 Onur Yazdan Balçık
Onur Yazdan Balçık Bilgin Demir2
Bilgin Demir2 Baran Akagündüz
Baran Akagündüz- 1Department of Medical Oncology, Mardin Training and Research Hospital, Mardin, Türkiye
- 2Department of Medical Oncology, Ataturk State Hospital, Aydın, Türkiye
- 3Department of Medical Oncology, Antalya Training and Research Hospital, Antalya, Türkiye
- 4Department of Medical Oncology, Mengücek Gazi Training and Research Hospital, Erzincan, Türkiye
Introduction: Several prognostic factors have been identified in patients with metastatic bladder cancer (BC). As it is known, older adult patients are prone to nutritional deficiency. The knowledge about nutrition and impact on survival in older patients with metastatic bladder cancer is missing. It is necessary to specifically examine this population. Because timely interventions can make a positive impact on this patients population. This retrospective study aimed to evaluate the prognostic effect of the Geriatric Nutritional Risk Index (GNRI), Controller Nutritional Status (CONUT) score and Prognostic Nutritional Index (PNI) before first-line chemotherapy in the metastatic stage in patients with metastatic bladder cancer over 70.
Participants and methods: Patients over 70 with pathologically confirmed denovo metastatic or recurrent metastatic bladder cancer were included in the study. Patients with infections diagnosed at the time of diagnosis, autoimmune diseases or history of steroid use were excluded. Since our population consists of a specific age group with a specific cancer, we found a new cut-off value by performing ROC analysis to ensure optimal sensitivity and specificity in terms of progression. Low GNRI value was related with poor nutritional status. Low PNI value was related with poor nutritional status and high CONUT score was related with poor nutritional status. Factors predicting overall survival (OS) and Progression-Free Survival (PFS) were assessed using both univariate and multivariate Cox proportional hazards analyses.
Results: 106 patients were included in the study and the average age was 75.5 years. In the GNRI-Low group, PFS was significantly shorter than that in the GNRI-High group [HR (95% CI) = 57.1 (12.8–255.5), (p < 0.001)]. Among those with a low-CONUT score, PFS was found to be longer than that in the high-CONUT group [HR (95% CI) = 1.7 (1.0–3.0), (p = 0.039)]. The median PFS of the PNI-Low group wasn’t significantly shorter than that of the PNI-High group [HR (95% CI) = 1.8 (0.5–6.2), (p = 0.359)].
Conclusion: Our study suggests that the GNRI and CONUT scores are useful for predicting survival in patients over 70 years of age with BC.
1 Introduction
Bladder cancer (BC) ranks 11th among cancers worldwide. It is four times more common in men than in women. About 10–15% of patients are metastatic at the time of diagnosis (1, 2). Although immunotherapy and other drug conjugates slightly improve prognosis in metastatic BC, platinum regimens have remained the standard of care since the early 1980s, with an overall survival (OS) of approximately 15 months (3, 4). Age, performance status, renal function, and sites of metastasis have been recognized as key prognostic factors in metastatic bladder cancer (BC) (5, 6). Determining reversible nutritional prognostic factors that may have an impact on prognosis, especially in frail and older patients is important. Because timely interventions can make a positive impact on this patient’s population. Hence, there is a necessity to delineate additional prognostic factors linked to survival in BC patients.
Malnutrition is prevalent among older individuals diagnosed with cancer, often stemming from reduced food intake, altered nutrient processing, and the impact of cancer therapies. This condition not only affects treatment decisions but also escalates the likelihood of complications and mortality, prolongs hospitalizations, and diminishes overall quality of life (7, 8). The significance of nutritional status is on the rise among cancer patients. Cancer-related cachexia often leads to muscle wasting and protein depletion, triggering systemic inflammation and hypercatabolism. Malnourished patients experience heightened toxicity rates, reduced treatment compliance, and adverse impacts on survival (9, 10).
Many methods such as Subjective Global Assessment (SGA) score and Mini-Nutritional Assessment-Short Form (MNA-SF) score (11), HALP score (12) modified Glasgow prognostic score (13) have been used to evaluate bladder cancer prognosis.
There is a need for prognostic factors that can be an objective evaluation tool, independent of physical measurements, history and anamnesis taken from the patient, which can be calculated in a short time, are non-invasive and do not require any special skills (14, 15). Nutritional status is related with survival and quality of life in older patients with cancer. We need simple blood-based biomarkers to evaluate malnutrition to predict survival and intervention. Therefore, we decided to evaluate prognostic indexes such as Geriatric Nutritional Risk Index (GNRI), Control of Nutritional Status (CONUT), Prognostic Nutritional index (PNI) in metastatic bladder cancer.
GNRI is a screening tool to predict nutrition-related risk of morbidity and mortality in older patients. GNRI is calculated using body weight, height, and serum albumin levels (16). A low GNRI has been associated with poor prognosis in many cancer types, such as prostate cancer and non-small cell lung cancer (NSCLC) (17, 18). Low GNRI has been shown to be associated with a significantly increased risk of 1-month mortality after BC surgery (19).
CONUT score is comprising serum albumin, total cholesterol, and total lymphocyte counts (20). A high CONUT score has been associated with poor prognosis (21). In a meta-analysis of esophageal and gastric cancer patients comprised the majority, a high CONUT score was associated with poor prognosis (22). In BC patients several studies demonstrated that high CONUT score was associated with poor prognosis (23).
PNI was calculated using albumin and lymphocyte counts (24). Low PNI has been found to be poor prognostic in small cell lung cancer (SCLC) and metastatic laryngeal cancer. In addition, a low PNI was found to have a poor prognosis in a study of patients with geriatric non-Hodgkin lymphoma (25, 26). A meta-analysis evaluating 13 studies with bladder cancer showed that low PNI was associated with worse survival (23).
To our knowledge, there is no other study evaluating GNRI CONUT, and PNI scores in patients over 70 years of age with metastatic BC.
This retrospective study aimed to determine whether CONUT score, GNRI, and PNI before metastatic first-line chemotherapy could be used as useful indicators of survival in metastatic BC patients.
2 Participants and methods
Patients with pathologically diagnosed metastatic BC aged 70 years and over in three different centers in Turkey between May 2016 and December 2022 were included in this study. We divided the patients into two groups; Patients who are metastatic at the time of diagnosis (denovo) or patients who are not metastatic at the time of diagnosis but are followed with surgery and/or adjuvant treatments and subsequently develop recurrence (recurrent metastatic).
Patient records and hospital databases were retrospectively reviewed. Demographic characteristics, parameters such as height and weight, initial hemogram parameters (neutrophil, monocyte, and lymphocyte counts), and biochemical parameters (albumin and total cholesterol) were recorded. The death dates of the patients who died were accessed from the death notification system where death records are kept in Turkey. The last arrival date of the surviving patients was accessed from the database of 3 different hospitals and survival outcomes were documented. Patients with a history of other malignant tumors, steroid use, known autoimmune disease, active infection at the time of diagnosis, extra-bladder urothelial disease, or missing data were excluded from the study.
GNRI, CONUT and PNI scores were determined according to the basic hematological and biochemical parameters of denovo metastatic patients before receiving their first-line chemotherapy, while recurrent metastatic patients were determined according to the parameters before receiving their first-line chemotherapy after the development of metastasis. The GNRI was computed using the formula: [1.489 × albumin g/L] + [41.7 × body weight/ideal body weight]. Ideal body weight was calculated as: body height2(m) x 22. If body weight/ideal body weight is greater than 1, this ratio is taken as 1. Since our population consists of a specific age group with a specific cancer, we found a new cut-off value by performing ROC analysis to ensure optimal sensitivity and specificity in terms of progression. The Controlled Nutritional Status (CONUT) score was derived from total cholesterol level, total lymphocyte count, and peripheral albumin level (19). PNI was calculated as 10 × serum albumin value (g/dl) + 0.005 × peripheral lymphocyte count (per mm3) (27). Low GNRI value was related with poor nutritional status. Low PNI value was related with poor nutritional status and high CONUT score was related with poor nutritional status.
