 Ana Lucia Domingues Neves1†Luiz Eduardo Galvão Martins2†
Ana Lucia Domingues Neves1†Luiz Eduardo Galvão Martins2† Mônica Andrade Lima Gabbay3,4Paula Pascali4
Mônica Andrade Lima Gabbay3,4Paula Pascali4 Tiago de Oliveira2Aldo Martinazzo1
Tiago de Oliveira2Aldo Martinazzo1 Sérgio Atala Dib3,4
Sérgio Atala Dib3,4 Dulce Elena Casarini1Sebastião Vagner Aredes5Fernanda Silva Tenorio1†
Dulce Elena Casarini1Sebastião Vagner Aredes5Fernanda Silva Tenorio1† Tatiana Sousa Cunha2*†
Tatiana Sousa Cunha2*†- 1Postgraduate Program in Translational Medicine, Department of Medicine, Paulista School of Medicine, Federal University of São Paulo, São Paulo, Brazil
- 2Department of Science and Technology, Institute of Science and Technology, Federal University of São Paulo, São Paulo, Brazil
- 3Department of Medicine, Paulista School of Medicine, Federal University of São Paulo, São Paulo, Brazil
- 4Diabetes Center Insulin Pump Ambulatory, Federal University of São Paulo, São Paulo, Brazil
- 5DeltaLife, São José dos Campos, Brazil
Introduction: Insulin Infusion Sets (IIS) play a crucial role in ensuring the safe delivery of insulin through a Continuous Subcutaneous Insulin Infusion (CSII) for individuals with Type 1 Diabetes (T1D). Recent advancements in therapy have highlighted the need to address issues such as unexplained hyperglycemia and IIS occlusion.
Objective: To investigate the adverse events (AEs) associated with IIS that impact the treatment of T1D, with a specific focus on promoting effective educational practices.
Methods: One hundred and eighteen patients under treatment at the Diabetes Center Insulin Pump Ambulatory, Federal University of São Paulo responded to a semi-structured questionnaire. Over 6 months, a nurse researcher interviewed them via video calls.
Results: Catheter-related adverse events (AEs) included catheter knots, folding, and accidental traction. AEs associated with cannula use were mainly related to cannula fixation adhesive, insulin leakage, bleeding episodes, and skin problems. The cannula patch tends to detach easily in hot conditions or when used for more than 3 days, leading to local itching. Adhesive glue can cause redness and pain. Insulin leakage typically occurs after the catheter disconnects from the cannula, accidental cannula traction, or beneath the cannula patch. Bleeding has been reported inside the cannula or at the insertion site, resulting in local pain and, in some cases, obstruction of insulin flow. When accidental cannula traction occurs, it is recommended to replace the entire IIS system. In situations involving bleeding, leakage, insulin odor, or unsuccessful attempts to correct hyperglycemic episodes with a “bolus” of insulin, it is advisable to change the IIS system and evaluate appropriate techniques for handling and infusing the device. Moreover, regular inspections of the device and reservoir/cartridge are essential.
Conclusion: Serious AEs can occur even in cases where the occlusion alarm is not activated, leading to interruptions in insulin flow. Conversely, in less severe situations, alarm activation can occur even in the absence of insulin flow interruption. Accidental catheter traction and catheter bending are commonly encountered in everyday situations, while issues related to the cannula directly affect blood glucose levels. AEs related to the IIS cannula often involve insulin leakage into the skin, bleeding, and skin events attributed to adhesive issues with the cannula.
1 Introduction
The treatment of Type 1 Diabetes Mellitus (T1D) can be performed through continuous subcutaneous insulin infusion (CSII) or multiple daily injections (MDI) (1). These methods are effective and safe for implementing intensive management of Diabetes Mellitus (DM) (2, 3).
We describe CSII as an evolutionary form of insulin administration that effectively maintains glycemic levels, offers flexibility to patients, and induces fewer instances of hypoglycemia. The Diabetes Control Complications Trial (DCCT) study (1) demonstrated that intensive treatment with CSII reduces the incidence and progression of microvascular complications when compared to conventional treatment with MDI (3–6).
There is evidence from reviews and meta-analyses showing that the use of CSII reduces the frequency and duration of hypoglycemic events, decreases episodes of recurrent diabetic ketoacidosis, and improves glycemic control and quality of life compared to conventional treatment with MDI (7–13). Moreover, for young children, CSII may be the only option, as their daily insulin needs are very low, requiring doses lower than 0.5 U, which is impractical with MDI therapy (14).
It is well-established that CSII is a critical medical device that introduces new challenges and vulnerabilities due to the inherent risk of technological failures (15). The safety and efficacy of CSII use are highly dependent on appropriate selection of the patient, their level of diabetes education, adherence to therapeutic recommendations, and the technical proficiency and competence of the multidisciplinary team responsible for their care (16). Thus, the use of CSII should be based on strict criteria and the indication should be exclusively for eligible patients. It is known that approximately 15% of patients with T1D have an absolute indication for its use (17).
Conceptually, adverse events (AEs) can be categorized into “nonmetabolic AEs” related to events in the catheter infusion set, issues with the device itself (such as software or screen problems, keyboard issues, battery or component failures, insulin leakage, or water damage), or skin complications. “Metabolic AEs” result from diabetic ketoacidosis and severe hypoglycemia, among other reasons, often tied to failures in the infusion set or errors in the calculation of the “bolus” (18).
According to the Food and Drug Administration (FDA) Code of Federal Regulations (CFR) 21, part 803 (19), the primary language for defining an AE is as follows:
Caused or contributed means that death or serious injury was or may have been attributed to a medical device, or that a medical device was or may have been a factor in death or serious injury, including events occurring as a result of (1) Failure, (2) Malfunction, (3) Improper or inadequate design, (4) Manufacture, (5) Labeling, or (6) User error.
Reliable insulin delivery depends directly on the proper functioning of the IIS, which includes the cannula and catheter associated with fluid transfer (20, 21). Recent advances in IIS technology emphasize the importance of discussing aspects related to these components of CSII therapy, as all users of the device rely on the IIS for the predictable delivery of insulin to the subcutaneous tissue (22).
Issues related to IIS accounted for the majority of CSII recalls by the US FDA (2). Various studies (4, 15, 23) have examined the frequency and types of adverse events (AEs) associated with CSII, including blockages, bent catheters, and insertion site reactions such as irritation and areas of infection, all of which can compromise metabolic control. To minimize these AEs, manufacturers have historically recommended changing the catheter every 2–3 days (15, 18, 23–25).
Recent studies have examined potential causes of AEs associated with CSII models, including the MiniMed™ 670G, MiniMed™ 630G, Omnipod®, Omnipod DASH®, and t:slim X2™. These investigations utilized data from the FDA Manufacturer and User Facility Device Experience (MAUDE) database. Out of the 2,429 AEs reported, approximately 8% were linked to issues with the infusion set or site (26).
Problems related to the IIS, such as displacement, cannula blockage, skin reactions, the cannula being placed in unhealthy tissue (e.g., areas of Lipohypertrophy), and unpredictable variations in insulin absorption, significantly impact therapy. Additionally, uninterrupted insulin delivery can be affected by factors such as the choice of cannula insertion site, interstitial pressure, and occlusion by cell debris or insulin. The precise causes of insulin delivery inaccuracies related to IISs are multifactorial and not yet well understood (20, 21). Early detection of these factors is crucial to minimize the risk of prolonged hyperglycemia, especially in automatic insulin administration methods such as CSII therapy (27).
Given the limited information available regarding AEs linked to CSII and the substantial incidence of these events affecting the treatment of T1D, this study aims to describe the factors associated with IIS that significantly influence disease management. The primary objective is to facilitate the development of clinical practice protocols and patient guidance by presenting these factors, with a particular emphasis on promoting effective educational practices.
2 Materials and methods
2.1 Study stages
In this section, we present an overview of the proposed methodology, which is divided into four main steps, highlighting their sequence and iteration.
The study was conducted in four phases. In Phase I, a literature review was performed using databases such as Medline via PubMed, Lilacs, Science Direct, and Scielo to identify evidence related to prevalent AEs associated with the use of CSII systems. English descriptors and their Portuguese equivalents, such as “Diabetes Mellitus, Type 1,” “Health,” “Insulin,” “Insulin Infusion Systems,” and “Adverse Event,” were employed. These descriptors were combined using appropriate Boolean operators. No restrictions were placed on the year or language of publication. Additionally, manual searches were conducted by exploring the reference lists in the identified documents. During this stage, the entire process of searching, selecting, and extracting data from the articles was carried out in pairs. Data were organized into extraction tables containing basic information, including the title, authors, affiliation, country, journal title, and publication date. Studies involving pregnant women with T2D or the use of devices in a hospital environment, as well as studies with methodological inconsistencies, were excluded.
Subsequently, full-text articles were obtained, and in cases of uncertainty, consensus meetings were held with mentors to determine whether to include or exclude an article. Finally, AEs associated with the device, IIS, and device battery described in the literature were categorized.
Phase II marked the beginning of data collection, aiming to explore reports from patients followed at the Diabetes Center. This phase provided a general overview of prevalent AEs associated with the device and gathered essential data for the future description of safety requirements for the research group’s low-cost CSII prototype.
Before beginning this stage, the researcher established telephone contact with each research participant and their family members to explain the study, apply the Informed Consent Form, and clarify any potential doubts. Subsequently, the Data Collection Instrument was administered through semi-structured interviews conducted via video calls.
The data collection instrument was adapted from the “Survey on Complications of Insulin Pump Therapy,” mentioned in the publication “Nonmetabolic Complications of Continuous Subcutaneous Insulin Infusion: A Patient Survey” (28), and the copyright was kindly provided by the author John C. Pickup via email. This instrument was validated by the project’s interdisciplinary team and consisted of three sections: S1: Sociodemographic aspects; S2: General information about the disease and the device used for treatment; and S3: Data related to the insulin infusion set.
At the conclusion of Phase II, the data were organized into three main categories: “General data on the disease and CSII,” “Insulin Infusion Set Data,” and finally, “CSII Usability Data: User Interface.”
Phase III of the study involved the preparation of a document entitled “Description of Adverse Events associated with the use of CSII: contributions to the Safety Requirements of a low-cost medical device.” In this document, the AEs were organized into three main categories: “General Data on the disease and CSII,” “Insulin Infusion Set Data,” and finally, “CSII Usability Data: User Interface.”
In Phase IV of the study, the prevalence of identified AEs was calculated using simple arithmetic means.
2.2 Data collection
The present study was conducted at the Diabetes Center Insulin Pump Ambulatory, Federal University of São Paulo, following the guidelines of the Institutional Research Ethics Committee (REC) (reference no. REC/UNIFESP 1242/2019) and the principles of the Helsinki Declaration. A total of 189 patients who were undergoing treatment for T1D at the study site were invited to participate.
After excluding those who declined and those who did not respond, a total of 118 patients (with a participation rate of 63%), including children, adolescents, and adults, who had been using any brand and model of CSII for at least 6 months, participated in the study. Each participant provided electronic informed consent, and data collection was conducted remotely over 6 months due to the COVID-19 pandemic.
The data collection instrument consisted of a semi-structured interview conducted by a researcher nurse through video calls (29). We developed a questionnaire comprising three sections, which underwent content validation by the projects’ interdisciplinary team. The first section included sociodemographic aspects such as age, sex, city of origin, education, and ethnicity. The second section focused on general information about T1D, and the device being used, including the date of diabetes diagnosis, initiation of CSII treatment, number and reasons for device change, and device manufacturer/model, among other details. The last section included general data related to the IIS, as described below.
1. What are the dimensions of the cannula and catheter used?
2. How frequently do you replace the IIS cannula and catheter?
3. What factors contribute to the recommended change of the cannula after approximately 3 days, as advised by the healthcare facility responsible for the treatment of T1D?
4. How often and under what conditions are adverse events associated with accidental catheter traction, catheter knotting, and catheter bending observed?
