
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
OPINION article
Front. Med. , 19 June 2024
Sec. Geriatric Medicine
Volume 11 - 2024 | https://doi.org/10.3389/fmed.2024.1390695
This article is part of the Research Topic Pain in the Older Adult Patient View all 4 articles
 Camilla Elena Magi1
Camilla Elena Magi1 Yari Longobucco1*
Yari Longobucco1* Carla Amato1Claudia Camedda2,3Chiara Balestri1
Carla Amato1Claudia Camedda2,3Chiara Balestri1 Khadija El Aoufy1Paolo Iovino1Stefano Bambi1Laura Rasero1
Khadija El Aoufy1Paolo Iovino1Stefano Bambi1Laura Rasero1One of the main nursing responsibilities is to ensure patient wellbeing and comfort. In particular, comfort is closely related to nursing practices (1). Comfort is defined as relief from pain, and emotional and physical distress (2). However, hospitalized elderly patients often undergo several nursing procedures interventions during hospitalization, which are crucial for addressing their complex health needs (3). This extensive attention often exerts a toll, primarily in the form of pain (3). Effectively managing pain in this demographic group extends beyond clinical considerations because it represents a profound moral and ethical imperative given the distinctive challenges encountered by elderly individuals in hospital settings (4). These challenges include a higher prevalence of acute and chronic diseases, age-related physiological alterations, and cognitive impairment or delirium, which can seriously affect pain management (5).
Pain perception represents an intrinsic facet of human experience, which defies simplification as it is a profound subjective phenomenon shaped by an array of determinants (6). Psychological, physiological, and sociocultural factors contribute significantly to shaping how individuals perceive and cope with pain (7, 8). For elderly patients whose experiences of pain are often compounded by these multifarious factors, a tailored and specialized approach to pain management is essential.
During their hospital stay, elderly individuals undergo nursing procedures aimed at addressing their clinical condition (9). Nursing procedures encompass both basic (e.g., fundamentals of care) and advanced activities. The most frequently painful procedures in older adults include mobilization, wound dressing, bladder catheterization, and needle-related procedures, which are emerging as the most common sources of pain among elderly patients. These indispensable procedures, which are crucial during hospitalization, frequently induce discomfort (10). Unfortunately, inadequate pain management frequently persists, leading to heightened anticipatory responses to pain stimuli during subsequent procedures (11). This aspect has been widely explored in different types of patients, such as pediatric (12, 13), but evidence in elderly patients is still lacking.
From this perspective, recognizing the pivotal importance of the comfort of elderly patients and the inherently subjective nature of pain perception, it is imperative to identify effective pain management strategies customized to the unique needs and preferences of each individual patient (14). Such strategies should encompass a comprehensive spectrum spanning both pharmacological and non-pharmacological interventions (15). By addressing these pain experiences more frequently and empirically, healthcare providers can significantly improve the overall quality of life of elderly patients during their hospitalization (16).
While the comfort of older adults during hospitalization is a key concept, there is limited literature and insufficient evidence to indicate the optimal strategies for each individual nursing procedure that may cause discomfort. Furthermore, this issue is underemphasized in clinical practice, often relegated to a secondary consideration at the expense of providing quality, patient-centered care tailored to the specific needs of each hospitalized patient.
The aim of this article is to delve into the critical significance of managing acute procedure-related pain, presenting a compendium of efficacious strategies aimed at bridging the existing gap in pain management in hospitalized elderly individuals. From this perspective, this paper examines the challenges related to pain management in this specific population group, presenting evidence-based approaches that can be easily integrated among the acts of care by nurses, in order to enhance the quality of care provided to elderly patients during their hospital stay.
Effective management of pain during routine nursing procedures, such as blood draws, peripheral venous catheter placement, injections, urinary catheterization, tube insertions, and wound dressing changes, is essential for optimizing patient comfort and overall quality of healthcare delivery (3, 17).
The literature provides valuable insights into various strategies adopted by nurses, including non-pharmacological and technological approaches, to enhance patient experiences and minimize pain perception (18, 19).
These strategies encompass the nuances of evidence-based approaches, with different levels of invasiveness for elderly patients, as shown in Figure 1.