The analysis was performed using SPSS 28.0 software. OS was defined as the time from diagnosis to death or last visit for denovo metastatic patients, while for recurrent metastatic patients it was defined as the time from the date of metastasis to death or last visit. PFS was calculated as the time from the date of metastatic diagnosis to the date of progression or date of last observation. Patients were considered censored on the date of the last follow-up visit.
2.1 Statistical analysis
Data were summarized using descriptive statistics such as mean, standard deviation, median, minimum, maximum, frequency, and ratios. The distribution of variables was assessed using the Kolmogorov–Smirnov test. Independent quantitative data were analyzed using independent samples t-tests and Mann–Whitney U tests. Chi-square test was employed for qualitative independent data, with the Fischer test used when conditions for the chi-square test were not met. A significant cut-off point was observed, and sensitivity, specificity, and positive and negative predictive values were detected. Survival analyzes of prognostic indices and clinical and pathological features were calculated using the Kaplan–Meier method (log-rank test). Multivariate analyzes were used to identify independent prognostic variables based on the stepwise Cox proportional hazards regression model and variables potentially affecting survival (p < 0.05 in univariate analyses). The relationship between survival time and each independent factor was indicated using the 95% confidence interval (CI). Statistical significance was set at p < 0.05.
This study was planned and conducted in accordance with Good Clinical Practices and the Declaration of Helsinki and was approved by the ethics committee of Diyarbakır Gazi Yaşargil Training and Research Hospital (date of approval and no:23.6.2023–448).
3 Results
3.1 Optimal cutoff values of geriatric nutritional risk index, controller nutritional status score and prognostic nutritional index
ROC analysis was performed to determine the most optimal value for progression. This cut-off value was found to be 54 for GNRI (AUC = 0.7; 95% CI 0.6–0.7, p < 0.008, sensitivity 91%, specificity 39%). If GNRI ≤54, it was classified as GNRI-Low, and if >54, it was classified as GNRI-High. This cut-off value was found to be 2 for the CONUT score (AUC = 0.6; 95% CI 0.5–0.7, p < 0.019, sensitivity 94, specificity 33%). When the CONUT score was ≤2, it was classified as CONUT-Low, and when >2 it was classified as CONUT-High. The optimal cut-off value for PNI was found to be 37 (AUC = 0.7; 95% CI 0.6–0.7, p < 0.005, sensitivity 94, specificity 32%). PNI score was classified as PNI-Low when ≤37 and PNI-High when >37 (Figure 1).
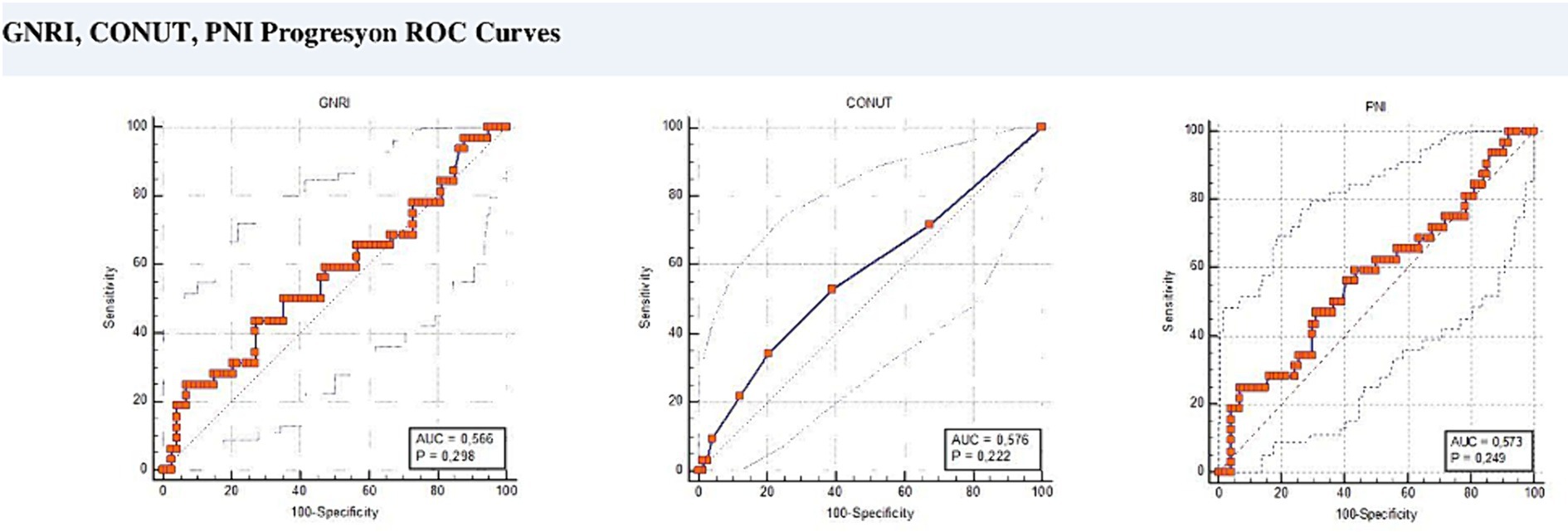
Figure 1. ROC curves for cut-off values.
3.2 Population characteristics
A total of 106 patients were included in this study and the median age was calculated as 75.5 (71–79) years. Of these patients, 89 (84.0%) were male. The number of patients with an Eastern Cooperative Oncology Group (ECOG) performance scale score of 0 or 1 was 79 (74%). While 62 (58.49%) of our patients were denovo metastatic, 44 (41.51%) were recurrent metastatic. The average time from diagnosis to metastasis development in recurrent metastatic patients is 4.7 years. The number of patients receiving TUR-M (Transurethral resection) and intravesical BCG as local treatment was 24 (22.4%). Patients received intravesical chemotherapy for 6 months. Adjuvant radiotherapy was received by 26 (24.5%) individuals. Patients received adjuvant radiotherapy for 10 workdays. The number of patients who underwent cystectomy surgery was 13 (12.3%). These 13 patients received adjuvant chemotherapy. They received adjuvant chemotherapy with a platinum analog (carboplatin or cisplatin) plus gemcitabine on the first day and gemcitabine alone on the 8th day, for a total of 3 months. The most common site of metastasis was the lung with 43.4% (46 patients). Of the total patients, 67% (n = 71) died. Demographic information of all patients is presented in Table 1.
