 Isabel Chateaubriand Diniz de Salles1*
Isabel Chateaubriand Diniz de Salles1* Renato Sernik1José Luiz Padilha da Silva2Cesar Taconeli2Ana Alice Amaral1
Renato Sernik1José Luiz Padilha da Silva2Cesar Taconeli2Ana Alice Amaral1 Christina May Moran de Brito1Ana Luiza Bierrenbach1
Christina May Moran de Brito1Ana Luiza Bierrenbach1- 1Hospital Sírio Libanês, Instituto de Ensino e Pesquisa, São Paulo, Brazil
- 2Departamento de Estatística, Universidade Federal do Paraná, Curitiba, Brazil
Background: Sarcopenia is a syndrome characterized by loss of muscle mass, strength and function. Frailty, a state of vulnerability with diminished reserves. The measurement of perioperative risk does not include the assessment of these variables, as little is known about how these conditions impact each other.
Methods: Observational study with a cross-sectional and a prospective cohort component. Elderly people over 60 years of age, able to walk and to independently perform activities of daily living were consecutively recruited in the preoperative period of non-emergency surgical procedures. Frailty was measured by the modified frailty index (mFI-11). Sarcopenia was measured by: (1) thickness and echogenicity on ultrasound; (2) handgrip strength on dynamometry and (3) gait speed. Data obtained from eight muscle groups were submitted to Principal Component Analysis. Postoperative complications were measured using the Clavien-Dindo scale. Follow-up was performed for 1 year to record readmissions and deaths.
Results: Between February and May 2019, 125 elderly people were recruited, median age of 71 years (IQR 65–77), 12% of whom were frail. Frailty was associated with older age, use of multiple medicines, presence of multimorbidity and greater surgical risk according to the American Society of Anesthesiologists (ASA) scale, in addition to lower gait speeds and lower handgrip strength. Frailty was also independently associated with smaller measurements of muscle thickness but not with echogenicity, and with longer hospital and Intensive care unit (ICU) stays. Prevalence of sarcopenia was 14% when considering at least two criteria: low walking speed and low handgrip strength. For muscle thickness, lower values were associated with female gender, older age, frailty, lower gait speeds and lower muscle strength, higher proportion of postoperative complications and higher occurrence of death. For echogenicity, higher values were related to the same factors as those of lower muscle thickness, except for postoperative complications. Lower gait speeds and lower handgrip strength were both associated with higher proportions of postoperative complications, and longer hospital stays. A higher mortality rate was observed in those with lower gait speeds.
Conclusion: Sarcopenia was associated with frailty in all its domains. Unfavorable surgical outcomes were also associated with these two conditions.
1. Introduction
Sarcopenia is a progressive and generalized muscle disease related to aging, characterized by loss of muscle mass, quality, and strength, with an impact on function, resulting in some degree of physical disability, loss of quality of life and increased mortality (1, 2). The prevalence and impact of sarcopenia vary substantially, as they depend on the definition applied, staging, and choice of instruments used for measurement, as well as the age range of the considered population (3). Sarcopenia is believed to be the main risk factor for aging-related functional decline (4, 5). Sarcopenia in the elderly and in patients with several comorbidities is related to prolonged hospitalizations, with higher rates of complications, especially infections, and higher overall mortality (6, 7). Impaired muscle function is an independent predictor of hospitalization, disability, and death (8).
Frailty is a state of vulnerability manifested by diminished physiological reserves that affect the ability to maintain homeostasis in the event of exposure to stressors, resulting in increased risk for adverse health outcomes (9–15). For a fragile patient, stressors can result in serious consequences, such as increased dependence on caregivers and a greater predisposition to falls and delirium. Frailty prevalence rates also vary widely, and this discrepancy can be explained by the lack of consensus on the definition applied, different instruments used for assessment, demographic characteristics, and particularities of the studied population (16, 17).
Elderly patients are at increased risk of postoperative complications (18), which require rapid recognition and treatment, particularly in this population, otherwise they can frequently lead to a cascade of events that may result in loss of independence and worsening of quality of life, higher treatment-related costs, some degree of disability, and greater mortality (19). Studies suggest that frailty is a condition that affects a large proportion of elderly patients who will undergo surgery (20–22).
