 Gabriela Fernández Castillo
Gabriela Fernández Castillo Maha Khalid
Maha Khalid Eduardo Salas
Eduardo Salas- Making Effective Teams Laboratory, Department of Psychological Science, Rice University, Houston, TX, United States
1 Introduction
In 2018, Salas et al. (1) offered 10 observations on the science of teams in healthcare. This perspective article offers a quick update, providing a new set of observations based on the latest findings. As a point-of-departure for these observations, we use one of medicine's most cited culprits of error: communication [see Table 1 for a complete list of articles discussing communication; see also Etherington et al. (2), Street et al. (3), Tiwary et al. (4)]—and our belief that while important, a sole focus on it fails to take a holistic approach.

Table 1. Articles included in the review of the literature.
Upon surveying recent literature (i.e., 2018–2023), we found that 89% of articles discuss communication in some way, and 28% mention communication as one of the leading causes of medical error (5–8). However, in the following piece, our stance is that despite communication having been repeatedly cited as “the” medical culprit, it may not be the source of all contention (9). More recent findings identify other challenges, such as accountability (10), conflict management (11, 12), decision-making (13), reflecting on progress, and coaching as the primary challenges healthcare teams face (14). Moreover, communication is a multi-faceted competency that also requires a holistic view.
In our review, it was clear that research on interprofessional collaboration was alive and well (around 48% of articles fit in this general category; see Table 1). However, more specific areas of research on interdisciplinary collaboration emerged, pointing to four primary areas of development: interprofessional education (24%), team development interventions [TDIs, see Lacarenza et al. (15); 20%], simulation-based training (SBT; 8%), and lastly, measurement (8%). Together, these areas point to a growing attention on the team as a whole—rather than on a single competency (i.e., communication). Guided by the findings from Table 1 and other extant developments, we provide an update on the observations made by Salas et al. (1). Doing so highlights what the last 5 years have taught us.
In the following subsections, we discuss how these observations can continue to transform healthcare teams for the better and how they all work together to foster teamwork throughout healthcare practitioners' workplace lifespans. Figure 1 summarizes this update.
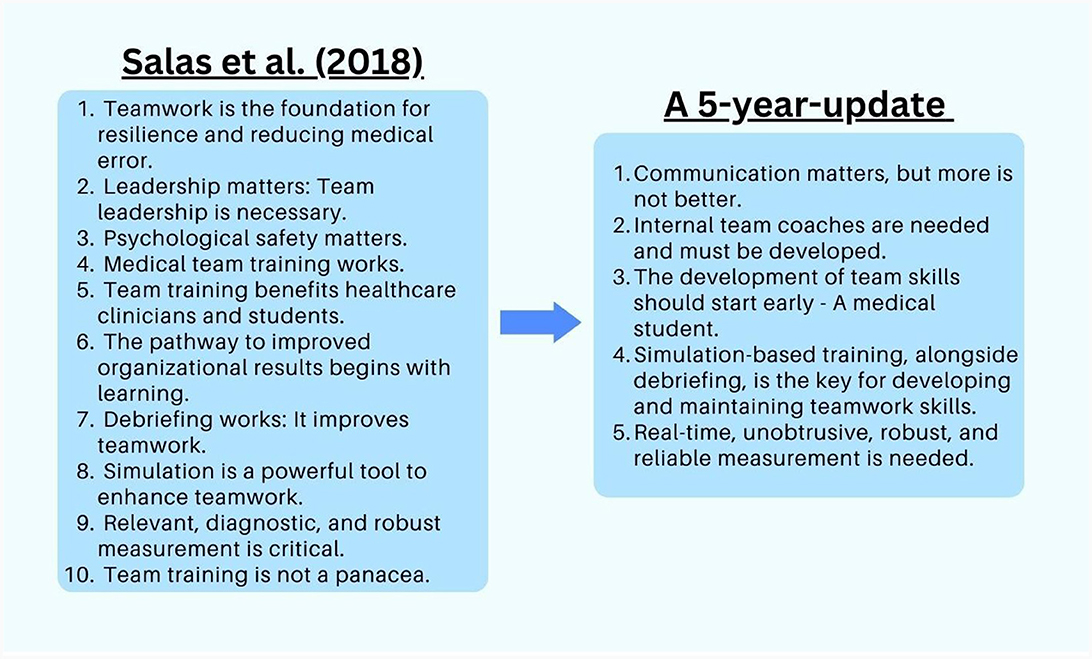
Figure 1. Holistic teamwork strategies.
