 Lin Zhang†
Lin Zhang† Rui Huang
Rui Huang
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Med. , 30 June 2023
Sec. Gastroenterology
Volume 10 - 2023 | https://doi.org/10.3389/fmed.2023.1185182
This article is part of the Research Topic Treatment and Prognostic Assessment of Liver Cirrhosis and Its Complications View all 11 articles
Introduction: Hepatic encephalopathy (HE) is a significant complication of cirrhosis, known to be associated with hospital readmission. However, few new serological indicators associated with readmission in HE patients have been identified and reported. The objective of our study was to identify simple and effective predictors reated to readmission in HE patients.
Materials and methods: We conducted a retrospective study at a single center on adult patients admitted with HE from January 2018 to December 2022. The primary endpoint was the first liver-related readmission within 30, 90, and 180 days, and we collected electronic medical records from our hospital for sociodemographic, clinical, and hospitalization characteristics. We utilized logistic regression analysis and multiple linear regression analysis to determine the predictors that were associated with the readmission rate and the length of the first hospitalization.
Results: A total of 424 patients were included in the study, among whom 24 (5.7%), 63 (14.8%), and 92 (21.7%) were readmitted within 30, 90, and 180 days, respectively. Logistic regression analysis showed that insurance status, alcoholic liver disease (ALD), ascites, the model for end-stage liver disease (MELD) score, and neutrophil-to-lymphocyte ratio (NLR) were significantly associated with 30-, 90-, and 180-day readmissions. Age and hepatocellular carcinoma (HCC) were predictors of 90- and 180-day readmissions. ALD was identified as a unique predictor of readmission in men, while hypertension was a predictor of 180-day readmission in women. Variceal bleeding, chronic kidney disease, and MELD score were associated with the length of the first hospitalization.
Conclusions: NLR at discharge was identified as a significant predictor of 30-, 90- and 180-day readmissions in patients with HE. Our findings suggest that incorporating NLR into routine clinical assessments could improve the evaluation of the prognosis of liver cirrhosis.
Hepatic encephalopathy (HE) is a significant complication of advanced liver disease that is associated with poor outcomes. The incidence of HE in patients with cirrhosis can reach 11.6/100 person-years (1). Once HE develops, the 1- and 3-year cumulative survival rates are only 50 and 25% (2). HE is characterized by changes in personality, consciousness, cognition, and motor function and is associated with a range of clinical complications (3). Additionally, HE has a negative impact on the health-related quality of life of affected patients (4).
According to reports, the readmission rates of patients with cirrhosis were 20.7 and 30.1% within 30 and 90 days, respectively, with HE being the most common reason for readmission (5). Furthermore, HE was also the leading cause of readmission for patients with decompensated cirrhosis within 180 days (45.4%), with a mortality rate of 35.0% within 180 days (p = 0.001) (6). Readmission not only predicts poor outcomes for cirrhotic and HE patients, but it also represents a significant financial burden. A national study conducted in America found that the total healthcare cost for cirrhotic patients with readmission was significantly higher than for those without readmission within 30 days ($64,795 vs. $31,017, p < 0.001) (7).
Several factors have been reported as predictors of readmission in HE patients, including insurance status, alcoholic liver disease (ALD), the presence of portal hypertension, international normalized ratio (INR), the model for end-stage liver disease (MELD) score, ascites, receiving paracentesis, and acute kidney injury (1, 7–9). Previous studies reported that volume status, including ascites, receiving paracentesis, and acute kidney injury, were associated with early readmission, as HE patients with refractory ascites and/or recurrent acute kidney injury often require repeated paracentesis (7, 10). Uninsured patients were found to have higher alcohol-related admissions and lower inpatient and 90-day transplant rates, even after controlling for age, gender, race, ethnicity, comorbid conditions, and cirrhosis status (8). INR was found to independently predict early readmission in patients with HE, and MELD score was the only predictor when HE was considered the only cause of readmission (9). Furthermore, portal hypertension was associated with HE, as patients with severe liver disease manifested by portal hypertension had an incidence rate of 27.11 (95% CI, 26.84, 27.38) hospitalizations compared to 4.25 (95% CI, 4.18, 4.31) hospitalizations per person-years for those without, giving an incidence rate ratio (IRR) of 6.38 (95% CI, 6.27, 6.51) (1).
Although the neutrophil-to-lymphocyte ratio (NLR) has been reported to be associated with diseases, such as cardiac and chronic obstructive pulmonary disease (11, 12), as well as hepatopathy-related diseases, such as alcoholic hepatitis, hepatocellular carcinoma (HCC), and others (13–16), its correlation with readmission in HE patients has not been clearly researched. To clarify whether NLR is one of the predictors of readmission in HE patients, we conducted this retrospective study.
We conducted a retrospective study at a single center, including adult patients admitted with HE between January 2018 and December 2022. The patients were identified through the electronic medical record of our hospital using admission diagnoses of HE with ICD-9 codes 570.X, 572.2, 348.3, 348.31, 348.39, and 291.2. Patients with incomplete information and those who were lost to follow-up were excluded. The study was conducted in accordance with the ethical guidelines of the 1975 Declaration of Helsinki (6th revision, 2008) and was approved by the Ethics Committee of Peking University People's Hospital (No. 2022PHB251-01). Informed consent was obtained from all patients included in the study.
