
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Med. , 07 July 2023
Sec. Dermatology
Volume 10 - 2023 | https://doi.org/10.3389/fmed.2023.1208817
This article is part of the Research Topic Patients-Oriented Treatments for Chronic Inflammatory Skin Diseases View all 8 articles
 Laura Macca1†
Laura Macca1† Federica Li Pomi1†
Federica Li Pomi1† Ylenia Ingrasciotta2
Ylenia Ingrasciotta2 Pietro Morrone3Gianluca Trifirò2
Pietro Morrone3Gianluca Trifirò2 Claudio Guarneri4*
Claudio Guarneri4*Psoriasis and hidradenitis suppurativa are chronic inflammatory skin diseases that can develop together, negatively impacting on the patient’s quality of life. We aimed to review the most up-to-date information regarding the epidemiology, pathogenesis, clinical presentation and possible therapeutical choices in patients with both psoriasis and hidradenitis suppurativa, thus linking these two autoimmune and autoinflammatory conditions. A narrative review of articles dating from 2017 to 2022 has been performed using the PubMed database. We analyzed the case reports and case series found in the literature regarding patients who suffered from both psoriasis and HS. Psoriasis arose before hidradenitis suppurativa in the majority of cases, while only a minority of them had hidradenitis suppurativa before psoriasis. Interestingly, some patients suffered from paradoxical hidradenitis suppurativa following biological therapy administered to treat the already present psoriasis. Lastly, new biological drugs have been marketed with great success for the outcome of psoriasis, but similar progress did not happen for hidradenitis. Novel therapeutic approaches and lines of research are needed for the treatment of these pathologies, even if concomitant, in order to improve patient’s quality of life.
Hidradenitis suppurativa (HS) is a debilitating, chronic, autoinflammatory cutaneous disease characterized by the inflammation of hair follicles in apocrine gland-rich areas (1, 2). Its prevalence estimates vary, ranging between 0.7 and 1.2%, with a more marked predisposition among females (3). It typically affects the intertriginous (axillary, submammary and inguinal), and anogenital areas, which later can lead to the development of abscesses, sinus tracts and scars, with devastating impact on patient’s quality of life (QoL) (1). The pathogenesis of HS is not yet well understood, but there is a general agreement on considering HS as a multifactorial disease having a plenty of implications with immunological factors and recruitment of self-perpetuating inflammatory mediators, which makes HS treatment a real challenge (4). HS is known to have a substantial impact on the QoL, being also associated with various comorbidities including increased cardiovascular risk, gastrointestinal, rheumatological and psychiatric comorbidities, as well as an increased risk of carcinogenesis (5). Having regard to this point of view, HS has been increasingly widely recognized as an inflammatory disease with several systemic implications, just like psoriasis (5). In fact, psoriasis is a chronic, immune-mediated, inflammatory disease which can also affect nails and joints (6). The reported prevalence is highly variable across countries ranging between 0.09 and 11.4%, with age-specific incidence rates showing a dual peak around 30–39 years of age and a second peak around 50–59 or 60–69 years of age (7, 8). Clinical presentation is morphologically and topographically heterogeneous. Plaque psoriasis, accounting for about 80% of all cases, is the classical phenotype, being characterized by well-defined, scaly, erythematous plaques, often covered by silvery scales, mostly affecting the extensor surfaces, scalp, and lumbosacral region (9). For a long time evaluated merely as a cutaneous disease, psoriasis is now recognized as a systemic inflammatory condition that shares pathogenetic pathways with several other disorders, including psoriatic arthritis, metabolic syndrome, cardiovascular diseases, inflammatory bowel diseases, uveitis, non-alcoholic fatty liver disease and HS (10). The coexistence of psoriasis and HS has been lately described, even if a possible association between them is yet to be firmly established. Several case reports of co-occurrence of HS and psoriasis suggest a causal relationship, but firm epidemiological data are lacking. To assess the link between HS and psoriasis, we performed a narrative review of the up-to-date literature on the topic (11–24).
A bibliographic search was conducted on PubMed database1 using the search string: “Psoriasis” [All Fields] AND “Hidradenitis suppurativa” [All Fields]. Basing on the abstract content, we collected papers concerning this association. Only papers written in English language, concerning humans and with 5 years’ time limits were included. Papers identified as irrelevant to the topic in question were excluded.
As of 1 November 2022, a PubMed search of “Psoriasis” AND “Hidradenitis suppurativa” yielded 21 articles. Among these, seven were excluded as not relevant and/or because the full text was not available, whereas 14 papers were selected as matching our search. Four case series and 10 case reports out of these 21 papers were studied and reviewed for epidemiological data, clinical features and treatment/outcomes. All these studies are summarized in Table 1.
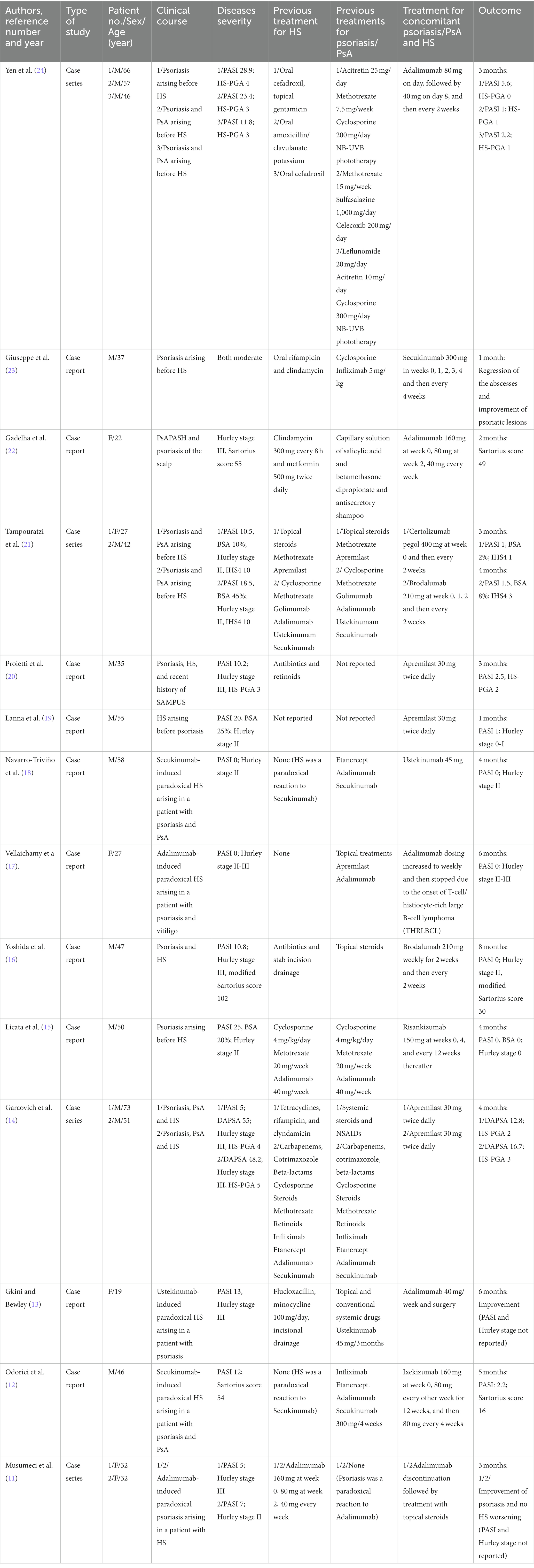
Table 1. Reported cases of concomitant psoriasis and hidradenitis suppurativa.
