 Edinson Dante Meregildo-Rodríguez1
Edinson Dante Meregildo-Rodríguez1 Gustavo Adolfo Vásquez-Tirado2*Claudia Vanessa Quispe-Castañeda2María del Carmen Cuadra-Campos2
Gustavo Adolfo Vásquez-Tirado2*Claudia Vanessa Quispe-Castañeda2María del Carmen Cuadra-Campos2 Jhuliana M. Contreras-Cabrera2Juan Luis Pinedo-Portilla3
Jhuliana M. Contreras-Cabrera2Juan Luis Pinedo-Portilla3- 1Escuela de Medicina, Universidad César Vallejo, Trujillo, Peru
- 2Facultad de Medicina Humana, Universidad Privada Antenor Orrego, Trujillo, Peru
- 3Servicio Cuidados Intermedios, Hospital Nacional Almanzor Aguinaga-Asenjo, Lambayeque, Perú
Introduction: Cervical spinal cord injury (CSCI) patients on mechanical ventilation often lack standardized guidelines for optimal ventilatory support. This study reviews existing literature to compare outcomes between high tidal volume (HTV) and low tidal volume (LTV) strategies in this unique patient population.
Methods: We searched for studies published up to August 30, 2023, in five databases, following a PECO/PICO strategy. We found six studies for quantitative analysis and meta-analyzed five studies.
Results: This meta-analysis included 396 patients with CSCI and mechanical ventilation (MV), 119 patients treated with high tidal volume (HTV), and 277 with low tidal volume (LTV). This first meta-analysis incorporates the few studies that show contradictory findings. Our meta-analysis shows that there is no significant statistical difference in developing VAP between both comparison groups (HTV vs. LTV) (OR 0.46; 95% CI 0.13 to 1.66; p > 0.05; I2: 0%), nor are there differences between the presence of other pulmonary complications when treating with HTV such as acute respiratory distress syndrome (ARDS), atelectasis, onset of weaning.
Conclusion: In patients with CSCI in MV, the use of HTV does not carry a greater risk of pneumonia compared to LTV; in turn, it is shown as a safe ventilatory strategy as it does not establish an increase in other pulmonary complications such as ARDS, atelectasis, the onset of weaning nor others associated with volutrauma. It is necessary to evaluate the role of HTV ventilation in this group of patients in primary RCT-type studies.
1 Introduction
Cervical spinal cord injury (CSCI) usually entails the need for constant ventilatory support as mechanical ventilator (MV), requiring mechanical ventilation immediately after the injury in most cases (1–3).
The management of ventilatory support in CSCI patients is not standardized according to their specific needs, since existing management protocols based on multiple clinical trials for optimal mechanical ventilation settings are designed for patients with acute respiratory distress syndrome (ARDS) without neurological injury (4–7). In these protocols it is suggested that an optimal tidal volume (TV) is 4 to 6 ml or 6 to 8 ml, since this range is considered safe due to the lower incidence of atelectasis, barotrauma and mortality (8, 9). However, there is a lack of research regarding optimal ventilator settings in people with acute CSCI.
Currently guidelines on acute spinal cord injury recommend high tidal volume (HTV) up to of >15 ml/kg predicted body weight (10). Peterson et al. (4) carried an investigation in patients with CSCI connected to MV and observed that patients managed with high tidal volumes had a lower frequency of ventilator-associated pneumonia (VAP), shorter duration of weaning time, and lower incidence of atelectasis compared to a low tidal volume group (LTV) (4). Other studies performed in CSCI populations reported that HTV management was not associated with major complications, suggesting that it is safe to use (5, 7, 11–13).
In CSCI patients with HTV exposure, the maximum values of airway pressure with higher volumes than the standard do not usually exceed 30 cm H2O due to the flaccidity of muscle tone in these patients, representing a potential benefit (14, 15). On the contrary, LTV fail to compensate for profound muscle weakness, and is associated with an increased need for sedation, mucosal obstruction, decreased surfactant production and increased incidence of atelectasis (16–21). It has even been reported that in quadriplegic patients a lower TV translates into greater dyspnea (11).
Due to the lack of consensus and a high level evidence on adequate ventilatory support settings in the CSCI population, we performed a systematic review and meta-analysis to revisit the recommendations that are being widely followed and provide data that will support decision making in regards to the respiratory support.
2 Materials and methods
2.1 Search strategy
Our systematic review was performed following the guidelines outlined in the Cochrane Handbook for Systematic Reviews (22), PRISMA (23), and AMSTAR 2 (24). The protocol was preregistered in PROSPERO (CRD42023452844). Thorough searches were conducted across multiple databases, including MEDLINE (PubMed), Scopus, EMBASE, Web of Science, Science Direct and the Cochrane Library. Database screening involved the application of thesaurus (MeSH, Emtree, etc.), free terms, and their synonyms. Using boolean operators, we implemented our PECO/PICO strategy (Population: adult patients with cervical spinal cord injury in mechanical ventilation; Exposure: ventilation with high tidal volume; Comparator: ventilation with normal tidal volume; Outcome: ventilator-associated pneumonia OR intrahospital mortality OR total weaning days OR other pulmonary complications). Keywords included terms related to exposure, such as “cervical spinal cord injury” OR “cervical spinal cord trauma” OR “tidal volume,” and outcome-related terms, such as “ventilator-associated pneumonia” OR “pulmonary complications.” The detailed search strategy is available in the (Supplementary Table 1A).
All the articles identified through primary and secondary screenings were compiled using Zotero® 6.0.15. Following the duplicate removal, the documents were stored in the Rayyan® tool, where two authors (EDMR and MCCC) conducted individual screenings of titles and abstracts independently (blinded). The selection of studies was achieved through consensus, and in instances of disagreement, a third researcher served as the arbitrator (GAVT). The chosen papers underwent a second full-text review to assess eligibility. A secondary manual search of reference lists and citing articles of included publications were also reviewed to increase the identification of relevant studies. The selection process is explained in detail in Figure 1.