We collected sociodemographic, clinical, and hospitalization characteristics, including gender, age, insurance (including Chinese medical insurance for residents and Chinese worker medical insurance), baseline liver disease [alcohol or non-alcohol (viral hepatitis, non-alcoholic steatohepatitis, drug-induced liver injury, and autoimmune liver disease)], comorbidities [hypertension, diabetes, and chronic kidney disease (CKD)], and complications [HCC, ascites, variceal bleeding, and spontaneous bacterial peritonitis (SBP)]. Laboratory results at the first discharge, including ammonia, MELD score, and ALD diagnosed as alcohol intake ≥40 g per day in men and ≥20 g per day in women, lasting ≥5 years, were also collected (17). Baseline liver disease (hepatitis B and C, autoimmune liver disease, and drug-induced liver injury), with the exception of alcoholic liver disease, were extracted from admission and discharge diagnoses, and only one occurrence of each diagnosis was recorded. Laboratory data were obtained from the hospital's clinical data center. The MELD score was calculated using total bilirubin, creatinine, INR, and a history of cholestatic liver disease. The NLR was calculated as the ratio of absolute neutrophil count to absolute lymphocyte count.
We collected information on readmissions through the electronic medical record of our hospital, which includes medical history, physical examinations, daily notes, laboratory results, and discharge summaries. To capture episodes of hospitalization at other hospitals, we contacted patients who had liver-related readmissions to any hospital since the first hospitalization. Hospitalization characteristics recorded included complications of cirrhosis at the first admission (volume-related complications such as ascites, edema, or SBP; other complications or more than one complication such as HCC, variceal bleeding, and hepatic hydrothorax), cause of readmission (HE, volume-related, other, or more than one complication), and the length of stay for the first hospitalization (calculated from admission to discharge).
We defined the primary endpoint as the first liver-related readmission occurring within 30, 90, and 180 days following the initial hospitalization. Liver-related readmission was defined as readmission due to any of the following: HE, volume-related complications (ascites, edema, and SBP), HCC, variceal bleeding, and hepatic hydrothorax. HE was diagnosed according to the West Haven criteria and patients' clinical manifestations and ammonia levels. Ascites were diagnosed by imaging examination or clinical percussion revealing fluid in the peritoneal cavity. HCC was diagnosed based on pathology or imaging examination. Variceal bleeding was diagnosed based on clinical features and endoscopy. SBP was diagnosed when the ascitic fluid neutrophil count exceeded 250/mm3. Edema was diagnosed based on patient complaints and pitting edema of both lower limbs. Hepatic hydrothorax was diagnosed based on an imaging examination. Patients could have more than one liver-related reason for admission, and all other readmissions were excluded from the analysis.
Continuous variables were presented as mean ± standard deviations (SD) and categorical variables as count with percentage. Differences between groups were analyzed using Student's t-test for age, length of stay, MELD, NLR, and ammonia at discharge, and chi-square test for insurance, baseline liver disease, comorbidities, complications, treatment, and cause of readmission. Predictors associated with readmission and the length of the first hospitalization were analyzed using logistic regression analysis and multiple linear regression analysis, respectively. Statistical significance was considered at p < 0.05. Data analyses were performed using SPSS version 23.0 (IBM Corp, Armonk, NY, USA).
We included 424 patients admitted with HE, and their baseline characteristics are presented in Table 1. Within 30, 90, and 180 days, 24 (5.7%), 63 (14.8%), and 92 (21.7%) patients were readmitted, respectively. Among the patients, 283 (66.7%) were male patients, and the mean age was 59.9 ± 11.5 years; 120 (28.3%) patients had alcoholic cirrhosis. There were 280 patients classified as grade 0, 66 were of grade 1, 42 were of grade 2, 33 were of grade 3, and 1 was of grade 4. At baseline, 40 (9.4%), 246 (58.0%), 67 (15.8%), and 20 (4.7%) patients had HCC, ascites, variceal bleeding, and SBP, respectively. Patients who were readmitted within 180 days were older (62.0 ± 9.6 vs. 59.3 ± 12.0, p = 0.025) and had a higher proportion of no insurance [25 (27.2%) vs. 52 (15.7%), p = 0.010], ALD [34 (37.0%) vs. 86 (25.9%), p = 0.027], CKD [21 (22.8%) vs. 39 (11.7%), p = 0.007], HCC [15 (16.3%) vs. 25 (7.5%), p = 0.012], and ascites [65 (70.7%) vs. 181 (54.5%), p = 0.004] than those who were not readmitted within 180 days.