2 Observation 1: communication matters, but more is not always better
A plethora of teamwork competency frameworks exist. However, team scientists widely recognize that for teams to function effectively, they need to communicate [see Bollen et al. (16), who found communication is the most commonly reported influencing factor of collaboration]. Nevertheless, simply communicating is not enough, as meta-analytic evidence has shown that more is not better: better is better (17). In other words, the quantity of communication may not rectify teamwork issues. Quality is more indicative of better performance (17), and to have communication quality, teams need to ensure they have four things. Teams need to share unique information (such as a critical detail of a patient's history), have closed-loop communications (initiating, following up, and closing conversations), convey information when received (i.e., “I understand I need to be here in person for the meeting”), and make sure boundary spanners exist to communicate with individuals outside of the team (18). Understanding communication as simply sending information is an incomplete picture—and, as is now widely recognized, many environments are not conducive to it at first.
One of the most pivotal factors in ensuring communication quality is psychological safety—loosely defined as the ability to take intrapersonal risks [(19, 20); also see Keller at al. (12) and Luo et al. (21)]. In order to foster psychological safety and enable teams to speak up when necessary [a problem consistent in healthcare—where medical hierarchies persist, see Neuhaus et al. (22) and Seaton et al. (23)], teams need to engage in a variety of behaviors—involving specific implicit and explicit actions from clarifying expectations to promoting inclusivity [for a complete list of behaviors, see Kolbe et al. (24)]. Moreover, research has shown that healthcare teams must adapt, listen, and speak up properly and definitively amongst their colleagues and collaborators (25).
Therefore, not only is communication multi-faceted, but it is also one of multiple team competencies. For this reason, we argue that if healthcare professionals require all these skills, it is worth investing in strategies that target most teamwork competencies at once and let go of the idea that communication is a sole perpetrator of medical mistakes. This is not to say communication is unimportant, but simply that it is a piece of a larger puzzle. If an improvement in communication is not complemented by other teamwork competencies, teamwork as a whole is not likely to improve. In other words, good communication does not directly translate into good teamwork, and a more holistic approach is necessary.
3 Observation 2: internal team coaches are needed and must be developed
Team development interventions (TDIs) are designed with distinct purposes in mind. For example, there are training and process approaches that are necessary on different occasions (15). From our literature review, it became evident that there is a growing interest in testing and developing distinct types of TDIs in everything from leadership training (26) to process interventions (27). However, in the entirety of our review, only one article (27) touched upon what we thought to be a holistic TDI fitted to healthcare's immediate leadership needs: team coaching. Using extant supporting research, we provide rationale for its strength as an intervention and call attention to it as a great tool in nurturing teams in their lifespan.
Salas et al.'s (1) review [and more recently, Vatnøy et al. (28)] corroborated the importance of team leadership—which, as many have found (29), can help members coordinate their collective resources in accomplishing the team's work (27, 30). Furthermore, as the team coaching literature has evolved, it has been mostly conceptualized as a leadership strategy that both internal and external coaches can provide (31). Körner et al. (27) systematically developed a team coaching approach with the goal of leaving behind a team leader empowered enough to coach their teams. More recent advancements made by Maynard et al. (29) suggest that for healthcare, a profession with high power distance and a high degree of technical skills, internal coaches might be more successful in yielding improvements in team performance. This is because internal team coaches are experts in their field who understand immediate teamwork needs (31), allowing them to adapt with the team during times of need.
Körner et al.'s (27) team coaching approach and Maynard et al.'s (29) empirical study provided the primary advancements made in the last 5 years in team coaching in healthcare. Maynard and colleagues had a retired surgeon coach current surgeons, and these surgeons proceeded to utilize coaching skills on their surgical teams [Körner et al. (27) had a professional coach aid healthcare teams]. The results indicated that teams that underwent the intervention showed better surgical outcomes over those that did not (29). However, team coaching is supported by literature compromising the last 5 years and beyond, with fields like technology showing great potential in nurturing a team's overall health rather than a single aspect [e.g., Liu et al. (32); also see Fernández Castillo and Salas (33)]. Team coaching offers a powerful avenue to foster teamwork because it can tackle multiple teamwork competencies simultaneously (29, 33). We know that it can do three specific things (33): increase group effort (27, 32, 34), better interpersonal processes via improvements in psychological safety (19, 35), and lastly, increase team knowledge and learning (27, 36). By improving these things, general teamwork is improved. For example, if a team is failing because of a lack of information sharing (a facet of quality communication), improvements in group effort where people are encouraged to share can address this issue [see Körner et al. (27), who approach this issue via goal attainment]. Suppose a team is failing because people have information but do not feel safe speaking up. In that case, team coaching can alleviate this by creating a climate for safety where the internal leader establishes norms of respect regardless of medicinal hierarchies (33). We seek to highlight the fact that rather than focusing on communication or any other single teamwork competency, team coaching seeks to nurture team wellbeing as a whole and over time—leaving behind team leaders who can guide their teams without external intervention (27). Moreover, if implemented as more than a one-time intervention over the lifespan of healthcare practitioners' professional development, we could see other benefits, such as improving teamwork outcomes stemming from teaching leadership competencies in healthcare curricula (37). For this reason, we believe team coaching should be the avenue to fostering healthcare leaders, as by doing so, we simultaneously create a climate where teamwork is valued and fostered and where team members learn to communicate and beyond. We hope the next 5 years invest in team coaching as a TDI for leadership training, as gaps in the field (such as a lack of research with ad-hoc teams) are prominent and fruitful avenues of research.