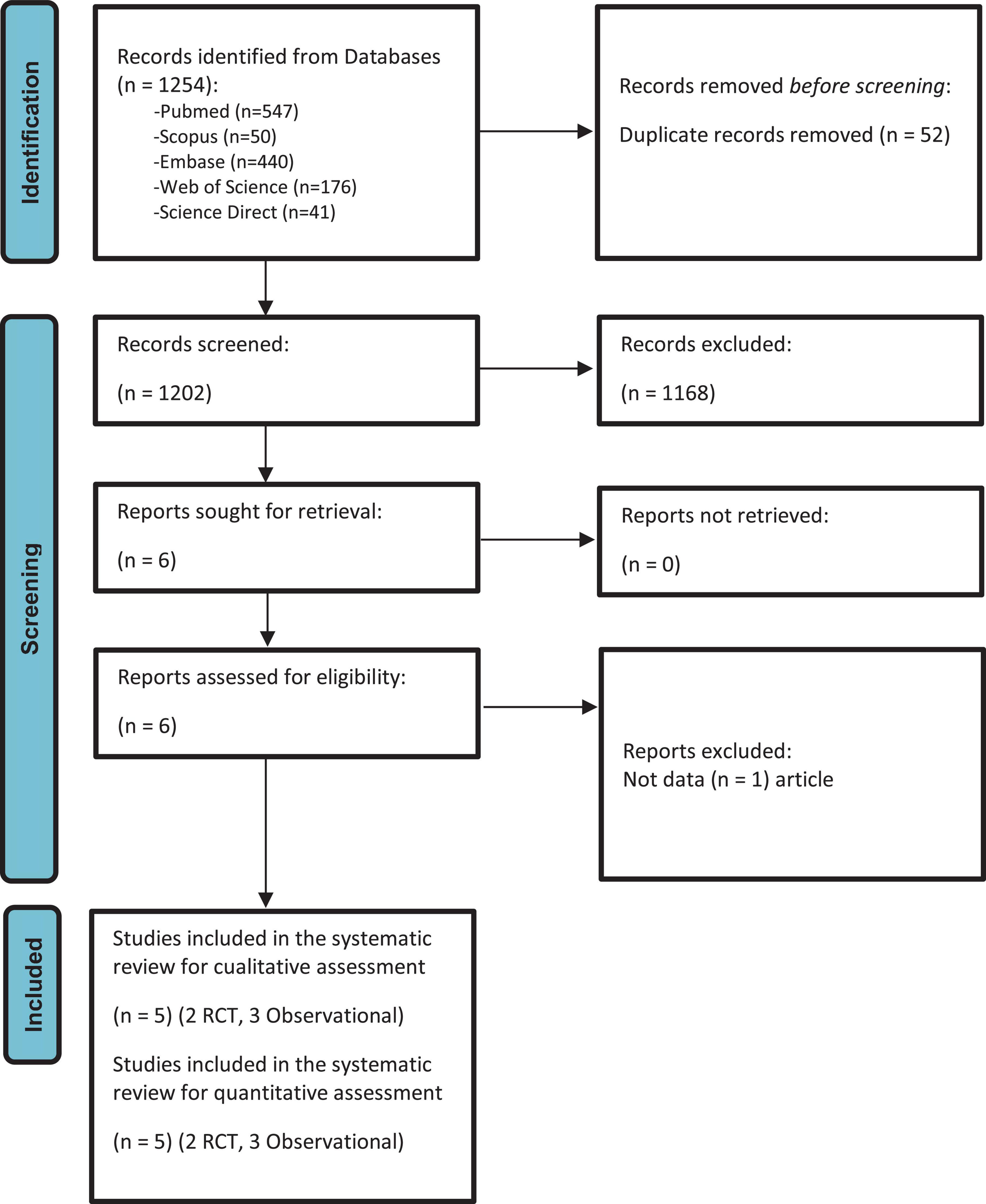
Figure 1. PRISMA 2020 flow diagram of the selection process of the primary studies included.
2.2 Selection criteria
We included observational studies (RCS) and randomized controlled trials (RCTs) that included adult patients (≥18) diagnosed with CSCI in need of MV assistance for more than 2 weeks and less than 6 months, with cervical lesions classified as AIS A, B, or C and initiated without pre-existing pulmonary pathology. We included articles published up until August 30, 2023, with no restrictions on date or language. Case reports, case series, and duplicated publications were excluded.
2.3 Outcomes
The primary outcome the frequency of VAP, defined as the occurrence or progression of new pulmonary infiltrates with at least two of three signs: temperature >38 or <36, leukocytosis or leukopenia, or left deviation of immature forms (10%), along with tracheobronchial purulent discharge (11, 12). Secondary outcomes included the presence of acute respiratory distress syndrome (ARDS), atelectasis, and composite mortality (VAP and overall mortality).
2.4 Data extraction
Two independent researchers, blindly, gathered and extracted relevant details of each included study using and standardized spreadsheet, including authors names, country and year of publication, clinical and epidemiological characteristics of the population, number of participants and cases, measures of association, confounding factors, and the outcomes. For dichotomous and time-to-event variables, we compiled odds ratios (OR), risk ratios (RR) and hazard ratios (HR) with 95% confidence intervals (CI 95%). Missing data were reported when appropriate.
2.5 Statistical analysis
We used the Mantel-Haenszel method in the meta-analysis to pool adjusted ORs with 95% CIs. All studies reported pooled ORs, none RRs. We conducted this meta-analysis using R® 4.2.226 software. To summarize the quantitative synthesis, we used forest plots with the library meta, function metabin, and Mantel-Haenszel method with Restricted Maximum Likelihood (REML) for tau (2). Our protocol stated that we would examine heterogeneity among studies with Cochran’s Q-test and Higgins I2 statistic. If heterogeneity was not statistically significant (p > 0.10, I2 statistics <40%), we would use a fixed effects model. On the other hand, we would use a random effects model if heterogeneity was statistically significant (22). We conducted sensitivity a using the function InfluenceAnalysis. Subgroup analysis could not be performed due to the small number of patients in the studies collected.
2.6 Quality assessment
We assessed the potential risk of bias using both the Risk Of Bias In Non-randomized Studies–of Exposure (ROBINS-E) (25) and the Cochrane risk-of-bias tool for randomized trials (RoB 2) (26). To examine the possibility of publication bias, we employed a funnel plot and Egger’s test calculation (27).
Two researchers (EDMR and MCCC) assessed the certainty of the evidence (CoE) of the study outcomes for each outcome based on the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) criteria (28, 29). Any discrepancies between the reviewers were resolved through discussion with the leading researcher (GAVT).
3 Results
3.1 Search results and study characteristics
Six records were included (4, 5, 7, 11, 12, 30) in the qualitative synthesis in our review (Table 1). Afterward, five articles remained for the meta-analysis (Supplementary Table 1B), three observational studies (4, 7, 10) and two RCTs (11, 12) (Figure 1); with a total of 396 MV patients enrolled, 119 patients with HTV, and 277 with LTV. Among the studies included for qualitative analysis, five were conducted in the USA (4, 5, 7, 11, 30) and one in India (12).
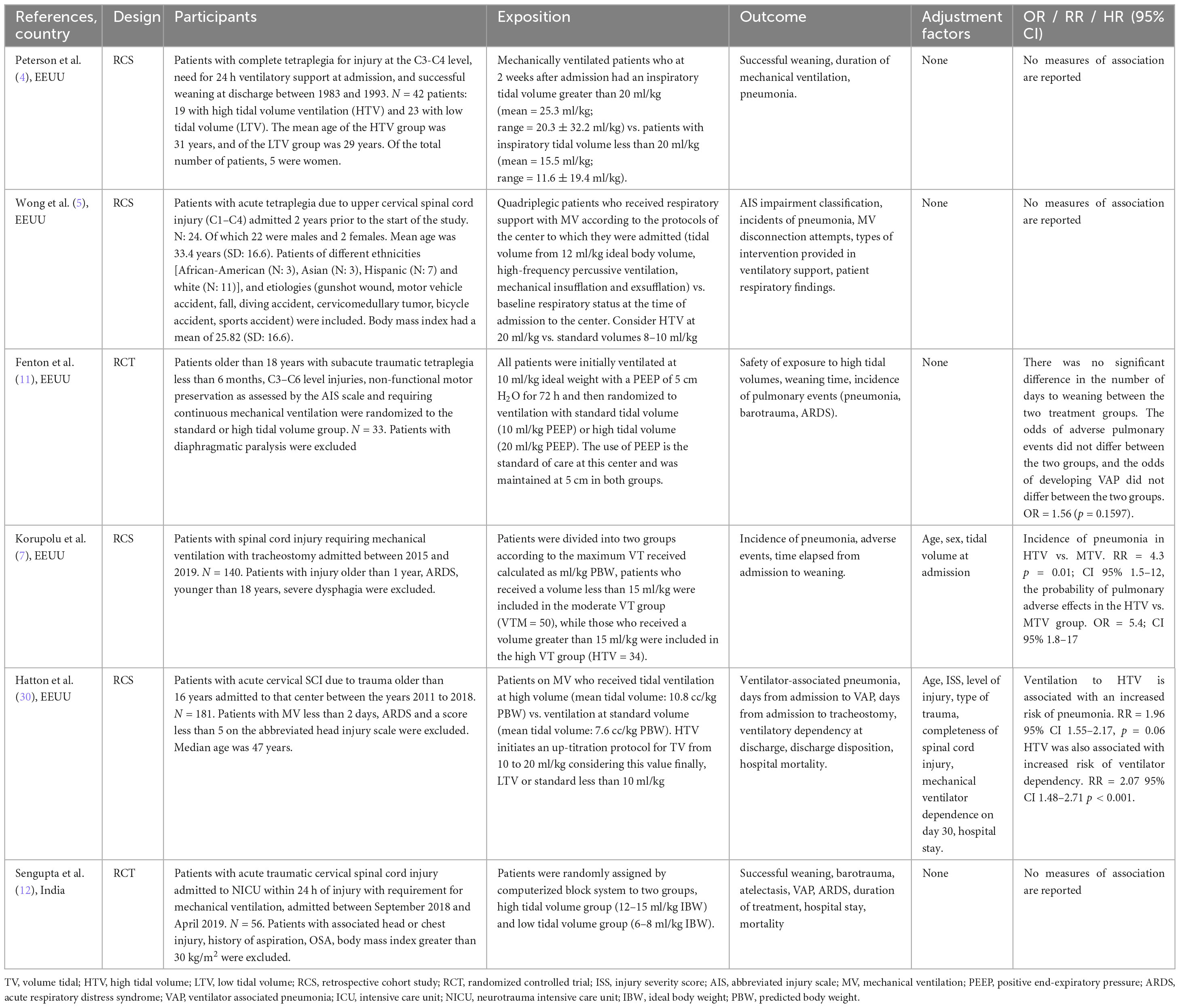
Table 1. General characteristics of included studies.
