 Regina Ruiz de Viñaspre-Hernández1,2
Regina Ruiz de Viñaspre-Hernández1,2 Rosana Garrido-Santamaria3Raquel Urra-Martínez3Paula Sáenz-Cabredo4Ana Elena Garrido-Rivas1,2,4
Rosana Garrido-Santamaria3Raquel Urra-Martínez3Paula Sáenz-Cabredo4Ana Elena Garrido-Rivas1,2,4 Raúl Juárez-Vela1,2
Raúl Juárez-Vela1,2 Juan Luis Sánchez-González5Alberto Lafuente-Jimenez4
Juan Luis Sánchez-González5Alberto Lafuente-Jimenez4 Enrique Ramón-Arbués6,7Noelia Navas-Echazarreta1,2*
Enrique Ramón-Arbués6,7Noelia Navas-Echazarreta1,2* Ivan Santolalla-Arnedo1,2
Ivan Santolalla-Arnedo1,2- 1Faculty of Health Sciences, University of La Rioja, Logroño, Spain
- 2Grupac Research Group, Department of Nursing, University of La Rioja, Logroño, Spain
- 3Family Planning Center, Rioja Health Service, Logroño, Spain
- 4Rioja Health Service, Logroño, Spain
- 5Department of Nursing and Physiotherapy, University of Salamanca, Salamanca, Spain
- 6Faculty of Health Sciences, San Jorge University, Villanueva de Gállego, Spain
- 7SAPIENF Investigation Group, University of Zaragoza, Zaragoza, Spain
Purpose: To know the discontinuation rate and characterize predictors and reasons of contraceptive implant removal within 12 months of insertion in our community setting.
Methods: This prospective cohort study included women receiving the etonogestrel contraceptive implant at sexual and reproductive health centers between September 2019 and September 2020. The variables collected were implanted insertion timing, reproductive and demographic characteristics, medical conditions, sexual activity and counseling. Our primary outcome was implant discontinuation. Kaplan–Meier survival curves were used to show the cumulative discontinuation rate of implants contraceptive within the first year of insertion. We also identified factors that increased the risk of implant removal using the log-rank test and the Cox regression model. Reasons for discontinuation were documented.
Results: 199 women were followed up. Implant discontinuation was documented in 17.1% of implant users prior to 12 months. Factors that increase the risk of implant removal are living with a partner, being aged 25–34 years and not receiving comprehensive and structured counseling from the midwife. The main reason for removal was unsatisfactory bleeding (97.1%), but this was combined with other reasons such as cessation of sexual intercourse (58.8%), worsening mood (58.8%), weight gain (55.9%) or decreased libido (50.0%).
Conclusion: The rate of discontinuous implant uses in the first year is relevant in relation to cost-effectiveness, there is room for improvement that should not be overlooked. Comprehensive and structured midwife-led counseling can reduce early implant abandonment removal. The development in different countries of the role of midwives in the management of contraceptives can contribute to the economic benefit of health services and the satisfaction of women.
Introduction
Women’s sexual and reproductive health (SRH) is associated with access to highly effective contraceptive methods that minimize the risk of having to bear the physical and psychological consequences of unwanted childbearing or abortion. The unintended pregnancy reduces maternal and infant quality of life, educational attainment, job opportunities and economic stability, and increases the economic costs for health system Worldwide, it is estimated that avoiding teenage pregnancies, spacing pregnancies, and ending unwanted pregnancies and abortions could prevent one in three maternal deaths (1). Furthermore, to exercise the right to sexual health and well-being, it is essential that women be able to choose their sexual practices without fear of pregnancy (2).
Etonogestrel subdermal implant (ESI) is a long-acting reversible contraceptive (LARC) which is safe and highly effective (3). Its effect is based on the slow and sustained release of etonogestrel which induces anovulation, inadequate development of the endometrium and thickening of the cervical mucus. In Spain it is marketed as Implanon NXT, an implant with a single, soft, flexible plastic rod containing 68 milligrams of the active ingredient, etonogestrel, and is currently approved by the European Medicines Agency for 3 years of use.
Studies report wide variability in continuation rates at one year after placement. The Moray 2021 review showed rates of 57 to 97%, and the two meta-analyses conducted in the same review showed that pooled one-year continuation rate was 77.5 and 76.5%, respectively. Continuation rates were higher in lower-middle-income or low-income countries compared to high-income countries (4). European studies also show this variability, with continuation rates of 72% (5) or 91% (6).
ESI commonly causes changes in the frequency, intensity, or duration of vaginal bleeding. In the first three months, it is estimated that irregular bleeding appears in 50% of users and prolonged bleeding in 30% (7) and these bleedings are the most frequent reason for early implant removal (8). Other reasons are headache, weight gain, changes in mood, decreased libido, skin conditions (acne, hair loss, or hirsutism), dizziness, lower abdominal pain, mastalgia, fatigue or localized pain at the insertion site, among others (9).
In Spain, implant insertion is free of charge and the health-care system funds between 40 and 100% of the pharmaceutical cost, depending on the woman’s income. Despite its high efficacy and the few medical situations that discourage its use (10), only 1.4% of Spanish women who use contraceptives had an implant in 2019 (11). Both low acceptance and early removal of the implant have been associated with non-existent or inadequate contraceptive counseling (8, 12).
Implant placement requires an initial financial outlay that is highly cost-effective for both the woman and the health system that funds it, provided it is not removed too early. In a weighted cost analysis in women aged 20–29, cost neutrality was estimated to be achieved at 2.1 years (13). Therefore, when looking at women’s interests and the sustainability of the health system, it is necessary to provide data on early discontinuation and the reasons that best explain it, aiming to establish measures that prevent early removal and result in greater cost savings. The objective of our study is to understand the discontinuation rate in the first year of implant use, as well as the conditions of the women that have an early implant removal and the reasons that they have for withdrawing the implant.
Methods
Prospective cohort study
The study started in September 2019 at the Centre for Sexual and Reproductive Health (CSHR) in La Rioja (Spain), data collection for this study was performed during one year (2019–2020).
Context of the study
La Rioja is a territory located in the north of Spain with an area of 5,000 km2 and a population of 319,485 inhabitants, of which 47% live in the city of Logroño (150,020 inhabitants), 30% in towns of between 25,000 and 5,000 inhabitants and 23% in towns of less than 5,000 inhabitants. It has a network of 19 health centers distributed throughout its geography and the community midwife is part of the primary care team in all of them. Travel to the city does not exceed 45 min.