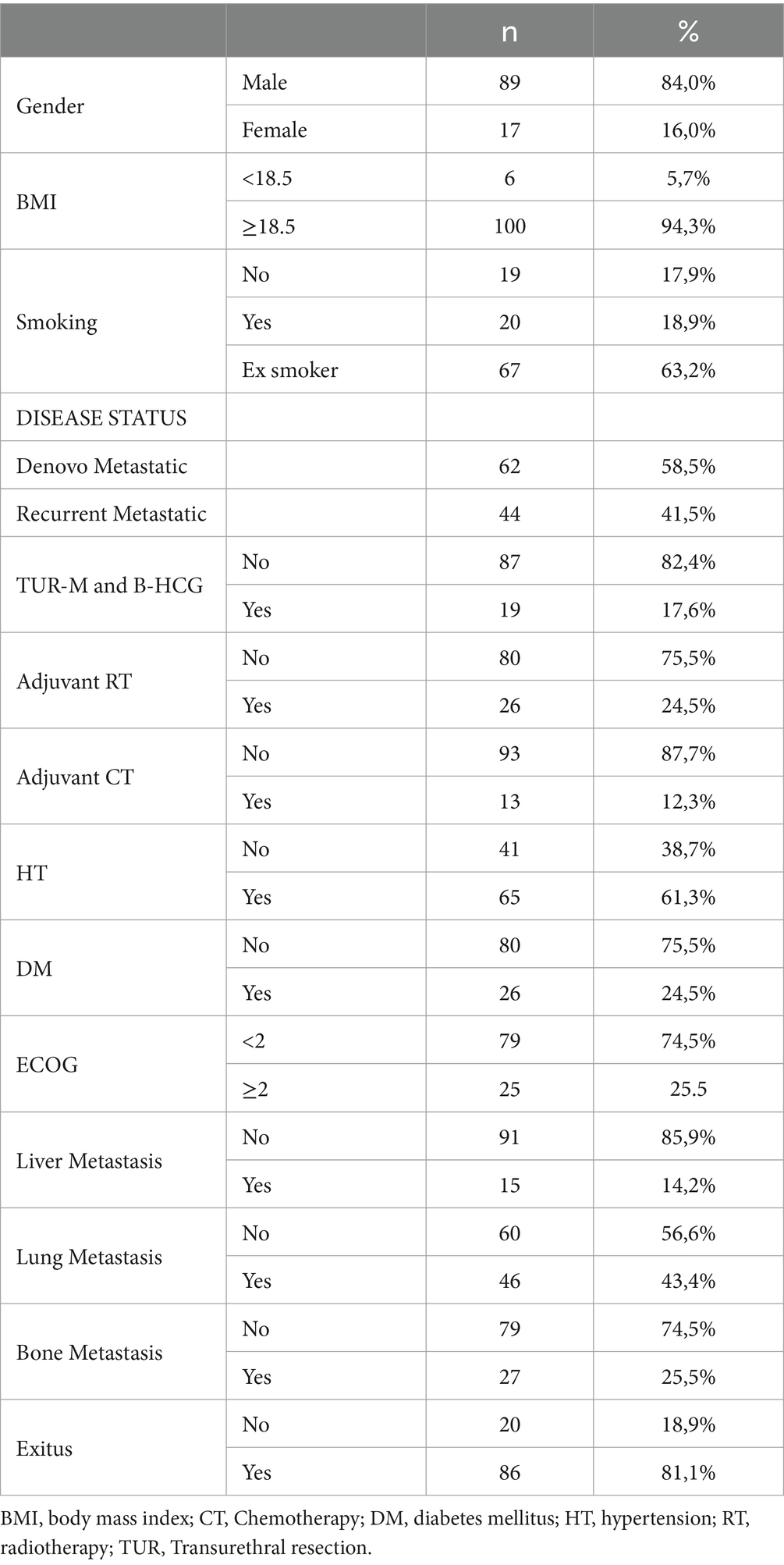
Table 1. Baseline characteristics of the all population.
3.3 Characteristics of groups according to univariate analysis
Number of GNRI-High group patients is 63, the number of GNRI-Low group patients is 43. In the GNRI-High group, the proportion of male patients was significantly higher than that in the GNRI-Low group (p < 0.05). Likewise, the ECOG 0–1 score in the GNRI-High group was significantly higher than in the group with GNRI-Low group (p < 0.05; Supplementary Table 1).
Number of CONUT-High group patients is 26, the number of CONUT-Low group patients is 80. The number of patients with ECOG scores II-III in the CONUT-Low group was significantly higher than in the CONUT- High group (p < 0.05; Supplementary Table 2).
Number of PNI-High group patients is 66, the number of PNI-Low group patients is 40. The proportion of male patients was significantly higher in the PNI-High group than in the PNI-Low group (p < 0.05). Similarly, the ECOG 0- I score in the PNI-High group was significantly higher than that in the PNI-Low group (p < 0.05). The exit us rate in the PNI-high group was significantly higher than that in the PNI-low group (p < 0.05). Apart from this, no statistically significant difference was found between the PNI-High and PNI-Low groups (p > 0.05; Supplementary Table 3).
3.4 Progression-free survival analyzes
The median PFS of all patients in the study was 6.9 (95% CI: 5.3–8.5) months. The median PFS of the GNRI-High group was 9.27 (95% CI:8.6–9.93) months, while the median PFS of the GNRI-Low group was 3.8 (95% CI:3.5–4.1) months. The median PFS of the GNRI-High group was significantly longer than that of the GNRI-Low group (p < 0.001; Figure 2).
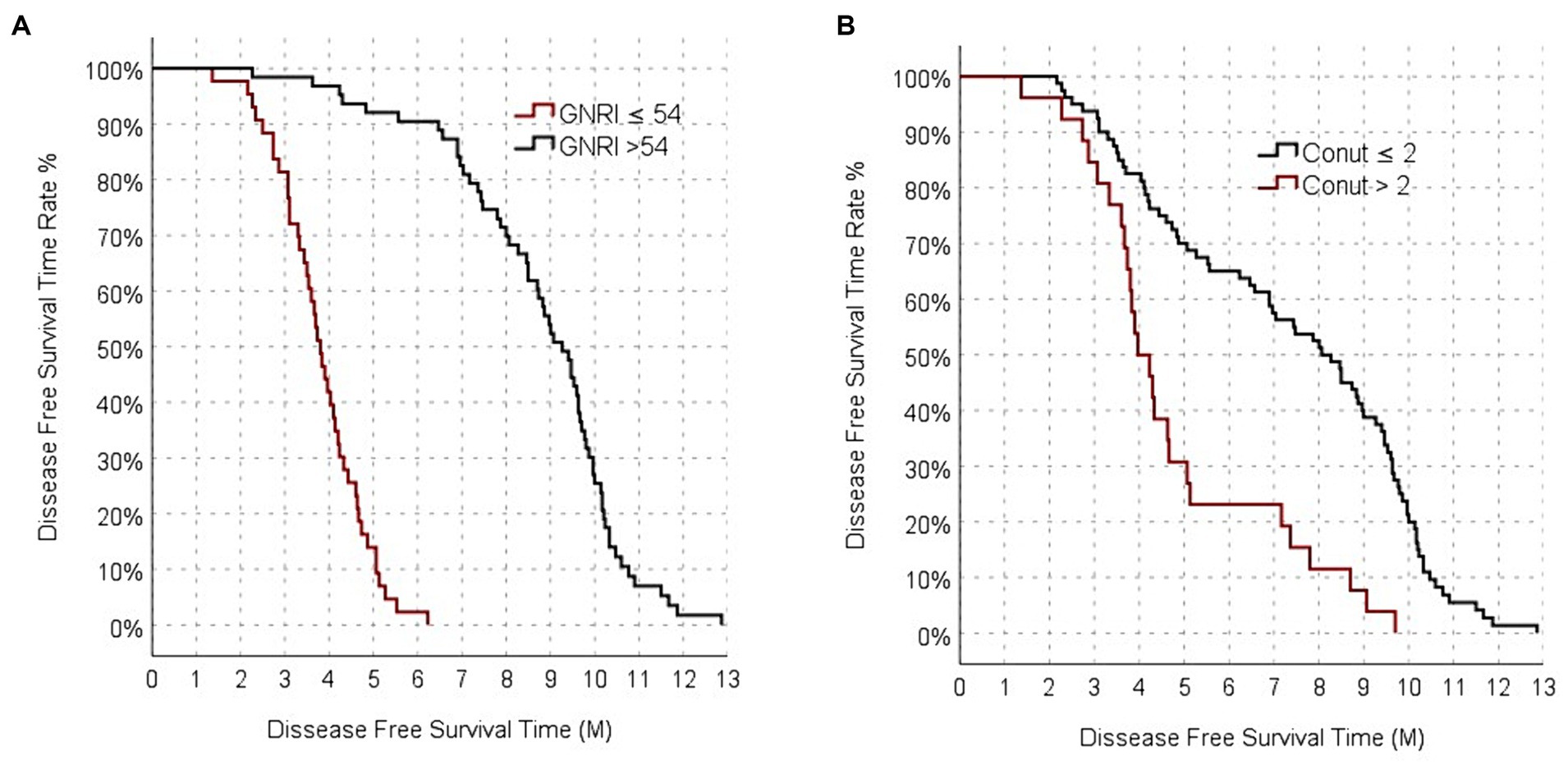
Figure 2. Progression-free survival analysis functions between GNRI (A), and CONUT (B).
The median PFS was 8.5 (95% CI: 7.5–9.1) months for CONUT-Low group, it was 4.3 (95% CI: 3.9–4.7) months for the CONUT- High group. The median PFS of the CONUT-Low group was significantly longer than that of the CONUT- High group (p < 0.001; Figure 2).