In this investigation, the authors use different definitions about TV, but in general, HTV are considered to be values greater than 15 ml/kg. For example, Peterson: HTV 20 ml/kg, LTV median of 15 ml/kg; Wong: HTV 20 ml/kg, LTV 8–10 ml/kg; Fenton: HTV 20 ml/kg LTV 10 ml/kg; Korupolu: HTV greater than 15 ml/kg LTV less than 15 ml/kg; Hatton: HTV initiates an up-titration protocol for TV from 10 to 20 ml/kg considering this value finally, LTV or standard less than 10 ml/kg; Sengupta HTV up to 15 ml/kg LVT 6–8 ml/kg).
Therefore, TV over 15 ml/kg are considered HTV, and volumes less than this are considered standard or LTV since the controls usually have less than 10 ml/kg except for Peterson (4, 5, 7, 11, 12, 30). The primary outcome across all studies was the presence of VAP, defined as the occurrence or progression of new pulmonary infiltrates with at least two of three signs: temperature >38 or <36, leukocytosis or leukopenia, or left deviation of immature forms (10%), along with tracheobronchial purulent discharge (11, 12). The HTV group developed fewer than 50 cases of VAP, while the LTV group had 130 cases.
Additional demographic characteristics of the study population are documented in Table 1.
3.2 Risk of bias in studies
Among the five studies included in our meta-analysis, two were RCTs assesed as “some concerns” risk of bias (11, 12), attributable to the absence of blinding, but no other transgressions were identified in other stages of the study protocol. In contrast, two RCS studies were assesed as “some concerns” risk of bias (7, 30) and one “high” risk of bias (4) (Table 2).
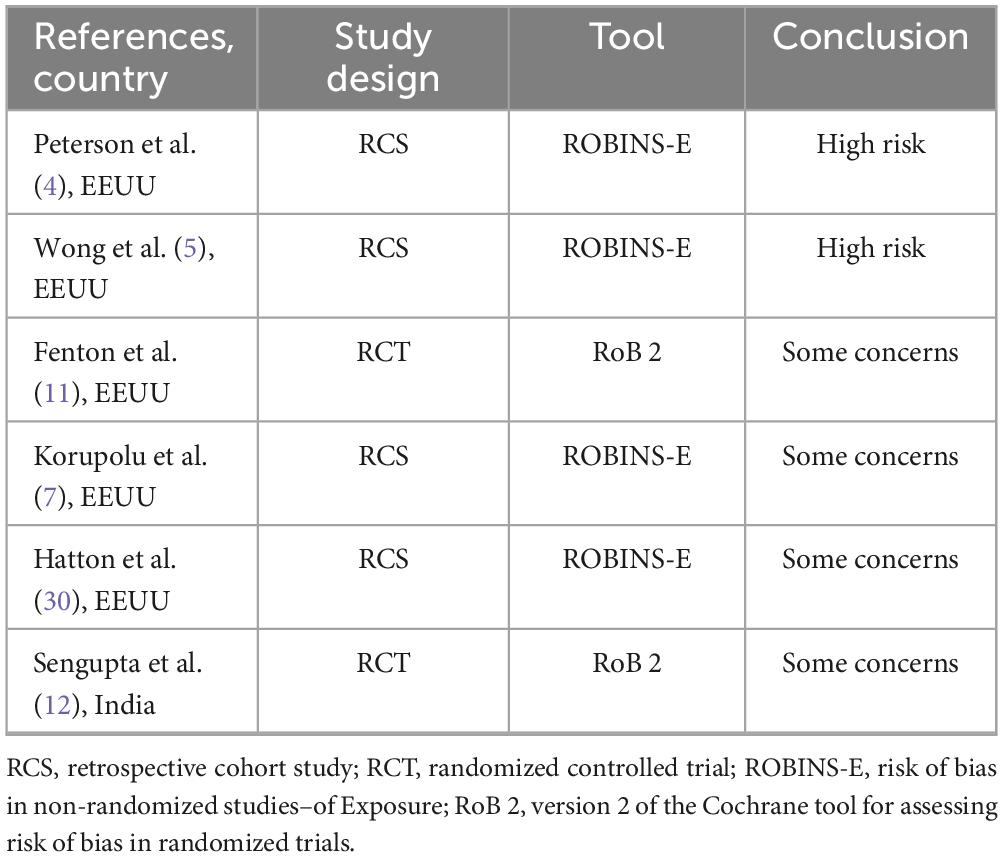
Table 2. Risk of bias of the included studies.
3.3 Risk of VAP
We conducted an initial meta-analysis including five studies (two RCTs and three observational studies). The analysis revealed that among 119 patients subjected to HTV, 50 exhibited VAP, whereas among 277 patients receiving LTV, 130 developed VAP. The meta-analysis indicated an absence of a significant relationship between the presence of VAP and HTV used (OR 0.78; 95% CI 0.20 to 3.02; p > 0.05), with an unacceptably high heterogeneity (I2: 63%) (Figure 2A).
