 Beatriz Araújo
Beatriz Araújo Sandra F. Gomes
Sandra F. Gomes Laura Ribeiro
Laura Ribeiro
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Med. , 14 June 2024
Sec. Healthcare Professions Education
Volume 11 - 2024 | https://doi.org/10.3389/fmed.2024.1358444
This article is part of the Research Topic Research on Teaching Strategies and Skills in Different Educational Stages View all 32 articles
Introduction: The development of critical thinking (CT) has been a universal goal in higher education. A systematic review of the literature was conducted to evaluate the effectiveness of currently used pedagogical practices to foster CT/ clinical reasoning (CR)/ clinical judgment (CJ) skills and/or dispositions in undergraduate medical students.
Methods: PubMed, Web of Science and Scopus databases were searched from January 2010 to April 2021 with a predefined Boolean expression.
Results: Of the 3221 articles originally identified, 33 articles were included by using PICOS methodology. From these, 21 (64%) reported CR pedagogical practices and 12 (36%) CT pedagogical practices.
Discussion: Overall, pedagogical practices such as cognitive/visual representation, simulation, literature exposure, test-enhancing and team-based learning, clinical case discussion, error-based learning, game-based learning seem to enhance CT/CR skills and/or dispositions. Further research is required to identify the optimal timing, duration and modality of pedagogical interventions for effectively foster CT/CR in medical education.
Due to demographic and disease pattern changes along with patient’s needs and aspirations, healthcare professionals are required to develop new skills such as creativity (1), leadership, teamwork, empathy, and communication skills (2), in order to provide high-quality, safe, and effective patient care (3). Physicians must be prepared to deal with all types of environments and make decisions in situations of crisis and epidemics (4). Therefore, skills for managing people-centered care, managing complex tasks, and creating a positive work culture are needed (5). Being aware of the importance of the development of a set of skills beyond knowledge acquisition in 2017, the United Nations Education, Scientific and Cultural Organization (6) suggested the development of critical thinking (CT) as a learning outcome, which is defined as “the ability to question norms, practices, and opinions; to reflect on own[sic] one’s values, perceptions, and actions and to take a position in the sustainability discourse” (7). In fact, CT seems to be a key ingredient for commitment to lifelong learning (8) and a deep learning experience, allowing a better understanding and ability to deal with complex concepts and problems (9). It has been positively related to academic achievements (10) and better patients’ assessments, diagnoses, and care in the future (11). Critical thinkers seem to develop a more questioning mind, better critical appraisal abilities, and a positive attitude concerning evidence-based medicine (12). Thus, fostering students to develop CT has been a universal goal “to create better doctors” (13), a desirable outcome that should be developed in an early stage of their training, as skills develop through experience and practice (11, 14).
According to the American Philosophical Association, critical thinking encompasses a broad set of cognitive skills such as interpretation, analysis, evaluation, inference, explanation, self-regulation, and dispositions, including truth-seeking, open-mindedness, analyticity, systematicity, self-confidence, inquisitiveness, and maturity (15). Definitions of CT in medical education tend to emphasize logical or rational thinking—the ability to reason, analyze information, evaluate alternatives, assess arguments and evidence, and reach relevant and appropriate solutions to a problem (16). Moreover, in medicine, CT has also been described and identified nearly as synonymous with “clinical judgment” (CJ), “clinical reasoning” (CR), “diagnostic thinking,” “problem-solving,” or “type 2 thinking” terms involving a mental process used to think through problems and achieve a final decision (11).
Although CT can be taught, both pedagogical and assessment practices are challenging, and there is no consensus on the most effective teaching approach. In part, the instructional methods are challenging due to the different understanding of CT. For instance, Krupat et al. (17) found that 43% of doctors describe CT as a process, 41% as a skill or ability, and 16% as disposition. Therefore, teaching CT remains both a challenge and a necessity in medical education (9).
Our systematic review aims to investigate the effectiveness of the pedagogical practices that are currently used to foster the development of CT/CR/CJ skills and/or dispositions in undergraduate medical students. The specific objectives of this review are as follows: (1) to identify the pedagogical practices currently in use to promote the development of CT/CR/CJ skills and/or dispositions in undergraduate medical students; (2) to identify the tools that are being used to assess CT/CR/CJ skills and/or dispositions in the above conditions; and (3) to investigate the effectiveness of those pedagogical practices, considering the CT/CR/CJ skills and/or dispositions gains, the assessment tools, and the intervention context.
This study followed the Cochrane recommendations (18–22) and the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) Guidelines (23) (Supplementary material—PRISMA Checklist). The protocol for this systematic review is registered on Open Science Framework (OSF): doi: 10.17605/OSF.IO/8PJ26.
Although this systematic review was based on the approach used in a previous study (24), it explored the effectiveness of pedagogical practices used to foster CT/CR/CJ skills and dispositions exclusively in undergraduate medical students while also including other pedagogical outcomes.
In April 2021, the literature search was conducted in PubMed, Web of Science, and Scopus using the following Boolean expressions: (“Critical Thinking” OR “Clinical Reasoning” OR “Clinical Judgement”) AND (Skill OR Ability OR Disposition OR Attitude) AND (Strategies OR Interventions OR Educat* OR Teach* OR Practice OR Train OR Develop* Analyse* OR Test* OR Evaluate* OR Assess*) AND (Student* OR Undergraduate* OR School OR Faculty OR College OR High* Education OR Universities) AND (Medic*). The filters “Article title, Abstract, and Keywords” and “All fields” were used in Scopus, PubMed, and Web of Science databases. In addition, a time filter from January 2010 to April 2021 was set, and the studies were included according to the eligibility criteria.
Studies were deemed eligible according to the following inclusion and exclusion criteria defined using the PICOS tool (25):
• P (Population) — undergraduate medical students;
• I (Interventions) — pedagogical practices to foster the development of CT/CR/CJ skills and/or dispositions;
• C (Comparison) — not applicable;
• O (Outcomes) — CT/CR/CJ skills and/or dispositions gains;
• S (Study design) — Qualitative, quantitative, and mixed studies.
Articles published from January 2010 to April 2021, referring to CT/CR/CJ pedagogical practices as interventions and undergraduate medical students as its target population, were included. Furthermore, articles with a clear description of the pedagogical practices that were used to foster the development of CT/CR/CJ were also included. For this systematic review, studies with qualitative, quantitative, and mixed-method designs were considered.
Letters, short communications, systematic reviews, reviews, and meta-analysis were excluded. Studies lacking a clear methodological description of the intervention, articles outside the scope of undergraduate medical education or studies with no access to the full text despite the attempt to contact the authors, were also excluded during the screening phase. Although the search terms used were in English, no language restrictions were applied in our research strategy.
Studies were screened and selected by two independent reviewers. After duplicate records were removed, first, studies were screened based on the title and then based on the abstract. The remaining records were eligible for full paper reading based on the inclusion and exclusion criteria. Any disagreement was solved by consensus.
Data were collected, organized, and synthesized in tables based on the following: author(s), publication year, country, study design, objectives, sample, pedagogical approach (pedagogical practices, curricular context, subject specificity, regime, subject, length of the intervention, interventional and/or control group, format, instructional support, and feedback), assessment tools (pre-intervention and post-intervention), and main findings (Supplementary material — data collection).
The included studies underwent a quality assessment by two independent reviewers using the Standard Quality Assessment Criteria for Evaluating Primary Research Papers from a Variety of Fields (26). The studies received scores for their compliance (“yes” = 2, “partial” = 1; and “no” = 0), with each of the 10 criteria for qualitative studies, 14 criteria for quantitative studies, and both (24) criteria for mixed studies. For each study, a sum score was calculated by adding the scores for these criteria and dividing them by the total possible score (26).
To synthesize the information and enable comparison between pedagogical practices, some studies were characterized and grouped according to the characteristics of the pedagogical approach (i.e., cognitive/visual problem representation when a cognitive knowledge organization strategy was used such as mind map, conceptual mapping, illness script, or case vignettes; simulation when a low-fidelity or high-fidelity patient simulation was used; literature exposure when students were exposed and instructed to reflect based on books, literary excerpts, or papers).
Then, pedagogical practices were also divided into CT, CR, or CJ. In studies where multiple pedagogical practices were mentioned (e.g., debates during problem-based learning), only the most prominent studies focusing on the development of CT/CR/CJ skills and/or dispositions were considered to characterize the intervention except for the innovative curriculums that purposefully combine different pedagogical practices.
The curricular context of the pedagogical approach was categorized as curricular (when the CT/CR/CJ pedagogical practices are implemented during the formal curriculum within the context of a specific year and subject content as part of the objectives of a given curricular unit) or extracurricular (when the CT/CR/CJ pedagogical practices are implemented during an elective course or workshop with a certain group of students regardless of the objectives of any curricular unit of the formal curriculum). According to Ennis (27), subject specificity was characterized as follows: general—an approach that attempts to teach CT/CR/CJ abilities and dispositions regardless of the subject content; infusive—an approach where students are encouraged to think critically in the subject (subject-related), in which general CT/CR/CJ principles are made explicit to the students; immersive—an approach where students are encouraged to think critically in the subject (subject-related), in which general CT/CR/CJ principles are not made explicit to the students; or mixed—an approach that combines the general approach with one of the other two, infusive or immersive.
Additionally, the analysis also considered the length of the intervention, the learning regime (face-to-face vs. e-learning), the work format (individual vs. collaborative), the presence or absence of a control group, the number of group interventions, the presence or absence of instructional support (contextualization, facilitators/tutors ‘guidance, or guidelines), or feedback during or at the end of the interventions.
To simplify the comparison between CT/CR/CJ pedagogical practices and learning outcomes, the assessment approach was classified according to the tool standard (standardized or non-standardized), the domain specificity (general, health sciences, or medical domain), and the assessment tool specificity to evaluate CT/CR/CJ skills and/or dispositions (tests or rubrics, knowledge tests, self-assessment surveys or questionnaires, and focus groups session).
