
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Med. , 21 February 2024
Sec. Nephrology
Volume 11 - 2024 | https://doi.org/10.3389/fmed.2024.1342344
 Yiwei Shen1,2
Yiwei Shen1,2 Xinyu Su1,2Zanzhe Yu1,2Hao Yan1,2Dahua Ma3Yimei Xu3Jiangzi Yuan1,2Zhaohui Ni1,2Leyi Gu1,2
Xinyu Su1,2Zanzhe Yu1,2Hao Yan1,2Dahua Ma3Yimei Xu3Jiangzi Yuan1,2Zhaohui Ni1,2Leyi Gu1,2 Wei Fang1,2*
Wei Fang1,2*Background: Whether sarcopenic obesity had unfavorable effect on survival of peritoneal dialysis (PD) patients is unknown. We aimed to investigate the association between sarcopenic obesity and survival in PD patients.
Methods: This was a prospective observational study. Eligible PD patients from November 2016 to December 2017 were enrolled and followed until August 31, 2023. Sarcopenia was defined following the recommendations of the Asian Working Group for Sarcopenia (AWGS) as low appendicular skeletal muscle mass index (ASMI) and handgrip strength (HGS). Obesity was defined using the percentage of body fat (PBF). Survival analysis was conducted using the Kaplan–Meier and log-rank test. The Cox regression and the cumulative incidence competing risk (CICR) analyzes were used to investigate the association between sarcopenic obesity and all-cause mortality.
Results: A total of 223 patients were enrolled with 133 (59.6%) males, a median age of 57.5 (44.6, 65.7) years, a median dialysis vintage of 20.3 (6.4, 57.7) months and 48 (21.5%) who had comorbid diabetes mellitus. Among them, 46 (20.6%) patients were sarcopenic, and 25 (11.2%) patients were diagnosed with sarcopenic obesity. After followed up for 51.6 (25.6, 73.9) months, the Kaplan–Meier curve showed the sarcopenic obesity (log-rank = 13.527, p < 0.001) group had significant lower survival rate compared to the nonsarcopenic non-obesity group. For multivariate analysis, the CICR method showed patients with sarcopenic obesity had significantly higher mortality rate (HR: 2.190, 95% CI: 1.011–4.743, p = 0.047) compared to those with nonsarcopenic non-obesity.
Conclusion: Sarcopenia is not uncommon in PD patients, with a considerable proportion having sarcopenic obesity. There is a significant association between sarcopenic obesity and an increased risk of mortality in PD patients.
Peritoneal dialysis (PD), one of the major kidney replacement therapies, has shown survival advantage among patients with end-stage kidney disease (ESKD) (1, 2). The incidence of PD initiation has increased rapidly worldwide in the last 10 years (3, 4). Factors such as the use of bio-incompatible dialysis solutions, accumulation of uremic toxins, and chronic inflammation may contribute to protein-energy waste, which refers to a state of insufficient nutrient intake, depleted energy reserves, disruptions in body composition, and heightened muscle protein breakdown in patients with ESKD (5). Consequently, it can result in the loss of lean body mass in this patient population (6). Sarcopenia, characterized by muscle atrophy and impaired muscle function, is strongly associated with adverse clinical outcomes in dialysis patients, including worse quality of life, higher hospitalization rate and increased mortality (7, 8). Similar to the trend in the general population, obesity is increasingly common in patients receiving PD (9). It has been shown that the prevalence of obesity has increased substantially after PD initiation (10). Daily access to glucose-based dialysis solutions, insulin resistance, lipid metabolism disorders and reduced physical activity are risk factors that contribute to obesity in long-term PD treatment. The coexistence of sarcopenia and obesity, namely sarcopenic obesity, has garnered increasing attention due to its association with poorer survival in both general and elderly populations (11, 12). As PD patients are susceptible to develop both sarcopenia and obesity, the clinical outcomes of this cross-linked pathology are of great interest.
Only a few studies have investigated the clinical impact of sarcopenic obesity on dialysis patients’ outcomes, and the findings have been inconsistent. In a study by Malhotra et al. (13), sarcopenic obesity showed no statistically significant association with mortality in 122 patients undergoing hemodialysis (HD). Conversely, in a study by Sabatino et al., it was found that among 212 HD patients, the group with sarcopenic obesity exhibited worse survival in comparison to their counterparts with nonsarcopenic non-obesity (14). Given that PD patients are particularly susceptible to sarcopenic obesity, it is obviously of clinical importance to understand the association between sarcopenic obesity and patient outcomes. Therefore, this study was designed to investigate the association between sarcopenic obesity and survival in patients undergoing PD.
This was a prospective observational study undertaken in Renji Hospital, School of Medicine, Shanghai Jiao Tong University. The study was approved by the Ethics Committee of Renji Hospital (protocol code: [2016]101 K). Written informed consent was obtained from all recruited patients.
Stable patients receiving continuous ambulatory peritoneal dialysis (CAPD) between November 1, 2016 and December 31, 2017 were screened for eligibility. Patients were eligible if they were aged 18 to 80 years and treated on PD for at least three months. Exclusion criteria included: (1) amputations; (2) implantation of cardiac pacemakers and internal defibrillators; (3) concomitant with severe diseases such as active malignancy, severe cardiac diseases, etc.; (4) ongoing severe infection; (5) planned or ongoing pregnancy or lactation; (6) combined HD; (7) refusal to give a written consent. All enrolled patients received treatment with lactate-buffered glucose-based dialysis solutions (Dianeal®, Baxter) utilizing a twin-bag system. No additional solutions were administered alongside the glucose-based dialysis solutions.
Demographic data were collected at enrollment including age, gender, height, weight, dialysis vintage, blood pressure, etiology of ESKD and comorbidities. Age-adjusted Charlson comorbidity index (aCCI) scores were calculated (15). Body mass index (BMI) was calculated as weight divided by height squared. Cardiovascular disease (CVD) was defined as the presence of myocardial infarction, coronary artery bypass surgery, percutaneous coronary intervention, congestive heart failure, angina pectoris, cerebrovascular disease and peripheral vascular disease. Fasting venous blood was collected from each patient at enrollment for the measurement of laboratory data including hemoglobin, serum albumin, fasting blood glucose (FBG), glycated hemoglobin (HbA1c), total cholesterol, total triglyceride, low-density lipoprotein-cholesterol (LDL-c), high-density lipoprotein-cholesterol (HDL-c) and high sensitivity C-reactive protein (hsCRP). Standard peritoneal equilibration test was performed to calculate the 4-h dialysate-to-plasma concentration ratio for creatinine (D/Pcr) (16). Weekly total urea clearance (Kt/Vurea) and creatinine clearance (Ccr) were estimated using standard methods (17). Residual renal function (RRF) was evaluated as the average clearance of 24-h urinary urea and creatinine (18). Normalized protein catabolic rate (nPCR) was calculated and normalized to standard body weight (19). Daily glucose exposure to dialysate was assessed according to dialysis prescriptions.