4 Observation 3: the development of team skills should start early—A medical student
As observed in Figure 1, Salas et al. (1) offered the observations that team training works, benefits healthcare students and clinicians, and organizational results begin with learning. They noted that future research needed to focus on training sustainment and emerging teamwork modalities. This is more important than ever before, with some arguing that healthcare curricula as they stand today do not provide students with the competencies they need to be successful team players in the workplace (9, 14). Although training is an umbrella, we believe that team-based curricula can be a path to take, as they ensure that medical students have teamwork skills that are vastly important in healthcare (9).
During the last 5 years, the literature on team-based curricula and interdisciplinary education has flourished—representing a near quarter of identified literature (see Table 1). Most importantly, educators are continually encouraging the idea that healthcare education needs to be constructivist. Learners can take part in their own learning through methods such as SBT, which has shown to increase teamwork competencies (38, 39). Recent findings state that the most effective healthcare curricula are those that incorporate interprofessional simulation-based education [IPSE, Sezgin and Bektas (40)]. Alongside other types of interprofessional training (41), these methods provide students and clinicians the capability to learn to interact with healthcare professionals without compromising patient safety (42, 43). Moreover, the reason we believe team-based curricula is a holistic approach that allows students to grow in their teamwork abilities beyond and including communication—is that these methods provide students with social capital (44). As proposed by Burguess et al. (44), methods such as interprofessional team-based learning strategies allow students to build trust in their network, access and build resources such as knowledge and skills that each individual holds, and lastly, develop norms and rules for a team; which we believe can also aid in a team's coordination (18) and reflection capabilities (45). In other words, team-based curricula and interdisciplinary methods teach students to be well-rounded team members, not simply communicators. Though we do not believe team-based curricula is the end-all-be-all, a broad incorporation of team-based curricula can help healthcare practitioners develop teamwork competencies from the inception of their careers. This allows them to have built-in experience by the time they get to work on surgical teams, on research teams, and so on. Accompanied by other strategies, such as team coaching and continued SBT, it works to nurse teamwork competencies over time.
However, the literature has continued to emphasize that team-based curricula face the challenge that current healthcare structures do not support such interventions (46). While students like these approaches, some concerns are the lack of infrastructure for said interventions and the time required for implementing them (47). Notwithstanding, this should not dissuade hospitals, medical schools, and undergraduate institutions [see Kolbe et al. (48)] from aiming for an overhaul. While recent years have reiterated the challenge of incorporating these practices, the research continues to uncover that interprofessional methods yield significant results, such as improvements in shared decision-making and teamwork competencies (49) and improvements in clinical skills and a sense of belonging in the workplace (50). Curricula that take these reforming steps, such as incorporating TeamSTEPPS into healthcare students' education, have already shown promising results (51, 52). In addition to this, some medical schools are already incorporating these findings into their educational structures. One concrete example is the multimodal curriculum TeamFIRST, which aims to equip students with ten teamwork competencies necessary for team-based, interprofessional care.1 In this program, things like patient handovers are explicitly taught to students. TeamFIRST includes modules where students actively learn to communicate with their teams during handovers to improve patient safety. Students complete a simulated handover, practice sending and receiving information, and reflect on the experience to learn what can be improved.1 Such techniques have resulted in better handoffs in perioperative environments (46).
Overall, a multitude of research supports teamwork curricula's ability to show improvements, such as increasing student teamwork competencies (52). Therefore, the last 5 years have left us with the following takeaway: in a world that increasingly requires more interpersonal skills as technology fills in technical ones, systems and critical thinking are necessities that interdisciplinary team-based methods can provide (53). We believe that if we are to move forward with a focus on training sustainment as remarked by Salas et al. (1), we need strategies from beginning to end, and team-based education provides the first step in doing so.
5 Observation 4: simulation-based training, alongside debriefing, is the key for developing and maintaining teamwork skills
Salas et al. (1) stated that debriefing works, and simulation is a powerful tool to enhance teamwork. The last 5 years of research support these observations, with many studies remarking on how SBT should be incorporated alongside team-based curricula (40). SBT provides realistic clinical scenarios that closely mimic the challenges and complexities students encounter in their actual settings, enhancing the probability of transferring learned skills to real scenarios (54, 55). However, the core element of SBT lies in debriefings, which enable structured feedback and reflection, enhancing patient care by providing controlled, planned opportunities for facilitator training (56–59).