Since some studies used more than one assessment tool, only the most effective in evaluating CT/CR/CJ pedagogical practices was used to describe the assessment approach in the following order:
1. Domain-specific standardized tests—any quantitative assessment tools used to measure CT/CR/CJ skills and/or dispositions specifically in the health science domain [e.g., The Health Science Reasoning Test (HSRT); Yoon’s Critical Thinking Disposition Instrument (YCTDI); Critical Thinking Disposition Assessment (CTDA); Objective Structured Clinical Examination (OSCE); and the Diagnostic Thinking Inventory (DTI)];
2. General standardized tests—any quantitative assessment tools used to measure CT/CR/CJ skills and/or dispositions with no specific domain [e.g., The California Critical Thinking Skills Test (CCTST); the Ennis–Weir Critical Thinking Essay Test; and the California Critical Thinking Disposition Inventory (CCTDI)];
3. Domain-specific non-standardized tests or rubrics—a quantitative assessment tool previously developed or adapted specifically to assess CT/CR/CJ skills and/or dispositions or students’ performance in CT/CR/CJ regarding the domain and the context of the intervention [e.g., Script Concordance Test (SCT), Key Feature Problem Examination (KFPE); Critical Thinking Skills Rating Instrument (CTSRI) — rubric, the Clinical reasoning performance — assessed with 3 knowledge tests as follows: (1) conceptual knowledge test with multiple choice questions, (2) strategic knowledge test with key feature questions, and (3) conditional knowledge with problem solving tests, clinical reasoning test, or problem solving tests assessed with rubrics];
4. Domain-specific non-standardized knowledge tests, self-assessment surveys, or questionnaires—a quantitative non-standardized or self-reported assessment tool previously developed to assess the learning experience as student knowledge retention, self-perception, or satisfaction with the pedagogical approach;
5. Domain-specific non-standardized focus group sessions—a qualitative non-standardized self-report assessment tool used to assess the learning experience such as the perception or satisfaction of the students with the pedagogical approach.
Considering the most significant assessment tool for the evaluation of the CT/CR/CJ pedagogical practices, the learning outcomes were classified as follows:
• CT/CR/CJ general gain (++) when a statistically significant gain in terms of a general set of CT/CR/CJ skills or dispositions was verified (based on the general score of domain-specific standardized tests, general standardized tests, or domain-specific non-standardized tests or rubrics);
• CT/CR/CJ specific gain (+) when a statistically significant gain was reported for a specific CT/CR/CJ skill or disposition (based on the individual score related to a specific item of domain-specific standardized tests, general standardized tests, or domain-specific non-standardized tests or rubrics);
• CT/CR/CJ no gain (−−) when no statistic gain in terms of a general set of CT/CR/CJ skills or dispositions was verified (based on the general score of domain-specific standardized tests, general standardized tests, domain-specific, or non-standardized tests or rubrics);
• Other gains (+?) as knowledge, satisfaction, or perception of the development of CT/CR/CJ skills and/or dispositions when a statistically significant gain or a qualitative gain was verified regarding the student learning experiences (based on the general score of domain-specific non-standardized tests, surveys or questionnaires, or a qualitative result of domain-specific focus group sessions).
• No other gains (−?) as knowledge, satisfaction, or perception of the development of CT/CR/CJ skills and/or dispositions when no statistically significant gain or a qualitative gain was verified regarding the student learning experiences (based on the general score of domain-specific non-standardized tests, surveys or questionnaires, or a qualitative result of domain-specific focus group sessions).
A total of 3,221 articles were identified through database screening and were subsequently subjected to a stepwise filtering process (Figure 1). After duplicate records were removed, the remaining 2,108 studies were screened in two phases. In the first phase, 726 studies were excluded based on the title and document type. In the second phase, 1,314 studies were excluded based on the abstract by applying the exclusion criteria. From the remaining 69 eligible records for full paper reading, 35 were excluded for not meeting the inclusion criteria. The remaining 33 studies were included in this systematic review.
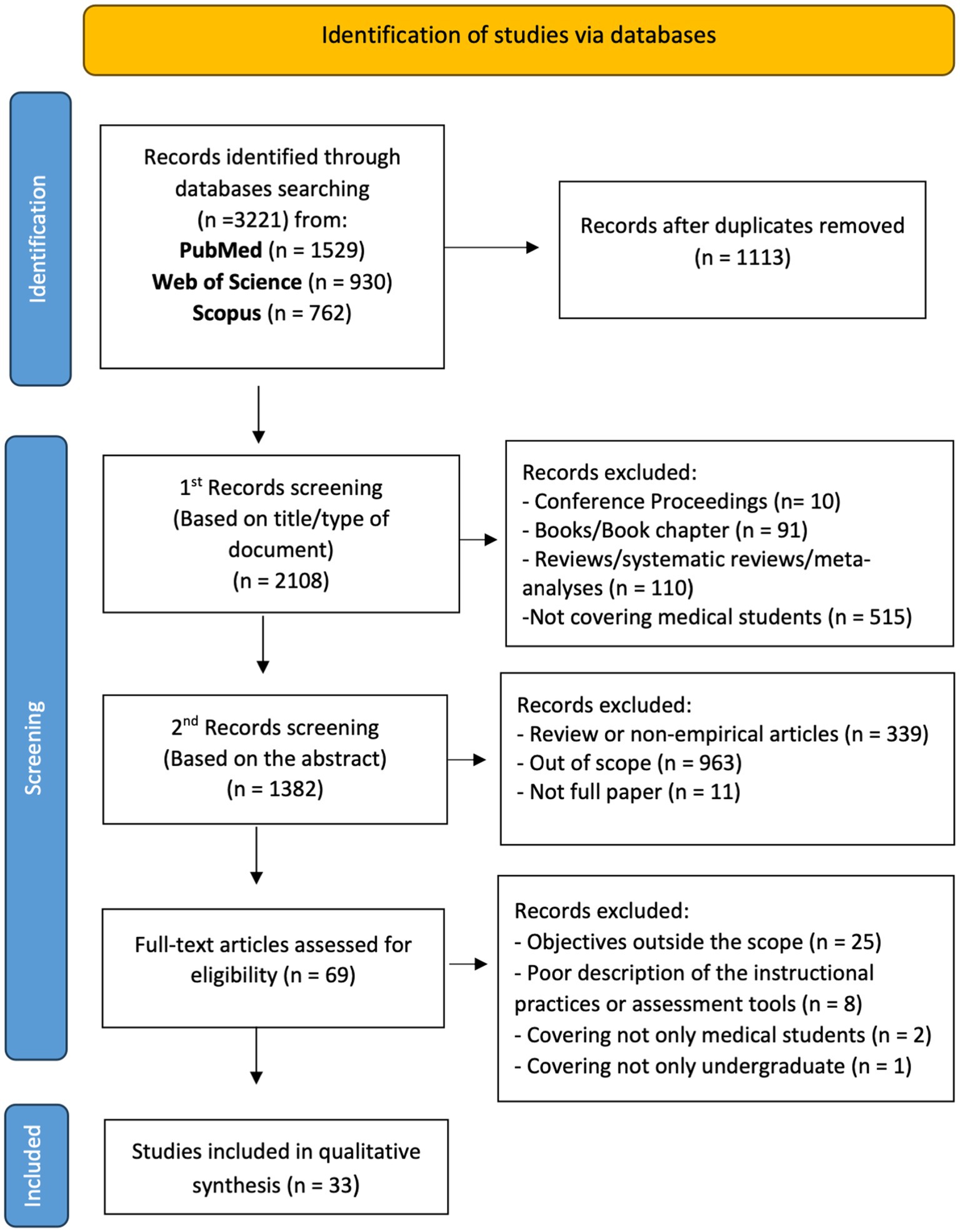
Figure 1. Flow PRISMA diagram of the included studies.
The results of the quality assessment are summarized in the Quality Assessment Table (Supplementary material). The quality rating ranged from 0.62 to 0.95 with a mean of 0.75. Lower ratings were due to a poor description of the sampling strategy and a lack of evidence of both verification procedures and reflexibility in qualitative and mixed studies. In quantitative and mixed studies, lower ratings were due to poor description and appropriateness of the sampling, incomplete baseline/demographic data, and lack of confounding assessment.
The included studies were markedly different in sample size, the smallest comprising 10 first-year medical students (28) and the largest comprising 214 third-year medical students (29).
The CT/CR/CJ pedagogical practices were applied to students attending the first 5 years of the medical course, with most studies covering the fourth year (n = 8) followed by the first (n = 6), second (n = 4), and third year (n = 4) (Tables 1, 2). In addition, of the 33 studies, 8 (40, 41, 46–49, 56, 58) studies recruited students from different academic years. Additionally, 61% of the studies did not mention the students’ age and 30% did not mention their gender.
