
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Med. , 15 May 2024
Sec. Family Medicine and Primary Care
Volume 11 - 2024 | https://doi.org/10.3389/fmed.2024.1384414
This article is part of the Research Topic New Frameworks for Chronic Diseases Treatment: Research, Prevention, Intervention View all 5 articles
 Júlio Belo Fernandes1,2*
Júlio Belo Fernandes1,2* Sónia Fernandes1,2
Sónia Fernandes1,2 Josefa Domingos1
Josefa Domingos1 Cidália Castro1,2
Cidália Castro1,2 Ana Romão1,2Susana Graúdo3Gonçalo Rosa1,2,3Tânia Franco3Ana Patrícia Ferreira3Claudine Chambino3Bruno Ferreira3Susana Courela3Maria José Ferreira3Isabel Silva3Vera Tiago4Maria João Morais4Joana Casal4Silvia Pereira4
Ana Romão1,2Susana Graúdo3Gonçalo Rosa1,2,3Tânia Franco3Ana Patrícia Ferreira3Claudine Chambino3Bruno Ferreira3Susana Courela3Maria José Ferreira3Isabel Silva3Vera Tiago4Maria João Morais4Joana Casal4Silvia Pereira4 Catarina Godinho4
Catarina Godinho4Introduction: Cognitive and motor impairments are common among stroke survivors. Physical therapy is often used to improve the functional capacity of stroke survivors. However, limited adherence to rehabilitation programs is a challenge. Motivation plays a crucial role in the success of rehabilitation programs as it influences individual adherence to treatment and overall health outcomes. This review aims to identify current trends in motivational strategies used by healthcare professionals for stroke survivor rehabilitation.
Methods: Following the framework developed by Arksey and O’Malley, a scoping review was conducted. We performed a literature search using MEDLINE, CINAHL, the Cochrane Central Register of Controlled Trials, Nursing & Allied Health, and MedicLatina databases.
Results: A total of 906 papers were identified. After selecting and analyzing the articles, 17 papers were included in this review. Health professionals use various strategies to motivate stroke survivors. These approaches include establishing a therapeutic alliance, improving patients’ health literacy, defining realistic goals, fostering problem-solving skills, personalizing the rehabilitation program, showcasing success stories, utilizing persuasive techniques, offering encouragement and compliments, providing emotional support, and effectively managing symptoms.
Conclusion: The knowledge gathered in this review can guide healthcare professionals in helping patients overcome barriers to rehabilitation, improve their motivation, and ultimately enhance their recovery outcomes.
Stroke, a cerebrovascular event, poses a significant health concern characterized by its multifaceted risk factors, incidence rates, and adverse outcomes (1). Risk factors for stroke include a broad spectrum, including but not limited to hypertension, diabetes, obesity, smoking, excessive alcohol consumption, physical inactivity, unhealthy diet, and cardiovascular diseases such as atrial fibrillation and coronary artery disease (2). Stroke rates have been on the rise, primarily due to an aging population and improved survival rates following stroke events (3, 4), with the projected global age-standardized incidence rate of ischemic stroke for the year 2030 estimated to rise to 89.32 per 100,000 population (5). Despite medical advancements, stroke persists as the second leading cause of death and the third leading cause of disability worldwide, imposing substantial burdens on individuals, families, and healthcare systems (6).
Worldwide, 60% of stroke survivors experience permanent disabilities such as cognitive and motor disturbances, specifically affecting balance, coordination, proprioception, muscle tone, muscle strength, and gait (7, 8). The natural recovery occurs in 50% of patients, predominantly within the initial month, with limited progress observed beyond 6 months (9). Enhancing functional capacity ranks among the most prevalent aspirations for stroke survivors (10). Post-rehabilitation, many of these individuals can regain their functional abilities (11).
Physical therapy is a valuable therapeutic approach for stroke survivors. Healthcare professionals commonly recommend home exercise programs to help stroke survivors with clinical rehabilitation or self-management of long-term health conditions. Research strongly supports intensive, repetitive, task-focused practices (11). Adhering to the prescribed rehabilitation program and maintaining consistency can have long-lasting health benefits, such as improved physical function and a better quality of life (12). This adherence can significantly enhance stroke survivors’ well-being and reduce the healthcare system’s burden by fostering their independence (13). However, a well-documented challenge in rehabilitation is the limited adherence to exercise programs (14, 15).
The outcome of rehabilitation often varies based on individual motivation, despite similar medical conditions (16). Numerous studies have highlighted the crucial role of individual motivation in achieving positive health outcomes (16, 17). Adherence to a rehabilitation program is a tangible motivation indicator (18), while its absence hampers physical activity and post-stroke training (19). Integrating motivational strategies into the rehabilitation process can enhance individual adherence and improve their overall health outcomes (20, 21).
Previous studies show a positive link between exercise self-efficacy and initiating and maintaining physical activity, particularly in the early and middle stages of planned programs (22–24). Bandura et al. (20) define self-efficacy as an individual’s belief in their ability to accomplish specific goals or tasks, while motivation reflects the drive or desire to engage in such behavior. Self-efficacy is critical in shaping motivation, behavior, and performance.
Bandura’s social cognitive theory of self-efficacy (25) suggests that individuals’ beliefs about their capabilities to perform a specific task or achieve a particular goal can be influenced by four primary sources: (1) Mastery experiences involve personal experiences of mastering or completing tasks. When individuals succeed at something, their self-efficacy for similar tasks increases; conversely, failure can lower self-efficacy; (2) Vicarious experiences imply observing others, particularly those like oneself, successfully performing tasks. This boosts their self-efficacy because it suggests they can attain similar results through effort and learning; (3) Social persuasion involves receiving feedback, encouragement, or support from others. Positive feedback and persuasive communication can help individuals believe in their abilities to overcome challenges; and (4) Physiological and affective states refer to the emotional and physiological reactions experienced during task performance if an individual associates a particular task with high anxiety or stress levels, their self-efficacy may be lower.
Motivation is crucial in driving behavior change and adherence to rehabilitation programs. Motivational theories can provide healthcare professionals with valuable insights into designing and implementing effective interventions tailored to individual needs (26). Self-determination theory sheds light on the relationship between motivation and behavior. It posits that individuals are inherently motivated to pursue activities that fulfill three basic psychological needs: autonomy, competence, and relatedness (27). Empowering patients by involving them in decision-making regarding their treatment plans and goals in stroke rehabilitation can enhance their intrinsic motivation to engage in rehabilitation activities. Likewise, fostering a sense of competence by providing appropriate feedback and setting achievable goals can boost patients’ confidence and motivation.
Another relevant theory is the transtheoretical model of health behavior change, which suggests that behavior change occurs in stages and involves a series of cognitive and behavioral processes (28, 29). In stroke rehabilitation, understanding where patients are in their readiness to change can inform the selection of appropriate motivational strategies. For instance, patients in the pre-contemplation stage may benefit from raising awareness about the importance of rehabilitation. In contrast, those in the action stage may require support in overcoming barriers to adherence.
Challenges to adhering to rehabilitation programs exist, and prior studies show that interventions enhancing motivation can be effective (21, 30). By integrating insights from motivational theories into clinical practice, healthcare professionals can tailor their interventions to address the diverse needs of stroke survivors. Ultimately this will enhance adherence to rehabilitation programs and improve health outcomes. This comprehensive understanding of motivational strategies can inform the development of more effective and sustainable approaches to stroke rehabilitation (20). Therefore, this review aims to identify motivational strategies used by healthcare professionals during stroke survivor rehabilitation.