Recent developments show that SBT has successfully increased teamwork perception levels (60) and enhanced interprofessional collaboration in post-anesthesia care units (43). Moreover, simulation allows team members to undergo conflict in real-time, which could increase their conflict management skills (14). This training also allows teams to maintain teamwork skills over time (61) and improve attitudes toward teamwork (62). While we face the continuing challenge of refining methodological design (55), SBT (alongside debriefing) is a holistic approach that allows teams to face problems repeatedly and without risk. This targets more than one team competency, allowing members to develop trust with each other and allowing for more efficient team functioning.
In a field short on time, with team training and education often being set on the back burner, it is tempting to try and use one-time interventions. While these can yield some improvements (and are sometimes a necessity), if we are to tackle deep-rooted issues, we have to approach problems as what they are: a web instead of a needle in a haystack. Focusing on these evidence-based strategies allows healthcare practitioners to become more well-rounded team leaders and members. Team-based education supports teamwork competencies through a healthcare practitioner's workplace lifespan; SBT allows student and clinician teams to work and fail together without the fear of harming patients; debriefs allow them to discuss learnings; and internal team coaches foster teams in action, making for a system that supports teamwork every step of the way. However, in order to strengthen these strategies, the aid of real-time, unobtrusive, robust, and reliable measurement is needed.
6 Observation 5: real-time, unobtrusive, robust, and reliable measurement is needed
In relation to real-time, unobtrusive, robust, and reliable measurement in clinical practice, progress is being made. There are several methods that can be utilized that support ongoing assessment and feedback to improve patient care. Examples of effective methods include direct observations of clinical encounters (DOCEs), event-coding, entrustable professional activities (EPAs), and behavioral markers of specific observable behaviors or action that serve as indicators of proficiency in a particular skill or competency (63–66). However, as some note, assessment tools rely on the assumption that team measurement is equivalent to adding individual performance together (67). In order to continue advancing the science of teaming, we must move past this and look at team systems holistically. Recommendations include studying methods that examine the team system as a whole. One is the Team Emergency Assessment Measure (TEAM), an assessment that moves away from the summative assumption (67). Yet, we need more studies that study methods like TEAM in distinct clinical settings (as TEAM has only been examined in emergency settings) as a “one-size-fits-all” approach is not recommended.
Effective design of team-based strategies is closely tied to sound measurement practices like those mentioned above. Akin to blaming communication for medical error as a one-size-fits-all response, tailored measurement is frequently overlooked when designing team interventions. Though typical, this “one-size-fits-all” approach is misguided, as individuals operate in diverse contexts and take on tasks of varying complexities throughout their career trajectory. Measurement should be rooted in an evidence-based model that targets the specific context and clinical area being examined (68) while continuing to place the team where it belongs: an intricate and never-isolated system. The gap between research and practice is well-documented but remarked for a reason: teams exist in the wild and not in a laboratory setting.
Healthcare settings are highly controlled environments regarding personnel, procedures, and protocols. Learning and development can be enhanced in such complex settings when individuals are provided with real-time, unobtrusive, robust, and reliable feedback. While we recognize that this research is expensive and time-consuming, we must expand our understanding of measurement and be willing to take on the challenge that teams do not exist in isolation because measuring them as if they do provides limited opportunities for our science. The last 5 years have not provided a significant comprehensive strategy to address this problem—and it may be another five before there are any comprehensive strategies to discuss. However, by pivoting research to enhance our understanding of design measures related to team performance, we believe we can better diagnose a team's root issues instead of attributing errors to “communication gaps” in the field. For this reason, we recommend focusing on strategies that foster teams while continuing to develop measurement strategies that look at them in their real-time context. This could mean using strategies such as DOCEs and making sure they are accurately contextualized with clinical environments and team- and organizational-level factors.
7 The next 5 years
The last 5 years have highlighted the resiliency of the healthcare field over a pandemic, fluctuating demands, and mass technological change. Notwithstanding, such events have highlighted the need for new methods. With healthcare burnout at an all-time high (69, 70), as well as a lack of psychological safety in the field (71), we need methods that work together and nurse systems as a whole. It starts with teaching students to be team players, allowing them to practice, measuring teamwork robustly and reporting results accurately, and coaching teams throughout their life cycle. Effective teamwork in healthcare requires a holistic approach beyond a focus on communication. Moreover, we must understand that communication itself is multi-faceted, part of a system, and should be treated as such. To address these issues, we highlighted five observations that need further improvement but show extreme promise: higher quality communication, team coaching, team-based curricula, and SBT, and continued reliable measuring practices. By implementing these strategies and considering these observations, healthcare teams can work toward improving overall teamwork competencies and ultimately enhance patient care and outcomes.