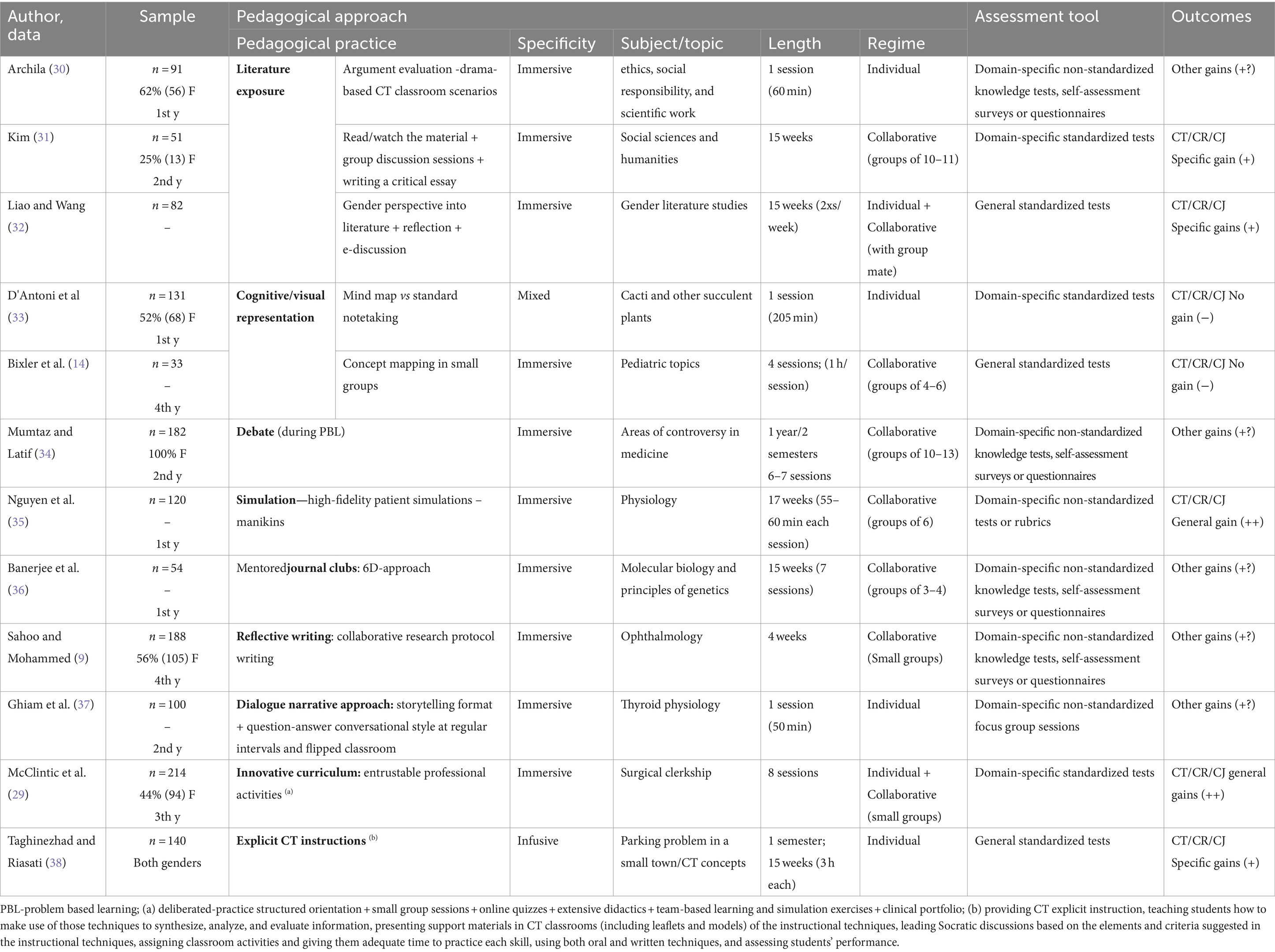
Table 1. Characteristics of the studies employing critical thinking pedagogical practices.
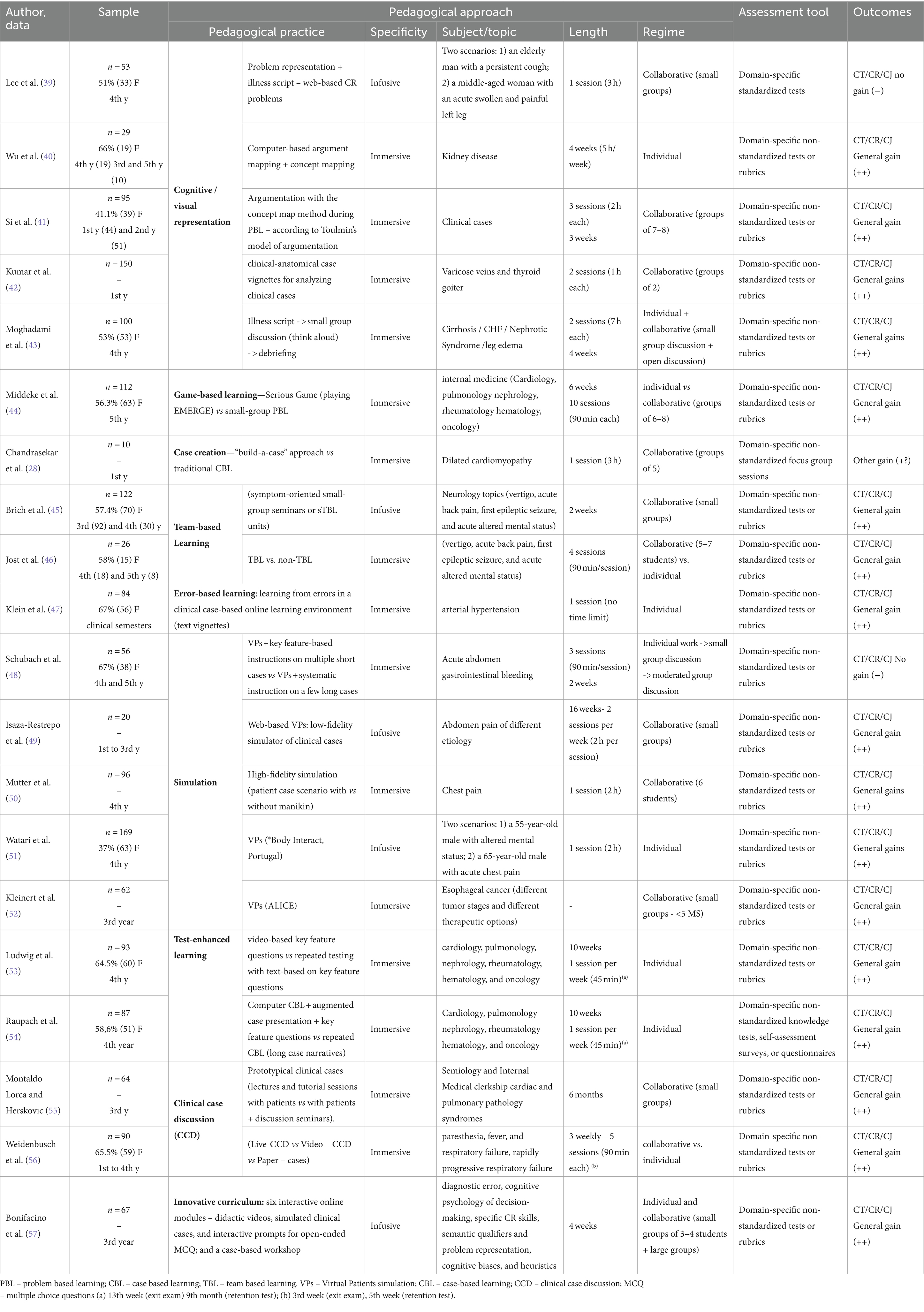
Table 2. Characteristics of the studies employing Clinical Reasoning pedagogical practices.
A diversity of pedagogical practices was used to foster the development of CT/CR/CJ skills and/or dispositions in undergraduate medical students (Tables 1, 2). The most frequently used were cognitive/visual representation approaches (8/33, 24.2%) as mind map (33), concept mapping (14, 40, 41), clinical-anatomical case vignettes (42), and illness script (39, 43, 59). In addition, simulation was also frequent (6/33, 18.2%) through virtual patients—low-fidelity patient simulations (48, 49, 51, 52) and manikins—high-fidelity patient simulations (35, 50).
Literature exposure was also reported (3/33, 9.0%) involving drama-based scenarios (30) and literature and film analysis (31) and integrating a gender perspective into literature studies (32).
Other approaches, such as test-enhancing learning (53, 54), team-based learning (46, 58), clinical case discussion (55, 56), case creation, team-based learning (46), game-based learning (44), error-based learning (47), dialog narrative approach (37), reflective writing (9), journal club (36), debate (34), and the explicit CT instruction approach (38), were mentioned in a few studies. Furthermore, some studies (29, 57) employed an innovative curriculum that combines different pedagogical approaches.
Pedagogical practices, such as cognitive/visual representation approaches, mind maps (33), illness-script (39, 43, 59), clinical-anatomy case vignettes (42), literature exposure by integrating the gender perspective into literature studies (32), simulation (50), clinical case discussion (55), team-based learning (46), test-enhancing learning (53, 54), explicit CT instruction approach (38), and the innovative curriculums (29, 57), were compared with the traditional format while case creation was compared with case-based learning (28).
Overall, CT/CR/CJ pedagogical practices were employed in both “curricular” (16/33; 48.5%) and “extracurricular” (17/33; 51.5%) contexts, predominantly with an “immersive” approach (25/33; 75.8%) and in a face-to-face regime (27/33; 78.8%).
The subjects/topics covered by the interventions were quite variable. Overall, as described in Tables 1, 2, they were mainly related to the medical curriculum (31/33; 93.9%), with just a few more associated with medical humanities (4/33; 12.1%) or not directly related to the typical medical curriculum topics (2/33; 6,1%) (33, 38).
Regarding other factors of the intervention, it is important to highlight that the length and/or the number of sessions were fairly different, with shorter interventions being implemented in a single session (9/33; 27.3%) and the longest over a year-long course. In addition, most of the studies (23/33; 69.7%) mentioned a collaborative format promoting peer learning with groups ranging from 2—discussion group mate and “think-pair-share” (32, 42)—to 15 students (59). Furthermore, most of the studies (29/33; 87.8%) mentioned the involvement of instructional support during the sessions by contextualizing the pedagogical practice and/or the aims of the session, providing guidelines/worksheets to provide clear and standardized instructions or providing facilitators/tutors’ guidance during the session, either by rising and/or answering questions or by moderating discussions. In addition, most studies (24/33; 72.7%) mentioned that debriefing or feedback was provided during or at the end of the interventions.
Table 3 shows the assessment tools that were identified in this review. Overall, the development of CT/CR/CJ skills and/or dispositions or students’ performance in CT/CR/CJ was mainly assessed by domain-specific non-standardized tests or rubrics (19 of 26; 73.1%), while student’s knowledge, satisfaction, or perceptions about the efficacy of the pedagogical practice to foster the development of CT/CR/CJ skills were mainly assessed through domain-specific knowledge tests, self-assessment surveys, or questionnaires (5 of 7; 71.4%).