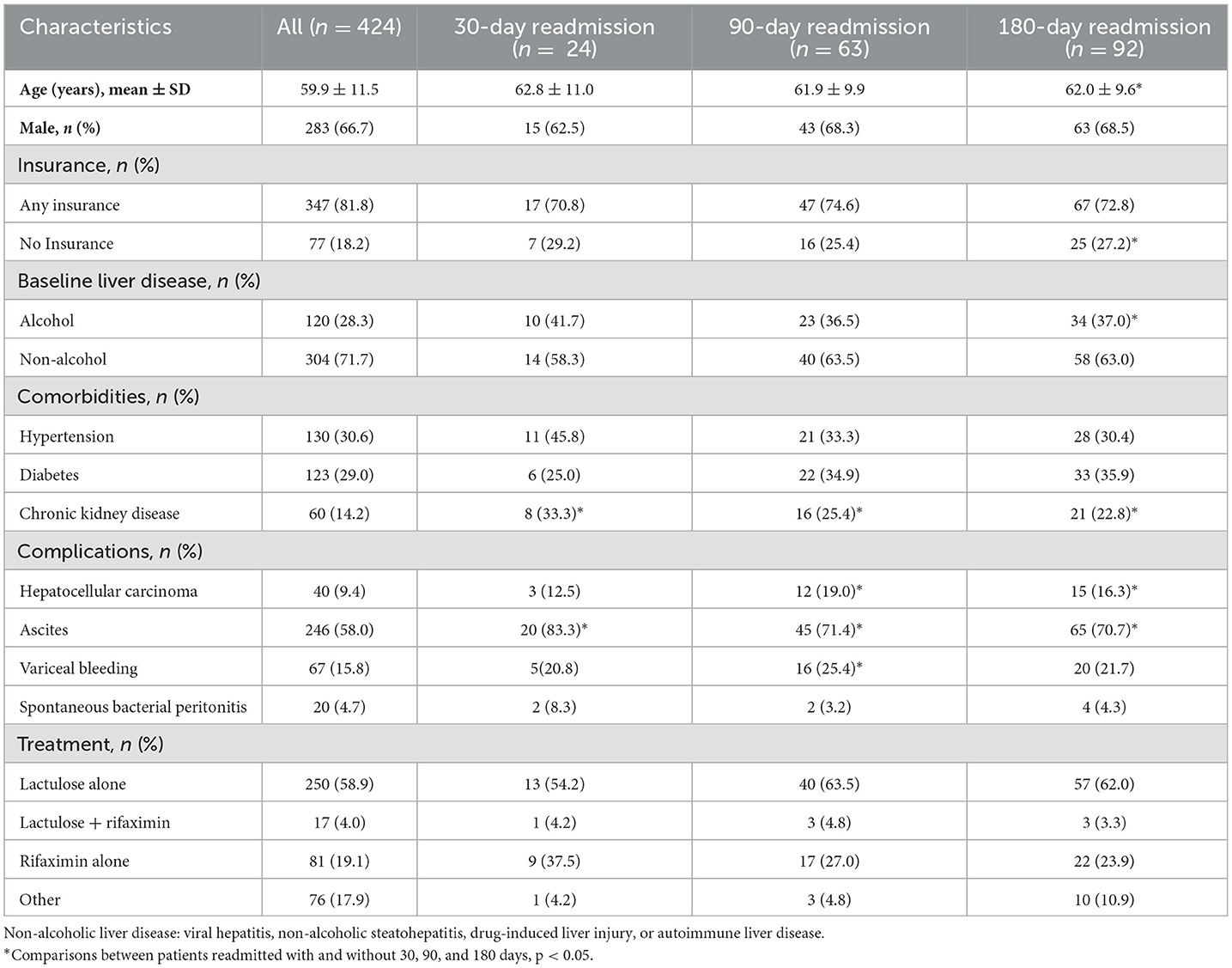
Table 1. Baseline characteristics of included patients.
Patients were admitted for liver-related reasons other than HE, including volume-related (247, 58.3) and other complications (177, 41.7%). The mean length of hospitalization for all patients at the time of admission was 17.9 ± 12.1 days. HE was the most common reason for readmission, with 15 (62.5%), 30 (47.6%), and 48 (52.1%) patients being readmitted for HE within 30, 90, and 180 days, respectively. Furthermore, patients who were readmitted had a higher NLR level at their first discharge (8.17 ± 12.1 vs. 3.95 ± 4.96; 7.17 ± 9.72 vs. 3.67 ± 4.44; 6.80 ± 8.62 vs. 3.47 ± 4.28, p < 0.001) compared to those without readmission in 30, 90, or 180 days (see Table 2). Patients who were readmitted within 30 days had the longest length of stay during their first hospitalization, which was significantly higher than those without readmission in 30 days (24.8 ± 19.2 vs. 17.7 ± 11.90, p < 0.001).

Table 2. Hospitalization characteristics.
Table 3 displays the results of logistic regression analysis for predictors of readmission within 30, 90, and 180 days. Significant predictors of readmission included no insurance, ALD, ascites, MELD score, and NLR at first discharge for all three time periods. Age and HCC were also significant predictors of readmission at 90 and 180 days.