The coexistence of psoriasis and HS had been revealed in several case reports and case series, whereas a established epidemiological evidence for an association between these diseases is still lacking. However, a large-scale population-based study revealed a significant association between psoriasis and HS, with an 80% increase in the odds for HS among patients with psoriasis versus matched controls (25). Interestingly, patients suffering from both diseases were younger and were more likely to be smokers and obese as compared to those affected exclusively by psoriasis, confirming the role of common inflammatory pathways in the pathogenesis of these conditions (25). Similarly, a recent nationwide Korean study evaluating the prevalence of psoriasis in HS-affected patients, highlighted that psoriasis was significantly increased compared to control subjects with a multivariate odd ratio (OR) of 4.6 (26). Moreover, HS was found to be associated to plaque psoriasis and palmar-plantar pustulosis in 9 and 11% of cases, respectively (27). The high prevalence of psoriasis in patients with HS was stated by the Authors on the basis of the common pathogenetic pathways (28).
The key moment in HS pathogenesis involves the infundibular epithelium of the apocrine glands and it is represented by the hyperkeratosis and the hyperplasia due to the interaction of environmental factors, genetic predisposition and immune dysregulation (5). This leads to follicular occlusion, followed by dilatation and rupture with a perifollicular lymphohistiocytic inflammation and development of retained hair tracts in pseudocysts and fistulas (29). Environmental factors include mechanical stress, metabolic syndrome, obesity, smoking, and dysbiosis (30). Genetic predisposition lays on alterations in Notch and γ-Secretase signaling pathways and in inflammasome response. As suggested by Moltrasio et al. three different forms of HS are to date recognized: the sporadic, the familial and the syndromic one (31). In each of these three forms the susceptibility and onset of the disease and the response to treatment are associated with different genetic variants, including genes encoding gamma-secretase subunits, while others involve autoinflammatory and/or keratinized genes (31). With regard to the immune dysregulation, several cytokines seem to be particularly expressed in the immunopathogenesis of HS (4). The “primum movens” is represented by the recognizing by Toll like receptors (TLRs) or NOD-like receptors (NLR) of bacteria and cellular debris as pathogen- and damage-associated molecular patterns (PAMPs and DAMPs) in the dermis, resulting in the activation of the innate immunity (30). PAMPs and DAMPs stimulate the inflammasome response thus activating the NOD-like receptor protein 3 (NLRP3) in macrophages and neutrophils followed by the production of caspase-1 and proinflammatory cytokines (e.g., TNF-α and IL-1β) (30). IL-1β causes the release of chemokines by fibroblasts, namely C-X-C motif chemokine ligand (CXCL)-1 and CXCL6, that will primarily draw neutrophils (30). Tumor necrosis factor-α (TNF-α), coming from macrophages and dendritic cells, upregulates TLR and provokes the releasing by keratinocytes of several chemokines, like CXCL8, CXCL11, C-C motif chemokine ligand (CCL)-20, and CCL2, which draw lymphocytes, neutrophils and monocytes into the dermis (30). Interleukin (IL)-23 and IL-12 produced by activated dendritic cells, favor polarization of CD4+ T lymphocytes toward T-helper lymphocytes type 17 (Th17) and Th1. On the same way, IL-17 produced by Th17 increases macrophage production of IL-1β and TNF-α, enhancing the immune response (32). Complement pathway activation by PAMPs and DAMPs takes part to the activation and recruitment of neutrophils performed by C3a and C5a (30). Interestingly, HS patients’ lesions express IL-10, an anti-inflammatory cytokine induced by the autocrine action of TNF in macrophages. IL-10 downregulates T cells and thus immune responses by suppressing the monocytes and macrophages production of pro-inflammatory mediators (33). Lastly, it has been noted a significant concentration of IL-36 α, −β, and -γ associated with a dysregulation on IL-36 receptor antagonist (IL-36RA) in lesional and perilesional HS skin (33). The unrestricted IL-36 signaling in these patients could serve as a potential target for future therapeutic strategies. Psoriasis shares several pathogenic pathways with HS, both being characterized by unbalanced interactions between the innate and the adaptive immune systems. Dendritic cells, activated by a variety of cell types (e.g., keratinocytes, natural killer T cells, macrophages, etc.), secrete IL-23 and IL-12, which in turn induce differentiation of native T-cells, respectively, to Th17 and Th1. IL-23 play a pivotal role in the survival and proliferation of Th17 and Th22 cells (9). Th17 cells produce IL-17 while Th1 and Th22 cells secrete TNF-α and IL-22, respectively. In psoriasis all these cytokines induce the activation of intracellular signal transduction in keratinocytes, leading to their overblown proliferation together with the augmented expression of angiogenic mediators, endothelial adhesion molecules, and immune cells infiltration into injured skin (34, 35). This immune dysregulation, based on genetic predisposition (presence of human leukocyte antigen (HLA) Cw6) and epigenetic modifications (desoxyribonucleic acid (DNA) methylation and histone acetylation), and environmental factors, such as smoking, alcohol, diet, infections, and mechanical stress, results in the inflammatory cascade that leads to erythematous scaly patches or plaques (34, 35). Epigenetic mechanism and their alterations play a pivotal role in keratinocytes differentiations and therefore in HS and psoriasis onset. Among them microRNAs (miRNA) are involved in keratinocytes proliferations and differentiations (36). MiR-146a and MiR-155have been found upregulated in psoriasis, thus promoting TNF expression, and correlating with IL-17 – driven inflammation (36).