At enrollment, body composition including extracellular water (ECW), intracellular water (ICW) and fat tissue mass (FTM) were measured using bioimpedance spectroscopy (BCM, Fresenius Medical Care, Germany) for each patient. The measurements were performed with patients in a supine position with 2 L dialysate dwell. The appendicular skeletal muscle mass index (ASMI) was calculated according to the regression models developed by using bioimpedance spectroscopy (20), as the sum of skeletal muscle mass of arms and legs divided by height squared. These regression models have been shown to strongly correlate with magnetic resonance imaging (MRI) measures of limb muscle mass. The equations for ASMI (arms) and ASMI (legs) were as following: ASMI (arms) = 1.69 + 0.301 × ICW (L) + 0.603 (male) + 0.0234 × weight (kg) – 0.123 × age (year), ASMI (legs) = 4.53 + 0.5005 × ICW (L) + 1.535 (male) + 0.0839 × weight (kg) – 0.0483 × age (year). Percentage of body fat (PBF) was calculated as the ratio of FTM and weight. Muscle strength, defined by handgrip strength (HGS), was measured using a digital dynamometer (CAMRY EH101, Guangdong, China). Patients were directed to perform three measurements using their dominant hand with maximum force, and the largest HGS was recorded.
Patients with low ASMI and low HGS were classified as sarcopenia. Low ASMI and low HGS were defined according to the recommendations of Asian Working Group for Sarcopenia (AWGS), as ASMI <7.0 kg/m2 for men and < 5.7 kg/m2 for women, and HGS < 26 kg for men and < 18 kg for women (21). Obesity was defined as PBF ≥ 25% for men and ≥ 35% for women (22). Therefore, our study population was divided into four groups based on muscle and fat status: non-sarcopenia and non-obesity (reference), nonsarcopenic obesity, nonobese sarcopenia, and sarcopenic obesity.
All enrolled participants were prospectively followed up from enrollment until death, transfer to permanent HD, kidney transplantation, loss to follow-up, transfer to other dialysis centers, or to the end of the study (August 31, 2023). The outcome measure in our study was patient survival.
Data normality was measured using Kolmogorov–Smirnov test. Continuous variables with normal distribution were presented as mean ± standard deviation and compared using One-Way ANOVA. Continuous variables with unnormal distribution were presented as median and interquartile range and compared using Kruskal-Wallis test. The Bonferroni or Tukey comparison post-hoc test was used in between-group comparisons. Categorical variables were presented as frequencies and percentages and compared using Chi-square test. Multivariate logistic regression analysis was run to explore the association between sarcopenia, sarcopenic obesity, and clinical and demographic variables. The Kaplan–Meier and log-rank test, and the Cox regression analysis were used to perform survival analysis. In addition, we used the cumulative incidence competing risk (CICR) analysis to mitigate the effect of competing events on survival. Analyzes were performed using IBM SPSS 22.0 for Windows software and R Statistical Software (v4.2.3). All statistical analysis used a significance level of 0.05 (2-sided).
As shown in Table 1, a total of 223 patients were enrolled, of whom 133 (59.6%) were males, with a median age of 57.5 (44.6, 65.7) years and a median dialysis vintage of 20.3 (6.4, 57.7) months. The prevalence of sarcopenia in the study cohort was 20.6%. Of them, 25 (11.2%) patients met the criteria for sarcopenic obesity. Sarcopenic patients were older, with higher aCCI scores and FBG, lower HGS and ASMI than nonsarcopenic patients (all p < 0.05). When compared to the reference group, the sarcopenic obesity group had higher BMI, PBF, ECW/ICW, hsCRP, HbA1c, and lower blood pressure, HDL-c and Ccr (all p < 0.05). With comparison to the nonobese sarcopenia group, the sarcopenic obesity group had higher BMI, PBF, ECW/ICW, hsCRP, and lower HDL-c, Kt/Vurea, Ccr (all p < 0.05). No significant difference was observed in the dialysis vintage, proportion of diabetes mellitus, serum albumin, glucose exposure and RRF (all p > 0.05) across the four subgroups.
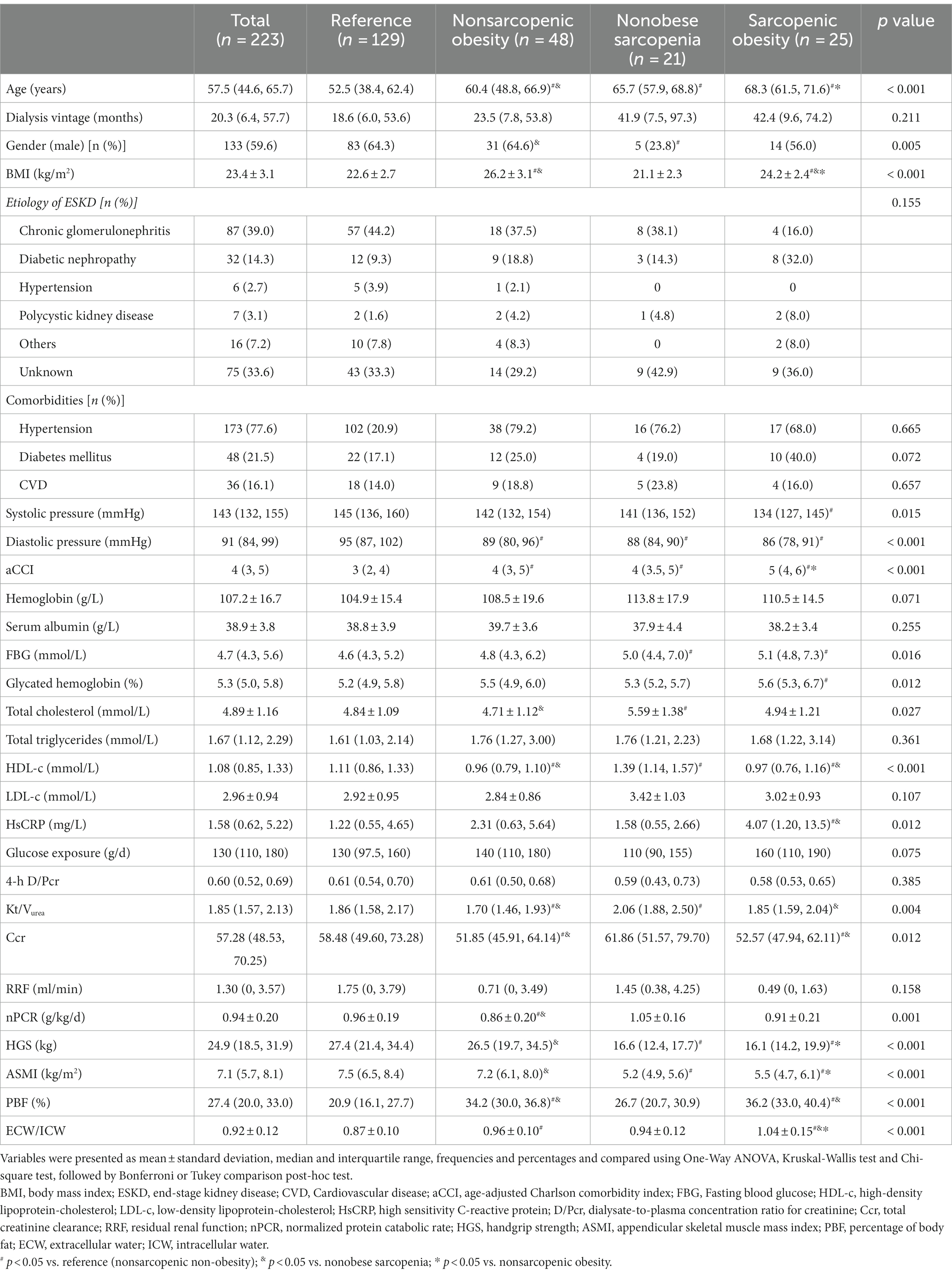
Table 1. Patient characteristics according to the groups based on muscle and fat status.