5. Were there any disruptions to basal/bolus programming and alarm systems during the occurrence of the aforementioned adverse events?
6. Have there been any reported complications at the site of cannula insertion, such as local bleeding or wounds, poor adhesive adhesion, signs of skin infection or allergies, or insulin leakage, among others?
7. How often and under what circumstances has insulin leakage occurred at the site where the catheter is connected to the insulin reservoir?
2.3 Context of the use of CSIIs at the time of data collection
The CSII system manufactured by Medtronic allows for connectivity with continuous glucose monitoring (CGM) sensors through radio frequency, except for the 715 model.
The CGM system comprises the Enlite® glucose sensor and the Guardian® Link transmitter, which capture real-time data from the sensor and transmit them to the CSII device. For optimal performance of the Medtronic device, it is recommended to use Energizer® batteries, specifically the AAA alkaline model (24).
The Roche system, notably the Accu-Chek Spirit Combo, is a medical device designed to simulate the functionality of a healthy pancreas. It consists of two primary components: the CSII and a glucometer referred to as the control unit. The CSII is responsible for delivering insulin according to the specific requirements of the patient, while the control unit is equipped with Bluetooth technology for wireless connectivity with the CSII. Additionally, the glucometer measures the patient’s blood glucose levels and calculates suggested insulin dosages for precise administration at each relevant moment.
The Secretary of Health in São Paulo adheres to rigorous criteria when approving local recommendations and authorizing the use of CSII therapy for patients. Generally, this therapy is indicated for patients who experience severe hypoglycemia (provided they are sufficiently insulinized through MDI), as well as those who suffer from nocturnal or asymptomatic hypoglycemia, particularly among children under 6 years of age. These very young children not only face a heightened risk of hypoglycemia but also exhibit substantial glycemic variability and require low-dose insulin treatment. In cases of severe hypoglycemia among very young children, the use of a sensor manufactured by Medtronic is recommended.
In this study, all participants using the Roche system were equipped with the Accu-Chek Spirit Combo, which includes the device and the glucometer, along with all necessary supplies such as cannulas and catheters. The integration of the glucometer into the Roche system enables patients to access real-time glucose readings, simplifying the process of precise insulin dosing. This functionality significantly enhances the management of T1D and leads to greater overall clinical stability.
3 Results
3.1 Characterization of the socio-demographic, disease profile, and device
Out of the total number of participants in the study (118), 71 were women and 47 were men. Among the participants, 51 belonged to the pediatric age group while 67 were adults, with mean ages x̄ = 10 years and 29 years, respectively. The majority of the participants, specifically 88 individuals, identified themselves as belonging to a white racial background. Additionally, 70 participants resided in the city of São Paulo. Lastly, it is worth noting that 39 participants had either completed their postgraduate studies or were currently pursuing higher education.
Regarding the moment of T1D diagnosis, we observed the following trends. In the pediatric population and adolescents aged 2–18 years, of the 51 patients, 8 were diagnosed during the 1990s and 43 were diagnosed during the 2000s. Among adults, who included 67 patients aged 19–55 years, 3 were diagnosed in 1984 and 1989, 19 were diagnosed between 1990 and 1999, and 45 were diagnosed between 2000 and 2016.
The time interval between the T1D diagnosis and the commencement of CSII therapy varied depending on the age group. For pediatric patients, the interval ranged from 1 to 15 years, while for adults, it spanned from 7 to 37 years. In terms of the average duration of device usage, the study found that pediatric patients utilized the device for an average of 5 years, whereas adult patients used it for an average of 9 years. According to Table 1, the most commonly used device was the CSII Roche - Accu-Chek Spirit Combo. Several Medtronic models were also used, and one patient in the study was using a Tandem® Diabetes Care device. It is noteworthy that out of the four interviewees using Medtronic devices who were unable to specify the model being used, three were mothers of children between 3 and 5 years old, and the fourth patient was 29 years old and had been using the device for 9 years.
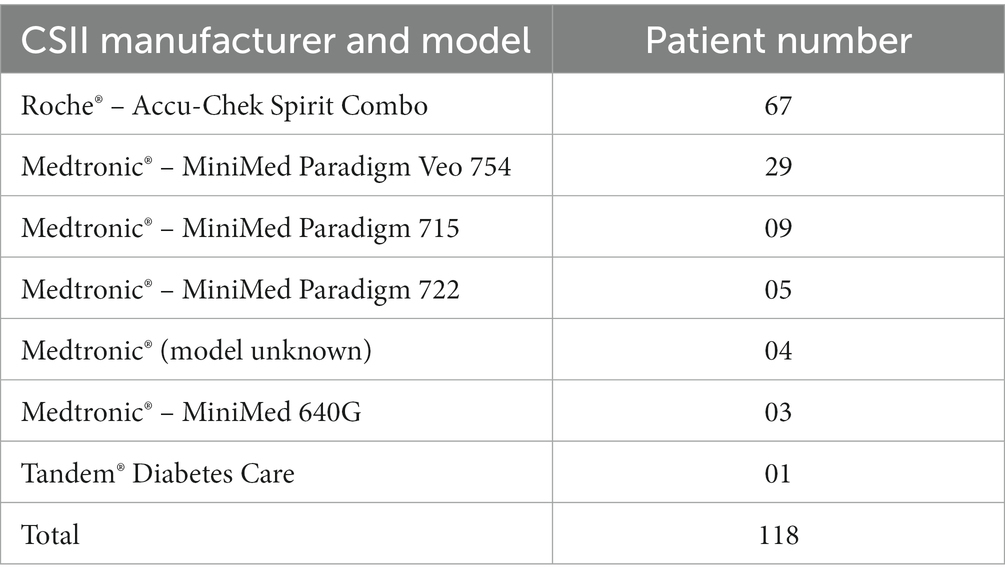
Table 1. Distribution of patients using different models and brands of CSII at the Diabetes Center Insulin Pump Ambulatory, Federal University of São Paulo (São Paulo, Brazil, 2021).
3.2 Characterization of the sizes and change frequencies of IIS, and proposals for educational actions
The frequency of replacing the IIS cannula and catheter varied among the patients in the study. Out of the 118 participants, 89 individuals reported replacing both the cannula and catheter at the same frequency of use. Within this group, 60 participants reported changing them up to every 3 days, while 29 participants reported changing them every 3–7 days (Table 2). In contrast, the remaining 29 individuals reported replacing the cannula and catheter at different frequencies (as shown in Table 3).
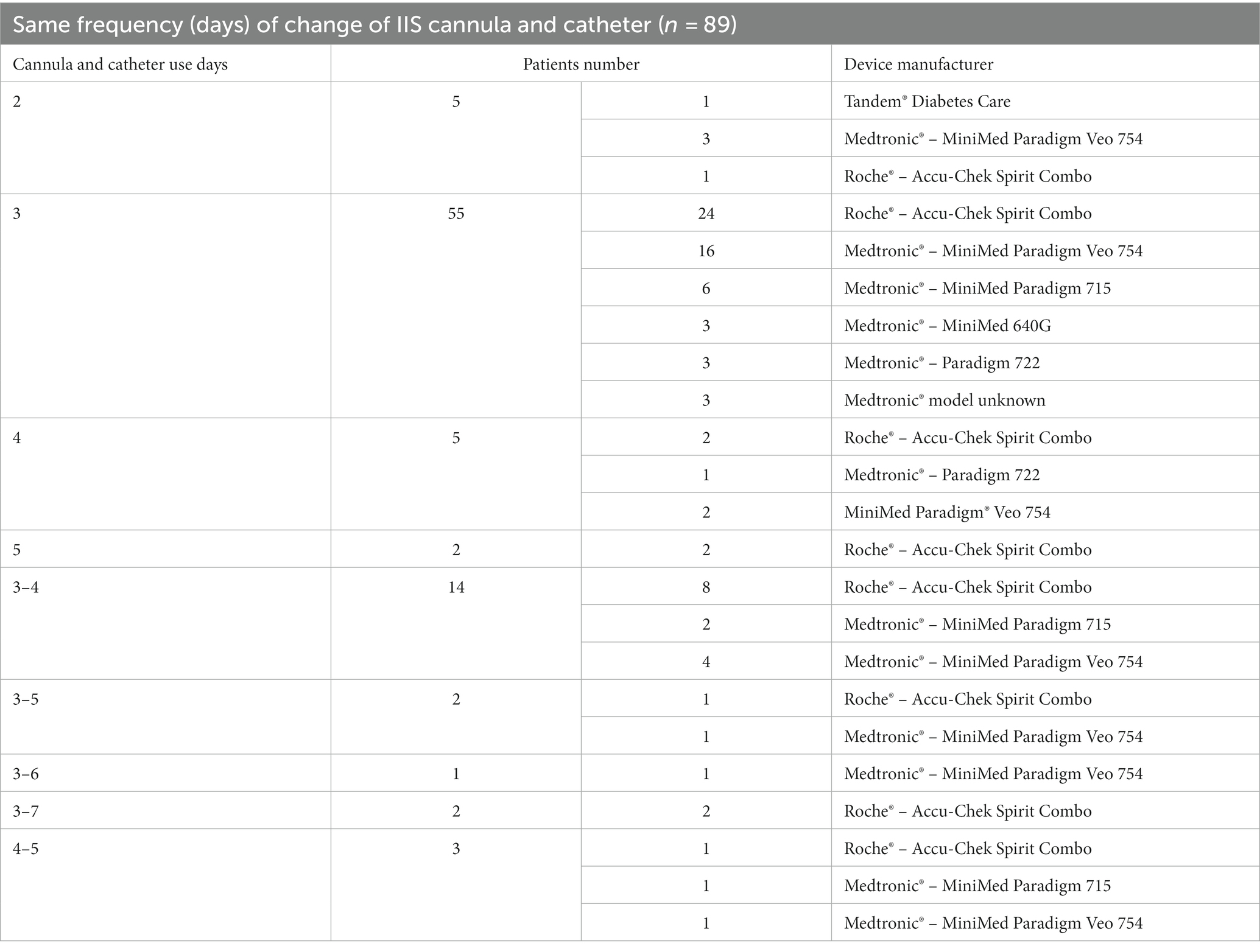
Table 2. Frequency of IIS cannula and catheter change in patients monitored at the Diabetes Center Insulin Pump Ambulatory, Federal University of São Paulo–change of both the cannula and catheter at the same frequency of use (São Paulo, Brazil, 2021).
