 Brian Alejandro Cáceres Munar1Adriana Urbina2Tatiana Ortíz3Ayda Rodríguez3Olga Lucía Fernández4Luisa Fernanda Ospina5Iris Flórez6Dora Uribe7Celia Alvarado8Eliana Patricia Calvo1
Brian Alejandro Cáceres Munar1Adriana Urbina2Tatiana Ortíz3Ayda Rodríguez3Olga Lucía Fernández4Luisa Fernanda Ospina5Iris Flórez6Dora Uribe7Celia Alvarado8Eliana Patricia Calvo1 Félix Giovanni Delgado1*
Félix Giovanni Delgado1* Jaime Eduardo Castellanos1
Jaime Eduardo Castellanos1- 1Grupo de Virología, Vicerrectoría de Investigaciones, Universidad El Bosque, Bogotá, Colombia
- 2Fundación Universitaria Sanitas, Bogotá, Colombia
- 3Banco Nacional de Sangre Cruz Roja Colombiana, Bogotá, Colombia
- 4Banco de Sangre Quindío, Cruz Roja Colombiana, Armenia, Colombia
- 5Hemocentro Valle del Cauca, Cruz Roja Colombiana, Cali, Colombia
- 6Banco de Sangre Bolívar, Cruz Roja Colombiana, Cartagena, Colombia
- 7Hemocentro del Café, Cruz Roja Colombiana, Manizales, Colombia
- 8Banco de Sangre Antioquia, Cruz Roja Colombiana, Medellín, Colombia
Objective: Arboviruses pose a challenge in ensuring the supply of pathogen-free blood components because they are not routinely screened in blood banks, and blood components from infected asymptomatic donors could be transfused. This study aimed to detect and characterize arboviral infections in Colombian blood donors.
Methods: In a cross-sectional study, the prevalence of dengue (DENV), Zika (ZIKV), and chikungunya (CHIKV) viruses and co-infections of blood donors were compared between an epidemic period (November 2019–February 2020, n = 462) and an endemic period (November 2021–August 2022, n = 1,119). Viral RNA from each donor serum was purified, and the viruses were detected using a previously standardized multiplex hemi-nested RT-PCR protocol. Subsequently, donors who tested positive were surveyed 15 days after the detection of the virus to identify clinical characteristics related to the arboviral infection. The prevalences of each virus were presented as percentages and compared between epidemic and endemic periods.
Results: Significantly higher prevalences were found in the epidemic period compared with the endemic period for DENV (14.5 vs. 1.9%), ZIKV (7.8 vs. 0.3%), CHIKV (8 vs. 3.3%), and co-infections (4.3 vs. 0.2%). The survey response rate of positive donors in the two periods was 83/175 (47%). In total, 57% of the donors surveyed were asymptomatic. Symptomatic donors most frequently reported headache (31%), malaise (13%), arthralgia (10%), and fever/chills (8%).
Conclusion: The prevalence observed in epidemic and endemic periods was higher than that reported in other studies in the Americas. The high proportion of asymptomatic cases found, in addition to the mild and nonspecific manifestations among the symptomatic, may limit the effectiveness of the donor selection criteria used to mitigate the risk of transfusion-transmitted arboviruses.
1 Introduction
Dengue (DENV), Zika (ZIKV), and chikungunya (CHIKV) are positive-strand RNA viruses (1–3) that cause a broad spectrum of clinical manifestations in the host (4–6). These viruses are classified as arboviruses and are generally transmitted through the bite of infected female Aedes mosquitoes. However, transfusion-transmitted infection (TTI) has recently been established as an alternative transmission route for these viruses, posing potential public health risks (7–10). Key factors such as the high rate of subclinical infections (11–13) and the high viral loads detected in infected blood donors support this assertion (14–20).
Since 2009, the Association for the Advancement of Blood and Biotherapies (AABB) has listed emerging infectious agents and classified them based on their potential risk for blood safety (9). According to the AABB, DENV has the highest priority level (red) due of to its potentially severe clinical outcomes when transmitted through blood transfusion. CHIKV is also included but at a lower priority level (orange). In addition, ZIKV was included (21) because its active transmission has been reported in 58 countries, and probable transfusion transmission cases have been disclosed in French Polynesia and Brazil (22–24).
Over the last 20 years, a significative circulation of arbovirus in blood donors has been documented during epidemics, with 5.5% of donors positive for DENV RNA in Saudi Arabia (25), 2.8% positive for ZIKV RNA in French Polynesia (26), and 1.9% positive for CHIKV in Puerto Rico (20). Moreover, infectious DENV and transmission cases have been associated with plasma, red blood cells, and platelet transfusions (27, 28). In contrast, transfusion transmission of ZIKV has only been observed during platelet transfusion (23). Although transfusion-transmitted cases of CHIKV infection have not been reported yet, it is considered a high-risk virus for future TTIs because of the high levels of viremia in asymptomatic infected donors (29).
Colombia is a hyperendemic country in which all four DENV serotypes, CHIKV, and ZIKV (30) circulate, and the Aedes aegypti vector is present in more than 90% of the territory (30). Therefore, it is estimated that more than half of the Colombian population is at risk of being infected by these arboviruses (31), especially during outbreaks that occur during periods of drought and high temperatures (32). To date, five dengue outbreaks (1998, 2002, 2010, 2013, and 2019), one CHIKV outbreak (2016), and one ZIKV outbreak (2015) have been reported in the country (33–35). Indeed, during the most recent DENV outbreak in 2019, 124,989 cases were reported, of which 48.1% had dengue without warning signs, 50.8% presented dengue without warning signs, and 1.1% had severe dengue (36). Hence, dengue fever is the most prevalent vector-borne viral disease in the country, with more than 1,500,000 cases registered from 1990 to 2016 (31), followed by CHIKV with over 460,000 cases (37–39) and ZIKV with over 100,000 confirmed cases (40).
Although no cases of arbovirus transmission by blood transfusion have been reported yet in Colombia, information should be collected to inform future public health policies. This study aimed to identify and characterize DENV, ZIKV, and CHIKV infections in blood donors residing in endemic and nonendemic cities who visited blood banks within the Colombian Red Cross network during the most recent dengue outbreak and a subsequent DENV endemic period. Our results showed a high prevalence of all these viruses, although DENV and CHIKV were the most frequently reported viruses during both epidemiological periods. Moreover, a clinical and epidemiological survey of the infected blood donors showed that many cases were asymptomatic and that among the symptomatic cases, the clinical manifestations were mild and nonspecific.
2 Materials and methods
2.1 Serum samples
A total of 1,581 serum samples from accepted blood donors were collected from six blood banks across Colombia in hyperendemic cities located below 1,800 m above sea level (m.a.s.l.) (Armenia, Cali, Cartagena, and Medellín) and those located above 1,800 m.a.s.l. (Bogotá and Manizales). Each blood bank collects blood from these cities and their nearby municipalities. Acceptability for blood donation was determined according to the National Technical Guideline for the Selection of Blood Donors (41). The blood donors provided informed consent for blood donation and collection of an additional blood sample to detect arboviruses. The Universidad El Bosque Institutional Ethics Committee approved this study.
During blood donation, 7 mL of blood were collected using a yellow cap tube to obtain serum. Sera from blood donors were stored in each blood bank at a temperature between −20 and − 30°C and sent to the Instituto de Virología at the Universidad El Bosque in the capital city, Bogotá, for processing within 7 days after collection.
Sera were sampled during two different periods: First, during a dengue outbreak from November 2019 to February 2020 (n = 462); second, during a dengue endemic period from November 2021 to August 2022 (n = 1,119; Table 1). Samples were classified as coming from an endemic or nonendemic area for arboviruses, according to the altitude above sea level of the donation site. In Colombia, it has been shown that the Aedes aegypti vector infected with at least one arbovirus circulates up to 1,984 m.a.s.l. (42). Therefore, samples collected between 0 and 1,984 m.a.s.l. were classified as coming from arbovirus-endemic areas, whereas those collected at higher altitudes were classified as coming from nonendemic areas.
