 Víctor Doménech-García1
Víctor Doménech-García1 Daniel Pecos-Martín2Julia Blasco-Abadía1
Daniel Pecos-Martín2Julia Blasco-Abadía1 Pablo Bellosta-López1*María Pilar López-Royo1
Pablo Bellosta-López1*María Pilar López-Royo1- 1Facultad de Ciencias de la Salud, Universidad San Jorge, Zaragoza, Spain
- 2Departamento de Enfermería y Fisioterapia, Universidad de Alcalá, Alcalá de Henares, Spain
Objective: This study aimed to investigate the influence of potential placebo and nocebo effects on pain perception of percutaneous needle electrolysis (PNE) in individuals with patellar tendinopathy.
Methods: In this secondary analysis of a three-arm randomized double-blinded controlled trial, intra and inter-session pain perception data from 48 sporting participants with patellar tendinopathy between 18 and 45 years were investigated. Participants were divided into 3 parallel groups: “no-sham group” [PNE intervention], “single-sham group” [sham PNE by using dry needling], and “double-sham group” [sham PNE by using sham needles]. Every group received 4 sessions of the needling therapies targeting the patellar tendon over 8 weeks and was instructed to perform a unilateral eccentric exercise program of the quadriceps muscle on the affected side. Clinical and needle-related pain was assessed before, during, and after each treatment session using a visual analog scale.
Results: No differences were found between groups intra- or inter-session in terms of pain reduction (P = 0.424) despite clinical pain decreased in all groups since the first treatment session (P < 0.001). Furthermore, although the double-sham group showed a lower percentage of participants reporting needle-related pain during needle intervention (P = 0.005), the needle-related pain intensity after needle intervention was similar between groups (P = 0.682). Moreover, there were no group differences for the duration of pain sensation after any needle intervention (P = 0.184), extending in many cases beyond 24 h.
Conclusion: Needling therapies for individuals with patellar tendinopathy are prone to elicit placebo effects regarding clinical pain and nocebo effects regarding needling-related pain. Clinicians and physical therapists treating musculoskeletal pain conditions should consider the added value and potential mechanisms of action before routinely using needle techniques.
1 Introduction
Musculoskeletal painful disorders represent the primary contributor to rehabilitation needs and a major worldwide health problem (1). Patients with musculoskeletal painful disorders often seek a physiotherapist for assistance, and physiotherapists employ various therapeutic interventions, which are often complex, to reduce pain and disability (2). Ideally, specific treatment effects drive most of these changes, although non-specific effects such as regression to the mean, natural history, and contextual effects also contribute (3). Placebo effects can be described as beneficial effects that are not due to an active treatment components (4). and depends on contextual factors related to the reduction of symptoms caused by the psychosocial context, such as positive expectations or patient satisfaction, and not solely by the properties of the treatment itself (5). In contrast, nocebo effects are adverse treatment outcomes elicited by non-active treatment components (4) and are produced by negative expectations or context that may exacerbate the patient’s symptoms (6).
Clinically, placebo and nocebo effects are important during therapy administration, representing the result of the adjuvant or harmful use of contextual factors (7, 8). Information provided about treatment, patient expectations, previous encounters with a procedure, therapist characteristics, and the therapeutic relationship between the patient and the therapist can all generate these effects (8–13). While isolated placebo treatments seem to lack clinical meaningfulness, recent meta-analysis findings show that within the realm of non-pharmacological conservative interventions for musculoskeletal conditions, the placebo effect can contribute up to 30% of the minimally clinically important difference (14). Interestingly, the authors hypothesized that certain interventions such as needles or manual therapy may elicit even more substantial placebo effects. However, despite adequately-designed randomized controlled clinical trials that should include placebo controls to disentangle placebo and nocebo effects from the general effect of the intervention (15), only a very small proportion of randomized controlled clinical trials testing physiotherapy interventions do so (16).
In recent years, minimally invasive procedures for managing musculoskeletal painful disorders, such as dry needling (DN) or percutaneous needle electrolysis (PNE), have gained global popularity (17, 18). PNE is an invasive approach that involves applying a galvanic current through an acupuncture needle into the soft tissue lesion to elicit a local inflammatory response (19). Discomfort related to applying galvanic current could make PNE an unpleasant procedure for the patient. Indeed, the most common adverse effects of PNE, such as pain during the intervention and in the days following treatment, (18) are similar to those observed in DN (20). Furthermore, using needles as a therapeutic tool may cause a certain degree of apprehension in the patient, (20) and fear of needles or fear of pain could predispose the subject to react with negative emotions to pain and in anticipation of pain (21, 22). Conversely, it is unknown to what extent these interventions produce improvements in patients with musculoskeletal painful disorders due to non-specific effects such as placebo hypoalgesia. Placebo hypoalgesia is observed when a sham intervention results in pain relief and can also be acquired through operant conditioning. This uncertainty is probably due to the challenge that represents its evaluation represents, not only in needling interventions but in musculoskeletal interventions in general (15). Although the PNE technique has been compared with placebo interventions, the potential influence of the placebo effect on the results has not been considered (23).
Therefore, this study aimed to investigate the influence of potential placebo and nocebo effects on pain perception of an intratissue PNE-based intervention in individuals with patellar tendinopathy.
2 Material and methods
2.1 Study design and settings
This study was part of a three-arm randomized double-blinded controlled trial (ClinicalTrial.gov: NCT02498795) (24). The study followed the Helsinki Declaration and was approved by the local Ethics Committee (C.P.−C.I. PI15/0017), and all participants consented their enrolling in this study.
2.2 Participants
Adults aged between 18 and 45 years were recruited from various sports clubs and federations. To be eligible, participants had to meet specific inclusion criteria: (1) experienced anterior knee pain below the patella while engaging in sports for over 3 months; (2) engaged in sports activities at least 3 times a week; and (3) scored below 80 on the Victorian Institute of Sport Assessment-Patellar questionnaire (VISA-p). Exclusion criteria included: (1) knee surgery in the past 6 months; (2) patellar tendon corticosteroid injection in the past 3 months; (3) diagnosed with chronic joint disease; (4) contraindications for needling (e.g., needle phobia, needle material allergy); (5) consumption of anti-inflammatory, analgesic, or antibiotic medications within the past 48 h; and (6) undergoing concurrent physiotherapy treatment. Additionally, ultrasound examination of the knee joint and adjacent musculoskeletal structures was conducted before enrollment in the study. This examination aimed to exclude the presence of joint effusion or signs of inflammation and to identify the presence of degenerative signs, characterized by a hypoechoic area in the body of the tendon. None of the participants in the final selected sample had received prior needling treatment in the tendon.
2.3 Groups and interventions
Participants were divided into three groups according to the intervention received: (1) PNE [no-sham group], (2) sham PNE by using DN [single-sham group], and (3) sham PNE by using sham needles [double-sham group]. The setting and procedure followed with each participant was similar regardless of group, isolating the effects related to galvanic current and needling (Figure 1). All interventions were targeted at the patellar tendon.