Age (OR = 1.145, 95% CI: 1.083–1.210, p < 0.001), ECW/ICW (OR = 1.091, 95% CI: 1.035–1.150, p = 0.001) and BMI (OR = 0.701, 95% CI: 0.585–0.839, p < 0.001) were significantly associated with sarcopenia after adjustment for gender, dialysis vintage, glucose exposure, serum albumin, total cholesterol, hsCRP, Kt/Vurea, RRF and diabetes mellitus. Age (OR = 1.096, 95% CI: 1.033–1.162, p = 0.002) and ECW/ICW (OR = 1.101, 95% CI: 1.040–1.166, p = 0.001) were significantly associated with sarcopenic obesity when adjusting for gender, dialysis vintage, glucose exposure, serum albumin, total cholesterol, hsCRP, Kt/Vurea, RRF and diabetes mellitus (Table 2).
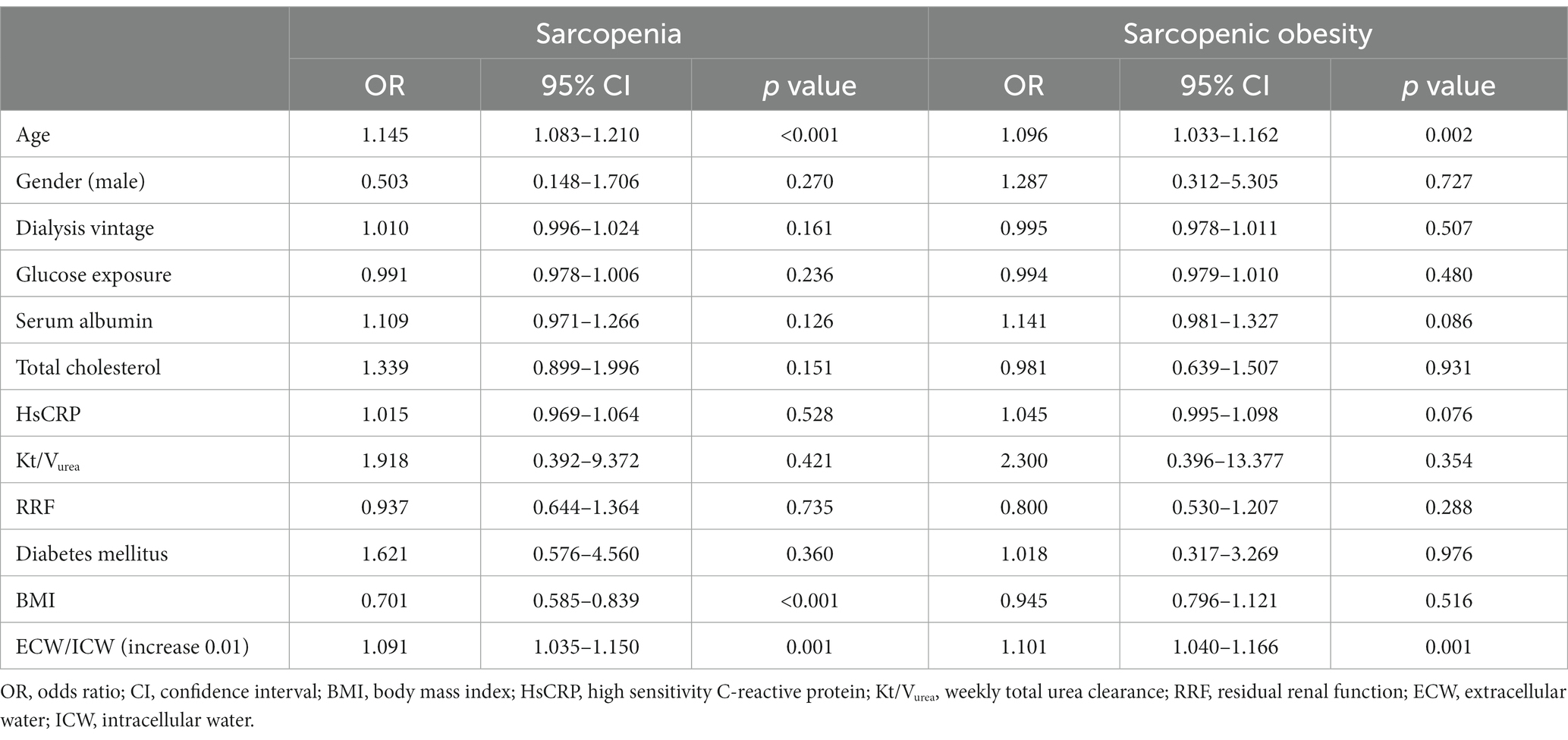
Table 2. Multivariate logistic regression of the association between sarcopenia, sarcopenic obesity and clinical and demographic variables.