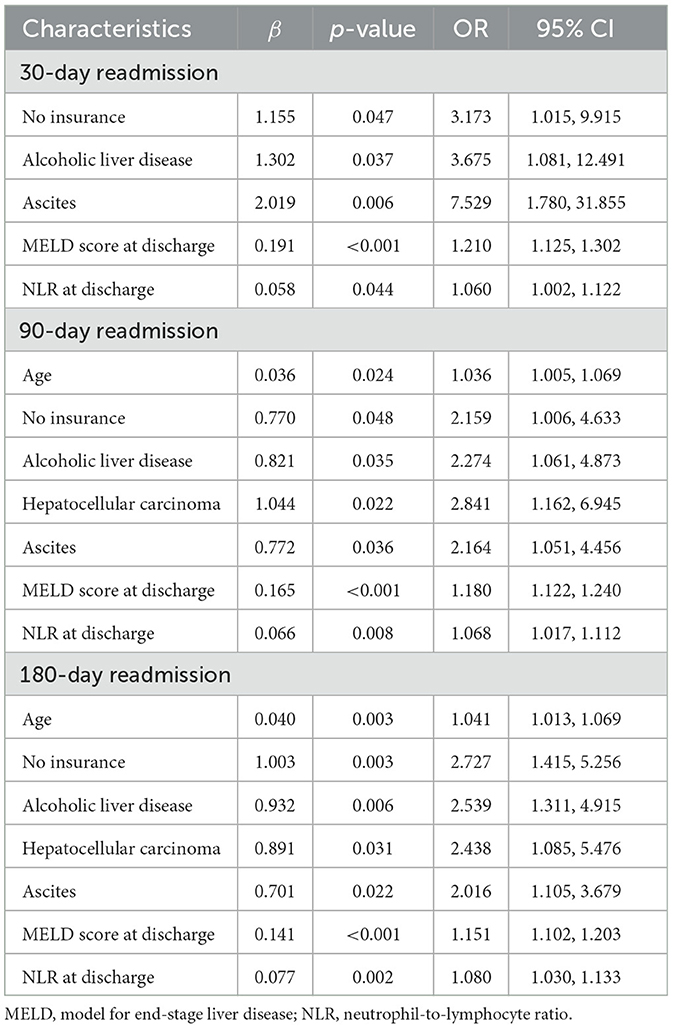
Table 3. Predictors of 30-, 90-, and 180-day readmissions.
However, gender differences were observed in the predictors of readmission. In men (Table 4), in addition to HCC, ascites, MELD score, and NLR at discharge, ALD was a significant predictor of 30-, 90-, and 180-day readmissions. Interestingly, ALD was not a significant predictor of readmission in women, while hypertension was significantly associated with 180-day readmission in women (Table 5).
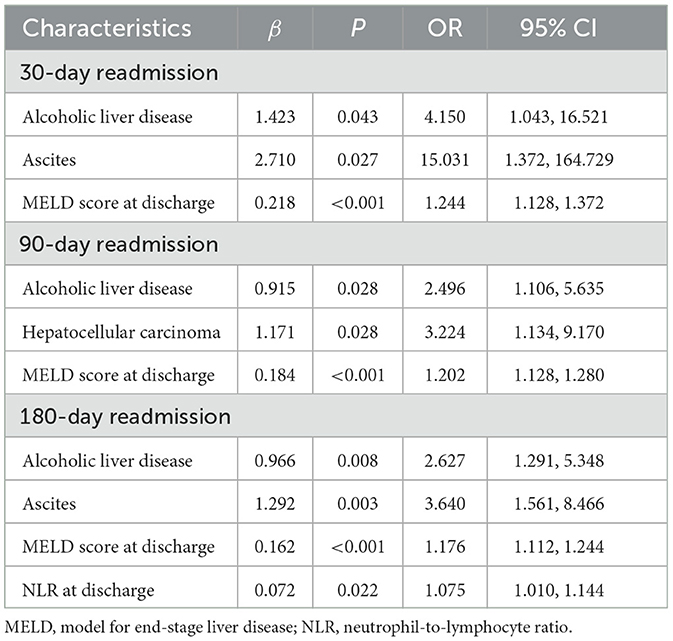
Table 4. Predictors of 30-, 90-, and 180-day readmissions in men.
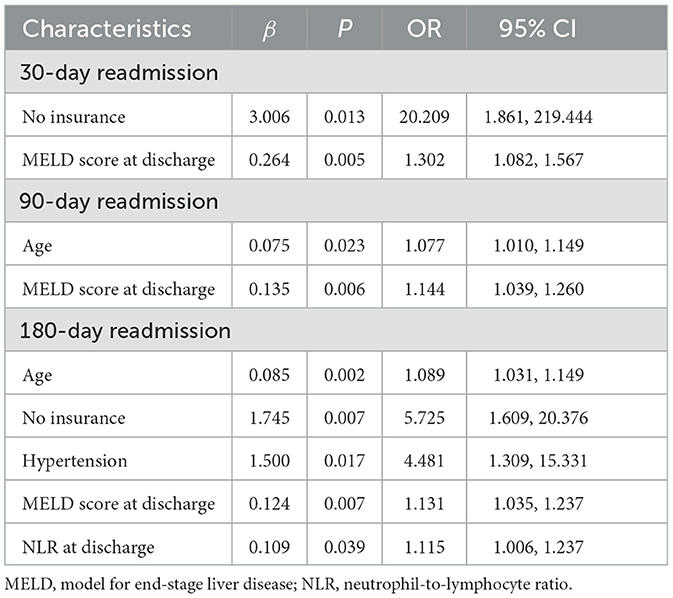
Table 5. Predictors of 30-, 90-, and 180-day readmissions in women.
Table 6 shows that variceal bleeding (p = 0.006), CKD (p = 0.003), and MELD score at discharge (p = 0.024) were significant predictors of the length of hospitalization for patients at their first admission.