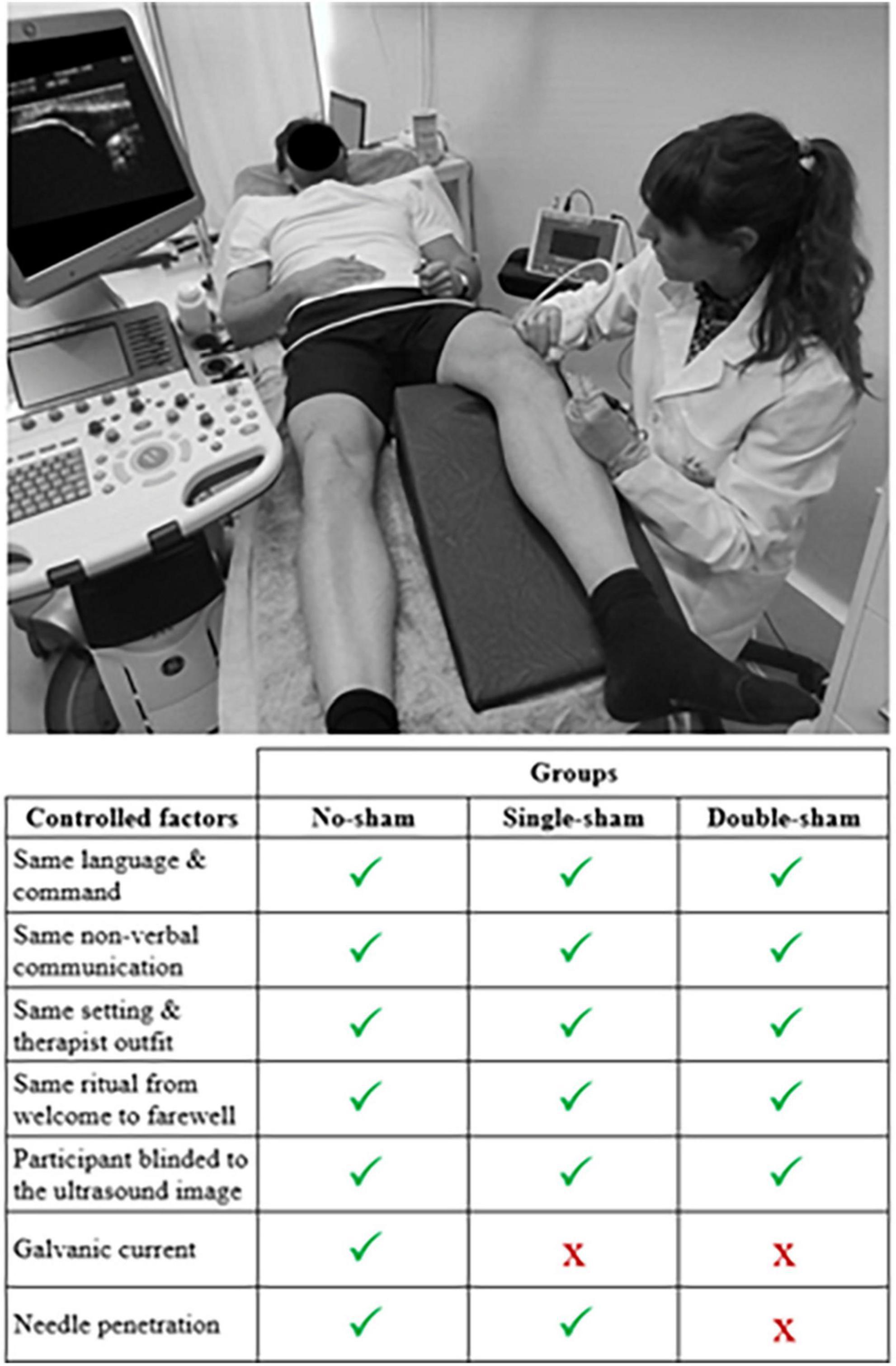
Figure 1. Illustration depicting the common setting and intervention procedures for all three groups, along with a list of controlled factors.
2.3.1 No-sham group
For the no-sham group, 0.25 × 0.25 mm needles (APS safety tube dry needles; Agupunt) were connected to the electrolysis device (model EPI®, CESMAR Electromedicina. S.L., Spain). The researcher utilized ultrasonography to guide the procedure, ensuring precise application to the injured area and maintaining safety. The needle was inserted into the injured area three times, targeting the hypoechoic region within the patellar tendon. Each insertion lasted 3 s and involved the use of 3 mA of galvanic current.
2.3.2 Single-sham group
In the single-sham group, the needle was inserted following the same protocol as in the no-sham group. The only difference was that the electrolysis device was turned on with a current intensity of 0 mA (i.e., no galvanic current). The needle reached the relevant treatment area in the patellar tendon guided by ultrasonography.
2.3.3 Double-sham group
For the double-sham group, a sham needle was placed upon the treatment zone, simulating the same procedure as in the other groups. In addition, the needle was manipulated in and out to simulate a real treatment. The holder had a cover over the bottom part to prevent the needle from contacting the skin.
2.4 Procedure
Participants underwent 4 intervention sessions over an 8-week period, with each session spaced 2 weeks apart. During each session, a standardized procedure was followed to ensure participant blinding during needle interventions, attempting to overcome biases found in previous studies on needling techniques (25). Participants were positioned supine with their knee flexed at 20°, supported by a pillow. The researcher performing the intervention wore latex gloves and cleansed the area with a 70% propan-2-ol antiseptic solution. A disposable protective cover was applied to a lubricated ultrasound probe (Logic S7 Expert, General Electric Healthcare), which was used for real-time ultrasound guidance. The ultrasound display screen was positioned behind the participants. Each participant held the anode connected to the electrolysis device and received the following instruction: “During the needle intervention, please try to remain still. The treatment may cause some pain or discomfort. If you experience any, please let me know, and I will stop immediately.” After needle removal, the area was gently compressed with cotton wool for 5 s (Figure 1).
At the end of the study, participants were asked via email to guess the type of treatment they received. The options provided were: “No needling treatment,” “Needling treatment,” or “I don’t know.” If participants selected “Needling treatment,” they were further asked to specify whether they received PNE or DN, with the options being “PNE,” “DN,” or “I don’t know.”
Complementary to the real or sham needle intervention, all participants were instructed to perform a unilateral eccentric exercise program of the quadriceps muscle on the affected side, specifically aimed at the patellar tendon. This program consisted of performing 3 sets of 15 repetitions daily on a decline board (26). The correct execution of the exercise as well as the follow-up of the prescribed program was monitored by the research team every two weeks, coinciding with the day the participant received the intervention.
2.5 Randomization
Participants who fulfilled the inclusion criteria and consented to participate in the trial were randomly assigned by a researcher not involved in the study by generating random participant sequences with a 1:1:1 allocation using an opaque envelope, with a block size of 15 participants, using a computer program (Randomizer).1
2.6 Outcome measures
Assessments were made by an assessor blinded to group allocation. The primary outcomes for placebo and nocebo effects were clinical pain reduction after needle intervention and needle-related pain intensity after needle intervention, respectively. While the secondary outcomes were clinical pain intensity before needle intervention, clinical pain intensity during a provocative test after needle intervention, needle-related pain during needle intervention, and days until needle-related pain sensation completely disappears after needle intervention. Outcome measures in this study are detailed in Table 1. Description and clinical findings in VISA-p and ultrasonographic measures after the 8-week period are available elsewhere (27).