As shown in Table 3, after followed up for 51.6 (25.6, 73.9) months, 60 (26.9%) patients died, 59 (26.5%) patients transferred to permanent HD, 18 (8.1%) patients underwent kidney transplantation, 8 (3.6%) patients transferred to other centers, 3 (1.3%) patients were lost to follow-up, and 75 (33.6%) patients were still on PD. The leading cause of death was cardiovascular events for 38 (63.3%) patients. No significant difference was found in the distribution of outcomes among four subgroups.
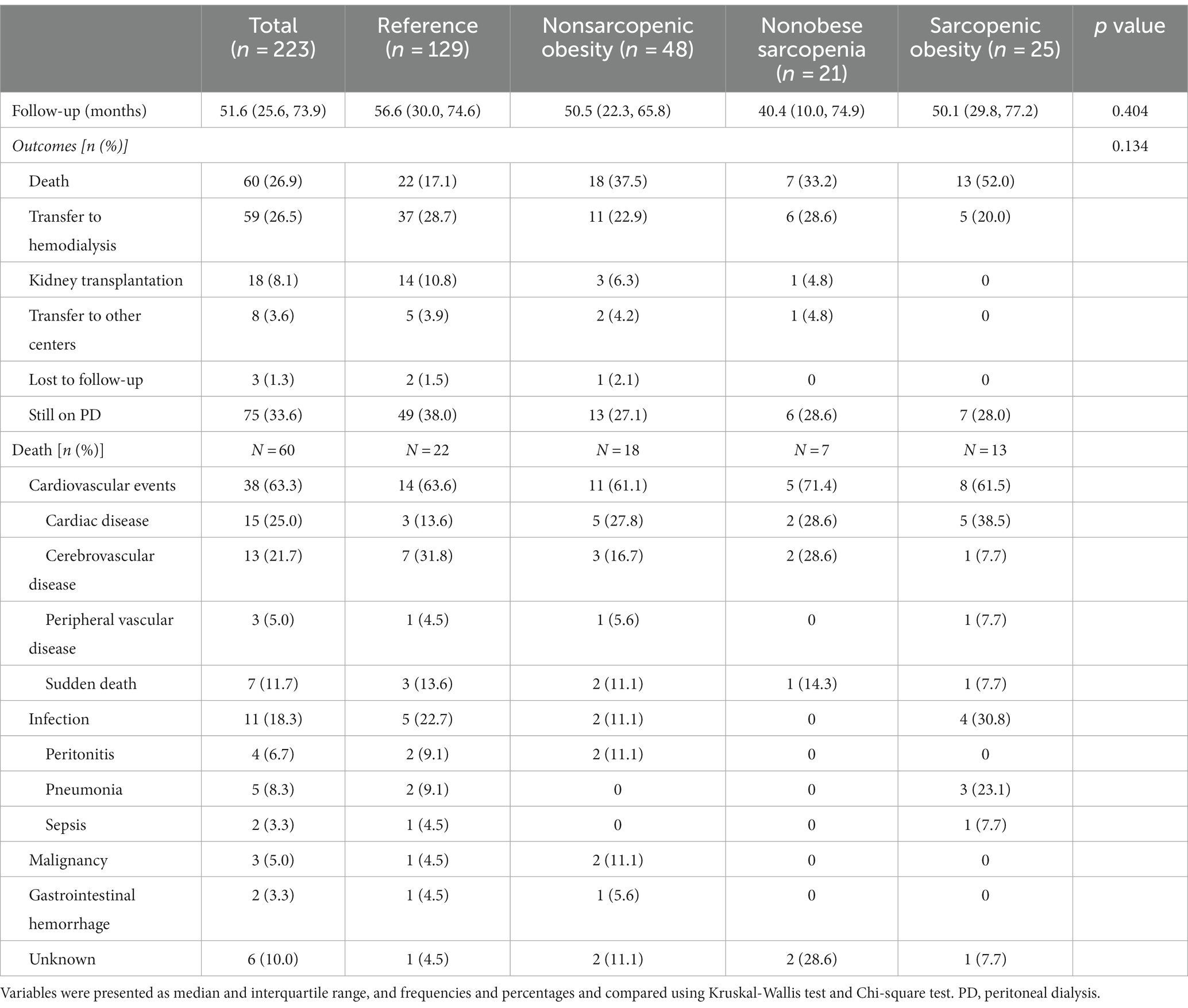
Table 3. Outcomes of patients.
As shown in Figure 1, the sarcopenic obesity (log-rank = 13.527, p < 0.001) and the nonobese sarcopenia groups (log-rank = 4.830, p = 0.028) had significantly inferior survival in comparison to the reference group. Among the patients with sarcopenia, no significant difference was found in survival between the sarcopenic obesity group and the nonobese sarcopenia group (log-rank = 0.310, p = 0.578).