In this scenario, the present study aimed to evaluate the association between sarcopenia, in its three domains, with frailty, in a population of elderly people admitted to hospital to undergo non-emergency surgical procedures. The association of sarcopenia with frailty is still unclear in the literature. There are studies that show the influence of sarcopenia on frailty overtime (23). Moreover, as a secondary objective, to evaluate the correlation of sarcopenia and frailty with postsurgical outcomes, as sarcopenia and frailty seem to have significant adverse impacts on the occurrence of postoperative outcomes (24).
2. Methods
An observational study was conducted in the preoperative units of the Hospital Sírio-Libanês, in São Paulo, Brazil–a tertiary, philanthropic institution with a 500-bed capacity. The participants were elderly people over 60 years of age, able to walk, with or without walking aids, admitted to hospital for non-emergency surgical procedures, who signed the Free and Informed Consent Term. Those with neuromuscular diseases, paresis, paralysis or limb amputation, dementia, and that were dependent for daily life activities, or lived with homecare, or were institutionalized were excluded. Patients were recruited consecutively, without prior selection. The initial interviews and measurements took place on the eve of the procedure and lasted an average of 20 min.
In the preoperative period, data were collected to characterize the population (Appendix 1 in Supplementary material). Frailty was characterized by the Modified Frailty Index 11 (which considers the presence of comorbidities and the functional status during the 30 days before surgery). Each one of the present comorbidities add one point, frailty adds on 3 or more points, and pre-frailty puts on 1 or 2 points (16, 17). The assessment of muscle mass was characterized using ultrasound measurement of the cross-sectional area of eight muscle groups: biceps brachii and brachii; rectus femoris; vastus intermedius; rectus abdominis; external and internal obliques; transversus abdominis; and medial gastrocnemius (Appendix 2 in Supplementary material). The percentage of fat was assessed by bioimpedance test (25). Muscle strength was measured with the use of a handgrip dynamometer (8, 9). Muscle function assessed by the 15-meter walk test (16, 17, 25, 26).
In the postoperative period, data related to surgical complications were collected daily, using the Clavien-Dindo Classification (Appendix 3 in Supplementary material), from the day after surgery until discharge (27). Hospital mortality and total length of stay were also computed. Mortality after discharge and hospital readmissions were accessed through telephone contact with the family or guardians, on the first, third and twelfth month after discharge.
Regarding the statistical analysis, categorical data were summarized by their absolute and relative frequencies and compared with the use of the Pearson’s Chi-square or Fisher’s Exact Test. Continuous data were summarized by their mean and standard deviations or by median and inter-quartile percentiles. When the data had a normal distribution, the Student’s t-test was used to compare two independent groups and the Analysis of Variance (ANOVA) and the F-test were used to compare three or more groups. When data were not normally distributed, the Wilcoxon-Mann–Whitney test was used when comparing two independent groups and the Kruskal-Wallis test was used when comparing three or more groups.
For the analysis of data on the thickness and echogenicity of muscle groups, we used the Principal Component Analysis (PCA). PCA was used to explore the correlation structure between the thickness and echogenicity measurements. In addition, it allowed us to reduce the dimension of the problem, by producing two new variables (principal components) able to explain a substantial amount of the original variation, registered by the eight thickness (or echogenicity). Parallel analysis was used to decide the number of principal components to be retained and studied. In the parallel analysis, new datasets are simulated completely at random, and the corresponding components are obtained. Then, the original components are compared with the simulated ones, and only those explaining more than the simulated ones should be considered. The principal components are defined by interpretable linear combinations based on the original variables, where the coefficients of each original variable are related to the correlations between the original variables and the components. Principal component analysis is a usual multivariate statistical method, largely used in medical sciences (28, 29).
The Hypothesis Tests of the association of the scores of the components 1 and 2 were performed separately with the main variables of the study, with the use of the tests for means described above. The Spearman’s correlation coefficient was calculated for the continuous variable “length of stay.” Interactions were also evaluated. Conclusions were based on a 5% significance level. All analysis were performed using the R statistical software, version 4.0.292. The R package psych was used to perform the principal component and parallel analysis.