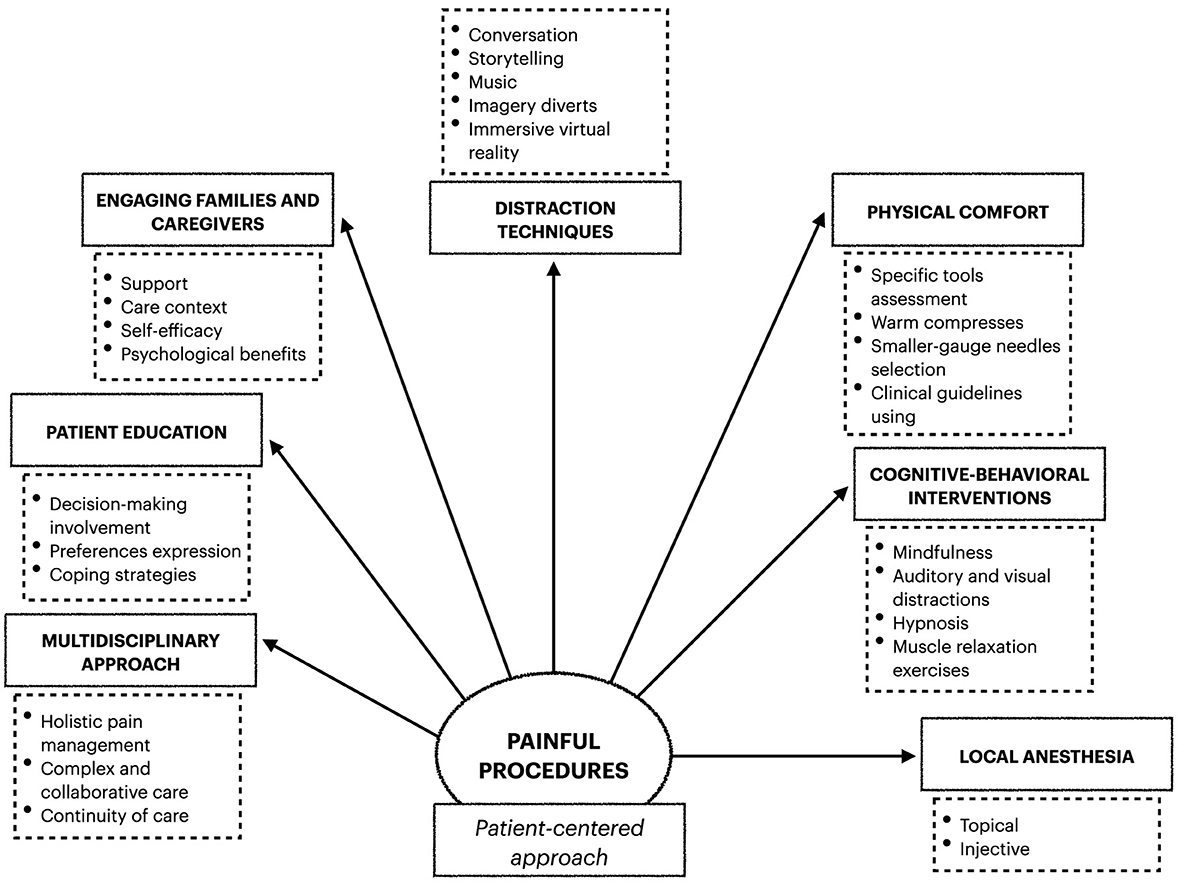
Figure 1. Pain management strategies.
First, a collaborative approach among healthcare professionals, including nurses, physicians, and pain specialists, is essential for the development of standardized pain management protocols. This interdisciplinary approach ensures that the most appropriate and effective pain control strategies are consistently employed, reducing painful procedures, such as through the implementation of mid- or long-term devices (e.g., peripherally inserted central catheters) (20).
Furthermore, embracing the principles of “complex and collaborative care” (21) signifies a shift in mindset and paradigms toward recognizing the multidimensional nature of patient needs. It involves combining diverse perspectives and valuing various resources and their composition (21). This requires valuing the active involvement of the patient and fostering new opportunities for inter-professional collaboration. This approach entails cooperation among various care resources and a reimagined conception and organization of the continuum of care, ensuring a holistic and integrated approach to the comfort of elderly patients (21).
Educating patients about the procedure, its purpose, and potential sensations can significantly contribute to reducing pain perception (22). In fact, patient involvement in decision-making and providing them with the opportunity to express their preferences can empower individuals and enhance their sense of control during procedures (23). Education can reduce anticipatory pain (24), the modulation of which can reduce anxiety and, consequently, pain perception, and promote positive and effective coping strategies (24, 25). Nevertheless, the patient education and engagement process is strictly related to patient satisfaction with the hospitalization experience, reducing healthcare avoidance (26).