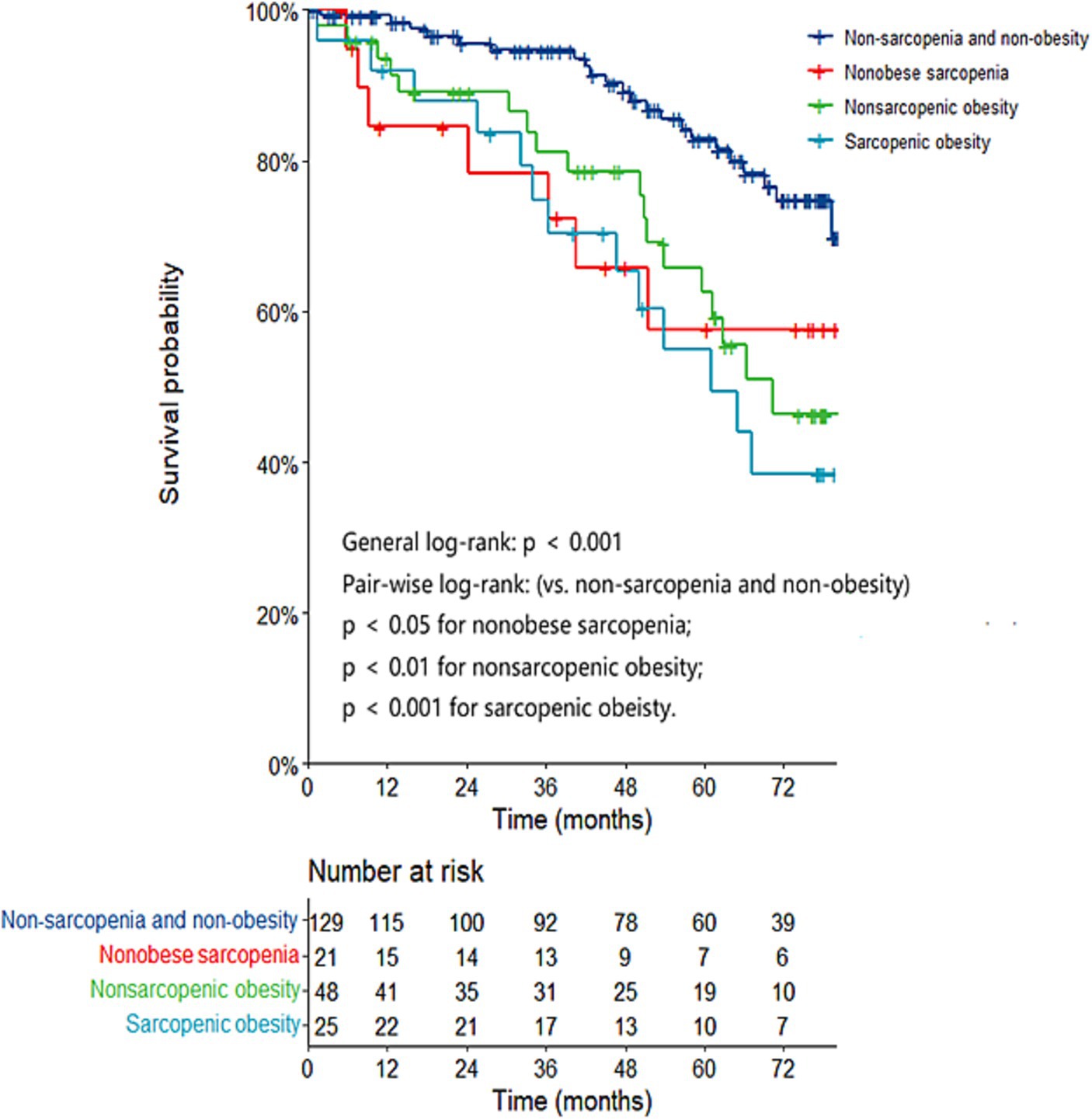
Figure 1. Kaplan–Meier curves based on muscle and fat status for patient survival.
In the multivariate Cox regression analysis, the nonobese sarcopenia (p = 0.191) and the sarcopenic obesity groups (p = 0.139) were no longer associated with all-cause mortality compared to the reference group when adjusting for gender, dialysis vintage, serum albumin, total cholesterol, hsCRP and aCCI. However, when the CICR model was used to mitigate the effect of censored events, the sarcopenic obesity group was independently associated with increased all-cause mortality compared to the reference group (HR: 2.190, 95% CI: 1.011–4.743, p = 0.047) (Table 4).
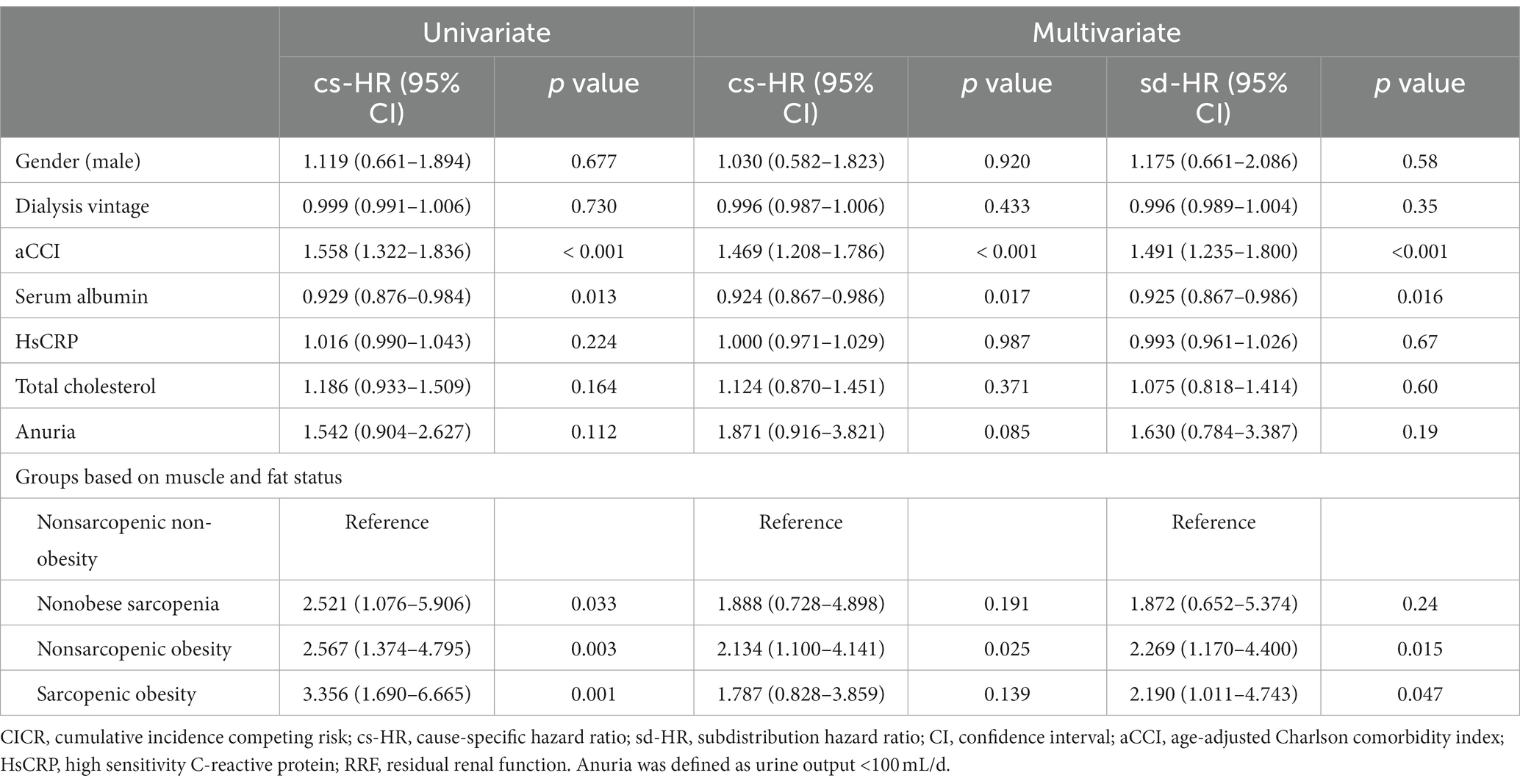
Table 4. Multivariate Cox regression and CICR analyzes for all-cause mortality according to groups based on muscle and fat status.