In 2019, the protocol of care for women requesting contraception included a comprehensive and standardized contraceptive counseling program that is modeled on the structure used in the CHOICE Project (14) whose components provide accurate and unbiased information to help women assess their needs and make an informed decision, within the framework of the Shared Decision Making (15). This type of structured contraceptive counseling service was led by community midwives, who had been previously trained. In a face-to-face visit lasting 15 to 20 min, oral and written information was provided, and doubts were resolved for an informed and shared decision on contraception. From this consultation, the midwives arranged a quick appointment at the CSHR, the only health care center where trained personnel (midwife or gynecologist) fitted the implants. Follow-up visits were scheduled at 3, 6, and 12 months and they were offered the possibility of making an appointment whenever they needed. Other women went to the CSHR on their own accord, without first attending the midwife’s consultation. These women received the routine counseling usually provided at the CSHR prior to implant insertion. Three months after implant insertion, a review appointment is scheduled at the community midwife’s office or at the same sexual and reproductive health center. Access to the community midwife’s consultation and the CSHR was universal, free and direct. The women paid between 0 and 60 euros per implant, and the health system paid the rest of the amount.
Participants
All women of childbearing age who, between 09/09/2019 and 09/08/2020, went to the CSHR for implant placement were invited to participate. The exclusion criteria were: lack of cognitive or language ability to understand and sign the consent for participation and the refusal of the legal representative or guardian of a girl under 16 years old to sign the informed consent. All eligible women agreed to participate.
The study was approved by the ethics committee of La Rioja (Ref. CEImLAR P.I 386).
The participants underwent a standardized contraceptive evaluation in the family planning protocol to identify medical situations that contraindicated its use (10). The research staff collected the data reported by the patient in relation to her socio-demographic status (age, place of residence, nationality, studies, work relationship, affective relationship, cohabitation with a partner), gynecological and obstetric history (pregnancies, births, abortions, living children, history of STIs, previous use of hormonal contraceptives), medical conditions (BMI, smoking and physical exercise), sexual activity (sexual satisfaction and frequency of intercourse) and counseling. After pregnancy was ruled out, the implant was inserted by a qualified professional. Follow-up visit was scheduled at 3 month.
The dependent variable -discontinuation rate- was defined as the cumulative probability that women who received the implant have it removed in the first year. The independent variables were the sociodemographic and medical variables collected in the contraceptive evaluation: age was categorized into three ranges (15 to 24 years old, 25 to 34 years old and 35 or more years old); place of residence (capital city with 150,022 inhabitants, towns of 25,000 to 5,000 inhabitants and towns with less than 5,000); stability of the relationship: stable (little tension, little uncertainty, low-risk break-up) or unstable (tension, uncertainty, high-risk break-up); cohabitation as a couple: yes (usually sharing the same household) or no (usually living in different houses) partner relationship: monogamous (a couple) and non-monogamous (several couple and single): yes or no; employment situation: unemployed, salaried employee, self-employed, student; education level: compulsory education was defined as period of education that is required of all people and is imposed by the Spanish government (up to 16 years old) or non-compulsory (above 16 years old); country of birth: Spain (native women) or other country (migrant women), physical exercise was defined as the performance of some activity in order to develop or maintain physical fitness and overall health, 1 or more days a week; yes or no; smoker yes or no; Body Mass Index (BMI) was categorized into four groups: underweight (BMI <20 kg/m2), normal weight (20–24.9 kg/m2), overweight (25–29.9 kg/m2) and obese class I (≥30 kg/m2); frequency of sexual intercourse: occasional, monthly, weekly or daily; history of hormonal contraceptives and Sexually Transmitted Infections (STIs): yes or no; history of pregnancy, childbirth, voluntary abortion: yes or no and having children: yes or no. Sexual satisfaction was defined as overall contentment with emotional and sexual aspects of the sex life and was assessed with the validated Spanish version of the sexual satisfaction scale for women (SSS-W-e), at the beginning of the method. The scale that measures contentment is made up of 6 items: 1. I feel content with my present sex life; 2. I feel some-thing is missing from my present sex life; 3. I feel I do not have enough emotional closeness; 4. I feel content with the frequency of sexual intimacy; 5. I do not have any problems or concerns about sex; 6. Overall, I am satisfied with my sex life. Women are instructed to rate their level of agreement with each item using a Likert scale from 1 = strongly disagree to 5 = strongly agree. The score range is 6–30, and it is calculated by adding the scores of the individual items (16). Sexual satisfaction was low when its value was below the median and high when it was above the median. Type of counseling: Women were considered to have received “midwife-led structured counseling” when they had attended the scheduled consultation with the community midwife. Women who did not use this service were provided with the “usual counseling.”
Women who requested implant removal in the first year were asked to complete an ad-hoc questionnaire, on the day of implant removal, to collect two types of information: (a) their level of satisfaction, with the safety, comfort and price of the method and the accessibility of the service (ease and speed of appointment for implant insertion and removal) on a scale of 0 to 10 (from zero to maximum satisfaction), and (b) the reason(s) leading them to request implant removal: the questionnaire included a predetermined list and they could indicate only one or more than one, together with an open question to add other reasons not contemplated in the previous list. Both questionnaires were designed based on a literature review and information collected in the medical records of other women who had their implants removed before the start of the study.
Statistical analysis
Women’s characteristics and reasons for early implant removal were reported in terms of frequency and percentage and satisfaction levels with median and interquartile range. To estimate the discontinuation rate, we will calculate the cumulative incidence based on the Kaplan–Meier approach (exact-events times) and to assess whether there are differences in the distribution of method discontinuation times in the first year, based on different factors, we will calculate the chi-square using the log-rank test. The Cox regression model was used to estimate the risk of discontinuing contraception in the first year. Variables that showed statistical significance in the log-rank test were included in the model and those that continued to show statistical significance in the model were retained (p < 0.05).
Results
Sample description
232 women were recruited for the study, of whom 33 (14.2%) could not be traced in the first year of follow-up. The remaining 199 (85.8%) continued in the study. Of these 199 women, 34 (17.1%) had the implant removed within the first year (Figure 1).

Figure 1. Flow diagram of cohort.
The observed cohort (199 women) was between 15 and 50 years old. The majority were migrant women,117 (60.3%) in monogamous 166 (83.8%) and stable160 (80.8%) relationships and lived with their partner 124 (62.6%). Almost 117 (60%) were employed while the other 80 (40%) were unemployed 49 (25%) or students 31 (15%), and 86 (45%) of the women had compulsory education (up to the age of 16). Among them, 83 (41.75%) were of normal weight, 77 (39.1%) exercised at least once a week, the majority 127 (64.5%) did not smoke. For 71 (57.7%) of the women their sexual satisfaction was high and most of them had sex at least once a week 109 (56.5%). Approximately half of the women had received prior advice from the midwife (Table 1).