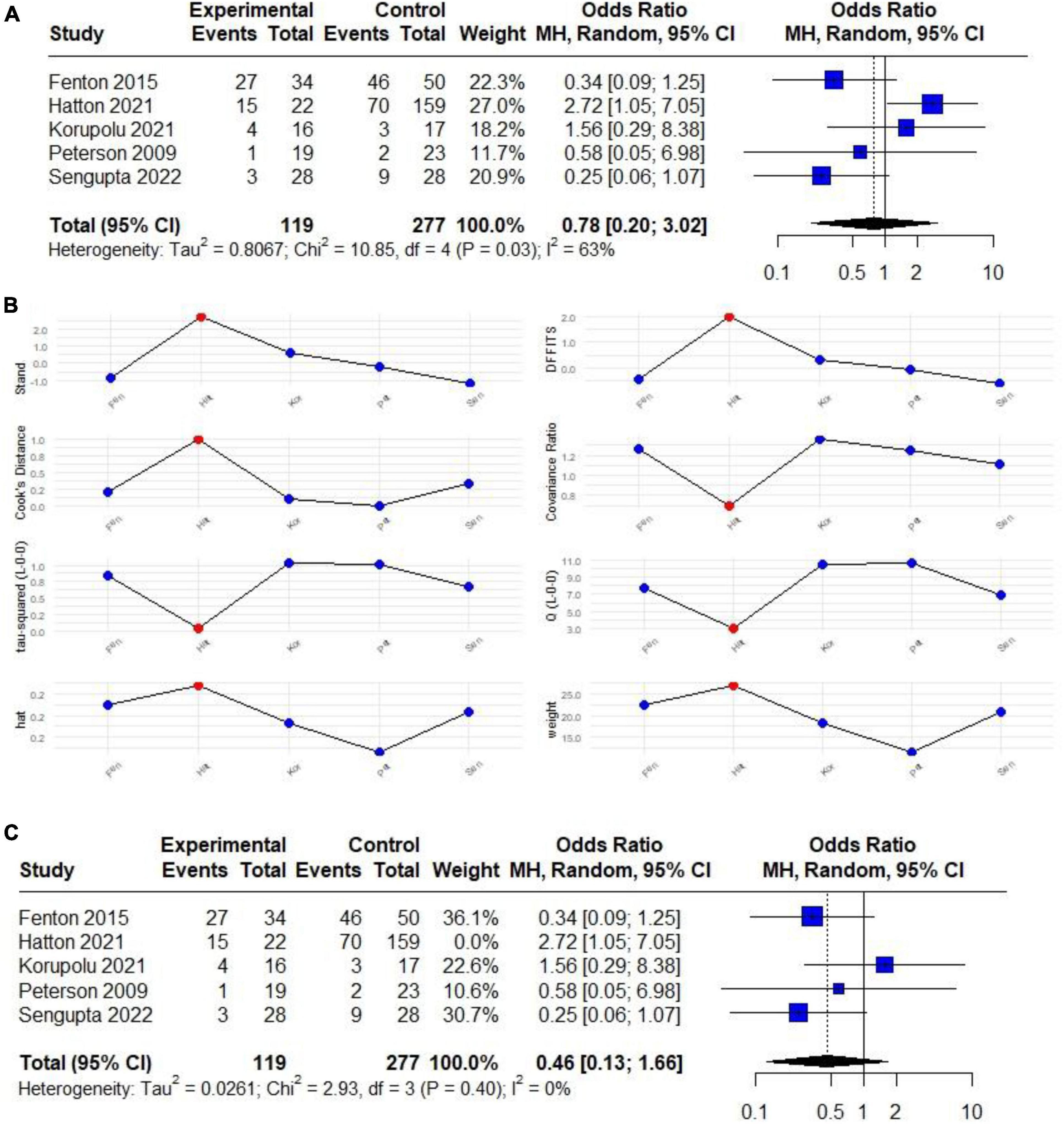
Figure 2. (A) Forest plot of the effect of HTV compared with LTV on the risk of developing VAP in patients with CSCI (RCTs and observational) studies. (B) Plot of the influence analysis considering (RCTs and observational) studies included in the initial meta-analysis to determine a high heterogeneity, revealing that Hatton behaves like an outlier study. (C) Forest plot of the effect of HTV compared with LTV on the risk of developing VAP in patients with CSCI without outlier study.
Due to the limited number of studies, subgroup analysis could not be performed. However, a sensitivity analysis through Influence Analysis revealed that excluding Hatton et al. (30), who behaved as an outlier (Figure 2B), the overall results showed a trend indicating that ventilation with HTV may provide protection against VAP (OR 0.46; 95% CI 0.13 to 1.66; p > 0.05) with no heterogeneity (I2: 0%) (Figure 2C).
3.4 Risk of VAP and mortality
Only three studies assessed a composite outcome (VAP and mortality) (7, 12, 30). There was no significant difference in VAP and mortality rates among patients ventilated with both HTV and LTV (OR 1.04; 95% CI 0.04–29.27) with unacceptable high heterogeneity (I2: 84%) (Figure 3A). Upon further investigation of heterogeneity using Influence Analysis, it was identified that Korupolu et al. (7) acted as a significant outlier (Figure 3B). Upon excluding this, the analysis demonstrated that ventilation with HTV emerged as a protective factor for the composite outcome under consideration (OR 0.48; 95% CI 0.30 to 0.79; p < 0.05) with no heterogeneity (I2: 0%) (Figure 3C).
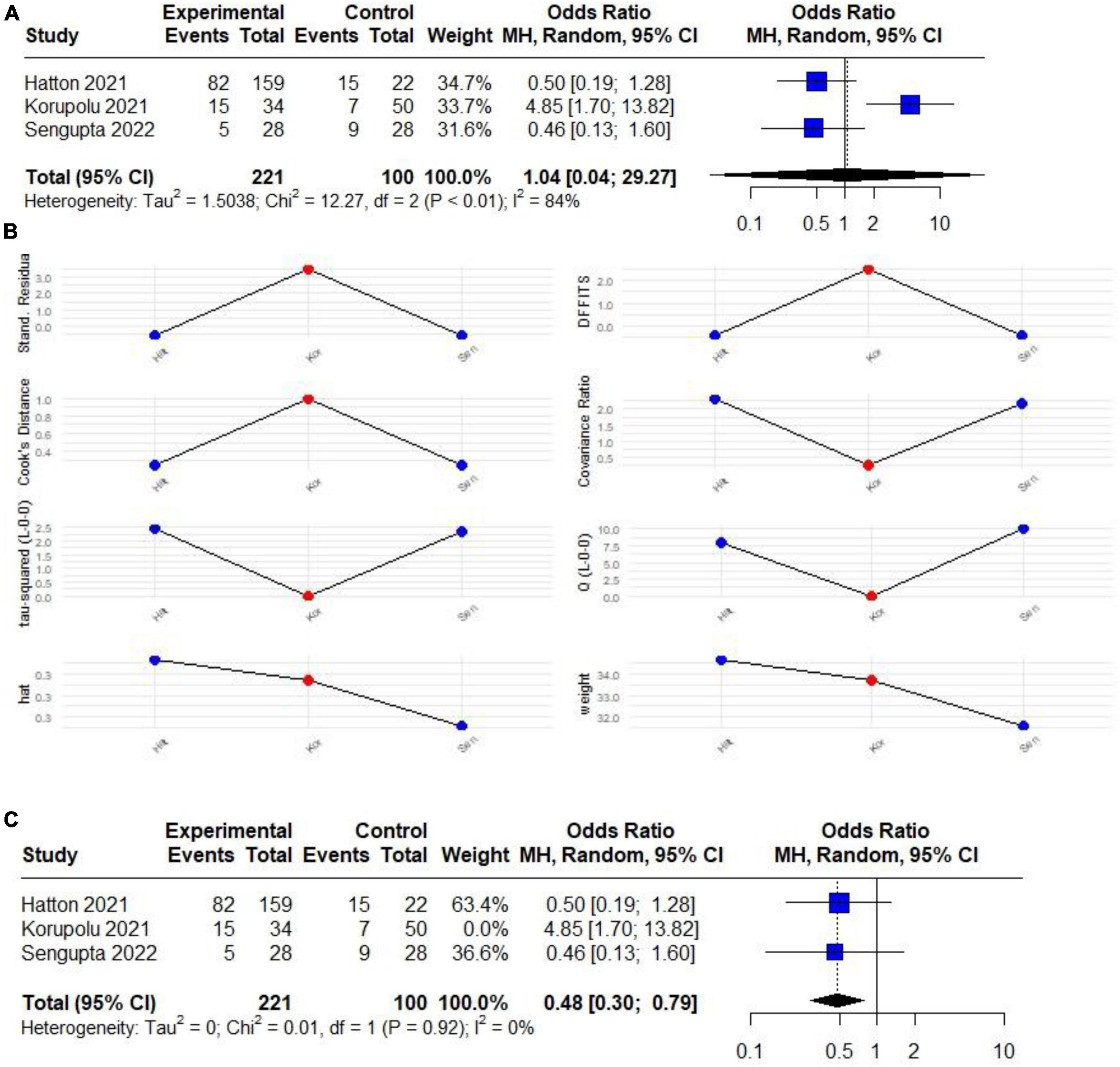
Figure 3. (A) Forest plot of the effect of HTV compared with LTV on the risk of developing a composite outcome (VAP and mortality) in patients with CSCI (RCTs and observational) studies. (B) Plot of the influence analysis considering (RCTs and observational) studies included in the initial meta-analysis to determine a high heterogeneity, revealing that Korupolu behaves like an outlier study. (C) Forest plot of the effect of HTV compared with LTV on the risk of developing a composite outcome (VAP and mortality) in patients with CSCI without outlier study.