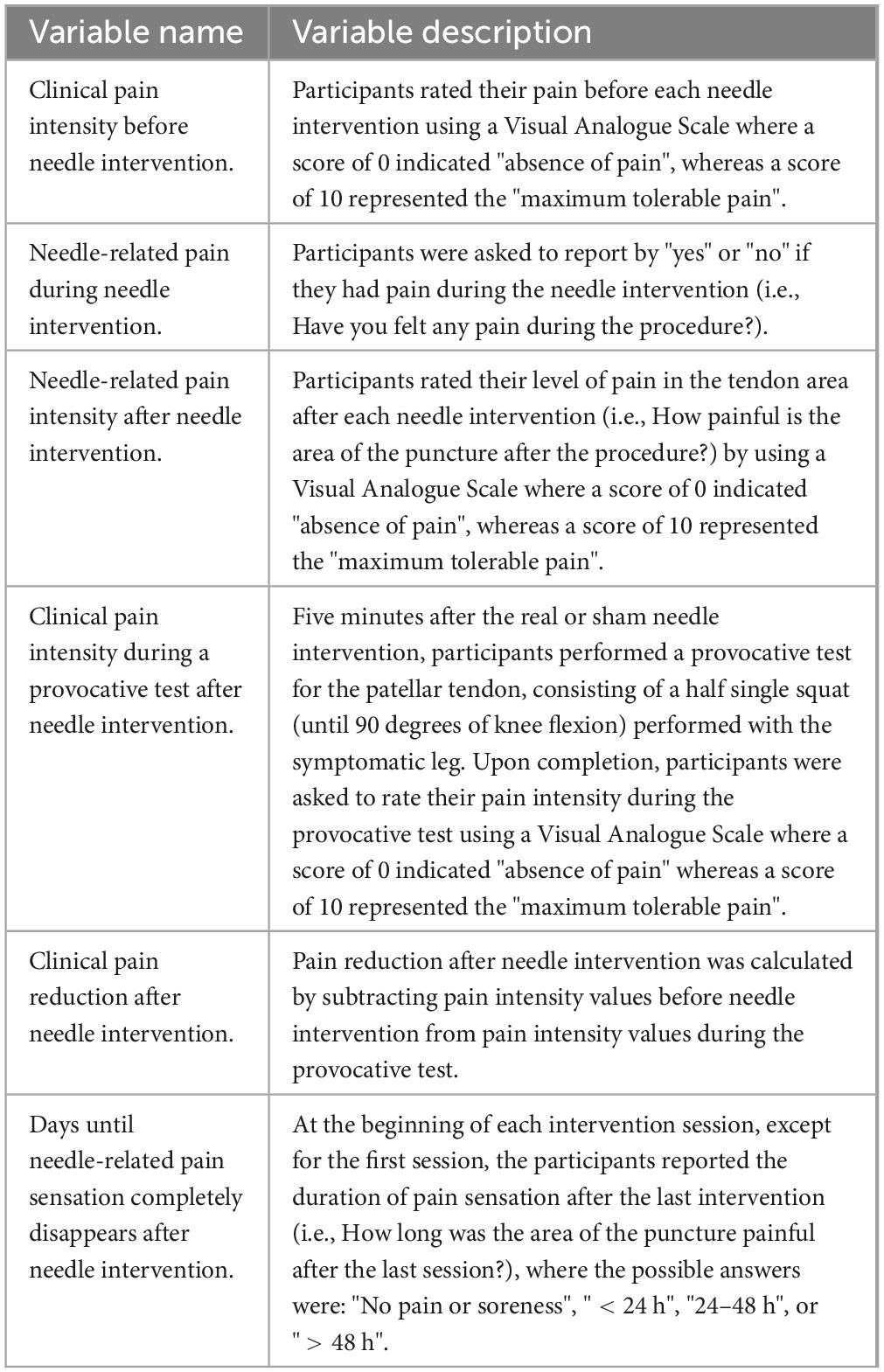
Table 1. Detailed description of the outcome variables included in the study.
2.7 Statistical analysis
Statistical analysis was performed using SPSS, v.25 (IBM Corp., Chicago, IL). A P-value < 0.05 was accepted as a significant difference between compared variables. Variables distribution was assessed using the Shapiro-Wilk test and described in percentage, mean and standard deviation or median and interquartile range, according to the distribution of data. Differences between groups were compared using chi-squared tests (χ2) for categorical data and mixed-model repeated-measures analysis of variance (RM-ANOVA) for continuous data with time (session 1, 2, 3, and 4) as within and group (no-sham group, single-sham group, and double-sham group) as between factors. Pairwise Bonferroni comparisons were performed as post hoc analyses.
2.8 Sample size calculation
The original sample size was calculated based on the VISA-p, and details were reported elsewhere (27). However, a secondary post hoc sample size calculation with G*Power (v3.1.9.2, Heinrich-Heine-University, Dusseldorf, Germany) revealed the feasible sample size for a mixed model RM-ANOVA with three groups (no-sham group, single-sham group, and double-sham group) participating in four experimental sessions. With a power of 90% and an alpha level of 0.01, a total of 42 participants (14 per group) were needed for participation to detect the minimal important difference of 1.2 points (partial η2 = 0.05) in the Visual Analogue Scale (28).
3 Results
Recruitment began in January 2019 and was completed in December 2019. Out of the 72 subjects assessed for eligibility, 5 declined to participate, while 19 did not meet eligibility criteria (24). A total of 48 participants (16 per group) were enrolled and received the allocated intervention. One participant in the no-sham group withdrew after the first session due to moving to another city and was subsequently removed from the statistical analysis. Figure 2 shows the study flowchart.