The typical lesions of HS include deep, inflammatory, painful nodules, abscesses, suppurative sinus tracts or tunnels, bridged scars and double-ended comedones (37, 38). Frequent complications of subcutaneous nodules and abscesses are represented by rupture, bleeding and production of purulent secretions, with serious consequences on the patient’s QoL. Patients are often restricted in their daily and interpersonal activities as the lesions are painful, foul-smelling, burning, and itchy (3). In a minority of patients, HS presents as “syndromic” being associated with other immune-mediated inflammatory diseases (39). The presence of HS is distinctive for the PASH (Pyoderma gangrenosum, Acne, and Suppurative Hidradenitis), PAPASH (Pyogenic Arthritis, Pyoderma gangrenosum, Acne, and Suppurative Hidradenitis), PsaPASH (Psoriatic Arthritis, Pyoderma gangrenosum, Acne, and Suppurative Hidradenitis) and PASS syndromes (Pyoderma gangrenosum, Acne, and Suppurative Hidradenitis, and Ankylosing Spondylitis) (39). The complex comorbidity profile and significant heterogeneity in clinical presentation, further complicates the diagnostic framing of these rare syndromic forms. Since clinical manifestations of HS are polymorphic, various phenotypic classifications have been proposed. With regard to this, Gonzalez-Manso has recently hypothesized two endotypic clusters. To cluster 1 belong non-obese males with early onset disease and a positive history of pilonidal sinus (40). Clinically, the lesions are mostly nodular, localized in the posterior sites; in addition, elevated serum levels of IL-10 and the presence of gamma-secretase mutations were found (40). Cluster 2 is mostly characterized by late-onset disease in obese females (40). Sinuses and abscesses, located in the anterior sites, are more frequent than nodules; furthermore, elevated serum levels of IL-1, C-reactive protein, IL-17 and IL-6 were found (40). Ultrasound imaging can further define lesion morphology and depth, thus enabling the precise staging of the disease (41). In this regard, a disagreement between clinical and ultrasound scores is emerging, as ultrasound is proving capable of detecting non-clinically evident HS lesions, in particular fistulas, suggesting the greater sensitivity of ultrasound compared to clinical scores (42). Similarly to psoriasis, numerous tools have been using. Hurley staging is the most recommended in the clinical setting due to its ease of use and usefulness (43). However, it is a static score since it does not calculate the number of injured areas and, above all, it does not allow to evaluate the activity of the disease or the response to treatment. A refined Hurley score was then proposed, that further distinguishes mild (A), moderate (B), and severe (C) forms in the context of stages I and II (44). The Modified Sartorius Score (MSS) is an additional scoring system which evaluates disease severity from a more clinically relevant point of view (32). A novel dynamic scoring system to assess HS severity is represented by International Hidradenitis Suppurativa Severity Score System (IHS4). The determination of IHS4 requires counting the nodules, abscesses and draining tunnels, making it clear to use in both research and clinical practice (45).
With regard to psoriasis, it usually presents with a plethora of clinical features that widely differ among some variants, including chronic plaque, guttate, erythrodermic, and pustular form (35, 46). Different variants can sometimes occur in the same patient (47). Beyond the peculiar characteristics, all phenotypes share peculiar features such as erythema, thickening and scales (48). Plaque psoriasis represents approximately 80 to 90% of all cases of psoriasis (49). It presents with sharply demarcated, erythematous, scaly patches or plaques and, although it can affect any part of the body, commonly occurs on the extensor surfaces, such as the elbows and knees, on the trunk, mostly in the sacral region, on the scalp and on the intergluteal fold (50). Based on these three characteristics and on the extent of the lesions, Psoriasis Area Severity Index (PASI) score and Body surface area (BSA) score are the most used tools to assess the severity of psoriasis and the treatment outcomes (51). The coexistence of HS and psoriasis in the same patient is rare, but well described in literature (11–24). In fact, it is well known that these two pathologies share common pathogenetic pathways which can induce both psoriatic plaques and the inflammatory nodules of HS.
On this topic, we reviewed all the case reports and case series available in the literature regarding patients who suffered from both psoriasis and HS. In most cases, psoriasis outbreak preceded the diagnosis of HS (12, 13, 15, 17, 18, 21, 23, 24). Only a minority of patients developed HS before psoriasis (11, 19). The analysis of data clearly suggests an important pathogenic link between the two entities, where the IL-23/Th17 axis plays a crucial role (15). Moreover, some patients suffered from paradoxical HS following biological therapy to treat the already present psoriasis (12, 13, 17, 18). Paradoxical immune-mediated inflammatory reactions, defined as the development of inflammatory immune-mediated tissue manifestations, are increasingly associated with biological targeted therapy (52). HS has also been reported to be paradoxically induced in patients treated with TNFα blockers, such as infliximab or adalimumab (53). Complete resolution of paradoxical hidradenitis suppurativa has been found to occur after drug discontinuation or switching to another biological agent, whereas reintroduction of the same biological agent resulted in the relapse of the disease (54). A case of unexpected flare of HS, probably due to a paradoxical reaction to ustekinumab, an anti-IL12/23 antibody, has been recently described (13). Also, secukinumab, a human IgG1κ monoclonal antibody that binds to the IL-17A, can trigger a paradoxical HS reaction (12). Marasca tried to summarize the immunological complex subtending the pathogenesis of autoinflammatory diseases, showing the potential dual role of secukinumab in two differen cases of HS, as trigger of pardoxical HS, successflully treated with the TNF-α inhibitor adalimumab, or capable of controlling HS caused by treatment with adalimumab, respectively (55). Th17/ILC3 lymphocytes, with high levels of IL-1β, TNF-α, IL-17 and peripheral recruitment of IL-17-producing neutrophils and Th17-cells represent the main hallmarks of hidradenitis suppurativa immune response pattern. In addition, paradoxical HS responses have been recently reported in patients with rheumatoid arthritis or psoriatic arthritis (PsA) during long-term treatment with TNF inhibitors, tocilizumab or rituximab (52–54). Physicians should be aware of this possible complication, so the causative agent should be stopped, and other treatment options be considered.