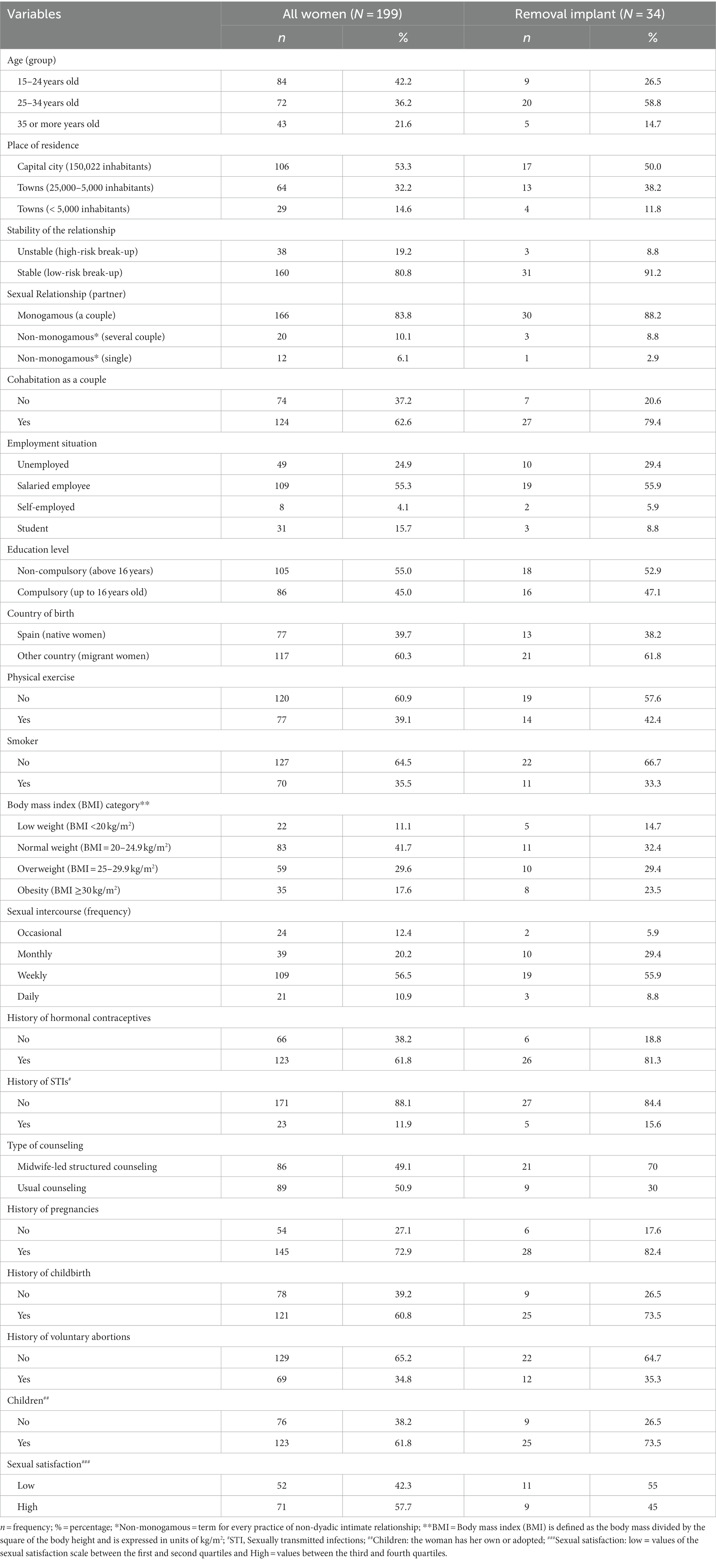
Table 1. Baseline women characteristics.
When comparing the socio-demographic and medical characteristics of the untraceable women to the women who remained in the study, we only found statistically significant differences (p > 0.05) in 4 of the 18 variables measured. Among the untraceable women there was a significantly higher proportion of Spanish women (χ2 = 4.388; p = 0.04), in non-stable relationships (χ2 = 4.715; p = 0.03), who did not live with their partners (χ2 = 4.043; p = 0.04), who were not monogamous (χ2 = 6.770; p = 0.03), nor did they practiced sport or physical exercise (χ2 = 5,671; p = 0.02).
Discontinuation rate in the first 12 months was 17.1%. The mean of time to discontinuation (time form the start of implant to the end of implant) during the first year was 11.06 months (standard deviation 0.16) (Figure 2).
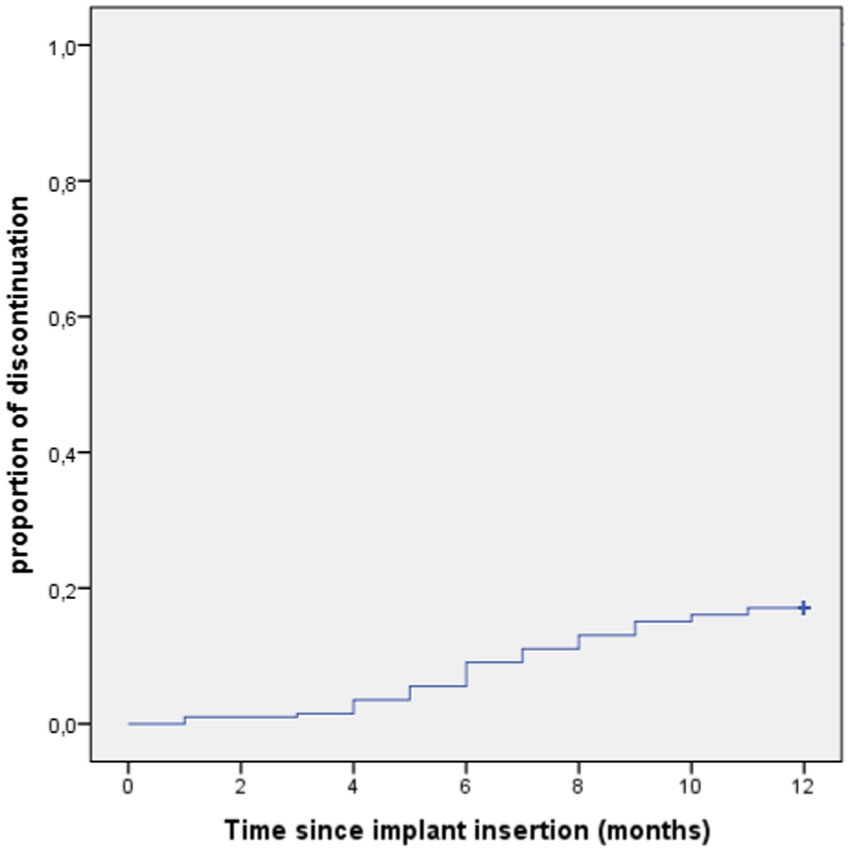
Figure 2. Survival analysis of first year discontinuation (Kaplan–Meier’s plots).