The median PFS of the PNI-High group was 9 (95% CI:8.4–9.7) months, while the median PFS of the PNI-Low group was calculated as 3.80 (95% CI: 3.4–4.2) months. The median PFS of the PNI-Low group was significantly shorter than that of the PNI-High group (p < 0.001).
The median PFS was 5.1 (95% CI: 3.7–6.5) months in male patients. It was 7.4 (95% CI: 6.1–8.7) months in female patients, but it was not statistically significant (p: 0.337). The median PFS of those with ECOG Performance score I was 8 (95% CI: 6.7–9.3) months, while the median PFS of those with ECOG II-III was 4.3 (95% CI: 3.8–4.9) months. It was statistically significant (p: 0.004). While the median PFS of those receiving platinum plus taxane as metastatic first-line chemotherapy was 7.4 (95% CI: 6.1–8.7) months, the median PFS of those receiving single-agent gemcitabine was 4.2 (95% CI: 1.1–7.4) months. The median PFS of patients receiving the platinum plus gemcitabine combination was found to be 3.5 (95% CI: 2.3–4.1) months. The median PFS of those receiving platinum plus taxane was statistically higher and more significant than the other groups (p: 0.008). No significance was found in median PFS according to lung, liver, and bone metastases. No significance was found in median PFS according to diabetes mellitus and hypertension. PFS according to univariate analysis is shown in Table 2.
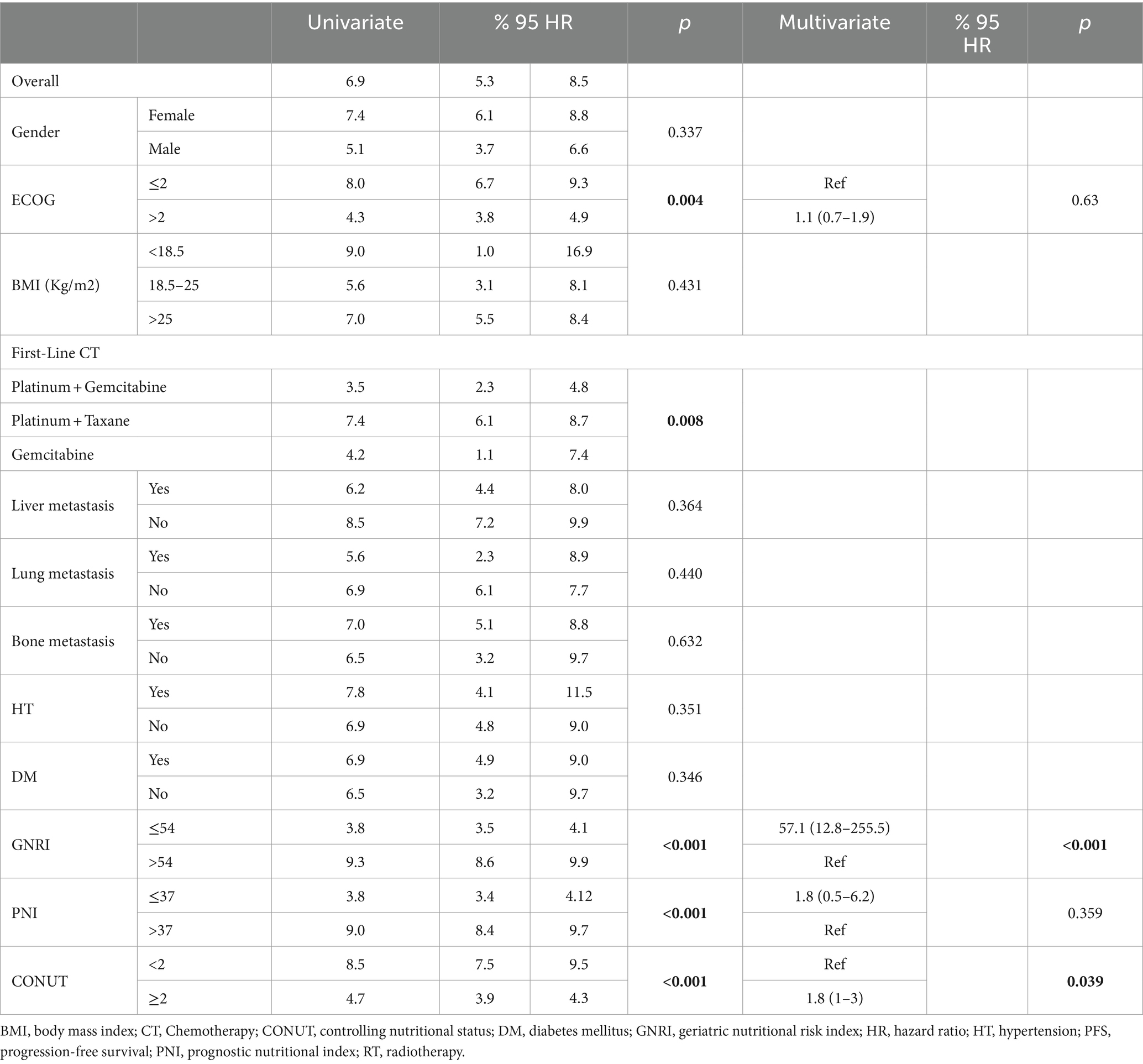
Table 2. Univariate and multivariate analysis of PFS.
According to the univariate analysis results, there was significance in GNRI, PNI, CONUT score, first-line chemotherapy selection, ECOG, and gender parameters. Since our primary hypothesis was to examine the effect of GNRI, PNI and CONUT score on prognosis and also because the patients’ ECOG performance status may affect prognosis, we planned a multivariate analysis regarding these 4 parameters.
Multivariate Cox regression analysis was performed to identify independent prognostic factors that could determine PFS. PFS was found to be lower in the GNRI-Low group than in the GNRI-High group [HR (95% CI) = 57.1 (12.8–255.5), (p < 0.001)]. In the CONUT-Low group, PFS was found to be higher than in the CONUT- High group [HR (95% CI) = 1.7 (1.0–3.01, p: 0.039)]. PFS of the PNI-Low group was shorter than that of the PNI-High group. But it was not significant [HR (95% CI) = 1.8 (0.5–6.2), (p = 0.359)]. PFS of those with ECOG Performance score I was longer than PFS of those with ECOG II-III. [HR (95% CI) = 1.1 (0.7–1.9), (p < 0.001)]. PFS according to Multivariate analysis is shown in Table 2.
3.5 Overall survival analyzes
In the entire population, median OS was 8.78 (95% CI: 1.85–16.02) months. The median OS value of the GNRI-High group was 15.9 (95% CI: 1.56–22.03) months, while the median OS value of the GNRI-Low group was 4.89 (95% CI: 0.63–7.38) months. The median OS of the GNRI-High group was significantly longer than that of the GNRI-Low group (p < 0.001; Figure 3).