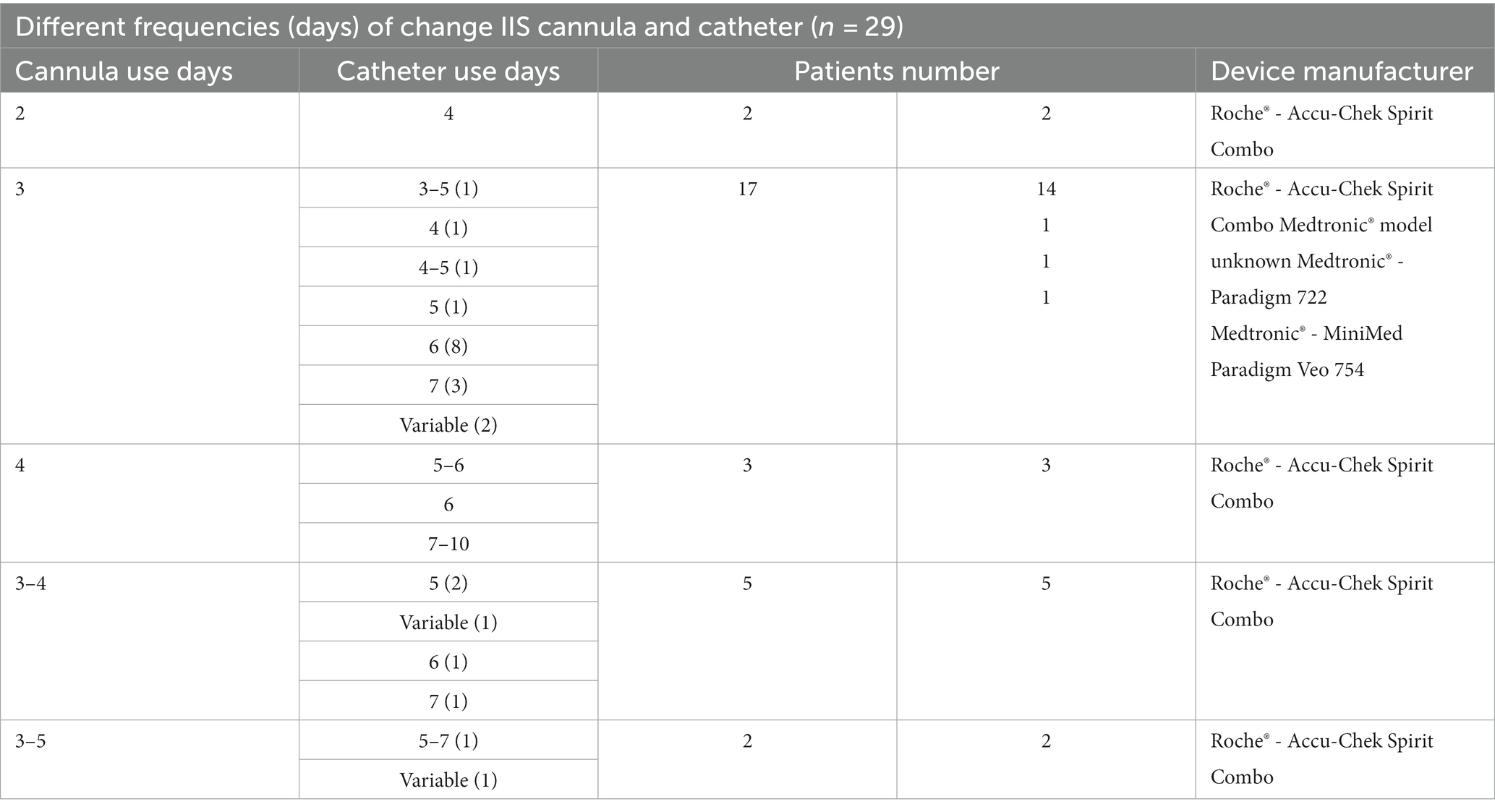
Table 3. Frequency of IIS cannula and catheter change in patients monitored at the Diabetes Center Insulin Pump Ambulatory, Federal University of São Paulo –change of cannula and catheter at different frequencies (São Paulo, Brazil, 2021).
The cannula size and catheter length reported by the patients at the time of the study are shown in Table 4.
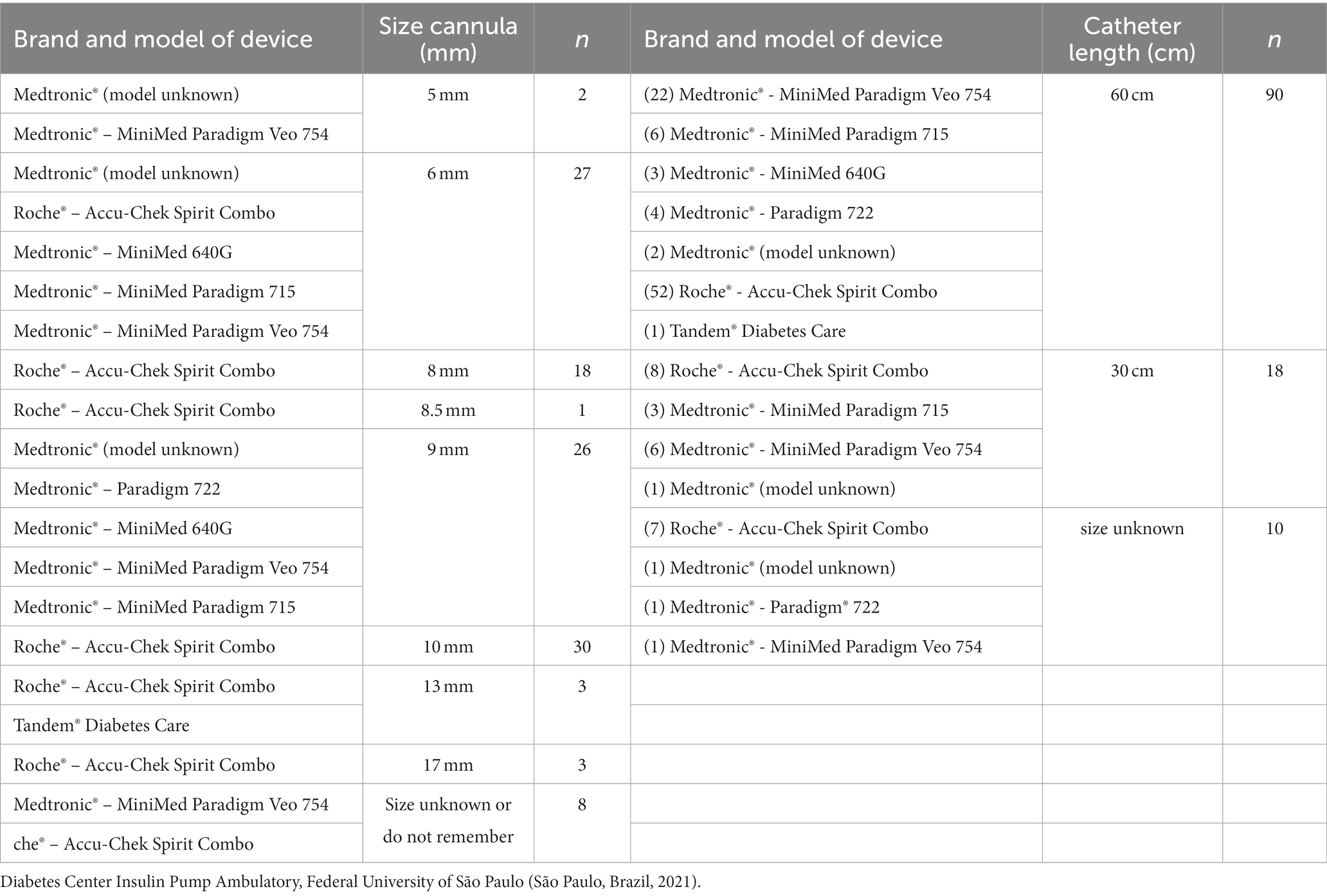
Table 4. Characterization of the cannula size and catheter length.
The recommendations below aim to ensure close monitoring of glycemic control, effectively address hyperglycemic episodes, and take appropriate actions if blood glucose levels remain high. Additionally, monitoring device disconnects and suspensions can help identify any issues related to the pump’s functionality. It is important to address any factors that may delay the IIS change and provide educational support to help patients overcome these challenges. Finally, engaging in open discussions with patients about their concerns allows for personalized treatment planning and helps establish realistic goals.
The recommendations regarding changing the IIS for the patients are as follows:
1. When uncertain about the date of the last cannula and catheter change, it is advised to change the entire IIS.
2. Consider changing the catheter if you notice changes in your glycemic profile, such as inadequate correction or ineffective “meal bolus,” as well as correcting pre-meal hyperglycemia.
3. It is recommended to increase your glycemic monitoring if the duration between IIS changes exceeds the recommended 3 days set by the study site team.
The Healthcare Team/Educators in diabetes follow these recommendations:
1. Monitor the glycemic profile while using the current device settings. In the case of hyperglycemic episodes, after administering two corrections, if blood glucose levels remain high, administer insulin with a pen and change the entire IIS.
2. Observe device disconnects/suspend patterns, and whenever there are changes in settings, administer insulin with a pen and change the entire IIS.
3. Pay attention to factors that may delay the IIS change, such as financial or motivational issues, and take educational actions to address these concerns.
4. Initiate a dialogue with the patient regarding their concerns about the IIS change technique to develop an individualized and realistic treatment plan.
The following tables (Tables 5, 6) provide a comprehensive overview of the reasons given for various scenarios regarding cannula and IIS catheter change.
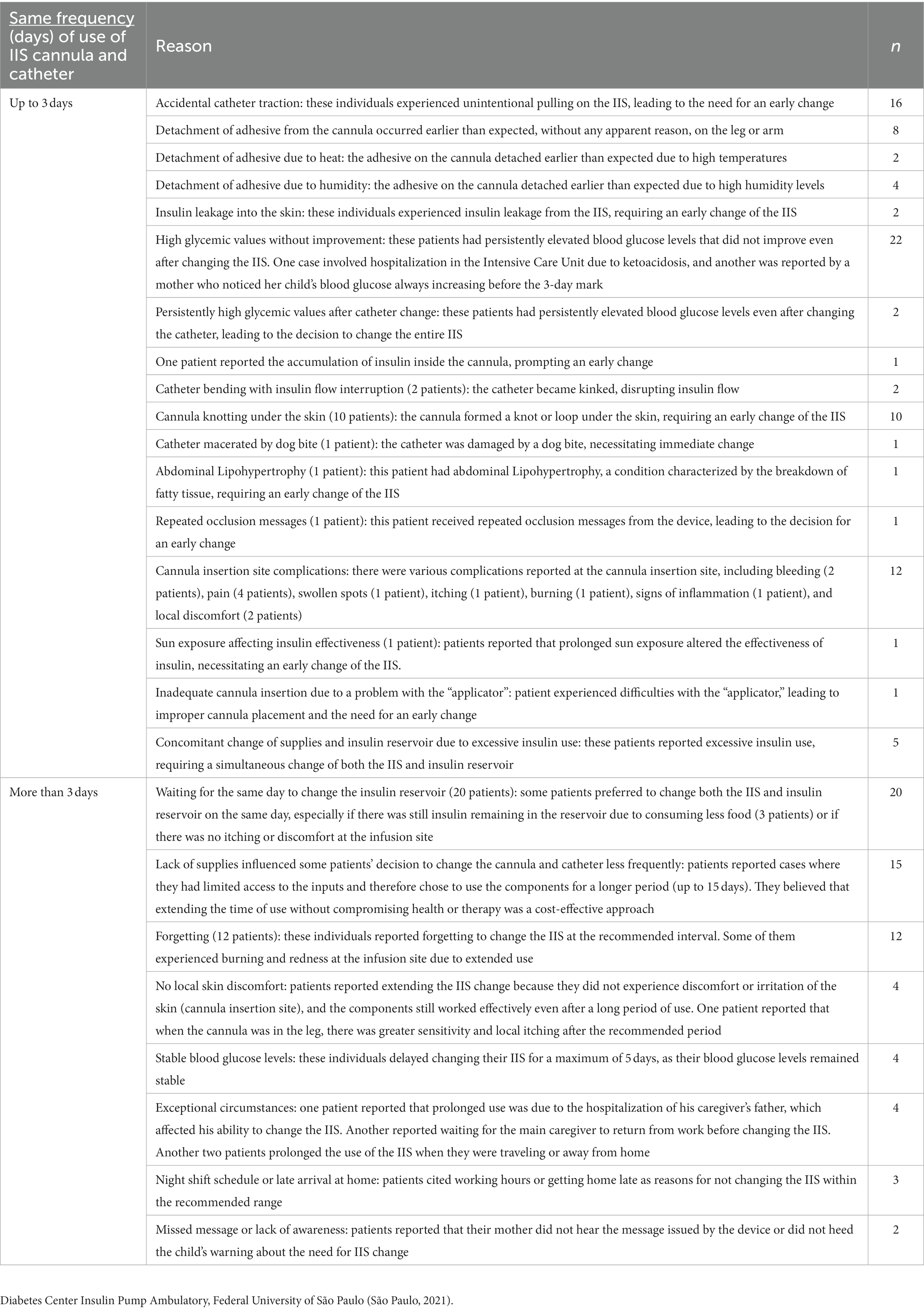
Table 5. Characterization of reasons reported for cannula and catheter change within 3 days or more–change at the same frequency.