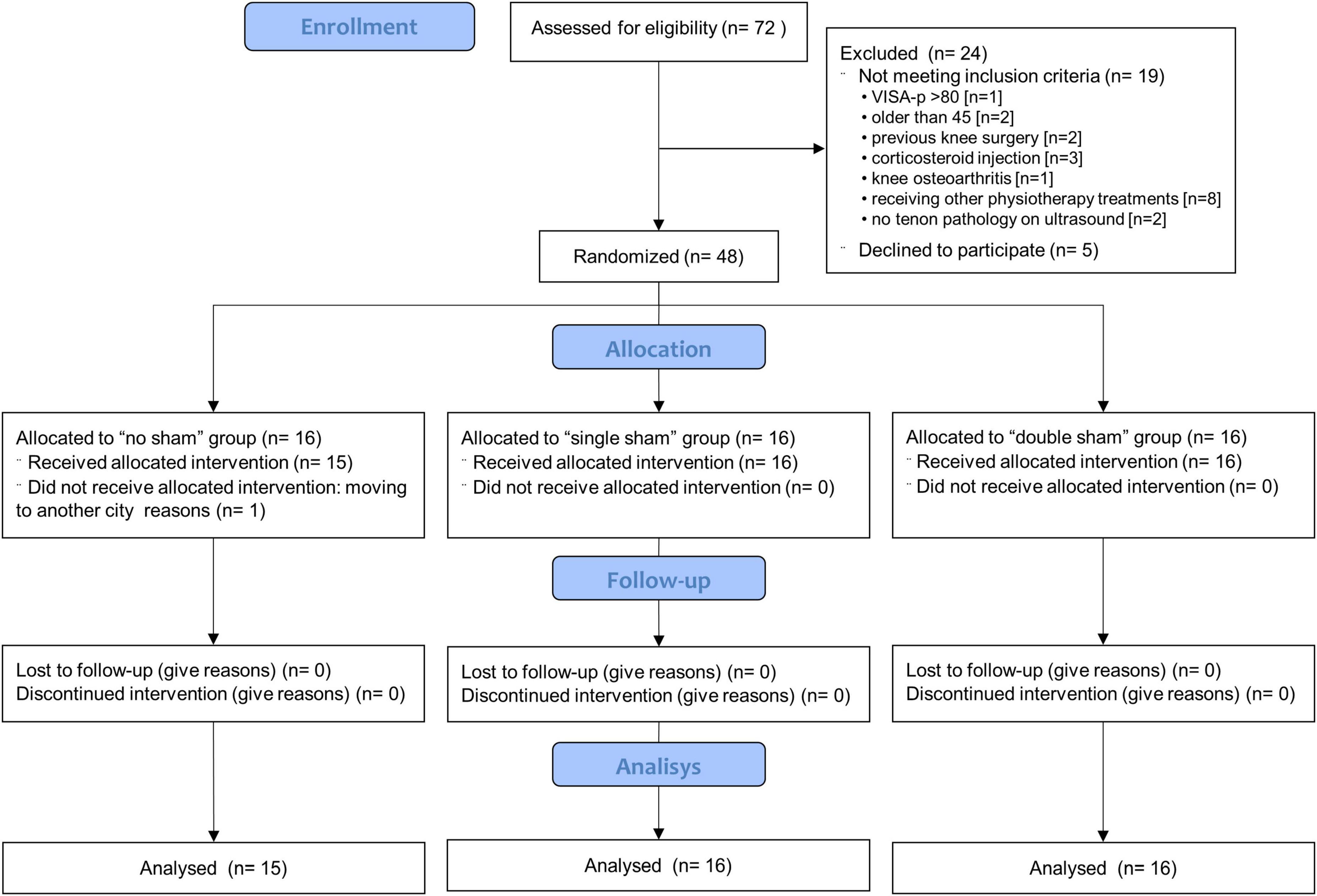
Figure 2. Participant flow chart. DN, dry needling group; PNE, Percutaneous needle electrolysis group.
Table 2 shows the characteristics of the 47 participants who completed the study. No significant differences were found between the groups regarding sociodemographic and clinical variables at baseline. Participants who completed the blinding questionnaire (n = 29; no-sham group: 12; single-sham group: 9, and double-sham group: 8) reported receiving a needle intervention, from which 82% (n = 23) indicated PNE as the needle intervention.
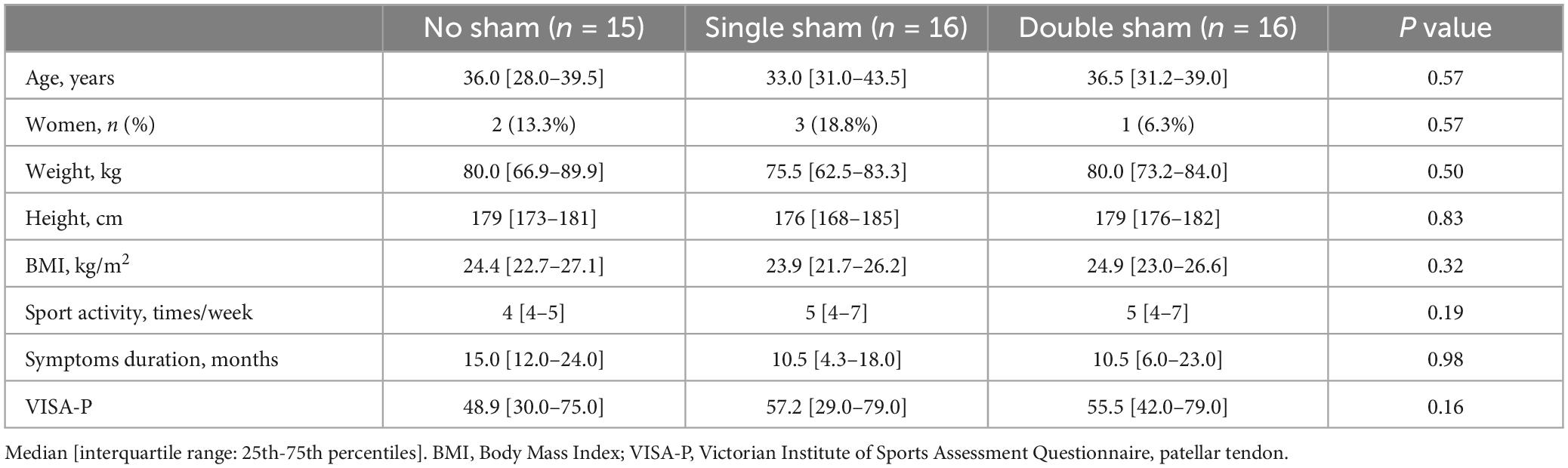
Table 2. Participant characteristics in the three study groups.
3.1 Clinical pain intensity before needle intervention
No time and group interaction (RM-ANOVA: F6,132 = 1.1; P = 0.357) was found for pain intensity before needle intervention, indicating no differences in the evolution of pain intensity between groups across sessions. However, a time effect was found (RM-ANOVA: F3,132 = 16.5; P < 0.001), indicating that the three groups decreased pain intensity over the sessions. Post-hoc analysis showed a lower pain intensity at the beginning of session 4 compared to session one in all groups (no-sham group: P < 0.001; single-sham group: P = 0.011, and double-sham group: P = 0.037). See Table 3.