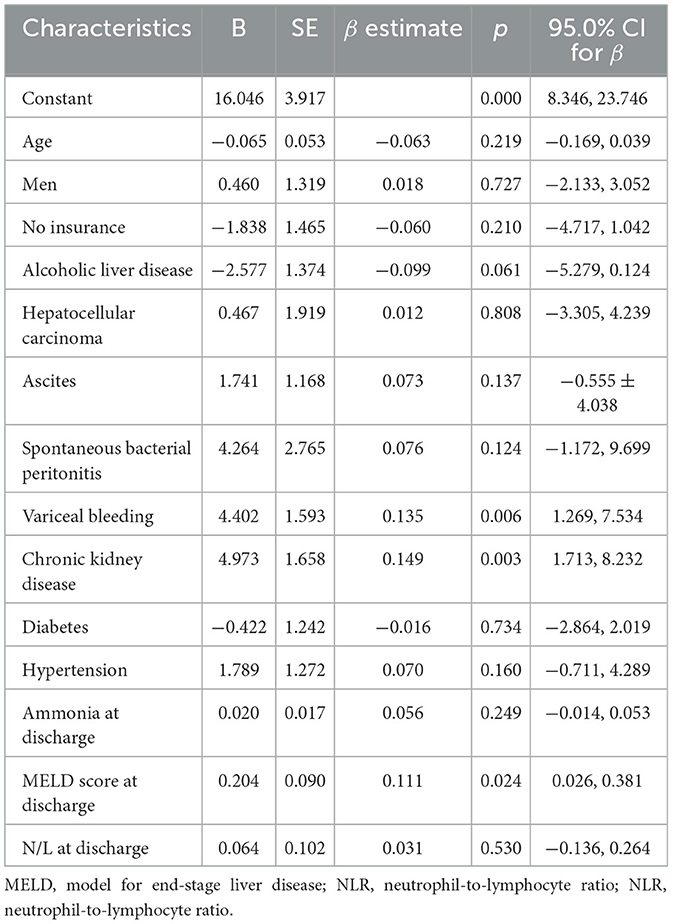
Table 6. Predictors of the length of hospitalization at the first admission.
Patients who are readmitted for HE are at an increased risk of morbidity and mortality, making readmissions costly for both patients and healthcare systems. Our study found that NLR at discharge was a significant predictor of 30-, 90-, and 180-day readmissions for patients with HE. This new predictor offers valuable insights that can inform clinical decision-making and improve the evaluation of the prognosis of liver cirrhosis. Additionally, our study showed that CKD, one of the most important comorbidities, was a significant factor affecting the length of hospitalization at the first admission for patients with HE. Therefore, managing comorbidities in addition to treating HE can help reduce the length of hospital stay for these patients.
We found that NLR at the first discharge was a crucial predictor of 30-, 90-, and 180-day readmissions. As neutrophils play an important role in many types of liver disease and inappropriate activation and homing of neutrophils to the microvasculature can induce immune-mediated liver injury, NLR is a serological marker that reflects the level of inflammation and is superior to simple white blood cell counts in cirrhotic patients (18). It was reported that NLR could correctly identify these patients who had a high risk of mortality despite low MELD scores and a high risk of mortality (11), and NLR was positively correlated with Child–Turcotte–Pugh (CTP) score. In patients with Child–Pugh class C, NLR is an independent predictor of poor 1-month survival (13). A high NLR reflects the severity and progression of cirrhosis and has been associated with an increased risk of mortality in patients with alcoholic hepatitis and HE (14, 15). It has been reported that for every 1-unit increase in NLR at admission, the increased risk of death in patients with alcoholic hepatitis was 20 and 9% in 30 days and 12 months, respectively (16). Another study reported that elevated NLR was significantly associated with an increased risk of 30-day mortality in HE patients (14). As NLR reflects the level of inflammation, it may aggravate the symptoms of HE by enhancing ammonia-induced neurotoxicity through the blood–brain barrier (19). Elevated plasma levels of inflammatory markers in patients with HE are correlated with the severity of HE and are not determined by the severity of underlying liver disease or ammonia levels (20). Additionally, the neutrophil count is higher in decompensated cirrhotic patients than in compensated cirrhotic patients, while the lymphocyte count is lower in decompensated cirrhosis (21). This suggests that a higher level of NLR reflects worse patient status in decompensated cirrhosis. In patients with HCC, NLR has been identified as an independent factor for worse survival and predicts the response to treatment (18). Low NLR was significantly associated with a better survival rate and recurrence-free or disease-free survival (22). A review of the association between NLR and SBP concluded that NLR was a valid biomarker that can be readily integrated into clinical settings to prevent and predict SBP in cirrhotic patients (23). NLR has also been found to be a predictor of survival and readmission in other diseases such as cardiac and chronic obstructive pulmonary disease (11, 12). To the best of our knowledge, our study is the first to report the predictive role of NLR in the readmission of patients with HE. The correlation between NLR and readmission suggests that controlling inflammation in HE patients in clinical practice can help reduce the liver disease-related readmission rate in HE patients.
In our study, demographic variables, except for age and insurance, were not found to be significant predictors of readmission. It is worth noting that in China, not all individuals have access to medical insurance. Lack of medical insurance can hinder access to timely treatment and routine examinations, which may lead to a worsened condition and an increased risk of readmission. This is consistent with previous research by Andrew, who identified age and medical insurance as social-demographic predictors of 30-day readmission in patients with HE (7). Our study further found that insurance status was a significant predictor of readmission within 180 days. Therefore, access to medical insurance is crucial for patients with HE to receive timely and appropriate medical care and reduce the risk of readmission.