The hitch in the therapeutic management of HS is represented by the lack of approval to several biologic drugs by the United States Food and Drug Administration (FDA) and by the European Medicines Agency (EMA) (4). As recommended in international guidelines, the first ‘steps’ of oral treatment are represented by clindamycin and rifampicin, both administered at a dose of 300 mg twice daily for an average duration of 10 weeks in patients with Hurley stage II-III (30). The use of acitretin in HS, exerting antiproliferative activity in keratinocytes, is characterized by controversial outcomes given the high recurrence rates in monotherapy and overall response rates of 50% (30, 56). So, it is categorized as third line treatment (30). Isotretinoin has shown discordant results in HS, however it could be considered in patients with severe concomitant acne (30, 57, 58). The well-known influence of sexual hormones on the course of the disease, suggested by perimenstrual exacerbations and improvement during pregnancy, has been the rationale of use of estroprogestinic drugs (e.g., ethinylestradiol and noregestrel or cyproterone acetate, spironolactone, finasteride, metformin), either alone as monotherapy in mild/moderate disease or in combination therapy for more severe cases (30). The efficacy of systemic and intralesional steroids in acute HS flares has been widely demonstrated, even if high dose and protracted oral administrations of steroids are not recommended, given the possible flares after dose tapering, whereas the exact dosages and volumes to be used in intralesional administration remains undefined (30). For uncontrolled acute HS lesions, the surgical management may be a good therapeutic alternative, however clinical outcomes depend on the location of lesions: vulvar., perianal, and inferior breast excisions present higher recurrence rates. Variable results have been highlighted with laser and photodynamic therapy (PDT), however no standardized treatment protocols have been established, the variability of response is closely related to the used light source (30). The new frontiers of treatments are now represented by targeted biotechnological therapy with anti-TNFα and anti-IL-17 agents (30). Up to day, the unique biologic drug approved by the FDA and EMA for the treatment of moderate to severe HS is Adalimumab, a fully human monoclonal antibody targeting TNFα (59). Nevertheless, according with the real-life experience, its long-term efficacy seems to be highly variable (60). Infliximab, a chimeric mouse / human monoclonal IgG1 antibody against TNF-α, actually represents the second line therapy in moderate to severe HS unresponsive to adalimumab (33). Although several studies and anectodical reports have proved its efficacy and safety, it is not under investigation in any ongoing clinical trials (61, 62). Results about the efficacy of Golimumab, a human anti-TNFα monoclonal antibody, remain not encouraging and suggest that higher dosing may be needed for HS treatment (33). With regard to the last approved TNFα inhibitor, the humanized antibody IgG4 Certolizumab pegol, the effectiveness in HS across the published studies is promising, but, due to the still insufficient data, its role in HS warrants further investigation (33). About Canakinumab, a human monoclonal antibody against IL-1 β, no large clinical trials investigated its safety and efficacy in HS, in fact the results are not univocal and come from single case reports or case series (63–65). It also worth mentioning that Anakinra, a recombinant IL-1 receptor antagonist, might be a safe and effective treatment option for patients with acne inversa (33). Currently, the most promising biologics in phase III trials are anti-IL-17 antibodies, namely Secukinumab, a human monoclonal immunoglobulin G1 kappa antibody that binds to IL-17A, and Bimekizumab, a humanized IgG1κ monoclonal antibody that neutralizes both IL-17A and IL-17F (60). Furthermore, Bermekimab, a recombinant human IgG1 monoclonal antibody that binds IL-1α, is presently in phase II trials and shows encouraging results (60). Several research also investigated the efficacy of Brodalumab, a fully monoclonal antibody that binds to the IL-17 receptor A, and of Ixekizumab, a humanized IgG4 monoclonal antibody that neutralizes soluble IL-17A and IL-17 A/F. However, the few data on the use of Ixekizumab in HS come from case reports (12, 33) and only one ongoing early phase I clinical trial is trying to assess the response to treatment at a molecular level, through the collection of blood and tissue samples (66). Randomized controlled trials about the use of Ustekinumab, a IL-12/23 inhibitor, for patients with HS are lacking (33). IL-23 inhibitors (e.g., Guselkumab and Risankizumab), showed varied results as similarly complement C5a inhibitors (e.g., Vilobelimab, Avacopan), CD20 inhibitors (e.g., Rituximab), CD40 inhibitors (e.g., Iscalimab), phosphodiesterase-4 (PDE-4) inhibitors (e.g., Apremilast), anti-Il-36 agents (e.g., Spesolimab, Imsidolimab), leukotriene A4 (LTA4) inhibitor (e.g., LYS006), janus kinase (JAK) inhibitors (e.g., INCB054707, Tofacitinib, Upadacitinib) and CXC receptors (e.g., LY3041658) (33). Switching to psoriasis, based on the prevalence including about 125 million people in the world, it seems intuitive to understand why its therapeutic management enjoys a wide range of alternatives. In mild psoriasis, topical agents (e.g., steroids, vitamin D analogs, calcineurin inhibitors and keratolytics) remain the pivot of treatment together with the narrowband UV-B phototherapy (35). When conventional drugs (e.g., methotrexate, acitretin, cyclosporine, apremilast) are contraindicated or show primary or secondary ineffectiveness, the first line treatment for moderate to severe psoriasis is represented by biologics. Inhibitors of TNFα include Adalimumab, Etanercept, Certolizumab and Infliximab. Other biotech drugs block the p40 subunit of IL-12 and IL-23 (Ustekinumab), IL-17 (Secukinumab, Ixekizumab, Brodalumab and Bimekizumab), and the p19 subunit of IL-23 (Guselkumab, Tildrakizumab, Risankizumab and Mirikizumab) (35). When psoriasis occurs in association with HS therapeutic strategy should be chosen in concordance to diseases severity bearing in mind that almost all the biologics approved for the treatment of psoriasis are still off label for HS due to the absence of randomized controlled trials. In real life several treatments have been used for concomitant psoriasis/PsA and HS. Yen and Gadelha, in their studies described the improvement of both pathologies after the injection of Adalimumab and similarly Pistone referring to the use of Secukinumab (22–24). However, some cases reported in literature highlight paradoxical phenomena in which Adalimumab induced paradoxical HS in patients treated for psoriasis and vice versa (11, 17, 67, 68). Likewise, also Odorici and Navarro-Triviño pointed out paradoxical HS induced by Secukinumab used to treat psoriasis and PsA. Due to these reactions the drug was stopped and Ixekizumab and Ustekinumab were introduced respectively, with improvement of both conditions (12, 18). In non-responders, other biological drugs not yet approved by EMA and FDA, have shown encouraging results. Tampouratzi evidenced the efficacy of Certolizumab pegol and Brodalumab in two different patients previously treated with several drugs without response (21). Also, Yoshida conducted a study investigating the effectiveness of Brodalumab and Licata observed the complete resolution of the psoriatic and suppurative lesions 4 months after therapy with Risankizumab (15, 16). Lastly, a valid alternative option is represented by Apremilast as illustrated by Garcovic, Lanna, Proietti, although the results appear not always univocal (14, 19, 20). Approved and on-going studied biologic treatments for HS and psoriasis are summarized in Figure 1.