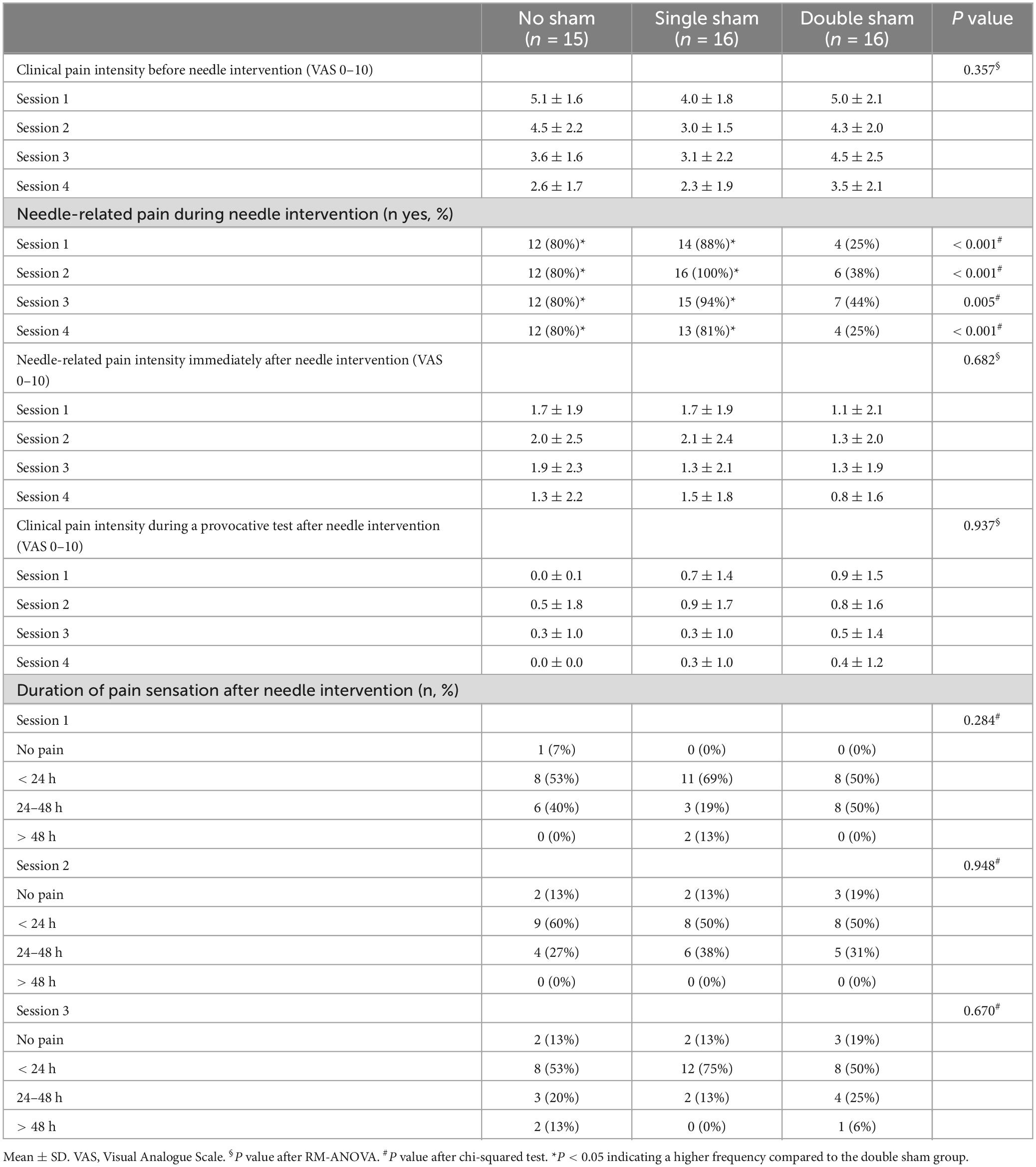
Table 3. Outcome measures in the three study groups.
3.2 Needle-related pain during needle intervention
Significant differences existed between the frequencies of participants reporting pain in the three groups during all the needle interventions (χ2 ≥ 10.6; P ≤ 0.005). Specifically, 80% of the no-sham group, 81% to 100% of the single-sham group, and 25% to 44% of the double-sham group reported pain during needle intervention. See Table 3.
3.3 Needle-related pain intensity immediately after needle intervention
No time and group interaction (RM-ANOVA: F6,132 = 0.7; P = 0.682) or time effect (RM-ANOVA: F3,132 = 1.7; P = 0.168) was found for pain intensity after needle intervention, indicating that the painful sensation after needle intervention was similar between groups in all sessions. See Table 3.
3.4 Clinical pain intensity during a provocative test after needle intervention
No time and group interaction (RM-ANOVA: F6,132 = 0.4; P = 0.937) or time effect (RM-ANOVA: F3,132 = 1.7; P = 0.179) was found for painful sensation after needle intervention, indicating that the painful sensation after needle intervention was similar between groups in all sessions. See Table 3.
3.5 Clinical pain reduction after needle intervention
No time and group interaction (RM-ANOVA: F6,132 = 1.0; P = 0.424) was found for pain reduction after needle intervention, indicating no differences in the evolution of pain reduction between groups across sessions. However, a time effect was found (RM-ANOVA: F3,132 = 6.3; P < 0.001), indicating that pain reduction within the three groups differed between sessions. Post hoc analysis showed a lower pain reduction at session 2 (P = 0.027) and session 4 (P = 0.001), compared to session 1 in all groups. See Figure 3.
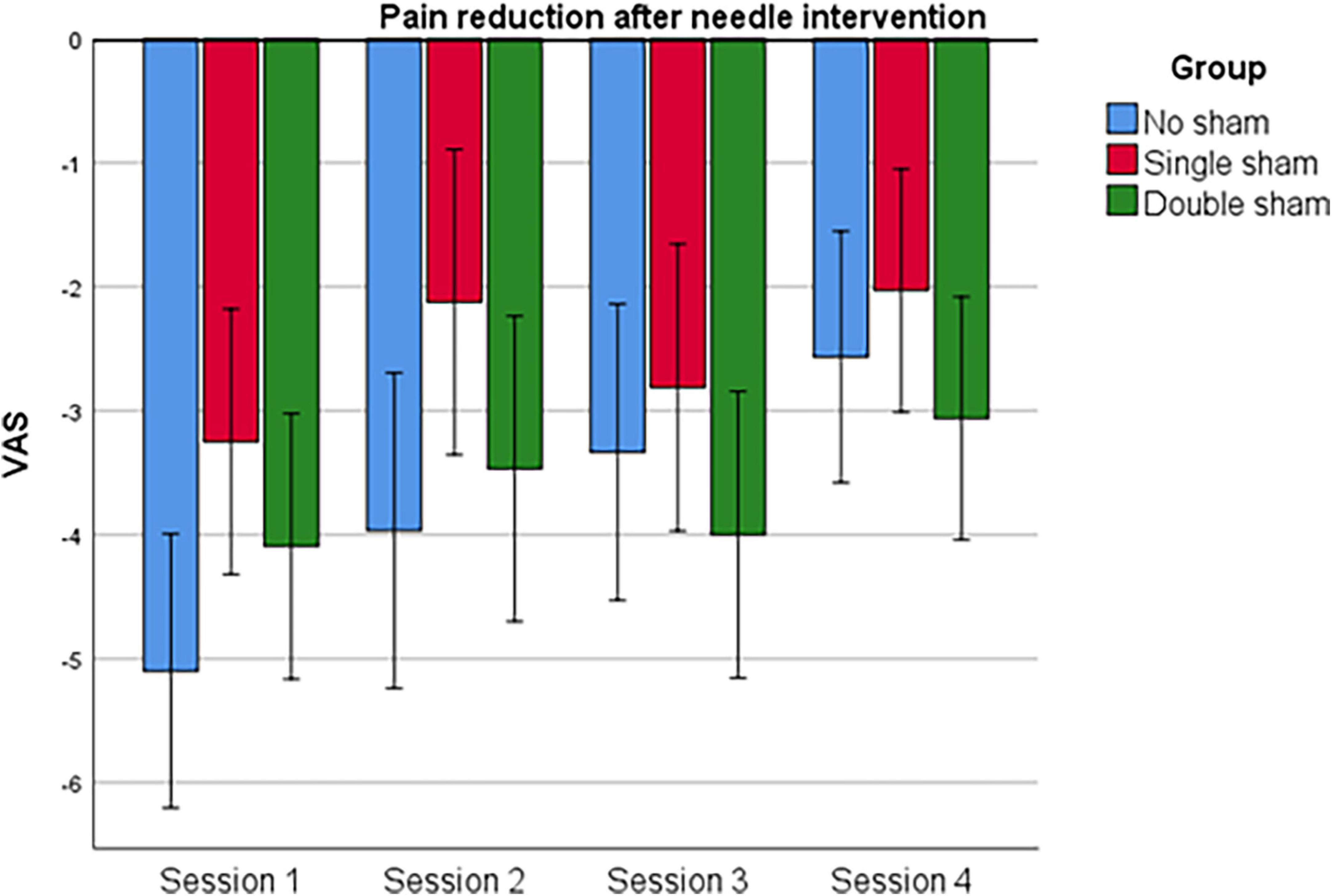
Figure 3. Clinical pain (tendon pain) reduction after the intervention.
