 Shijun Xia
Shijun Xia Lidan Luo
Lidan Luo- Shenzhen Hospital of Guangzhou University of Chinese Medicine, Shenzhen, China
Background: Pudendal nerve block (PNB) is a commonly used anesthesia method that has been widely used in postoperative analgesia for hemorrhoids in recent years. Therefore, we conducted a systematic review and meta-analysis of double-blind randomized controlled trials (RCTs) to analyze the effectiveness of PNB in postoperative analgesia for hemorrhoids.
Methods: Relevant data and studies published from inception until August 14, 2023, were retrieved from PubMed, Embase, and Web of Science to evaluate the beneficial effects of PNB for analgesia following hemorrhoidectomy.
Results: This meta-analysis included 6 double-blind RCTs comprising 501 patients. We evaluated the function of PNB in improving outcomes of postoperative analgesia of hemorrhoids. Visual analogue scale (VAS) scores on postoperative within 6 h (MD, −3.04; 95% CI, −4.13 to −1.95; P < 0.0001), 12 h (MD, −3.14; 95% CI, −3.87 to −2.40; P < 0.0001), and 24 h (MD, −2.25; 95% CI, −2.95 to −1.55; P < 0.0001) were enhanced by the application of PNB, but not in 48 h (MD, −2.54; 95% CI, −5.29 to 0.20; P = 0.07).
Conclusion: Pudendal nerve block (PNB) could effectively relieve postoperative pain of hemorrhoids. However, our results still need to be confirmed by multi-center clinical studies.
1 Introduction
Hemorrhoids are normal vascular structures in the anal canal. Approximately 5% of the general population suffers from hemorrhoidal disease (1), the cardinal features of which include bleeding, anal pruritus, prolapse, and pain due to thrombosis or inflammatory crisis. Most patients with hemorrhoidal disease initially undergo conservative treatment. In cases where internal medicine treatment is unsuccessful, non-surgical outpatient treatment procedures may be suitable. Only patients with persistent symptoms after conservative or outpatient treatment are considered candidates for surgical intervention.
Pain after hemorrhoidectomy is extremely common and is caused, to some extent, by spasms of the anal sphincter (2). The first-choice medication for controlling postoperative pain includes oral analgesics, such as non-steroidal anti-inflammatory drugs and acetaminophen (3). When these analgesics are ineffective for pain control, opioid drugs can be used; however, they may cause adverse reactions such as constipation. The PROSPECT group recommends the application of a pudendal nerve block (PNB) to relieve postoperative pain in patients who have undergone hemorrhoidectomy (4).
The pudendal nerve is a mixed sensory and motor nerve originating from the S2, S3, and S4 nerve roots of the sacral plexus (5). It exits the pelvis through the greater sciatic foramen and then re-enters the perineum, passing through the ischiorectal fossa and Alcock’s canal. Here, the pudendal nerve is accompanied by pudendal blood vessels and splits into three branches. The pudendal nerve innervates the urethral muscles, clitoris, penis, perineum, pelvic floor sphincters, urethra, and bladder triangle (6, 7).
Pudendal nerve blocks (PNBs) are suitable for postoperative pain relief following hemorrhoidectomy and are considered an optional pain management strategy. Multiple randomized trials have been published on PNBs, confirming a longer analgesic duration and lower incidence of complications compared with the abovementioned drugs (8, 9). Although some systematic reviews and meta-analyses support the analgesic effect of PNBs in hemorrhoid surgery (10, 11), most of them are based on low-quality research data.
Therefore, we expanded the search scope and performed an updated meta-analysis based on all published double-blind randomized controlled trials to evaluate the beneficial effects of PNBs for analgesia following hemorrhoidectomy.
2 Materials and methods
This systematic review and meta-analysis was performed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines (12). Ethical approval or informed consent was not required.
2.1 Search strategy
We searched the PubMed, Embase, and Web of Science electronic databases for English articles from database inception until August 14, 2023. The following search terms were used: (“pudend*” or “ischiorectal”) and (“anesthesia” or “anaesthesia”), and (“hemorrhoids” or “haemorrhoid” or “hemorrhoidectomy” or “haemorrhoidectomy”). The search strategy was implemented using a combination of index words and free-text keywords.
2.2 Eligibility criteria
Two researchers (LL and KL) analyzed and independently reviewed all studies retrieved through the literature search. Any disagreements were resolved through discussion. The inclusion criteria were as follows: (1) double-blind randomized controlled trials, (2) investigation of patients with hemorrhoidal disease, (3) comparison of PNBs with any other treatment, and (4) studies published in English. The exclusion criteria were as follows: (1) studies involving participants with non-hemorrhoidal disease and (2) those involving perianal blocks. Following the application of the inclusion and exclusion criteria, a full-text evaluation of the remaining potentially eligible studies was conducted to determine whether they should be included in the analysis. Additionally, the reference lists of the evaluated full-text articles were reviewed to make the search more comprehensive.