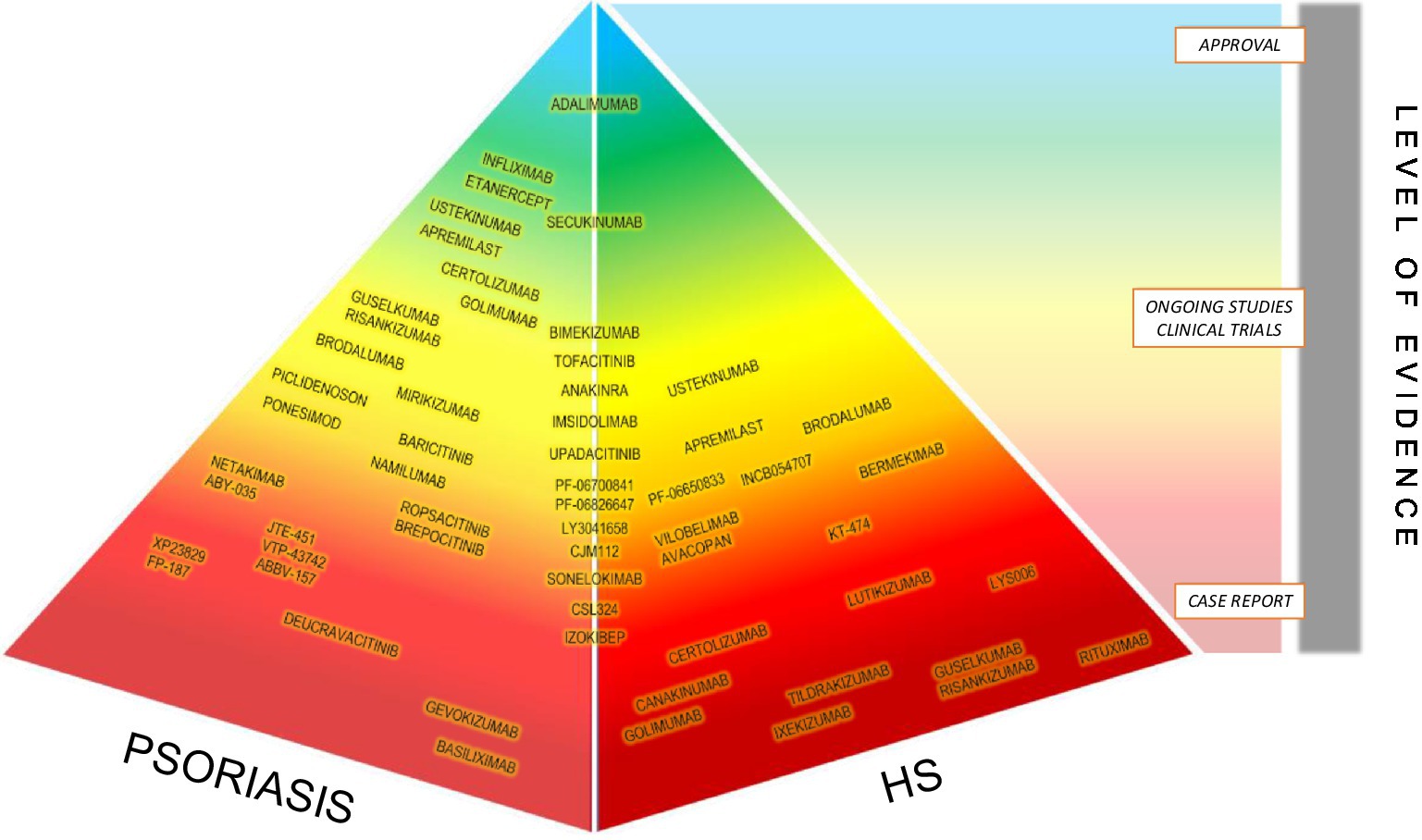
Figure 1. Approved and on-going studied biologic treatments for HS and psoriasis.
HS and psoriasis are chronic inflammatory skin diseases associated with a decrease in patients’ QoL, whose co-existence is increasingly being described in literature. It is assumed to depend on common pathogenic pathways in which IL-17 and IL-23 play a pivotal role. HS usually arises on a framework of already present psoriasis, and this can be explained by the different prevalence and incidences of the pathologies, being psoriasis much more frequent. However, the substantial difference that seem to emerge relates to the therapeutical approaches and their efficacy: while many biological drugs have been developed for psoriasis with excellent results in the reduction of the PASI and improving patients’ symptoms and QoL, the same goal was not reached for HS. Unlike psoriasis, the only registered biologic by the FDA and EMA in the treatment of moderate to severe HS is adalimumab, with sometimes unsatisfactory results. Nevertheless, the safety and efficacy of adalimumab have paved the way for comparing possible new drugs with adalimumab. Many other molecules with several immunological targets such as IL-12/23, IL-17, IL-23, IL-36, C5a, CD-20, CD-40, LTA4 and CXCR1/2 are currently under investigation for the treatment of moderate to severe HS. However, larger clinical trials of new therapeutic agents are mandatory in order to discover their effective therapeutic role, to evaluate the efficacy and safety and possible side effects.
LM and FL: conceptualization, investigation, writing–original draft preparation, and project administration. GT and CG: methodology and supervision. LM, FL, and CG: validation. LM, FL, and YI: formal analysis and resources. CG: data curation and visualization. PM, GT, and CG: writing–review and editing. YI, GT, and CG: funding acquisition. All authors have read and agreed to the published version of the manuscript.
CG has received consultation fees and/or grants for research projects, advisory panels and giving educational lectures from Wyeth-Pfizer, Abbott Immunology-Abbvie, Janssen-Cilag, Novartis, LEO-Pharma, LEO-Pharma Denmark, Ely-Lilly, Celgene, Merck-Serono, Sanofi-Aventis, Amgen and Almirall.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. ^https://ncbi.nlm.nih.gov/PubMed – accessed on 01 November 2022.