Regarding patients' complications and comorbidities, our study found that HCC and ascites were significantly related to HE patients' readmission. Ascites is a common complication of decompensated cirrhosis, and it directly increases the risk of further complications such as SBP, umbilical hernias, and respiratory compromise, all of which may require readmission (24). A previous study concluded that ascites were associated with early readmission in patients with cirrhosis (25). Ascites production is related to portal hypertension and splanchnic vasodilation, and it can also lead to renal dysfunction and hepatorenal syndrome (26). Previous research has suggested that ascites and renal dysfunction played important roles in the outcomes of patients with cirrhosis, and the use of diuretics and renal failure may impact HE as well (19, 26). Meanwhile, HCC is difficult to treat and associated with high mortality rates and surgical morbidity, increasing the risk of readmission (27). Hepatic resection and transplantation of HCC patients are still associated with a high risk of mortality and postoperative readmission rates. Furthermore, these procedures subject patients to higher medical and surgical morbidities compared to those encountered in the general surgery population (28). These complications and comorbidities can undoubtedly aggravate the condition of HE patients. In view of gender differences, ALD was a significant predictor of readmission in men. ALD has been found to be an important predictor of readmission in patients with cirrhosis and HE (29), and alcohol abuse is a common reason for readmission in cirrhotic patients (30). A study reported that in patients with alcoholic liver cirrhosis, there was a steady rise in the risk-adjusted 30-day all-cause readmission rate as well as alcoholic liver cirrhosis-specific readmission rate and readmission proportion (31). Furthermore, the increasing rate of readmission in ALD patients also increases the total hospital cost and the total days of hospital stay. Effective alcohol use disorder interventions can help reduce costs related to inpatient cirrhosis management (32). Managing HCC and ALD patients well in clinical practice can reduce the risk of readmission for patients with HE.
MELD score was used to identify prognosis and survival in patients with cirrhosis (33). Previous studies found that MELD score, INR, and hemoglobin were predictors of early readmission in cirrhotic patients after the resolution of HE (9). We did not include INR as a single factor, as the MELD score at discharge could represent the HE patients' status.
In our study, we observed gender differences in the predictors of readmission for patients with HE. In addition to ascites, MELD score, and NLR at the first discharge, ALD was significantly associated with readmission in men. Interestingly, hypertension, instead of ALD, predicted long-term readmission in women. Gender differences have been observed in many studies on chronic liver disease and HE. For example, women may experience a more favorable clinical course than men in early chronic liver disease, with sex hormones believed to have a protective effect on fibrosis progression (34, 35). Women with HE exhibited better cognitive performance than men. In a study on gut microbial composition in HE patients, it was observed that certain pathways and microbiota, such as Lactobacillaceae, androstenedione degradation, and cell wall synthesis, remained different between the sexes. These differences may contribute to the disparity in cognition between men and women with cirrhosis and ultimately affect the morbidity of HE in each gender (36). It should be noted that only 141 (33.3%) participants were women, and 9, 20, and 29 female patients were readmitted in 30, 90, and 180 days, so the smaller proportion of female patients may also be a contributing factor to the observed results. Therefore, large-scale studies are needed to further confirm the gender differences in the readmission of HE that we have observed.
Our study has identified NLR as a novel predictor of readmission in HE patients, improving the diagnosis of HE. The management of comorbidities, such as hypertension and CKD, is also crucial to the healthcare of patients with HE. However, our study has some limitations. First, although we took measures to ensure the accuracy of our data by conducting follow-ups with patients, as a retrospective single-center study, to confirm our results, multicenter studies should be carried out in the future. Moreover, we did not explore the mechanisms underlying the relationship between NLR and readmission or potential interventions to reduce readmission rates. Additionally, our study did not include other treatments, such as anti-infection and diuresis, which may become confounding factors for HE readmission. Anti-infection treatment may also affect NLR, and the lack of data on other inflammation indicators, such as CRP and IL-6, is another limitation. Furthermore, we did not collect information on HE patients' comorbidities and complications, such as dehydration, diuretic usage, human albumin infusion, and malnutrition, which may have influenced our findings. Therefore, future studies should aim to address these limitations and better understand these aspects.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
The studies involving human participants were reviewed and approved by the Ethics Committee of Peking University People's Hospital. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
RH designed the work and reviewed the article. LZ and WZ interpreted the data and drafted the manuscript. LZ, WZ, JW, QJ, and DM collected the data. All authors read and approved the final manuscript.
The project (RDJ2022-21) was supported by Peking University People's Hospital Scientific Research Development Funds and Peking University Hepatology Institute Qi-Min Project.