The researchers conducted a scoping review following the five-step framework initially developed by Arksey and O’Malley (31) and the recommendations of Levac et al. (32). These steps included:
1. Defining the research question(s)
2. Identifying relevant studies
3. Selecting the studies
4. Charting the data
5. Collating, summarizing, and reporting the results
The review involved an extensive literature search on the motivational strategies used by healthcare professionals in stroke survivors’ rehabilitation. The reporting adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) (33).
The following research question was formulated employing the PCC framework (Population, Concept, and Context) to ensure the inclusion of all pertinent literature in this review: What motivational strategies (C) do healthcare professionals employ in the rehabilitation (C) of stroke survivors (P)?
The researchers searched five databases: MEDLINE, CINAHL, the Cochrane Central Register of Controlled Trials, Nursing & Allied Health, and MedicLatina, covering 2003–2023. The search included publications in English, Portuguese, and Spanish. The final search was performed on June 28, 2023.
The PCC framework served as the foundation for developing the search strategy and establishing criteria for inclusion and exclusion (Table 1).
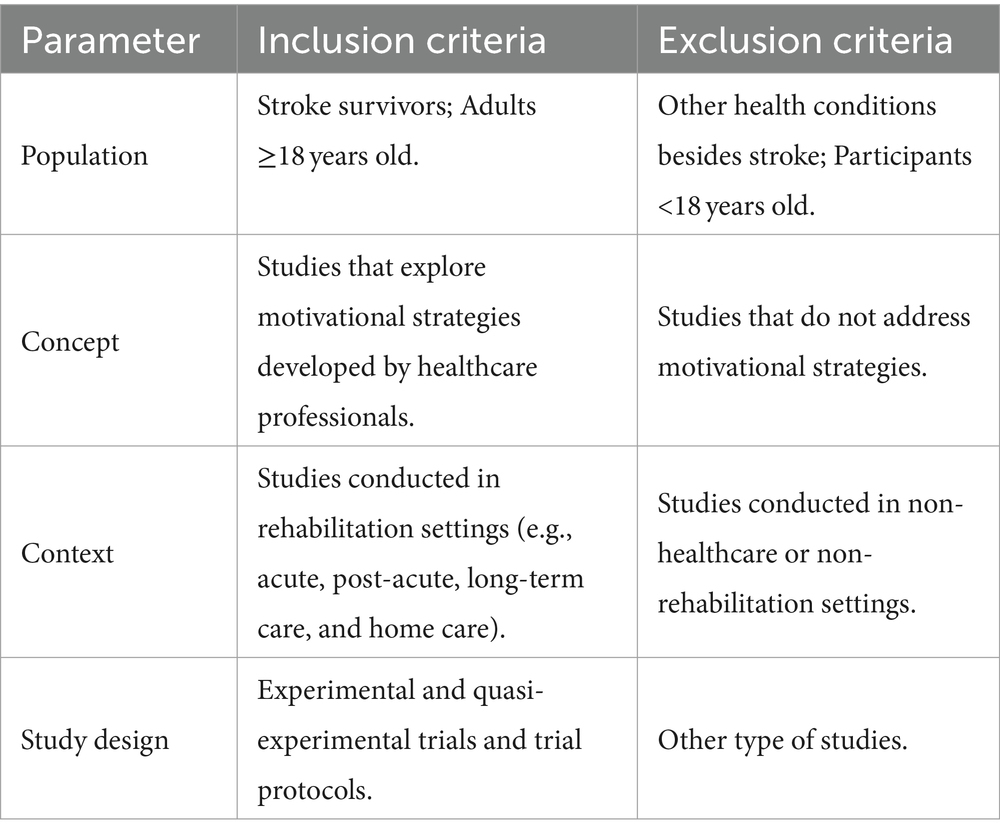
Table 1. Eligibility criteria.
Medical Subject Headings (MeSH) terms were employed in conjunction with Boolean operators to create the following search string: (Stroke) AND (Motivation OR Adherence OR Self Efficacy OR Patient Compliance) AND (Rehabilitation OR Exercise OR Physical Therapy Modalities OR Physiotherapy OR Physical therapy).
After removing duplicates, the titles and abstracts of each citation were independently screened by two researchers utilizing Rayyan, an AI-powered tool for systematic literature reviews. After obtaining relevant studies in full text, each researcher individually assessed each study to ensure agreement on whether it satisfied the inclusion/exclusion criteria. Any disparities in eligibility were resolved either through consensus or with the assistance of an additional researcher.
Two reviewers conducted data extraction employing a standardized electronic data extraction form. The following data were extracted from each study:
• General data (author’s name, publication year, title, and country).
• Methodological data (study design and objectives).
• Results (strategies employed to motivate participants).
All authors underwent a thorough review and discussion of the final extraction chart.
A data-driven thematic analysis, guided by Braun and Clarke’s framework (34), was employed to structure and synthesize the data. Two researchers individually examined the data, manually applying codes during the analysis process. Patterns and consistencies were systematically explored to determine prevalent themes from data based on Bandura’s framework (25).
A quality assessment or critical appraisal was not performed due to the objective of this review.
The initial search retrieved 906 studies (Figure 1), which were exported to Rayyan AI-powered tool for systematic literature reviews. After the duplicate removal, 512 titles and abstracts were screened for eligibility, of which 495 were excluded. The remaining 17 were read in full, meeting the inclusion criteria and being incorporated into this study.