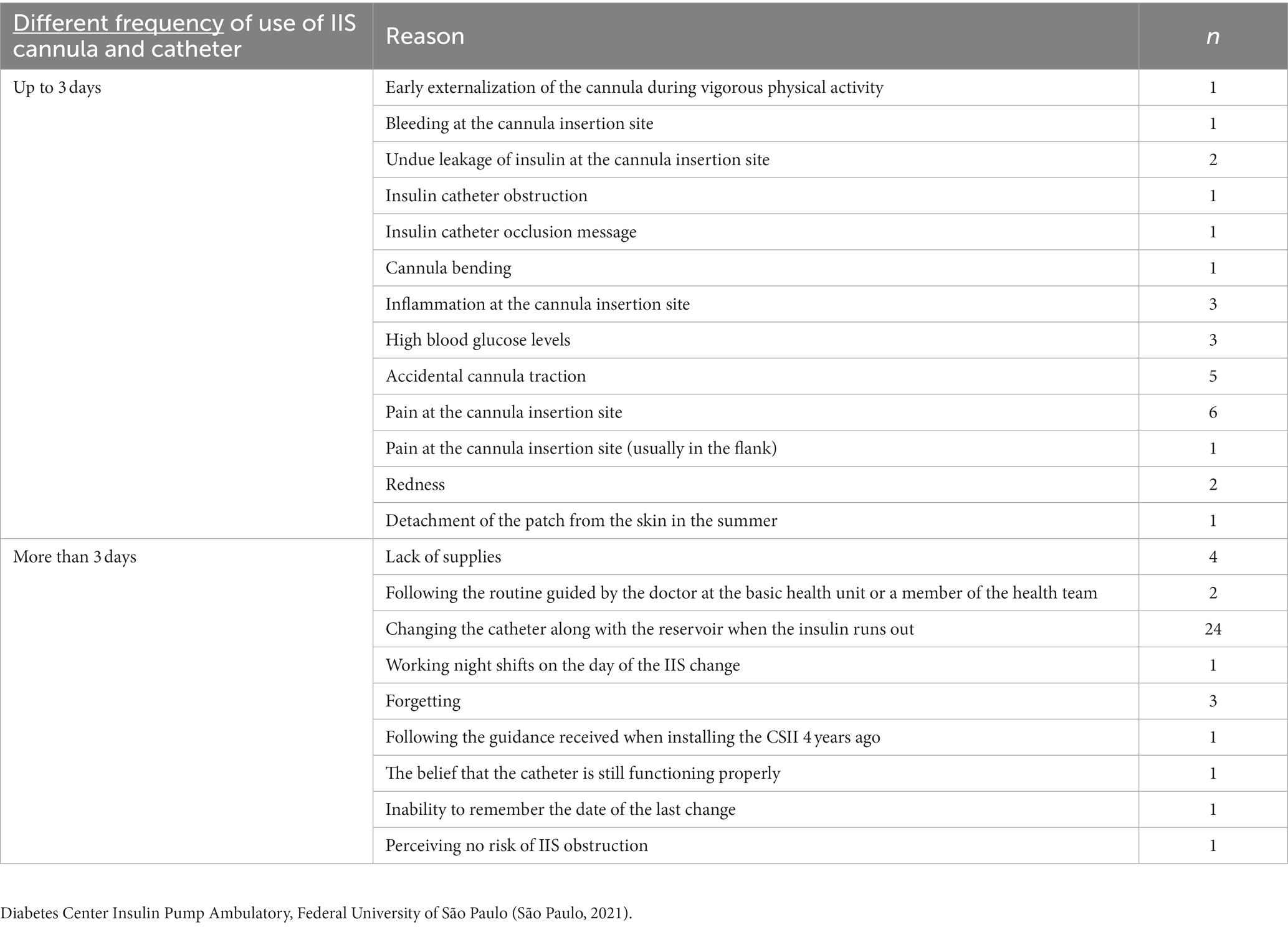
Table 6. Characterization of reasons reported for cannula and catheter change within 3 days or more–change at different frequencies.
3.3 AEs associated with IIS cannula and catheter
Catheter- and cannula-related AEs can be classified as cutaneous and subcutaneous complications and technical issues.
3.3.1 Catheter
Among the patients included in the study, three relevant AEs directly involving the IIS catheter were identified (Tables 7–9). These AEs are described below, along with their respective characteristics and frequencies of occurrence.
• Occurrence of accidental catheter traction: this AE rarely occurred among 62 patients and involved the unintended removal or dislodgement of the IIS catheter. The occurrences of this AE were distributed as follows:
− N = 11 patients experienced the event, but no explanation was provided for its occurrence.
− N = 30 patients attributed the AE to physical contact with another person, such as during play, in a water park, while getting dressed, falling, sleeping, or accidental contact with objects like doors, tables, chairs, or zippers. These incidents resulted in either partial or total traction of the catheter.
− N = 18 patients reported that the occurrence of accidental catheter traction was more frequent depending on the positioning site of the cannula. It was more commonly reported in the leg (10 cases), arm (5 cases), buttocks (2 cases), or belly (1 case).
− N = 1 patient reported an accidental catheter traction that resulted.
in the rupture of the catheter at the cannula-catheter intersection.
− N = 1 patient attributed the occurrence of the AE to the absence of a clip to secure the device on clothing, especially when fixed on the belly or leg.
− N = 1 patient experienced accidental catheter traction due to inadvertently pressing the cannula “button.”
− In three exceptional cases (N = 3), accidental traction involved both the cannula and catheter, such as when the catheter was caught in a car door or during use on the leg.
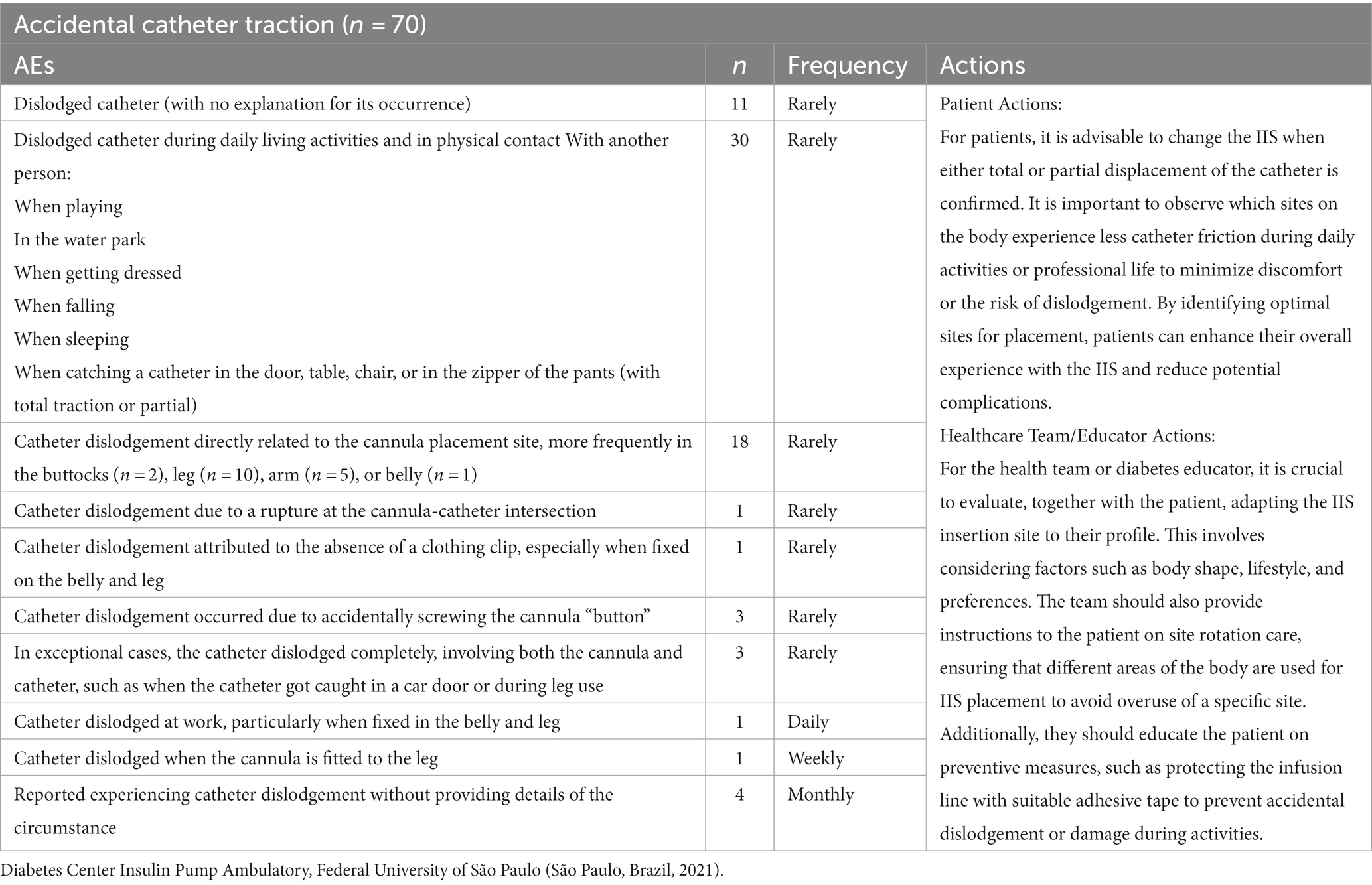
Table 7. Characterization of the type and frequency of “accidental catheter traction” and proposals for educational actions.
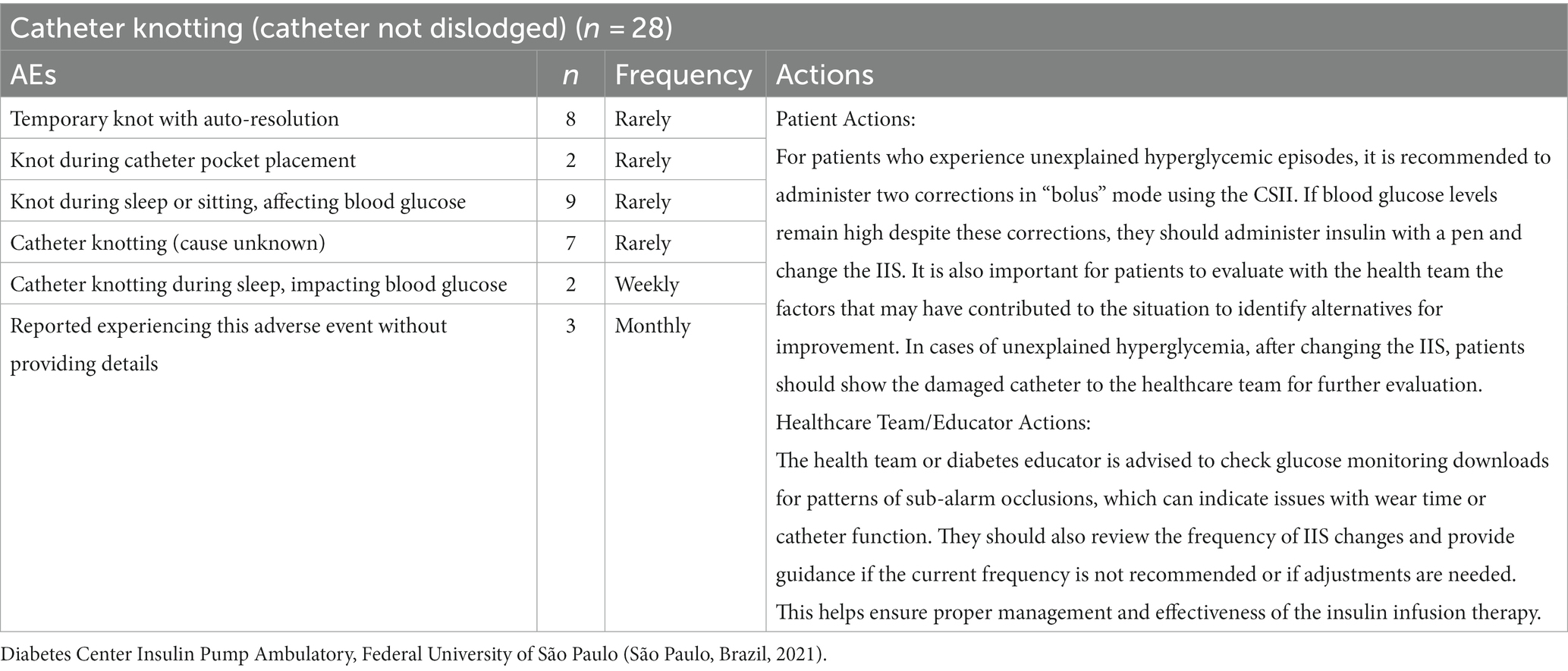
Table 8. Characterization of the type and frequency of “Catheter knotting” and proposals for educational actions.