1. Li Pomi, F , Macca, L , Motolese, A , Ingrasciotta, Y , Berretta, M , and Guarneri, C . Neoplastic implications in patients suffering from hidradenitis Suppurativa under systemic treatments. Biomedicine. (2021) 9:1594. doi: 10.3390/biomedicines9111594
2. Jemec, GBE . Hidradenitis Suppurativa. N Engl J Med. (2012) 366:158–64. doi: 10.1056/NEJMcp1014163
3. Nguyen, TV , Damiani, G , Orenstein, LAV , Hamzavi, I , and Jemec, GB . Hidradenitis suppurativa: an update on epidemiology, phenotypes, diagnosis, pathogenesis, comorbidities and quality of life. J Eur Acad Dermatol Venereol. (2021) 35:50–61. doi: 10.1111/jdv.16677
4. Macca, L , Moscatt, V , Ceccarelli, M , Ingrasciotta, Y , Nunnari, G , and Guarneri, C . Hidradenitis Suppurativa in patients with HIV: a scoping review. Biomedicine. (2022) 10:2761. doi: 10.3390/biomedicines10112761
5. Mohammadi, S , Gholami, A , Hejrati, L , Rohani, M , Rafiei-Sefiddashti, R , and Hejrati, A . Hidradenitis suppurativa; classification, remedies, etiology, and comorbidities; a narrative review. J Family Med Prim Care. (2021) 10:4009–16. doi: 10.4103/jfmpc.jfmpc_795_21
6. Peris, K , Fortina, AB , Bianchi, L , Fabbrocini, G , Gisondi, P , Balato, A, et al. Update on the Management of Pediatric Psoriasis: an Italian consensus. Dermatol Ther (Heidelb). (2022) 12:1753–75. doi: 10.1007/s13555-022-00758-2
7. World Health Organization . World Health Organization Global Report on Psoriasis. Geneva: World Health Organization (2022).
8. Parisi, R , Symmons, DPM , Griffiths, CEM , and Ashcroft, DM . Global epidemiology of psoriasis: a systematic review of incidence and prevalence. J Investig Dermatol. (2013) 133:377–85. doi: 10.1038/jid.2012.339
9. Motolese, A , Ceccarelli, M , Macca, L , Li Pomi, F , Ingrasciotta, Y , Nunnari, G, et al. Novel therapeutic approaches to psoriasis and risk of infectious disease. Biomedicine. (2022) 10:228. doi: 10.3390/biomedicines10020228
10. Borgia, F , Ciodaro, F , Guarneri, F , Bartolotta, A , Papaianni, V , Guarneri, C, et al. Auditory system involvement in psoriasis. Acta Dermatol Venereol. (2018) 98:655–9. doi: 10.2340/00015555-2937
11. Musumeci, ML , Nasca, MR , Pavone, A , and Micali, G . Anti-TNFα-induced psoriasis under treatment of hidradenitis suppurativa: report of 2 cases. G Ital Dermatol Venereol. (2020) 155:377–9. doi: 10.23736/S0392-0488.18.06054-6
12. Odorici, G , Pellacani, G , and Conti, A . Ixekizumab in hidradenitis suppurativa in a psoriatic patient. G Ital Dermatol Venereol. (2021) 155:788–9. doi: 10.23736/S0392-0488.18.06135-7
13. Gkini, MA , and Bewley, AP . Development of hidradenitis suppurativa in a patient treated with ustekinumab for her psoriasis: a potential paradoxical reaction? Dermatol Ther. (2018) 31:e12742. doi: 10.1111/dth.12742
14. Garcovich, S , Giovanardi, G , Malvaso, D , de Simone, C , and Peris, K . Apremilast for the treatment of hidradenitis suppurativa associated with psoriatic arthritis in multimorbid patients. Medicine. (2020) 99:e18991. doi: 10.1097/MD.0000000000018991
15. Licata, G , Gambardella, A , Buononato, D , de Rosa, A , Calabrese, G , Pellerone, S, et al. A case of moderate hidradenitis suppurativa and psoriasis successfully treated with risankizumab. Int J Dermatol. (2022) 61:e126–9. doi: 10.1111/ijd.15704
16. Yoshida, Y , Oyama, N , Iino, S , Shimizu, C , and Hasegawa, M . Long-standing refractory hidradenitis suppurativa responded to a brodalumab monotherapy in a patient with psoriasis: a possible involvement of Th17 across the spectrum of both diseases. J Dermatol. (2021) 48:916–20. doi: 10.1111/1346-8138.15807
17. Vellaichamy, G , Townsend, SM , Lyons, AB , and Hamzavi, IH . T-cell/histiocyte-rich large B-cell lymphoma in a 27-year-old with hidradenitis suppurativa, psoriasis, and vitiligo: implications for screening. JAAD Case Rep. (2020) 6:1252–3. doi: 10.1016/j.jdcr.2020.08.032
18. Navarro-Triviño, FJ , Sanchez-Parera, R , and Ruiz-Villaverde, R . Secukinumab-induced paradoxical hidradenitis suppurativa. Dermatol Ther. (2020) 33:1. doi: 10.1111/dth.13150
19. Lanna, C , Mazzilli, S , Zangrilli, A , Bianchi, L , and Campione, E . One drug and two diseases: a case of multidrug-resistant hidradenitis suppurativa and psoriasis treated with apremilast. Dermatol Ther. (2019) 32:e13089. doi: 10.1111/dth.13089
20. Proietti, I , Michelini, S , Mambrin, A , di Fraia, M , Tolino, E , Balduzzi, V, et al. A case of hidradenitis suppurativa successfully treated with apremilast in a patient with psoriasis andSAMPUS. Dermatol Ther. (2020) 33:e13448. doi: 10.1111/dth.13448
21. Tampouratzi, E , Kanni, T , Katsantonis, J , and Douvali, T . Case report: treating a co-existence of hidradenitis suppurativa and psoriasis with different therapeutic approaches. F1000Res. (2020) 8, 8:2002. doi: 10.12688/f1000research.21216.2
22. De Lima Gadelha, R , Da Silveira Rodrigues Paiva, R , Palitot, EB , and Da Costa, JE . PsAPASH: a rare and recent autoinflammatory syndrome associated with hidradenitis suppurativa. An Bras Dermatol. (2020) 95:203–6. doi: 10.1016/j.abd.2019.02.012
23. Giuseppe, P , Nicola, P , Valentina, C , Elena, C , Salvatrice, C , Rosario, G, et al. A case of moderate hidradenitis Suppurativa and psoriasis treated with Secukinumab. Ann Dermatol. (2018) 30:462–4. doi: 10.5021/ad.2018.30.4.462
24. Yen, CF , Huang, YH , and Chi, CC . Concomitant psoriasis and hidradenitis suppurativa responsive to adalimumab therapy: a case series. Indian J Dermatol Venereol Leprol. (2021) 87:223–6. doi: 10.4103/ijdvl.IJDVL_455_18