Table 2 shows that four variables were significantly linked to discontinuation time with the implant (age, cohabitation with partner, contraceptive counseling, and previous use of hormonal contraception). Of these, the first three remained statistically significant in the regression model (Table 3).
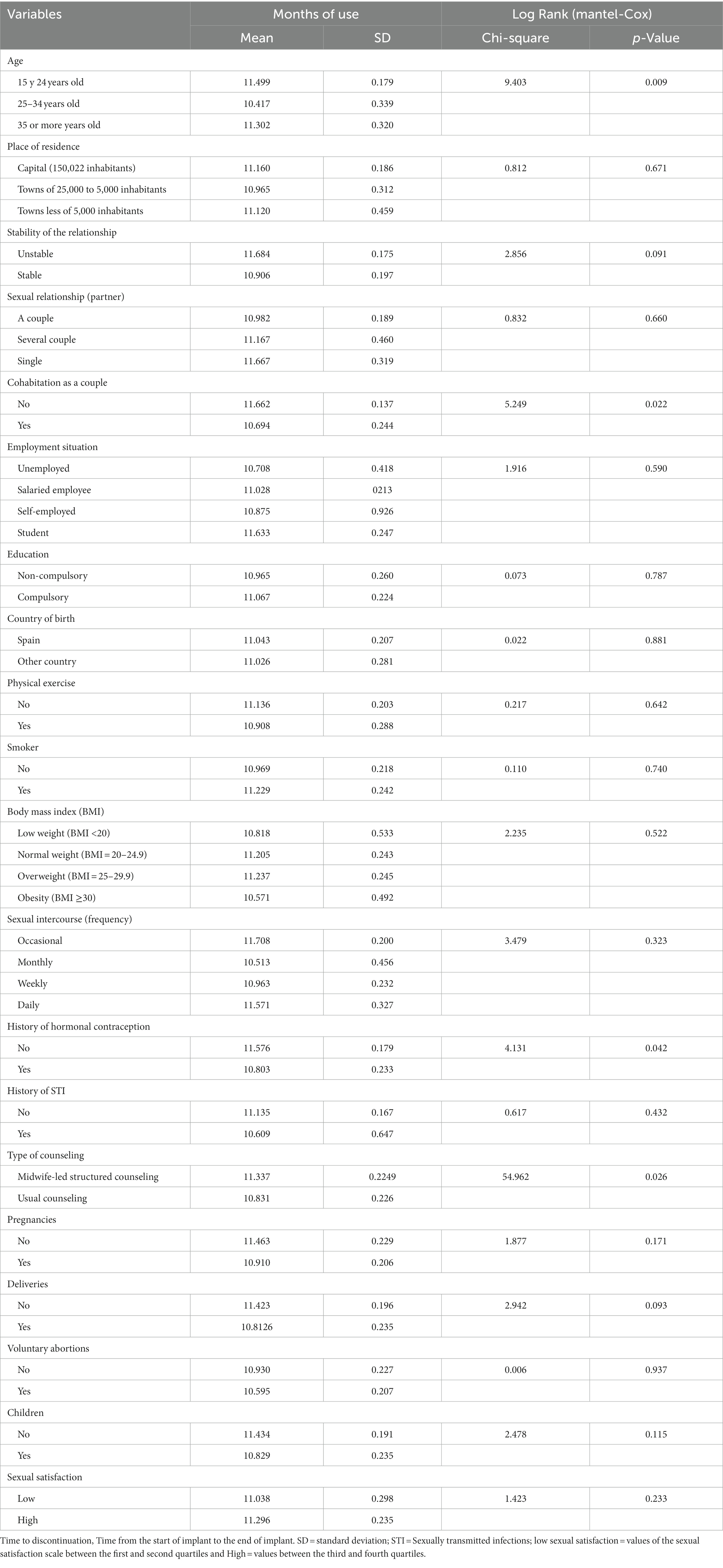
Table 2. Variables related to the time to discontinuation (TTD) with the implant.
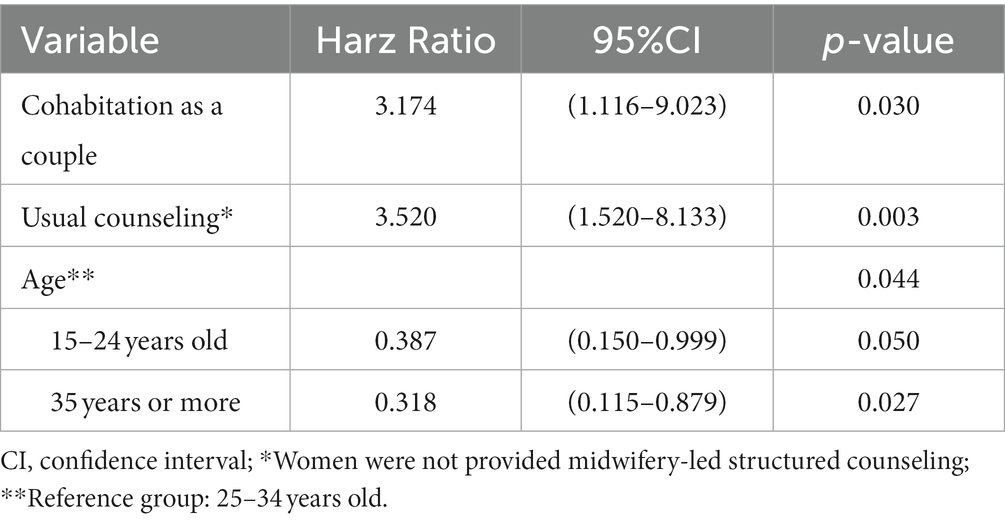
Table 3. Proportional Hazards model (Cox’s regression).