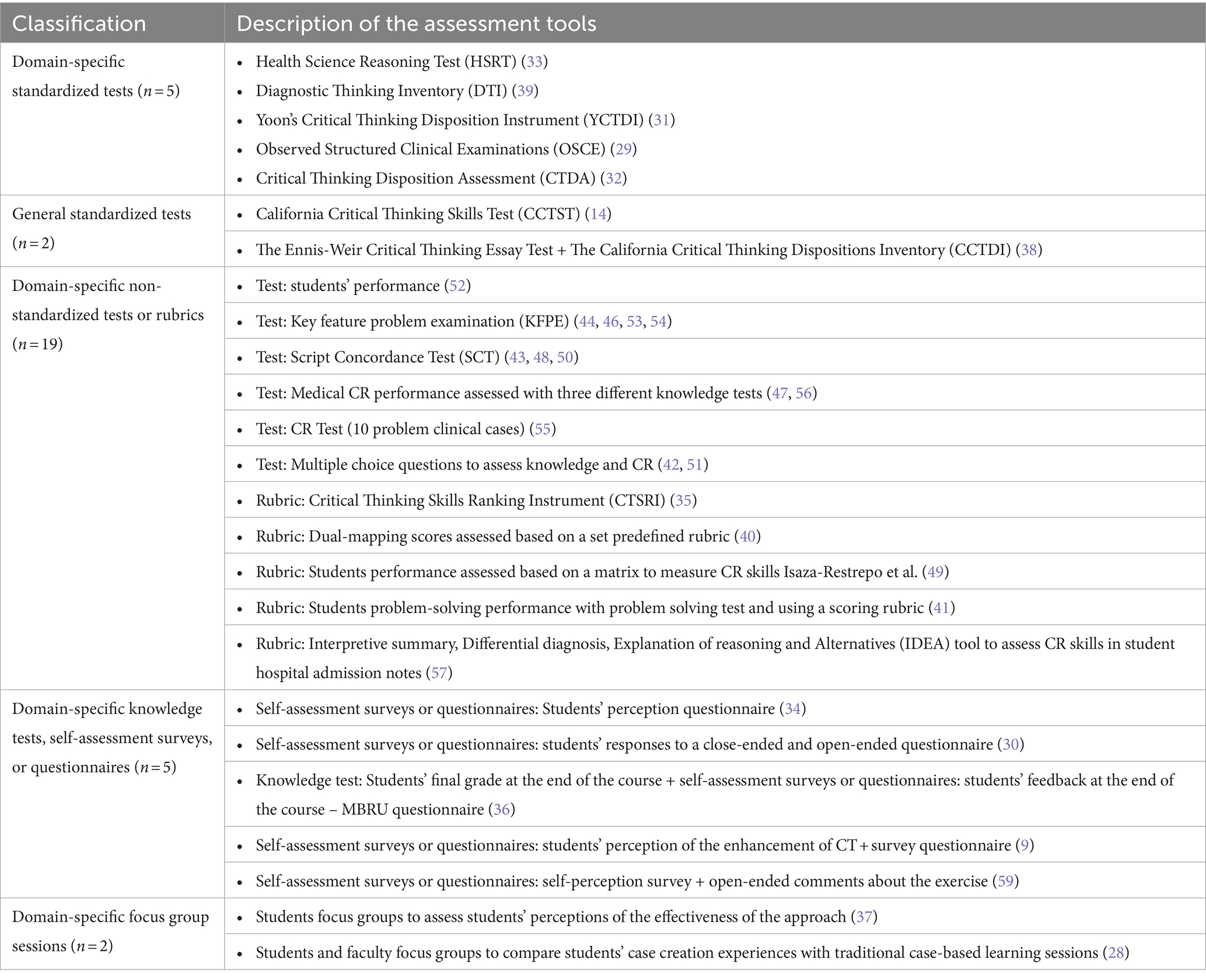
Table 3. Assessment tools mentioned in the selected studies (n = 33).
Of the 33 articles, 19 (57.6%) reported CT/CR/CJ general gains (++), 3 (9.1%) reported CT/CR/CJ specific gains (+), and 4 (12.1%) reported CT/CR/CJ no gains (−−). The remaining seven (21.2%) reported positive effects of the CT/CR/CJ pedagogical practices, but the gains were measured by considering improvements in knowledge or by assessing the students’ satisfaction or perceptions of the effectiveness of the intervention (Figure 2; Table 3).
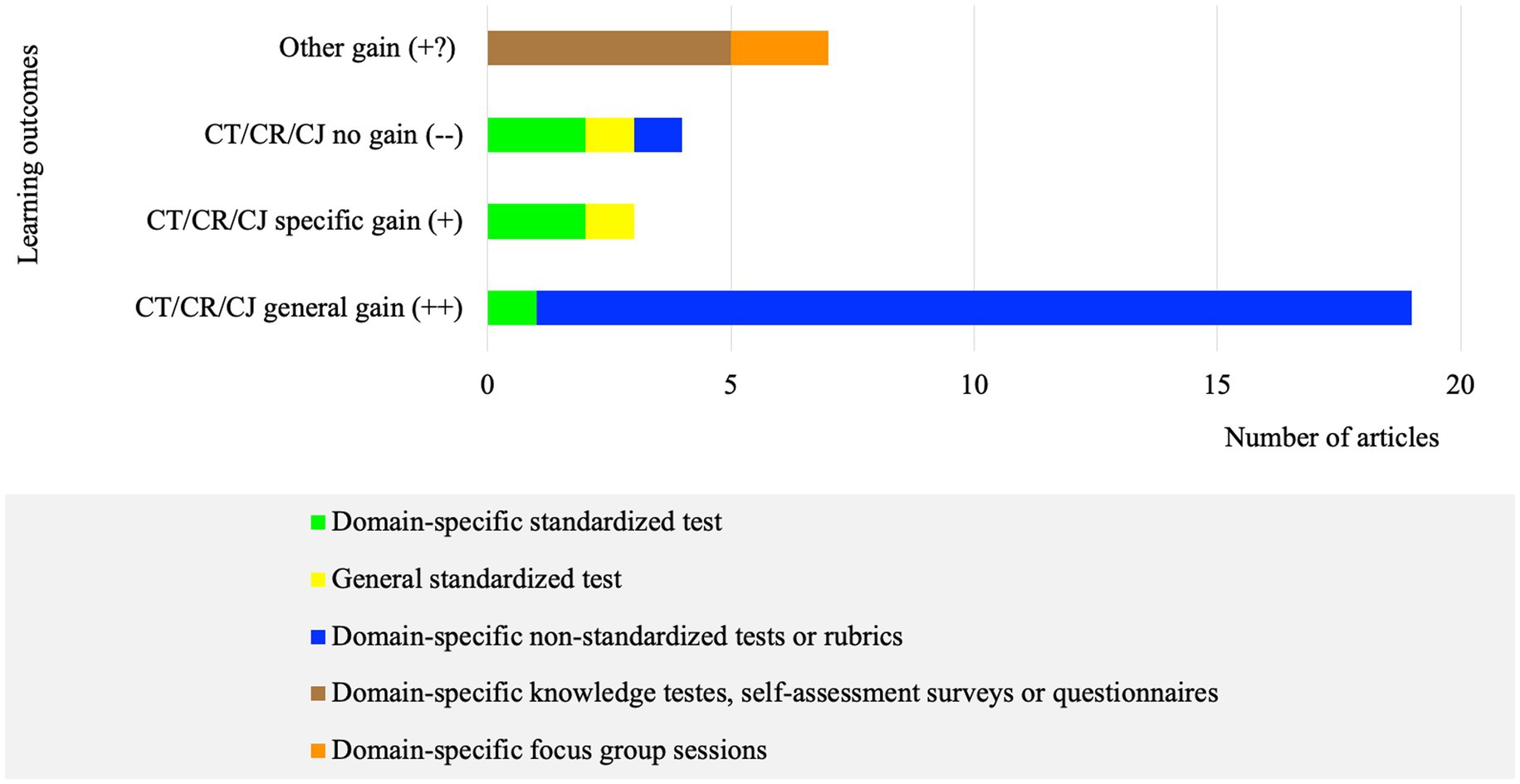
Figure 2. Number of articles per assessment tool regarding the learning outcomes (n = 33).
Learning outcomes were also analyzed according to curricular context, subject specificity, regime, format, presence or absence of instructional support, and feedback (Tables 1, 2). Table 4 summarizes the methodological characteristics of the articles.