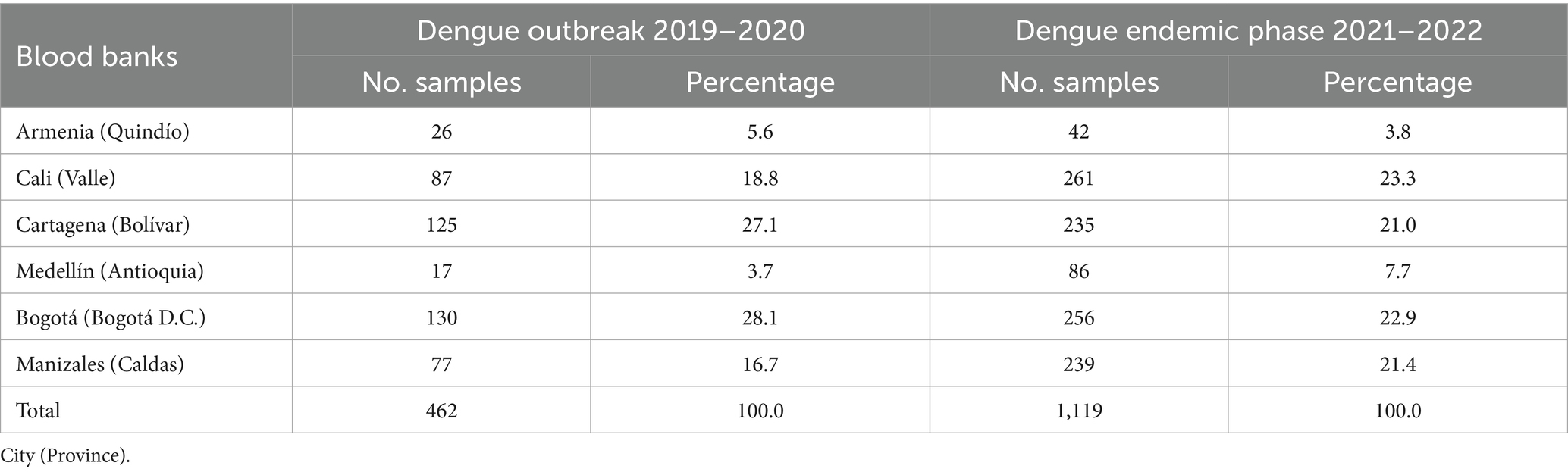
Table 1. Origin and distribution of serum samples from accepted blood donors for arboviral detection.
2.2 One-step hemi-nested RT-PCR for DENV, ZIKV, and CHIKV simultaneous detection
A volume of 200 μL of serum was used to purify RNA using a commercial DNA/RNA Virus Mini Kit (Stratec). Culture supernatants (200 μL) from DENV-infected C6/36 cells (DENV-1 S24, DENV-2 S3, DENV-3 S7, and DENV-4 S29 strains) and ZIKV (COL8565 strain)- or CHIKV (COL7624 strain)-infected Vero cells were used as positive controls. These viral isolates had undergone an adaptation process involving 4–5 passages. Purified arboviral RNA was amplified using a one-step multiplex hemi-nested RT-PCR (hnRT-PCR) previously described by our group (43). Briefly, the first round of amplification was performed using a final volume of 20 μL using Luna Universal Probe One-Step RT-qPCR (NEB), 5 μL of template RNA (60–80 ng/μL), and 0.2 μM of each primer (a total of six primers). The amplification temperatures were 15 min at 55°C and 3 min at 95°C; 30 s at 95°C, 30 s at 55°C, and 30 s at 72°C, for 30 amplification cycles; and finally, 5 min at 72°C.
The four DENV serotypes, ZIKV, and CHIKV were detected in separate reactions in a final volume of 20 μL, using 2 μL of template (from the first round of amplification), 3 mM MgCl2, 0.4 mM dNTPs, and 0.2 μM of each specific primer. The amplification program was as follows: 3 min at 95°C; 30 s at 95°C, 30 s at 55°C (ZIKV and DENV) or 30 s at 60°C (CHIKV); 30 s at 72°C for 30 cycles of amplification and 5 min at 72°C. The products were visualized using ethidium bromide on 2% agarose gels. Figure 1 shows representative samples for arbovirus RNA detection.
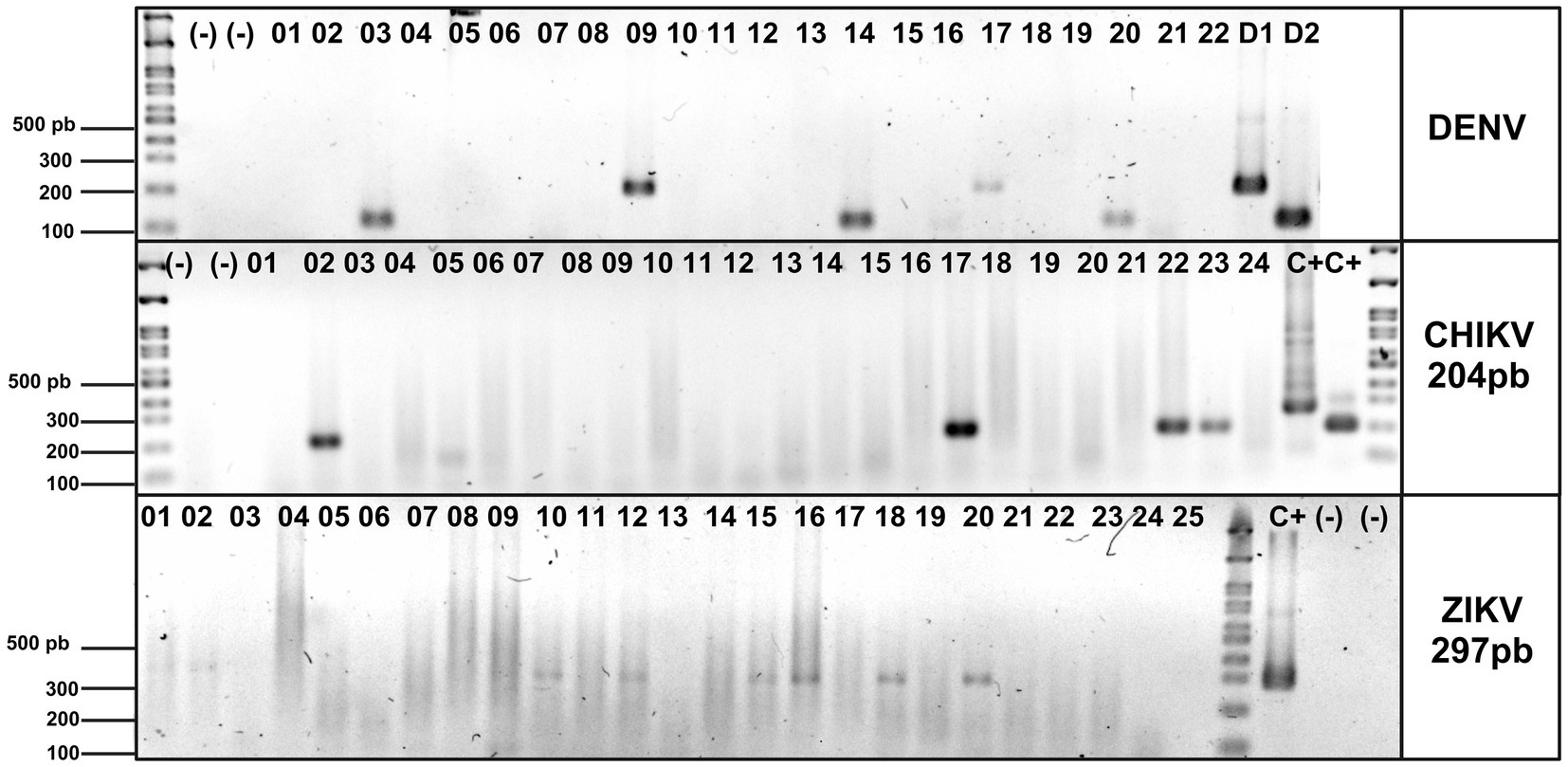
Figure 1. Detection of DENV, ZIKV, and CHIKV in blood donor sera by multiplex semi-nested RT-PCR. Specific DENV, ZIKV, and CHIKV products were separated on a 2% agarose gel and stained with ethidium bromide, a DNA molecular weight marker (100 bp ladder), to verify amplicon size. Blood donor sera are between lanes 01 and 26, negative controls: (−), positive controls: D1, D2, and C+. C+* plasmid DNA used as internal laboratory control.
In addition, the analytical sensitivity of the hnRT-PCR assay was determined by testing viral RNA obtained from serial dilutions of laboratory virus strains that had been previously titrated. The limit of detection (LoD) for DENV-2, ZIKV, and CHIKV was 1 × 102, 6 × 100, and 1 × 102 viral RNA copies/mL, respectively. Similarly, an alternative RT-qPCR assay to detect these viruses was evaluated under the same test conditions, resulting in LoDs of 1 × 103, 6 × 100, and 4 × 104 viral RNA copies/mL, respectively. Consequently, the hnRT-PCR assay exhibited a higher analytical sensitivity compared to the RT-qPCR assay.
2.3 Survey of blood donors positive for arbovirus
Two weeks after blood donation, a healthcare professional contacted the blood donors who tested positive for at least one of the tested arboviruses to record their sociodemographic, clinical, and epidemiological characteristics.
2.4 Statistical analysis
The positivity rates for arboviruses are presented as prevalences (percentages) and their 95% confidence intervals (95% CI). Categorical variables are presented as frequencies. Comparisons between the dengue outbreak and the endemic period and between arbovirus-endemic and nonendemic areas were performed using the chi-square or Fisher’s exact test. The significance level was set to p < 0.05. Statistical analyses were performed using Stata v16.
3 Results
3.1 Prevalence of arboviral RNA in blood donors in Colombia
We collected 1,581 samples from six blood banks in Colombia between 2019 and 2022. After individual sample screening, arboviral RNA was detected in 175 of the 1,581 samples tested, indicating a prevalence of arboviral RNA of 11% in accepted blood donors. The prevalence of DENV was 88/1,581 (5.6%), CHIKV was 74/1,581 (4.7%), and ZIKV was 39/1,581 (2.5%). Interestingly, in addition to single-virus infections, we found co-infections in 23/1,581 donors (1.4%).