3.5 Risk of other pulmonary complications
When analyzing potential complications associated with HTV, in terms of atelectasis, there is no heightened occurrence in the HTV compared to the LTV group (OR 0.45; 95% CI 0.02 to 9.28; p > 0.05), with no heterogeneity detected (I2: 0%). Similarly, the incidence of complications after tracheostomy did not differ between the HTV and LTV groups (OR 0.45; 95% CI 0.00 to 165.22; p > 0.05) without heterogeneity (I2: 0%). The most recent study by Sengupta et al. (12) exclusively provides data on ARDS showing no significant difference between the HTV and LTV ventilation groups (OR 0.30; 95% CI 0.08 to 1.11; p > 0.05).
It was not feasible to conduct a meta-analysis for other crucial outcomes, as these data were presented solely in a single study, including parameters such as the time of weaning onset and isolated mortality (Figure 4).
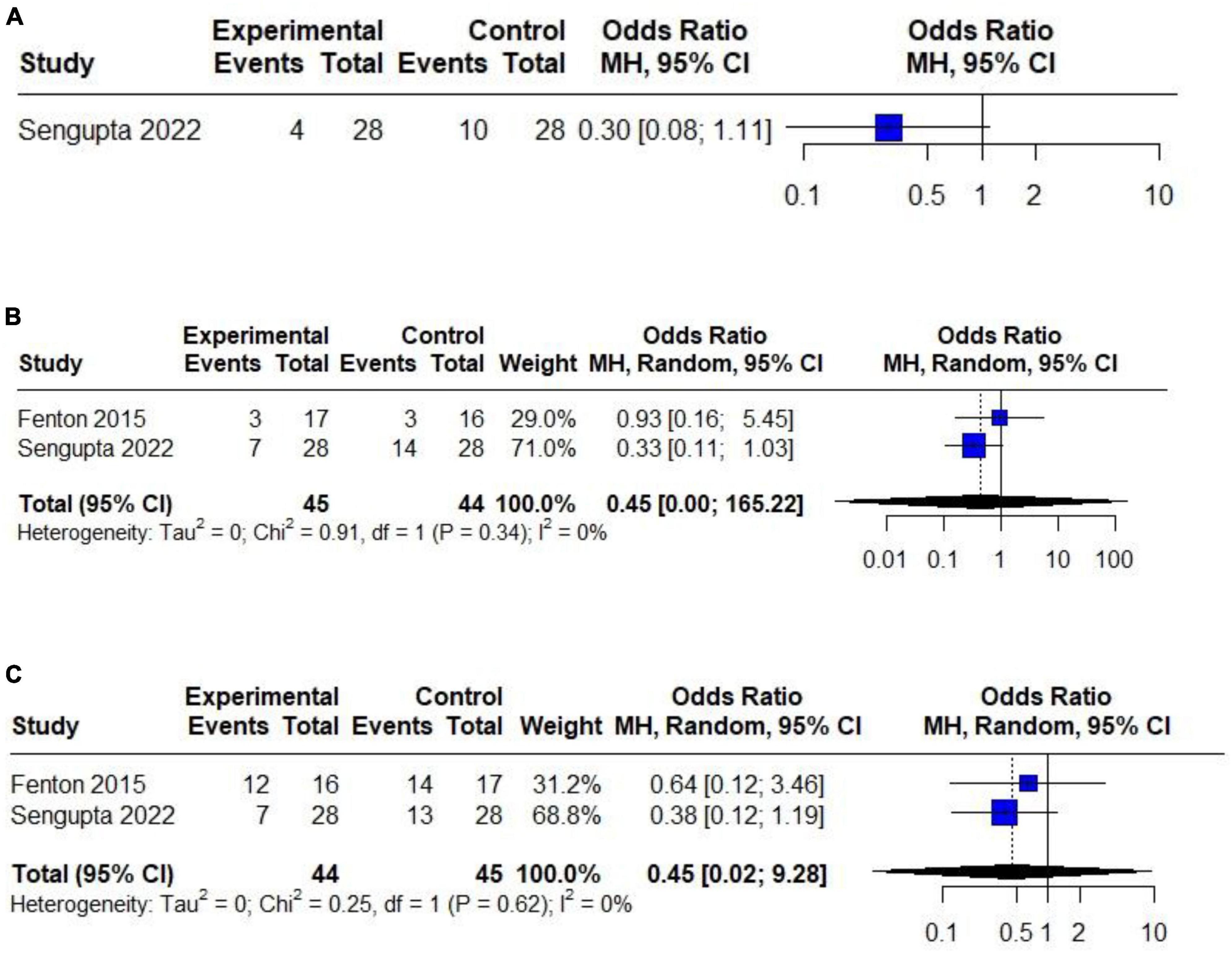
Figure 4. Forest plot of the effect of HTV compared with LTV in patients with CSCI on the risk of developing: (A) ARDS (only one RCT). (B) Atelectasis (only two RCTs). (C) complications after tracheostomy (only two RCTs).
3.6 GRADE assessment
We used GRADE to assess the certainty of evidence (CoE) for the presence of VAP in five studies that involved 396 patients. Despite the small number of studies, we found no evidence of publication bias [Egger’s test (27): 1.79; 95% CI −3.14 to 6.72; p > 0.1] (Figure 5). Table 3 shows that the percentage of VAP in the HTV group was lower (−6.1%, 95% CI −27.7 to 20), but this difference was not statistically significant with a low certainty of evidence.