3.6 Days until needle-related pain sensation completely disappears after needle intervention
There were no differences between the frequencies of participants reporting the duration of pain sensation after any needle intervention (χ2 ≤ 8.8; P ≥ 0.184). See Table 3.
3.7 Adverse effects
No adverse events were reported other than the previously described needle-related pain itself and the post-puncture pain described above, which were part of the outcome measures.
4 Discussion
This study is the first to investigate placebo and nocebo effects potentially associated with an invasive needle technique by implementing single-sham and double-sham procedures in individuals with patellar painful tendinopathy. The findings suggest that needling techniques, specifically PNE, induce significant placebo and nocebo effects on both clinical and needle-related pain, respectively.
4.1 Contextual effects in clinical tendon pain
The three groups similarly improving their pain over time, both at rest (before and after intervention) and during a functional provocative test, might reflect different effects. On the one hand, these findings might only indicate a direct positive effect of eccentric exercise on tendon pain, as previously reported (29). Furthermore, it is unlikely that there was no effect at all from the PNE intervention on pain, as previous studies have found a pain reduction effect in tendinopathies (18). Therefore, it is unlikely that eccentric exercise explains the clinical pain improvements observed in the three groups.
On the other hand, the persistence of patellar tendinopathy symptoms for 18 months in the present study, consistent with previous literature, (30) suggests that non-specific effects such as regression to the mean or natural history might partially explain the observed improvements in clinical pain. However, both the present study and previous literature show a high standard deviation in the duration of symptoms, either at the mean value or above. This substantial variability makes regression to the mean and natural history less likely to account for the clinical pain improvement observed in the three groups. Moreover, it is important to note that these non-specific factors would not explain the observed nocebo effect in needle-related pain. Therefore, it can be inferred that non-specific effects, such as placebo and nocebo responses, are at least partially responsible for the reduction in pain among patients with patellar tendinopathy undergoing needling therapies.
A recent study has shown that expectations may not play as significant role as prior therapeutic experiences in placebo and nocebo responses in healthy individuals (31). Although the connection between these non-specific effects and the psychological characteristics of the participants remains unknown, a recent study with high methodological quality and one of the largest samples in placebo research has shown that individuals with chronic pain benefiting from placebo are characterized by low emotional stress, pain-related fear, and catastrophizing (5). However, catastrophizing has been linked to patellar tendinopathy only in individuals with more severe symptoms (32). The present study, based on the baseline pain VAS values of participants, indicates that in most cases, tendinopathies were moderate to low. Therefore, it can be hypothesized that the sample in the current study did not have a high psychological burden and were more likely to benefit from placebo effects.
4.2 Contextual effects in needling-related pain
As expected, most participants reported pain during the intervention when a needle was inserted into the tendon. Interestingly, up to 44% of participants in the double-sham group also reported pain during intervention. Furthermore, all groups reported the same amount of needle-related pain immediately after the intervention, and up to 25% of participants in the double-sham group continued experiencing pain even 24-48h after the intervention. Overall, these findings indicate that needling interventions are susceptible to non-specific effects, aligning with previous literature (33).
Although not measured on participants, subjective factors such as expectations may have modulated pain (34) after the needling intervention (35). Increased pain due to the expectation of more pain following an intervention is a nocebo effect observed previously (36, 37). A study in patients with chronic shoulder pain found increased mechanical hyperalgesia immediately following sham dry needling that lasted for 24h in individuals with shoulder pain. The study attributed these changes to a nocebo effect generated by negative expectations associated with the instructions given before the procedure (38). In addition to negative expectations, other factors that might have mediated a nocebo effect in post needling-related pain include classical conditioning, observational learning, (39) and prior therapeutic experiences (31).
4.3 Clinical implications
These findings clearly reflect that needling interventions in individuals with patellar tendinopathy involve intrinsic positive and negative non-specific factors. Therefore, the contextual factors of needling therapies can trigger both placebo and nocebo responses and must be considered in the clinical context. This serves as a general recommendation for physiotherapists and musculoskeletal clinicians, who are encouraged to understand and manage the contextual factors [e.g., patients’ expectations, past treatments, verbal suggestions (40)] that enhance placebo effects and avoid nocebo effects (2, 41).
In this context, it has been shown that individuals with low back pain who received an intense briefing on the adverse side effects of acupuncture tended to exhibit a higher adverse side effect score compared to participants who received a regular adverse side effect briefing (42). However, other studies did not find a significant effect of patient expectations on the short-term effects of DN on pain intensity and pain-inducing stimulus intensities in people with neck pain; (43) or showed that DN treatment can produce beneficial effects on neck pain and tissue mechanosensitivity, regardless of whether participants received a positive, negative, or neutral verbal stimulus before treatment (44).
All participants in the current study experienced post-DN soreness that did not influence treatment outcomes. Interestingly, participants were not very concerned about post-needling soreness as long as their clinical pain complaint decreased. Therefore, it seems that briefings about treatment in routine care might not be as important as previously thought (42). Other variables, such as previous therapeutic experiences (31) or patient satisfaction, might also be important for clinically managing placebo and nocebo effects, as these are factors that can impact the outcome of rehabilitation (45). Indeed, according to several double-blind trials testing pain treatments, the placebo effect can be similar to specific treatment effects (9). In summary, current research on placebo effects indicates that the ethical enhancement of a placebo without using placebos or misinforming patients is feasible and ethical.
4.4 Limitations
This study did not control for demand characteristics, (46) potentially influencing results as participants may have guessed evaluator’s expectations. Including measures of psychological factors such as fear, emotional stress, catastrophizing, and participants’ satisfaction or subjective perception of improvement as indirect measures of the expectations, would have strengthened the study design. This would have allowed ascribing the consistent placebo and nocebo effects found to specific contextual factors. Future studies should explore placebo and nocebo effects in other needle-based techniques for the treatment of musculoskeletal pain.
5 Conclusion
The results of this research show that needling therapies for individuals with patellar tendinopathy are prone to elicit placebo and nocebo effects regarding clinical and needling-related pain, respectively. Future studies involving participants with musculoskeletal painful disorders should incorporate placebo-controlled designs and monitor both clinical and needling-related pain during the treatment period. Additionally, given the clear presence of these effects, physiotherapists and musculoskeletal clinicians are encouraged to delve into the knowledge of placebo and nocebo to better manage their patients with tendinopathies.