Actively engaging families and caregivers in the pain management process can significantly reduce patient anxiety, enhance overall support, and provide a more empathetic and comprehensive care environment. The involvement of families and caregivers can make a substantial contribution to the patient's comfort and, consequently, pain management (27) in order to improve the effects of the chosen interventions (28). Furthermore, in elderly patients with dementia, caregivers can play a pivotal role in the surveillance of pain levels (29), although there is evidence that self-efficacy support interventions need to be planned to support this role (30). Nevertheless, caregivers' engagement also shows benefits such as anxiety, stress, and depression (31).
Distraction techniques have proven to be valuable in reducing pain perception during procedures (32, 33). Engaging patients in calming conversations, storytelling, soothing music, and guided imagery diverts their attention from the procedure itself. These techniques have successfully mitigated subjective experiences of pain (34). Furthermore, the integration of immersive virtual reality (VR) technology into healthcare settings offers an innovative means of transporting patients to alternative environments, effectively diminishing pain perception during procedures (35). However, although VR is a well-known, useful, and scalable intervention, the costs of this technology still represent an implementation barrier (21), and cognitive impairment can hinder its application depending on the level of severity (36).
Physical comfort plays a vital role in pain management, particularly during nursing procedures. In this demographic group, optimizing physical comfort is essential for controlling the symptoms and ensuring patient comfort. personalized care should adopt a preventive approach based on evaluation through specific assessment tools. For example, as reported in the literature, over a third of adults exhibit difficult venous access (DiVA) (37), making the evaluation of venous heritage essential. From this perspective, adopting rating scales, such as the ADIVA scale, makes it possible to identify at-risk patients and adopt personalized strategies (38).
Utilizing warm compresses to facilitate vein dilation is instrumental in enhancing patient comfort and reducing procedural discomfort (39). Additionally, careful selection of smaller-gauge needles is imperative to minimize tissue trauma and discomfort during venipuncture (40), aligning with best practices outlined in clinical guidelines (41). Moreover, employing appropriate techniques and adopting a gentle approach in handling elderly patients during procedures are integral components of pain management strategies, all contributing to minimizing discomfort (40).
Cognitive-behavioral interventions include mindfulness meditation, auditory and visual distractions, hypnosis, and progressive muscle relaxation exercises (42). These interventions offer psychological tools for patients to effectively modulate pain perception and emotional responses (15, 43). Hypnosis is an effective intervention in pain management (44), particularly in wound dressing (45). In patients without cognitive impairment, hypnotic susceptibility can be assessed with easy-to-administer tools such as the Stanford Hypnotic Susceptibility Scale (46).
Nursing procedures that require localized pain relief should be treated pharmacologically with options such as local anesthesia and systemic analgesics.
Local anesthesia, whether administered topically or via injections, has shown significant efficacy, particularly in procedures where localized pain management is pivotal for patient comfort and procedural success (47–49). When local anesthesia is applied in a specific area, immediate relief is provided, allowing procedures to be performed with minimal discomfort to the patient. Nevertheless, analgesics are tailored to individual patient needs (47), considering factors such as medical history, and concurrent medications, to optimize pain management outcomes and minimize potential adverse effects (50). However, in order to promote a safe and comfortable procedural experience for elderly patients, other approaches besides local anesthesia should be considered, especially for lengthy procedures. For example, following a multidisciplinary approach, a timely adoption of opioids or other systemic analgesia techniques may be adopted for painful wound-related procedures (51).
In the context of pain management during nursing procedures, there are a plethora of techniques and strategies to reduce discomfort in elderly patients (Figure 1). These techniques and strategies encompass different approaches that fit tailored and personalized care. The key concept of pain management emphasizes the importance of a patient-centered approach, highlighting the multitude of factors that influence treatment decisions within each individual's unique clinical and social context (52). This involves meticulous evaluation of pain levels, consideration of medical history, and recognition of individual needs and preferences (53). In this landscape, it is crucial to acknowledge the subjective nature of pain perception and to recognize other contributing factors, such as anxiety, which can amplify pain experience (52). In this perspective, the inclusion of non-pharmacological strategies in the nursing care plan, such as distraction techniques, is advisable. These dynamic strategies are continually evolving, alongside technological advancements and ongoing research. The overarching goal remains consistent with alleviating pain and enhancing the overall comfort of elderly patients. Healthcare providers can deliver high-quality care while prioritizing patient comfort by effectively managing acute pain and minimizing distress during procedures.