3.2 The prevalence of arboviral RNA in blood donors changed between the outbreak and endemic periods
Considering that samples were collected in two different epidemiological periods, we calculated the prevalence of arboviral RNA separately for each one: the dengue outbreak in 2019–2020 (n = 462) and an endemic period in 2021–2022 (n = 1,119). As shown in Table 2, arboviral RNA from DENV, ZIKV, CHIKV, and co-infections were detected in blood donors, although their prevalences significantly differed between these two epidemiological periods.
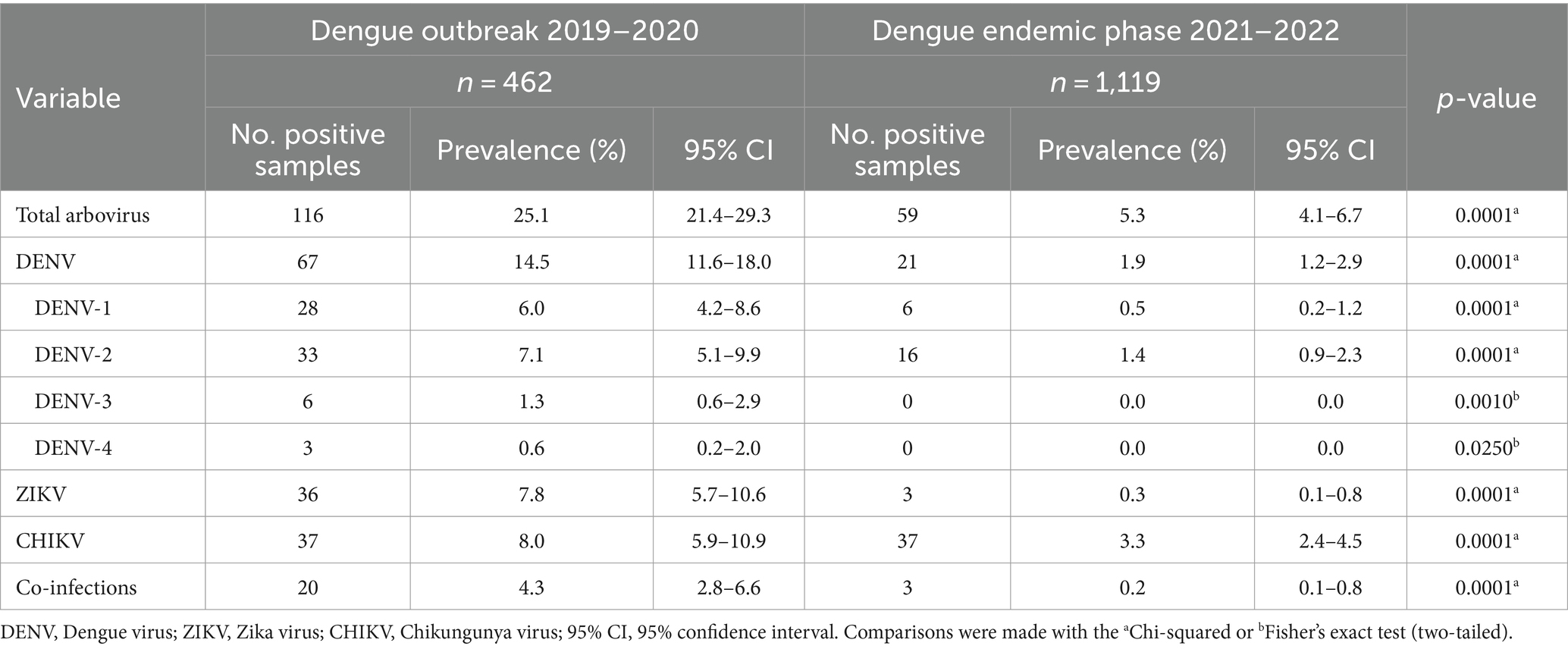
Table 2. Prevalence of arboviral RNA in blood donors in Colombia during a dengue outbreak (2019–2020) and an endemic period (2021–2022).
During the dengue outbreak, the overall prevalence of arboviral RNA was 25.1%, with the highest prevalence for the four dengue serotypes (14.5%), followed by CHIKV (8.0%) and ZIKV (7.8%). In contrast, during the endemic phase, the overall prevalence of arboviral RNA decreased to 5.3% (p = 0.0001), with the highest prevalence for CHIKV (3.3%), followed by DENV (1.9%) and ZIKV (0.3%). In addition, co-infections were observed with a frequency of 4.3% during the outbreak and 0.2% during the endemic phase (p = 0.0001). These results indicate the simultaneous circulation of DENV, ZIKV, and CHIKV, and the occurrence of co-infections in blood donors during the dengue outbreak and endemic period.
3.3 Various arbovirus co-infections were detected in blood donors
During the dengue outbreak, more than one arbovirus was detected in 20 of 462 samples. Interestingly, in most cases, two arboviruses were present (14/20), but three or four arboviruses in the same sample were also detected (5/20 and 1/20, respectively; Table 3). Among the most frequent co-infecting arboviruses detected were ZIKV and CHIKV (4/20), followed by DENV-1 and ZIKV (3/20) and DENV-1 and CHIKV (3/20; Table 3). Figure 2 shows the geographical origin of the co-infections observed during the dengue outbreak in Colombia.
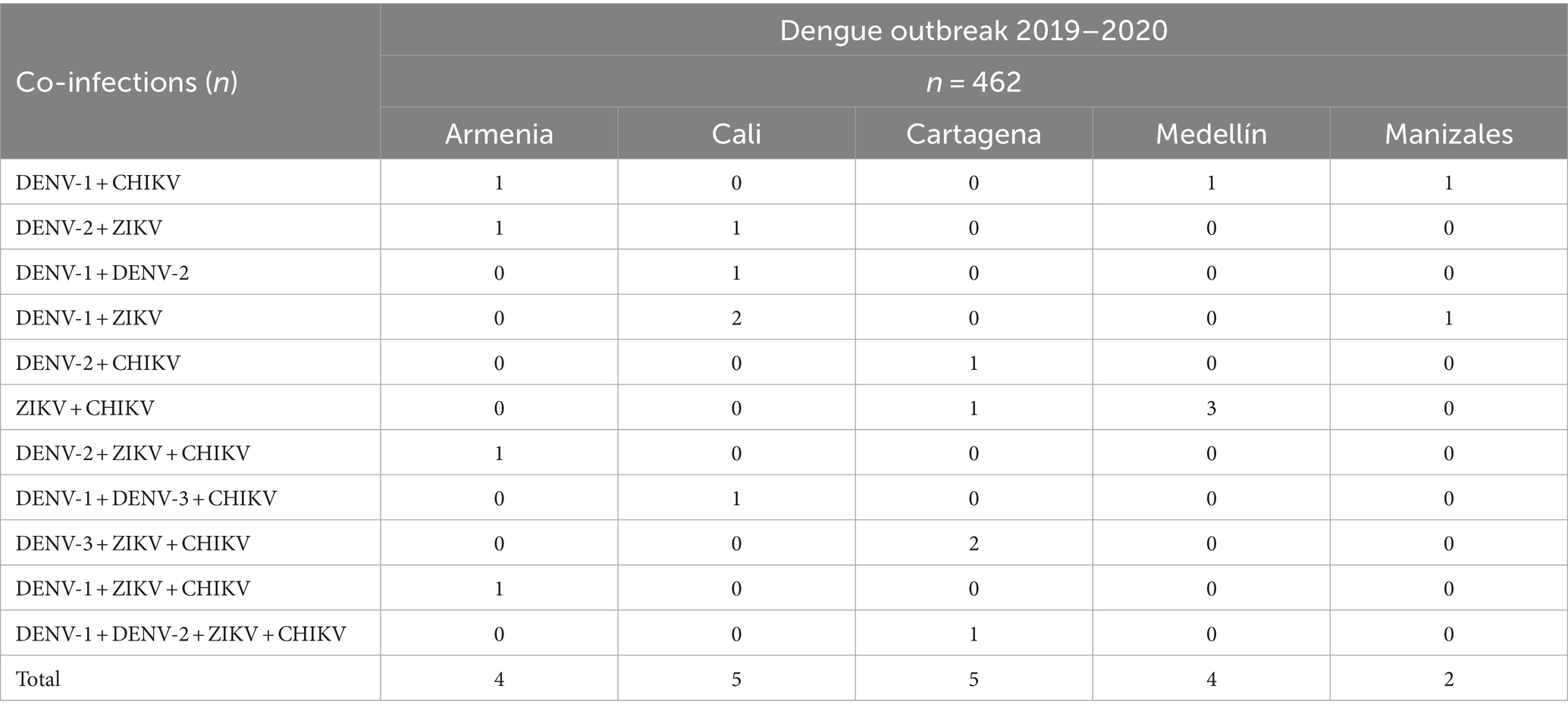
Table 3. Arbovirus co-infections in blood donors in Colombia during a dengue outbreak (2019–2020).