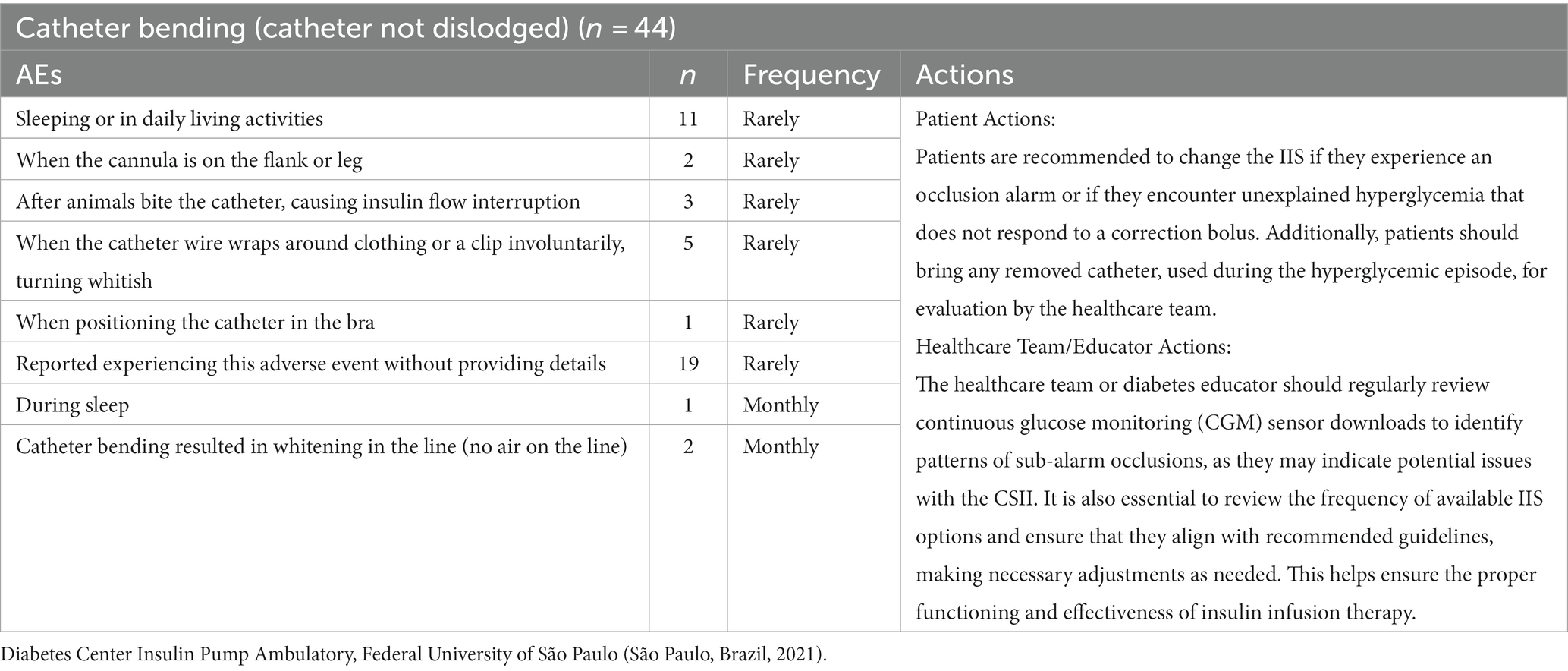
Table 9. Characterization of the type and frequency of “Catheter bending” and proposals for educational actions.
These findings highlight the potential risk of accidental catheter traction and the various circumstances in which it may occur. It is important to address this AE to minimize its occurrence and ensure the stability and effectiveness of the IIS.
• Occurrence of catheter knotting: this AE refers to the rare occurrence of a knot in the catheter of the IIS, with the following characteristics:
− N = 8 patients experienced the AE, and in these instances, the catheter knotting dissolved spontaneously without any occlusion message or interruption in the insulin flow.
− N = 2 reported experiencing this AE when the catheter was positioned in a pocket.
− N = 9 patients experienced the AE while sleeping or sitting, which had negative repercussions on their blood glucose levels.
− Additionally, n = 7 patients experienced this AE without providing any specific reason for the occurrence.
− N = 2 patients reported experiencing this AE weekly while sleeping, and it had negative effects on their glycemic control.
− N = 3 patients reported experiencing this AE monthly, but no further details about the circumstances were provided.
It is important to note that the occurrence of an IIS catheter knot, although rare, can have implications for the functionality and effectiveness of the insulin infusion system. The negative impact on blood glucose control in certain situations emphasizes the importance of addressing and mitigating this AE to ensure optimal treatment outcomes.
• Occurrence of catheter bending: this AE has been reported by 36 patients and involves catheter bending, highlighting potential challenges and complications associated with its use. This AE manifests itself in a variety of circumstances as described below.
− N = 11 patients experienced the AE while sleeping or during their daily activities.
− N = 2 patients reported a bent catheter when it was positioned on the flank or leg.
− N = 3 patients encountered the AE after animals bit the catheter, leading to interruption of insulin flow.
− N = 5 patients described the catheter wire involuntarily getting wrapped around clothing or a clip, resulting in the catheter becoming whitish.
− N = 1 patient experienced the AE when positioning the catheter in the bra.
− Additionally, n = 14 patients reported experiencing this AE without providing further details about the circumstances.
− N = 1 patient reported this AE occurring monthly during sleep.
− N = 2 patients reported that catheter bending led to its whitening, but the circumstances were not specified.
The various situations mentioned highlight the need for careful handling and positioning of the catheter to minimize the occurrence of these AEs.
Insulin leakage at the catheter-reservoir intersection is another occurrence related to catheters. This event was not experienced by 103 out of the total number of patients and was rarely reported by 15 patients. The circumstances contributing to this issue included accidental traction at the connection point (reported by 1 patient), incorrect positioning of the catheter in the device (reported by 2 patients), improper passage of the catheter (reported by 2 patients), and incorrect threading of the reservoir cap (reported by 4 patients). These factors can lead to insulin leakage at the junction between the catheter and the reservoir, which must be addressed to ensure proper functioning of the IIS.
These incidents underscore the importance of proper handling and installation of the catheter and reservoir to prevent insulin leakage and ensure effective insulin infusion therapy. To address this issue, it is recommended that patients inspect the device, reservoir/cartridge, tubing, and IIS if they experience unexplained hyperglycemia symptoms. If any leakage is detected, the odor of insulin is present, or if a bolus correction is ineffective, the IIS should be changed.
During the initial training, healthcare teams or diabetes educators should familiarize the patient with the scent of insulin, enabling them to detect any potential leakage. They should also verify the patient’s technique when installing the IIS and closing the cartridge/reservoir to ensure proper installation and minimize the risk of insulin leakage. Proper education and training on IIS handling and installation, along with regular monitoring and immediate corrective actions, can help prevent and address insulin leakage at the catheter-reservoir intersection, ensuring the safety and efficacy of insulin infusion therapy.
3.3.2 Cannula
Table 10 describes AEs related to the IIS cannula, along with proposed solutions to ensure patient clinical stability in response to these occurrences. In the study, 114 patients (96.7%) adhered to the recommended rotation of the cannula application site across five designated areas: 69% on the abdomen, 65% on the flank, 54% on the gluteus, 40% on the leg, and 37% on the arm. However, despite adherence to these guidelines, the incidence of Lipohypertrophy remained persistently high, reaching 64.4%.
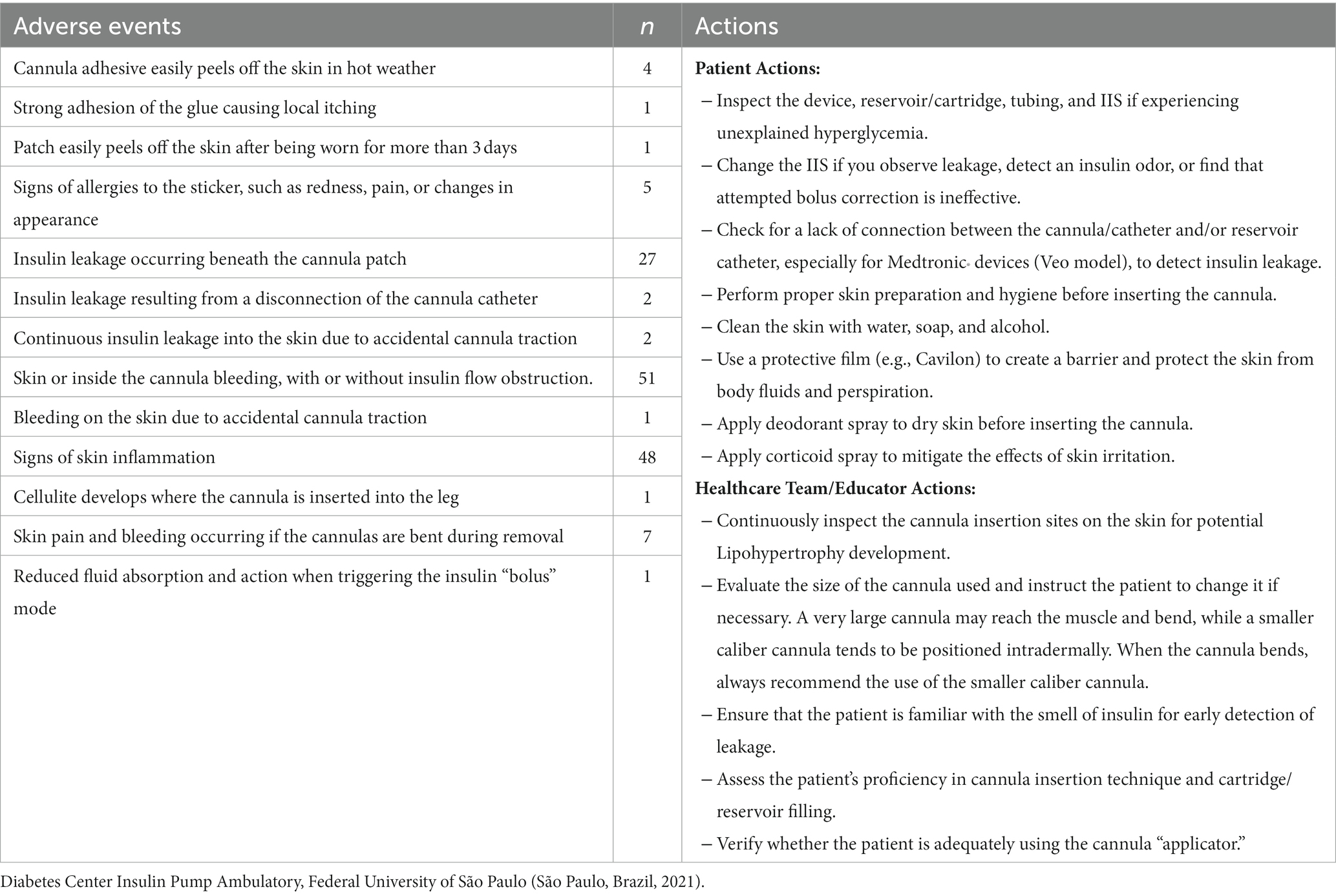
Table 10. Characterization of the type and frequency of AEs related to IIS cannula and proposals for educational actions.