Author contributions
GF: Writing—original draft, Writing—review & editing. MK: Writing—original draft, Writing—review & editing. ES: Writing—original draft, Writing—review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work was partially supported by the U.S. Army Research Institute (ARI) for the Behavioral and Social Sciences and was accomplished under Cooperative Agreement Number W911NF-19-2-0173. The views and conclusions contained in this document are those of the authors and should not be interpreted as representing the official policies, either expressed or implied, of the US Army Research Institute (ARI) for the Behavioral and Social Sciences or the US Government. This work was also partially supported by the Center for Clinical and Translational Sciences (UT Health Science Center, Houston, TX), which is funded by National Institutes of Health Clinical and Translational Award UL1 TR003167 from the National Center for Advancing Translational Sciences. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Advancing Translational Sciences or the National Institutes of Health. Rice University and University of Texas Health Sciences Center Houston are partners in this grant.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Footnotes
1. ^Paquette S, Hernandez J, Preble R, Sadighi M, Kilcullen M, Hoffman O, et al. Team first: An innovative educational strategy for teaching teamwork competencies to health profession and medical students. (2023). Unpublished manuscript.
References
1. Salas E, Zajac S, Marlow SL. Transforming health care one team at a time: ten observations and the trail ahead. Group Organ Manag. (2018) 43:357–81. doi: 10.1177/1059601118756554
2. Etherington C, Wu M, Cheng-Boivin O, Larrigan S, Boet S. Interprofessional communication in the operating room: a narrative review to advance research and practice. Can J Anesth. (2019) 66:1251–60. doi: 10.1007/s12630-019-01413-9
3. Street R Jr, Petrocelli JV, Amroze A, Bergelt C, Murphy M, Wieting JM, et al. How communication “failed” or “saved the day”: counterfactual accounts of medical errors. J Patient Exp. (2020) 7:1247–54. doi: 10.1177/2374373520925270
4. Tiwary A, Rimal A, Paudyal B, Sigdel KR, Basnyat B. Poor communication by health care professionals may lead to life-threatening complications: examples from two case reports. Wellcome Open Res. (2019) 4:1–4. doi: 10.12688/wellcomeopenres.15042.1
5. *Chamberland C, Hodgetts HM, Kramer C, Breton E, Chiniara G, Tremblay S. The critical nature of debriefing in high-fidelity simulation-based training for improving team communication in emergency resuscitation. Appl Cogn Psychol. (2018) 32:727–38. doi: 10.1002/acp.3450
6. *Real K, Santiago J, Fay L, Isaacs K, Carll-White A. The social logic of nursing communication and team processes in centralized and decentralized work spaces. Health Commun. (2018) 34:1751–63. doi: 10.1080/10410236.2018.1536940
7. *Seidlein A-H, Hannich A, Nowak A, Salloch S. Interprofessional health-care ethics education for medical and nursing students in Germany: an interprofessional education and practice guide. J Interprof Care. (2022) 36:144–51. doi: 10.1080/13561820.2021.1879748
8. Wu M, Tang J, Etherington C, Walker M, Boet S. Interventions for improving teamwork in intrapartem care: a systematic review of randomized controlled trials. BMJ Qual Saf. (2020) 29:77–88. doi: 10.1136/bmjqs-2019-009689
9. Clapper TC, Ching K. Debunking the myth that the majority of medical errors are attributed to communication. Med Educ. (2020) 54:74–81. doi: 10.1111/medu.13821
10. Randall Curtis J, Sathitratanacheewin S, Starks H, Lee RY, Kross EK, Downey L, et al. Using electronic health records for quality measurement and accountability in care of the seriously ill: opportunities and challenges. J Palliat Med. (2018) 21:S52–60. doi: 10.1089/jpm.2017.0542
11. *Bajwa NM, Bochatay N, Muller-Juge V, Cullati S, Blondon KS, Junod Perron N, et al. Intra versus interprofessional conflicts: implications for conflict management training. J Interprof Care. (2020) 34:259–68. doi: 10.1080/13561820.2019.1639645
12. *Keller S, Tschan F, Semmer NK, Timm-Holzer E, Zimmermann J, Candinas D, et al. “Disruptive behavior” in the operating room: a prospective observational study of triggers and effects of tense communication episodes in surgical teams. PLoS ONE. (2019) 14;e0226437. doi: 10.1371/journal.pone.0226437
13. *Papermaster AE, Champion JD. Exploring the use of curbside consultations for interprofessional collaboration and clinical decision-making. J Interprof Care. (2021) 35:368–75. doi: 10.1080/13561820.2020.1768057