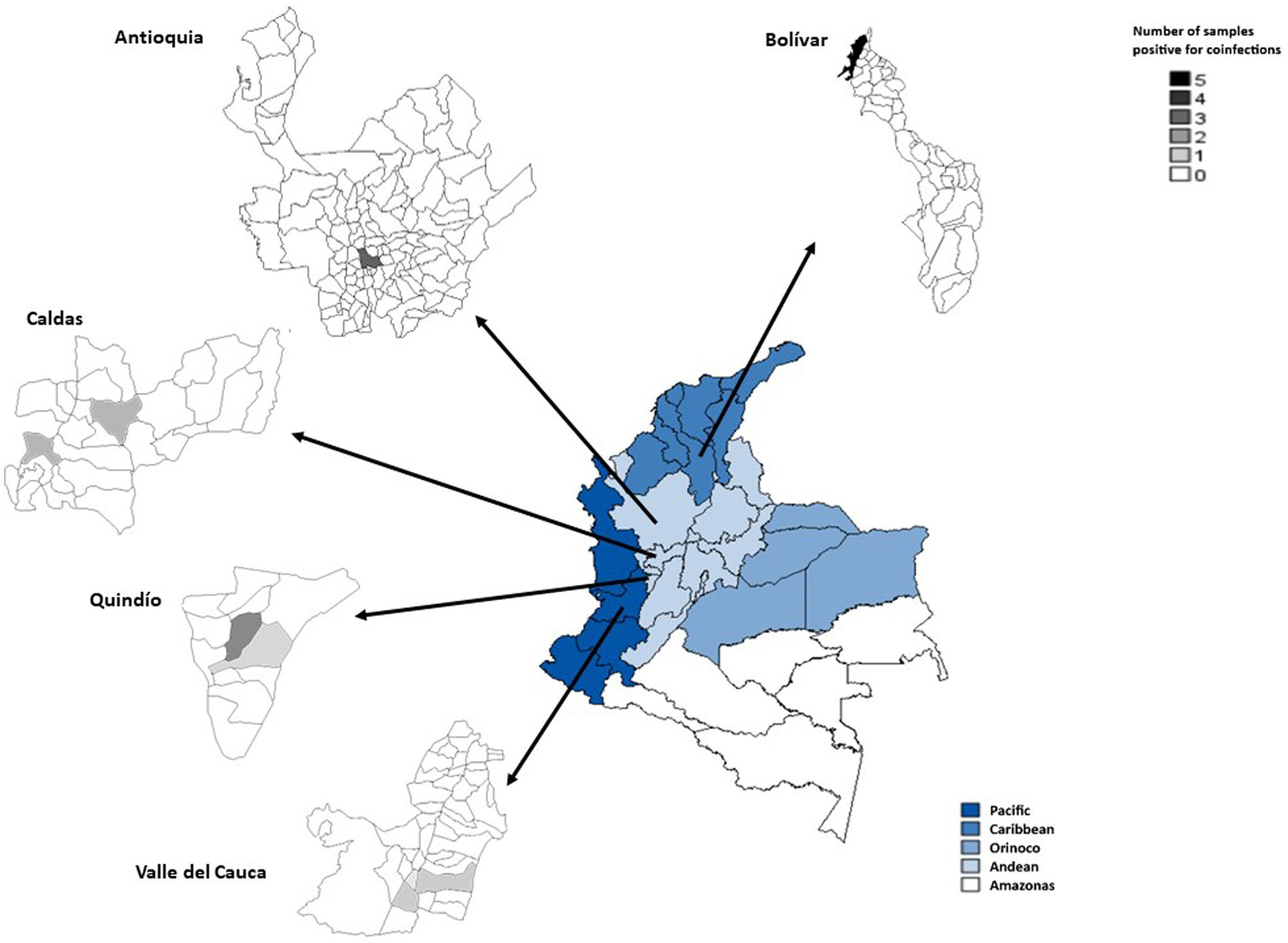
Figure 2. Regions of Colombia, highlighting the provinces and municipalities in which arboviral co-infections were observed during the dengue outbreak (2019–2020). The gradient colors on the map represent the number of samples positive for co-infection.
During the endemic phase, the frequency of arbovirus co-infections significantly decreased (three out of 1,119 samples) compared with the dengue outbreak (p = 0.0001; Table 2). Two out of three samples came from Medellín, Antioquia (DENV-1 + DENV-2 and ZIKV + CHIKV co-infections); and one case from Manizales, Caldas (DENV-1 + CHIKV co-infection). Thus, in an endemic country, multiple arboviruses can circulate in a single blood donor regardless of the epidemiological period of arbovirus circulation.
3.4 The highest reported prevalence of arbovirus in blood donors was observed in endemic areas during the dengue outbreak
As previously mentioned, each city in which samples were collected in two different epidemiological settings was classified as endemic or nonendemic for arbovirus circulation: two cities (Bogotá and Manizales) were classified as nonendemic, whereas four cities (Armenia, Cali, Cartagena, and Medellín) were classified as endemic. We then compared the prevalence of arbovirus circulation in blood donors from each group of cities during the dengue outbreak and the endemic period.
In endemic areas, the highest prevalence of arboviruses was observed in blood donors during the dengue outbreak (30.3%), with infection by any of the four DENV serotypes being the most prevalent (16.8%), followed by infection with CHIKV (12.1%), ZIKV (9.4%), and co-infections (6.7%). These frequencies in endemic areas decreased significantly during the endemic phase, with a global prevalence of arboviruses of 5.5%, caused first by CHIKV (3.5%), followed by DENV (2.0%), of which only serotypes 1 and 2 were observed. A prevalence of 0.3% of co-infections and 0.1% of ZIKV infection was detected (Table 4).
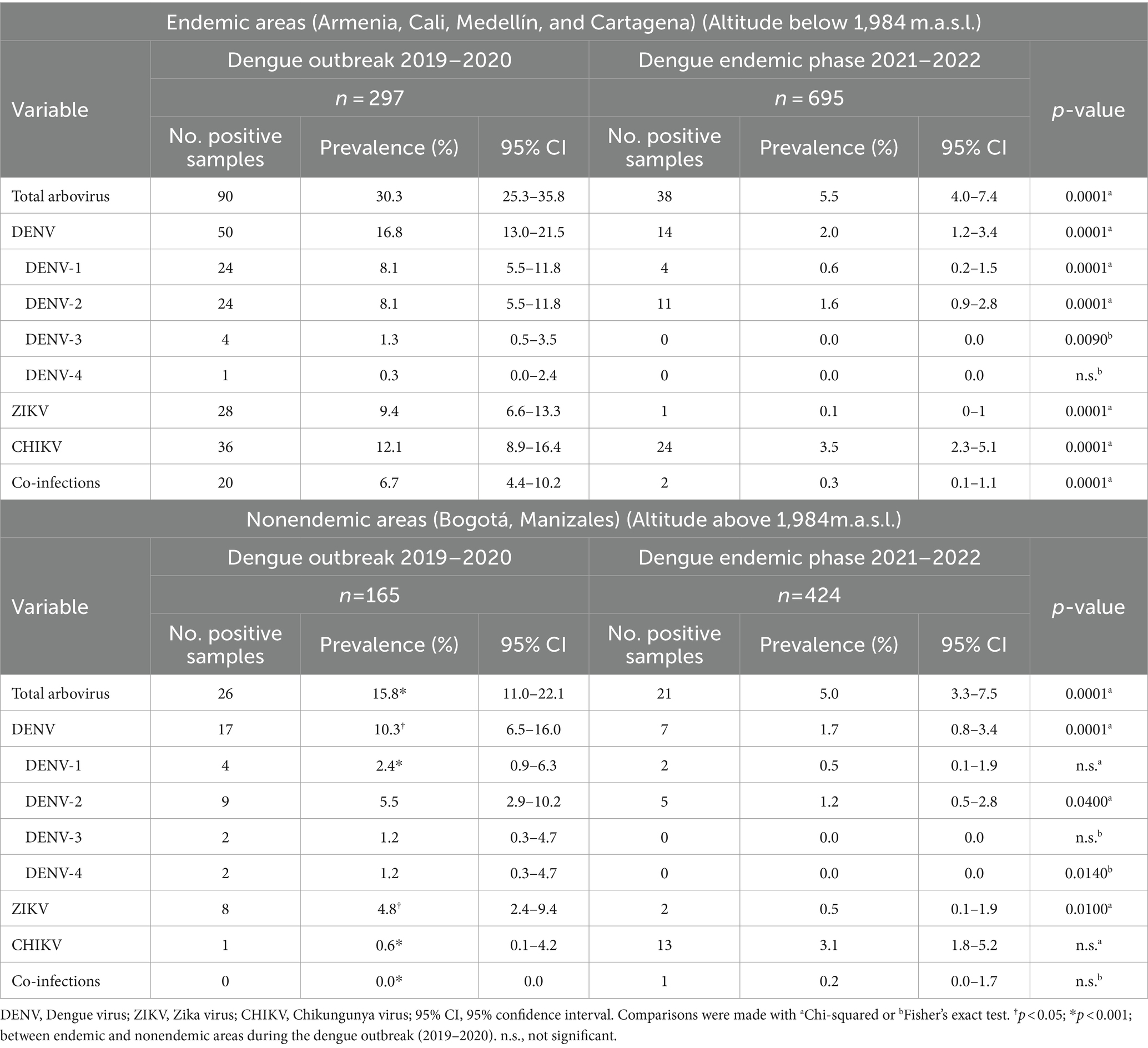
Table 4. Prevalence of arboviral RNA in blood donors in dengue endemic and nonendemic areas of Colombia during a dengue outbreak (2019–2020) and an endemic phase (2021–2022).