However, the existing literature and evidence concerning this topic are still lacking, underscoring the need for further exploration. Older adults are exposed to altered peripheral nerve conductivity, leading to a higher likelihood of developing pain (54). Moreover, aging is characterized by a low-grade inflammatory condition, known as “inflammation,” which affect the nociceptive system (55). Furthermore, the pharmacodynamics of analgesics are altered in older people as age-related changes in pain processing (56), enhancing the importance of non-pharmacological approaches.
Therefore, in general, managing pain related to nursing procedures involves integrating technical-operational skills with relational-communication abilities. Nevertheless, one of the key nursing interventions is advocacy, which implies both ethical and clinical relevance in nursing practice (57). Advocacy can enhance the overall quality of life of elderly patients by effectively documenting and reporting procedural pain, evaluating pain care skills, and identifying educational needs among the working group (57). We should not forget that pain management in elderly people who are unable to verbalize must be oriented to interventions that prevent the experience of pain before the beginning of a medical or nursing procedure (56).
This paper aims to represent a call to action at all levels, from the patient to healthcare management, through caregivers and individual healthcare professionals, advocating for an improvement in the quality of the evidence available on this increasingly discussed topic. By fostering a deeper understanding of pain management strategies and their impact on patient outcomes, we can collectively contribute to advancements in nursing practices and enhance the quality of care delivered to patients.
CM: Conceptualization, Methodology, Project administration, Visualization, Writing – original draft, Writing – review & editing. YL: Conceptualization, Methodology, Visualization, Writing – original draft, Writing – review & editing. CA: Visualization, Writing – review & editing. CC: Writing – review & editing. CB: Writing – review & editing. KE: Writing – review & editing. PI: Writing – review & editing. SB: Methodology, Supervision, Writing – review & editing. LR: Conceptualization, Methodology, Project administration, Supervision, Writing – review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Pinto S, Fumincelli L, Mazzo A, Caldeira S, Martins JC. Comfort, well-being and quality of life: Discussion of the differences and similarities among the concepts. Porto Biomed J. (2017) 2:6–12. doi: 10.1016/j.pbj.2016.11.003
2. Wensley C, Botti M, McKillop A, Merry AF. Maximising comfort: how do patients describe the care that matters? A two-stage qualitative descriptive study to develop a quality improvement framework for comfort-related care in inpatient settings. BMJ Open. (2020) 10:e033336. doi: 10.1136/bmjopen-2019-033336
3. Schattner A. The spectrum of hospitalization-associated harm in the elderly. Eur J Intern Med. (2023) 115:29–33. doi: 10.1016/j.ejim.2023.05.025
4. Hofmann B. Managing the moral expansion of medicine. BMC Med Ethics. (2022) 23:97. doi: 10.1186/s12910-022-00836-2
5. Gatchel R, Hulla R, Vanzzini N, Bevers K, Salas E, Garner T. Pain management and the elderly. Pract Pain Manag. (2017) 17:1–4.