2.3 Data collection and outcomes
Data for each eligible study were extracted, including the title, author, year, country, grouping method, number of patients, randomization type, blinding method, PNB technique, and postoperative pain data. The primary endpoint pain was postoperative pain. This was measured using a visual analog scale (VAS), which scored perceived pain on a level of 0–10 during rest, walking, sitting, or the first bowel movement.
2.4 Quality assessment
An independent review of bias risk and research quality was conducted based on the Cochrane Collaboration tool for assessing risk of bias (13).
2.5 Statistical methods
Review Manager v5.3 (Nordic Cochrane Center, Cochrane Collaboration, London, UK) was used for data analysis. We calculated the intergroup standardized mean difference (SMD) for each study as an estimate of effectiveness. In case of missing data, the mean and standard deviation (SD) were estimated based on the median, range, and interquartile values (14, 15). I2 values were used to classify heterogeneity as follows: no heterogeneity, I2 < 25%; low heterogeneity, 25% ≤ I2 < 50%; moderate heterogeneity, 50% ≤ I2 < 75%; and high heterogeneity, I2 ≥ 75%. When the I2 value was < 50%, the fixed effects model was used, whereas the random effects model was used when the I2 value was > 50%.
3 Results
3.1 Selected studies
Figure 1 describes the process of literature retrieval and screening. A total of 611 studies were retrieved, of which 453 were evaluated after eliminating duplications. Further, 401 studies were excluded because they did not meet the inclusion criteria, and only 6 (16–21) of the remaining 13 potential studies were ultimately included in this study. These 6 studies were published between 2000 and 2020, and included 501 patients from 6 countries, with a sample size of 20–200. The PNB procedure was achieved in one study under ultrasound guidance, in two studies under nerve stimulation and in the other three under anatomic landmarks (Table 1).
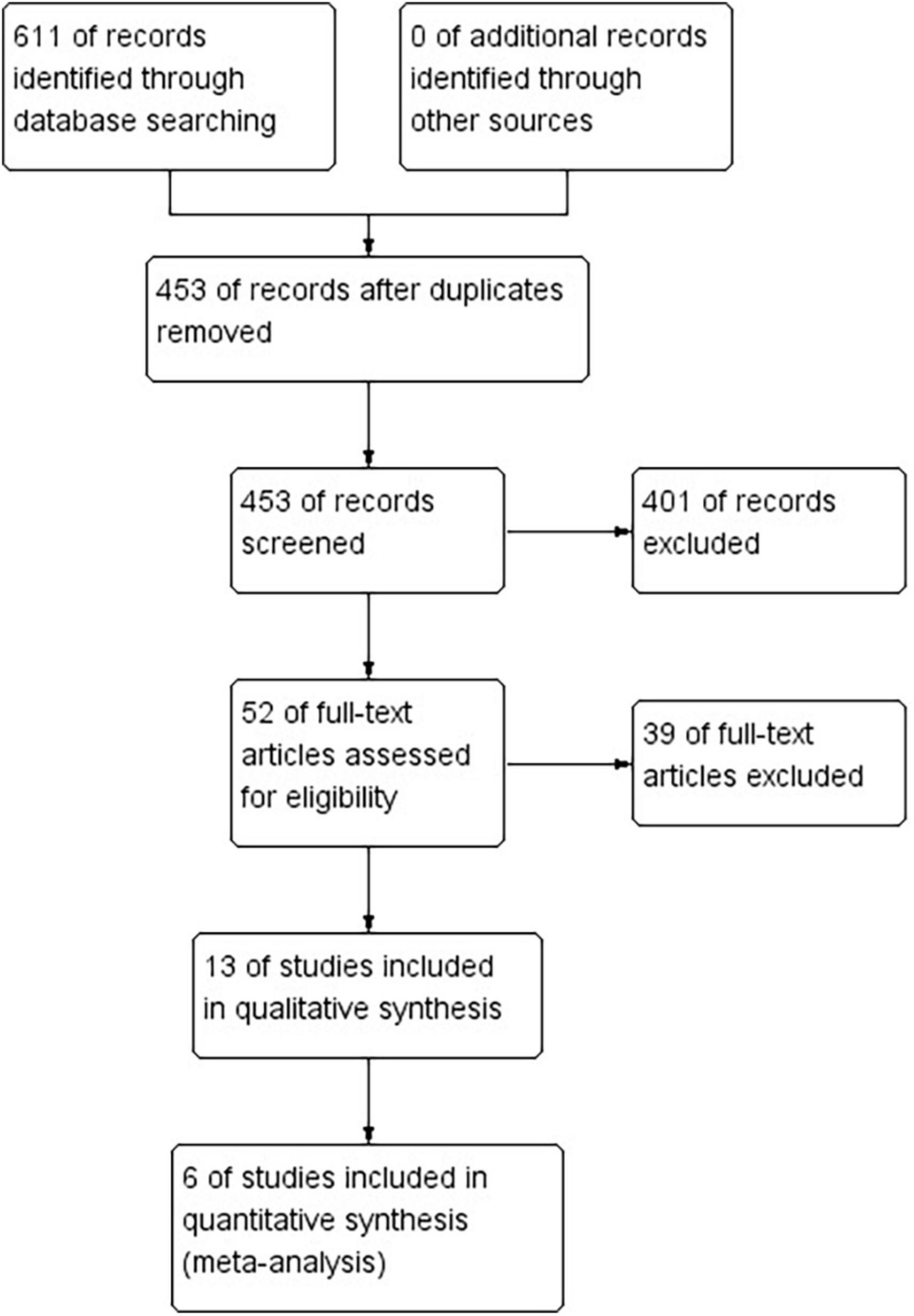
Figure 1. PRISMA flow diagram of study selection.