The present study showed that sarcopenia was not uncommon in PD patients, with a significant proportion of them having sarcopenic obesity. The group with sarcopenic obesity was independently associated with increased mortality in PD patients compared to the nonsarcopenic nonobese group. However, among patients with sarcopenia, there was no significant difference in survival between patients with nonobese sarcopenia and sarcopenic obesity.
The prevalence of sarcopenia and sarcopenic obesity in ESKD patients varies significantly depending on the diagnostic criteria, assessment tools and cut-off values used. Previous studies showed that the prevalence of sarcopenia and sarcopenic obesity in patients on PD ranging from 4 to 38.2%, and from 3 to 8.6%, respectively (23–27). Similarly, a prevalence of 20.6% for sarcopenia and 11.2% for sarcopenic obesity was reported in our study cohort. These findings suggested that sarcopenia and sarcopenic obesity were not uncommon in PD patients.
In the present study, we observed a significant association between sarcopenic obesity and advanced age, as well as higher ECW/ICW ratios. Age is widely recognized as an important risk factor for sarcopenic obesity in the general population (28). Elderly PD patients are particularly vulnerable to sarcopenia due to factors such as uremic toxins, dialysis treatment and dietary restrictions. They also tend to gain fat more easily due to exposure to glucose-based dialysis solutions and reduced physical activities. Consistent with our findings, Sabatino et al. conducted a retrospective study involving 212 HD patients and found age was independently associated with sarcopenic obesity (OR = 1.17, 95% CI: 1.09–1.25, p < 0.001). Therefore, it is crucial to pay close attention to the evaluation of sarcopenic obesity in elderly individuals undergoing dialysis. It has been indicated that there might be a strong association between volume status and nutritional status (29). Recent studies have suggested that the ECW/ICW ratio may be a more sensitive indicator of changes in muscle properties than muscle mass alone (30). While the exact mechanism underlying the interaction between volume overload and sarcopenic obesity in ESKD patients is not yet fully understood, it is speculated that chronic inflammation resulting from excessive fluid (31) might contribute to both the rise in ECW/ICW ratios and the development of sarcopenic obesity. In general, these findings suggested that sarcopenic obesity was more likely to occur in patients who were older and experiencing volume overload.
Regarding patient survival, we found that the sarcopenic obesity group had poorer survival than that with nonsarcopenic non-obesity. Several retrospective studies have consistently reported a strong association between sarcopenic obesity and an elevated risk of mortality among PD patients. Do and Kang (32) retrospectively evaluated the association between sarcopenia or its components, obesity and patient survival by analyzing the body composition of 199 incident PD patients. After 18 months of follow-up, they reported that the survival rate of patients with nonsarcopenic non-obesity, nonobese sarcopenia, and sarcopenic obesity were 97.5, 83.5, and 70.1%, respectively. Furthermore, patients with sarcopenic obesity had significantly lower survival rate compared to those with nonsarcopenic non-obesity. Another study conducted in Italy, which utilized abdominal computed tomography to diagnose sarcopenia and obesity in 212 HD patients, reported that the group with sarcopenic obesity exhibited inferior survival in comparison to the group with nonsarcopenic non-obesity (14). The present prospective study showed that sarcopenic obesity served as an independent predictor for higher mortality rate in PD patients, which was in accordance with previous studies.
Obesity is known to be an important risk factor for cardiovascular disease and increased mortality in the general population (33). However, there is evidence of a reverse epidemiology phenomenon referred to as the “obesity paradox” in ESKD patients, wherein patients with obesity may experience improved clinical outcomes (34). In a study conducted in a 2-year cohort of 54,535 HD patients in the United States, obesity was described to be associated with reduced cardiovascular mortality significantly (35). Moreover, another study enrolled 261 HD patients reported better quality of life and lower risk of all-cause mortality and cardiovascular risk in patients with sarcopenic obesity compared to those with nonobese sarcopenia (36). However, our study did not identify a survival advantage in the sarcopenic obesity group compared to the nonobese sarcopenia group, which aligned with the findings of studies conducted by Do and Kang (32) as well as Sabatino (14). Possible explanations for the varying results could be attributed to the different dialysis modalities, longer dialysis vintage, extended follow-up period and better nutritional status in our cohort. Body fat is thought to have positive effect on nutrition in the short term by serving as source of energy (34, 37). But excess body fat is known to be strongly associated with inflammation (38), which may have an adverse effect on survival in the long term, as supported by our finding that the sarcopenic obesity patients had higher hsCRP levels. Taken together, the reverse epidemiology phenomenon of obesity may be not present in patients on PD with a long dialysis vintage and favorable nutritional status.
Our study has several limitations. Firstly, due to the single-center design, the results might not be extrapolated to patients in other populations. Secondly, we did not conduct longitudinal monitoring of patients’ muscle and adipose tissue, thus limiting our understanding of the association between patient outcomes and changes in muscle and fat status. Thirdly, patients older than 80 were excluded in the present study, who may exhibit a higher prevalence of sarcopenic obesity. Fourthly, we lacked information regarding patient daily activity and personal habits such as smoking and alcohol consumption, which are known to be associated closely with patients’ outcomes. Fifthly, we did not document new onset hypertension, diabetes mellitus, and dyslipidemia during the 6-year follow-up, despite their potential impact on patient prognosis. Sixthly, the muscle and fat values obtained from bioimpedance analysis were not compared with those from other body composition assessment tools, such as muscle and fat ultrasound. The application of ultrasound technique has been reported to offer reliable and valid measurements of muscle and fat mass, and their parameters have shown significant correlation with the results of bioimpedance analysis (39, 40). Clearly, multicenter studies with better design and larger sample size are needed to confirm our results.
In summary, our results showed that sarcopenia, and in particular sarcopenic obesity, was not uncommon in PD patients. Sarcopenic obesity was significantly associated with increased mortality risk in PD patients. Therefore, we suggest attention should be directed towards this interconnected pathology, rather than solely focusing on alterations in muscle or adipose tissue.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
The studies involving humans were approved by Ethics Committee of Renji Hospital, School of Medicine, Shanghai Jiao Tong University, Shanghai, China. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
YS: Conceptualization, Formal analysis, Investigation, Writing – original draft, Writing – review & editing, Visualization. XS: Investigation, Writing – original draft. ZY: Investigation, Writing – original draft. HY: Investigation, Writing – original draft. DM: Investigation, Writing – original draft. YX: Investigation, Writing – original draft. JY: Writing – review & editing. ZN: Writing – review & editing. WF: Funding acquisition, Investigation, Project administration, Resources, Supervision, Writing – review & editing, Conceptualization, Writing – original draft, Visualization, Validation. LG: Resources, Visualization, Validation, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work was supported by the National Nature Science Foundation Grant of China (81370864, 81670691) and Shanghai Municipal Education Commission-Gaofeng Clinical Medicine Grant (20152211).