6. De Ridder D, Adhia D, Vanneste S. The anatomy of pain and suffering in the brain and its clinical implications. Neurosci Biobehav Rev. (2021) 130:125–46. doi: 10.1016/j.neubiorev.2021.08.013
7. Morais CA, Aroke EN, Letzen JE, Campbell CM, Hood AM, Janevic MR, et al. Confronting racism in pain research: a call to action. J Pain. (2022) 23:878–92. doi: 10.1016/j.jpain.2022.01.009
8. Nascimento MG, Kosminsky M, Chi M. Gender role in pain perception and expression: an integrative review. BrJP. (2020) 3:58–62. doi: 10.5935/2595-0118.20200013
9. Oliveira SM, Costa KN, Santos KF, Oliveira JD, Pereira MA, Fernandes MD. Comfort needs as perceived by hospitalized elders: an analysis under the light of Kolcaba's theory. Rev Bras Enferm. (2020) 73:e20190501. doi: 10.1590/0034-7167-2019-0501
10. Alnahhal KI, Rowse J, Kirksey L. The challenging surgical vascular access creation. Cardiovasc Diagn Ther. (2023) 13:162. doi: 10.21037/cdt-22-560
11. Buowari DY. Pain management in older persons. Update Geriatr. (2021) 2021:1–10. doi: 10.5772/intechopen.93940
12. Gao Y, Xu Y, Liu N, Fan L. Effectiveness of virtual reality intervention on reducing the pain, anxiety and fear of needle-related procedures in paediatric patients: a systematic review and meta-analysis. J Adv Nurs. (2023) 79:15–30. doi: 10.1111/jan.15473
13. Geagea D, Tyack Z, Kimble R, Polito V, Ayoub B, Terhune DB, et al. Clinical hypnosis for procedural pain and distress in children: a scoping review. Pain Med. (2023) 24:661–702. doi: 10.1093/pm/pnac186
14. Kuipers SJ, Cramm JM, Nieboer AP. The importance of patient-centered care and co-creation of care for satisfaction with care and physical and social well-being of patients with multi-morbidity in the primary care setting. BMC Health Serv Res. (2019) 19:1–9. doi: 10.1186/s12913-018-3818-y
15. Tang SK, Tse MMY, Leung SF, Fotis T. The effectiveness, suitability, and sustainability of non-pharmacological methods of managing pain in community-dwelling older adults: a systematic review. BMC Public Health. (2019) 19:1–10. doi: 10.1186/s12889-019-7831-9
16. Menezes TM, Oliveira AL, Santos LB, Freitas RA, Pedreira LC, Veras SM. Hospital transition care for the elderly: an integrative review. Rev Bras Enferm. (2019) 72:294–301. doi: 10.1590/0034-7167-2018-0286
17. Baril L, Nguyen E, Dufresne-Santerre L, Émond V, Émond M, Berthelot S, et al. Pain induced by investigations and procedures commonly administered to older adults in the emergency department: a prospective cohort study. Emerg Med J. (2021) 38:825–9. doi: 10.1136/emermed-2020-210535
18. Mohamed Bayoumi MM, Khonji LMA, Gabr WFM. Are nurses utilizing the non-pharmacological pain management techniques in surgical wards? PLoS ONE. (2021) 16:e0258668. doi: 10.1371/journal.pone.0258668
19. Flor H, Noguchi K, Treede RD, Turk DC. The role of evolving concepts and new technologies and approaches in advancing pain research, management, and education since the establishment of the International Association for the Study of Pain. Pain. (2023) 164:S16–21. doi: 10.1097/j.pain.0000000000003063
20. Warner BE, Lound A, Grailey K, Vindrola-Padros C, Wells M, Brett SJ. Perspectives of healthcare professionals and older patients on shared decision-making for treatment escalation planning in the acute hospital setting: a systematic review and qualitative thematic synthesis. EClinicalMedicine. (2023) 62:e51130. doi: 10.1016/j.eclinm.2023.102144
21. Ingrosso M. La cura complessa e collaborativa. Ric E Propos Sociol Della Cura. Roma: Aracne (2016).
22. Glaser J, Nouri S, Fernandez A, Sudore RL, Schillinger D, Klein-Fedyshin M, et al. Interventions to improve patient comprehension in informed consent for medical and surgical procedures: an updated systematic review. Med Decis Making. (2020) 40:119–43. doi: 10.1177/0272989X19896348
23. Drake G, Williams AC. Nursing education interventions for managing acute pain in hospital settings: a systematic review of clinical outcomes and teaching methods. Pain Manag Nurs. (2017) 18:3–15. doi: 10.1016/j.pmn.2016.11.001