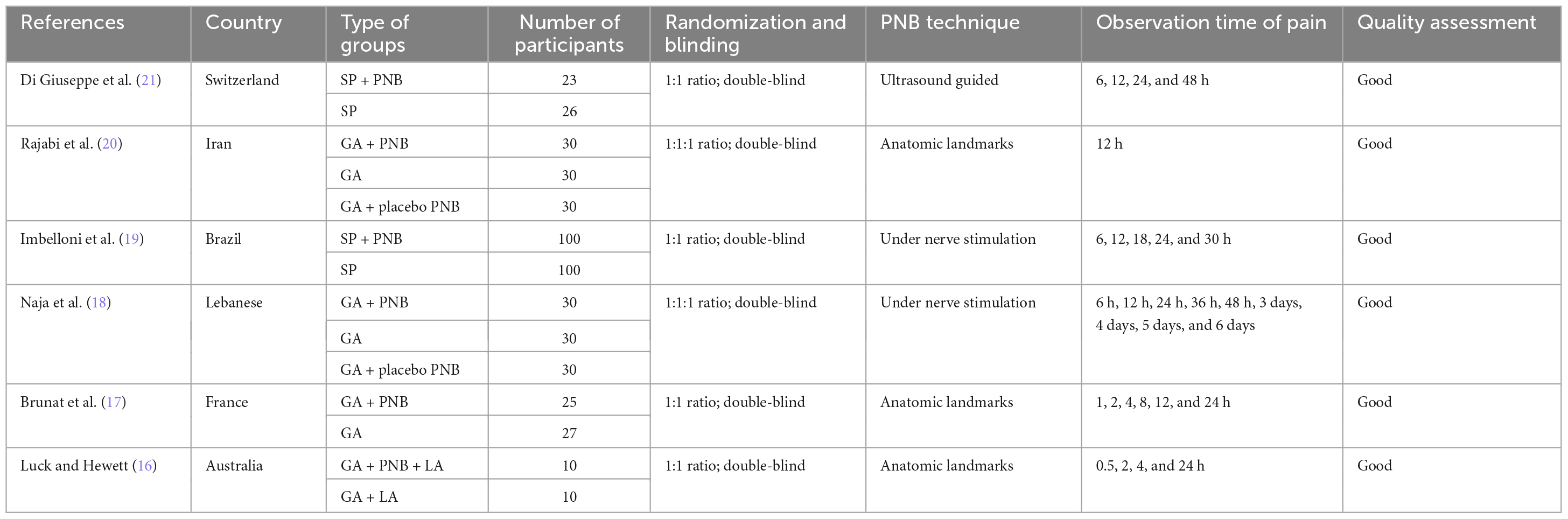
Table 1. Characteristics of the included trials.
3.2 Quality assessment
Figures 2, 3 present the results of the Cochrane risk of bias tool. Considering the nature of the intervention, all studies were not conducted blind analysis of researchers.