While the present study did not specifically analyze the outcomes of AEs alone, we conducted a recent study on AEs associated with the use of CSIIs. This study aimed to propose a taxonomy based on prevalent occurrences experienced by patients with T1D (29). In total, 159 AEs were identified, which resulted in 60 device changes for various reasons, including issues with cannulas and catheters.
3.4 Detection of alarm emission and interruption of insulin flow in response to AE related to the IIS catheter
3.4.1 Detection of interruptions in basal/bolus programming
Thirty-nine patients reported experiencing interruptions in basal/ bolus programming.
Sixty-five patients did not experience interruptions in basal/ bolus programming.
Six patients reported experiencing interruptions sometimes.
Two patients reported experiencing interruptions rarely. Six patients could not provide an answer.
3.4.2 Emission of insulin flow occlusion alarm
Thirty-five patients reported receiving an insulin flow occlusion alarm. Fifty-nine patients did not receive this type of communication.
Eighteen patients reported receiving the alarm sometimes. Six patients reported receiving the alarm rarely.
Devices manufactured by Medtronic trigger the alarm only when the insulin flow is completely occluded. Roche devices are capable of generating alarms only for partial occlusion.
When the “no adm” alarm occurs in the “basal” programming mode, it signifies a more serious issue (e.g., a motor problem with a potential risk of interrupting the insulin flow). However, when this alarm appears in “bolus” mode, it may indicate a fold or displacement of the IIS (Table 11).

Table 11. Characterization of interruption of basal/bolus programming in response to AEs.
4 Discussion
Recent innovations in CSII therapy demonstrate a heightened awareness of issues such as unexplained hyperglycemia and occlusion in IIS, regardless of the presence of an alarm. Early detection and prompt correction of these problems are critical for minimizing risks in automated insulin administration. The most common AEs include:
• Accidental catheter traction
• Catheter knotting
• Catheter bending
• Issues related to cannula fixation
• Insulin leakage
• Bleeding episodes
• Skin problems
The occurrence of alarms and occlusions highlights the need for further investigation and improvements in detection and response mechanisms to enhance patient safety.
4.1 Characteristics of IIS cannulas and catheters, and IIS change frequency recommendations
The sizes of IIS cannulas and catheters available in the market vary among manufacturers, as detailed below.
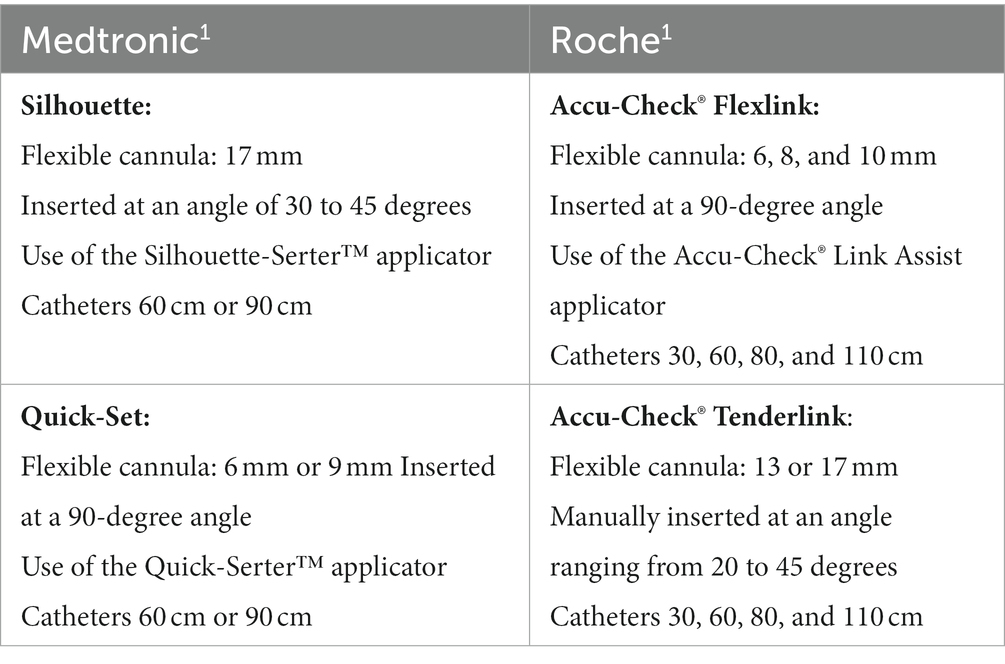
1Source: Oliveira and Galves (30).
The Diabetes Center Insulin Pump Ambulatory, Federal University of São Paulo recommends changing the IIS cannula and catheter every 3 days, regardless of the brand of the device. This schedule is based on their experience and research, ensuring the safety and effectiveness of the CSII. The rationale behind this recommendation is that after 3 days, the cannula could be perceived as a foreign object by the body, which may lead to potential inflammatory processes in the skin. Additionally, there is a possibility of fluids adhering to the pores of the catheter material, potentially impacting its performance. The center ensures that an adequate supply of materials is provided for this specific periodicity.
Similarly, the Medtronic company shares the same recommendation and justification for changing the cannula and catheter every 3 days. On the other hand, Roche suggests a different approach. They recommend replacing the cannula every 3 days and the catheter every 6 days. This means that a single catheter can be used for two cannula changes. Manufacturers often provide guidelines to ensure the proper functioning of their products. It is worth noting that, irrespective of these recommendations, all patients receive the necessary supplies free of charge from the Brazilian government.
The government’s costs in managing DM, in comparison to the benefits, can be partially mitigated by reducing expenses associated with treating T1D-related complications, and studies show that these additional costs can be recouped within 3 years (31). Furthermore, adhering to the recommended change intervals helps prevent skin inflammation and potential declines in the performance of the IIS and injection site (23, 25, 32). This not only ensures the continued effectiveness of treatment but also promotes optimal glycemic control and minimizes long-term complications of DM, guaranteeing the safe use of CSII.
It is interesting to note that patient behavior sometimes differs from official guidelines provided by healthcare teams or manufacturers. This can be due to various reasons, including:
1. User experience: some patients may find that adhering to the manufacturer’s recommended frequencies works best for them in terms of comfort, convenience, or insulin delivery effectiveness. They might have experienced fewer issues or complications by following this schedule.
2. Perceived effectiveness: users may believe that adhering to the manufacturer’s recommendations leads to better glycemic control or fewer episodes of hypoglycemia or hyperglycemia.
3. Resistance to change: individuals can be resistant to change, especially if they have successfully followed a particular routine for an extended period. They might hesitate to adopt a new schedule recommended by their healthcare team.
4. Lack of awareness: patients may not be aware of the official guidelines provided by their healthcare team or may not fully understand the rationale behind those guidelines.
Regardless of the reasons, healthcare professionals must maintain open lines of communication with their patients. Regular discussions about treatment plans and ensuring that patients understand the potential benefits and risks associated with different approaches are essential. Additionally, patients should feel comfortable discussing their concerns and preferences with their healthcare providers. By working collaboratively, they can make informed decisions about their diabetes management. Ultimately, the goal is to ensure that patients achieve the best possible outcomes and quality of life while effectively and safely managing their condition. In this context, it is known that changing the catheter in a 2- to 3-day regimen is not an evidence-based practice, with most reports in the scientific literature coming from the manufacturers themselves (15, 23, 25).
A double-blind, randomized, crossover study conducted in the USA in 2010 aimed to evaluate the impact of non-adherence to the recommended change interval for IIS lines. The study compared the use of insulin aspart and lispro, and investigated the effects of extending the use of the infusion line beyond 48 h. The results showed that to maintain glycemic control it is crucial to change the IIS every 48 h. However, it was also observed that, in the short term, this loss of glycemic control had no significant impact on oxidative stress and glycation, which are markers of metabolic and vascular complications associated with DM (23).
These findings highlight the importance of regular adherence to the recommended change interval for IIS lines to maintain optimal glycemic control. While short-term non-adherence may not immediately result in significant metabolic and vascular complications, it is still essential to follow the recommended guidelines to ensure long- term T1D management and minimize the risk of complications.
In the 2010 study conducted by Schmid et al., which involved 24 patients and had two observation periods of 3 months each, the tolerability of 2-day use of IIS was compared to 4-day use. The findings of the study indicated that using the IIS for longer than 2–3 days increased treatment-related tolerability issues. Specifically, the number of catheter-related AEs was 290 with 2-day use compared to 495 with 4-day use.
Delaying the change of IIS beyond the recommended interval (48–72 h) can pose risks and lead to various complications. One concern is the increased risk of inflammation or infection at the infusion site. Prolonged use of the IIS can create a conducive environment for bacterial growth and may result in localized infections. Additionally, a delay in changing the IIS can erode the patient’s confidence in effectively managing AEs, as they may face more frequent complications.
Furthermore, progressive worsening of glycemic control may occur as a result of prolonged use of the IIS. Insulin absorption and delivery can be compromised, leading to fluctuations in blood glucose levels and difficulties in maintaining stable glycemic control. This can have negative implications for overall DM management and may require additional interventions to regain control.
Patients need to be aware of the recommended guidelines for IIS change and understand the potential risks associated with delaying the change. Regular and timely change of the IIS is crucial for minimizing complications, maintaining treatment efficacy, and ensuring optimal glycemic control. It is essential to consider these contexts when developing educational actions for patients and health educators in the management of DM. By addressing patient specific needs and concerns, personalized educational initiatives can guide the use of IIS cannulas and catheters best suited to their needs, emphasizing factors such as hygiene, potential AEs, and the importance of regular changes to ensure effective insulin delivery and well-being.
Medical devices, including CSII, are continually evolving, and updated guidelines may become available as more research and real-world experiences contribute to the knowledge base.
4.2 Alarm emission and interruption of insulin flow in response to catheter AEs
Risk management, as per the ISO 14971 standard, is essential for the certification and safe use of CSII. It generates requirements aimed at safeguarding against adverse effects on safety caused by physical component failures, development errors, and user errors (33). These devices increasingly rely on embedded software and communication mechanisms that classify them as information systems (34).
In this context, Requirements Engineering utilizes methods, techniques, and tools to establish a foundation for software development, ensuring the definition and analysis of security requirements (35). Therefore, the elicitation and specification of requirements are crucial to ensure that the intended system operates following the relevant needs and constraints. Inadequate security requirements can result in damages and losses, rendering the entire CSII system development process infeasible and potentially endangering human lives. In this context, considering that the CSII is a critical safety system, additional care is taken to ensure that the description of safety requirements is organized into the following hazard categories: operational, hardware, and software (36).
The detection of alarms and interruption of insulin flow as a response to AEs specifically related to the IIS catheter indicates that a significant number of patients encountered disruptions in their basal or bolus programming, resulting in occlusion alarms. However, it is worth noting that a considerable portion of patients did not experience such interruptions or receive corresponding alarms. Various clinical factors and individual responses to insulin therapy may contribute to the occurrence of occlusions. Therefore, regular monitoring and adherence to the recommended IIS change intervals remain essential in clinical practice to ensure optimal insulin delivery and reduce the risk of occlusions.
There is a notable concern regarding “silent occlusions” in IIS. “Silent occlusions” refer to occlusions that may go unnoticed because IIS systems rely on in-line pressure to detect flow and activate occlusion alarms. Consequently, this can lead to inadequate glucose control and delays in recognizing insulin failure, resulting in hyperglycemia, diabetic ketosis, or ketoacidosis (37).
To evaluate the difference in occlusion rates among rapid-acting insulin analogs, in vitro tests were performed for 5 days. These tests showed no differences between the analogs in the first 48 h at high (bolus) or low administration rates. However, after that, occlusion rates varied with the analog used, with a rate of 40.9% for insulin glulisine and 9.2% for insulin aspart. The authors concluded that early occlusions are uncommon and independent of insulin type and that infusion sets should be changed at least every 72 h (37).