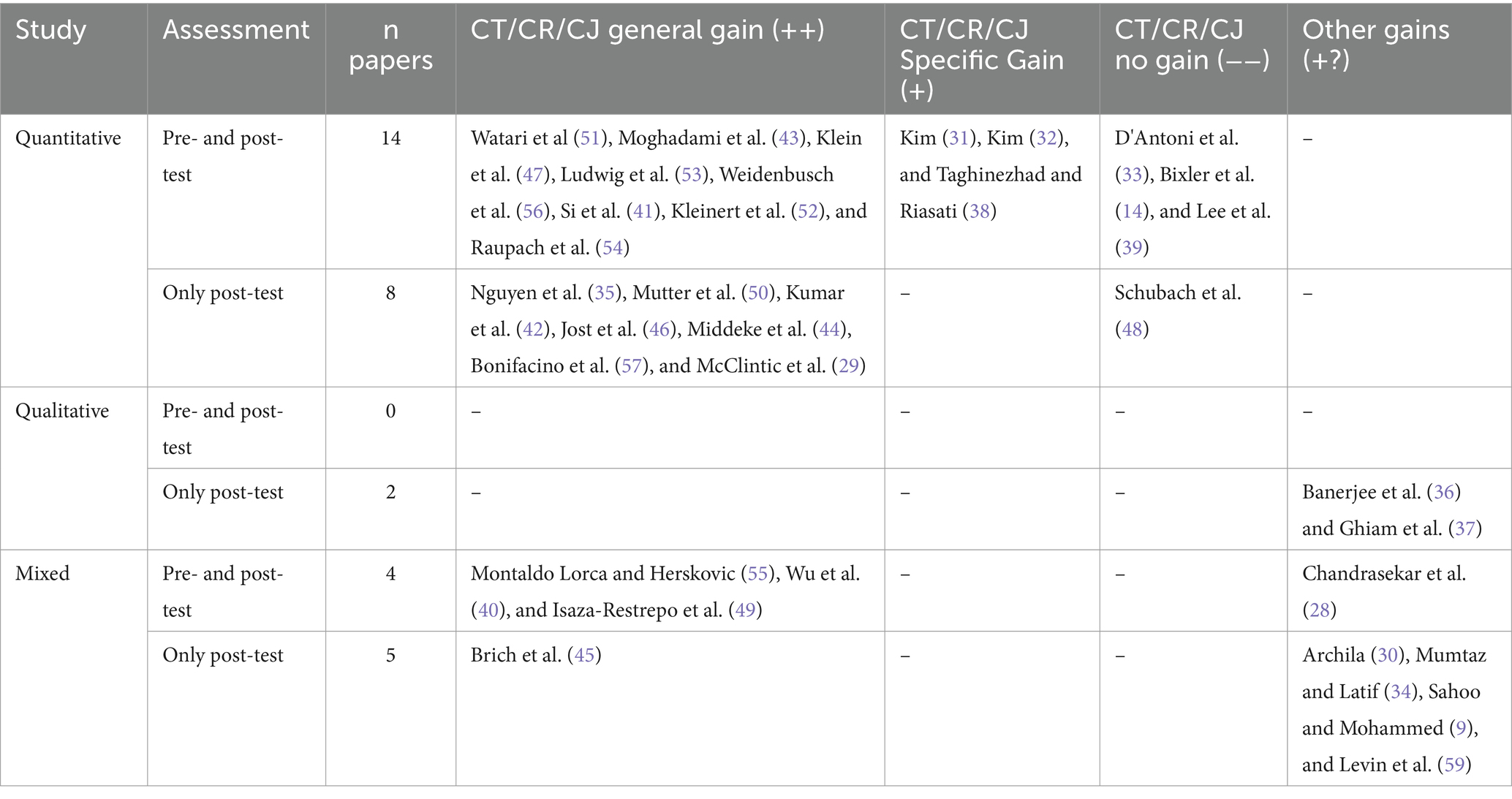
Table 4. Methodological characteristics of the selected articles (n = 33).
Of the 33 articles eligible for the review, 21 (63.6%) reported CR pedagogical practices and 12 (36.4%) reported CT pedagogical practices. No article reported interventions related to CJ pedagogical practices. Literature exposure, debate, journal club, reflective writing, dialog narrative approach, explicit CT instructions, high-fidelity patient simulation, and cognitive/visual representation (such as mind map and conceptual mapping) seem to be mainly used as CT pedagogical practices, while clinical case discussion, case creation, team-based learning, game-based learning, error-based learning, test-enhancing learning, low-fidelity simulation, and cognitive/visual representations (such as illness script, concept map, and clinical-anatomical case vignettes) seem to be mainly used as CR pedagogical practices. In addition, CT pedagogical practices were mostly applied to students attending the first (n = 4) and second (n = 3) academic years, while CR pedagogical practices, although applied in all academic years, were mostly used in the fourth year (n = 6), followed by third (n = 3), fourth plus fifth (n = 2), and first year (n = 2). Moreover, the studies that recruited students from different academic years only used CR pedagogical practices.
Regarding the multiple pedagogical practices, cognitive/visual representation and simulation were applied to the first 5 years of the curriculum. In addition, literature exposure, journal club, case creation, debate, and dialog narrative approach were implemented in the first 2 years of the curriculum, while game-based learning, team-based learning, error-based learning, and reflective writing were employed from the third to fifth years. Furthermore, domain-specific standardized tests, general standardized tests, domain-specific knowledge tests, self-assessment surveys, or questionnaires were mostly used to assess CT development, while domain-specific non-standardized tests or rubrics were mainly used to assess CR.
As for the development of CT/CR/CJ skills and dispositions based on targeted outcomes, CT pedagogical practices reported mostly other gains (+?) and specific gains (+), while CR pedagogical practices reported mainly general gains (++) (Figures 3, 4).
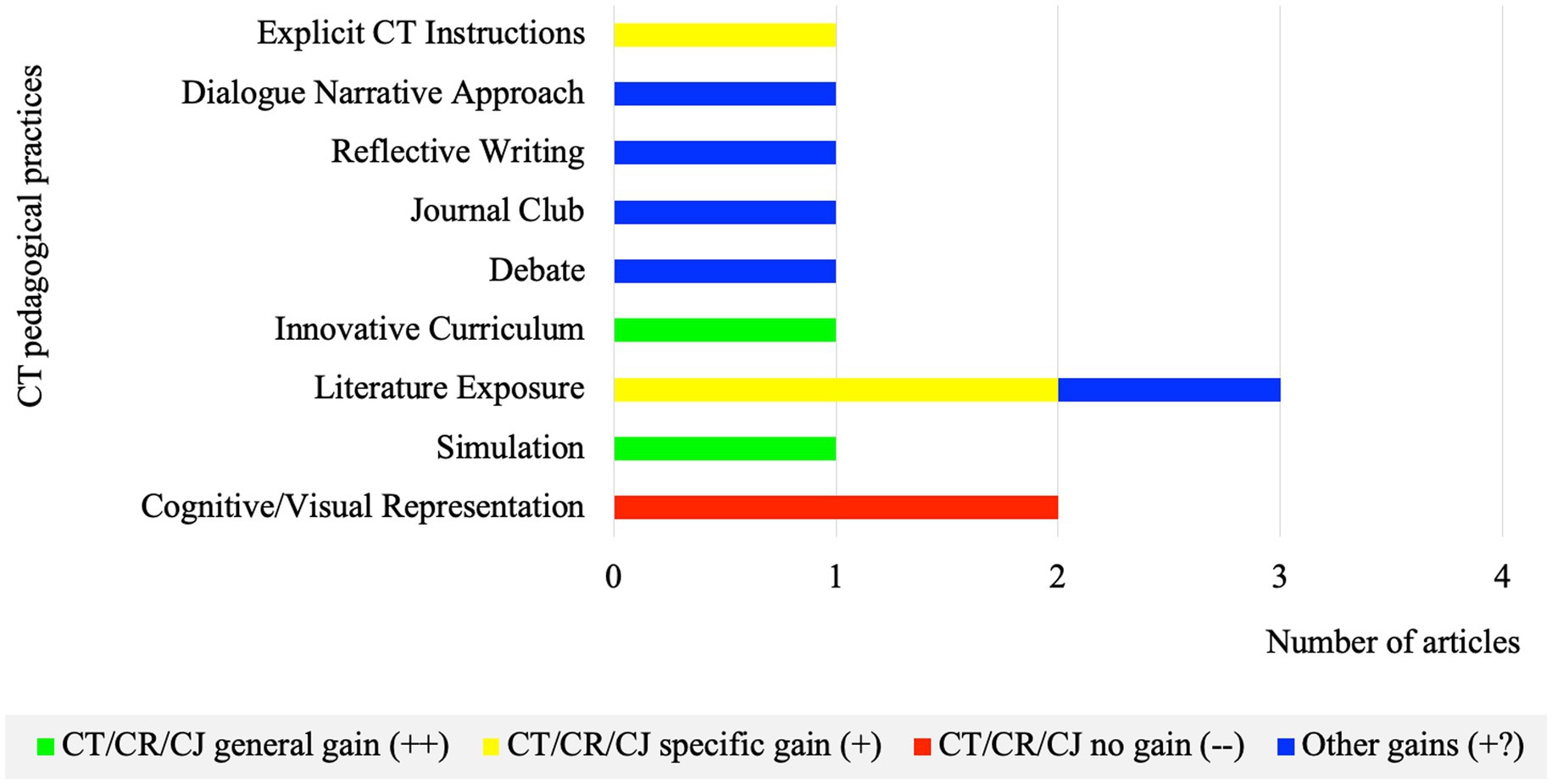
Figure 3. Number of articles per CT pedagogical practice regarding learning outcomes (n = 12).