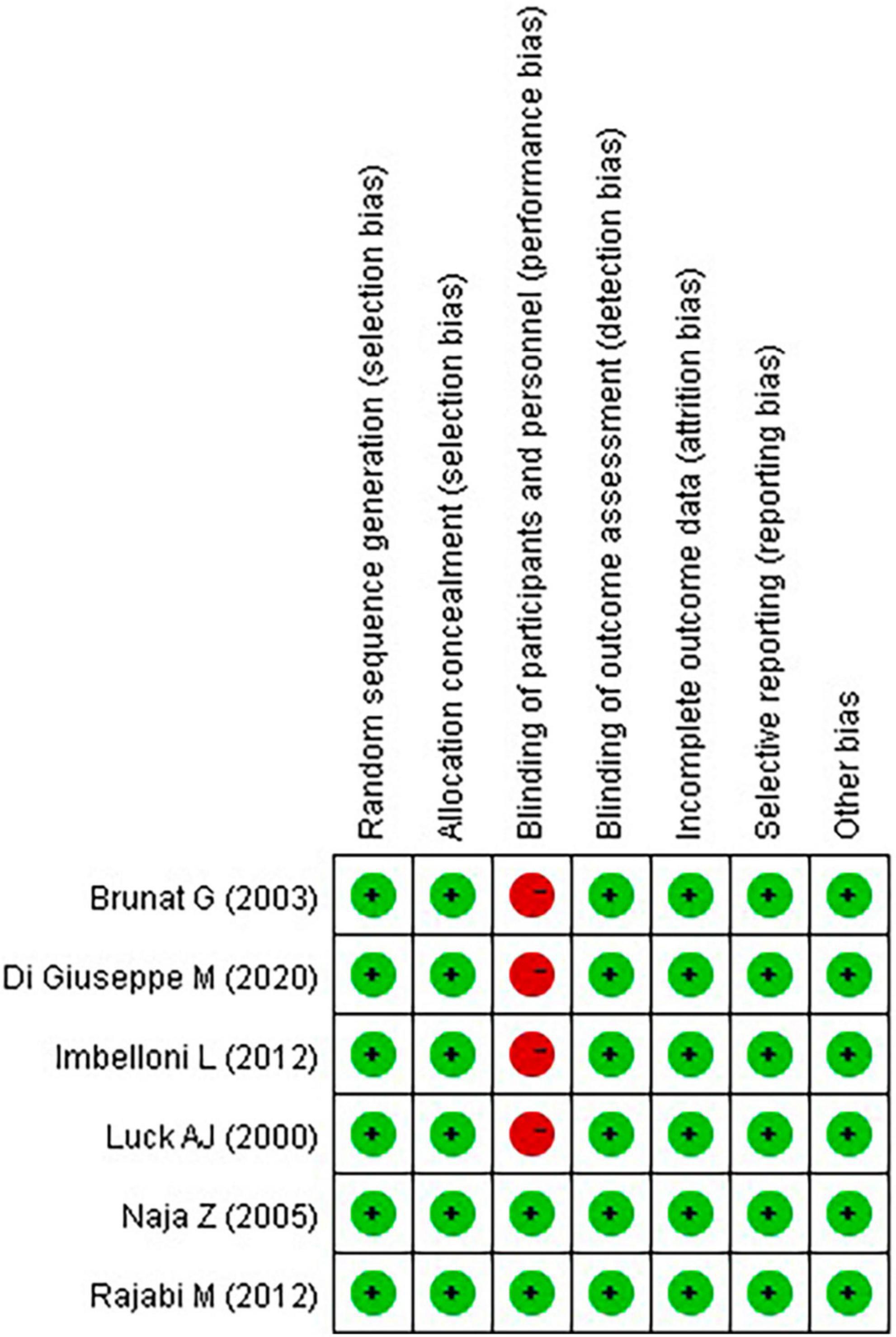
Figure 2. Summary of the risk of bias.
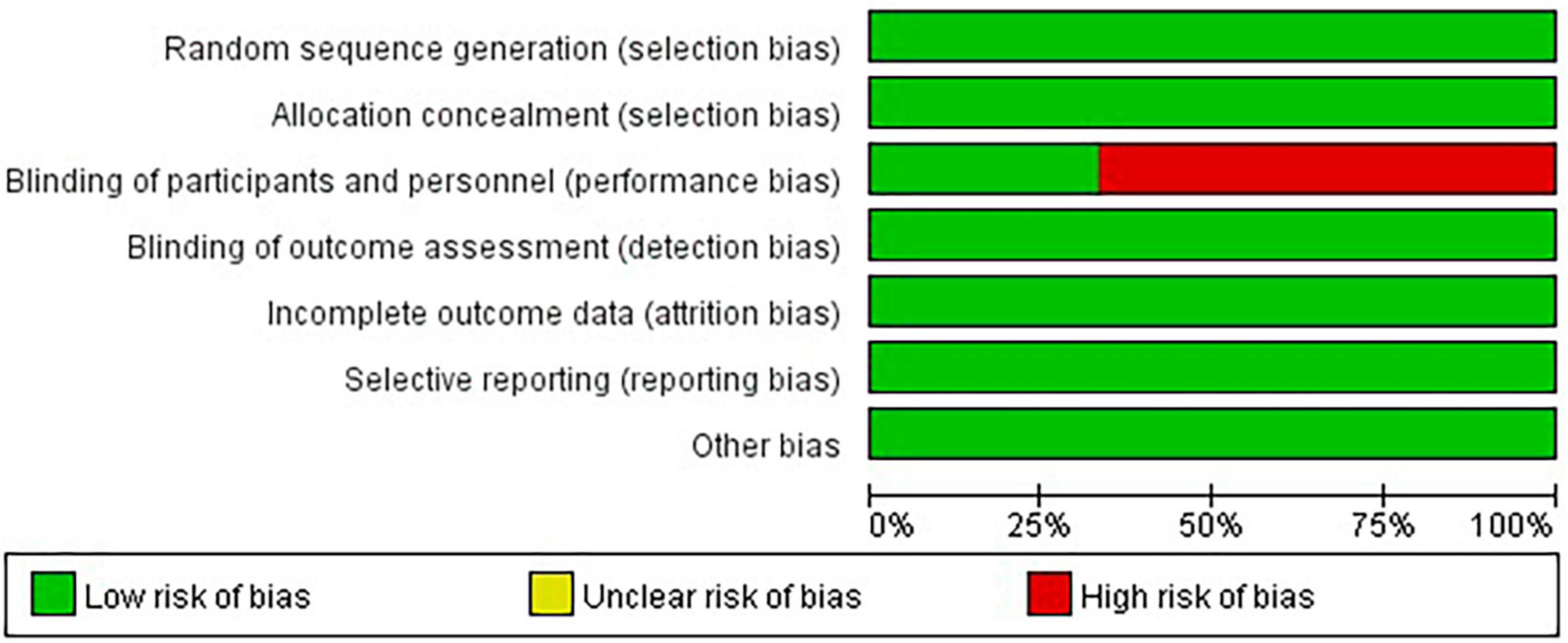
Figure 3. Graph of the risk of bias.