4.3 Catheter and cannula AEs, and proposals for educational actions
A randomized trial conducted in 2014 (38) compared the function of a Teflon(®) catheter [Dupont(™), Wilmington, DE] or a steel catheter for CSII therapy in T1D and revealed some important findings on IIS-related AEs. In total, 13% of catheters were removed due to pain; 10% were accidentally tractioned out; 10% experienced erythema (redness or inflammation); 5% fell out due to loss of adhesion; and 4% were removed due to infection.
These AEs cover a variety of complications that can arise from using the IIS, including discomfort, accidental dislocation, local skin reactions, and infections. This emphasizes the importance of carefully monitoring and managing IIS to minimize complications and ensure the optimal functioning of insulin delivery systems. Regular assessment of the infusion site, proper insertion techniques, and adherence to recommended change schedules can help reduce the occurrence of AEs associated with IIS and enhance the overall effectiveness of insulin therapy.
In a 2010 German study, several AEs related to IIS were investigated. The most common AE was hyperglycemic events, accounting for 74.8% (615 AEs) of the reported events. Other AEs included erythema (redness), rash, pain, redness at the injection site, skin irritation, bleeding, and various less frequent events. Skin irritations were reported by the patients. Specifically, patients reported 33 injection site reactions for the 2-day usage time, while 59 injection site reactions were reported for the 4-day usage time. This suggests that longer use of the IIS was associated with a higher frequency of problems with the adhesive used to secure the set in place (39).
These findings highlight the potential for various AEs and complications associated with the use of IIS. Skin irritations, problems with adhesive, and cannula crimping are among the challenges that may arise. Regular monitoring of the infusion site, proper adhesive application, and adherence to recommended usage times can help mitigate these issues and enhance patient comfort and safety during insulin therapy.
The considerations mentioned by (20) concerning preparing and maintaining skin integrity during the use of IIS are as follows:
1. Hand washing before changing the catheter site: this is an important step to ensure cleanliness and reduce the risk of infection.
2. Opening the IIS package on a table or clean area: maintaining a clean environment during the process helps minimize contamination.
3. Cleaning the top of the insulin vial with alcohol: wiping the vial with alcohol before drawing insulin helps maintain sterility.
4. Cleaning the infusion site with prepackaged skin cleansing wipes or soap and water: thoroughly cleaning the skin at the infusion site helps remove dirt and bacteria. This can be done using the prepackaged skin cleansing wipes (preferably non-alcoholic) or soap and water.
5. Cleaning the skin in an outward spiral: when cleaning the skin, it is recommended to wipe in an outward spiral motion rather than back and forth. This helps prevent the introduction of contaminants into the infusion site.
6. Letting the site air dry: allowing the cleaned infusion site to air dry is preferred over blowing on it, as blowing can introduce bacteria from the breath.
7. Testing for dryness by touching the outside edge, not the center: when checking if the site is dry, it is advised to touch the outside edge of the site rather than the center. This minimizes the risk of introducing contaminants to the center of the site.
Following these considerations can contribute to maintaining skin integrity, reducing the risk of infection, and promoting the safe and effective use of IIS.
Unexplained hyperglycemia can pose a significant challenge to the success of insulin infusion therapy. In cases where unexplained glucose levels remain elevated (>250 mg/dL or 13.88 mmol/L) and do not decrease at least 2 h after a correction bolus, the recommendation is to change the IIS and reservoir with insulin from a new vial or to consider manual dosing. The patient should make an effort to identify the cause of IIS failures, such as dislocation, blockage, scar tissue, or leakage, and take note of the circumstances if possible. If glycemic control cannot be restored within a reasonable period if nausea and vomiting persist, or if the patient’s condition continues to worsen, emergency care may be necessary (20, 38).
When it comes to disconnections of the CSII for activities such as showering or swimming, it is recommended to check blood glucose levels both before and after the disconnection period. If the anticipated disconnection is expected to last for an hour or longer, it is commonly suggested that the patient switch to basal insulin by administering a bolus dose immediately before the disconnection. This approach should be repeated if the disconnection time is extended, with intermittent CSII reconnections, until the disconnection period has ended (20).
These guidelines aim to address specific situations related to IIS use and help manage challenges such as unexplained hyperglycemia and temporary pump disconnections. Following these recommendations can assist in maintaining glycemic control and ensuring patient safety during the use of insulin infusion therapy.
Indeed, when a patient experiences IIS failure, it is important for the healthcare team to thoroughly review the site preparation and insertion technique. They should inspect the site, skin, and anchor line for any abnormalities or issues. Blood glucose and continuous glucose monitoring data should be carefully examined to identify any unexplained hyperglycemia that may be related to the IIS failure. It is also valuable to help the patient reconstruct the circumstances surrounding the episode, as this can provide insights and enable the development of self-care skills to prevent or manage future occurrences.
To deal with such occurrences, we list here possible proposals to solve the problems:
• Providing comprehensive education and training to patients on proper handling and care of the IIS catheter to minimize accidental catheter traction, catheter knotting, and catheter bending.
• Enhancing communication between healthcare providers and patients to promptly identify and address issues.
• Improving the accuracy and effectiveness of insulin flow occlusion alarms to promptly detect and communicate potential obstructions.
When it comes to diabetes education for patients using CSII treatment, there is a need to enhance training strategies. This includes increasing the availability of training materials from device manufacturers and suppliers. Additionally, it is recommended that healthcare professionals conduct in-person visits shortly after initial patient training to assess equipment settings, IIS placement, and application techniques, making necessary adjustments as needed.
By enhancing the quality of education and training materials, providing personalized support, and placing emphasis on ongoing maintenance, healthcare professionals can empower patients to effectively manage their treatment and optimize their insulin therapy. This approach ensures that patients who have difficulty identifying occlusion issues receive the appropriate guidance and assistance they need.
A study by Deeb et al. (40) aimed to evaluate the impact of targeted education on improving competence in solving alarm problems. They found that verbal and written instructions on alert solutions were well-received by patients, resulting in significant reductions in warnings and errors. Another review study conducted by Minicucci (16) highlighted that the safety and effectiveness of using CSII systems are strongly influenced by the level of diabetes education.
The educational approach directed toward patients who use CSII by the multi-professional team at the study site has proven highly beneficial for enhancing patients’ competence and response to diabetes management. Several noteworthy features of this approach in the Diabetes Center Insulin Pump Ambulatory program are as follows:
• Multidisciplinary team: the presence of a multidisciplinary healthcare team on-site is crucial for addressing the diverse needs of patients. This team includes psychologists, nutritionists, physical educators, nurses, insulin pump educators, and doctors. This holistic approach not only addresses the medical aspect but also focuses on the overall well-being of the patient.
• Educational initiatives: prioritizing diabetes education and proper device usage is essential for patients to comprehend their condition and the benefits of insulin therapy. The education provided by the Diabetes Center Insulin Pump Ambulatory team professionals equips patients with the knowledge and skills to manage their health effectively.
• Initial training: the initial training provided is tailored for newly diagnosed patients. This ensures that they acquire the necessary skills to safely and effectively use the device right from the start.
• Ongoing guidance: continual education and periodic guidance are essential for maintaining the quality of care over time and keeping patients informed about best practices in diabetes and insulin device management. The text messaging approach proves to be an effective way to maintain regular contact with patients.
• Age segmentation: segmenting patients into different age groups for educational guidance is a unique approach at the site. This recognizes that needs and challenges vary across different life stages, allowing the healthcare team to customize their guidance for each group. Patients are grouped into the following age categories for educational support: 0–3 years (group 1); 4–8 years (group 2); 8–10 years (group 3); 11–13 years (group 4); 13–15 years (group 5); 16 to 18 (group 6); 18–20 (group 7); 21–25 years (group 8); and over 30 years (group 10).
5 Conclusion
Educating patients about common causes of IIS failure is crucial for ensuring their safety and optimizing CSII therapy. The research results can serve as a guide to improve the understanding of possible AEs associated with IIS failures, thus enhancing patient education and treatment.
Standardized guidelines for preventing and diagnosing IIS issues are essential for maximizing the benefits of CSII therapy. While the optimal time to switch to IIS is still debated in the literature, recent studies and advancements in IIS science are shedding light on this matter. It is important to address problems such as unexplained hyperglycemia and occlusions when discussing IIS-related issues.
Patients should be trained and encouraged to follow the manufacturer’s recommendation regarding changing the cannula and catheter every 2–3 days. While the cost of frequent catheter changes may be a consideration, it should not be the determining factor for neglecting necessary changes.
The key findings from the research include:
• Serious situations (AEs) occur in cases where the occlusion alarm is not activated but the insulin flow is interrupted, or in less worrisome situations with alarm activation, without interruption of the insulin flow.
• Most individuals adhere to the recommended frequency of changing the IIS cannula and catheter within the recommended time.
• Individuals who change the cannula and catheter on different days tend to keep the catheter longer than recommended but usually change the cannula within 3 days.
• Prolonged catheter use is associated with an increased frequency of catheter-related AEs.
• Catheter-related accidental traction and catheter bending typically occur during everyday activities, while cannula-related issues directly affect blood glucose levels.
• AEs related to the IIS cannula often lead to skin problems.
By incorporating these findings into patient education and treatment protocols, healthcare professionals can enhance patient safety, improve glycemic control, and minimize the occurrence of AEs related to IIS failures. It is important to note that the main limitation of this study is its reliance on data from a single center, which restricts the generalizability of the findings. Therefore, conducting extended research through randomized trials or a prospective multicenter study to investigate clinical outcomes would provide valuable insights.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by Research Ethics Committee – University Federal of São Paulo. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
Author contributions
AN: Conceptualization, Formal analysis, Investigation, Methodology, Writing – review & editing, Writing – original draft. LM: Conceptualization, Formal analysis, Investigation, Methodology, Writing – review & editing, Funding acquisition, Project administration, Resources, Supervision, Validation, Visualization. MG: Conceptualization, Investigation, Project administration, Resources, Supervision, Validation, Writing – review & editing, Writing – original draft. PP: Formal analysis, Writing – original draft. TO: Formal analysis, Writing – original draft. AM: Formal analysis, Writing – original draft. SD: Formal analysis, Writing – original draft. DC: Formal analysis, Writing – original draft. SA: Formal analysis, Funding acquisition, Resources, Writing – original draft. FT: Formal analysis, Conceptualization, Investigation, Methodology, Validation, Writing – original draft, Writing – review & editing, Visualization. TC: Conceptualization, Formal analysis, Investigation, Methodology, Validation, Writing – original draft, Writing – review & editing, Funding acquisition, Project administration, Resources, Supervision, Visualization.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work was supported by the Coordination for the Improvement of Higher Education Personnel – Brazil (CAPES, Finance Code 001), the Research Support Foundation of the State of São Paulo (FAPESP n° 2018/22094–0), and the National Council for Scientific and Technological Development (CNPq 308721/2020–9).
Acknowledgments
We would like to thank the patients, family members, and professionals of the Diabetes Center Insulin Pump Ambulatory, Federal University of São Paulo.