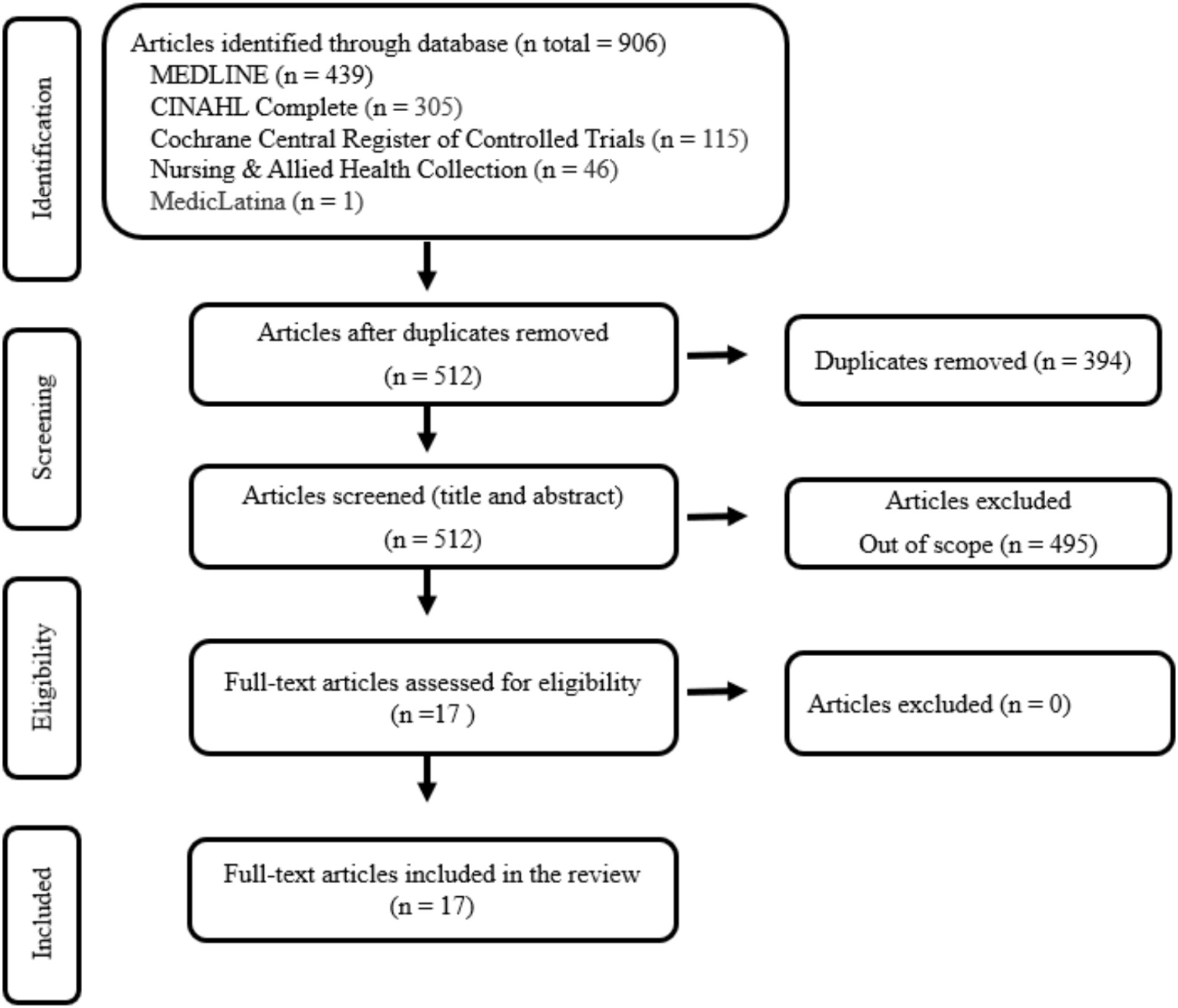
Figure 1. PRISMA flow diagram for study selection.
This scoping review has enabled the identification of various strategies to motivate stroke survivors to adhere to the rehabilitation program.
Among the included studies (Table 2), five were conducted in Australia (35, 36, 42, 44, 45) two in China (47, 48), two in Israel (43, 50), one in the Netherlands (37) one in Norway (38), one in France (40) one in Denmark (39), one in Spain (41) one in Thailand (46), one in Ghana (49), and one in Sweden (51).
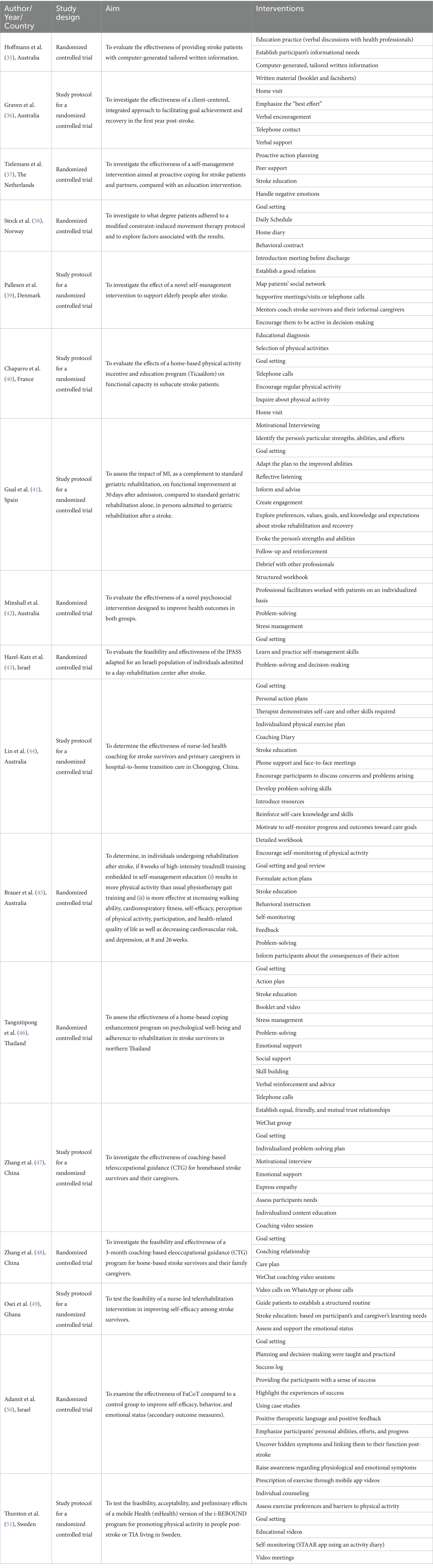
Table 2. Data extraction and synthesis.
Health professionals use several interventions to motivate stroke survivors to adhere to the rehabilitation program. These interventions were integrated into the four sources of influence on self-efficacy defined by Bandura et al. (25), as presented in Table 2 and detailed below.
Bandura’s theory (25) suggests that mastery experiences stem from an individual’s direct encounters with success or failure within a specific task or situation. These past performances can serve as potent influences in cultivating self-efficacy. In this context, several studies have been identified that applied strategies such as the establishment of a therapeutic alliance (39, 41, 44, 47, 48, 50), enhancing health literacy (35–37, 40–42, 44–49, 51), setting achievable goals (38, 40–42, 44–48, 50, 51), personalizing rehabilitation programs (37–42, 44, 46–49, 51), and honing problem-solving skills (39, 42–47, 50, 51).
In implementing these strategies, healthcare professionals employ specific interventions to establish a therapeutic alliance founded on equal, friendly, and mutual trust. This approach seeks insight into individuals’ unique qualities and discerns their needs. Healthcare professionals can use this knowledge to help patients set specific and relevant short-, medium-, and long-term goals, develop problem-solving skills, and customize exercise programs to fit their needs and abilities. This approach promotes consistent engagement in physical activities and encourages patients to make exercise a regular part of their lifestyle.
Researchers employed educational methods tailored to their learning needs to improve the comprehension of stroke survivors and caregivers regarding stroke and recovery. Several studies have supplemented verbal information with leaflets, booklets, and factsheets (35, 36, 46) to facilitate this process. One study used computer-generated personalized written information to create a tailored booklet based on the patient’s informational needs (35). Furthermore, Tangnitipong et al. (46) and Thurston et al. (51) complemented stroke education with educational videos (Table 3).