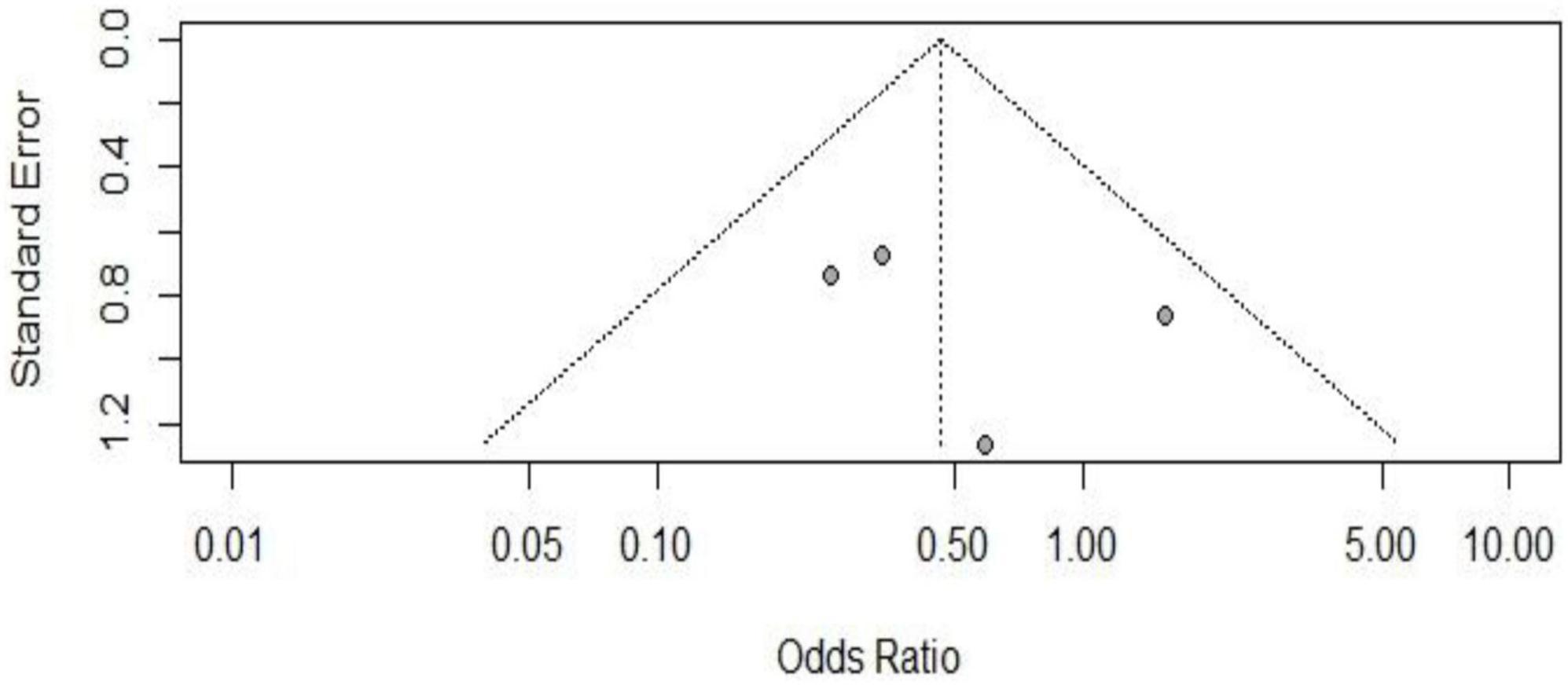
Figure 5. Funnel plot of the included studies in the meta-analysis on the effect of developing VAP in patients with CSCI considering observational and RCTs studies without outlier.
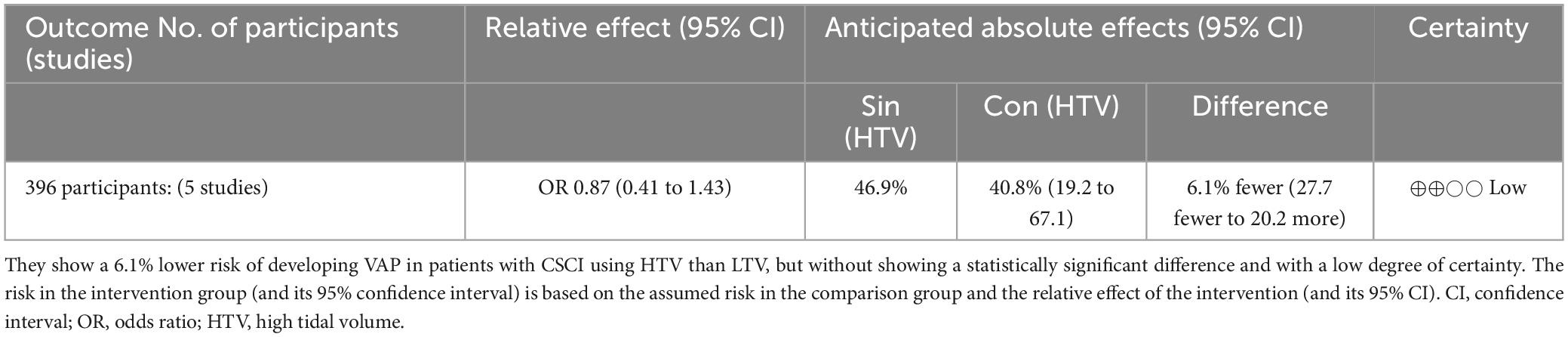
Table 3. Certainty of the evidence (CoE) through GRADE.
4 Discussion
This is the first systematic review and meta-analysis that investigates the effect of MV with HTV compared to LTV in patients with CSCI and its association with pulmonary complications and other undesirable respiratory outcomes. We found that there is no significant difference in the presence of VAP as the main outcome in patients with CSCI on MV if HTV vs. LTV is used (OR 0.48; 95% CI 0.30 to 0.79; p < 0.05; I2: 0%). In turn, there is no significant difference regarding the frequency of pulmonary complications such as ARDS, atelectasis, complications after TQT or delays on initiation of weaning in the HTV group compared to those in the LTV group. However, due to the very limited number of primary studies, the results are inconclusive and should be interpreted with caution.
The main complication in patients with CSCI is VAP, which causes significant morbidity and mortality. Therefore, it is necessary to prevent it and start the weaning the patient with CSCI from the MV as soon as possible; only then can the quality of life be improved and healthcare costs reduced (31–34). Poor lung expansion and secretion clearance lead to the development of pneumonia (35). Therefore, the concept of using HTV in patients with CSCI lies in the fact that the ventilatory pathophysiology in patients with CSCI is different from that in a critically ill patient with lung injury, given that there is less compliance of the respiratory system, composed of the thoracic cage and lung parenchyma. Additionally, the absence of adequate use of abdominal muscles makes achieving adequate TV for these patients more challenging (16, 35, 36). It is reasonable to think that using HTV would lead to controlled overdistension, inducing more outstanding production of surfactant in type II pneumocytes and the alveoli and, therefore, prevent complications such as VAP and atelectasis, among other pulmonary complications (11, 12, 35). Something similar is based on the fact that Gattinoni and Pesenti’s concept of “baby lung” does not intuitively apply to the generally healthy lungs of patients with CSCI. Tetraplegic patients often experience air hunger when LVT ventilation is used, even with normal PaCO2, and there is evidence that HTV ventilation may improve weaning success from MV (37, 38).
There are only two RCTs published to date that evaluate MV-dependent CSCI patients and outcomes associated with pulmonary complications (11, 12). Sengupta et al. (12) carried out an RCT, the most currently published, in patients with CSCI where they evaluated the use of HTV compared to LTV and its effect on outcomes such as days to achieve MV release, VAP, atelectasis, and ARDS, enrolling a total of 28 patients for each study group (experimental and control). They found that although there is a higher frequency of VAP in the LTV group compared to HTV (32.14 vs. 10.71%, p: 0.05), there is no statistical significance. The author, when evaluating the role of using HTV with respect to the presence of ARDS, length of hospital stay, and use of vasopressor support, did not find significant differences concerning the LTV group. Only 4 (14%) patients with ARDS were in the HTV group compared to 10 patients (36%) in the LTV group. However, without statistical significance (p = 0.14), although there is no data on the PEEP values used in the ARDS groups, higher peak pressure values are shown in HTV vs. LTV (29 vs. 19 mmHg, p < 0.01), probably attributed to HTV and PEEP but without more significant evidence of injuries due to barotrauma (pneumothorax, VILI, among others). This demonstrates that the use of HTV is safe. This study is one of the few that assesses mortality as an isolated outcome, where no difference is evident, considering more deaths in the LTV group (9 patients, 37%) compared to the HTV group (5 patients, 18%), but without statistical significance (p = 0.22).
On the other hand, Fenton et al. (11) conducted an RCT with 35 tracheotomized patients with CSCI (at level C3-C6) MV dependant, using high TV (HTV, experimental group) at values of up to 20 ml/kg per PBW compared to the control group with 10 ml/kg by PBW of TV (LTV, control group). They found no significant difference in the frequency of VAP in both groups (OR 1.56; p > 0.05). Of the total of 7 VAPs found, four were from the LTV group, and three were from the HTV group. They also did not find a significant difference in the presence of ARDS or other complications resulting from barotrauma, concluding that it may be safe to use HTV in patients with CSCI based on those above and on the quantification of forced vital capacity (FVC) of both groups of 1231 ml (HTV group) and 1122 (LTV group), with no significant difference (p > 0.05). These findings suggest that using HTV is not harmful and should be evaluated in RCTs with larger population.