14. Zajac S, Woods A, Tannenbaum S, Salas E, Holladay CL. Overcoming challenges to teamwork in healthcare: a team effectiveness framework and evidence-based guidance. Front Commun. (2021) 6:606445. doi: 10.3389/fcomm.2021.606445
15. Lacerenza CN, Marlow SL, Tannenbaum SI, Salas E. Team development interventions: evidence-based approaches for improving teamwork. Am Psychol. (2018) 73:517–31. doi: 10.1037/amp0000295
16. *Bollen A, Harrison R, Aslani P, van Haastregt JCM. Factors influencing interprofessional collaboration between community pharmacists and general practitioners—a systematic review. Health Soc Care Community. (2019) 27:e189–212. doi: 10.1111/hsc.12705
17. Marlow SL, Lacerenza CN, Paoletti J, Burke CS, Salas E. Does team communication represent a one-size-fits-all approach?: a meta-analysis of team communication and performance. Organ Behav Hum Decis Process. (2018) 144:145–70. doi: 10.1016/j.obhdp.2017.08.001
18. Tannenbaum S, Salas E. Teams that Work: The Seven Drivers of Team Effectiveness. New York, NY: Oxford University Press (2021) doi: 10.1093/oso/9780190056964.001.0001
19. Edmondson A. Psychological safety and learning behavior in work teams. Adm Sci Q. (1999) 44:350–83. doi: 10.2307/2666999
20. Edmondson AC, Bransby DP. Psychological safety comes of age: observed themes in an established literature. Annu Rev Organ Psychol Organ Behav. (2023) 10:55–78. doi: 10.1146/annurev-orgpsych-120920-055217
21. *Luo J, Jeon M, Lee M, Ho E, Pfammatter AF, Shetty V, et al. Relationships between changing communication networks and changing perceptions of psychological safety in a team science setting: analysis with actor-oriented social network models. PLoS ONE. (2022) 17:e0273899. doi: 10.1371/journal.pone.0273899
22. *Neuhaus C, Lutnæs DE, Bergström J. Emergence of power and complexity in obstetric teamwork. PLoS ONE. (2022) 17:e0269711. doi: 10.1371/journal.pone.0269711
23. *Seaton J, Jones A, Johnston C, Francis K. Allied health professionals' perceptions of interprofessional collaboration in primary health care: an integrative review. J Interprof Care. (2021) 35:217–28. doi: 10.1080/13561820.2020.1732311
24. Kolbe M, Eppich W, Rudolph J, Meguerdichian M, Catena H, Cripps A, et al. Managing psychological safety in debriefings: a dynamic balancing act. BMJ Simul Technol Enhance Learn. (2020) 6:164–71. doi: 10.1136/bmjstel-2019-000470
25. Rosen MA, DiazGranados D, Dietz AS, Benishek LE, Thompson D, Pronovost PJ, et al. Teamwork in healthcare: key discoveries enabling safer, high-quality care. Am Psychol. (2018) 73:433–50. doi: 10.1037/amp0000298
26. *Iachini AL, DeHart DD, Browne T, Dunn BL, Blake EW, Blake C. Examining collaborative leadership through interprofessional education: findings from a mixed methods study. J Interprof Care. (2019) 33:235–42. doi: 10.1080/13561820.2018.1516635
27. *Körner M, Becker S, Dinius J, Müller C, Zimmermann L, Rundel M. A patient-centered team-coaching concept for medical rehabilitation. J Interprof Care. (2018) 32:123–6. doi: 10.1080/13561820.2017.1357542
28. *Vatnøy TK, Dale B, Sundlisæter Skinner M, Karlsen T. Associations between nurse managers' leadership styles, team culture and competence planning in Norwegian municipal in-patient acute care services: a cross-sectional study. Scand J Caring Sci. (2022) 36:482–92. doi: 10.1111/scs.13064
29. Maynard MT, Mathieu JE, Rapp TL, Gilson LL, Kleiner C. Team leader coaching intervention: an investigation of the impact on team processes and performance within a surgical context. J Appl Psychol. (2021) 106:1080–92. doi: 10.1037/apl0000814
30. Hackman JR, Wageman R. A theory of team coaching. Acad Manag Rev. (2005) 30:269–87. doi: 10.5465/amr.2005.16387885
31. Traylor AM, Stahr E, Salas E. Team coaching: three questions and a look ahead: a systematic literature review. Int Coach Psychol Rev. (2020) 15:54–67. doi: 10.53841/bpsicpr.2020.15.2.54
32. Liu C, Pirola-Merlo A, Yang C-A, Huang C. Disseminating the functions of team coaching regarding research and development team effectiveness: evidence from high-tech industries in taiwan. Soc Behav Pers. (2009) 37:41–57. doi: 10.2224/sbp.2009.37.1.41
33. Fernández Castillo G, Salas E. Can team coaching provide healthcare the remedy it needs? J Interdiscip Care. (2023) 1–11. doi: 10.1080/13561820.2023.2285030
34. Rousseau V, Aube C, Tremblay S. Team coaching and innovation in work teams: an examination of the motivational and behavioral intervening mechanisms. Leadersh Organ Dev J. (2013) 34:344–64. doi: 10.1108/LODJ-08-2011-0073