3.3 Outcomes
For each study, we compared the VAS scores at different time points between the experimental and control groups to evaluate the differences in analgesic effects between the two groups.
3.4 Pain within 6 h on the VAS
According to the studies by Brunat et al. (17), Di Giuseppe et al. (21), Imbelloni et al. (19), Luck and Hewett (16), and Naja et al. (18), VAS scores within 6 h of hemorrhoidectomy were lower in the experimental group than in the control group (MD, −3.04; 95% confidence interval [CI], −4.13 to −1.95; P < 0.0001; I2 = 95%) (Figure 4).
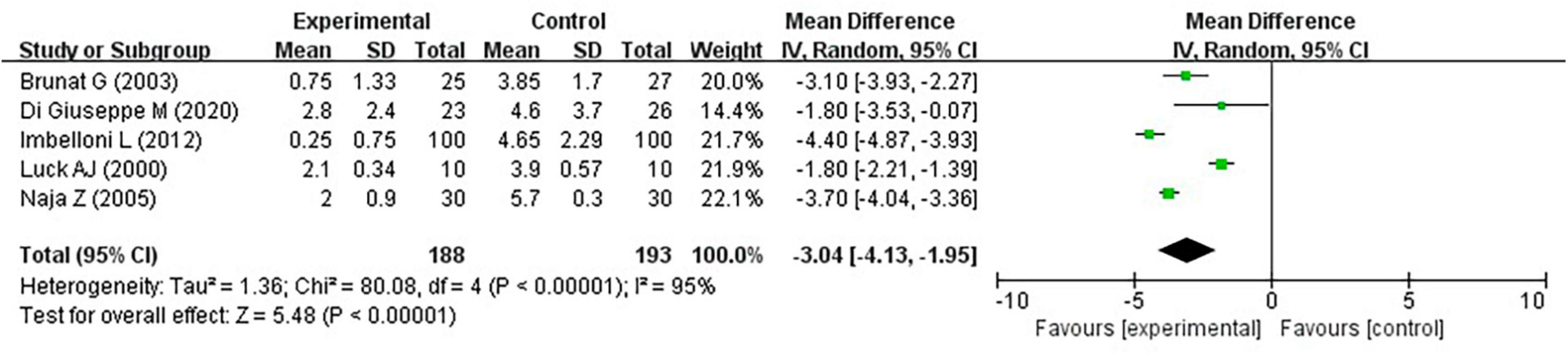
Figure 4. Pain within 6 h on the VAS.
3.5 Pain at 12 h on the VAS
Brunat et al. (17), Di Giuseppe et al. (21), Imbelloni et al. (19), Naja et al. (18), and Rajabi et al. (20) reported that the VAS score at 12 h after hemorrhoidectomy was lower in the experimental group than in the control group (MD, −3.14; 95% CI, −3.87 to −2.40; P < 0.0001; I2 = 82%) (Figure 5).
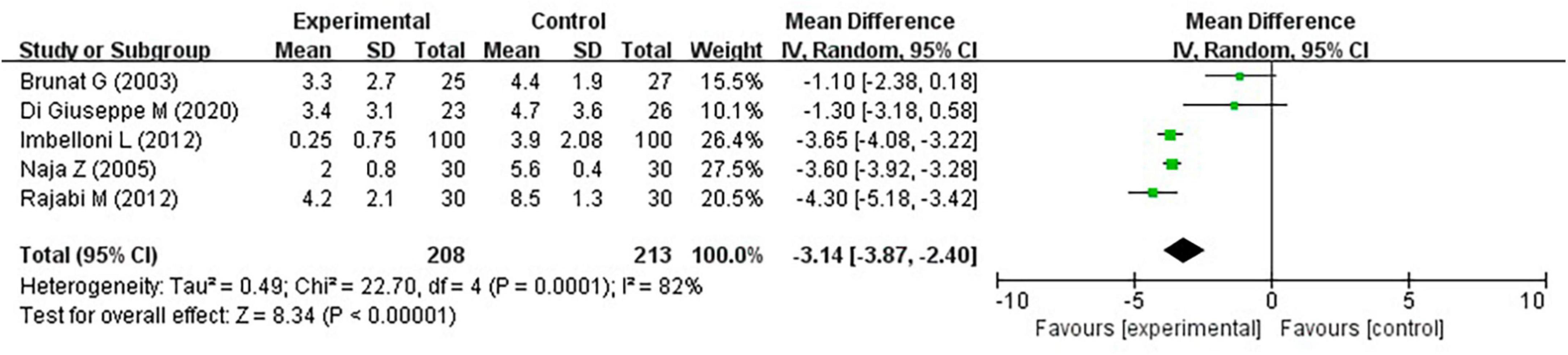
Figure 5. Pain at 12 h on the VAS.