Additionally, comparing the endemic areas during the dengue outbreak with the nonendemic areas, a significantly lower global prevalence of arboviruses in blood donors was observed in the latter (15.8%), with infections caused by dengue being the first. The prevalence of circulation for the four DENV serotypes (10.3%) was followed by ZIKV (4.8%) and CHIKV (0.6%), and no co-infections were observed (Table 4). The prevalence of arboviruses during the endemic phase was similar in both endemic and nonendemic areas, although only serotypes 1 and 2 were observed for DENV.
3.5 Most arbovirus infections in blood donors were asymptomatic or mildly symptomatic
Blood donors who tested positive for viral RNA were contacted to record their sociodemographic, clinical, and epidemiological information. The response rate was 47% (83 of 175 donors), and the results are presented in Table 5. In the nonendemic region, 67% of the infected donors had no travel history to endemic areas. In total, 57% of the survey respondents were asymptomatic, and 43% reported any of the most common arboviral symptoms. The most frequent self-reported symptoms were headache, general malaise, and arthralgia, but none of them were diagnosed with an arboviral disease. No significant differences were observed between endemic and nonendemic areas or between viruses.
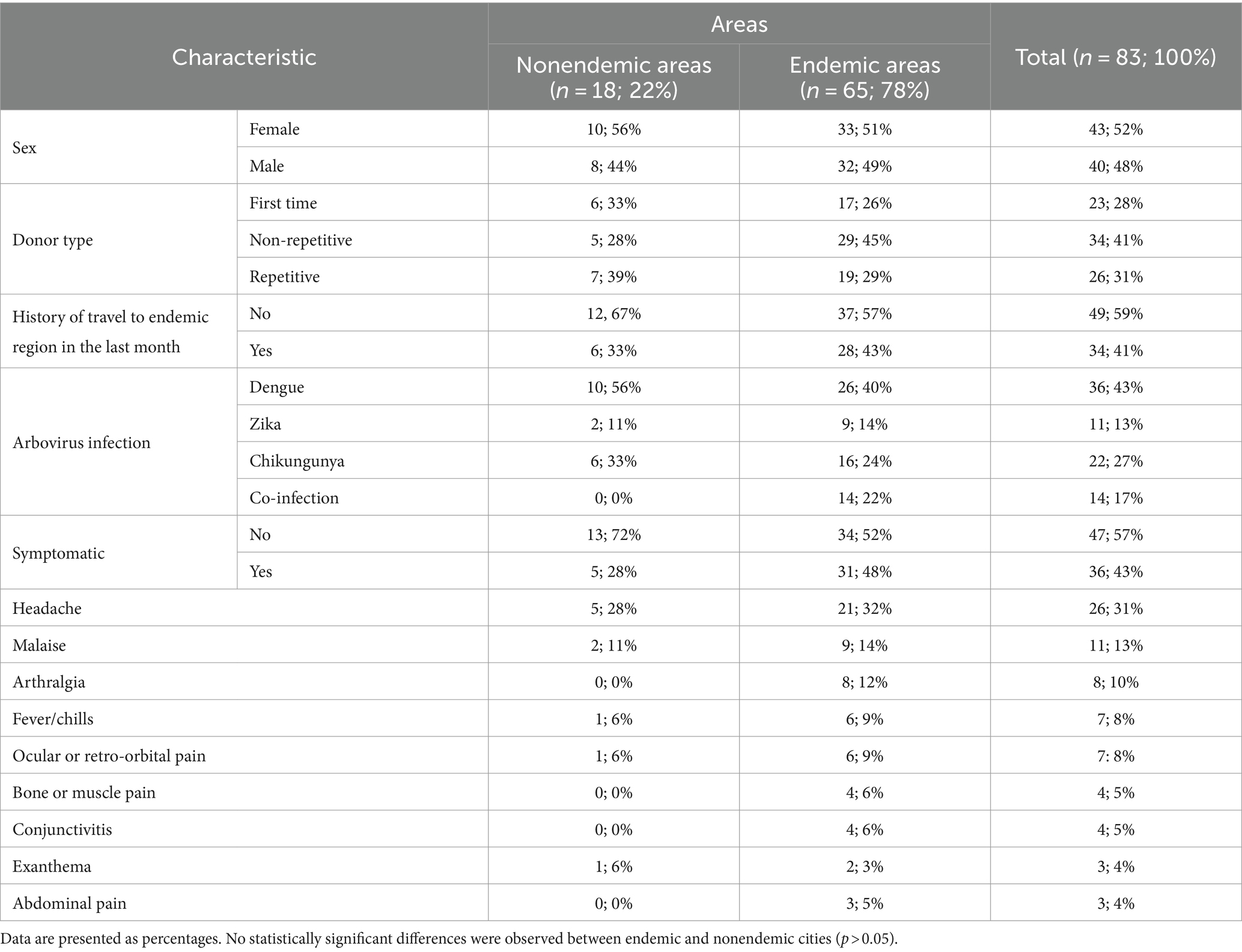
Table 5. Clinical and epidemiological characteristics of blood donors infected with arbovirus in Colombia.
4 Discussion
In this study, we used a hemi-nested RT-PCR approach previously developed in our laboratory (43) to detect arboviral RNA of DENV, ZIKV, and CHIKV in sera from accepted blood donors in Colombia during two different epidemiological periods, one during a dengue outbreak (2019–2020) and the other during a dengue endemic phase (2021–2022). Interestingly, we found a DENV prevalence of 14.5% during the dengue outbreak and 1.9% during the dengue endemic phase, which are significantly higher than the prevalence previously reported in the Americas (<1%) (44–48), the Asian continent (<1%) (49, 50), Saudi Arabia (5.5%) (25), and Portugal (2.3%) (51). Indeed, studies performed in endemic countries during dengue outbreaks did not find a rate of arbovirus viremic donations as high as we found in Colombia during a dengue outbreak (52). However, it should be noted that several studies reporting a low prevalence of DENV RNA in blood donors used samples frozen at −80°C for a long time (46, 53–55), and as it is known viral RNA in serum can degrade over time if stored at temperatures above −70°C (56, 57). The high prevalence observed in this study can be partly explained by the short time between sample collection and processing (maximum 7 days), which enhances RNA stability. On the other hand, enhanced detection of arboviral RNA can also be attributed to the higher analytical sensitivity of the nested PCR approach compared with conventional PCR and real-time PCR (58–61). It is also crucial to consider that a major problem exacerbated by the highly sensitive nature of the hnRT-PCR is the risk of contamination. However, precautions such as the use of dedicated locations and equipment were implemented to minimize this eventuality.
The 2019 dengue outbreak was most severe in Colombia, with 127,553 symptomatic dengue cases reported (33). The high prevalence of DENV in blood donors at this time could be due to the approximately 65% of DENV-infected people who are asymptomatic (62). Consequently, this study shows that the hyperendemic status of the country could also be reflected in the population of accepted blood donors who were probably asymptomatic or presymptomatic at the time of blood donation. In addition to a high prevalence of DENV, other arboviruses such as CHIKV and ZIKV occurred at frequencies of 8% and 7.8% in blood donors, respectively, during this dengue outbreak. Concurrent circulation of four serotypes of DENV, ZIKV, and CHIKV has been reported in the general population of Colombia (36, 63, 64). However, the number of reported symptomatic cases of ZIKV and CHIKV was low in the country during the dengue outbreak and the endemic period (65–71). According to the national epidemiological surveillance system (SIVIGILA), more than 38% of symptomatic dengue cases reported during the dengue outbreak and 30% during the endemic phase were not confirmed by laboratory techniques but registered as probable or as cases with epidemiological links (33, 62). Considering that the clinical symptoms of DENV, ZIKV, and CHIKV infections are nonspecific and include general malaise, headache, and arthralgias/myalgias (64), it is plausible that a proportion of probable dengue cases unconfirmed by laboratory tests include infections with CHIKV and/or ZIKV. However, more studies are needed to confirm this hypothesis.
In hyperendemic countries for arboviruses such as Colombia, co-infections are often found in patients with febrile syndromes compatible with DENV infection, where arboviral RNA from more than one arbovirus is detected (64, 72). Thus, we found co-infections with DENV/ZIKV, DENV/CHIKV, and ZIKV/CHIKV, not to mention co-infections with the three arboviruses. In the context of blood safety, if arboviral RNA in the serum of blood donors is accompanied by infectious viral particles in the blood components obtained from them, co-infections in blood donors could transmit not only one but also several arboviruses to a susceptible recipient. Future studies should measure the quantity, stability, and viability of viral particles in blood components obtained from infected donors.