In the first year after implant insertion, women who live with their partner are 3.4 times more likely to have the implant removed; if they do not receive midwife counseling, the risk is 3.4 times higher. Regarding age, younger women (aged 15–24 years) and older women (>35 years) have a lower risk of removal, 61 and 68% respectively, than women aged 25–34 years.
Satisfaction with the safety and comfort of the method, and accessibility rated between 8 and 10 points on a scale of 0 to 10. No woman became pregnant with the implant in the first year. The price of the implant was the least satisfactory aspect (Table 4).
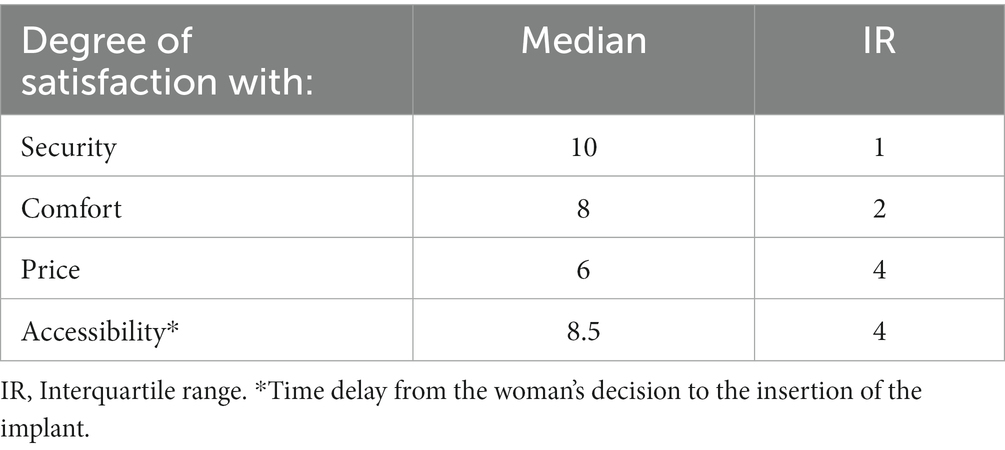
Table 4. Evaluation of the women’ satisfaction with implant.
Only one woman reported a single reason for abandoning the method, and that was the desire to become pregnant in the short term. The rest of them, lists two or more reasons, the most common one (97.1%) was an excessive or unexpected bleeding pattern. However, in all cases, bleeding was accompanied by other reasons reported as such: 58.8% cessation of intercourse, 58.8% worsening of their mood, 55.9% weight gain, or 50% decreased libido (Table 5).
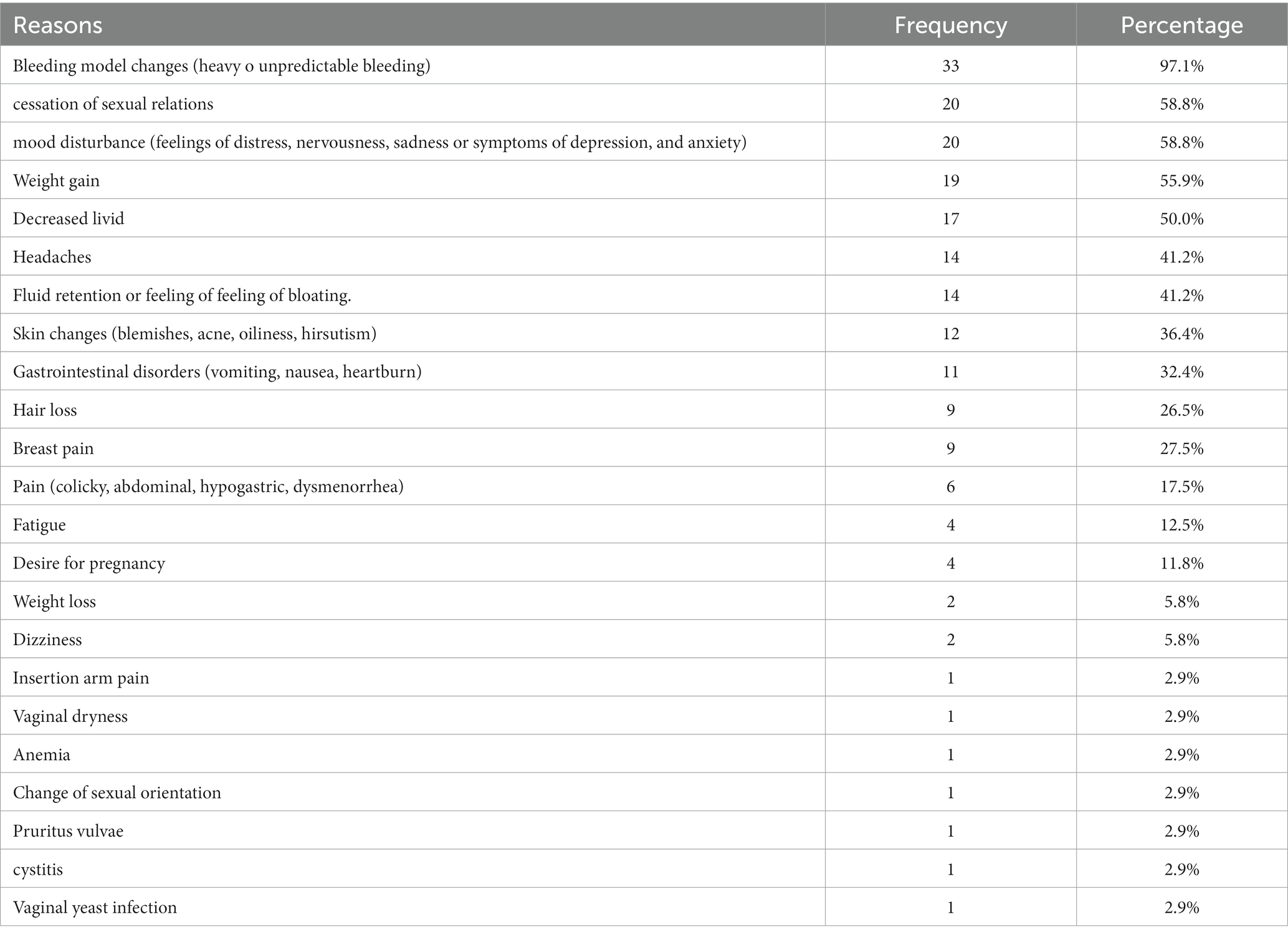
Table 5. Reasons given by women for removal the implant during the first year.