24. Woo KY. Unravelling nocebo effect: the mediating effect of anxiety between anticipation and pain at wound dressing change. J Clin Nurs. (2015) 24:1975–84. doi: 10.1111/jocn.12858
25. Reicherts P, Wiemer J, Gerdes AB, Schulz SM, Pauli P, Wieser MJ. Anxious anticipation and pain: the influence of instructed vs conditioned threat on pain. Soc Cogn Affect Neurosci. (2017) 12:544–54. doi: 10.1093/scan/nsw181
26. Leyva B, Taber JM, Trivedi AN. Medical care avoidance among older adults. J Appl Gerontol. (2020) 39:74–85. doi: 10.1177/0733464817747415
27. Gheshlaghi PA, Farahani ZB, Anboohi SZ, Nasiri M, Ziapour A, Garosi VH. Effect of family presence on pain and anxiety levels among patients during invasive nursing procedures in an emergency department at a public hospital in Western Iran. Afr J Emerg Med. (2021) 11:31–6. doi: 10.1016/j.afjem.2020.11.003
28. Bello CM, Mackert S, Harnik MA, Filipovic MG, Urman RD, Luedi MM. Shared Decision-Making in Acute Pain Services. Curr Pain Headache Rep. (2023) 27:193–202. doi: 10.1007/s11916-023-01111-8
29. Riffin C, Patrick K, Lin SL, Carrington Reid M, Herr K, Pillemer KA. Caregiver–provider communication about pain in persons with dementia. Dementia. (2022) 21:270–86. doi: 10.1177/14713012211036868
30. Boon JT, Herr K, Schirle L, Dietrich MS, Maxwell CA. Caregiving self-efficacy and pain assessment by family caregivers of people living with dementia. Geriatr Nur (Lond). (2023) 53:146–52. doi: 10.1016/j.gerinurse.2023.06.025
31. Yasmeen I, Krewulak KD, Zhang C, Stelfox HT, Fiest KM. The effect of caregiver-facilitated pain management interventions in hospitalized patients on patient, caregiver, provider, and health system outcomes: a systematic review. J Pain Symptom Manage. (2020) 60:1034–46. doi: 10.1016/j.jpainsymman.2020.06.030
32. Ghadimi M, Rejeh N, Heravi-Karimooi M, Tadrisi SD. The effect of audio distraction technique on the intensity of pain caused by the insertion of dialysis needles in hemodialysis elderly patients. سابق پرستاري پژوهش-ايران پرستاري پژوهش. (2019) 13:1060. doi: 10.34172/jsums.2022.16
33. Moradipoor Y, Rejeh N, Heravi Karimooi M, Dahmardehei M, Tadrisi SD. Evaluation of the effect of visual distraction on the anxiety and pain associated with wound dressing changes in burn elderly patients. Iran J Nurs Res. (2020) 15:102–11.
34. Ergin E, Çinar Yücel S. The effect of music on the comfort and anxiety of older adults living in a nursing home in Turkey. J Relig Health. (2019) 58:1401–14. doi: 10.1007/s10943-019-00811-z
35. Colloca L, Raghuraman N, Wang Y, Akintola T, Brawn-Cinani B, Colloca G, et al. Virtual reality: physiological and behavioral mechanisms to increase individual pain tolerance limits. Pain. (2020) 161:2010. doi: 10.1097/j.pain.0000000000001900
36. Hung L, Mann J, Wallsworth C, Upreti M, Kan W, Temirova A, et al. Facilitators and barriers to using virtual reality and its impact on social engagement in aged care settings: a scoping review. Gerontol Geriatr Med. (2023) 9:23337214231166355. doi: 10.1177/23337214231166355
37. Sou V, McManus C, Mifflin N, Frost SA, Ale J, Alexandrou E. A clinical pathway for the management of difficult venous access. BMC Nurs. (2017) 16:1–7. doi: 10.1186/s12912-017-0261-z
38. van Loon FH, van Hooff LW, de Boer HD, Koopman SS, Buise MP, Korsten HH, et al. The modified A-DIVA scale as a predictive tool for prospective identification of adult patients at risk of a difficult intravenous access: a multicenter validation study. J Clin Med. (2019) 8:144. doi: 10.3390/jcm8020144
39. Widyastuti D, Ismahmudi R, Burhanto B, Fazalina AA, Fitri A, Az-Zahra F, et al. Literature review: warm compress with medicine plants to reduce joint pain in the elderly. In: Proceedings of the International Conference on Nursing and Health Sciences. (2021). p. 127–32. doi: 10.37287/picnhs.v2i2.933
40. Mitra TP, Coulter-Nile S, Jegathees T, Luong J, Shetty A, Lai K. SPICED RCT: success and pain associated with intravenous cannulation in the emergency department randomized control trial. J Emerg Med. (2023) 66:57–63. doi: 10.1016/j.jemermed.2023.10.008