We appreciate the help of data analysis from Jiajun Feng.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Tapper EB, Henderson JB, Parikh ND, Ioannou GN, Lok AS. Incidence of and risk factors for hepatic encephalopathy in a population-based cohort of Americans with cirrhosis. Hepatol Commun. (2019) 3:1510–9. doi: 10.1002/hep4.1425
2. Krishnarao A, Gordon FD. Prognosis of hepatic encephalopathy. Clin Liver Dis. (2020) 24:219–29. doi: 10.1016/j.cld.2020.01.004
3. Weissenborn K. Hepatic encephalopathy: definition, clinical grading and diagnostic principles. Drugs. (2019) 79:5–9. doi: 10.1007/s40265-018-1018-z
4. Bianchi G, Giovagnoli M, Sasdelli AS, Marchesini G. Hepatic encephalopathy and health-related quality of life. Clin Liver Dis. (2012) 16:159–70. doi: 10.1016/j.cld.2011.12.003
5. Seraj SM, Campbell EJ, Argyropoulos SK, Wegermann K, Chung RT, Richter JM. Hospital readmissions in decompensated cirrhotics: factors pointing toward a prevention strategy. World J Gastroenterol. (2017) 23:6868–76. doi: 10.3748/wjg.v23.i37.6868
6. Gaspar R, Rodrigues S, Silva M, Costa-Moreira P, Morais R, Andrade P, et al. Predictive models of mortality and hospital readmission of patients with decompensated liver cirrhosis. Dig Liver Dis. (2019) 51:1423–9. doi: 10.1016/j.dld.2019.03.016
7. Kruger AJ, Aberra F, Black SM, Hinton A, Hanje J, Conteh LF, et al. A validated risk model for prediction of early readmission in patients with hepatic encephalopathy. Ann Hepatol. (2019) 18:310–7. doi: 10.1016/j.aohep.2018.08.001
8. Bajaj JS, O'Leary JG, Tandon P, Wong F, Kamath PS, Biggins SW, et al. Insurance status but not race and ethnicity are associated with outcomes in a large hospitalized cohort of patients with cirrhosis. Clin Gastroenterol Hepatol. (2021) 19:565–72 e5. doi: 10.1016/j.cgh.2020.04.081
9. Hu XP, Gao J. International normalized ratio and Model for End-stage Liver Disease score predict short-term outcome in cirrhotic patients after the resolution of hepatic encephalopathy. World J Gastroenterol. (2019) 25:3426–37. doi: 10.3748/wjg.v25.i26.3426
10. Gines P, Uriz J, Calahorra B, Garcia-Tsao G, Kamath PS, Del Arbol LR, et al. Transjugular intrahepatic portosystemic shunting versus paracentesis plus albumin for refractory ascites in cirrhosis. Gastroenterology. (2002) 123:1839–47. doi: 10.1053/gast.2002.37073
11. Biyik M, Ucar R, Solak Y, Gungor G, Polat I, Gaipov A, et al. Blood neutrophil-to-lymphocyte ratio independently predicts survival in patients with liver cirrhosis. Eur J Gastroenterol Hepatol. (2013) 25:435–41. doi: 10.1097/MEG.0b013e32835c2af3
12. Dai L, Liang B-M, Ou X-M. Predictive value of neutrophil-to-lymphocyte ratio and bilirubin levels in the readmission of acute exacerbation of chronic obstructive pulmonary disease. Am J Med Sci. (2023) 365:169–75. doi: 10.1016/j.amjms.2022.05.026
13. Sahani S, Das D. Neutrophil to lymphocyte ratio (NLR) and its correlation with Child Turcotte Pugh (CTP) score in predicting severity of decompensated liver cirrhosis. J Assoc Physicians India. (2022) 70:11–2.
14. Shi K, Huang Y, Zhang Q, Li Y, Wang X. Neutrophil–lymphocyte ratio and the risk of 30-day mortality in patients with overt hepatic encephalopathy. Eur J Gastroenterol Hepatol. (2022) 34:529–36. doi: 10.1097/MEG.0000000000002368
15. Shi K, Huang Y, Zhang Q, Ran C, Hou J, Zhang Y, et al. A dynamic nomogram to predict transplant-free mortality in patients with hepatitis B-related cirrhosis and overt hepatic encephalopathy. Int Immunopharmacol. (2022) 108:108879. doi: 10.1016/j.intimp.2022.108879
16. Vaz K, Little R, Majeed A, Kemp W, Roberts SK. Determinants of short- and long-term outcomes of an Australian cohort of patients admitted with alcoholic hepatitis. Dig Dis Sci. (2021) 67:3356–65. doi: 10.1007/s10620-021-07140-w
17. The Chinese National Workshop on Fatty Liver and Alcoholic Liver Disease for the Chinese Liver Disease Association. Guidelines for management of nonalcoholic fatty liver disease: an updated and revised edition. Chin J Hepatol. (2010) 18:163–6. doi: 10.3760/cma.j.issn.1007-3418.2010.03.002
18. Xu R, Huang H, Zhang Z, Wang F-S. The role of neutrophils in the development of liver diseases. Cell Mol Immunol. (2014) 11:224–31. doi: 10.1038/cmi.2014.2
19. Wijdicks EF. Hepatic encephalopathy. N Engl J Med. (2016) 375:1660–70. doi: 10.1056/NEJMra1600561
20. Shawcross DL, Wright G, Olde Damink SW, Jalan R. Role of ammonia and inflammation in minimal hepatic encephalopathy. Metab Brain Dis. (2007) 22:125–38. doi: 10.1007/s11011-006-9042-1