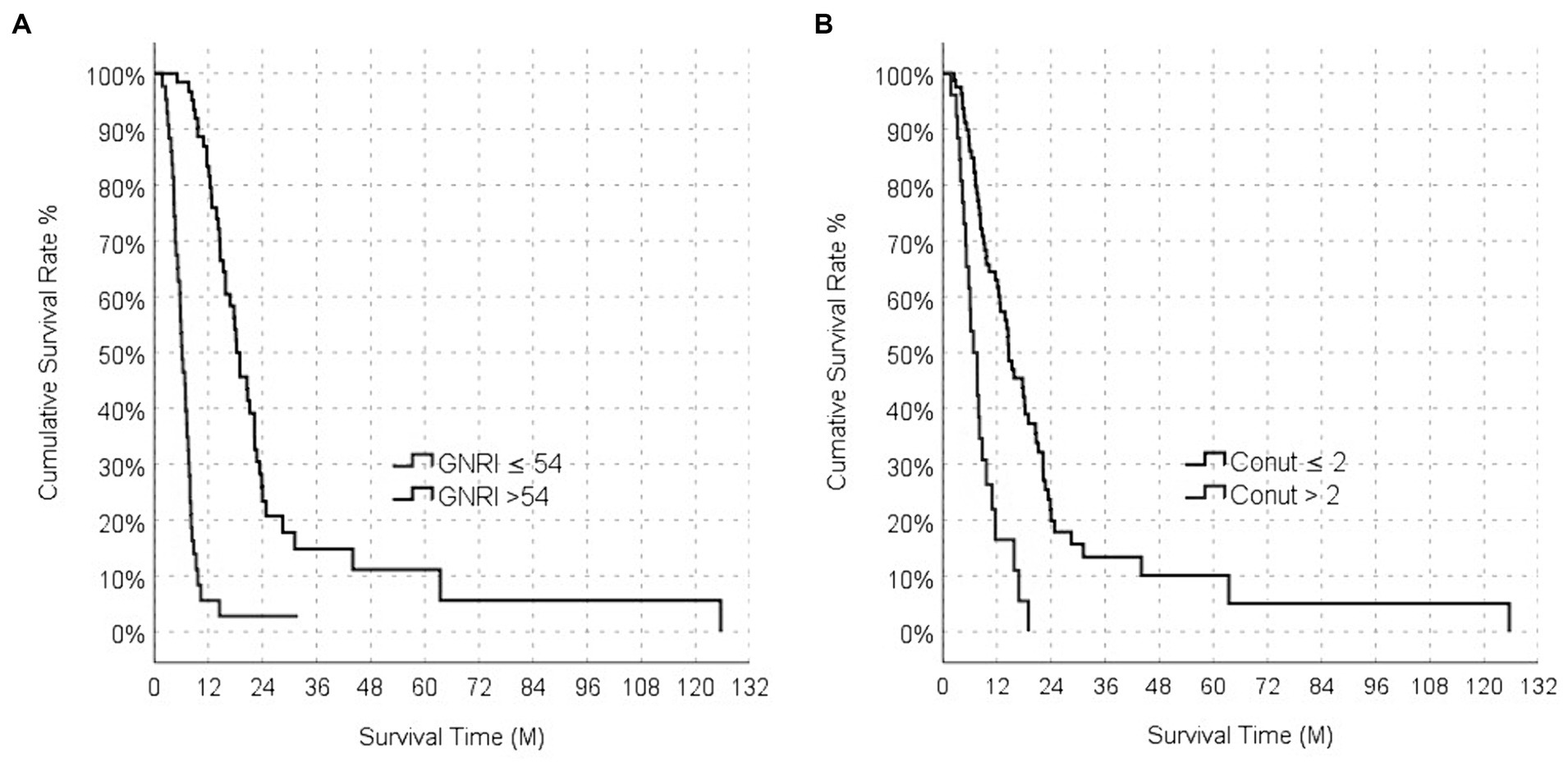
Figure 3. Overall survival analysis functions between GNRI (A), and CONUT (B).
The median OS of the CONUT-Low group was 11.3 (95% CI: 2.3–20.3) months, while the median OS of the CONUT-High group CONUT was 5.1 (95% CI: 0.7–8.0) months. The median OS in the CONUT-Low group was longer than that in the CONUT- High group, and this difference was statistically significant (p < 0.001; Figure 3).
The median OS of the PNI-High group was calculated as 15.7 (95% CI: 1.2–20.5) months, while the median OS value of the PNI-Low group was calculated as 5.2 (95% CI: 0.5–6.9) months. The median OS of the PNI-Low group was significantly shorter than that of the PNI-High group (p < 0.001).
The median OS was 12.4 (95% CI: 4.8–14.1) months in male patients; it was 7.5 (95% CI: 10.7–18.1) months in female patients. The median OS of male patients was higher than that of female patients and was statistically significant (p:0.004). The median OS of those with ECOG Performance score I was 14.7 (95% CI: 10.9–18.4) months while the median OS of those with ECOG II-III was 6.3 (95% CI: 4.2–8.5) months, which was statistically significant (p < 0.001). While the median OS of those receiving platinum plus taxane as metastatic first-line chemotherapy was 13.7 (95% CI: 11.1–16.4) months, the median OS of those receiving single-agent gemcitabine was 5.2 (95% CI: 0–12.8) months. The median OS of patients receiving the platinum plus gemcitabine combination was found to be 5.6 (95% CI: 1.4–9.9) months. The median OS of those receiving platinum plus taxane was statistically higher and more significant than the other groups (p < 0.001). No significance was found in median OS according to lung, liver and bone metastases. No significance was found in median OS according to diabetes mellitus and hypertension. OS according to univariate analysis is shown in Table 3.
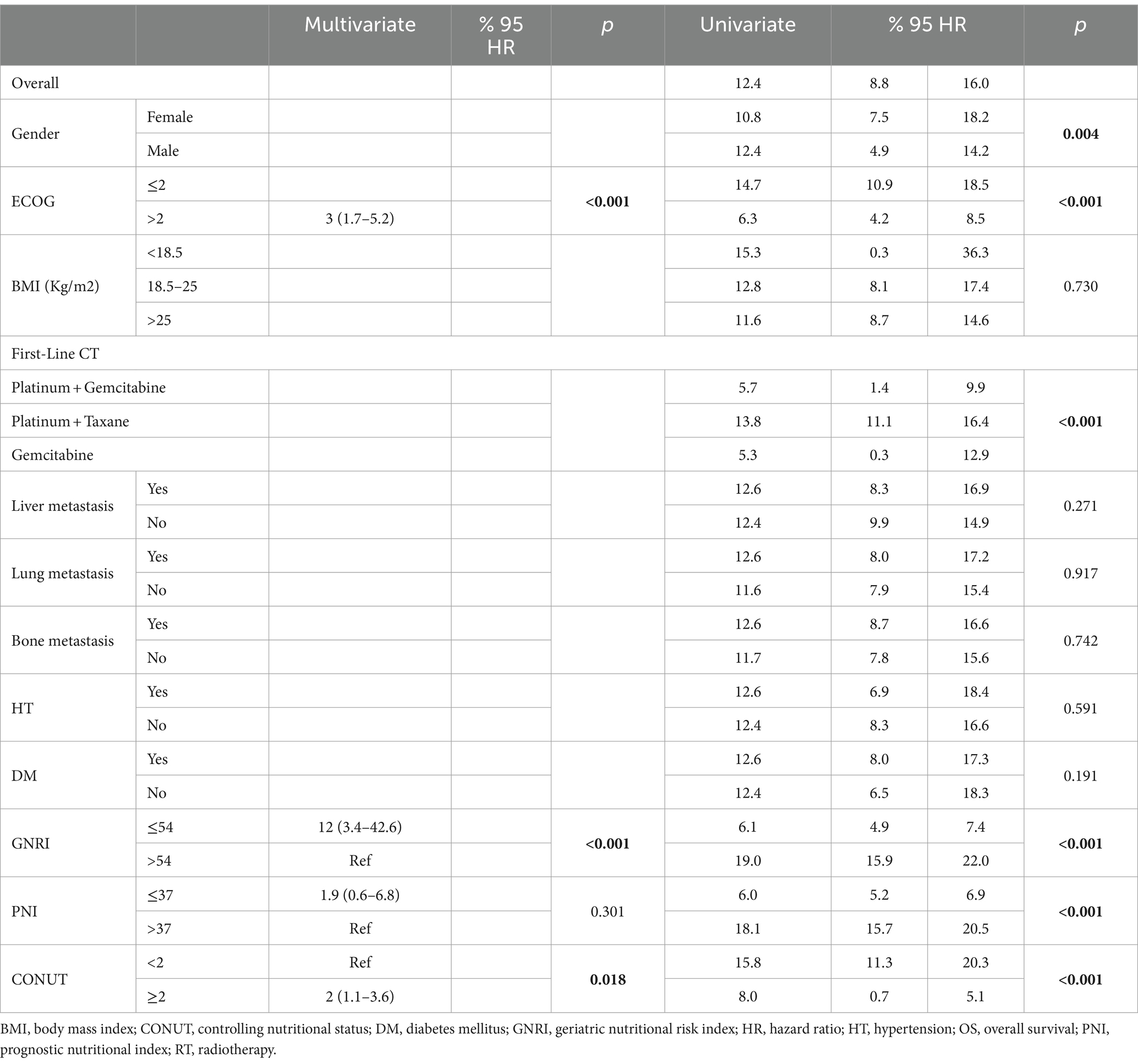
Table 3. Univariate and multivariate analysis of OS.