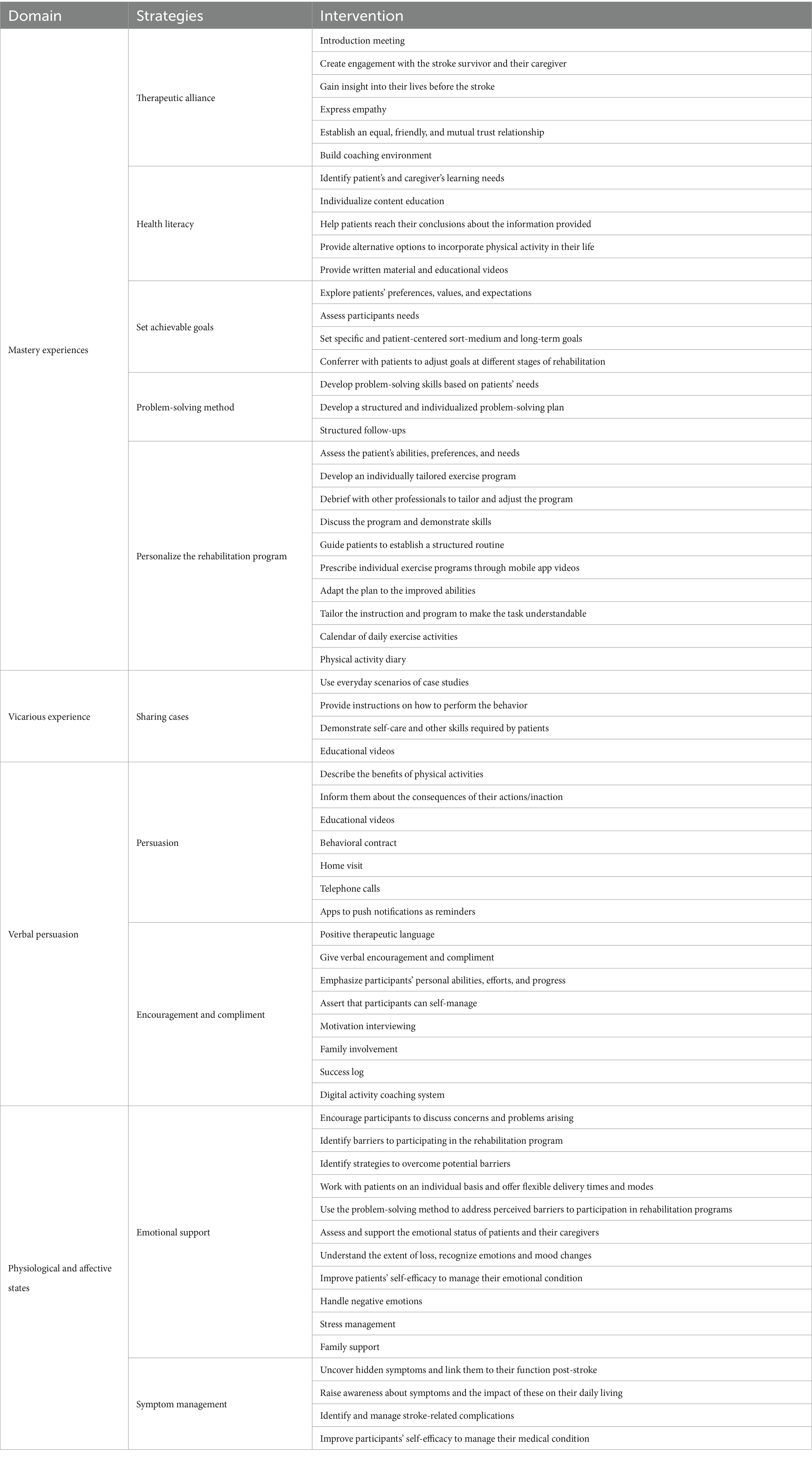
Table 3. Strategies and interventions.
In various studies, vicarious experiences have played a crucial role (44–51). In this context, researchers have shared the success stories of other patients, thereby fostering confidence and motivation among individuals encountering similar challenges. By observing the achievements of others in similar situations, participants were expected to develop the determination needed to reach their own goals. Additionally, researchers provide clear instructions for desired behaviors, demonstrate essential self-care skills for patients, and use educational videos as informative resources.
Various strategies directed toward persuasion and encouragement have been identified. Studies described the benefits of engaging in physical activities, informing individuals about the consequences of their actions (or inaction), and encouraging them to consider the costs and benefits of their behavior carefully (36, 38, 39, 41, 44–49, 51).
Moreover, educational videos have been used in this context, highlighting the health advantages of physical activity, particularly for secondary stroke prevention and overall well-being. Additionally, researchers have employed behavioral contracts, conducted home visits, made telephone calls, and utilized mobile apps equipped with push notifications to act as reminders for performing activities. These apps also provide feedback on the percentage of goal fulfillment over time.
In addition to these strategies, Zhang et al. (47, 48) introduced a unique approach by asking stroke survivors to create and share videos. These videos featured the practice of occupational exercises and participation in activities of daily living, among other relevant content.
Researchers implemented a comprehensive set of interventions to provide encouragement and compliments (36, 38–41, 46–48, 50, 51). These interventions encompassed positive therapeutic language and acknowledged and praised participants for their efforts. Furthermore, they provided verbal encouragement and compliments to boost participants’ confidence and motivation. Another aspect of this strategy involved emphasizing each participant’s unique personal abilities, efforts, and progress, instilling a sense of individual achievement and growth. Researchers encouraged participants to believe in their capacity to self-manage their rehabilitation process, promoting a sense of autonomy and self-efficacy.
Family involvement played a significant role, enlisting the support of the participant’s family to provide additional encouragement and a strong support network.
One study used a success log to record and celebrate participants’ successes and achievements throughout their rehabilitation journey to reinforce the sense of accomplishment. Zhang et al. (47, 48) also used digital activity coaching systems to offer ongoing guidance and support for physical activities and rehabilitation, leveraging technology to enhance motivation and progress.
In physiological and affective states, participants were encouraged to discuss their concerns and problems, identify potential barriers to engagement, and create strategies to overcome these obstacles (37, 39, 42–49).
Moreover, problem-solving was employed to address perceived barriers to participation in rehabilitation programs (45, 51). Emotional assessment and support were integral, encompassing the evaluation and assistance of patients and their caregivers in managing their emotional well-being. Researchers sought to understand the extent of loss, recognize emotions and mood changes, and identify personalized coping strategies tailored to everyone’s needs.
The emotional support approach included strategies for managing negative emotions, dealing with stress, and getting family support. Under Symptom Management, researchers designed a set of interventions to address various aspects (39, 41–46, 49, 50). These interventions involved uncovering hidden symptoms and establishing connections with their post-stroke functionality. Participants were also aware of symptoms such as fatigue, cognitive impairments, low self-efficacy, and their impact on daily living. The strategy also included the identification and management of complications related to stroke. Moreover, participants were actively supported to enhance their self-efficacy in managing their medical condition and participating in rehabilitation programs.
This review identified 72 interventions used by health professionals to motivate stroke survivors. Utilizing Bandura’s Theory (25) as the conceptual framework, the findings of this review were categorized and interpreted, grouping the interventions into 11 strategies.
The results of this review emphasize the significance of engaging the patient and their family right from the outset of stroke rehabilitation. Establishing a therapeutic alliance from the beginning is not merely a procedural formality but a foundational step with profound implications for rehabilitation. It acknowledges that the rehabilitation process is a collaborative journey, recognizing the patient as an active participant rather than a passive recipient of care, thereby enabling the early identification of the patient’s needs (52, 53). Early identification is instrumental in tailoring the rehabilitation process to each person.
Collaboratively setting achievable goals is another cornerstone of effective stroke rehabilitation. By involving stroke survivors and their families in this process, goals become more meaningful and aligned with the patient’s desires and capabilities. This enhances motivation and promotes a greater sense of ownership and commitment to the rehabilitation journey (31).