41. Oliveira DFDL, Azevedo RC, Gaíva MAM. Guidelines for intravenous therapy in elderly: a bibliographic research. Rev Pesqui Cuid É Fundam Online. (2014) 6:86–100. doi: 10.9789/2175-5361.2014.v6i1.86-100
43. Holler M, Koranyi S, Strauss B, Rosendahl J. Efficacy of hypnosis in adults undergoing surgical procedures: a meta-analytic update. Clin Psychol Rev. (2021) 85:102001. doi: 10.1016/j.cpr.2021.102001
44. Moss D, Willmarth E. Hypnosis, anesthesia, pain management, and preparation for medical procedures. Ann Palliat Med. (2019) 8:498–503. doi: 10.21037/apm.2019.07.01
45. Ma Y, Li Y, Wang C, Zhang Y, Wang L, Hu R, et al. Effects of non-pharmacological interventions on pain in wound patients during dressing change: A systematic review. Nurs Open. (2024) 11:e2107. doi: 10.1002/nop2.2107
46. Kekecs Z, Roberts L, Na H, Yek MH, Slonena EE, Racelis E, et al. Test–retest reliability of the stanford hypnotic susceptibility scale, form C and the Elkins Hypnotizability scale. Int J Clin Exp Hypn. (2021) 69:142–61. doi: 10.1080/00207144.2021.1834858
47. Alzaatreh MY, Abdalrahim MS. Management strategies for pain associated with arteriovenous fistula cannulation: an integrative literature review. Hemodial Int. (2020) 24:3–11. doi: 10.1111/hdi.12803
48. Rzhevskiy A, Popov A, Pavlov C, Anissimov Y, Zvyagin A, Levin Y, et al. Intradermal injection of lidocaine with a microneedle device to provide rapid local anaesthesia for peripheral intravenous cannulation: a randomised open-label placebo-controlled clinical trial. PLoS ONE. (2022) 17:e0261641. doi: 10.1371/journal.pone.0261641
49. Alobayli FY. Factors influencing nurses' use of local anesthetics for venous and arterial access. J Infus Nurs. (2019) 42:91–107. doi: 10.1097/NAN.0000000000000316
50. Waldinger R, Weinberg G, Gitman M. Local anesthetic toxicity in the geriatric population. Drugs Aging. (2020) 37:1–9. doi: 10.1007/s40266-019-00718-0
51. Admassie BM, Ferede YA, Tegegne BA, Lema GF, Admass BA. Wound-related procedural pain management in a resource limited setting: systematic review. Int J Surg Open. (2022) 47:100549. doi: 10.1016/j.ijso.2022.100549
52. Chayadi E, McConnell BL. Gaining insights on the influence of attention, anxiety, and anticipation on pain perception. J Pain Res. (2019) 10:851–64. doi: 10.2147/JPR.S176889
53. Fenske JN, Berland DW, Chandran S, Van Harrison R, Schneiderhan J, Hilliard PE, et al. Pain Management. Ann Arbor (MI): Michigan Medicine University of Michigan. (2021).
54. Hosseini F, Mullins S, Gibson W, Thake M. Acute pain management for older adults. Clin Med. (2022) 22:302. doi: 10.7861/clinmed.22.4.ac-p
55. Ronchetti S, Migliorati G, Delfino D. Association of inflammatory mediators with pain perception. Biomed Pharmacother. (2017) 96:1445–52.doi: 10.1016/j.biopha.2017.12.001
56. McLachlan AJ, Bath S, Naganathan V, Hilmer SN, Le Couteur DG, Gibson SJ, et al. Clinical pharmacology of analgesic medicines in older people: impact of frailty and cognitive impairment. Br J Clin Pharmacol. (2011) 71:351–64. doi: 10.1111/j.1365-2125.2010.03847.x
Keywords: pain, nursing, elderly, painful procedures, advocacy, nursing approach, non-pharmacological intervention, pain management
Citation: Magi CE, Longobucco Y, Amato C, Camedda C, Balestri C, El Aoufy K, Iovino P, Bambi S and Rasero L (2024) Enhancing the comfort of hospitalized elderly patients: pain management strategies for painful nursing procedures. Front. Med. 11:1390695. doi: 10.3389/fmed.2024.1390695
Received: 23 February 2024; Accepted: 05 June 2024;
Published: 19 June 2024.
Edited by:
Rose Penfold, University of Edinburgh, United KingdomReviewed by:
Omar Dyara, Medical College of Wisconsin, United StatesCopyright © 2024 Magi, Longobucco, Amato, Camedda, Balestri, El Aoufy, Iovino, Bambi and Rasero. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yari Longobucco, eWFyaS5sb25nb2J1Y2NvQHVuaWZpLml0
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.