Conflict of interest
SA is the director of DeltaLife.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Diabetes Control and Complications Trial Research GroupNathan, DM, Genuth, S, Lachin, J, Cleary, P, Crofford, O, et al. The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. N Engl J Med. (1993) 329:977–86. doi: 10.1056/NEJM199309303291401
2. Heinemann, L, Fleming, GA, Petrie, JR, Holl, RW, Bergenstal, RM, and Peters, AL. Insulin pump risks and benefits: a clinical appraisal of pump safety standards, adverse event reporting, and research needs. Diabetes Care. (2015) 38:716–22. doi: 10.2337/dc15-0168
3. Pickup, J, Mattock, M, and Kerry, S. Glycaemic control with continuous subcutaneous insulin infusion compared with intensive insulin injections in patients with type 1 diabetes: meta-analysis of randomised controlled trials. BMJ. (2002) 324:705–6. doi: 10.1136/bmj.324.7339.705
4. Garvey, K, and Wolfsdorf, J. The impact of technology on current diabetes management. Pediatr Clin N Am. (2015) 62:873–88. doi: 10.1016/j.pcl.2015.04.005
5. Johnson, SR, Cooper, MN, Jones, TW, and Davis, EA. Long-term outcome of insulin pump therapy in children with type 1 diabetes assessed in a large population-based case-control study. Diabetologia. (2013) 56:2392–400. doi: 10.1007/s00125-013-3007-9
6. Ribeiro, MEB, Junior, DRL, Custodio, R, and Martinelli, CE. Continuous insulin therapy versus multiple insulin injections in the management of type 1 diabetes: a longitudinal study. Revista Paulista Pediatria. (2016) 34:86–90. doi: 10.1016/j.rpped.2015.06.011
7. Chaput de Saintonge, DM, and Vere, DW. Controlled trials. Lancet. (1977) 310:759. doi: 10.1016/S0140-6736(77)90256-2
8. Conget Donlo, I, Serrano Contreras, D, Rodríguez Barrios, JM, Levy Mizrahi, I., Castell Abat, C, Roze, S., et al. Análisis coste-utilidad de las bombas de insulina frente a múltiples dosis diarias en pacientes con diabetes mellitus tipo 1 en españa [Cost-utility analysis of insulin pumps compared to multiple daily doses of insulin in patients with type 1 diabetes mellitus in Spain]. Rev Esp Salud Publica. (2006) 80:679–95. doi: 10.1590/s1135-57272006000600008
9. Lenhard, M. J., and Reeves, G. D. (2001). Christiana Care health services (Dr Lenhard), and the division of pediatric endocrinology, DuPont Hospital for children (Dr Reeves), Wilmington, Del; and Jefferson Medical College. Available at: https://jamanetwork.com/.
10. Pickup, JC, Freeman, SC, and Sutton, AJ. Glycaemic control in type 1 diabetes during real time continuous glucose monitoring compared with self monitoring of blood glucose: meta-analysis of randomized controlled trials using individual patient data. BMJ. (2011) 343:d3805. doi: 10.1136/bmj.d3805
11. Roze, S, Valentine, WJ, Zakrzewska, KE, and Palmer, AJ. Health-economic comparison of continuous subcutaneous insulin infusion with multiple daily injection for the treatment of type 1 diabetes in the UK. Diabet Med. (2005) 22:1239–45. doi: 10.1111/j.1464-5491.2005.01576.x
12. Saunders, R, Boye, K, van Brunt, K, Pollock, R, and Valentine, W. Cost-effectiveness of rapid-acting analog insulin for type 1 diabetes in the UK setting. Value Health. (2015) 18:A610. doi: 10.1016/j.jval.2015.09.2114
13. Weissberg-Benchell, J., Antisdel-Lomaglio, J., and Seshadri, R. (2003). Insulin pump therapy a meta-analysis. Available at: http://diabetesjournals.org/care/article-df/26/4/1079/659360/dc0403001079.pdf
14. Silva Júnior, WS, Gabbay, M, Lamounier, R, and Bertoluci, M. Insulinoterapia no diabetes mellitus tipo 1 (DM1). Diretriz Oficial Sociedade Brasileira Diabetes. (2022). 1–18. doi: 10.29327/557753.2022-5
15. Clausen, TS, Kaastrup, P, and Stallknecht, B. Effect of insulin catheter Wear-time on subcutaneous adipose tissue blood flow and insulin absorption in humans. Diabetes Technol Ther. (2009) 11:575–80. doi: 10.1089/dia.2009.0058
16. Minicucci, WJ. Use of continuous subcutaneous insulin infusion and its indications. Arq Bras Endrocrinol Metab. (2008) 52:340–8. doi: 10.1590/S0004-27302008000200022
17. Tenorio, FS, Martins, LEG, and Cunha, TS. Accuracy of a low-cost continuous subcutaneous insulin infusion pump prototype: in vitro study using combined methodologies. Ann Biomed Eng. (2021) 49:1761–73. doi: 10.1007/s10439-020-02721-8
18. Ross, P, Gray, A, Milburn, J, Kumarasamy, I, Wu, F, Farrand, S, et al. Insulin pump- associated adverse events are common, but not associated with glycemic control, socio- economic status, or pump/infusion set type. Acta Diabetol. (2016) 53:991–8. doi: 10.1007/s00592-016-0897-2
19. US Food & Drug Administration. (2014) MDR adverse event codes. Date unknown Available at: https://www.ecfr.gov/current/title-21/chapter-I/subchapter-H/part-803#part-803
20. Evert, AB, Bode, BW, Buckingham, BA, Nardacci, E, Verderese, CA, Wolff- McDonagh, P, et al. Improving patient experience with insulin infusion sets: practical guidelines and future directions. Diabetes Educ. (2016) 42:470–84. doi: 10.1177/0145721716642526
21. Heinemann, L., and Krinelke, L. (2012). Insulin infusion set: The Achilles heel of continuous subcutaneous insulin infusion. J Diabetes Sci Technol. (2012) 6:954–64. doi: 10.1177/193229681200600429
22. Deiss, D, Adolfsson, P, Alkemade-van Zomeren, M, Bolli, GB, Charpentier, G, Cobelli, C, et al. Insulin infusion set use: European perspectives and recommendations. Diabetes Technol Ther. (2016) 18:517–24. doi: 10.1089/dia.2016.07281.sf
23. Thethi, TK, Rao, A, Kawji, H, Mallik, T, Yau, CL, Christians, U, et al. Consequences of delayed pump infusion line change in patients with type 1 diabetes mellitus treated with continuous subcutaneous insulin infusion. J Diabetes Complicat. (2010) 24:73–8. doi: 10.1016/j.jdiacomp.2009.03.002
24. Bonato, L, Taleb, N, Gingras, V, Messier, V, Gobeil, F, Ménard, J, et al. Duration of catheter use in patients with diabetes using continuous subcutaneous insulin infusion: a review. Diabetes Technol Ther. (2018) 20:506–15. doi: 10.1089/dia.2018.0110
25. Kerr, D, Morton, J, Whately-Smith, C, Everett, J, Phil, M, and Begley, JP. Laboratory-based non-clinical comparison of occlusion rates using three rapid-acting insulin analogs in continuous subcutaneous insulin infusion catheters using low flow rates. J Diabetes Sci Technol. (2008) 2:450–5. doi: 10.1177/193229680800200314
26. Estock, JL, Codario, RA, Keddem, S, Zupa, MF, Rodriguez, KL, and DiNardo, MM. Insulin pump-associated adverse events: a qualitative descriptive study of clinical consequences and potential root causes. Diabetes Technol Ther. (2023) 25:343–55. doi: 10.1089/dia.2022.0498
27. Cescon, M, DeSalvo, DJ, Ly, TT, Maahs, DM, Messer, LH, Buckingham, BA, et al. Early detection of infusion set failure during insulin pump therapy in type 1 diabetes. J Diabetes Sci Technol. (2016) 10:1268–76. doi: 10.1177/1932296816663962
28. Pickup, JC, Yemane, N, Brackenridge, A, and Pender, S. Nonmetabolic complications of continuous subcutaneous insulin infusion: a patient survey. Diabetes Technol Ther. (2014) 16:145–9. doi: 10.1089/dia.2013.0192
29. Neves, ALD, Martins, LEG, Gabbay, MAL, Cavicchioli, G, Tenorio, FS, and Cunha, TS. Insulin pump-associated adverse events in a Brazilian reference Center for the Treatment of diabetes mellitus: proposal for a taxonomy of device failures in adults, adolescents, and children. J Diabetes Sci Technol. (2022) 1–8:19322968221106196. doi: 10.1177/19322968221106196
30. Oliveira, ÉH, and Galves, VF. Conjunto de Infusão In: M Gabbay, editor. Manual Prático de Bombas de Insulina, autora/coordenadora (2019). Clannad.
31. David, G, Shafiroff, J, Saulnier, A, and Gunnarsson, C. Multiple daily injection therapy (MDI) versus durable insulin pump therapy in type II diabetics: a breakeven analysis. Value Health. (2012) 15:A65. doi: 10.1016/j.jval.2012.03.359
32. Schmid, V, Hohberg, C, Borchert, M, Forst, T, and Pfützner, A. Pilot study for assessment of optimal frequency for changing catheters in insulin pump therapy-trouble starts on day 3. J Diabetes Sci Technol. (2010) 4:976–82. doi: 10.1177/193229681000400429
33. Martinazzo, A, Martins, L. E. G, Aredes, S. V, and Cunha, T. S. (2021). Risk management of a low-cost insulin infusion. IEEE 34th International Symposium on Computer-Based Medical Systems (CBMS). Aveiro, Portugal. 336–341
34. Moreno, ED. Segurança em sistemas embarcados modernos desafios e tendências. Aracaju: ArtNer Comunicação (2015). XXp. II.
35. Grande JI., Especificação e implementação de uma ferramenta para gerenciamento de requisitos. [dissertação mestrado]. Orientador: Luiz Eduardo Galvão Martins, Piracicaba, SP (2006).
36. Martins, L. E. G., De, Faria H., Cunha, T., De, Oliveira T., Casarini, D. E., and Colucci, J. A. (2015). Development of a low-cost insulin infusion pump: Lessons learned from an industry case. In: 2015 IEEE 28th International Symposium on Computer-Based Medical Systems, Sao Carlos, Brazil (2016), pp. 338–343.
37. Slover, RH. Best ways and practices to avoid insulin pump catheter occlusions. Diabetes Technol Ther. (2016) 18:118–9. doi: 10.1089/dia.2016.0025
38. Patel, PJ, Benasi, K, Ferrari, G, Evans, MG, Shanmugham, S, Wilson, DM, et al. Randomized trial of infusion set function: steel versus teflon. Diabetes Technol Ther. (2014) 16:15–9. doi: 10.1089/dia.2013.0119
39. Pfützner, A, Sachsenheimer, D, Grenningloh, M, Heschel, M, Walther- Johannesen, L, Gharabli, R, et al. Using insulin infusion sets in CSII for longer than the recommended usage time leads to a high risk for adverse events: results from a prospective randomized crossover study. J Diabetes Sci Technol. (2015) 9:1292–8. doi: 10.1177/1932296815604438
Keywords: insulin infusion system, technology, diabetes mellitus, type 1, catheters, cannula
Citation: Neves ALD, Martins LEG, Gabbay MAL, Pascali P, de Oliveira T, Martinazzo A, Dib SA, Casarini DE, Aredes SV, Tenorio FS and Cunha TS (2023) Insulin infusion sets associated with adverse events: strategies for improved diabetes education. Front. Med. 10:1275394. doi: 10.3389/fmed.2023.1275394
Edited by:
Allah Nawaz, Joslin Diabetes Center and Harvard Medical School, United StatesReviewed by:
Sailesh Palikhe, University of Kansas Medical Center, United StatesHalima Nazar, Jinnah University for Women, Pakistan
Raj Mongre, Boston Children's Hospital and Harvard Medical School, United States
Safila Naveed, University of Karachi, Pakistan
Copyright © 2023 Neves, Martins, Gabbay, Pascali, de Oliveira, Martinazzo, Dib, Casarini, Aredes, Tenorio and Cunha. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Tatiana Sousa Cunha, dHMuY3VuaGFAdW5pZmVzcC5icg==
†ORCID: Ana Lucia Domingues Neves, https://orcid.org/0000-0001-5172-0428
Luiz Eduardo Galvão Martins, https://orcid.org/0000-0002-7266-5840
Fernanda Silva Tenorio, https://orcid.org/0000-0003-1966-3384
Tatiana Sousa Cunha, https://orcid.org/0000-0001-9070-1414