25. Kridin, K , Shani, M , Schonmann, Y , Fisher, S , Shalom, G , Comaneshter, D, et al. Psoriasis and hidradenitis Suppurativa: a large-scale population-based study. J Am Acad Dermatol. (2018) 88:e231–6. doi: 10.1016/j.jaad.2018.11.036
26. Lee, JH , Kwon, HS , Jung, HM , Kim, GM , and Bae, JM . Prevalence and comorbidities associated with hidradenitis suppurativa in Korea: a nationwide population-based study. J Eur Acad Dermatol Venereol. (2018) 32:1784–90. doi: 10.1111/jdv.15071
27. Richette, P , Molto, A , Viguier, M , Dawidowicz, K , Hayem, G , Nassif, A, et al. Hidradenitis Suppurativa associated with Spondyloarthritis–results from a multicenter National Prospective Study. J Rheumatol. (2014) 41:490–4. doi: 10.3899/jrheum.130977
28. Patel, M , Cohen, JM , Wright, NA , Merola, JF , Qureshi, AA , and Vleugels, RA . Epidemiology of concomitant psoriasis and hidradenitis suppurativa (HS): experience of a tertiary medical center. J Am Acad Dermatol. (2015) 73:701–2. doi: 10.1016/j.jaad.2015.06.050
29. Napolitano, M , Megna, M , Timoshchuk, E , Patruno, C , Balato, N , Fabbrocini, G, et al. Hidradenitis suppurativa: from pathogenesis to diagnosis and treatment. Clin Cosmet Investig Dermatol. (2017) 10:105–15. doi: 10.2147/CCID.S111019
30. Amat-Samaranch, V , Agut-Busquet, E , Vilarrasa, E , and Puig, L . New perspectives on the treatment of hidradenitis suppurativa. Ther Adv Chronic Dis. (2021) 12:204062232110559. doi: 10.1177/20406223211055920
31. Moltrasio, C , Tricarico, PM , Romagnuolo, M , Marzano, AV , and Crovella, S . Hidradenitis Suppurativa: a perspective on genetic factors involved in the disease. Biomedicine. (2022) 10:2039. doi: 10.3390/biomedicines10082039
32. Goldburg, SR , Strober, BE , and Payette, MJ . Hidradenitis suppurativa. J Am Acad Dermatol. (2020) 82:1045–58. doi: 10.1016/j.jaad.2019.08.090
33. Świerczewska, Z , Lewandowski, M , Surowiecka, A , and Barańska-Rybak, W . Immunomodulatory drugs in the treatment of hidradenitis Suppurativa—possibilities and limitations. Int J Mol Sci. (2022) 23:9716. doi: 10.3390/ijms23179716
34. Roszkiewicz, M , Dopytalska, K , Szymańska, E , Jakimiuk, A , and Walecka, I . Environmental risk factors and epigenetic alternations in psoriasis. Ann Agric Environ Med. (2020) 27:335–42. doi: 10.26444/aaem/112107
35. Armstrong, AW , and Read, C . Pathophysiology, clinical presentation, and treatment of psoriasis. JAMA. (2020) 323:1945. doi: 10.1001/jama.2020.4006
36. Moltrasio, C , Romagnuolo, M , and Marzano, AV . Epigenetic mechanisms of epidermal differentiation. Int J Mol Sci. (2022) 23:4874. doi: 10.3390/ijms23094874
37. Gulliver, W , Zouboulis, CC , Prens, E , Jemec, GBE , and Tzellos, T . Evidence-based approach to the treatment of hidradenitis suppurativa/acne inversa, based on the European guidelines for hidradenitis suppurativa. Rev Endocr Metab Disord. (2016) 17:343–51. doi: 10.1007/s11154-016-9328-5
38. Sabat, R , Jemec, GBE , Matusiak, Ł , Kimball, AB , Prens, E , and Wolk, K . Hidradenitis suppurativa. Nat Rev Dis Primers. (2020) 6:18. doi: 10.1038/s41572-020-0149-1
39. Garcovich, S , Genovese, G , Moltrasio, C , Malvaso, D , and Marzano, AV . PASH, PAPASH, PsAPASH, and PASS: the autoinflammatory syndromes of hidradenitis suppurativa. Clin Dermatol. (2021) 39:240–7. doi: 10.1016/j.clindermatol.2020.10.016
40. González-Manso, A , Agut-Busquet, E , Romaní, J , Vilarrasa, E , Bittencourt, F , Mensa, A, et al. Hidradenitis Suppurativa: proposal of classification in two Endotypes with two-step cluster analysis. Dermatology. (2021) 237:365–71. doi: 10.1159/000511045
41. Oranges, T , Vitali, S , Benincasa, B , Izzetti, R , Lencioni, R , Caramella, D, et al. Advanced evaluation of hidradenitis suppurativa with ultra-high frequency ultrasound: a promising tool for the diagnosis and monitoring of disease progression. Skin Res Technol. (2020) 26:513–9. doi: 10.1111/srt.12823
42. Nazzaro, G , Passoni, E , Muratori, S , Moltrasio, C , Guanziroli, E , Barbareschi, M, et al. Comparison of clinical and sonographic scores in hidradenitis suppurativa and proposal of a novel ultrasound scoring system. Italian journal of. Dermatol Venereol. (2021) 156:235–9. doi: 10.23736/S2784-8671.18.06196-5
43. Ingram, JR , Collier, F , Brown, D , Burton, T , Burton, J , Chin, MF, et al. British Association of Dermatologists guidelines for the management of hidradenitis suppurativa (acne inversa) 2018. Br J Dermatol. (2019) 180:1009–17. doi: 10.1111/bjd.17537
44. Horváth, B , Janse, I , Blok, J , Driessen, R , Boer, J , Mekkes, J, et al. Hurley staging refined: a proposal by the Dutch hidradenitis Suppurativa expert group. Acta Dermatol Venereol. (2017) 97:412–3. doi: 10.2340/00015555-2513
45. Zouboulis, CC , Tzellos, T , Kyrgidis, A , Jemec, GBE , Bechara, FG , Giamarellos-Bourboulis, EJ, et al. Development and validation of the international hidradenitis Suppurativa severity score system (IHS4), a novel dynamic scoring system to assess HS. Br J Dermatol. (2017) 177:1401–9. doi: 10.1111/bjd.15748
46. Menter, A , Gottlieb, A , Feldman, SR , van Voorhees, AS , Leonardi, CL , Gordon, KB, et al. Guidelines of care for the management of psoriasis and psoriatic arthritis. J Am Acad Dermatol. (2008) 58:826–50. doi: 10.1016/j.jaad.2008.02.039
47. Clebak, KT , Helm, L , Helm, MF , and Seiverling, EV . The many variants of psoriasis. J Fam Pract. (2020) 69:192–200.