Donors in whom arboviral RNA was detected were inquired about their sociodemographic, clinical, and epidemiological characteristics within 15 days after blood donation. As expected, most patients reported being asymptomatic after donating blood (57%). Among those who reported symptoms, these were mild and nonspecific, such as headache, general malaise, and arthralgia. Arboviral infections are frequently subclinical or inapparent and therefore insufficient for clinical consultation, even with positive viral or antibody tests (4). Therefore, an infected but asymptomatic subject could donate blood. Blood donors should be educated so that they can notify the blood bank if they notice any symptoms after donating blood. On the other hand, 67% of the blood donors positive for arbovirus who were interviewed and who came from nonendemic areas for dengue stated that they had not traveled to endemic areas in the past 3 months before donating blood. To classify the country’s regions as endemic or nonendemic, 1,984 m.a.s.l. was defined as the cut-off because dengue-positive Aedes aegypti vector has been documented in Colombia even at this altitude (42). However, uninfected specimens of this vector have also been observed up to 2,302 m.a.s.l. in Colombia (42) and 2,900 m.a.s.l. in other countries (73). More recently, it was also reported that another vector species, Aedes albopictus, can transmit CHIKV at a temperature of 20°C and at high altitude (74). Therefore, epidemiological surveillance studies are required to determine whether infected mosquitoes are circulating at increasingly higher altitudes.
One limitation of this study is that only arboviral RNA from DENV, CHIKV, and ZIKV was detected in individual serum samples from accepted blood donors, which may have contained viral particles that could infect a transfusion recipient. It is important to note that DENV has been isolated in cell cultures (using C6/36 lines) from positive blood donor samples (16). It is also important to consider whether these arboviruses are stable and remain infectious when stored in blood components such as red blood cells, platelets, and plasma. To our knowledge, only one report confirmed that DENV-2 is stable in platelets and red blood cells stored under standard blood bank conditions (75). Additionally, despite the high prevalence of arbovirus in blood donors, there are no reports in Colombia suggesting its transmission through transfusion. Therefore, active hemovigilance studies should be performed to detect arboviruses from index cases of adverse transfusion reactions that present with fever, for example.
In conclusion, for the first time, we report the presence of arboviral RNA of DENV, ZIKV, and CHIKV, as well as co-infections, in sera from blood donors from endemic and nonendemic cities in Colombia. Furthermore, we found that most donors who tested positive had asymptomatic infection or mild and nonspecific symptoms. Finally, these results inform future studies on the risks these viruses can pose to blood safety in Colombia.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by the Universidad El Bosque Institutional Ethics Committee. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
BC: Conceptualization, Formal analysis, Methodology, Writing – original draft, Writing – review & editing. AU: Conceptualization, Data curation, Formal analysis, Writing – original draft, Writing – review & editing. TO: Methodology, Writing – review & editing. AR: Funding acquisition, Methodology, Writing – review & editing. OF: Funding acquisition, Methodology, Writing – review & editing. LO: Funding acquisition, Methodology, Writing – review & editing. IF: Funding acquisition, Methodology, Writing – review & editing. DU: Funding acquisition, Methodology, Writing – review & editing. CA: Funding acquisition, Methodology, Writing – review & editing. EC: Conceptualization, Methodology, Writing – review & editing. FD: Conceptualization, Formal analysis, Funding acquisition, Writing – original draft, Writing – review & editing. JC: Conceptualization, Funding acquisition, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. The Colombian Ministry of Science, Technology, and Innovation (MinCiencias), code #130884467713, contract #898-2019, and Universidad El Bosque, Bogotá, Colombia, PCI 2018-10209, funded this study.
Acknowledgments
The authors gratefully acknowledge the technical and administrative staff of the blood bank network of the Colombian Red Cross and the Grupo de Virología of the Universidad El Bosque.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Khetarpal, N, and Khanna, I. Dengue fever: causes, complications, and vaccine strategies. J Immunol Res. (2016) 2016:1–14. doi: 10.1155/2016/6803098
2. Faye, O, Freire, CCM, Iamarino, A, Faye, O, de Oliveira, JVC, Diallo, M, et al. Molecular evolution of Zika virus during its emergence in the 20th century. PLoS Negl Trop Dis. (2014) 8:36. doi: 10.1371/JOURNAL.PNTD.0002636
3. Schwartz, O, and Albert, ML. Biology and pathogenesis of chikungunya virus. Nat Rev Microbiol. (2010) 8:491–500. doi: 10.1038/nrmicro2368
4. Grange, L, Simon-Loriere, E, Sakuntabhai, A, Gresh, L, Paul, R, and Harris, E. Epidemiological risk factors associated with high global frequency of inapparent dengue virus infections. Front Immunol. (2014) 5:280. doi: 10.3389/fimmu.2014.00280
5. de Almeida Barreto, FK, Alencar, CH, de Carvalho Araújo, FM, Oliveira, RDMAB, Cavalcante, JW, Lemos, DRQ, et al. Seroprevalence, spatial dispersion and factors associated with flavivirus and chikungunha infection in a risk area: a population-based seroprevalence study in Brazil. BMC Infect Dis. (2020) 20:1–14. doi: 10.1186/s12879-020-05707-y
6. Petersen, LR, Jamieson, DJ, Powers, AM, and Honein, MA. Zika Virus. N Engl J Med. (2016) 374:1552–63. doi: 10.1056/NEJMra1602113
7. Pealer, LN, Marfin, AA, Petersen, LR, Lanciotti, RS, Page, PL, Stramer, SL, et al. Transmission of West Nile virus through blood transfusion in the United States in 2002. N Engl J Med. (2003) 349:1236–45. doi: 10.1056/NEJMoa030969
8. Biggerstaff, BJ, and Petersen, LR. Estimated risk of West Nile virus transmission through blood transfusion during an epidemic in Queens, new York City. Transfusion (Paris). (2002) 42:1019–26. doi: 10.1046/j.1537-2995.2002.00167.x
9. Stramer, SL, Hollinger, FB, Katz, LM, Kleinman, S, Metzel, PS, Gregory, KR, et al. Emerging infectious disease agents and their potential threat to transfusion safety. Transfusion (Paris). (2009) 49:1S–29S. doi: 10.1111/J.1537-2995.2009.02279.X
10. Stramer, SL. Current perspectives in transfusion-transmitted infectious diseases: emerging and re-emerging infections. ISBT Sci Ser. (2014) 9:30. doi: 10.1111/voxs.12070
11. Morrison, AC, Minnick, SL, Rocha, C, Forshey, BM, Stoddard, ST, Getis, A, et al. Epidemiology of dengue virus in Iquitos, Peru 1999 to 2005: Interepidemic and epidemic patterns of transmission. PLoS Negl Trop Dis. (2010) 4:e670. doi: 10.1371/journal.pntd.0000670
12. Duffy, MR, Chen, T-H, Hancock, WT, Powers, AM, Kool, JL, Lanciotti, RS, et al. Zika virus outbreak on Yap Island, Federated States of Micronesia. N Engl J Med. (2009) 360:2536–43. doi: 10.1056/NEJMoa0805715
13. Mascarenhas, M, Garasia, S, Berthiaume, P, Corrin, T, Greig, J, Ng, V, et al. A scoping review of published literature on chikungunya virus. PLoS One. (2018) 13:e0207554. doi: 10.1371/journal.pone.0207554
14. Waggoner, JJ, Gresh, L, Vargas, MJ, Ballesteros, G, Tellez, Y, Soda, KJ, et al. Viremia and clinical presentation in Nicaraguan patients infected with Zika virus, chikungunya virus, and dengue virus. Clin Infect Dis. (2016) 63:1584–90. doi: 10.1093/cid/ciw589
15. De La Cruz-Hernández, SI, Flores-Aguilar, H, González-Mateos, S, López-Martinez, I, Alpuche-Aranda, C, Ludert, JE, et al. Determination of viremia and concentration of circulating nonstructural protein 1 in patients infected with dengue virus in Mexico. Am J Trop Med Hyg. (2013) 88:446–54. doi: 10.4269/ajtmh.12-0023
16. Busch, MP, Linnen, JM, Vinelli, E, Sabino, EC, Tobler, LH, Hyland, C, et al. Dengue viremia in blood donors from Honduras, Brazil, and Australia. Transfusion (Paris). (2008) 48:1355–62. doi: 10.1111/j.1537-2995.2008.01772.x
17. Corman, VM, Rasche, A, Baronti, C, Aldabbagh, S, Cadar, D, Reusken, CBEM, et al. Assay optimization for molecular detection of Zika virus. Bull World Health Organ. (2016) 94:880. doi: 10.2471/BLT.16.175950
18. Mansuy, JM, Mengelle, C, Pasquier, C, Chapuy-Regaud, S, Delobel, P, Martin-Blondel, G, et al. Zika virus infection and prolonged viremia in whole-blood specimens. Emerg Infect Dis. (2017) 23:863–5. doi: 10.3201/eid2305.161631
19. Riswari, SF, Ma’roef, CN, Djauhari, H, Kosasih, H, Perkasa, A, Yudhaputri, FA, et al. Study of viremic profile in febrile specimens of chikungunya in Bandung, Indonesia. J Clin Virol. (2016) 74:61–5. doi: 10.1016/j.jcv.2015.11.017
20. Simmons, G, Brès, V, Lu, K, Liss, NM, Brambilla, DJ, Ryff, KR, et al. High incidence of chikungunya virus and frequency of Viremic blood donations during epidemic, Puerto Rico, USA, 2014. Emerg Infect Dis. (2016) 22:1221–8. doi: 10.3201/eid2207.160116
21. Donna, M. (2016). Association for the Advancement of Blood & Biotherapies. 1–15. Available at: https://www.aabb.org/docs/default-source/default-document-library/resources/association-bulletins/ab16-07.pdf
22. Musso, D, Nhan, T, Robin, E, Roche, C, Bierlaire, D, Zisou, K, et al. Potential for Zika virus transmission through blood transfusion demonstrated during an outbreak in French Polynesia, November 2013 to February 2014. Euro Surveill. (2014) 19:20761. doi: 10.2807/1560-7917.ES2014.19.14.20761
23. Motta, IJF, Spencer, BR, Cordeiro da Silva, SG, Arruda, MB, Dobbin, JA, Gonzaga, YBM, et al. Evidence for transmission of Zika virus by platelet transfusion. N Engl J Med. (2016) 375:1101–3. doi: 10.1056/NEJMc1607262
24. Barjas-Castro, ML, Angerami, RN, Cunha, MS, Suzuki, A, Nogueira, JS, Rocco, IM, et al. Probable transfusion-transmitted Zika virus in Brazil. Transfusion (Paris). (2016) 56:1684–8. doi: 10.1111/trf.13681
25. Ashshi, AM. The prevalence of dengue virus serotypes in asymptomatic blood donors reveals the emergence of serotype 4 in Saudi Arabia. Virol J. (2017) 14:107. doi: 10.1186/s12985-017-0768-7
26. Beau, F, Lastère, S, Mallet, HP, Mauguin, S, Broult, J, and Laperche, S. Impact on blood safety of the last arboviruses outbreaks in French Polynesia (2012-2018). Transfus Clin Biol. (2020) 27:4–9. doi: 10.1016/j.tracli.2019.12.001
27. Chuang, V, Wong, T, Leung, Y, Ma, E, Law, Y, Tsang, O, et al. Review of dengue fever cases in Hong Kong during 1998 to 2005. Hong Kong Med J. (2008) 14:170–7.