3.6 Pain at 24 h on the VAS
Brunat et al. (17), Di Giuseppe et al. (21), Imbelloni et al. (19), Luck and Hewett (16), and Naja et al. (18), reported that the VAS score at 24 h after hemorrhoidectomy was also lower in the experimental group (MD, −2.25; 95% CI, −2.95 to −1.55; P < 0.0001; I2 = 88%) (Figure 6).
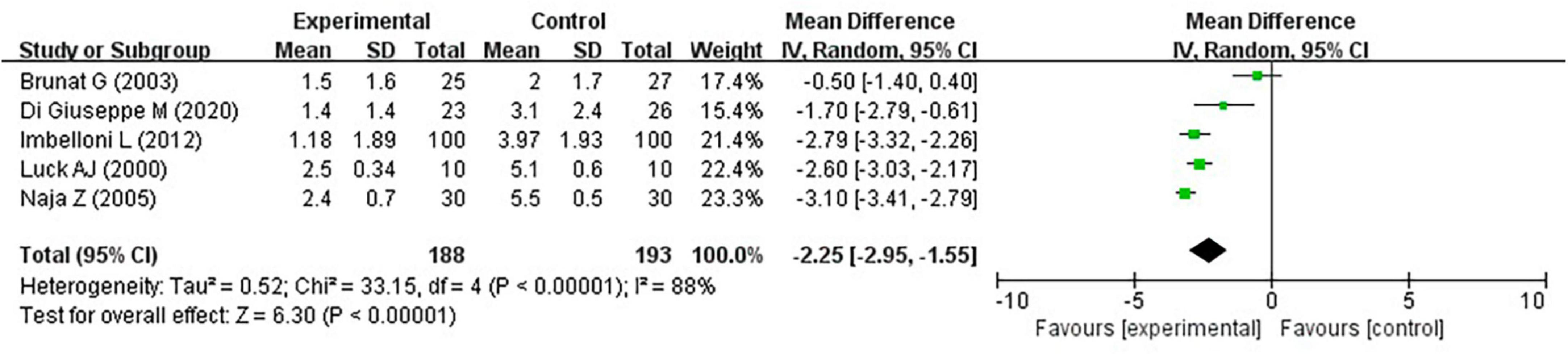
Figure 6. Pain at 24 h on the VAS.
3.7 Pain at 48 h on the VAS
However, at 48 h after hemorrhoidectomy, Di Giuseppe et al. (21) and Naja et al. (18) reported no difference in VAS scores between the experimental and control groups (MD, −2.54; 95% CI, −5.29 to 0.20; P = 0.07; I2 = 96%) (Figure 7).

Figure 7. Pain at 48 h on the VAS.
3.8 Publication bias
As the number of included studies was < 10, we could not evaluate publication bias.
4 Discussion
Our systematic review and meta-analysis based on six high-quality double-blind randomized controlled trials revealed that the use of PNBs in patients undergoing hemorrhoidectomy can reduce pain within 6, 12, and 24 h after surgery, but it is ineffective 48 h after surgery. Thus, our findings support the wider use of PNBs in hemorrhoidectomy.
Hemorrhoids are detected in many anorectal diseases. Although surgery is the most effective treatment method, postoperative pain is one of the main reasons attributed to surgery refusal (22). The main sources of post-hemorrhoidectomy pain are the surgical incision site, perianal skin, and areas of mucosal edema (23). Because the perineum is extremely sensitive, patients undergoing hemorrhoidectomy always experience severe postoperative pain. Perioperative analgesia mainly relies on local anesthesia and painkillers (24) as well as local application of diltiazem (25) and injections of botulinum toxin (26) or metronidazole (topical or oral) (27, 28). Tail or spinal anesthesia can also relieve pain, but the analgesic effect is short-lived, often accompanied with side effects, particularly urinary retention (29). Local infiltration can alleviate postoperative pain in patients undergoing hemorrhoid surgery, but this pain relief only lasts for 5–12 h (30, 31). Further, improvement in their analgesic effects remains unsatisfactory.
Pudendal nerve blocks (PNBs) are mainly used for anorectal diseases, and they alleviate pain by blocking the anal nerve at the bifurcation of the pubic nerve. Due to its anatomical structure, PNBs can be an effective post-hemorrhoidectomy analgesic method. Complications related to PNB surgery, such as intravenous anesthesia, permanent nerve injury, hematoma, and abscess, have never been described in relevant literature searches, although there may be reporting bias. A meta-analysis not only confirmed the highly beneficial safety of PNBs but also showed that the incidence of nausea and vomiting were significantly reduced (10). PNBs were also reported to reduce the incidence of urinary retention (11), which is a relatively common complication after hemorrhoid surgery that may hinder outpatient treatment.