Discussion
Our study found that the rate of discontinuity with the implant one year after insertion was 17.1% and the conditions that increase the risk of removal were: living with an intimate partner, being between 25–34 years old and not attending the midwife for contraceptive counseling. Excessive or unexpected bleeding was a reason almost always present, but not enough on its own for the woman to decide to have the implant removed. The price of the implant was the worst rated aspect by women.
The characteristics of women who opted for the implant (40% of Spanish women and 60% of migrant women) do not correspond to the profile of women of childbearing age in La Rioja in 2019, where only 17.7% were migrant women. This finding was not an objective of our study, but we believe it is important to highlight. Another Spanish study already found that migrant women had a much higher use of LARC than Spanish women (17). We believe that this phenomenon could be associated with the persistence of misconceptions among Spanish clinicians that could lead to information biases (18). A paternalistic attitude in contraceptive counseling would lead to preferentially recommending the use of the implant to women with low economic resources or to non-compliant women (17, 19). The study by Loder (20) found that women with a higher perception of discrimination were more likely to use a highly effective, reversible method. It is possible that in our country’s health care model we have not managed to fully integrate person-centered care and that joint decision-making is not yet the norm when we talk about sexual and reproductive health. It is necessary that health professionals believe in women’s autonomy and train in those communication and counseling skills that make it possible (12).
.The discontinuation rate found in this study (17.1%) is similar to that reported in the national survey of the Spanish Society of Contraception in 2020 (16%) (11) and virtually identical to the rate reported by the CHOICE project (17%) in a cohort of 5,097 women in St. Louis, USA (21) or to the 16.7% found in another study in the Spanish population (22), albeit below the 9% also found in the Spanish population (6). Other European studies find somewhat lower continuation rates, in the Netherlands 26% (5) and in a multicenter clinical trial in Australia, Finland, Norway, Sweden and the United Kingdom 26.8% (9).
Among the factors that increase the risk of removal, counseling is the most easily rectifiable situation. We measured community midwife-led counseling because it was a programmed, homogenous intervention based on the structured contraceptive counseling provided by the Contraceptive CHOICE Project (14). This model, which includes counseling about the side effects of the method, has shown its effect on the choice and continued use of the implant (23) and subsequent studies support this result (12, 14). The parts of counseling that show greater efficiency are personalization of counseling and shared decision-making, questions about the patient’s reproductive life plan/pregnancy intentions and a discussion of contraceptive methods by level of effectiveness (24). Furthermore, the women who received prior advice from the community midwife had the opportunity to establish a relationship of trust that allowed her to return to visit her to resolve their doubts or complaints, which could avoid, in some cases, early removal of the implant.
According to our data, the risk of early implant removal is lower in women younger than 25 and older than 35. The review by Hendrick (2020) (25) included nine studies that considered age as a factor in the continuation of the LARC method (IUD and implant), the results were not consistent, one of the studies reported that the older the age at implant placement the higher the risk of early removal (26). Data from the CHOICE Project find no significant difference in continuation rates in relation to age (27).
A woman’s motivation to avoid pregnancy is associated with continuation of contraceptive use (28). A more precarious economic situation, for younger women, or an already satisfied reproductive project, for older women, may justify a stronger and irrevocable decision to avoid pregnancy. On the other hand, most Spanish women make their decision to become pregnant while living with their partner, a situation that facilitates access to housing, the sharing of expenses and childcare responsibilities, and therefore places them in a better position to take on an unplanned pregnancy (29). We believe that the conscious and unconscious cost/benefit balance that women make to continue with the implant could explain why some of them feel less motivated to avoid pregnancy and consequently may have a lower tolerance for the side effects of the method. In the CHOICE study, the only socio-demographic characteristic associated with removal before six months of LARC methods (IUD and implant) was being single (23). In Spain, the percentage of single women who live with their partners and have children is very significant. In 2019, according to data from the Spanish statistics institute (INE) the proportion of children born to unmarried mothers was 48.41%.
Excessive or unexpected bleeding is the main reason for early implant removal, which is consistent with the scientific literature (3, 4). The other reasons found have also been widely cited in the literature (8). The collected reasons are women’s perceptions, unproven but sufficient for them to decide to remove the implant. Changes in bleeding pattern is well-documented in the scientific literature (30, 31), however, there is no consistent evidence of the effect of the implant on weight gain (32) on mood (33, 34) or libido and sexual function (35), and it has even been found that perceived weight gain may be inaccurate and poorly correlated with actual weight (36). The mood disturbance and cessation of sexual intercourse was the seconds most frequently cited reasons for implant removal, but as in all cases this reason was accompanied by unsatisfactory bleeding; we cannot discriminate which of these reasons was more important in the woman’s decision. Other studies report a single reason for implant removal (8, 9), but most of our behaviors do not occur for a single reason, so it is necessary to understand the full range of women’s motivations and needs for choosing and continuing with a method (37). Open and ongoing communication between midwives and women could improve method adherence and women’s satisfaction (38).
Implication for practice
Our data show the relevance of all women receiving counseling before implant insertion, that the counseling is structured and has demonstrated its effectiveness, and that health providers (midwives, nurses, and doctors) receive specific training to perform it. Informing women of the discomforts or side effects that may be associated with the implant allows them to decide in advance whether to accept them or not, improving their tolerance and adherence to the method. In addition, women can be provided with resources that mitigate these drawbacks, for example, strategies to improve libido, avoid vaginal dryness, weight changes, or fluid retention. Regarding changes in the bleeding pattern, only an excessive increase in bleeding could put the woman’s health at risk. In this case, it is suggested to rule out underlying pathology, provide drugs that relieve anemia and fatigue or pain if they appear and maintain close contact until checking how the bleeding evolves and how it affects the woman.
Strengths and limitations
This study included all women who chose the implant for contraception for one year, no woman refused to participate, which provides a reliable scenario of what happens in our community. The insertion and removal of the implant was performed in a single center so that we were able to verify the actual time of continuity with the implant, avoiding self-report recall bias. A limitation of this study is the rate of losses in the first year, 14%, which corresponded to those women who moved to other Spanish regions, a situation caused by the COVID-19 pandemic in 2020. We do not believe that these losses have substantially modified the results, but we do not know for sure. Other limitations were the exclusion of women with low proficiency in Spanish and intellectual disability has meant that two very vulnerable groups of women are not part of this research. Future research would have to establish measures to avoid this bias. This study analyzed the variable place of birth, which dichotomized women into two groups: those born in Spain and those born in other countries but did not include the variable race or ethnic group, which could have shown differences in withdrawal behavior that could be related to cultural factors. Other variables not included in the study such as sexual orientation, gender identity or experience of gender violence or belonging to the gypsy ethnic group could have improved information on vulnerable situations that can modify women’s contraceptive behavior. Finally, the design of the study prevents us from exploring the psychological or social reasons that lead women to accept or not accept the side effects of the implant. Qualitative or mixed studies could shed light on women’s contraceptive expectations and needs and on clinicians’ biases in contraceptive counseling.