In contrast to the two RCTs mentioned, a RCS carried out by Korupolu et al. (7) evaluated the use of HTV as a risk factor for VAP, incorporating 84 patients with CSCI tracheostomized on MV, making up the HTV group with 34 patients and 50 patients in the LTV group. They found that there is a greater risk of VAP with the use of HTV (RR 4.3; 95% CI 1.5 to 1.2; p: 0.01), and although in the general characteristics of the patients, the HTV group has a TV (ml) of 875 vs. 750 in the LTV group, and in the same way the peak pressure (mmHg) 21 vs. 19, respectively; they conclude in the multivariate analysis that the increase of 1 ml in the TV is associated with a lower risk of VAP (RR 1.28; 95% CI 1.1 to 1.6; p: 0.02), including mortality when analyzed as a composite outcome (VAP plus mortality) (OR 1.4; 95% CI 1.1 to 1.8; p: 0.01). It is striking in this study by Korupolu et al. (7) that, on the contrary, in its general characteristics, the group of patients who have HTV has a lower TV compared to the group of patients with LTV. In addition, this study does not carry out sample selection through a probabilistic method, the confounding variables are not necessarily the most appropriate, and the HTV group was considerably older compared to the LTV group. Therefore, the conclusions mentioned above must be interpreted with caution.
The postulated mechanism by which HTV should lead to a lower rate of VAP and other pulmonary complications has yet to be fully understood. However, it is rationally and physiopathological based on the concept that using restrictive TV (LTV or standard, as per our investigation) at 6–8 ml/kg is based on protective lung principles supported by the Acute Respiratory Distress Syndrome (ARDS) Network (13). It is necessary to understand that the evidence supporting lower mortality with low tidal volumes proceed from patients with specific lung pathologies. In contrast, patients with an initial CSCI typically have healthy lungs, suggesting they benefit from using HTV for the aforementioned physiopathological reasons (4, 16, 36).
In addition to the complication due to VAP in patients with CSCI, the presence of atelectasis is a non-negligible situation. The two RCTs that assess this complication found no differences between the presence of atelectasis and the use of tidal volume in HTC or LTV. Fenton et al. (11) report 100% compliance in both groups. Sengupta et al. (12), on the other hand, found a more significant number of atelectasis in the LTV group compared to HTV in 18 patients (64%) compared to 13 patients (46%), respectively, suggesting, again, that the use of HTV can help reduce complications such as atelectasis without entailing problems associated with volutrauma or barotrauma in VM. The same authors also do not report differences in the rate of complications when performing tracheostomy in these groups of patients.
Although there are no significant differences in mortality, in our meta-analysis, when evaluating as a composite outcome (VAP and mortality), excluding Korupolu et al. (7) for behaving as an outlier, we found a reduction in the rate of VAP and mortality in the HTV use group up to 52% less (RR: 0.48; 95% CI 0.30 to 0.79; I2: 0%) but larger RCT-type studies are needed to demonstrate what is stated in this research.
Our study has numerous strengths. Firstly, we carried out a comprehensive search strategy, which covered six essential databases and clinical trial registers. Secondly, we utilized a rigorous methodology to conduct our review and meta-analysis, which included a thorough quality assessment of studies and a statistical analysis that accounted for heterogeneity. Thirdly, as there was no statistical heterogeneity, it suggests that our findings are dependable and robust. Moreover, the results of individual studies are consistent.
It is important to note that our study has some limitations. First, only a few completed studies have explicitly addressed our PECO/PICO question. Second, the studies included in our meta-analysis were a mix of observational (three) and RCTs (two), with observational studies being more prone to bias than RCTs. Third, while most of the studies used HTV values over 15 ml/K PWB (4, 7, 11, 12, 30), one study used similar but different management points (5). Finally, due to the limited number of studies available, we had to analyze both observational and RCTs, considering the moderate risk of bias found in the reported observational studies.
5 Conclusion
Our study suggests that there is no significant difference in the development of VAP as a complication when using HTV compared to LTV in patients with CSCI in MV, nor are there differences in the presentation of other pulmonary complications such as ARDS, atelectasis, and onset of MV weaning. There is also no evidence that there are more complications associated with volutrauma in the HTV group, indicating that this strategy could be safe. In the composite outcome, when evaluating both VAP and mortality, the results suggest a lower rate of VAP and mortality by up to 52% after excluding outliers. The conclusions above have a low level of evidence. RCTs are necessary to demonstrate the effectiveness of using HTV in patients with CSCI or to rule it out definitively and to be able to couple this evidence into management guidelines.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Author contributions
EM-R: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Project administration, Software, Supervision, Writing – original draft. GV-T: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Project administration, Software, Supervision, Writing – original draft, Methodology, Resources, Validation, Validation, Writing – review and editing. CQ-C: Data curation, Formal Analysis, Methodology, Resources, Visualization, Writing – original draft. MC: Funding acquisition, Investigation, Project administration, Resources, Software, Validation, Visualization, Writing – original draft. JC-C: Formal Analysis, Funding acquisition, Investigation, Methodology, Resources, Writing – review and editing. JP-P: Conceptualization, Writing – original draft.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2024.1362318/full#supplementary-material
References
1. Jackson A, Groomes T. Incidence of respiratory complications following spinal cord injury. Arch Phys Med Rehabil. (1994) 75:270–5. doi: 10.1016/0003-9993(94)90027-2
2. Harrop J, Sharan A, Scheid E, Vaccaro A, Przybylski G. Tracheostomy placement in patients with complete cervical spinal cord injuries: American spinal injury association grade A. J Neurosurg. (2004) 100:20–3. doi: 10.3171/spi.2004.100.1.0020
3. Reines H, Harris R. Pulmonary complications of acute spinal cord injuries. Neurosurgery. (1987) 21:193–6. doi: 10.1227/00006123-198708000-00010
4. Peterson W, Barbalata L, Brooks C, Gerhart K, Mellick D, Whiteneck G. The effect of tidal volumes on the time to wean persons with high tetraplegia from ventilators. Spinal Cord. (1999) 37:284–8. doi: 10.1038/sj.sc.3100818
5. Wong S, Shem K, Crew J. Specialized respiratory management for acute cervical spinal cord injury: A retrospective analysis. Top Spinal Cord Inj Rehabil. (2012) 18:283–90. doi: 10.1310/sci1804-283
6. Kumar A, Khandelwal A, Jamil S. Ventilatory strategies in traumatic cervical spinal cord injury: Controversies and current updates. Asian Spine J. (2023) 17:615–9. doi: 10.31616/asj.2023.0094
7. Korupolu R, Stampas A, Uhlig-Reche H, Ciammaichella E, Mollett P, Achilike E, et al. Comparing outcomes of mechanical ventilation with high vs. moderate tidal volumes in tracheostomized patients with spinal cord injury in acute inpatient rehabilitation setting: A retrospective cohort study. Spinal Cord. (2021) 59:618–25. doi: 10.1038/s41393-020-0517-4
8. Brower R, Matthay M, Morris A, Schoenfeld D, Thompson B, Wheeler A. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med. (2000) 342:1301–8. doi: 10.1056/NEJM200005043421801
9. Fan E, Del Sorbo L, Goligher E, Hodgson C, Munshi L, Walkey A, et al. An official American thoracic society/European society of intensive care medicine/society of critical care medicine clinical practice guideline: Mechanical ventilation in adult patients with acute respiratory distress syndrome. Am J Respir Crit Care Med. (2017) 195:1253–63. doi: 10.1164/RCCM.201703-0548ST
10. Cosortium for Spinal Cord Medicine. Respiratory management following spinal cord injury: A clinical practice guideline for health-care professionals. J Spinal Cord Med. (2005) 28:259–93. doi: 10.1080/10790268.2005.11753821
11. Fenton J, Warner M, Lammertse D, Charlifue S, Martinez L, Dannels-McClure A, et al. A comparison of high vs standard tidal volumes in ventilator weaning for individuals with sub-acute spinal cord injuries: A site-specific randomized clinical trial. Spinal Cord. (2016) 54:234–8. doi: 10.1038/sc.2015.145
12. Sengupta D, Bindra A, Kapoor I, Mathur P, Gupta D, Khan M. Comparison of different tidal volumes for ventilation in patients with an acute traumatic cervical spine injury. Neurol India. (2022) 70:S282–7. doi: 10.4103/0028-3886.360926
13. Thompson B, Bernard GRARDS. Network (NHLBI) studies – successes and challenges in ARDS clinical research. Crit Care Clin. (2011) 27:459–68. doi: 10.1016/j.ccc.2011.05.011
14. Winslow C, Bode R, Felton D, Chen D, Meyer P. Impact of respiratory complications on length of stay and hospital costs in acute cervical spine injury. Chest. (2002) 121:1548–54. doi: 10.1378/chest.121.5.1548
15. Winslow C, Rozovsky J. Effect of spinal cord injury on the respiratory system. Am J Phys Med Rehabil. (2003) 82:803–14. doi: 10.1097/01.PHM.0000078184.08835.01
16. Arora S, Flower O, Murray N, Lee B. Respiratory care of patients with cervical spinal cord injury: A review. Crit Care Resusc. (2012) 14:64–73.