The development of personalized programs reflects the acknowledgment that each stroke survivor’s experience is unique, and their rehabilitation plan should be tailored accordingly (54, 55). These personalized plans address not only physical needs but also emotional and psychological requirements, promoting holistic recovery. In addition, personalizing rehabilitation programs ensures that the interventions are closely aligned with the patient’s needs, abilities, and aspirations (56). This tailored approach maximizes the chances of success and minimizes the risk of interventions that may be irrelevant or overwhelming (57). Stroke survivors often encounter a range of challenges during their recovery. By honing problem-solving skills, patients and their families can develop strategies to overcome obstacles as they arise (55). This proactive approach empowers patients to navigate the complexities of rehabilitation more effectively.
Sharing success stories of other patients who have faced similar challenges is a powerful motivational strategy. It allows stroke survivors to identify with the achievements of their peers, fostering a sense of confidence and hope. These inspiring cases demonstrate that recovery is possible, which is fundamental for patient motivation (58).
Persuasion and encouragement are pivotal in motivating stroke survivors to actively engage in their rehabilitation journey. In addition to face-to-face contact and phone or video calls, several studies use educational videos focusing on the health benefits of physical activity for secondary stroke prevention, and overall health stands out as a particularly influential strategy (46–48, 51). Previous studies also show that educational videos can be a powerful persuasion tool, providing concrete evidence of the positive outcomes they can achieve through their efforts (59).
Behavioral contracts can be another persuasive intervention that should be taken into consideration. These contracts formalize the patient’s commitment to their rehabilitation goals. Previous studies verified that by signing such a contract, patients commit to the prescribed activities and interventions. This formalized commitment can significantly boost motivation and accountability, as patients feel responsible for honoring the agreement (60).
The study by Thurston et al. (51) used a mobile application to push notifications. These applications serve as continuous reminders to patients to carry out their rehabilitation activities. Moreover, they can deliver a concrete sense of progress by providing feedback on the goal attainment percentage over time.
In addition to persuasion, several studies used encouragement and compliments to boost patients’ self-esteem and self-efficacy. When healthcare professionals acknowledge and praise patients’ efforts, it can enhance their confidence and motivation to continue striving. It reinforces progress and successes along the journey (17, 61).
Providing emotional support and effective management of post-stroke symptoms is critical, as survivors often face significant symptoms and emotional challenges (62, 63). Encouraging open discussion of concerns, identifying post-stroke symptoms and emotional barriers, and providing flexible support can help patients cope with their condition, enhancing their overall well-being.
The results of this review indicate a growing trend in incorporating new technologies to improve stroke survivors’ adherence to rehabilitation programs. Interestingly, several studies (64, 65) have already embraced mobile applications as an integral part of their interventions to educate, monitor, and counsel patients. This underscores the increasing awareness of the potential of digital technologies to enhance the effectiveness and accessibility of rehabilitation.
Mobile apps hold the potential to offer a range of benefits, including the delivery of personalized information, the ability to monitor patient progress, the provision of real-time reminders and feedback, and making rehabilitation more accessible, especially in situations where in-person therapy may be limited (66, 67).
As technology continues to evolve and become more accessible, it is reasonable to anticipate that more studies and rehabilitation programs will adopt and adapt these tools.
Overall, the review pioneers a motivational approach to stroke rehabilitation. Stroke rehabilitation is a complex journey that demands physical recovery and patient commitment. Motivation is pivotal in ensuring stroke survivors actively engage in and adhere to their rehabilitation programs, significantly influencing their recovery outcomes (68). This review fills a crucial gap by being the first to systematically identify and categorize motivational strategies healthcare professionals use to support stroke patients during their rehabilitation process. It provides an overview of the different techniques that can be used to increase motivation in this group.
From a practical perspective, the study’s findings offer actionable insights for healthcare professionals involved in stroke rehabilitation. The study equips health professionals with a toolkit to tailor interventions to individual patient needs by delineating various motivational strategies. For instance, the emphasis on establishing a therapeutic alliance underscores the importance of building rapport and trust with patients from the outset, laying a solid foundation for collaborative goal-setting and personalized care plans. Similarly, incorporating technology, such as mobile applications, presents tangible opportunities to enhance stroke survivors’ engagement and adherence through real-time feedback, reminders, and educational resources.
Furthermore, identifying specific interventions, such as sharing success stories and providing emotional support, offers practical guidance on fostering motivation within rehabilitation settings. By leveraging these strategies, healthcare professionals can create supportive environments that empower stroke survivors to participate actively in their recovery journey, ultimately improving rehabilitation outcomes.
Theoretically, the study contributes to the ongoing discourse on self-efficacy and motivation within the context of health behavior change. Bandura’s Theory of self-efficacy (25) serves as a theoretical framework, elucidating how mastery experiences, vicarious experiences, verbal persuasion, and physiological/affective states influence individuals’ beliefs in their ability to achieve desired outcomes. By mapping the identified interventions onto these sources of influence, the study provides theoretical validation for their effectiveness in enhancing self-efficacy and motivating behavior change among stroke survivors.
Moreover, the study underscores the dynamic interplay between individual, interpersonal, and environmental factors in shaping motivational processes. The emphasis on collaborative goal-setting, family involvement, and personalized care highlights the socioecological nature of motivation, wherein interactions between individuals and their social contexts influence motivational outcomes. This aligns with contemporary behavior change theories, emphasizing the reciprocal determinism between personal factors, behavior, and environmental influences (27–29).
The review fosters a more nuanced understanding of motivational processes in stroke rehabilitation by bridging practical insights with theoretical frameworks. It underscores the importance of adopting holistic approaches that consider individual needs and broader socioenvironmental factors in promoting sustained behavior change and optimal recovery outcomes. Furthermore, this review provides solid evidence to inform the development of a specific care pathway for motivating stroke survivors. By integrating the identified strategies, best practices, and clinical recommendations, a care pathway can guide healthcare professionals in addressing patient motivation throughout the post-stroke rehabilitation process.
A well-designed care pathway can offer a systematic framework to ensure that motivational interventions are consistently personalized and applied to each patient’s needs and preferences (69). Additionally, by integrating appropriate outcome assessment measures, a care pathway can enable continuous monitoring of patient progress and adaptation of interventions as needed over time (70, 71).
By developing a patient-centered care pathway focused on motivation, healthcare providers can maximize the potential for stroke survivors’ recovery, promoting more consistent and enduring adherence to the rehabilitation process. This can significantly improve patients’ physical, cognitive, and emotional functionality and overall quality of life.
Furthermore, a motivation-focused care pathway can help optimize healthcare resources, minimizing the time and costs associated with treating complications resulting from a lack of adherence to rehabilitation. By promoting a proactive and preventive approach to post-stroke management, a care pathway can reduce hospital readmissions and improve long-term outcomes for stroke survivors.
The findings from this review can have significant implications for future research, potentially serving as the groundwork for developing tailored care pathways that motivate patients to adhere to rehabilitation programs. This approach could enable healthcare professionals to integrate these interventions into daily practice effectively. However, it is important to acknowledge several limitations in this research. Firstly, the exclusive focus on experimental studies may introduce a bias toward strategies primarily employed by researchers rather than those commonly used by healthcare professionals in their routine care. Secondly, the restriction of databases might have excluded relevant studies. Lastly, including only English, Portuguese, and Spanish papers opens the possibility that studies in other languages could have influenced the review’s outcomes differently.