This study has some limitations. The most relevant limitation is related to publication bias and heterogeneity, with high I2 values in various studies. Furthermore, the sample size included in some studies was relatively small, which may cause bias. Finally, in cases of missing data, the impact was estimated using mean and SD, which may not accurately reflect the original data.
5 Conclusion
Our meta-analysis and systematic review of the studies extracted from the literature revealed that the use of PNBs in patients undergoing hemorrhoidectomy has a significant advantage in alleviating postoperative pain. Despite the limitations, all patients undergoing hemorrhoidectomy should consider treatment with PNB.
Data availability statement
Publicly available datasets were analyzed in this study. This data can be found here: https://pubmed.ncbi.nlm.nih.gov/.
Author contributions
SX: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Writing – original draft, Writing – review & editing. LL: Data curation, Formal analysis, Software, Writing – review & editing. WW: Conceptualization, Writing – review & editing, Writing – original draft. KL: Data curation, Software, Writing – review & editing. TJ: Data curation, Software, Writing – review & editing. YL: Data curation, Writing – review & editing.
Funding
The authors declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
PNB, pudendal nerve block; RCTs, randomized controlled trials; SD, standard deviation; SMD, standardized mean difference; VAS, visual analog scale.
References
1. Sneider E, Maykel J. Diagnosis and management of symptomatic hemorrhoids. Surg Clin North Am. (2010) 90:17–32. doi: 10.1016/j.suc.2009.10.005
2. Jin J, Unasa H, Bahl P, Mauiliu-Wallis M, Svirskis D, Hill A. Can targeting sphincter spasm reduce post-haemorrhoidectomy pain? A systematic review and meta-analysis. World J Surg. (2023) 47:520–33. doi: 10.1007/s00268-022-06807-3
3. Joshi G, Neugebauer E. Evidence-based management of pain after haemorrhoidectomy surgery. Br J Surg. (2010) 97:1155–68. doi: 10.1002/bjs.7161
4. Sammour T, Barazanchi A, Hill A. Evidence-Based Management of Pain After Excisional Haemorrhoidectomy Surgery: A PROSPECT Review Update. World J Surg. (2017) 41:603–14. doi: 10.1007/s00268-016-3737-1
5. Alkhaldi H, Salaita W, Shabaneh M, Al-Horut M, Aldabbas R, Uraiqat A. Postoperative outcome comparison between pudendal nerve block and caudal block after lateral open internal sphincterotomy. Med Arch. (2015) 69:187–9. doi: 10.5455/medarh.2015.69.187-189
6. Romanzi L. Techniques of pudendal nerve block. J Sex Med. (2010) 7:1716–9. doi: 10.1111/j.1743-6109.2010.01822.x
7. Imbelloni L, Beato L, Beato C, Cordeiro J, de Souza D. Bilateral pudendal nerves block for postoperative analgesia with 0.25% S75:R25 bupivacaine. Pilot study on outpatient hemorrhoidectomy. Rev Bras Anestesiol. (2005) 55:614–21. doi: 10.1590/s0034-70942005000600004
8. Nadri S, Mahmoudvand H, Rokrok S, Tarrahi M. Comparison of two methods: spinal anesthesia and ischiorectal block on post hemorrhoidectomy pain and hospital stay: a randomized control trial. J Invest Surg. (2018) 31:420–4. doi: 10.1080/08941939.2017.1349221
9. He J, Zhang L, Li D, He W, Xiong Q, Zheng X, et al. Ultrasound-guided pudendal nerve block combined with propofol deep sedation versus spinal anesthesia for hemorrhoidectomy: a prospective randomized study. Pain Res Manag. (2021) 2021:6644262. doi: 10.1155/2021/6644262
10. Mongelli F, Treglia G, La Regina D, Di Giuseppe M, Galafassi J, Majno-Hurst P, et al. Pudendal Nerve Block in Hemorrhoid Surgery: A Systematic Review and Meta-analysis. Dis Colon Rectum. (2021) 64:617–31. doi: 10.1097/DCR.0000000000001985
11. Li J, Liu H, Qin K, Liu M, Yang H, Li Y. Efficacy and safety of pudendal nerve block for postoperative analgesia of hemorrhoids: a systematic review of 7 randomized controlled trials. Ann Palliat Med. (2021) 10:2283–92. doi: 10.21037/apm-20-2109
12. Moher D, Liberati A, Tetzlaff J, Altman D. Reprint–preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Phys Ther. (2009) 89:873–80.