28. Tambyah, PA, Koay, ESC, Poon, MLM, Lin, RVTP, and Ong, BKC. Dengue hemorrhagic fever transmitted by blood transfusion. N Engl J Med. (2008) 359:1526–7. doi: 10.1056/NEJMc0708673
29. Sharp, TM, Ryff, KR, Alvarado, L, Shieh, WJ, Zaki, SR, Margolis, HS, et al. Surveillance for chikungunya and dengue during the first year of chikungunya virus circulation in Puerto Rico. J Infect Dis. (2016) 214:S475–81. doi: 10.1093/infdis/jiw245
30. Rico-Mendoza, A, Porras-Ramírez, A, Chang, A, Encinales, L, and Lynch, R. Co-circulation of dengue, chikungunya, and Zika viruses in Colombia from 2008 to 2018. Rev Panam Salud Publica. (2019) 43:1. doi: 10.26633/RPSP.2019.49
31. Padilla, JC, Lizarazo, FE, Murillo, OL, Mendigaña, FA, Pachón, E, and Vera, MJ. Epidemiología de las principales enfermedades transmitidas por vectores en Colombia, 1990-2016. Biomedica. (2017) 37:27–40. doi: 10.7705/biomedica.v37i0.3769
32. Castrillón, JC, Castaño, JC, and Urcuqui, S. Dengue en Colombia: diez años de evolución. Rev Chilena Infectol. (2015) 32:142–9. doi: 10.4067/S0716-10182015000300002
33. Gutierrez-Barbosa, H, Medina-Moreno, S, Zapata, JC, and Chua, JV. Dengue infections in Colombia: epidemiological trends of a Hyperendemic country. Trop Med Infect Dis. (2020) 5:156. doi: 10.3390/tropicalmed5040156
34. Ospina, ML, Tong, VT, Gonzalez, M, Valencia, D, Mercado, M, Gilboa, SM, et al. Zika virus disease and pregnancy outcomes in Colombia. N Engl J Med. (2020) 383:537. doi: 10.1056/NEJMoa1911023
35. Vidal, OM, Acosta-Reyes, J, Padilla, J, Navarro-Lechuga, E, Bravo, E, Viasus, D, et al. Chikungunya outbreak (2015) in the Colombian Caribbean: latent classes and gender differences in virus infection. PLoS Negl Trop Dis. (2020) 14:1–18. doi: 10.1371/JOURNAL.PNTD.0008281
36. Instituto Nacional de Salud (2019). Informe de evento dengue, Colombia, 2019. Available at: https://www.ins.gov.co/buscador-eventos/Informesdeevento/DENGUE_2019.pdf (Accessed March 08, 2024).
37. Instituto Nacional de Salud (2014). Informe final del evento chikungunya, Colombia, 2014. Available at: https://www.ins.gov.co/buscador-eventos/Informesdeevento/Chikungun%CC%83a%202014.pdf (Accessed March 08, 2024).
38. Instituto Nacional de Salud (2015). Informe final del evento chikungunya, Colombia, 2015. Available at: https://www.ins.gov.co/buscador-eventos/Informesdeevento/Chikungun%CC%83a%202015.pdf (Accessed March 08, 2024).
39. Instituto Nacional de Salud (2016). Informe del evento chikunguña periodo epidemiológico XIII, Colombia 2016. Available at: https://www.ins.gov.co/buscador-eventos/Informesdeevento/Chikungu%C3%B1a%202016.pdf (Accessed March 08, 2024).
40. Instituto Nacional de Salud (2016). Boletín epidemiológico semanal, semana epidemiológica 52 de 2016. Available at: https://www.ins.gov.co/buscador-eventos/BoletinEpidemiologico/2016%20Bolet%C3%ADn%20epidemiol%C3%B3gico%20semana%2052%20-.pdf (Accessed March 08, 2024).
41. Instituto Nacional de Salud (2022). Lineamiento técnico para la selección de donantes de sangre en Colombia (Actualización agosto de 2022). Available at: https://www.ins.gov.co/bibliotecadigital/seleccion-donantes-sangre.pdf (Accessed March 08, 2024).