This review identified several strategies used by healthcare professionals to motivate stroke survivors to engage in rehabilitation programs. These strategies involve establishing a therapeutic alliance, enhancing patients’ health literacy, setting attainable goals, tailoring rehabilitation programs, employing problem-solving techniques, sharing case studies, utilizing persuasion, offering encouragement and compliments, and providing emotional support and symptom management. This research has a unique focus on motivation in stroke rehabilitation and highlights its importance in enhancing the quality of care and outcomes for stroke survivors. It contributes valuable insights that can positively impact the lives of those recovering from stroke and assist healthcare professionals in delivering more effective rehabilitation services.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
JF: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Supervision, Visualization, Writing – original draft, Writing – review & editing. SF: Data curation, Formal analysis, Methodology, Writing – original draft, Writing – review & editing. JD: Writing – original draft, Writing – review & editing. CCa: Writing – original draft, Writing – review & editing. AR: Writing – original draft, Writing – review & editing. SG: Writing – original draft, Writing – review & editing. GR: Writing – original draft, Writing – review & editing. TF: Writing – original draft, Writing – review & editing. AF: Writing – original draft, Writing – review & editing. CCh: Writing – original draft, Writing – review & editing. BF: Writing – original draft, Writing – review & editing. SC: Writing – original draft, Writing – review & editing. MF: Writing – original draft, Writing – review & editing. IS: Writing – original draft, Writing – review & editing. VT: Writing – original draft, Writing – review & editing. MM: Writing – original draft, Writing – review & editing. JC: Writing – original draft, Writing – review & editing. SP: Writing – original draft, Writing – review & editing. CG: Writing – original draft, Writing – review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors thank FCT/MCTES for the financial support to CiiEM (UIDB/04585/2020) through national funds.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Donkor, ES. Stroke in the 21(st) century: a snapshot of the burden, epidemiology, and quality of life. Stroke Res Treat. (2018) 2018:3238165. doi: 10.1155/2018/3238165
2. Boehme, AK, Esenwa, C, and Elkind, MS. Stroke risk factors, genetics, and prevention. Circ Res. (2017) 120:472–95. doi: 10.1161/CIRCRESAHA.116.308398
3. GBDS Collaborators. Global, regional, and national burden of stroke and its risk factors, 1990-2019: a systematic analysis for the global burden of disease study 2019. Lancet Neurol. (2021) 20:795–820.
4. King, D, Wittenberg, R, Patel, A, Quayyum, Z, Berdunov, V, and Knapp, M. The future incidence, prevalence and costs of stroke in the UK. Age Ageing. (2020) 49:277–82. doi: 10.1093/ageing/afz163
5. Pu, L, Wang, L, Zhang, R, Zhao, T, Jiang, Y, and Han, L. Projected global trends in ischemic stroke incidence, deaths and disability-adjusted life years from 2020 to 2030. Stroke. (2023) 54:1330–9. doi: 10.1161/STROKEAHA.122.040073
6. eClinicalMedicine. The rising global burden of stroke. EClinicalMedicine. (2023) 59:102028. doi: 10.1016/j.eclinm.2023.102028
7. Gittins, M, Lugo-Palacios, D, Vail, A, Bowen, A, Paley, L, Bray, B, et al. Stroke impairment categories: a new way to classify the effects of stroke based on stroke-related impairments. Clin Rehabil. (2021) 35:446–58. doi: 10.1177/0269215520966473
8. Yao, YY, Wei, ZJ, Zhang, YC, Li, X, Gong, L, Zhou, JW, et al. Functional disability after ischemic stroke: a community-based cross-sectional study in Shanghai, China. Front Neurol. (2021) 12:649088. doi: 10.3389/fneur.2021.649088
9. Lee, KB, Lim, SH, Kim, KH, Kim, KJ, Kim, YR, Chang, WN, et al. Six-month functional recovery of stroke patients: a multi-time-point study. Int J Rehabil Res. (2015) 38:173–80. doi: 10.1097/MRR.0000000000000108
10. Dharma, KK, Damhudi, D, Yardes, N, and Haeriyanto, S. Increase in the functional capacity and quality of life among stroke patients by family caregiver empowerment program based on adaptation model. Int J Nurs Sci. (2018) 5:357–64. doi: 10.1016/j.ijnss.2018.09.002
11. Winstein, CJ, Stein, J, Arena, R, Bates, B, Cherney, LR, Cramer, SC, et al. Guidelines for adult stroke rehabilitation and recovery: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. (2016) 47:e98–e169. doi: 10.1161/STR.0000000000000098
12. Peek, K, Sanson-Fisher, R, Mackenzie, L, and Carey, M. Interventions to aid patient adherence to physiotherapist prescribed self-management strategies: a systematic review. Physiotherapy. (2016) 102:127–35. doi: 10.1016/j.physio.2015.10.003
13. Gibson-Moore, H. UK chief medical officers’ physical activity guidelines 2019: What’s new and how can we get people more active? Nutr Bull. (2019) 44:320–8. doi: 10.1111/nbu.12409
14. Argent, R, Daly, A, and Caulfield, B. Patient involvement with home-based exercise programs: can connected health interventions influence adherence? JMIR Mhealth Uhealth. (2018) 6:e47. doi: 10.2196/mhealth.8518
15. Levy, T, Laver, K, Killington, M, Lannin, N, and Crotty, M. A systematic review of measures of adherence to physical exercise recommendations in people with stroke. Clin Rehabil. (2018) 33:535–45. doi: 10.1177/0269215518811903
16. Rapoliene, J, Endzelyte, E, Jaseviciene, I, and Savickas, R. Stroke patients motivation influence on the effectiveness of occupational therapy. Rehabil Res Pract. (2018) 2018:9367942. doi: 10.1155/2018/9367942
17. Oyake, K, Suzuki, M, Otaka, Y, and Tanaka, S. Motivational strategies for stroke rehabilitation: a descriptive cross-sectional study. Front Neurol. (2020) 11:553. doi: 10.3389/fneur.2020.00553
18. Palacio, A, Garay, D, Langer, B, Taylor, J, Wood, BA, and Tamariz, L. Motivational interviewing improves medication adherence: a systematic review and Meta-analysis. J Gen Intern Med. (2016) 31:929–40. doi: 10.1007/s11606-016-3685-3
19. Nicholson, S, Sniehotta, FF, van Wijck, F, Greig, CA, Johnston, M, McMurdo, ME, et al. A systematic review of perceived barriers and motivators to physical activity after stroke. Int J Stroke. (2013) 8:357–64. doi: 10.1111/j.1747-4949.2012.00880.x
20. Fernandes, JB, Ferreira, N, Domingos, J, Ferreira, R, Amador, C, Pardal, N, et al. Health Professionals’ motivational strategies to enhance adherence in the rehabilitation of people with lower limb fractures. Scop Rev Int J Environ Res Public Health. (2023) 20:7050. doi: 10.3390/ijerph20227050
21. McGrane, N, Galvin, R, Cusack, T, and Stokes, E. Addition of motivational interventions to exercise and traditional physiotherapy: a review and meta-analysis. Physiotherapy. (2015) 101:1–12. doi: 10.1016/j.physio.2014.04.009
22. Isa, T, Ueda, Y, Nakamura, R, Misu, S, and Ono, R. Relationship between the intention-behavior gap and self-efficacy for physical activity during childhood. J Child Health Care. (2019) 23:79–86. doi: 10.1177/1367493518777297
23. Pedersen, MM, Zebis, MK, Langberg, H, Poulsen, OM, Mortensen, OS, Jensen, JN, et al. Influence of self-efficacy on compliance to workplace exercise. Int J Behav Med. (2013) 20:365–70. doi: 10.1007/s12529-012-9239-0
24. Pekmezi, D, Jennings, E, and Marcus, BH. Evaluating and enhancing self-efficacy for physical activity. ACSMs Health Fit J. (2009) 13:16–21. doi: 10.1249/FIT.0b013e3181996571
25. Bandura, A, Freeman, WH, and Lightsey, R. Self-efficacy: the exercise of control. J Cogn Psychother. (1999) 13:158–66. doi: 10.1891/0889-8391.13.2.158
26. Karloh, M, Matias, TS, de Oliveira, JM, de Lima, FF, Araujo Pinheiro, DH, Barbosa, GB, et al. Breaking barriers to rehabilitation: the role of behavior change theories in overcoming the challenge of exercise-related behavior change. Braz J Phys Ther. (2023) 27:100574. doi: 10.1016/j.bjpt.2023.100574
27. Patrick, H, and Williams, GC. Self-determination theory: its application to health behavior and complementarity with motivational interviewing. Int J Behav Nutr Phys Act. (2012) 9:18. doi: 10.1186/1479-5868-9-18