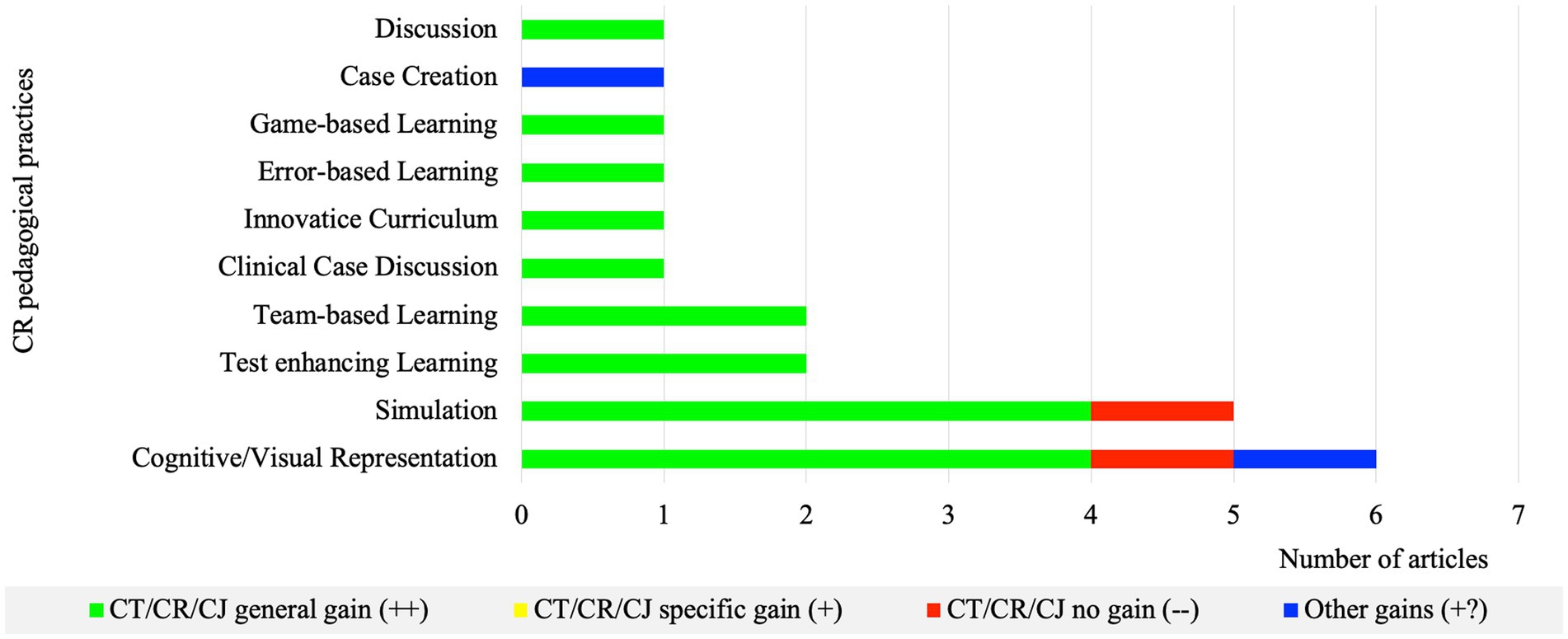
Figure 4. Number of articles per CR pedagogical practice regarding learning outcomes (n = 21).
Due to differences in study designs and methodologies, as well as the diversity of CT/CR/CJ pedagogical practices and respective assessment tools used in the selected studies, it is challenging to identify the most effective pedagogical practices in fostering the development of CT/CR/CJ skills and/or dispositions in medical students.
Nevertheless, pedagogical practices, such as cognitive/visual representation, simulation, literature exposure, test-enhancing and team-based learning, clinical case discussion, error-based learning, game-based learning, explicit CT instructions, and the innovative curriculum approaches, seem to be effective in the development of the CT/CR/CT skills and/or dispositions as most of them reported CT/CR/CJ general gains (++). Alternatively, pedagogical practices, such as debate, journal club, reflective writing, dialog narrative approach, and case creation, seem to have a positive impact on students’ learning experience, showing improvements in student’s knowledge, satisfaction, and perception of the development of CT/CR/CJ. However, these outcomes do not directly express CT/CR/CJ since, knowledge per se is not enough for its development (60). In addition, the concept of CT/CR/CJ is still complex and ambiguous, leading to different perceptions among students, teachers, and experts on CT (17). Therefore, no conclusion can be inferred either from knowledge improvements or students’ perceptions of the development of CT/CR/CJ and the effective development of those skills.
When comparing CT and CR pedagogical practices, despite the differences in the medical curriculum length across countries, usually the first years are basic science-oriented while the last years are clinical training-orientated. This may be particularly interesting given that CT pedagogical practices seem to be mainly employed during the first 2 years of the curriculum, and CR pedagogical approaches are more commonly used in the last years, which may be related to the fact that CR constitutes CT application within a clinical context (61).
Most studies seem to foster CT mainly through the development of skills and dispositions. On the other hand, studies fostering CR development, in line with past evidence, were more profession-oriented and focused mainly on the development of diagnostic and decision-making skills (24, 62). In addition, the studies evaluating the effectiveness of pedagogical practices were mainly focused on fostering and assessing both CT and CR skills, whereas studies focused on dispositions were limited (n = 3) and only used in the context of CT (31, 32). Therefore, this can be related to how doctors conceptualize CT (i.e., in their definitions) (17). As we know, CT “requires mastery of context-specific knowledge to evaluate specific beliefs, claims, and actions” (63). Therefore, it may be useful to apply pedagogical practices that encourage the development of CT dispositions as “open-mindedness, willingness to reconsider, honesty about personal biases and persistence” (15) in the early years of the medical curriculum. As students acquire a deeper knowledge, pedagogical practices that foster CT/CR skills, more oriented to clinical decision and problem solving, could be explored. According to students’ needs and learning objectives, CT and CR pedagogical practices could be combined to achieve a more comprehensive development of skills and dispositions.
Regarding the “curricular” and “extracurricular” approaches, we have found contrasting results, with both reporting CT/CR/CJ general gains (++) (56.3% versus 58.8%) and CT/CR/CJ no gains (−−) (6.3% versus 17.6%). In agreement with previous literature, some authors believe that CT skills can be assessed regardless of the context, while others disagree (64).
Regarding the subject specificity, most studies that adopted an “immersive” followed by an “infusive” approach positively impacted the development of CT/CR/CJ skills and/or dispositions and students’ learning experiences (92.0 and 85.7%, respectively). Considering these results, and that the only study with a mixed approach reported CT/CR/CJ no gains (−−), it seems that an approach in which students are encouraged to think critically about a subject (subject-related) could be more effective, especially when they have prior knowledge on the topic. In fact, some studies show the need for a sustained specific-knowledge background to enable its application in more complex systems (60, 65). In contrast, when comparing the “immersive” and “infusive” approaches, despite the limited number of studies reporting an “infusive” approach (n = 7), we can suggest that the most effective are those that make these principles explicit to students. Furthermore, gains resulting from the explicit CT instructions approach corroborate this (38). Therefore, it would be interesting to incorporate CT as a specific subject in the medical curriculum, ideally during the first year.
Regarding the intervention length, some studies report that longer, progressive, and continuous interventions can lead to better outcomes, indicating that length may be an important factor in the development of CT. Although supported by a previous systematic review (24), the results herein presented are not enough to support this association.
Regarding the regime of the approach, most strategies applied the face-to-face approach, although both face-to-face and e-learning methodologies seem to positively impact the development of CT/CR/CJ.
Both individual and collaborative approaches seem to have a positive impact on the development of CT/CR. However, the learning experience can be improved by students’ engagement in discussions with each other (56). In addition, pedagogical practices seem to increase their efficacy in the following order: passive < active < constructive < interactive learning environments (66). This highlights the need to better understand the role of group interaction in the development of CT when assessing the impact of the number of students per group, both large (7 to 8 medical students) and small groups (2 medical students), and induced CT/CR/CJ general gains (++). In addition to group size, constitution seems to play a pivotal role in the effectiveness of the pedagogical practices. For instance, in heterogeneous groups, the strongest students may end up doing all the work, especially when a limited amount of time is available to perform a task. However, heterogeneity may also breed different backgrounds and perspectives on a subject, thus enriching discussion and aiding group productivity (67). In contrast, a homogeneous group will probably operate on the extremes, with the strongest groups completing their work more quickly, while the weaker groups need more time or do not complete the task by themselves (67).
Additionally, the pedagogical practice effectiveness seems to depend on the tutor and his CT proficiency (44, 68, 69). Although most studies mentioned instructional support (87.9%) or feedback (66.7%), only a minority considered their educational role and impact in fostering CT. Kim (31) highlights that activities based on interactions and feedback (e.g., group discussion and narrative comments) were more advantageous for CT development than those done individually (i.e., book reading and essay writing) (31). In agreement, some authors (28, 46, 70) suggest that the presence of an instructor through students’ guidance and prevention of misunderstandings or misconceptions can benefit both the pedagogical approach and learning experiences. Instructional support and feedback ensure that learners with learning difficulties are adequately supported in their learning process (47).
The lack of results regarding the learning outcomes may be related to differences between studies in terms of methodology and design, particularly in the intervention length, subject specificity, and assessment tools. Hence, negative outcomes might have resulted from the unfamiliarity with the approach that may have led to less proficiency (37) or from the short duration of studies with high cognitive load interventions that may compromise student adjustment to pedagogical practice and consequent performance (48).
Overall, developing CT/CR/CJ skills represents a complex learning challenge. The learner is involved in a combination of meaningful learning activities that promote both knowledge, by integrating new information into pre-existing frameworks (71), and skills such as observation, analysis, evaluation, contextualization, questioning, and, finally, reflection on a subject or a problem (72, 73). A learning environment that promotes individual growth through peer instruction, meaningful learning, and learning by doing, in which students play an active role in the learning process and receive proper feedback, is essential to ensure the efficacy of a pedagogical approach (49).
To the best of our knowledge, this is the first systematic review focused on the effectiveness of CT/CR/CJ pedagogical practices in medical education. Some limitations were identified. Although most studies were mainly focused on pedagogical practice, the presence of other approaches may have had an impact on the results. In addition, gains may also have been influenced by the educational environment, other concurrent courses, or the existence of residual or unmeasured confounders (31). Caution must also be taken with the studies describing assessment tools not previously validated for the study population (e.g., general standardized tests), as well as when a domain-specific non-standardized test or rubric was used, compromising the reproducibility of the intervention in other fields, as well as when studies relied upon a post-test assessment and/or there was no control group or other comparative intervention. Finally, no language restrictions were applied to our research strategy, but the search terms we used were in English. Given that most of the non-English language journals translate the abstract into English, we suggest that the search terms used only in English did not significantly affect the search outcomes.
Future studies should be planned and designed detailing the context of the intervention, the subject specificity, objectives, length, regime (face-to-face vs. e-learning), format (individual vs. collaborative), the role of the facilitators, the presence or absence of feedback, and the teacher’s expertise in CT/CR/CJ. Future research should also explore how to assess the long-term impact of the interventions on CT retention over time.