Data availability statement
The original contributions presented in this study are included in this article/Supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by the Comité de Ética de la Investigación de la Comunidad Autónoma de Aragón (C.P.−C.I. PI15/0017). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
VD-G: Conceptualization, Funding acquisition, Investigation, Resources, Writing−original draft, Writing−review and editing. DP-M: Validation, Writing−original draft, Writing−review and editing. JB-A: Conceptualization, Investigation, Visualization, Writing−review and editing. PB-L: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Software, Supervision, Validation, Writing−original draft, Writing−review and editing. ML-P: Conceptualization, Data curation, Investigation, Methodology, Project administration, Resources, Supervision, Writing−original draft, Writing−review and editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of the article. VD-G, JB-A, PB-L, and ML-R are members of the research group MOTUS supported by “Gobierno de Aragón” (n. B60_23D). Julia Blasco-Abadía is supported by the Grant PIF 2022-2026 from “Gobierno de Aragón”. The funders did not have any role in the study.
Conflict of interest
The reviewer MG-A declared a shared affiliation, with no collaboration, with one of the authors DP-M to the handling editor at the time of the review.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2024.1381515/full#supplementary-material
Footnotes
References
1. Cieza A, Causey K, Kamenov K, Hanson SW, Chatterji S, Vos T. Global estimates of the need for rehabilitation based on the global burden of disease study 2019: A systematic analysis for the global burden of disease study 2019. Lancet. (2021) 396:2006–17. doi: 10.1016/s0140-6736(20)32340-0
2. Testa M, Rossettini G. Enhance placebo, avoid nocebo: How contextual factors affect physiotherapy outcomes. Manual Ther. (2016) 24:65–74. doi: 10.1016/j.math.2016.04.006
3. Zou K, Wong J, Abdullah N, Chen X, Smith T, Doherty M, et al. Examination of overall treatment effect and the proportion attributable to contextual effect in osteoarthritis: Meta-analysis of randomised controlled trials. Ann Rheum Dis. (2016) 75:1964–70. doi: 10.1136/annrheumdis-2015-208387
4. Meeuwis SH, van Middendorp H, van Laarhoven AIM, van Leijenhorst C, Pacheco-Lopez G, Lavrijsen APM, et al. Placebo and nocebo effects for itch and itch-related immune outcomes: A systematic review of animal and human studies. Neurosci Biobehav Rev. (2020) 113:325–37. doi: 10.1016/j.neubiorev.2020.03.025
5. Wang Y, Chan E, Dorsey SG, Campbell CM, Colloca L. Who are the placebo responders? A cross-sectional cohort study for psychological determinants. Pain. (2022) 163:1078–90. doi: 10.1097/j.pain.0000000000002478
6. Blasini M, Corsi N, Klinger R, Colloca L. Nocebo and pain: An overview of the psychoneurobiological mechanisms. Pain Rep. (2017) 2:e585. doi: 10.1097/pr9.0000000000000585
7. Chavarria V, Vian J, Pereira C, Data-Franco J, Fernandes BS, Berk M, et al. The placebo and nocebo phenomena: Their clinical management and impact on treatment outcomes. Clin Ther. (2017) 39:477–86. doi: 10.1016/j.clinthera.2017.01.031
8. Rossettini G, Geri T, Palese A. What physiotherapists specialized in orthopedic manual therapy know about nocebo-related effects and contextual factors: Findings from a national survey. Front Psychol. (2020) 11:582174. doi: 10.3389/fpsyg.2020.582174
9. Colloca L, Barsky AJ. Placebo and nocebo effects. N Engl J Med. (2020) 382:554–61. doi: 10.1056/NEJMra1907805
10. Bialosky JE, George SZ, Horn ME, Price DD, Staud R, Robinson ME. Spinal manipulative therapy-specific changes in pain sensitivity in individuals with low back pain (NCT01168999). J Pain. (2014) 15:136–48. doi: 10.1016/j.jpain.2013.10.005
11. Bishop MD, Mintken PE, Bialosky JE, Cleland JA. Patient expectations of benefit from interventions for neck pain and resulting influence on outcomes. J Orthop Sports Phys Ther. (2013) 43:457–65. doi: 10.2519/jospt.2013.4492
12. Riley SP, Bialosky J, Cote MP. Thoracic spinal manipulation for musculoskeletal shoulder pain: Can an instructional set change patient expectation and outcome? Manual Ther. (2015) 20:469–74. doi: 10.1016/j.math.2014.11.011
13. Rossettini G, Palese A, Geri T, Fiorio M, Colloca L, Testa M. Physical therapists’ perspectives on using contextual factors in clinical practice: Findings from an Italian national survey. PLoS One. (2018) 13:e0208159. doi: 10.1371/journal.pone.0208159
14. Saueressig T, Owen PJ, Pedder H, Arora NK, Simons M, Kaczorowski S, et al. The importance of context (placebo effects) in conservative interventions for musculoskeletal pain: A systematic review and meta-analysis of randomized controlled trials. Eur J Pain. (2023) 28:675–704. doi: 10.1002/ejp.2222
15. Cashin AG, McAuley JH, Lamb SE, Lee H. Disentangling contextual effects from musculoskeletal treatments. Osteoarthrit Cartil. (2021) 29:297–9. doi: 10.1016/j.joca.2020.12.011
16. Cashin AG, Lee H, Bagg MK, O’Hagan E, Traeger AC, Kamper SJ, et al. A systematic review highlights the need to improve the quality and applicability of trials of physical therapy interventions for low back pain. J Clin Epidemiol. (2020) 126:106–15. doi: 10.1016/j.jclinepi.2020.06.025
17. Romero-Morales C, Bravo-Aguilar M, Abuín-Porras V, Almazán-Polo J, Calvo-Lobo C, Martínez-Jiménez EM, et al. Current advances and novel research on minimal invasive techniques for musculoskeletal disorders. Dis Mon. (2021) 67:101210. doi: 10.1016/j.disamonth.2021.101210
18. Gómez-Chiguano GF, Navarro-Santana MJ, Cleland JA. Effectiveness of ultrasound-guided percutaneous electrolysis for musculoskeletal pain: A systematic review and meta-analysis. Pain Med. (2021) 22:1055–71. doi: 10.1093/pm/pnaa342
19. Valera-Garrido F, Minaya-Muñoz F, Medina-Mirapeix F. Ultrasound-guided percutaneous needle electrolysis in chronic lateral epicondylitis: Short-term and long-term results. Acupunct Med. (2014) 32:446–54. doi: 10.1136/acupmed-2014-010619
20. Brady S, McEvoy J, Dommerholt J, Doody C. Adverse events following trigger point dry needling: A prospective survey of chartered physiotherapists. J Man Manip Ther. (2014) 22:134–40. doi: 10.1179/2042618613y.0000000044
21. Aslaksen PM, Lyby PS. Fear of pain potentiates nocebo hyperalgesia. J Pain Res. (2015) 8:703–10. doi: 10.2147/jpr.S91923
22. McLenon J, Rogers MAM. The fear of needles: A systematic review and meta-analysis. J Adv Nurs. (2019) 75:30–42. doi: 10.1111/jan.13818