28. Raihan, N, and Cogburn, M. Stages of Change Theory. Treasure Island (FL): StatPearls Publishing (2024).
29. Prochaska, JO, and Velicer, WF. The transtheoretical model of health behavior change. Am J Health Promot. (1997) 12:38–48. doi: 10.4278/0890-1171-12.1.38
30. Pudkasam, S, Feehan, J, Talevski, J, Vingrys, K, Polman, R, Chinlumprasert, N, et al. Motivational strategies to improve adherence to physical activity in breast cancer survivors: a systematic review and meta-analysis. Maturitas. (2021) 152:32–47. doi: 10.1016/j.maturitas.2021.06.008
31. McClain, C. Collaborative rehabilitation goal setting. Top Stroke Rehabil. (2005) 12:56–60. doi: 10.1310/ELB1-EGKF-QUQC-VFE9
32. Levac, D, Colquhoun, H, and O’Brien, KK. Scoping studies: advancing the methodology. Implement Sci. (2010) 5:69. doi: 10.1186/1748-5908-5-69
33. Tricco, AC, Lillie, E, Zarin, W, O’Brien, KK, Colquhoun, H, Levac, D, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. (2018) 169:467–73. doi: 10.7326/M18-0850
34. Braun, V, and Clarke, V. Using thematic analysis in psychology. Qual Res Psychol. (2006) 3:77–101. doi: 10.1191/1478088706qp063oa
35. Hoffmann, T, McKenna, K, Worrall, L, and Read, SJ. Randomised trial of a computer-generated tailored written education package for patients following stroke. Age Ageing. (2007) 36:280–6. doi: 10.1093/ageing/afm003
36. Graven, C, Brock, K, Hill, K, Ames, D, Cotton, S, and Joubert, L. From rehabilitation to recovery: protocol for a randomised controlled trial evaluating a goal-based intervention to reduce depression and facilitate participation post-stroke. BMC Neurol. (2011) 11:73. doi: 10.1186/1471-2377-11-73
37. Tielemans, NS, Visser-Meily, JM, Schepers, VP, van de Passier, PE, Port, IG, Vloothuis, JD, et al. Effectiveness of the Restore4Stroke self-management intervention “plan ahead!”: a randomized controlled trial in stroke patients and partners. J Rehabil Med. (2015) 47:901–9. doi: 10.2340/16501977-2020
38. Stock, R, Thrane, G, Askim, T, Karlsen, G, Langorgen, E, Erichsen, A, et al. Norwegian constraint-induced therapy multisite trial: adherence to treatment protocol applied early after stroke. J Rehabil Med. (2015) 47:816–23. doi: 10.2340/16501977-2000
39. Pallesen, H, Naess-Schmidt, ET, Kjeldsen, SS, Pedersen, SKS, Sorensen, SL, Brunner, I, et al. “stroke −65 plus. Continued active life”: a study protocol for a randomized controlled cross-sectoral trial of the effect of a novel self-management intervention to support elderly people after stroke. Trials. (2018) 19:639.
40. Chaparro, D, Daviet, JC, Borel, B, Kammoun, B, Salle, JY, Tchalla, A, et al. Home-based physical activity incentive and education program in subacute phase of stroke recovery (Ticaa’dom): study protocol for a randomized controlled trial. Trials. (2018) 19:68. doi: 10.1186/s13063-017-2410-9
41. Gual, N, Pérez, LM, Castellano-Tejedor, C, Lusilla-Palacios, P, Castro, J, Soto-Bagaria, L, et al. IMAGINE study protocol of a clinical trial: a multi-center, investigator-blinded, randomized, 36-month, parallel-group to compare the effectiveness of motivational interview in rehabilitation of older stroke survivors. BMC Geriatr. (2020) 20:321. doi: 10.1186/s12877-020-01694-6
42. Minshall, C, Castle, DJ, Thompson, DR, Pascoe, M, Cameron, J, McCabe, M, et al. A psychosocial intervention for stroke survivors and carers: 12-month outcomes of a randomized controlled trial. Top Stroke Rehabil. (2020) 27:563–76. doi: 10.1080/10749357.2020.1738677
43. Harel-Katz, H, Adar, T, Milman, U, and Carmeli, E. Examining the feasibility and effectiveness of a culturally adapted participation-focused stroke self-management program in a day-rehabilitation setting: a randomized pilot study. Top Stroke Rehabil. (2020) 27:577–89. doi: 10.1080/10749357.2020.1738676
44. Lin, S, Xiao, LD, and Chamberlain, D. A nurse-led health coaching intervention for stroke survivors and their family caregivers in hospital to home transition care in Chongqing, China: a study protocol for a randomized controlled trial. Trials. (2020) 21:240. doi: 10.1186/s13063-020-04748-7
45. Brauer, SG, Kuys, SS, Ada, L, and Paratz, JD. IMproving physical ACtivity after stroke via treadmill training (IMPACT) and self-management: a randomized trial. Int J Stroke. (2022) 17:1137–44. doi: 10.1177/17474930221078121
46. Tangnitipong, S, Vuttanon, N, Pothiban, L, and Chintanawat, R. Effectiveness of a home-based coping enhancement program for stroke survivors: a randomized controlled trial. Pac Rim Int J Nurs Res. (2022) 26
47. Zhang, L, Yan, Y, Sun, Z, Ge, X, Qin, X, and Lin, KC. Coaching-based Teleoccupational guidance for home-based stroke survivors and their family caregivers: study protocol for a superior randomized controlled trial. Evid Based Complement Alternat Med. (2022) 2022:9123498. doi: 10.1155/2022/9123498
48. Zhang, L, Yan, YN, Sun, ZX, Yan, DR, Chen, YW, Lin, KC, et al. Effects of coaching-based teleoccupational guidance for home-based stroke survivors and their family caregivers: a pilot randomised controlled trial. Int J Environ Res Public Health. (2022) 19:16355. doi: 10.3390/ijerph192316355
49. Osei, SKJ, Adomako-Bempah, E, Yeboah, AA, Owiredu, LA, and Ohene, LA. Nurse-led telerehabilitation intervention to improve stroke efficacy: protocol for a pilot randomized feasibility trial. PLoS One. (2023) 18:e0280973. doi: 10.1371/journal.pone.0280973
50. Adamit, T, Shames, J, and Rand, D. Functional and cognitive occupational therapy (FaC(o)T) improves self-efficacy and behavioral-emotional status of individuals with mild stroke; analysis of secondary outcomes. Int J Environ Res Public Health. (2023) 20:5052. doi: 10.3390/ijerph20065052