Conclusion
This study shows that out of every 100 implants inserted, 17 will have been removed before one year, wasting an important part of the economic effort and health resources invested in their placement and increasing the risk of unwanted pregnancy. One factor that would significantly reduce the risk of early removal, and which is easily rectifiable, is to work toward ensuring that all women, before requesting an implant, make an appointment with the midwife at their health center for comprehensive and reliable information on the expected adverse effects.
Limitation
This is the first planned interim analysis and includes 199 women. The whole three-year cohort will (three years) be present in future studies.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by committee of La Rioja (Ref. CEImLAR P.I 386). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
RR: conceptualization, methodology, formal analysis, writing—original draft preparation, and writing—review and editing. RG-S: investigation, validation, and project administration. RU-M: investigation, validation, and writing—original draft preparation. PS-C: investigation, writing—original draft preparation, and project administration. AG-R: investigation and methodology. RJ-V: supervision. JS-G: software. AL-J: resources. ER-A: data curation. NN-E: writing—review and editing and funding. IS-A: supervision and writing—review and editing. All authors have read and agreed to the published version of the manuscript.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Birgisson, NE, Zhao, Q, Secura, GM, Madden, T, and Peipert, JF. Preventing unintended pregnancy: the contraceptive CHOICE project in review. Womens Health Rep (New Rochelle). (2015) 24:349–53. doi: 10.1089/jwh.2015.5191
2. Alomair, N, Alageel, S, Davies, N, and Bailey, JV. Factors influencing sexual and reproductive health of Muslim women: a systematic review. Reprod Health. (2020) 17:33. doi: 10.1186/s12978-020-0888-1
3. Rocca, ML, Palumbo, AR, Visconti, F, and Di Carlo, C. Safety and benefits of contraceptives implants: a systematic review. Pharmaceuticals. (2021) 14:1–26. doi: 10.3390/ph14060548
4. Moray, KV, Chaurasia, H, Sachin, O, and Joshi, B. A systematic review on clinical effectiveness, side-effect profile and meta-analysis on continuation rate of etonogestrel contraceptive implant. Reprod Health. (2021) 18:4–24. doi: 10.1186/s12978-020-01054-y
5. Teunissen, AM, Grimm, B, and Roumen, FJME. Continuation rates of the subdermal contraceptive Implanon® and associated influencing factors. Eur J Contracept Reprod Heal Care. (2014) 19:15–21. doi: 10.3109/13625187.2013.862231
6. Arribas-Mir, L, Rueda-Lozano, D, Agrela-Cardona, M, Cedeño-Benavides, T, Olvera-Porcel, C, and Bueno-Cavanillas, A. Insertion and 3-year follow-up experience of 372 etonogestrel subdermal contraceptive implants by family physicians in Granada. Spain Contraception. (2009) 80:457–62. doi: 10.1016/j.contraception.2009.04.003
7. Ramdhan, RC, Simonds, E, Wilson, C, Loukas, M, Oskouian, RJ, and Tubbs, RS. Complications of subcutaneous contraception: a review. Cureus. (2018) 10:e2132. doi: 10.7759/cureus.2132
8. Flore, M, Chen, X, Bonney, A, Mullan, J, Dijkmans-Hadley, B, Hodgkins, A, et al. Patients’ perspectives about why they have their contraceptive Implanon NXT device removed early. Aust Fam Physician. (2016) 45:740–4.
9. Apter, D, Briggs, P, Tuppurainen, M, Grunert, J, Lukkari-Lax, E, Rybowski, S, et al. A 12-month multicenter, randomized study comparing the levonorgestrel intrauterine system with the etonogestrel subdermal implant. Fertil Steril. (2016) 106:151–157.e5. doi: 10.1016/j.fertnstert.2016.02.036
10. World Health Organization (WHO). Medical eligibility criteria for contraceptive use. 5th ed. Geneva: World Health Organization (2015). 276 p.
11. Sociedad Española de contracepcion (SEC). Encuesta de anticoncepción en España (2020). Available at: https://hosting.sec.es/descargas/Encuesta_anticoncepcion2020.pdf
12. Mazza, D, Amos, N, Watson, CJ, McGeechan, K, Haas, M, Peipert, JF, et al. Increasing the uptake of long-acting reversible contraception in general practice: the Australian contraceptive ChOice pRoject (ACCORd) cluster randomised controlled trial longitudinal follow-up protocol. BMJ Open. (2020) 10:e035895. doi: 10.1136/bmjopen-2019-035895
13. Trussell, J, Hassan, F, Lowin, J, Law, A, and Filonenko, A. Achieving cost-neutrality with long-acting reversible contraceptive methods. Contraception. (2015) 91:49–56. doi: 10.1016/j.contraception.2014.08.011
14. Madden, T, Mullersman, JL, Omvig, KJ, Secura, GM, and Peipert, JF. Structured contraceptive counseling provided by the contraceptive CHOICE project. Contraception. (2013) 88:243–9. doi: 10.1016/j.contraception.2012.07.015
15. National Institute for Health and Care Excellence (NICE). (2021). Shared decision making. NICE Guideline. Available at: https://www.nice.org.uk/guidance/ng197
16. Ruiz de Viñaspre-Hernández, R, Garrido-Santamaria, R, Urra-Martínez, R, Sáenz-Cabredo, P, Martínez-Tofe, J, Burgos-Esteban, A, et al. Transcultural adaptation and validation of the Spanish version of the sexual satisfaction scale for women (SSS-W-E). Int J Environ Res Public Health. (2021) 18:9663. doi: 10.3390/ijerph18189663
17. Reyes-Lacalle, A, Montero-Pons, L, Manresa-Domínguez, JM, Cabedo-Ferreiro, R, Seguranyes, G, and Falguera-Puig, G. Perinatal contraceptive counseling: effectiveness of a reinforcement intervention on top of standard clinical practice. Midwifery. (2020) 83:102631. doi: 10.1016/j.midw.2020.102631
18. Politi, MC, Estlund, A, Milne, A, Buckel, CM, Peipert, JF, and Madden, T. Barriers and facilitators to implementing a patient-centered model of contraceptive provision in community health centers. Contracept Reprod Med. (2016) 1:21. doi: 10.1186/s40834-016-0032-3
19. Lasa, IL. Eficacia, seguridad y tolerabilidad del implante anticonceptivo de varilla única con etonogestrel. Progresos Obstet y Ginecol. (2020) 63:81–93.