13. Higgins J, Altman D, Gøtzsche P, Jüni P, Moher D, Oxman A, et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ. (2011) 343:d5928. doi: 10.1136/bmj.d5928
14. Walter S, Yao X. Effect sizes can be calculated for studies reporting ranges for outcome variables in systematic reviews. J Clin Epidemiol. (2007) 60:849–52. doi: 10.1016/j.jclinepi.2006.11.003
15. Wan X, Wang W, Liu J, Tong T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med Res Methodol. (2014) 14:135. doi: 10.1186/1471-2288-14-135
16. Luck A, Hewett P. Ischiorectal fossa block decreases posthemorrhoidectomy pain: randomized, prospective, double-blind clinical trial. Dis Colon Rectum. (2000) 43:142–5. doi: 10.1007/BF02236970
17. Brunat G, Pouzeratte Y, Mann C, Didelot J, Rochon J, Eledjam J. Posterior perineal block with ropivacaine 0.75% for pain control during and after hemorrhoidectomy. Reg Anesth Pain Med. (2003) 28:228–32. doi: 10.1053/rapm.2003.50132
18. Naja Z, Ziade M, Lönnqvist P. Nerve stimulator guided pudendal nerve block decreases posthemorrhoidectomy pain. Can J Anaesth. (2005) 52:62–8. doi: 10.1007/BF03018582
19. Imbelloni L, Vieira E, Carneiro A. Postoperative analgesia for hemorrhoidectomy with bilateral pudendal blockade on an ambulatory patient: a controlled clinical study. J Coloproctol. (2012) 32:291–6.
20. Rajabi M, Hosseinpour M, Jalalvand F, Afshar M, Moosavi G, Behdad S. Ischiorectal block with bupivacaine for post hemorrhoidectomy pain. Korean J Pain. (2012) 25:89–93. doi: 10.3344/kjp.2012.25.2.89
21. Di Giuseppe M, Saporito A, La Regina D, Tasciotti E, Ghielmini E, Vannelli A, et al. Ultrasound-guided pudendal nerve block in patients undergoing open hemorrhoidectomy: a double-blind randomized controlled trial. Int J Colorectal Dis. (2020) 35:1741–7. doi: 10.1007/s00384-020-03630-x
22. Engel A, Eijsbouts Q. Haemorrhoidectomy: painful choice. Lancet. (2000) 355:2253–4. doi: 10.1016/S0140-6736(05)72753-7
23. Pattana-Arun J, Sooriprasoet N, Sahakijrungruang C, Tantiphlachiva K, Rojanasakul A. Closed vs ligasure hemorrhoidectomy: a prospective, randomized clinical trial. J Med Assoc Thai. (2006) 89:453–8.
24. Acheson A, Scholefield J. Management of haemorrhoids. BMJ. (2008) 336:380–3. doi: 10.1136/bmj.39465.674745.80
25. Silverman R, Bendick P, Wasvary HJ. A randomized, prospective, double-blind, placebo-controlled trial of the effect of a calcium channel blocker ointment on pain after hemorrhoidectomy. Dis Colon Rectum. (2005) 48:1913–6. doi: 10.1007/s10350-005-0135-4
26. Patti R, Almasio P, Muggeo V, Buscemi S, Arcara M, Matranga S, et al. Improvement of wound healing after hemorrhoidectomy: a double-blind, randomized study of botulinum toxin injection. Dis Colon Rectum. (2005) 48:2173–9. doi: 10.1007/s10350-005-0179-5
27. Ala S, Saeedi M, Eshghi F, Mirzabeygi P. Topical metronidazole can reduce pain after surgery and pain on defecation in postoperative hemorrhoidectomy. Dis Colon Rectum. (2008) 51:235–8. doi: 10.1007/s10350-007-9174-3
28. Lyons N, Cornille J, Pathak S, Charters P, Daniels I, Smart N. Systematic review and meta-analysis of the role of metronidazole in post-haemorrhoidectomy pain relief. Colorectal Dis. (2017) 19:803–11. doi: 10.1111/codi.13755
29. Kim J, Lee D, Jang S, Shim M, Jee D. The effect of pudendal block on voiding after hemorrhoidectomy. Dis Colon Rectum. (2005) 48:518–23. doi: 10.1007/s10350-004-0798-2
30. Jinjil K, Dwivedi D, Bhatnagar V, Ray R, Tara S. Perianal Block: Is It as Good as Spinal Anesthesia for Closed Hemorrhoidectomies? Anesth Essays Res. (2018) 12:36–41. doi: 10.4103/aer.AER_225_17
Keywords: hemorrhoid, surgery, pudendal nerve block, anesthesia, visual analog scale
Citation: Xia S, Luo L, Wu W, Lu K, Jiang T and Li Y (2023) The role of pudendal nerve block in hemorrhoid surgery: a systematic review and meta-analysis of double-blind randomized controlled trials. Front. Med. 10:1283512. doi: 10.3389/fmed.2023.1283512
Received: 26 August 2023; Accepted: 27 November 2023;
Published: 13 December 2023.
Edited by:
Arnaud Alves, Université de Caen Normandie, FranceReviewed by:
Vincent de Parades, Hôpital Saint-Joseph, FranceChiara Eberspacher, Sapienza University of Rome, Italy
Copyright © 2023 Xia, Luo, Wu, Lu, Jiang and Li. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Wenjiang Wu, MTA1MzY2MDY0NUBxcS5jb20=