51. Thurston, C, Bezuidenhout, L, Humphries, S, Johansson, S, von Koch, L, Hager, CK, et al. Mobile health to promote physical activity in people post stroke or transient ischemic attack—study protocol for a feasibility randomised controlled trial. BMC Neurol. (2023) 23:124. doi: 10.1186/s12883-023-03163-0
52. Bishop, M, Kayes, N, and McPherson, K. Understanding the therapeutic alliance in stroke rehabilitation. Disabil Rehabil. (2021) 43:1074–83. doi: 10.1080/09638288.2019.1651909
53. Stubbe, DE. The therapeutic Alliance: the fundamental element of psychotherapy. Focus. (2018) 16:402–3. doi: 10.1176/appi.focus.20180022
54. Fernandes, JB, Teixeira, F, and Godinho, C. Personalized care and treatment compliance in chronic conditions. J Personal Med. (2022) 12:737. doi: 10.3390/jpm12050737
55. Tavares, E, Coelho, J, Rogado, P, Correia, R, Castro, C, and Fernandes, JB. Barriers to gait training among stroke survivors. Integrat Rev J Function Morphol Kinesiol. (2022) 7:85. doi: 10.3390/jfmk7040085
56. Domingos, J, Dean, J, Cruickshank, TM, Smilowska, K, Fernandes, JB, and Godinho, C. A novel boot camp program to help guide personalized exercise in people with Parkinson disease. J Personal Med. (2021) 11:938. doi: 10.3390/jpm11090938
57. Fernandes, JB, Fernandes, SB, Almeida, AS, Vareta, DA, and Miller, CA. Older Adults’ perceived barriers to participation in a falls prevention strategy. J Personal Med. (2021) 11:450. doi: 10.3390/jpm11060450
58. Smith, M, Scott, A, Mellish, S, and Faulkner, J. Understanding the experiences of people living with stroke engaging in a community-based physical-activity Program. Health. (2023) 11:154. doi: 10.3390/healthcare11020154
59. Denny, MC, Vahidy, F, Vu, KY, Sharrief, AZ, and Savitz, SI. Video-based educational intervention associated with improved stroke literacy, self-efficacy, and patient satisfaction. PLoS One. (2017) 12:e0171952. doi: 10.1371/journal.pone.0171952
60. Savani, M. Can commitment contracts boost participation in public health programs? J Behav Exp Econ. (2019) 82:101457. doi: 10.1016/j.socec.2019.101457
61. Yoshida, T, Otaka, Y, Osu, R, Kumagai, M, Kitamura, S, and Yaeda, J. Motivation for rehabilitation in patients with subacute stroke: a qualitative study. Front Rehabil Sci. (2021) 2:664758. doi: 10.3389/fresc.2021.664758
62. Devereux, N, and Berns, AM. Evaluation & Treatment of psychological effects of stroke. Delaware J Public Health. (2023) 9:62–9. doi: 10.32481/djph.2023.08.011
63. McCurley, JL, Funes, CJ, Zale, EL, Lin, A, Jacobo, M, Jacobs, JM, et al. Preventing chronic emotional distress in stroke survivors and their informal caregivers. Neurocrit Care. (2019) 30:581–9. doi: 10.1007/s12028-018-0641-6
64. Marwaa, MN, Guidetti, S, Ytterberg, C, and Kristensen, HK. Use of Mobile/tablet and web-based applications to support rehabilitation after stroke: a scoping review. J Rehabil Med. (2022) 54:jrm00269. doi: 10.2340/jrm.v54.452
65. Burns, SP, Terblanche, M, Perea, J, Lillard, H, DeLaPena, C, Grinage, N, et al. mHealth intervention applications for adults living with the effects of stroke: a scoping review. Arch Rehabil Res Clin Transl. (2021) 3:100095. doi: 10.1016/j.arrct.2020.100095
66. Cao, W, Kadir, AA, Tang, W, Wang, J, Yuan, J, and Hassan, II. Effectiveness of mobile application interventions for stroke survivors: systematic review and meta-analysis. BMC Med Inform Decis Mak. (2024) 24:6. doi: 10.1186/s12911-023-02391-1
67. Rivera, BD, Nurse, C, Shah, V, Roldan, C, Jumbo, AE, Faysel, M, et al. Do digital health interventions hold promise for stroke prevention and care in black and Latinx populations in the United States? A scoping review. BMC Public Health. (2023) 23:2549. doi: 10.1186/s12889-023-17255-6
68. Verrienti, G, Raccagni, C, Lombardozzi, G, De Bartolo, D, and Iosa, M. Motivation as a measurable outcome in stroke rehabilitation: a systematic review of the literature. Int J Environ Res Public Health. (2023) 20:4187. doi: 10.3390/ijerph20054187
69. Schrijvers, G, van Hoorn, A, and Huiskes, N. The care pathway: concepts and theories: an introduction. Int J Integr Care. (2012) 12:e192. doi: 10.5334/ijic.812
70. Monzio Compagnoni, M, Caggiu, G, Allevi, L, Barbato, A, Carle, F, D’Avanzo, B, et al. Assessment and monitoring of the quality of clinical pathways in patients with depressive disorders: results from a multiregional Italian investigation on mental health care quality (the QUADIM project). J Clin Med. (2023) 12. doi: 10.3390/jcm12093297
Keywords: stroke, motivational interviewing, patient compliance, rehabilitation, medicine
Citation: Fernandes JB, Fernandes S, Domingos J, Castro C, Romão A, Graúdo S, Rosa G, Franco T, Ferreira AP, Chambino C, Ferreira B, Courela S, Ferreira MJ, Silva I, Tiago V, Morais MJ, Casal J, Pereira S and Godinho C (2024) Motivational strategies used by health care professionals in stroke survivors in rehabilitation: a scoping review of experimental studies. Front. Med. 11:1384414. doi: 10.3389/fmed.2024.1384414
Edited by:
Francesca Tessitore, University of Salerno, ItalyReviewed by:
Virginia Campedelli, Sapienza University of Rome, ItalyCopyright © 2024 Fernandes, Fernandes, Domingos, Castro, Romão, Graúdo, Rosa, Franco, Ferreira, Chambino, Ferreira, Courela, Ferreira, Silva, Tiago, Morais, Casal, Pereira and Godinho. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Júlio Belo Fernandes, anVsaW9iZWxvMDFAZ21haWwuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.