20. Loder, C, Hall, K, Kusunoki, Y, Harris, LH, and Dalton, V. Associations between perceived discrimination and contraceptive method use: why we need better measures of discrimination in reproductive healthcare. Women Heal. (2021) 61:461–9. doi: 10.1080/03630242.2021.1919816
21. Peipert, JF, Zhao, Q, Allsworth, JE, Petrosky, E, Madden, T, Eisenberg, D, et al. Continuation and satisfaction of reversible contraception. Obstet Gynecol. (2011) 117:1105–13. doi: 10.1097/AOG.0b013e31821188ad
22. Lozano, M, Obiol, MA, Peiró, J, and Ramada, JM. Effect of cost on early removal of contraceptive implants: a prospective cohort study. Eur J Contracept Reprod Heal Care. (2019) 24:24–9. doi: 10.1080/13625187.2018.1564817
23. McNicholas, C, Madden, T, Secura, G, and Peipert, JF. The contraceptive CHOICE project round up. Clin Obstet Gynecol. (2014) 57:635–43. doi: 10.1097/GRF.0000000000000070
24. Zapata, LB, Pazol, K, Dehlendorf, C, Curtis, KM, Malcolm, NM, Rosmarin, RB, et al. Contraceptive counseling in clinical settings: an updated systematic review. Am J Prev Med. (2018) 55:677–90. doi: 10.1016/j.amepre.2018.07.006
25. Hendrick, CE, Cone, JN, Cirullo, J, and Maslowsky, J. Determinants of long-acting reversible contraception (LARC) initial and continued use among adolescents in the United States. Adolesc Res Rev. (2020) 5:243–79. doi: 10.1007/s40894-019-00126-w
26. Berlan, E, Mizraji, K, and Bonny, AE. Twelve-month discontinuation of etonogestrel implant in an outpatient pediatric setting. Contraception. (2016) 94:81–6. doi: 10.1016/j.contraception.2016.02.030
27. Rosenstock, JR, Peipert, JF, Madden, T, Zhao, Q, and Secura, GM. Continuation of reversible contraception in teenagers and young women. Obstet Gynecol. (2012) 120:1298–305. doi: 10.1097/AOG.0b013e31827499bd
28. Chace Dwyer, S, Baruwa, S, Okafor, E, Daini, BO, Ubuane, O, and Jain, A. How do changes in motivation to prevent pregnancy influence contraceptive continuation? Results from a longitudinal study with women who receive family planning services from community pharmacists and patent and proprietary medicine vendors in Nigeria. Reprod Health. (2022) 19:39. doi: 10.1186/s12978-022-01326-9
29. Davia, MÁ, and Legazpe, N. Factores determinantes en la decisión de tener el primer hijo en las mujeres españolas. Papeles de población. (2013) 19:183–212.
30. Zigler, RE, and McNicholas, C. Unscheduled vaginal bleeding with progestin-only contraceptive use. Am J Obstet Gynecol. (2017) 216:443–50. doi: 10.1016/j.ajog.2016.12.008
31. Lazorwitz, A, Aquilante, CL, Dindinger, E, Harrison, M, Sheeder, J, and Teal, S. Relationship between Etonogestrel concentrations and bleeding patterns in contraceptive implant users. Obstet Gynecol. (2019) 134:807–13. doi: 10.1097/AOG.0000000000003452
32. Gallo, MF, Legardy-Williams, J, Hylton-Kong, T, Rattray, C, Kourtis, AP, Jamieson, DJ, et al. Association of Progestin Contraceptive Implant and Weight Gain. Obstet Gynecol. (2016) 127:573–6. doi: 10.1097/AOG.0000000000001289
33. Robakis, T, Williams, KE, Nutkiewicz, L, and Rasgon, NL. Hormonal contraceptives and mood: review of the literature and implications for future research. Curr Psychiatry Rep. (2019) 21:57. doi: 10.1007/s11920-019-1034-z
34. Kuntz, K, McCullough, S, Beach, P, and Lyon, C. Do progesterone-only contraceptives lead to more mood changes than other types? J Fam Pract. (2016) 65:938–43.
35. Caruso, S, Palermo, G, Caruso, G, and Rapisarda, AMC. How does contraceptive use affect Women’s sexuality? A novel look at sexual acceptability. J Clin Med. (2022) 11:810. doi: 10.3390/jcm11030810
36. Lazorwitz, A, Dindinger, E, Harrison, M, Aquilante, CL, Sheeder, J, and Teal, S. An exploratory analysis on the influence of genetic variants on weight gain among etonogestrel contraceptive implant users. Contraception. (2020) 102:180–5. doi: 10.1016/j.contraception.2020.05.002
37. Nappi, RE, Vermuyten, N, and Bannemerschult, R. Missed opportunities in contraceptive counseling: findings from a European survey-based study with simulated patient consultation. Eur J Contracept Reprod Heal Care. (2022) 27:85–94. doi: 10.1080/13625187.2021.2010040
Keywords: etonogestrel, contraceptive, implant, early removal, cohort study
Citation: Ruiz de Viñaspre-Hernández R, Garrido-Santamaria R, Urra-Martínez R, Sáenz-Cabredo P, Garrido-Rivas AE, Juárez-Vela R, Sánchez-González JL, Lafuente-Jimenez A, Ramón-Arbués E, Navas-Echazarreta N and Santolalla-Arnedo I (2024) Early removal of the etonogestrel contraceptive implant in Spanish women: a prospective cohort study. Front. Med. 11:1172793. doi: 10.3389/fmed.2024.1172793
Edited by:
Anne E. Burke, Johns Hopkins University, United StatesCopyright © 2024 Ruiz de Viñaspre-Hernández, Garrido-Santamaria, Urra-Martínez, Sáenz-Cabredo, Garrido-Rivas, Juárez-Vela, Sánchez-González, Lafuente-Jimenez, Ramón-Arbués, Navas-Echazarreta and Santolalla-Arnedo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Noelia Navas-Echazarreta, bm9lbGlhLm5hdmFzQHVuaXJpb2phLmVz