17. Massaro G, Massaro D. Morphologic evidence that large inflations of the lung stimulate secretion of surfactant. Am Rev Respir Dis. (1983) 127:235–6. doi: 10.1164/ARRD.1983.127.2.235
19. Seymour C, Pandharipande P, Koestner T, Hudson L, Thompson J, Shintani A, et al. Diurnal sedative changes during intensive care: Impact on liberation from mechanical ventilation and delirium. Crit Care Med. (2012) 40:2788–96. doi: 10.1097/CCM.0B013E31825B8ADE
20. Kallet R, Campbell A, Dicker R, Katz J, Mackersie R. Effects of tidal volume on work of breathing during lung-protective ventilation in patients with acute lung injury and acute respiratory distress syndrome. Crit Care Med. (2006) 34:8–14. doi: 10.1097/01.CCM.0000194538.32158.AF
21. Brown R, DiMarco A, Hoit J, Garshick E. Respiratory dysfunction and management in spinal cord injury. Respir Care. (2006) 51:853–853. doi: 10.1007/978-981-19-0228-4_23
22. Cochrane Training.Cochrane handbook for systematic reviews of interventions. (2023). Available online at: https://training.cochrane.org/handbook/archive/v6.3 (accessed December 27, 2023).
23. Moher D, Liberati A, Tetzlaff J, Altman D, Prisma Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. (2009) 6:e1000097. doi: 10.1371/journal.pmed.1000097
24. Shea B, Reeves B, Wells G, Thuku M, Hamel C, Moran J, et al. AMSTAR 2: A critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. (2017) 358:j4008. doi: 10.1136/bmj.j4008
25. ROBINS-E_LAUNCH-VERSION.Risk of bias in non-randomized studies – of exposure (ROBINS-E). (2023). Available online at: https://drive.google.com/file/d/17xCWqLVi01PIjffqkC4yJYJnF7VyGNOn/view?usp=drive_link&usp=embed_facebook (accessed December 27, 2023).
26. Sterne J, Savoviæ J, Page M, Elbers R, Blencowe N, Boutron I, et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ. (2019) 366:l4898. doi: 10.1136/bmj.l4898
27. Lin L, Chu H. Quantifying publication bias in meta-analysis. Biometrics. (2018) 74:785–94. doi: 10.1111/biom.12817
28. Meader N, King K, Llewellyn A, King K, Llewellyn A, Norman G, et al. A checklist designed to aid consistency and reproducibility of GRADE assessments: Development and pilot validation. Syst Rev. (2014) 3:82. doi: 10.1186/2046-4053-3-82
29. Granholm A, Alhazzani W, Møller M. Use of the GRADE approach in systematic reviews and guidelines. Br J Anaesth. (2019) 123:554–9. doi: 10.1016/j.bja.2019.08.015
30. Hatton G, Mollett P, Du R, Wei S, Korupolu R, Wade C, et al. High tidal volume ventilation is associated with ventilator-associated pneumonia in acute cervical spinal cord injury. J Spinal Cord Med. (2021) 44:775–81. doi: 10.1080/10790268.2020.1722936
31. Lee S, Roh S, Jeon S, Park J, Kim K, Lee Y, et al. A prognostic factor for prolonged mechanical ventilator-dependent respiratory failure after cervical spinal cord injury: Maximal canal compromise on magnetic resonance imaging. J Korean Neurosurg Soc. (2021) 64:791–8. doi: 10.3340/JKNS.2020.0346
32. Lertudomphonwanit T, Wattanaapisit T, Chavasiri C, Chotivichit A. Risk factors relating to the need for mechanical ventilation in isolated cervical spinal cord injury patients. J Med Assoc Thai. (2014) 97(Suppl. 9):S10–5.
33. Montoto-Marqués A, Trillo-Dono N, Ferreiro-Velasco M, Salvador-de la Barrera S, Rodriguez-Sotillo A, Mourelo-Fariña M, et al. Risks factors of mechanical ventilation in acute traumatic cervical spinal cord injured patients. Spinal Cord. (2018) 56:206–11. doi: 10.1038/s41393-017-0005-7
34. Stocker R, Bürgi U. [Respiratory problems after injuries of the cervical spine]. Schweiz Med Wochenschr. (1998) 128:1462–6.
35. Hendershot K, O’Phelan K. Respiratory complications and weaning considerations for patients with spinal cord injuries: A narrative review. J Pers Med. (2023) 13:97. doi: 10.3390/jpm13010097
36. Galeiras Vázquez R, Rascado Sedes P, Mourelo Fariña M, Montoto Marqués A, Ferreiro Velasco M. Respiratory management in the patient with spinal cord injury. Biomed Res Int. (2013) 2013:168757. doi: 10.1155/2013/168757
37. Gattinoni L, Marini J, Pesenti A, Quintel M, Mancebo J, Brochard L. The “baby lung” became an adult. Intensive Care Med. (2016) 42:663–73. doi: 10.1007/s00134-015-4200-8
Keywords: cervical spinal cord injury, tidal volume, mechanical ventilation, ventilator associated pneumonia, systematic review, meta-analysis
Citation: Meregildo-Rodríguez ED, Vásquez-Tirado GA, Quispe-Castañeda CV, del Carmen Cuadra-Campos M, Contreras-Cabrera JM and Pinedo-Portilla JL (2024) High vs. low tidal volume and pulmonary complications in patients with cervical spinal cord injury on mechanical ventilation: systematic review. Front. Med. 11:1362318. doi: 10.3389/fmed.2024.1362318
Received: 28 December 2023; Accepted: 19 February 2024;
Published: 01 March 2024.
Edited by:
Christian Waydhas, Department Trauma Surgery, GermanyReviewed by:
Oliver Cruciger, BG University Hospital Bergmannsheil GmbH, GermanyAhilanandan Dushianthan, University Hospital Southampton NHS Foundation Trust, United Kingdom
Copyright © 2024 Meregildo-Rodríguez, Vásquez-Tirado, Quispe-Castañeda, del Carmen Cuadra-Campos, Contreras-Cabrera and Pinedo-Portilla. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Gustavo Adolfo Vásquez-Tirado, Z2F2dDEzQGdtYWlsLmNvbQ==