21. Zhao Z, Liu J, Wang J, Xie T, Zhang Q, Feng S, et al. Platelet-to-lymphocyte ratio (PLR) and neutrophil-to-lymphocyte ratio (NLR) are associated with chronic hepatitis B virus (HBV) infection. Int Immunopharmacol. (2017) 51:1–8. doi: 10.1016/j.intimp.2017.07.007
22. Qi X, Li J, Deng H, Li H, Su C, Guo X. Neutrophil-to-lymphocyte ratio for the prognostic assessment of hepatocellular carcinoma: A systematic review and meta-analysis of observational studies. Oncotarget. (2016) 7:45283–301. doi: 10.18632/oncotarget.9942
23. Seyedi SA, Nabipoorashrafi SA, Hernandez J, Nguyen A, Lucke-Wold B, Nourigheimasi S, et al. Neutrophil to lymphocyte ratio and spontaneous bacterial peritonitis among cirrhotic patients: a systematic review and meta-analysis. Can J Gastroenterol Hepatol. (2022) 2022:8604060. doi: 10.1155/2022/8604060
24. European Association for the Study of the Liver. EASL Clinical Practice Guidelines for the management of patients with decompensated cirrhosis. J Hepatol. (2018) 69:406–60. doi: 10.1016/j.jhep.2018.03.024
25. Orman ES, Ghabril MS, Desai AP, Nephew L, Patidar KR, Gao S, et al. Patient-reported outcome measures modestly enhance prediction of readmission in patients with cirrhosis. Clin Gastroenterol Hepatol. (2022) 20:e1426–37. doi: 10.1016/j.cgh.2021.07.032
26. Tsochatzis EA, Bosch J, Burroughs AK. Liver cirrhosis. Lancet. (2014) 383:1749–61. doi: 10.1016/S0140-6736(14)60121-5
27. Woodrell CD, Goldstein NE, Moreno JR, Schiano TD, Schwartz ME, Garrido MM. Inpatient specialty-level palliative care is delivered late in the course of hepatocellular carcinoma and associated with lower hazard of hospital readmission. J Pain Symptom Manage. (2021) 61:940–7 e3. doi: 10.1016/j.jpainsymman.2020.09.040
28. Khan S, Chidi A, Hrebinko K, Kaltenmeier C, Nassour I, Hoehn R, et al. Readmission after surgical resection and transplantation for hepatocellular carcinoma: a retrospective cohort study. Am Surg. (2022) 88:83–92. doi: 10.1177/0003134820973739
29. Garg SK, Sarvepalli S, Singh D, Obaitan I, Peeraphatdit T, Jophlin L, et al. Incidence and risk factors associated with 30-day readmission for alcoholic hepatitis. J Clin Gastroenterol. (2019) 53:759–64. doi: 10.1097/MCG.0000000000001202
30. Tapper EB, Halbert B, Mellinger J. Rates of and reasons for hospital readmissions in patients with cirrhosis: a multistate population-based cohort study. Clin Gastroenterol Hepatol. (2016) 14:1181–8 e2. doi: 10.1016/j.cgh.2016.04.009
31. Kichloo A, El-Amir Z, Dahiya DS, Wani F, Singh J, Solanki D, et al. Trends of alcoholic liver cirrhosis readmissions from 2010 to 2018: rates and healthcare burden associated with readmissions. World J Hepatol. (2021) 13:2128–36. doi: 10.4254/wjh.v13.i12.2128
32. Barritt IV AS, Jiang Y, Schmidt M, Hayashi PH, Bataller R. Charges for alcoholic cirrhosis exceed all other etiologies of cirrhosis combined: a national and state inpatient survey analysis. Dig Dis Sci. (2019) 64:1460–9. doi: 10.1007/s10620-019-5471-7
33. Huo TI, Lin HC, Wu JC, Lee FY, Hou MC, Lee PC, et al. Proposal of a modified Child-Turcotte-Pugh scoring system and comparison with the model for end-stage liver disease for outcome prediction in patients with cirrhosis. Liver Transpl. (2006) 12:65–71. doi: 10.1002/lt.20560
34. Rubin JB, Sundaram V, Lai JC. Gender differences among patients hospitalized with cirrhosis in the United States. J Clin Gastroenterol. (2020) 54:83–9. doi: 10.1097/MCG.0000000000001192
35. Yang JD, Abdelmalek MF, Pang H, Guy CD, Smith AD, Diehl AM, et al. Gender and menopause impact severity of fibrosis among patients with nonalcoholic steatohepatitis. Hepatology. (2014) 59:1406–14. doi: 10.1002/hep.26761
Keywords: hepatic encephalopathy, decompensated cirrhosis, neutrophil-to-lymphocyte ratio, readmission, hospitalization
Citation: Zhang L, Zhang W, Wang J, Jin Q, Ma D and Huang R (2023) Neutrophil-to-lymphocyte ratio predicts 30-, 90-, and 180-day readmissions of patients with hepatic encephalopathy. Front. Med. 10:1185182. doi: 10.3389/fmed.2023.1185182
Received: 13 March 2023; Accepted: 12 June 2023;
Published: 30 June 2023.
Edited by:
Xingshun Qi, General Hospital of Shenyang Military Command, ChinaReviewed by:
Piero Amodio, University of Padua, ItalyCopyright © 2023 Zhang, Zhang, Wang, Jin, Ma and Huang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Rui Huang, c3RyYW5nZWhlYWRAMTYzLmNvbQ==
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.