35. Graen G, Canedo JC, Grace M. Team coaching can enhance psychological safety and drive organizational effectiveness. Organ Dyn. (2020) 49:100697. doi: 10.1016/j.orgdyn.2019.01.003
36. Schaubroeck J, Carmeli A, Bhatia S, Paz E. Enabling team learning when members are prone to contentious communication: the role of team leader coaching. Hum Relat. (2016) 69:1709–27. doi: 10.1177/0018726715622673
37. van Diggele C, Burgess A, Roberts C, Mellis C. Leadership in healthcare education. BMC Med Educ. (2020) 20:456. doi: 10.1186/s12909-020-02288-x
38. Barton G, Bruce A, Schreiber R. Teaching nurses teamwork: integrative review of competency-based team training in nursing education. Nurse Educ Pract. (2018) 32:129–37. doi: 10.1016/j.nepr.2017.11.019
39. Keiser NL, Arthur W Jr. A meta-analysis of the effectiveness of the after-action review (or debrief) and factors that influence its effectiveness. J Appl Psychol. (2021) 106:1007–32. doi: 10.1037/apl0000821
40. Sezgin MG, Bektas H. Effectiveness of interprofessional simulation-based education programs to improve teamwork and communication for students in the healthcare profession: a systematic review and meta-analysis of randomized controlled trials. Nurse Educ Today. (2023) 120:105619–105619. doi: 10.1016/j.nedt.2022.105619
41. *Block L, LaVine NA, Martinez J, Strawser J, Lu C, Cacace F, et al. A novel longitudinal interprofessional ambulatory training practice: the improving patient access care and cost through training (IMPACcT) clinic. J Interprof Care. (2021) 35:472–5. doi: 10.1080/13561820.2020.1751595
42. Driskell JE, Johnston JH. Stress exposure training. In: Cannon-Bowers JA, Salas E, , editors. Making Decisions Under Stress: Implications for Individual and Team Training. Washington, DC: American Psychological Association (1998), p. 191–217. doi: 10.1037/10278-007
43. *Villemure C, Georgescu LM, Tanoubi I, Dube J-N, Chiocchio F, Houle J. Examining perceptions from in situ simulation-based training on interprofessional collaboration during crisis event management in post-anesthesia care. J Interprof Care. (2019) 33:182–9. doi: 10.1080/13561820.2018.1538103
44. Burgess A, van Diggele C, Matar E. Interprofessional team-based learning: building social capital. J Med Educ Curric Dev. (2020) 7:2382120520941820. doi: 10.1177/2382120520941820
45. Aitken JA, Torres EM, Kaplan S, DiazGranados D, Su L, Parker S. Influence of simulation-based training on reflective practice. BMJ Simul Technol Enhanc Learn. (2021) 7:638. doi: 10.1136/bmjstel-2021-000870
46. Paquette S, Kilcullen M, Hoffman O, Hernandez J, Mehta A, Salas E, et al. Handoffs and the challenges to implementing teamwork training in the perioperative environment. Front Psychol. (2023) 14:1187262. doi: 10.3389/fpsyg.2023.1187262
47. *Vincent-Onabajo G, Mustapha SA, Gujba FK. Attitudes toward interprofessional practice among healthcare students in a Nigerian university. J Interprof Care. (2019) 33:336–42. doi: 10.1080/13561820.2019.1605980
48. Kolbe M, Goldhahn J, Useini M, Grande B. “Asking for help is a strength”—How to promote undergraduate medical students' teamwork through simulation training and interprofessional faculty. Front Psychol. (2023) 14:1214091. doi: 10.3389/fpsyg.2023.1214091
49. Hsiao C-Y, Wu J-C, Lin P-C, Yang P-Y, Liao F, Guo S-L, et al. Effectiveness of interprofessional shared decision-making training: a mixed-method study. Patient Educ Couns. (2022) 105:3287–97. doi: 10.1016/j.pec.2022.07.010
50. O'Mahony S, Baron A, Ansari A, Deamant C, Nelson-Becker H, Fitchett G, et al. Expanding the interdisciplinary palliative medicine workforce: a longitudinal education and mentoring program for practicing clinicians. J Pain Symptom Manage. (2020) 60:602–12. doi: 10.1016/j.jpainsymman.2020.03.036
51. *Chen AS, Yau B, Revere L, Swails J. Implementation, evaluation, and outcome of TeamSTEPPS in interprofessional education: a scoping review. J Interprof Care. (2019) 33:795–804. doi: 10.1080/13561820.2019.1594729
52. Ross JG, Latz E, Meakim CH, Mariani B. Teamstepps curricular-wide integration: baccalaureate nursing students' knowledge, attitudes, and perceptions. Nurse Educ. (2021) 46:355–60. doi: 10.1097/NNE.0000000000000999
53. Clark K, Hoffman A. Educating healthcare students: strategies to teach systems thinking to prepare new healthcare graduates. J Prof Nurs. (2019) 35:195–200. doi: 10.1016/j.profnurs.2018.12.006
