Gouronnec A, Pautas E, Senet P, Verny M, et al. Scurvy in hospitalized elderly patients. J Nutr Health Aging. (2010) 14:407–10. doi: 10.1007/s12603-010-0032-y
38. Hashizume H, Ishikawa Y, Ajima S. Modern scurvy revisited: Japanese cases of a “forgotten” disease. J Dermatol. (2023) 50:e388–9. doi: 10.1111/1346-8138.16891
39. Azar J, Varasteh A, Iltchev D, Soliman M, Baez V, Altaqi B, et al. A very uncommon case of pulmonary arterial hypertension. Am J Med Case Rep. (2019) 7:79–86. doi: 10.12691/ajmcr-7-5-2
40. Doll S, Ricou B. Severe vitamin C deficiency in a critically ill adult: a case report. Eur J Clin Nutr. (2013) 67:881–2. doi: 10.1038/ejcn.2013.42
41. Maltos AL, Portari GV, Saldanha JC, Bernardes Júnior AG, Pardi GR, da Cunha DF. Scurvy in an alcoholic malnourished cirrhotic man with spontaneous bacterial peritonitis. Clinics. (2012) 67:405–7. doi: 10.6061/clinics/2012(04)16
42. Allender WJ. Post mortem tissue levels of ascorbic acid in a scurvy case. J Anal Toxicol. (1982) 6:202–4 doi: 10.1093/jat/6.4.202
43. Tomasa-Irriguible TM, Bielsa-Berrocal L. COVID-19: Up to 82% critically ill patients had low vitamin C values. Nutr J. (2021) 20:66. doi: 10.1186/s12937-021-00727-z
44. Chiscano-Camón L, Ruiz-Rodriguez JC, Plata-Menchaca EP, Martin L, Bajaña I, Martin-Rodríguez C, et al. Vitamin C deficiency in critically ill COVID-19 patients admitted to intensive care unit. Front Med. (2023) 10:1301001. doi: 10.3389/fmed.2023.1301001
45. Jafri A, Edwards O, Gupta P, Abdul-Aziz R. Scurvy in a pediatric patient unable to bear weight: a case report. Cureus. (2023) 15:e38687. doi: 10.7759/cureus.38687
46. Hemilä H. Divergence in mortality at 5 days is overlooked by Adhikari et al. (2023) in a trial on vitamin C for COVID-19 patients. PubPeer. (2024). Available online at: https://pubpeer.com/publications/38194670B815AEE6450D922AA405E2#2
Keywords: ascorbic acid, intensive care, mortality, SARS-CoV-2, scurvy, sepsis, time factors, vitamins
Citation: Hemilä H and Chalker E (2024) Rebound effect explains the divergence in survival after 5 days in a controlled trial on vitamin C for COVID-19 patients. Front. Med. 11:1391346. doi: 10.3389/fmed.2024.1391346
Received: 25 February 2024; Accepted: 06 May 2024;
Published: 21 May 2024.
Edited by:
Sebastien Gibot, Centre Hospitalier Universitaire de Nancy, FranceReviewed by:
Margreet C. M. Vissers, University of Otago, New ZealandCopyright © 2024 Hemilä and Chalker. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Harri Hemilä, aGFycmkuaGVtaWxhQGhlbHNpbmtpLmZp