Pedagogical practices that actively engage undergraduate medical students in the learning process are likely more effective than traditional lectures in fostering the development of CT/CR/CJ skills and/or dispositions. However, comparison between practices is not easy due to the limited number of studies and diverse methodologies and assessment tools employed. Despite these challenges, our systematic review raises important questions about the timing, length, curricular context, regime (face-to-face vs. e-learning), and format (individual vs. collaborative) of interventions that should be carefully considered to enhance the effectiveness of the pedagogical approaches. Furthermore, it acknowledges the complexity of fostering critical thinking in medical education, recognizing that there is no “one-size-fits-all solution.” Overall, we can conclude that different pedagogical practices should be used and combined throughout the curriculum considering diverse learning environments and student needs to effectively enhance CT skills and dispositions of medical students.
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
BA: Conceptualization, Investigation, Methodology, Writing – original draft. SG: Investigation, Methodology, Writing – review & editing. LR: Conceptualization, Supervision, Writing – review & editing, Investigation, Methodology.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2024.1358444/full#supplementary-material
1. Patterson, F, and Zibarras, LD. Selecting for creativity and innovation potential: implications for practice in healthcare education. Adv Health Sci Educ Theory Pract. (2017) 22:417–28. doi: 10.1007/s10459-016-9731-4
2. Guragai, M, and Mandal, D. Five skills medical students should have. J Nepal Med Ass. (2020) 58:269–71. doi: 10.31729/jnma.4878
3. Kerins, J, Smith, SE, Phillips, EC, Clarke, B, Hamilton, AL, and Tallentire, VR. Exploring transformative learning when developing medical students' non-technical skills. Med Educ. (2020) 54:264–74. doi: 10.1111/medu.14062
4. Revere, D, Turner, AM, Madhavan, A, Rambo, N, Bugni, PF, Kimball, A, et al. Understanding the information needs of public health practitioners: a literature review to inform design of an interactive digital knowledge management system. J Biomed Inform. (2007) 40:410–21. doi: 10.1016/j.jbi.2006.12.008
5. OECD Health Division team. (2018). Feasibility study on health workforce skills assessment—supporting health workers achieve person-centred care. Available at: https://www.oecd.org/els/health-systems/Feasibility-Study-On-Health-Workforce-Skills-Assessment-Feb2018.pdf
6. UNESCO. (2017). Education for sustainable development goals: learning objectives. Available at: https://unesdoc.unesco.org/ark:/48223/pf0000247444
7. Straková, Z, and Cimermanová, I. Critical thinking development—a necessary step in higher education transformation towards sustainability. Sustain For. (2018) 10:3366. Available at: https://www.mdpi.com/2071-1050/10/10/3366
8. Kuiper, RA, and Pesut, DJ. Promoting cognitive and metacognitive reflective reasoning skills in nursing practice: self-regulated learning theory. J Adv Nurs. (2004) 45:381–91. doi: 10.1046/j.1365-2648.2003.02921.x
9. Sahoo, S, and Mohammed, CA. Fostering critical thinking and collaborative learning skills among medical students through a research protocol writing activity in the curriculum. Korean J Med Educ. (2018) 30:109–18. doi: 10.3946/kjme.2018.86
10. Ross, D, Loeffler, K, Schipper, S, Vandermeer, B, and Allan, GM. Do scores on three commonly used measures of critical thinking correlate with academic success of health professions trainees? A systematic review and meta-analysis. Acad Med. (2013) 88:724–34. doi: 10.1097/ACM.0b013e31828b0823
11. Papp, KK, Huang, GC, Lauzon Clabo, LM, Delva, D, Fischer, M, Konopasek, L, et al. Milestones of critical thinking: a developmental model for medicine and nursing. Acad Med. (2014) 89:715–20. doi: 10.1097/acm.0000000000000220
12. Shehata, GM, Zaki, A, Dowidar, NL, and El Sayed, I. Critical thinking and attitude of physicians toward evidence-based medicine in Alexandria, Egypt. J Egypt Public Health Ass. (2015) 90:115–20. doi: 10.1097/01.EPX.0000470848.07476.f9
13. Zayapragassarazan, Z, Vikas, M, Sitanshu, SK, and Gitanjali, B. Understanding critical thinking to create better doctors. J Adv Med Educ Res. (2016) 1:9–13.
14. Bixler, GM, Brown, A, Way, D, Ledford, C, and Mahan, JD. Collaborative concept mapping and critical thinking in fourth-year medical students. Clin Pediatr. (2015) 54:833–9. doi: 10.1177/0009922815590223
15. Facione, P. (1990). Critical thinking: a statement of expert consensus for purposes of educationalassessment and instruction. Research findings and recommendations. AmericanPhilosophical Association. Available at: http://files.eric.ed.gov/fulltext/ED315423.pdf
16. Zia, A, and Dar, UF. Critical thinking: perception and disposition of students in a medical College of Pakistan. J Pak Med Assoc. (2019) 69:968–72.
17. Krupat, E, Sprague, JM, Wolpaw, D, Haidet, P, Hatem, D, and O'Brien, B. Thinking critically about critical thinking: ability, disposition or both? Med Educ. (2011) 45:625–35. doi: 10.1111/j.1365-2923.2010.03910.x
18. Lefebvre, C, Glanville, J, Briscoe, S, Littlewood, A, Marshall, C, Metzendorf, M-I, et al. Searching for and selecting studies In: JPT Higgins, J Thomas, J Chandler, M Cumpston, T Li, and MJ Page, et al. (Editors), Cochrane Handbook for Systematic Reviews of Interventions (2019). 67–107.
19. Li, T, Higgins, JPT, and Deeks, JJ. Collecting data In: JPT Higgins, J Thomas, J Chandler, M Cumpston, T Li, and MJ Page, et al. (Editors), Cochrane handbook for systematic reviews of interventions (2019). 109–41.
20. McKenzie, JE, Brennan, SE, Ryan, RE, Thomson, HJ, Johnston, RV, and Thomas, J. Defining the criteria for including studies and how they will be grouped for the synthesis In: JPT Higgins, J Thomas, J Chandler, M Cumpston, T Li, and MJ Page, et al. (Editors), Cochrane handbook for systematic reviews of interventions (2019). 33–65.
21. Schünemann, HJ, Vist, GE, Higgins, JPT, Santesso, N, Deeks, JJ, Glasziou, P, et al. Interpreting results and drawing conclusions In: JPT Higgins, J Thomas, J Chandler, M Cumpston, T Li, and MJ Page, et al. (Editors), Cochrane handbook for systematic reviews of interventions (2019). 403–31.
22. Thomas, J, Kneale, D, McKenzie, JE, Brennan, SE, and Bhaumik, S. Determining the scope of the review and the questions it will address In: JPT Higgins, J Thomas, J Chandler, M Cumpston, T Li, and MJ Page, et al. (Editors), Cochrane handbook for systematic reviews of interventions (2019). 13–31.
23. Page, MJ, McKenzie, JE, Bossuyt, PM, Boutron, I, Hoffmann, TC, Mulrow, CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. (2021) 372:n71. doi: 10.1136/bmj.n71
24. Payan-Carreira, R, Cruz, G, Papathanasiou, IV, Fradelos, EC, and Jiang, L. The effectiveness of critical thinking instructional strategies in health professions education: a systematic review. Stud High Educ. (2019) 44:829–43. doi: 10.1080/03075079.2019.1586330
25. Methley, AM, Campbell, S, Chew-Graham, C, McNally, R, and Cheraghi-Sohi, S. PICO, PICOS and SPIDER: a comparison study of specificity and sensitivity in three search tools for qualitative systematic reviews. BMC Health Serv Res. (2014) 14:579. doi: 10.1186/s12913-014-0579-0
26. Kmet, L., Lee, R., and Cook, L. (2004). Standard quality assessment criteria for evaluating primary research papers from a variety of FieldsAHFMRHTA Initiative20040213. HTA Initiative, 2. Available at: https://era.library.ualberta.ca/items/48b9b989-c221-4df6-9e35-af782082280e/view/a1cffdde-243e-41c3-be98-885f6d4dcb29/standard_quality_assessment_criteria_for_evaluating_primary_research_papers_from_a_variety_of_fields.pdf
27. Ennis, RH. “Critical Thinking and Subject Specificity: Clarification and Needed Research.” Educ Res. (1989) 18:4–10.
28. Chandrasekar, H, Gesundheit, N, Nevins, AB, Pompei, P, Bruce, J, and Merrell, SB. Promoting student case creation to enhance instruction of clinical reasoning skills: a pilot feasibility study. Adv Med Educ Pract. (2018) 9:249–57. doi: 10.2147/amep.S155481
29. McClintic, JA, Snyder, CL, and Brown, KM. Curricular innovation in the surgery clerkship: can assessment methods influence development of critical thinking and clinical skills? [article]. J Surg Educ. (2018) 75:1236–44. doi: 10.1016/j.jsurg.2018.02.012
30. Archila, P. Evaluating arguments from a play about ethics in science: a study with medical learners. Argumentation. (2018) 32:53–76. doi: 10.1007/s10503-017-9429-7
31. Kim, DH. Evaluation of critical thinking course for premedical students using literature and film. Korean J Med Educ. (2019) 31:19–28. doi: 10.3946/kjme.2019.115
32. Liao, HC, and Wang, YH. Integrating the gender perspective into literature studies to enhance medical university students’ gender awareness and critical thinking [article]. Int J Environ Res Public Health. (2020) 17:Article 9245:1–13. doi: 10.3390/ijerph17249245
33. D'Antoni, AV, Zipp, GP, Olson, VG, and Cahill, TF. Does the mind map learning strategy facilitate information retrieval and critical thinking in medical students? BMC Med Educ. (2010) 10:61. doi: 10.1186/1472-6920-10-61
34. Mumtaz, S, and Latif, R. Learning through debate during problem-based learning: an active learning strategy [article]. Adv Physiol Educ. (2017) 41:390–4. doi: 10.1152/advan.00157.2016
35. Nguyen, K, Khallouq, BB, Schuster, A, Beevers, C, Dil, N, Kay, D, et al. Developing a tool for observing group critical thinking skills in first-year medical students: a pilot study using physiology-based, high-fidelity patient simulations [article]. Adv Physiol Educ. (2017) 41:604–11. doi: 10.1152/ADVAN.00126.2017
36. Banerjee, Y, Azar, AJ, Tuffnell, C, Lansberg, PJ, Bayoumi, R, and Davis, D. A novel 6D-approach to radically transform undergraduate medical education: preliminary reflections from MBRU. BMC Med Educ. (2018) 18:304. doi: 10.1186/s12909-018-1402-0
37. Ghiam, BK, Loftus, S, and Kamel-ElSayed, S. Dialogical narrative approach to enhance critical thinking and student engagement during lecture-based classes. Focus Health Prof Educ Multidiscipl J. (2019) 20:30–43. doi: 10.11157/fohpe.v20i3.344
38. Taghinezhad, A, and Riasati, MJ. The interplay of critical thinking explicit instruction, academic writing performance, critical thinking ability, and critical thinking dispositions: an experimental study [article]. IJERI. (2020) 13:143–65. doi: 10.46661/ijeri.4594
39. Lee, A, Joynt, GM, Lee, AK, Ho, AM, Groves, M, Vlantis, AC, et al. Using illness scripts to teach clinical reasoning skills to medical students. Fam Med. (2010) 42:255–61.