23. Fernández-Rodríguez T, Fernández-Rolle Á, Truyols-Domínguez S, Benítez-Martínez JC, Casaña-Granell J. Prospective randomized trial of electrolysis for chronic plantar heel pain. Foot Ankle Int. (2018) 39:1039–46. doi: 10.1177/1071100718773998
24. López-Royo MP, Ríos-Díaz J, Galán-Díaz RM, Herrero P, Gómez-Trullén EM. A comparative study of treatment interventions for patellar tendinopathy: A randomized controlled trial. Arch Phys Med Rehabil. (2021) 102:967–75. doi: 10.1016/j.apmr.2021.01.073
25. Braithwaite FA, Walters JL, Li LSK, Moseley GL, Williams MT, McEvoy MP. Blinding strategies in dry needling trials: Systematic review and meta-analysis. Phys Ther. (2019) 99:1461–80. doi: 10.1093/ptj/pzz111
26. Alfredson H, Pietilä T, Jonsson P, Lorentzon R. Heavy-load eccentric calf muscle training for the treatment of chronic achilles tendinosis. Am J Sports Med. (1998) 26:360–6. doi: 10.1177/03635465980260030301
27. López-Royo MP, Gómez-Trullén EM, Ortiz-Lucas M, Galán-Díaz RM, Bataller-Cervero AV, Al-Boloushi Z, et al. Comparative study of treatment interventions for patellar tendinopathy: A protocol for a randomised controlled trial. BMJ Open. (2020) 10:e034304. doi: 10.1136/bmjopen-2019-034304
28. Challoumas D, Zouvani A, Creavin K, Murray E, Crosbie G, Ng N, et al. Determining minimal important differences for patient-reported outcome measures in shoulder, lateral elbow, patellar and Achilles tendinopathies using distribution-based methods. BMC Musculoskelet Disord. (2023) 24:158. doi: 10.1186/s12891-023-06261-9
29. Burton I. Interventions for prevention and in-season management of patellar tendinopathy in athletes: A scoping review. Phys Ther Sport. (2022) 55:80–9. doi: 10.1016/j.ptsp.2022.03.002
30. Zwerver J, Bredeweg SW, van den Akker-Scheek I. Prevalence of Jumper’s knee among nonelite athletes from different sports: A cross-sectional survey. Am J Sports Med. (2011) 39:1984–8. doi: 10.1177/0363546511413370
31. Colloca L, Akintola T, Haycock NR. Prior therapeutic experiences, not expectation ratings, predict placebo effects: An experimental study in chronic pain and healthy participants. Psychother Psychosom. (2020) 89:371–8. doi: 10.1159/000507400
32. Slagers AJ, van Veen E, Zwerver J, Geertzen JHB, Reininga IHF, van den Akker-Scheek I. Psychological factors during rehabilitation of patients with Achilles or patellar tendinopathy: A cross-sectional study. Phys Ther Sport. (2021) 50:145–52. doi: 10.1016/j.ptsp.2021.04.010
33. Ho RST, Ho FF, Adams J, Cramer H, Leung B, Ward L, et al. Patients’ perceptions on non-specific effects of acupuncture: Qualitative comparison between responders and non-responders. Integr Med Res. (2022) 11:100771. doi: 10.1016/j.imr.2021.100771
34. Damien J, Colloca L, Bellei-Rodriguez C, Marchand S. Pain modulation: From conditioned pain modulation to placebo and nocebo effects in experimental and clinical pain. Int Rev Neurobiol. (2018) 139:255–96. doi: 10.1016/bs.irn.2018.07.024
35. Musial F. Acupuncture for the treatment of pain – A mega-placebo? Front Neurosci. (2019) 13:1110. doi: 10.3389/fnins.2019.01110
36. Petersen GL, Finnerup NB, Colloca L, Amanzio M, Price DD, Jensen TS, et al. The magnitude of nocebo effects in pain: A meta-analysis. Pain. (2014) 155:1426–34. doi: 10.1016/j.pain.2014.04.016
37. Lorenz J, Hauck M, Paur RC. Cortical correlates of false expectations during pain intensity judgments–a possible manifestation of placebo/nocebo cognitions. Brain Behav Immun. (2005) 19:283–95. doi: 10.1016/j.bbi.2005.03.010
38. Laramée A, Léonard G, Morin M, Roch M, Gaudreault N. Neurophysiological and psychophysical effects of dry versus sham needling of the infraspinatus muscle in patients with chronic shoulder pain: A randomized feasibility study. Arch Physiother. (2021) 11:23. doi: 10.1186/s40945-021-00118-x
39. Colloca L. Placebo, nocebo, and learning mechanisms. Handb Exp Pharmacol. (2014) 225:17–35. doi: 10.1007/978-3-662-44519-8_2
40. Rossettini G, Carlino E, Testa M. Clinical relevance of contextual factors as triggers of placebo and nocebo effects in musculoskeletal pain. BMC Musculoskelet Disord. (2018) 19:27. doi: 10.1186/s12891-018-1943-8
41. Hohenschurz-Schmidt D, Thomson OP, Rossettini G, Miciak M, Newell D, Roberts L, et al. Avoiding nocebo and other undesirable effects in chiropractic, osteopathy and physiotherapy: An invitation to reflect. Musculoskelet Sci Pract. (2022) 62:102677. doi: 10.1016/j.msksp.2022.102677
42. Barth J, Muff S, Kern A, Zieger A, Keiser S, Zoller M, et al. Effect of briefing on acupuncture treatment outcome expectations, pain, and adverse side effects among patients with chronic low back pain: A randomized clinical trial. JAMA Netw Open. (2021) 4:e2121418. doi: 10.1001/jamanetworkopen.2021.21418
43. Gallego-Sendarrubias GM, Voogt L, Arias-Buría JL, Bialosky J, Fernández-de-Las-Peñas C. Can patient expectations modulate the short-term effects of dry needling on sensitivity outcomes in patients with mechanical neck pain? A randomized clinical trial. Pain Med. (2022) 23:965–76. doi: 10.1093/pm/pnab134
44. Almaee Nejad F, Dommerholt J, Attarbashi Moghadam B, Shadmehr A, Khazaei Pour Z. Impact of physical therapists’ instructions on function and the perception of post-dry needling soreness in mechanical cervical pain; a randomized clinical trial. J Bodyw Mov Ther. (2020) 24:118–23. doi: 10.1016/j.jbmt.2020.06.023
45. Iolascon G, Moretti A. Myths and truths about placebo effect in rehabilitation for musculoskeletal pain. Adv Ther. (2021) 38:4995–5001. doi: 10.1007/s12325-021-01894-5
Keywords: placebo, nocebo, needling techniques, percutaneous needle electrolysis, dry needling, tendinopathy
Citation: Doménech-García V, Pecos-Martín D, Blasco-Abadía J, Bellosta-López P and López-Royo MP (2024) Placebo and nocebo effects of percutaneous needle electrolysis and dry-needling: an intra and inter-treatment sessions analysis of a three-arm randomized double-blinded controlled trial in patients with patellar tendinopathy. Front. Med. 11:1381515. doi: 10.3389/fmed.2024.1381515
Received: 03 February 2024; Accepted: 23 May 2024;
Published: 06 June 2024.
Edited by:
Metoda Lipnik-Stangelj, Faculty of Medicine, University of Ljubljana, SloveniaReviewed by:
Mónica Grande-Alonso, University of Alcalá, SpainJosé Luis Arias Buría, Rey Juan Carlos University, Spain
Raúl Ferrer-Peña, La Salle University Center, Spain
Copyright © 2024 Doménech-García, Pecos-Martín, Blasco-Abadía, Bellosta-López and López-Royo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Pablo Bellosta-López, cGJlbGxvc3RhQHVzai5lcw==