Multivariate Cox regression analysis was performed to identify independent prognostic factors that could determine OS. OS was lower in the GNRI-Low group than in the GNRI-High group [HR (95% CI) = 12 (3.4–42.6), (p < 0.001)]. OS was found to be higher in CONUT-Low group than in the CONUT- High group [HR (95% CI) = 2.0 (1.2–3.6), (p = 0.018)]. OS of the PNI-Low group was shorter than that of the PNI-High group. But it was not significant [HR (95% CI) = 1.9 (0.6–6.8), (p = 0. 301)]. PFS of those with ECOG Performance score I was longer than PFS of those with ECOG II-III. [HR (95% CI) = 3 (1.7–5.2), (p: 0.063)]. OS according to multivariate analysis is shown in Table 3.
4 Discussion
Many prognostic nutritional factors have been identified in metastatic bladder cancer. Lower body mass index led to increased post-operative complications in patients with operated upper urothelial cancer. Malnutrition seriously affected the prognosis (28). Acar et al., the study revealed that patients with higher HALP scores, which are associated with nutrition, exhibited better survival rates in metastatic bladder cancer. In another study, the correlated prognostic effect of the modified Glasgow prognostic score, which indicates nutritional status, was observed in metastatic bladder cancer (13).
4.1 Geriatric nutritional risk index
In this study, we found that the GNRI score are useful prognostic factors in patients with BC aged over 70. Owing to the increasing older adult patients population, special nutritional approaches and prognostic markers have become mandatory. The GNRI, which is a factor that evaluates albumin and desired weight and actual weight, is an important index that combines the two factors and shows acute and chronic problems of nutrition (29).
When we look at the literature, there are many studies on the relationship between GNRI and older cancer. GNRI is a better prognostic factor than the Mini Nutritional Assessment (MNA), previously found in older patients with cancer (30). In a study of 854 patients aged 65 years and older with early-stage cancer, primarily stomach and NSCLC, low GNRI was associated with poor prognosis (31). In a study conducted by Riveros et al. with 1,564 patients aged 65 and over with operated bladder cancer, low GNRI was associated with low survival (19). In a study conducted by Pan et al., which included 442 patients aged 65 and over with bladder cancer who underwent cystectomy, low GNRI was associated with low survival (32).
Many studies have been conducted on urothelial carcinoma in both early and metastatic stages. In a study of 458 patients with upper urinary tract urothelial carcinoma who underwent radical nephrouterectomy, GNRI was found to be an independent predictor of prognosis and postoperative complications (33). In a study of 68 patients with metastatic urothelial cancer receiving cisplatin-gemcitabine in the first row, low GNRI was associated with poor survival (34). In a study evaluating 198 patients with metastatic urothelial carcinoma who received second-line immune checkpoint inhibitors, low GNRI was associated with poor survival (35).
As can be seen, the effect of nutrition on the prognosis of bladder cancer is clear. The prognostic effect of GNRI has been demonstrated in older adult cancer patients. The prognostic effect of GNRI has also been demonstrated in non-bladder cancer and early-stage bladder cancer in patients over the age of 65. To our knowledge, there is no other study other than ours showing the prognostic effect of GNRI in patients with metastatic urothelial cancer over 70.
4.2 Controller nutritional status score
Hypoalbuminemia indicates malnutrition. In the presence of malignancy, hypoalbuminemia is observed due to both nutrition and inflammation, and it is known that this leads to a poor prognosis (36). It has been shown that hypercholesterolemia plays a role in cancer pathogenesis and prognosis by causing a decrease in the resistance of cells in tumor growth and metastasis (37). It has been shown that some hematological parameters, especially lymphocyte neutrophils, play an important role in cancer prognosis (38). The CONUT score was developed because these three parameters play a separate role in prognosis (20).
There have been many studies related to this phenomenon in urogenital system. In a study by Claps et al., a high CONUT score was associated with poor PFS in patients with operated bladder cancer (39). In a meta-analysis of 5,040 patients with RCC and upper urothelial carcinoma who underwent nephrectomy, a high CONUT score correlated with poor survival (40). In a study of 347 patients who underwent radical cystectomy, with a median age of 72, it was observed that a high preoperative CONUT score was associated with poor survival (39). In a study of 94 patients with non-invasive BC, the CONUT score obtained before treatment was correlated with poor survival and recurrence (41). In another meta-analysis examining 4,044 patients with metastatic urothelial carcinoma, pretreatment CONUT score was correlated with poor survival (42).
We conducted our study because nutrition affects the prognosis of both bladder cancer and the geriatric population, and we found that a high CONUT score is correlated with a poor prognosis. Our study is consistent with the literature. As far as we know, it is the first study to evaluate the poor prognostic effect of a high CONUT score in patients with metastatic bladder cancer over 70.
High-risk patients can be identified by calculating the GNRI and CONUT score, which affect the prognosis in bladder cancer patients. Thus, if we can identify treatable nutritional factors, starting treatment by correcting them as much as possible before chemotherapy will help improve the prognosis.
4.3 Prognostic nutritional index
The PNI is a practical test calculated using serum albumin and lymphocyte counts. Albumin, alone or in combination with other factors, is a negative acute-phase reactant that indicates the nutritional status. Since albumin is a marker regulated by the proinflammatory cytokines IL-1 and IL-6 and Tumor necrosis factor alpha (TNF-alpha), it is associated with inflammation (43). On the other hand, lymphocytes play an important role in cellular immunity by inhibiting the migration of cancer cells, and in the case of lymphocytopenia, the migration and invasion capabilities of cancer cells increase (44).
In the study conducted by Yılmaz et al. in 154 patients with muscle invasive bladder cancer, low PNI was associated with low PFS (45). In the study conducted by Bi et al., which included 387 high-risk NMIBC patients, high PNI predicted higher survival outcomes (46). In a study involving patients with metastatic urothelial carcinoma, a low PNI was associated with poor prognostic factors (47).
The PNI is a prognostic marker for evaluating nutrition and inflammation. We aimed to determine the prognostic effect of PNI in the geriatric population, and found that high PNI led to high survival, but this was not statistically significant. If a study with a homogeneous population with a higher number of patients is planned, PNI may gain prognostic importance.
4.4 Strengths and limitations
The fact that recurrent metastatic patients receive treatment until the time of recurrence and different protocols make our population heterogeneous. Considering the high variability of the population and the small sample size, it reduces the power of our analysis.
We acknowledge a limitation of our study in not excluding patients with conditions like familial short stature, obesity, heart failure, and protein-losing nephropathy, which may impact GNRI. Similarly, patients with conditions leading to hypoalbuminemia, such as familial hypercholesterolemia unrelated to nutrition, were not excluded, potentially influencing the CONUT score. Interpretation of these scores should be approached cautiously as they may be influenced by conditions unrelated to nutritional status. A holistic evaluation is recommended to better understand their impact on prognosis.
Although our study is the first to show GNRI and CONUT score as independent predictive factors for PFS and OS in patients in the geriatric population, the retrospective nature of our study was one of the most important limiting factors. Since we could not examine the molecular features of metastatic BC due to technical reasons, the prognosis of the patients may have been affected. Another limiting factor was the lack of clear consensus on cut-off points for the GNRI and CONUT scores due to the limited number of studies. We hope that our study will provide the basis for prospective multicenter studies to better understand the factors that cause survival benefits.
We believe that our study is the first to show that both GNRI and CONUT scores independently serve as prognostic factors for progression-free survival (PFS) and overall survival (OS) in BC patients over 70. However, it is important to note that the retrospective design and the relatively small sample size were the primary constraints of our study.