42. Ruiz-López, F, González-Mazo, A, Vélez-Mira, A, Gómez, GF, Zuleta, L, Uribe, S, et al. Presence of Aedes (Stegomyia) aegypti (Linnaeus, 1762) and its natural infection with dengue virus at unrecorded heights in Colombia. Biomedica. (2016) 36:303–8. doi: 10.7705/biomedica.v36i2.3301
43. Calvo, EP, Sánchez-Quete, F, Durán, S, Sandoval, I, and Castellanos, JE. Easy and inexpensive molecular detection of dengue, chikungunya and zika viruses in febrile patients. Acta Trop. (2016) 163:32–7. doi: 10.1016/j.actatropica.2016.07.021
44. Busch, MP, Sabino, EC, Brambilla, D, Lopes, ME, Capuani, L, Chowdhury, D, et al. Duration of dengue viremia in blood donors and relationships between donor viremia, infection incidence and clinical case reports during a large epidemic. J Infect Dis. (2016) 214:49–54. doi: 10.1093/infdis/jiw122
45. Sabino, E, Loureiro, P, Lopes, M, Capuani, L, Oliveira, C, Oliveira, L, et al. Dengue RNA among blood donors and recipients during large epidemics of Denv-4 in Rio de Janeiro and Recife, Brazil. Vox Sang. (2013) 105:39. doi: 10.1111/vox.12047
46. Slavov, SN, Hespanhol, MR, Ferreira, AR, Rodrigues, ES, Covas, DT, and Kashima, S. Silent dengue virus circulation among asymptomatic blood donors from a hyperendemic Brazilian region. Transfus Med. (2018) 28:465–7. doi: 10.1111/tme.12521
47. Mohammed, H, Linnen, JM, Muhoz-Jorddn, JL, Tomashek, K, Foster, G, Broulik, AS, et al. Dengue virus in blood donations, Puerto Rico, 2005. Transfusion (Paris). (2008) 48:1348–54. doi: 10.1111/j.1537-2995.2008.01771.x
48. Dias, LL, Amarilla, AA, Poloni, TR, Covas, DT, Aquino, VH, and Figueiredo, LTM. Detection of dengue virus in sera of Brazilian blood donors. Transfusion (Paris). (2012) 52:1667–71. doi: 10.1111/j.1537-2995.2012.03729.x
49. Liao, Q, Shan, Z, Wang, M, Huang, J, Xu, R, Huang, K, et al. An evaluation of asymptomatic dengue infections among blood donors during the 2014 dengue outbreak in Guangzhou, China. J Med Virol. (2017) 89:2037–40. doi: 10.1002/jmv.24883
50. Tsai, JJ, Lin, PC, Tsai, CY, Wang, YH, and Liu, LT. Low frequency of asymptomatic dengue virus-infected donors in blood donor centers during the largest dengue outbreak in Taiwan. PLoS One. (2018) 13:e0205248. doi: 10.1371/journal.pone.0205248
51. Escoval, MA, Sousa, G, Freitas, B, Sousa, AP, Alves, MJ, Núncio, MS, et al. Dengue outbreak in Madeira Island (Portugal). Blood safety measures. Vox Sang. (2013) 105:192–3. doi: 10.1111/vox.12048
52. Gimenez-Richarte, A, De Salazar, MO, Arbona, C, Gimenez-Richarte, MP, Collado, M, Fernandez, PL, et al. Prevalence of chikungunya, dengue and Zika viruses in blood donors: a systematic literature review and meta-analysis. Blood Transfus. (2022) 20:267. doi: 10.2450/2021.0106-21
53. Ranjan, P, Natarajan, V, Bajpai, M, and Gupta, E. High Seroprevalence of dengue virus infection in blood donors from Delhi: a single Centre study. J Clin Diagn Res. (2016) 10:DC08–10. doi: 10.7860/JCDR/2016/21262.8711
54. Slavov, SN, Cilião-Alves, DC, Gonzaga, FAC, Moura, DR, de Moura, ACAM, de Noronha, LAG, et al. Dengue seroprevalence among asymptomatic blood donors during an epidemic outbreak in central-West Brazil. PLoS One. (2019) 14:e0213793. doi: 10.1371/journal.pone.0213793
55. Sharma, R, Costa Santos, L, da Silva, RA, and Gonçalves, C V., de Melo, Calado S, Santos, DP, Andrade de Melo, JP, de Cássia Pontello Rampazzo, R, Requião, L, Krieger, MA, et al. (2018). Surveillance of donated blood during the 2016 arbovirus outbreak in Brazil. J Med Virol 90: 1406–1410. doi: 10.1002/JMV.25193
56. Schmid, P, Tong, M, Conrad, A, McHutchison, J, and Blatt, LM. Analysis of the viability of freezer stored serum samples for hepatitis C virus RNA analysis by the SUPERQUANT® method: results of a 16 year retrospective study. J Virol Methods. (1999) 82:201–6. doi: 10.1016/S0166-0934(99)00094-4
57. Halfon, P, Khiri, H, Gerolami, V, Bourliere, M, Feryn, JM, Reynier, P, et al. Impact of various handling and storage conditions on quantitative detection of hepatitis C virus RNA. J Hepatol. (1996) 25:307–11. doi: 10.1016/S0168-8278(96)80116-4
58. Sharifdini, M, Mirhendi, H, Ashrafi, K, Hosseini, M, Mohebali, M, Khodadadi, H, et al. Comparison of nested polymerase chain reaction and real-time polymerase chain reaction with parasitological methods for detection of Strongyloides stercoralis in human fecal samples. Am J Trop Med Hyg. (2015) 93:1285. doi: 10.4269/ajtmh.15-0309
59. Hafez, HM, Hauck, R, Lüschow, D, and McDougald, L. Comparison of the specificity and sensitivity of PCR, nested PCR, and real-time PCR for the diagnosis of histomoniasis. Avian Dis. (2005) 49:366–70. doi: 10.1637/7341-020805R.1
60. Manuel, CS, Suther, C, Moore, MD, and Jaykus, LA. Comparison of a one-step real-time RT-PCR and a nested real-time RT-PCR for a genogroup II norovirus reveals differences in sensitivity depending upon assay design and visualization. PLoS One. (2021) 16:e0248581. doi: 10.1371/journal.pone.0248581
61. Jalal, S, Hwang, SY, Kim, CM, Kim, DM, Yun, NR, Seo, JW, et al. Comparison of RT-PCR, RT-nested PCRs, and real-time PCR for diagnosis of severe fever with thrombocytopenia syndrome: a prospective study. Sci Rep. (2021) 11:1–8. doi: 10.1038/s41598-021-96066-4
62. Asish, PR, Dasgupta, S, Rachel, G, Bagepally, BS, and Girish Kumar, CP. Global prevalence of asymptomatic dengue infections—a systematic review and meta-analysis. Int J Infect Dis. (2023) 134:292–8. doi: 10.1016/j.ijid.2023.07.010
63. Instituto Nacional de Salud (2020). Informe de evento dengue, Colombia 2020. Available at: https://www.ins.gov.co/buscador-eventos/Informesdeevento/DENGUE_2020.pdf (Accessed March 08, 2024).
64. Carrillo-Hernández, MY, Ruiz-Saenz, J, Villamizar, LJ, Gómez-Rangel, SY, and Martínez-Gutierrez, M. Co-circulation and simultaneous co-infection of dengue, chikungunya, and zika viruses in patients with febrile syndrome at the Colombian-Venezuelan border. BMC Infect Dis. (2018) 18:61. doi: 10.1186/s12879-018-2976-1
65. Instituto Nacional de Salud (2019). Enfermedad por virus zika y chikungunya Colombia 2019. Available at: https://www.ins.gov.co/buscador-eventos/Informesdeevento/CHIKUNGUNYA%20Y%20ENFERMEDAD%20POR%20VIRUS%20ZIKA_2019.pdf (Accessed March 08, 2024).
66. Instituto Nacional de Salud (2020). Informe de evento de chikungunya Colombia, 2020. Available at: https://www.ins.gov.co/buscador-eventos/Informesdeevento/CHIKUNGUNYA_2020.pdf (Accessed March 08, 2024).
67. Instituto Nacional de Salud (2020). Informe de evento Zika, Colombia, 2020. Available at: https://www.ins.gov.co/buscador-eventos/Informesdeevento/ENFERMEDAD%20POR%20VIRUS%20ZIKA_2020.pdf (Accessed March 08, 2024).
68. Instituto Nacional de Salud (2021). Informe de evento de chikungunya Colombia, 2021. Available at: https://www.ins.gov.co/buscador-eventos/Informesdeevento/CHIKUNGUNYA%20INFORME%202021.pdf (Accessed March 08, 2024).
69. Instituto Nacional de Salud (2022). Informe de evento de chikungunya Colombia, 2022. Available at: https://www.ins.gov.co/buscador-eventos/Informesdeevento/CHIKUNGUNYA%20INFORME%202022.pdf (Accessed March 08, 2024).
70. Instituto Nacional de Salud (2021). Informe de evento Zika, Colombia, 2021. Available at: https://www.ins.gov.co/buscador-eventos/Informesdeevento/ZIKA%20INFORME%202021.pdf (Accessed March 08, 2024).
71. Instituto Nacional de Salud (2022). Informe de evento Zika, Colombia, 2022. Available at: https://www.ins.gov.co/buscador-eventos/Informesdeevento/ZIKA%20INFORME%202022.pdf (Accessed March 08, 2024).
72. Frota, CC, Correia, FGS, Alves Vasconcelos, LR, de Sousa, PRC, Da Silva Ferreira, ML, Saraiva, SP, et al. Positivity of dengue, chikungunya, and Zika infections in women in Northeast Brazil post-Zika epidemic. Pathog Glob Health. (2023) 117:485–92. doi: 10.1080/20477724.2022.2142187
73. More, MDPM, Castañeda, C, and Suyón, M. New altitudinal registration of Aedes aegypti in the region of Piura, Peru. Rev Peru Med Exp Salud Publica. (2018) 35:536–7. doi: 10.17843/RPMESP.2018.353.3791
74. Mercier, A, Obadia, T, Carraretto, D, Velo, E, Gabiane, G, Bino, S, et al. Impact of temperature on dengue and chikungunya transmission by the mosquito Aedes albopictus. Sci Rep. (2022) 12:1–13. doi: 10.1038/s41598-022-10977-4
Keywords: dengue virus, Zika virus, chikungunya virus, blood donors, blood components, blood transfusion, blood banks, Colombia
Citation: Cáceres Munar BA, Urbina A, Ortíz T, Rodríguez A, Fernández OL, Ospina LF, Flórez I, Uribe D, Alvarado C, Calvo EP, Delgado FG and Castellanos JE (2024) High prevalence of dengue, Zika, and chikungunya viruses in blood donors during a dengue outbreak and an endemic period in Colombia. Front. Med. 11:1380129. doi: 10.3389/fmed.2024.1380129
Edited by:
Robert W. Maitta, Case Western Reserve University, United StatesReviewed by:
José Eduardo Levi, University of São Paulo, BrazilPritom Chowdhury, Tea Research Association, India
Copyright © 2024 Cáceres Munar, Urbina, Ortíz, Rodríguez, Fernández, Ospina, Flórez, Uribe, Alvarado, Calvo, Delgado and Castellanos. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Félix Giovanni Delgado, ZGVsZ2Fkb2ZlbGl4QHVuYm9zcXVlLmVkdS5jbw==