40. Wu, B, Wang, M, Johnson, JM, and Grotzer, TA. Improving the learning of clinical reasoning through computer-based cognitive representation. Med Educ Online. (2014) 19:25940. doi: 10.3402/meo.v19.25940
41. Si, J, Kong, HH, and Lee, SH. Developing clinical reasoning skills through argumentation with the concept map method in medical problem-based learning. Interdiscipl J prob Learn. (2019) 13:17763. doi: 10.7771/1541-5015.1776
42. Kumar, V, Rajprasath, R, Priyadharshini, NA, Murugan, M, and Devi, R. Infusing the axioms of clinical reasoning while designing clinical anatomy case vignettes teaching for novice medical students: a randomised cross over study. Anat Cell Biol. (2020) 53:151–61. doi: 10.5115/acb.19.199
43. Moghadami, M, Amini, M, Moghadami, M, Dalal, B, and Charlin, B. Teaching clinical reasoning to undergraduate medical students by illness script method: a randomized controlled trial. BMC Med Educ. (2021) 21:87. doi: 10.1186/s12909-021-02522-0
44. Middeke, A, Anders, S, Schuelper, M, Raupach, T, and Schuelper, N. Training of clinical reasoning with a serious game versus small-group problem-based learning: a prospective study. PLoS One. (2018) 13:e0203851. doi: 10.1371/journal.pone.0203851
45. Brich, J, Jost, M, Brüstle, P, Giesler, M, and Rijntjes, M. Teaching neurology to medical students with a simplified version of team-based learning [article]. Neurology. (2017) 89:616–22. doi: 10.1212/WNL.0000000000004211
46. Jost, M, Brüstle, P, Giesler, M, Rijntjes, M, and Brich, J. Effects of additional team-based learning on students' clinical reasoning skills: a pilot study. BMC Res Notes. (2017) 10:282. doi: 10.1186/s13104-017-2614-9
47. Klein, M, Otto, B, Fischer, MR, and Stark, R. Fostering medical students' clinical reasoning by learning from errors in clinical case vignettes: effects and conditions of additional prompting procedures to foster self-explanations. Adv Health Sci Educ Theory Pract. (2019) 24:331–51. doi: 10.1007/s10459-018-09870-5
48. Schubach, F, Goos, M, Fabry, G, Vach, W, and Boeker, M. Virtual patients in the acquisition of clinical reasoning skills: does presentation mode matter? A quasi-randomized controlled trial. BMC Med Educ. (2017) 17:165. doi: 10.1186/s12909-017-1004-2
49. Isaza-Restrepo, A, Gomez, MT, Cifuentes, G, and Arguello, A. The virtual patient as a learning tool: a mixed quantitative qualitative study [article]. BMC Med Educ. (2018) 18:Article 297. doi: 10.1186/s12909-018-1395-8
50. Mutter, MK, Martindale, JR, Shah, N, Gusic, ME, and Wolf, SJ. Case-based teaching: does the addition of high-Fidelity simulation make a difference in medical Students' clinical reasoning skills? Med Sci Educ. (2020) 30:307–13. doi: 10.1007/s40670-019-00904-0
51. Watari, T, Tokuda, Y, Owada, M, and Onigata, K. The utility of virtual patient simulations for clinical reasoning education. Int J Environ Res Public Health. (2020) 17:5325. doi: 10.3390/ijerph17155325
52. Kleinert, R, Heiermann, N, Plum, PS, Wahba, R, Chang, DH, Maus, M, et al. Web-based immersive virtual patient simulators: positive effect on clinical reasoning in medical education. J Med Internet Res. (2015) 17:e263. doi: 10.2196/jmir.5035
53. Ludwig, S, Schuelper, N, Brown, J, Anders, S, and Raupach, T. How can we teach medical students to choose wisely? A randomised controlled cross-over study of video- versus text-based case scenarios. BMC Med. (2018) 16:107. doi: 10.1186/s12916-018-1090-y
54. Raupach, T, Andresen, JC, Meyer, K, Strobel, L, Koziolek, M, Jung, W, et al. Test-enhanced learning of clinical reasoning: a crossover randomised trial. Med Educ. (2016) 50:711–20. doi: 10.1111/medu.13069
55. Montaldo Lorca, G, and Herskovic, LP. Teaching of clinical reasoning to medical students using prototypical clinical cases. Revista Medica de Chile. (2013) 141:823–30. doi: 10.4067/S0034-98872013000700001
56. Weidenbusch, M, Lenzer, B, Sailer, M, Strobel, C, Kunisch, R, Kiesewetter, J, et al. Can clinical case discussions foster clinical reasoning skills in undergraduate medical education? A randomised controlled trial. BMJ Open. (2019) 9:e025973. doi: 10.1136/bmjopen-2018-025973
57. Bonifacino, E, Follansbee, WP, Farkas, AH, Jeong, K, McNeil, MA, and DiNardo, DJ. Implementation of a clinical reasoning curriculum for clerkship-level medical students: a pseudo-randomized and controlled study. Diagnosi. (2019) 6:165–72. doi: 10.1515/dx-2018-0063
58. Brich, J. Feasibility, acceptance and impact of team-based learning in neurology: a pilot study. GMS Z Med Ausbild. (2013) 30:Doc20. doi: 10.3205/zma000863
59. Levin, M, Cennimo, D, Chen, S, and Lamba, S. Teaching clinical reasoning to medical students: a case-based illness script worksheet approach. MedEdPORTAL. (2016) 12:10445. doi: 10.15766/mep_2374-8265.10445
60. Abrami, P, Bernard, R, Borokhovski, E, Wade, A, Surkes, M, Tamim, R, et al. Instructional interventions affecting critical thinking skills and dispositions: a stage 1 Meta-analysis. Rev Educ Res. (2008) 78:1102–34. doi: 10.3102/0034654308326084
61. Victor-Chmil, J. Critical thinking versus clinical reasoning versus clinical judgment: differential diagnosis. Nurse Educ. (2013) 38:34–6. doi: 10.1097/NNE.0b013e318276dfbe
62. Cruz, G, Payan Carreira, R, and Dominguez, C. Critical thinking education in the portuguese higher education institutions: a systematic review of educational practices. Revista Lusófona de Educação. (2017) 38:43–61. doi: 10.24140/issn.1645-7250.rle38.03
64. Nair, GG, and Stamler, LL. A conceptual framework for developing a critical thinking self-assessment scale. J Nurs Educ. (2013) 52:131–8. doi: 10.3928/01484834-20120215-01
65. Hughes, C. Theory of knowledge aims, objectives and assessment criteria: an analysis of critical thinking descriptors. J Res Int Educ. (2014) 13:30–45. doi: 10.1177/1475240914528084
66. Chi, MTH, and Wylie, R. “The ICAP Framework: Linking Cognitive Engagement to Active Learning Outcomes.” Educ Psychol (2014) 49:219–243.
67. Schullery, N, and Schullery, S. Are heterogeneous or homogeneous groups more beneficial to students? J Manag Educ. (2006) 30:542–56. doi: 10.1177/1052562905277305
68. Biggs, J. Enhancing teaching through constructive alignment. High Educ. (1996) 32:347–64. doi: 10.1007/BF00138871
69. Spencer, JA, and Jordan, RK. Learner centred approaches in medical education. BMJ. (1999) 318:1280–3. doi: 10.1136/bmj.318.7193.1280
70. Kassirer, JP. Teaching clinical reasoning: case-based and coached. Acad Med. (2010) 85:1118–24. doi: 10.1097/acm.0b013e3181d5dd0d
71. Ausubel, DP. A subsumption theory of meaningful verbal learning and retention. J Gen Psychol. (1962) 66:213–24. doi: 10.1080/00221309.1962.9711837
72. Imwattana, K, Dangprapai, Y, and Ngamskulrungroj, P. Active learning classes in a preclinical year may help improving some soft skills of medical students. Siriraj Med J. (2020) 72:415–23. doi: 10.33192/SMJ.2020.56
Keywords: critical thinking, clinical reasoning, skills, dispositions, medical education, systematic review
Citation: Araújo B, Gomes SF and Ribeiro L (2024) Critical thinking pedagogical practices in medical education: a systematic review. Front. Med. 11:1358444. doi: 10.3389/fmed.2024.1358444
Edited by:
Pedro Gil-Madrona, University of Castilla-La Mancha, SpainReviewed by:
Nataly Martini, The University of Auckland, New ZealandCopyright © 2024 Araújo, Gomes and Ribeiro. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Laura Ribeiro, bHJpYmVpcm9AbWVkLnVwLnB0
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.