We thank all the staff at the Nephrology Department of Renji Hospital in Shanghai, China for their work.
DM and YX were employed by Jiangsu Hengrui Pharmaceuticals Co., Ltd., Shanghai, China.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Vonesh, EF, Snyder, JJ, Foley, RN, and Collins, AJ. Mortality studies comparing peritoneal dialysis and hemodialysis: what do they tell us? Kidney Int Suppl. (2006) 103:S3–S11. doi: 10.1038/sj.ki.5001910
2. Wong, B, Ravani, P, Oliver, MJ, Holroyd-Leduc, J, Venturato, L, Garg, AX, et al. Comparison of patient survival between hemodialysis and peritoneal Dialysis among patients eligible for both modalities. Am J Kidney Dis. (2018) 71:344–51. doi: 10.1053/j.ajkd.2017.08.028
3. Li, PK, Chow, KM, Van de Luijtgaarden, MW, Johnson, DW, Jager, KJ, Mehrotra, R, et al. Changes in the worldwide epidemiology of peritoneal dialysis. Nat Rev Nephrol. (2017) 13:90–103. doi: 10.1038/nrneph.2016.181
4. Teitelbaum, I, and Finkelstein, FO. Why are we not getting more patients onto peritoneal Dialysis? Observations from the United States with global implications. Kidney Int Rep. (2023) 8:1917–23. doi: 10.1016/j.ekir.2023.07.012
5. Kalantar-Zadeh, K, Ikizler, TA, Block, G, Avram, MM, and Kopple, JD. Malnutrition-inflammation complex syndrome in dialysis patients: causes and consequences. Am J Kidney Dis. (2003) 42:864–81. doi: 10.1016/j.ajkd.2003.07.016
6. Han, SH, and Han, DS. Nutrition in patients on peritoneal dialysis. Nat Rev Nephrol. (2012) 8:163–75. doi: 10.1038/nrneph.2012.12
7. Hara, H, Nakamura, Y, Hatano, M, Iwashita, T, Shimizu, T, Ogawa, T, et al. Protein energy wasting and sarcopenia in Dialysis patients. Contrib Nephrol. (2018) 196:243–9. doi: 10.1159/000485729
8. Wathanavasin, W, Banjongjit, A, Avihingsanon, Y, Praditpornsilpa, K, Tungsanga, K, Eiam-Ong, S, et al. Prevalence of sarcopenia and its impact on cardiovascular events and mortality among Dialysis patients: a systematic review and Meta-analysis. Nutrients. (2022) 14:4077. doi: 10.3390/nu14194077
9. Ng, JK, Than, WH, and Szeto, CC. Obesity, weight gain, and fluid overload in peritoneal Dialysis. Front Nephrol. (2022) 2:880097. doi: 10.3389/fneph.2022.880097
10. Than, WH, Ng, JK, Chan, GC, Fung, WW, Chow, KM, and Szeto, CC. The change in the prevalence of obesity and new-onset diabetes in Chinese peritoneal dialysis patients over 25 years. Clin Kidney J. (2022) 15:70–8. doi: 10.1093/ckj/sfab139
11. Baumgartner, RN, Wayne, SJ, Waters, DL, Janssen, I, Gallagher, D, and Morley, JE. Sarcopenic obesity predicts instrumental activities of daily living disability in the elderly. Obes Res. (2004) 12:1995–2004. doi: 10.1038/oby.2004.250
12. Janssen, I, Heymsfield, SB, and Ross, R. Low relative skeletal muscle mass (sarcopenia) in older persons is associated with functional impairment and physical disability. J Am Geriatr Soc. (2002) 50:889–96. doi: 10.1046/j.1532-5415.2002.50216.x
13. Malhotra, R, Deger, SM, Salat, H, Bian, A, Stewart, TG, Booker, C, et al. Sarcopenic obesity definitions by body composition and mortality in the hemodialysis patients. J Ren Nutr. (2017) 27:84–90. doi: 10.1053/j.jrn.2016.09.010
14. Sabatino, A, Avesani, CM, Regolisti, G, Adinolfi, M, Benigno, G, Delsante, M, et al. Sarcopenic obesity and its relation with muscle quality and mortality in patients on chronic hemodialysis. Clin Nutr. (2023) 42:1359–68. doi: 10.1016/j.clnu.2023.06.032
15. Koppie, TM, Serio, AM, Vickers, AJ, Vora, K, Dalbagni, G, Donat, SM, et al. Age-adjusted Charlson comorbidity score is associated with treatment decisions and clinical outcomes for patients undergoing radical cystectomy for bladder cancer. Cancer. (2008) 112:2384–92. doi: 10.1002/cncr.23462
16. Twardowski, ZJ. Clinical value of standardized equilibration tests in CAPD patients. Blood Purif. (1989) 7:95–108. doi: 10.1159/000169582
17. Nolph, KD, Moore, HL, Twardowski, ZJ, Khanna, R, Prowant, B, Meyer, M, et al. Cross-sectional assessment of weekly urea and creatinine clearances in patients on continuous ambulatory peritoneal dialysis. ASAIO J. (1992) 38:M139–42. doi: 10.1097/00002480-199207000-00004
18. van Olden, RW, Krediet, RT, Struijk, DG, and Arisz, L. Measurement of residual renal function in patients treated with continuous ambulatory peritoneal dialysis. J Am Soc Nephrol. (1996) 7:745–50. doi: 10.1681/asn.V75745
19. Randerson, DH, Chapman, GV, and Farrell, PC. Amino acid and dietary status in CAPD patients In: RC Atkins, PC Farrell, and N Thomson, editors. Peritoneal dialysis. Edinburgh: Churchill-Livingstone (1981). 180–91.