5 Conclusion
In conclusion, the GNRI and CONUT represent practical and successful indices for predicting prognosis in patients over 70 with metastatic BC receiving chemotherapy. If validated through prospective studies, these indices could be useful in routine clinical practice for predicting the prognosis of older patients with metastatic BC.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Ethics committee of Diyarbakır Gazi Yaşargil Training and Research Hospital (date of approval and no: 23.6.2023–448). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
OB: Conceptualization, Investigation, Methodology, Project administration, Resources, Software, Supervision, Visualization, Writing – original draft, Writing – review & editing, Data curation, Formal analysis, Validation. BD: Conceptualization, Data curation, Methodology, Project administration, Resources, Supervision, Writing – review & editing. Yİ: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Resources, Supervision, Writing – original draft. BA: Conceptualization, Investigation, Methodology, Resources, Supervision, Visualization, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2024.1376607/full#supplementary-material
References
1. Burger, M, Catto, JW, Dalbagni, G, Grossman, HB, Herr, H, Karakiewicz, P, et al. Epidemiology and risk factors of urothelial bladder cancer. Eur Urol. (2013) 63:234–41. doi: 10.1016/j.eururo.2012.07.033
2. Antoni, S, Ferlay, J, Soerjomataram, I, Znaor, A, Jemal, A, and Bray, F. Bladder cancer incidence and mortality: a global overview and recent trends. Eur Urol. (2017) 71:96–108. doi: 10.1016/j.eururo.2016.06.010
3. De Santis, M, Bellmunt, J, Mead, G, Kerst, JM, Leahy, M, Maroto, P, et al. Randomized phase II/III trial assessing gemcitabine/carboplatin and methotrexate/carboplatin/vinblastine in patients with advanced urothelial cancer who are unfit for cisplatin-based chemotherapy: EORTC study 30986. J Clin Oncol. (2012) 30:191–9. doi: 10.1200/JCO.2011.37.3571
4. Bellmunt, J, von der Maase, H, Mead, GM, Skoneczna, I, De Santis, M, Daugaard, G, et al. Randomized phase III study comparing paclitaxel/cisplatin/gemcitabine and gemcitabine/cisplatin in patients with locally advanced or metastatic urothelial cancer without prior systemic therapy: EORTC intergroup study 30987. J Clin Oncol. (2012) 30:1107–13. doi: 10.1200/JCO.2011.38.6979
5. Apolo, AB, Ostrovnaya, I, Halabi, S, Iasonos, A, Philips, GK, Rosenberg, JE, et al. Prognostic model for predicting survival of patients with metastatic urothelial cancer treated with cisplatin-based chemotherapy. J Natl Cancer Inst. (2013) 105:499–503. doi: 10.1093/jnci/djt015
6. Galsky, M, Moshier, E, and Krege, S. Nomogram for predicting survival in patients with unresectable and/or metastatic urothelial cancer who are treated with cisplatin-based chemotherapy. Cncr. (2013) 119:3012–9. doi: 10.1002/cncr.28146
7. Marshall, KM, Loeliger, J, Nolte, L, Kelaart, A, and Kiss, NK. Prevalence of malnutrition and impact on clinical outcomes in cancer services: a comparison of two time points. Clin Nutr. (2019) 38:644–51. doi: 10.1016/j.clnu.2018.04.007
8. Charlton, K, Nichols, C, Bowden, S, Milosavljevic, M, Lambert, K, Barone, L, et al. Poor nutritional status of older subacute patients predicts clinical outcomes and mortality at 18 months of follow-up. Eur J Clin Nutr. (2012) 66:1224–8. doi: 10.1038/ejcn.2012.130
9. Zhang, X, Tang, T, Pang, L, Sharma, SV, Li, R, Nyitray, AG, et al. Malnutrition and overall survival in older adults with cancer: A systematic review and meta-analysis. J Geriatr Oncol. (2019) 10:874–83. doi: 10.1016/j.jgo.2019.03.002
10. Fearon, K, Strasser, F, Anker, SD, Bosaeus, I, Bruera, E, Fainsinger, RL, et al. Definition and classification of cancer cachexia: an international consensus. Lancet Oncol. (2011) 12:489–95. doi: 10.1016/S1470-2045(10)70218-7
11. Takagi, K, Takahashi, H, Miura, T, Yamagiwa, K, Kawase, K, Muramatsu-Maekawa, Y, et al. Prognostic value of various nutritional risk markers in patients hospitalized for the treatment of genitourinary cancer: A retrospective study. Clinical Nutrition ESPEN. (2023) 55:44–50. doi: 10.1016/j.clnesp.2023.03.002
12. Acar, O, Ayhan, M, Demir, B, Ekinci, F, Aytac, A, and Erdogan, AP. HALP score as a new prognostic factor for patients with metastatic bladder Cancer. J Coll Physicians Surg Pak. (2023) 33:1405–9. doi: 10.29271/jcpsp.2023.12.1405
13. Nagai, T, Naiki, T, Isobe, T, Sugiyama, Y, Etani, T, Iida, K, et al. Modified Glasgow prognostic score 2 as a prognostic marker in patients with metastatic urothelial carcinoma. In Vivo. (2021) 35:2793–800. doi: 10.21873/invivo.12565
14. Matsumoto, S, Miyamoto, H, Hirose, Y, Nishimura, B, Tanaka, S, Wada, T, et al. The geriatric nutritional risk index as a prognostic factor in patients with advanced head and neck cancer. Laryngoscope. (2021) 131:E151e6. doi: 10.1002/lary.28587
15. Zhu, X, Zhao, Y, Ma, F, and Wu, S. Controlling nutritional status score predicts the individualized survival of patients with gastric cancer. Asia Pac J Clin Nutr. (2021) 30:51e9. doi: 10.6133/apjcn.202103_30(1).0007
16. Bouillanne, O, Morineau, G, Dupont, C, Coulombel, I, Vincent, JP, Nicolis, I, et al. Geriatric nutritional risk index: a new index for evaluating at-risk elderly medical patients. Am J Clin Nutr. (2005) 82:777–83. doi: 10.1093/ajcn/82.4.777
17. Chang, LW, Hung, SC, Li, JR, Chiu, KY, Yang, CK, Chen, CS, et al. Geriatric nutritional risk index as a prognostic marker for patients with metastatic castration-resistant prostate Cancer receiving docetaxel. Front Pharmacol. (2021) 11:601513. doi: 10.3389/fphar.2020.601513
18. Yang, M, Liu, Z, Li, G, Li, B, Li, C, Xiao, L, et al. Geriatric nutritional risk index as a prognostic factor of patients with non-Small cell lung Cancer: A Meta-analysis. Hormone and metabolic research = Hormon- und Stoffwechselforschung =. Hormones. (2022) 54:604–12. doi: 10.1055/a-1903-1943
19. Riveros, C, Jazayeri, SB, Chalfant, V, Ahmed, F, Bandyk, M, and Balaji, KC. The geriatric nutritional risk index predicts postoperative outcomes in bladder cancer: a propensity score-matched analysis. J Urol. (2022) 207:797–804. doi: 10.1097/JU.0000000000002342
20. de Ulíbarri, JI, González-Madroño, A, de Villar, NG, González, P, González, B, Mancha, A, et al. CONUT: a tool for controlling nutritional status. First validation in a hospital population. Nutr Hosp. (2005) 20:38–45.
21. Chen, L, Sun, H, Zhao, R, Huang, R, Pan, H, Zuo, Y, et al. Controlling nutritional status (CONUT) predicts survival in gastric Cancer patients with immune checkpoint inhibitor (PD-1/PD-L1) outcomes. Front Pharmacol. (2022) 13:836958. doi: 10.3389/fphar.2022.836958
22. Liang, RF, Li, JH, Li, M, Yang, Y, and Liu, YH. The prognostic role of controlling nutritional status scores in patients with solid tumors. Clin Chim Acta. (2017) 474:155–8. doi: 10.1016/j.cca.2017.09.021
23. Jiao, H, Wang, L, Zhou, X, Wu, J, and Li, T. Prognostic ability of nutritional indices for outcomes of bladder Cancer: A systematic review and Meta-analysis. Urol Int. (2023) 107:886–94. doi: 10.1159/000531884
24. Onodera, T, Goseki, N, and Kōsaki, G. Prognostic nutritional index in gastrointestinal surgery of malnourished cancer patients. Nihon Geka Gakkai Zasshi. (1984) 85:1001–5.