54. *Costello M, Prelack K, Faller J, Huddleston J, Adly S, Doolin J. Student experiences of interprofessional simulation: findings from a qualitative study. J Interprof Care. (2018) 32:95–7. doi: 10.1080/13561820.2017.1356810
55. *Wooding E, Gale T, Maynard V. Evaluation of teamwork assessment tools for interprofessional simulation: a systematic literature review. J Interprof Care. (2020) 34:162–72. doi: 10.1080/13561820.2019.1650730
56. Berger-Estilita J, Lüthi V, Greif R, Abegglen S. Communication content during debriefing in simulation-based medical education: an analytic framework and mixed-methods. Med Teach. (2021) 43:1381–90. doi: 10.1080/0142159X.2021.1948521
57. Lyons R, Lazzara E, Benishek L, Zajac S, Gregory M, Sonesh S, et al. Enhancing the effectiveness of team debriefings in medical simulation: more best practices. Jt Comm J Qual Saf . (2015) 41:115–25. doi: 10.1016/S1553-7250(15)41016-5
58. Paige JT, Kerdolff KE, Rogers CL, Garbee DD, Yu Q, Cao W, et al. Improvement in student-led debriefing analysis after simulation-based team training using a revised teamwork assessment tool. Surgery. (2021) 170:1659–64. doi: 10.1016/j.surg.2021.06.014
59. Reyes DL, Tannenbaum SI, Salas E. Team development: the power of debriefing. People Strategy. (2018) 41:46–52. Available online at: https://ctsicn.org/sites/g/files/zaskib901/files/2021-04/Reyes%2C%20Tannenbaum%2C%20%26%20Salas%202018%20Team_Development_The_Power_of%20Debriefing.pdf
60. Laco RB, Stuart WP. Simulation-based training program to improve cardiopulmonary resuscitation and teamwork skills for the urgent care clinic staff. Mil Med. (2022) 187:e764–9. doi: 10.1093/milmed/usab198
61. Eismann H, Palmaers T, Hagemann V, Flentje M. Training of airway management for anesthesia teams – measurement of transfer into daily work routine by questionnaire. J Med Educ Curric Dev. (2021) 8:1–8. doi: 10.1177/23821205211063363
62. Eismann H, Palmaers T, Tsvetanov S, Hagemann V, Flentje M. Changes of collective orientation through a medical student's anesthesia simulation course–simulation-based training study with non-technical skills debriefing versus medical debriefing. BMC Med Educ. (2019) 19:1–9. doi: 10.1186/s12909-019-1765-x
63. Bracco F, De Tonetti G, Masini M, Passarelli M, Geretto F, Celleno D. Crisis resource management in the delivery room: development of behavioral markers for team performance in emergency simulation. Int J Environ Res Public Health. (2018) 15:439. doi: 10.3390/ijerph15030439
64. Seelandt JC, Tschan F, Keller S, Beldi G, Jenni N, Kurmann A, et al. Assessing distractors and teamwork during surgery: developing an event-based method for direct observation. BMJ Qual Saf. (2014) 23:918. doi: 10.1136/bmjqs-2014-002860
65. Shorey S, Lau TC, Lau ST, Ang E. Entrustable professional activities in health care education: a scoping review. Med Educ. (2019) 53:766–77. doi: 10.1111/medu.13879
66. Stojan JN, Clay MA, Lypson ML. Assessing patient-centered care through direct observation of clinical encounters. BMJ Qual Saf. (2016) 25:135–7. doi: 10.1136/bmjqs-2015-004584
67. *Etherington N, Larrigan S, Liu H, Wu M, Sullivan KJ, Jung J, et al. Measuring the teamwork performance of operating room teams: a systematic review of assessment tools and their measurement properties. J Interprof Care. (2021) 35:37–45. doi: 10.1080/13561820.2019.1702931
68. Pavez I, Gomez H, Liu C, Gonzalez VA. Measuring project team performance: a review and conceptualization. Int J Project Manag. (2022) 40:951–71. doi: 10.1016/j.ijproman.2022.11.001
69. *Norful AA, He Y, Rosenfeld A, Abraham CM, Chang B. Mitigating primary care provider burnout with interdisciplinary dyads and shared care delivery. J Eval Clin Pract. (2022) 28:363–70. doi: 10.1111/jep.13642
70. Rotenstein LS, Sinsky C, Cassel CK. How to measure progress in addressing physician well-being: beyond burnout. J Am Med Assoc. (2021) 326:2129–30. doi: 10.1001/jama.2021.20175
Keywords: team science, team coaching, team-based curricula, simulation-based training, measurement
Citation: Fernández Castillo G, Khalid M and Salas E (2024) Beyond communication: an update on transforming healthcare teams. Front. Med. 11:1282173. doi: 10.3389/fmed.2024.1282173
Received: 23 August 2023; Accepted: 01 February 2024;
Published: 21 February 2024.
Edited by:
Julia Carolin Seelandt, University Hospital Zürich, SwitzerlandReviewed by:
Vera Hagemann, University of Bremen, GermanyCopyright © 2024 Fernández Castillo, Khalid and Salas. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Eduardo Salas, ZWR1YXJkby5zYWxhc0ByaWNlLmVkdQ==