20. Kaysen, GA, Zhu, F, Sarkar, S, Heymsfield, SB, Wong, J, Kaitwatcharachai, C, et al. Estimation of total-body and limb muscle mass in hemodialysis patients by using multifrequency bioimpedance spectroscopy. Am J Clin Nutr. (2005) 82:988–95. doi: 10.1093/ajcn/82.5.988
21. Chen, LK, Liu, LK, Woo, J, Assantachai, P, Auyeung, TW, Bahyah, KS, et al. Sarcopenia in Asia: consensus report of the Asian working Group for Sarcopenia. J Am Med Dir Assoc. (2014) 15:95–101. doi: 10.1016/j.jamda.2013.11.025
22. Gracia-Iguacel, C, Qureshi, AR, Avesani, CM, Heimbürger, O, Huang, X, Lindholm, B, et al. Subclinical versus overt obesity in dialysis patients: more than meets the eye. Nephrol Dial Transplant. (2013) 28:iv175–81. doi: 10.1093/ndt/gft024
23. Wu, J, Guan, J, Lin, S, Wu, X, Ding, M, Ren, Z, et al. Prediction of sarcopenia among peritoneal dialysis patients using a combination of irisin and phase angle. Nephrol Ther. (2023) 19:66–75. doi: 10.1684/ndt.2023.7
24. Abro, A, Delicata, LA, Vongsanim, S, and Davenport, A. Differences in the prevalence of sarcopenia in peritoneal dialysis patients using hand grip strength and appendicular lean mass: depends upon guideline definitions. Eur J Clin Nutr. (2018) 72:993–9. doi: 10.1038/s41430-018-0238-3
25. da Silva, MZC, Vogt, BP, Reis, N, and Caramori, JCT. Update of the European consensus on sarcopenia: what has changed in diagnosis and prevalence in peritoneal dialysis? Eur J Clin Nutr. (2019) 73:1209–11. doi: 10.1038/s41430-019-0468-z
26. Lin, YL, Wang, CH, Tsai, JP, Chen, CT, Chen, YH, Hung, SC, et al. A comparison of SARC-F, calf circumference, and their combination for sarcopenia screening among patients undergoing peritoneal Dialysis. Nutrients. (2022) 14:923. doi: 10.3390/nu14050923
27. Yoowannakul, S, Tangvoraphonkchai, K, and Davenport, A. The prevalence of muscle wasting (sarcopenia) in peritoneal dialysis patients varies with ethnicity due to differences in muscle mass measured by bioimpedance. Eur J Clin Nutr. (2018) 72:381–7. doi: 10.1038/s41430-017-0033-6
28. Lombardo, M, Boaria, A, Aulisa, G, Padua, E, Annino, G, Pratesi, A, et al. Sarcopenic obesity: etiology and lifestyle therapy. Eur Rev Med Pharmacol Sci. (2019) 23:7152–62. doi: 10.26355/eurrev_201908_18761
29. Cheng, LT, Tang, W, and Wang, T. Strong association between volume status and nutritional status in peritoneal dialysis patients. Am J Kidney Dis. (2005) 45:891–902. doi: 10.1053/j.ajkd.2005.01.037
30. Tanaka, H, Kitamura, G, Nankaku, M, Taniguchi, M, Shide, K, Fujita, M, et al. Association of Physical Activity and Nutritional Intake with muscle quantity and quality changes in acute stroke patients. J Stroke Cerebrovasc Dis. (2022) 31:106442. doi: 10.1016/j.jstrokecerebrovasdis.2022.106442
31. Dekker, MJ, Marcelli, D, Canaud, BJ, Carioni, P, Wang, Y, Grassmann, A, et al. Impact of fluid status and inflammation and their interaction on survival: a study in an international hemodialysis patient cohort. Kidney Int. (2017) 91:1214–23. doi: 10.1016/j.kint.2016.12.008
32. Do, JY, and Kang, SH. Association between low handgrip strength and obesity with mortality in peritoneal dialysis patients. Sci Rep. (2023) 13:1852. doi: 10.1038/s41598-023-28708-8
33. Atkins, JL, and Wannamathee, SG. Sarcopenic obesity in ageing: cardiovascular outcomes and mortality. Br J Nutr. (2020) 124:1102–13. doi: 10.1017/s0007114520002172
34. Park, J, Ahmadi, SF, Streja, E, Molnar, MZ, Flegal, KM, Gillen, D, et al. Obesity paradox in end-stage kidney disease patients. Prog Cardiovasc Dis. (2014) 56:415–25. doi: 10.1016/j.pcad.2013.10.005
35. Kalantar-Zadeh, K, Kopple, JD, Kilpatrick, RD, McAllister, CJ, Shinaberger, CS, Gjertson, DW, et al. Association of morbid obesity and weight change over time with cardiovascular survival in hemodialysis population. Am J Kidney Dis. (2005) 46:489–500. doi: 10.1053/j.ajkd.2005.05.020
36. Beberashvili, I, Azar, A, Khatib, A, Abu Hamad, R, Neheman, A, Efrati, S, et al. Sarcopenic obesity versus nonobese sarcopenia in hemodialysis patients: differences in nutritional status, quality of life, and clinical outcomes. J Ren Nutr. (2023) 33:147–56. doi: 10.1053/j.jrn.2022.05.003
37. Park, J. Kidney disease and obesity paradox. Kidney Res Clin Pract. (2017) 36:1–2. doi: 10.23876/j.krcp.2017.36.1.1
38. Kalantar-Zadeh, K, Kuwae, N, Wu, DY, Shantouf, RS, Fouque, D, Anker, SD, et al. Associations of body fat and its changes over time with quality of life and prospective mortality in hemodialysis patients. Am J Clin Nutr. (2006) 83:202–10. doi: 10.1093/ajcn/83.2.202
39. Battaglia, Y, Ullo, I, Massarenti, S, Esposito, P, Prencipe, M, Ciancio, G, et al. Ultrasonography of quadriceps Femoris muscle and subcutaneous fat tissue and body composition by BIVA in chronic Dialysis patients. Nutrients. (2020) 12:1388. doi: 10.3390/nu12051388
40. Sabatino, A, Regolisti, G, Delsante, M, Di Motta, T, Cantarelli, C, Pioli, S, et al. Noninvasive evaluation of muscle mass by ultrasonography of quadriceps femoris muscle in end-stage renal disease patients on hemodialysis. Clin Nutr. (2019) 38:1232–9. doi: 10.1016/j.clnu.2018.05.004
Keywords: sarcopenic obesity, sarcopenia, prevalence, survival, peritoneal dialysis
Citation: Shen Y, Su X, Yu Z, Yan H, Ma D, Xu Y, Yuan J, Ni Z, Gu L and Fang W (2024) Association between sarcopenic obesity and mortality in patients on peritoneal dialysis: a prospective cohort study. Front. Med. 11:1342344. doi: 10.3389/fmed.2024.1342344
Edited by:
Sree Bhushan Raju, Nizam's Institute of Medical Sciences, IndiaReviewed by:
Yuri Battaglia, University of Verona, ItalyCopyright © 2024 Shen, Su, Yu, Yan, Ma, Xu, Yuan, Ni, Gu and Fang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Wei Fang, ZmFuZ3dlaV9zaEAxMjYuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.