25. Wu, CY, Lin, YH, Lo, WC, Cheng, PC, Hsu, WL, Chen, YC, et al. Nutritional status at diagnosis is prognostic for pharyngeal cancer patients: a retrospective study. Eur Arch Otorrinolaringol. (2022) 279:3671–8. doi: 10.1007/s00405-021-07222-5
26. Hong, S, Zhou, T, Fang, W, Xue, C, Hu, Z, Qin, T, et al. The prognostic nutritional index (PNI) predicts overall survival of small-cell lung cancer patients. Tumour Biol. (2015) 36:3389–97. doi: 10.1007/s13277-014-2973-y
27. Ni, L, Huang, J, Ding, J, Kou, J, Shao, T, Li, J, et al. Prognostic nutritional index predicts response and prognosis in Cancer patients treated with immune checkpoint inhibitors: A systematic review and Meta-analysis. Front Nutr. (2022) 9:823087. doi: 10.3389/fnut.2022.823087
28. Yeh, HC, Li, CC, Chien, TM, Li, CY, Cheng, YC, Woldu, SL, et al. Interethnic differences in the impact of body mass index on upper tract urothelial carcinoma following radical nephroureterectomy. World J Urol. (2021) 39:491–500. doi: 10.1007/s00345-020-03204-0
29. Cereda, E, and Pedrolli, C. The geriatric nutritional risk index. Curr Opin Clin Nutr Metab Care. (2009) 12:1–7. doi: 10.1097/MCO.0b013e3283186f59
30. Cereda, E, Pusani, C, Limonta, D, and Vanotti, A. The ability of the geriatric nutritional risk index to assess the nutritional status and predict the outcome of home-care resident elderly: a comparison with the Mini nutritional assessment. Br J Nutr. (2009) 102:563–70. doi: 10.1017/S0007114509222677
31. Liu, C, Lu, Z, Chen, L, Yang, X, Xu, J, Cui, H, et al. Predictive value of geriatric nutritional risk index in older adult Cancer patients. J Nutr. (2022) 26:153–6. doi: 10.1007/s12603-022-1729-4
32. Pan, Y, Zhong, X, and Liu, J. The prognostic significance of geriatric nutritional risk index in elderly patients with urinary bladder cancer after radical cystectomy. Asian J Surg. (2023) 46:2178–9. doi: 10.1016/j.asjsur.2022.11.082
33. Wu, P, Liu, J, Wang, X, Lai, S, Wang, J, Wang, J, et al. Development and validation of a nomogram based on geriatric nutritional risk index for predicting prognosis and postoperative complications in surgical patients with upper urinary tract urothelial carcinoma. J Cancer Res Clin Oncol. (2023) 149:18185–200. doi: 10.1007/s00432-023-05462-y
34. Naiki, T, Nagai, T, Sugiyama, Y, Etani, T, Nozaki, S, Iida, K, et al. First Report of Oncological Outcome and Prognostic Analysis in a First-Line Setting of Short Hydration Gemcitabine and Cisplatin Chemotherapy for Patients with Metastatic Urothelial Carcinoma. Oncol. (2021) 99:622–631.
35. Isobe, T, Naiki, T, Sugiyama, Y, Naiki-Ito, A, Nagai, T, and Etani, T. Chronological transition in outcome of second-line treatment in patients with metastatic urothelial cancer after pembrolizumab approval: a multicenter retrospective analysis. Int J Clin Oncol. (2022) 1–10.
36. Hamaker, ME, Oosterlaan, F, van Huis, LH, Thielen, N, Vondeling, A, and van den Bos, F. Nutritional status and interventions for patients with cancer - A systematic review. J Geriatr Oncol. (2021) 12:6–21. doi: 10.1016/j.jgo.2020.06.020
37. Liu, W, Chakraborty, B, Safi, R, Kazmin, D, Chang, CY, and McDonnell, DP. Dysregulated cholesterol homeostasis results in resistance to ferroptosis increasing tumorigenicity and metastasis in cancer. Nat Commun. (2021) 12:5103. doi: 10.1038/s41467-021-25354-4
38. Scilla, KA, Bentzen, SM, Lam, VK, Mohindra, P, Nichols, EM, Vyfhuis, MA, et al. Neutrophil-lymphocyte ratio is a prognostic marker in patients with locally advanced (stage IIIA and IIIB) non-Small cell lung Cancer treated with combined modality therapy. Oncologist. (2017) 22:737–42. doi: 10.1634/theoncologist.2016-0443
39. Claps, F, Mir, MC, van Rhijn, BWG, Mazzon, G, Soria, F, D’Andrea, D, et al. Impact of the controlling nutritional status (CONUT) score on perioperative morbidity and oncological outcomes in patients with bladder cancer treated with radical cystectomy. Urol Oncol. (2023) 41:49.e13–22. doi: 10.1016/j.urolonc.2022.09.023
40. Xue, W, Hu, X, and Zhang, Y. The Association of Controlling Nutritional Status (CONUT) score with survival in patients with surgically treated renal cell carcinoma and upper tract urothelial carcinoma: A systematic review and Meta-analysis. Nutr Cancer. (2022) 74:1907–16. doi: 10.1080/01635581.2021.1974894
41. Zhao, L, Sun, J, Wang, K, Tai, S, Hua, R, Yu, Y, et al. Development of a new recurrence-free survival prediction nomogram for patients with primary non-muscle-invasive bladder cancer based on preoperative controlling nutritional status score. Cancer Manag Res. (2021) 13:6473–87. doi: 10.2147/CMAR.S323844
42. Peng, L, Du, C, Meng, C, Li, J, You, C, Li, X, et al. Controlling nutritional status score before receiving treatment as a prognostic indicator for patients with urothelial cancer: an exploration evaluation methods. Front Oncol. (2021) 11:702908. doi: 10.3389/fonc.2021.702908
43. Du, XJ, Tang, LL, Mao, YP, Sun, Y, Zeng, MS, Kang, TB, et al. The pretreatment albumin to globulin ratio has predictive value for long-term mortality in nasopharyngeal carcinoma. PLoS One. (2014) 9:94473. doi: 10.1371/journal.pone.0094473
44. Mantovani, A, Allavena, P, Sica, A, and Balkwill, F. Cancer-related inflammation. Nature. (2008) 454:436–44. doi: 10.1038/nature07205
45. Yılmaz, A, Yılmaz, H, Tekin, SB, and Bilici, M. The prognostic significance of hemoglobin-to-red cell distribution width ratio in muscleinvasive bladder cancer. Biomark Med. (2020) 14:727–38. doi: 10.2217/bmm-2020-0045
46. Bi, H, Shang, Z, Jia, C, Wu, J, Cui, B, Wang, Q, et al. Predictive values of preoperative prognostic nutritional index and systemic immune-inflammation index for long-term survival in high-risk non-muscle-invasive bladder cancer patients: a single-Centre retrospective study. Cancer Manag Res. (2020) 12:9471–83. doi: 10.2147/CMAR.S259117
Keywords: GNRI, CONUT, geriatric, bladder cancer overall survival, nutrition, progression
Citation: Balçık OY, Demir B, Ilhan Y and Akagündüz B (2024) Geriatric nutritional risk index and controller nutritional status score before metastatic first-line chemotherapy predict survival in patients over 70 years of age with metastatic bladder cancer. Front. Med. 11:1376607. doi: 10.3389/fmed.2024.1376607
Edited by:
Gülistan Bahat, Istanbul University, TürkiyeReviewed by:
Taha Koray Sahin, Hacettepe University, TürkiyeElanur Karaman, Karadeniz Technical University, Türkiye
Copyright © 2024 Balçık, Demir, Ilhan and Akagündüz. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Baran Akagündüz, ZHJiYXJhbjA0QGhvdG1haWwuY29t