48. Kimmel, GW , and Lebwohl, M . Evidence-based psoriasis: overview and diagnosis. Cham: Springer, 1–16. (2018).
49. Wu, JJ . Contemporary management of moderate to severe plaque psoriasis. Am J Manag Care. (2017) 23:S403–16.
50. Kim, WB , Jerome, D , and Yeung, J . Diagnosis and management of psoriasis. Can Fam Physician. (2017) 63:278–85.
51. Mrowietz, U , Kragballe, K , Reich, K , Spuls, P , Griffiths, CEM , Nast, A, et al. Definition of treatment goals for moderate to severe psoriasis: a European consensus. Arch Dermatol Res. (2011) 303:1–10. doi: 10.1007/s00403-010-1080-1
52. Garcovich, S , de Simone, C , Genovese, G , Berti, E , Cugno, M , and Marzano, AV . Paradoxical skin reactions to biologics in patients with rheumatologic disorders. Front Pharmacol. (2019) 10:10. doi: 10.3389/fphar.2019.00282
53. Delobeau, M , Abdou, A , Puzenat, E , Deveza, E , Biver-Dalle, C , van de Laak, A, et al. Observational case series on adalimumab-induced paradoxical hidradenitis suppurativa. J Dermatol Treat. (2016) 27:251–3. doi: 10.3109/09546634.2015.1094179
54. Faivre, C , Villani, AP , Aubin, F , Lipsker, D , Bottaro, M , Cohen, JD, et al. Hidradenitis suppurativa (HS): an unrecognized paradoxical effect of biologic agents (BA) used in chronic inflammatory diseases. J Am Acad Dermatol. (2016) 74:1153–9. doi: 10.1016/j.jaad.2016.01.018
55. Marasca, C , Megna, M , Balato, A , Balato, N , Napolitano, M , and Fabbrocini, G . Secukinumab and hidradenitis suppurativa: friends or foes? JAAD Case Rep. (2019) 5:184–7. doi: 10.1016/j.jdcr.2018.12.002
56. Nazzaro, G , and Muratori, S . Hidradenitis suppurativa associated with systemic lupus erythematosus and psoriasis: a therapeutical challenge. Ital J Dermatol Venereol. (2022) 156:13–4. doi: 10.23736/S2784-8671.19.06209-6
57. Chu, S , Michelle, L , Ekelem, C , Sung, CT , Rojek, N , and Mesinkovska, NA . Oral isotretinoin for the treatment of dermatologic conditions other than acne: a systematic review and discussion of future directions. Arch Dermatol Res. (2021) 313:391–430. doi: 10.1007/s00403-020-02152-4
58. Alikhan, A , Sayed, C , Alavi, A , Alhusayen, R , Brassard, A , Burkhart, C, et al. North American clinical management guidelines for hidradenitis suppurativa: a publication from the United States and Canadian hidradenitis Suppurativa foundations. J Am Acad Dermatol. (2019) 81:91–101. doi: 10.1016/j.jaad.2019.02.068
59. Włodarek, K , Ponikowska, M , Matusiak, Ł , and Szepietowski, JC . Biologics for hidradenitis suppurativa: an update. Immunotherapy. (2019) 11:45–59. doi: 10.2217/imt-2018-0090
60. Markota Čagalj, A , Marinović, B , and Bukvić, MZ . New and emerging targeted therapies for hidradenitis Suppurativa. Int J Mol Sci. (2022) 23:3753. doi: 10.3390/ijms23073753
61. Lesage, C , Adnot-Desanlis, L , Perceau, G , Bonnet, M , Palot, JP , Bernard, P, et al. Efficacy and tolerance of prolonged infliximab treatment of moderate-to-severe forms of hidradenitis suppurativa. Eur J Dermatol. (2012) 22:640–4. doi: 10.1684/ejd.2012.1795
62. Ghias, MH , Johnston, AD , Kutner, AJ , Micheletti, RG , Hosgood, HD , and Cohen, SR . High-dose, high-frequency infliximab: a novel treatment paradigm for hidradenitis suppurativa. J Am Acad Dermatol. (2020) 82:1094–101. doi: 10.1016/j.jaad.2019.09.071
63. Sun, NZ , Ro, T , Jolly, P , and Sayed, CJ . Non-response to Interleukin-1 antagonist Canakinumab in two patients with refractory pyoderma Gangrenosum and hidradenitis Suppurativa. J Clin Aesthet Dermatol. (2017) 10:36–8.
64. Houriet, C , Seyed Jafari, SM , Thomi, R , Schlapbach, C , Borradori, L , Yawalkar, N, et al. Canakinumab for severe hidradenitis Suppurativa. JAMA Dermatol. (2017) 153:1195–7. doi: 10.1001/jamadermatol.2017.2392
65. Jaeger, T , Andres, C , Grosber, M , Zirbs, M , Hein, R , Ring, J, et al. Pyoderma gangrenosum and concomitant hidradenitis suppurativa – rapid response to canakinumab (anti-IL-1β). Eur J Dermatol. (2013) 23:408–10. doi: 10.1684/ejd.2013.2018
66. Renert-Yuval, Y . Molecular characteristics of Brodalumab in hidradenitis Suppurativa. United States: US National Library of Medicine (2022).
67. Burzi, L , Repetto, F , Ribero, S , Mastorino, L , Quaglino, P , and Dapavo, P . Paradoxical psoriasiform reactions during treatment with adalimumab for hidradenitis suppurativa: real-life experience and therapeutic response to other biological drugs. Dermatol Ther. (2022) 35:e15866. doi: 10.1111/dth.15866
68. Kanelleas, A , Efthymiou, O , Routsi, E , Sgouros, D , Pappa, G , Tsoureli Nikita, E, et al. Clinical and epidemiological characteristics of hidradenitis Suppurativa patients with paradoxical Psoriasiform reactions following treatment with adalimumab. Skin Appendage Disord. (2022) 8:415–8. doi: 10.1159/000524174
Keywords: psoriasis, hidradenitis suppurativa, biologics, Th1, Th17, Th22, TNF-α, IL-12/23/17
Citation: Macca L, Li Pomi F, Ingrasciotta Y, Morrone P, Trifirò G and Guarneri C (2023) Hidradenitis suppurativa and psoriasis: the odd couple. Front. Med. 10:1208817. doi: 10.3389/fmed.2023.1208817
Edited by:
Luca Mastorino, University of Turin, ItalyReviewed by:
Chiara Moltrasio, IRCCS Ca’Granda Foundation Maggiore Policlinico Hospital, ItalyCopyright © 2023 Macca, Li Pomi, Ingrasciotta, Morrone, Trifirò and Guarneri. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Claudio Guarneri, Y2d1YXJuZXJpQHVuaW1lLml0
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.