3. Results
Between February and May 2019, 125 elderly people were recruited during the preoperative period of non-emergency surgeries. The studied group of patients had a slight male predominance (52.8%) and an average age of 71 years (IQR 65–77). The patients used a median of 4 different medications (IQR 2–6), had an average of 3 comorbidities (IQR 2–4), and an ASA score distributed as follows: 12 (9.6%) at level 1; 85 (68%) at level 2; and 28 (22.4%) at level 3. Regarding frailty, 77 (61.6%) were not frail, 33 (26.4%) were pre-frail, and 15 (12%) were frail. It was observed that older people, those who took more medications, had more comorbidities, and had higher ASA scores were more often considered frail (value of ps ≤0.001).
Of the 125 patients, 34 (28.3%) had low gait speed (the cut-off points for gait speed was ≤0.8 m/s). There were 20 (16%) patients with handgrip strength below the expected limit (the cut-off points for dynamometry were ≤ 27 kgf for men and ≤ 16 kgf for women). There were 38 (30.4%) patients with gait speed below 0.8 m/s or handgrip strength below the expected limit. Sarcopenia, measured by the 15-meter gait speed test and by the handgrip strength dynamometry, was positively correlated with frailty (Table 1).
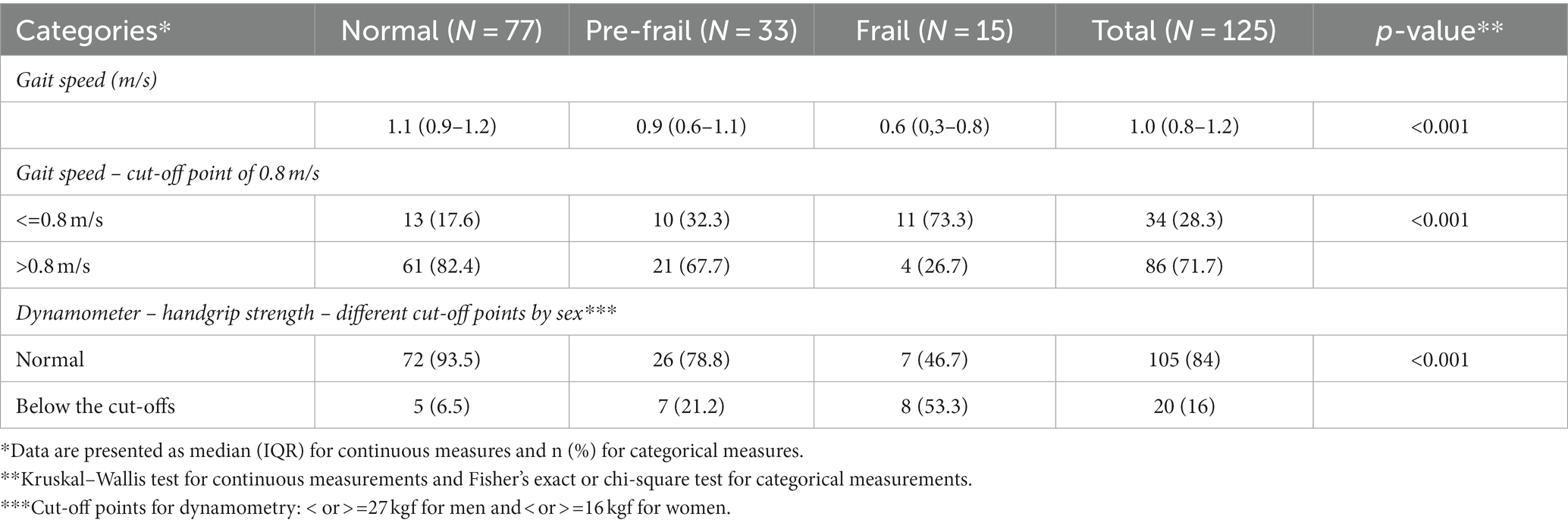
Table 1. Distribution of measurements of gait speed and strength, by degrees of frailty.
The other parameters used to characterize sarcopenia, which were muscle thickness and echogenicity obtained by ultrasound, are presented in Table 2, separated into the degrees of frailty. Lower values of muscle thickness were associated with frailty, except for the biceps and brachii, medial gastrocnemius, and rectus abdominis. Nevertheless, for echogenicity, there was no relationship between this measurement and frailty.
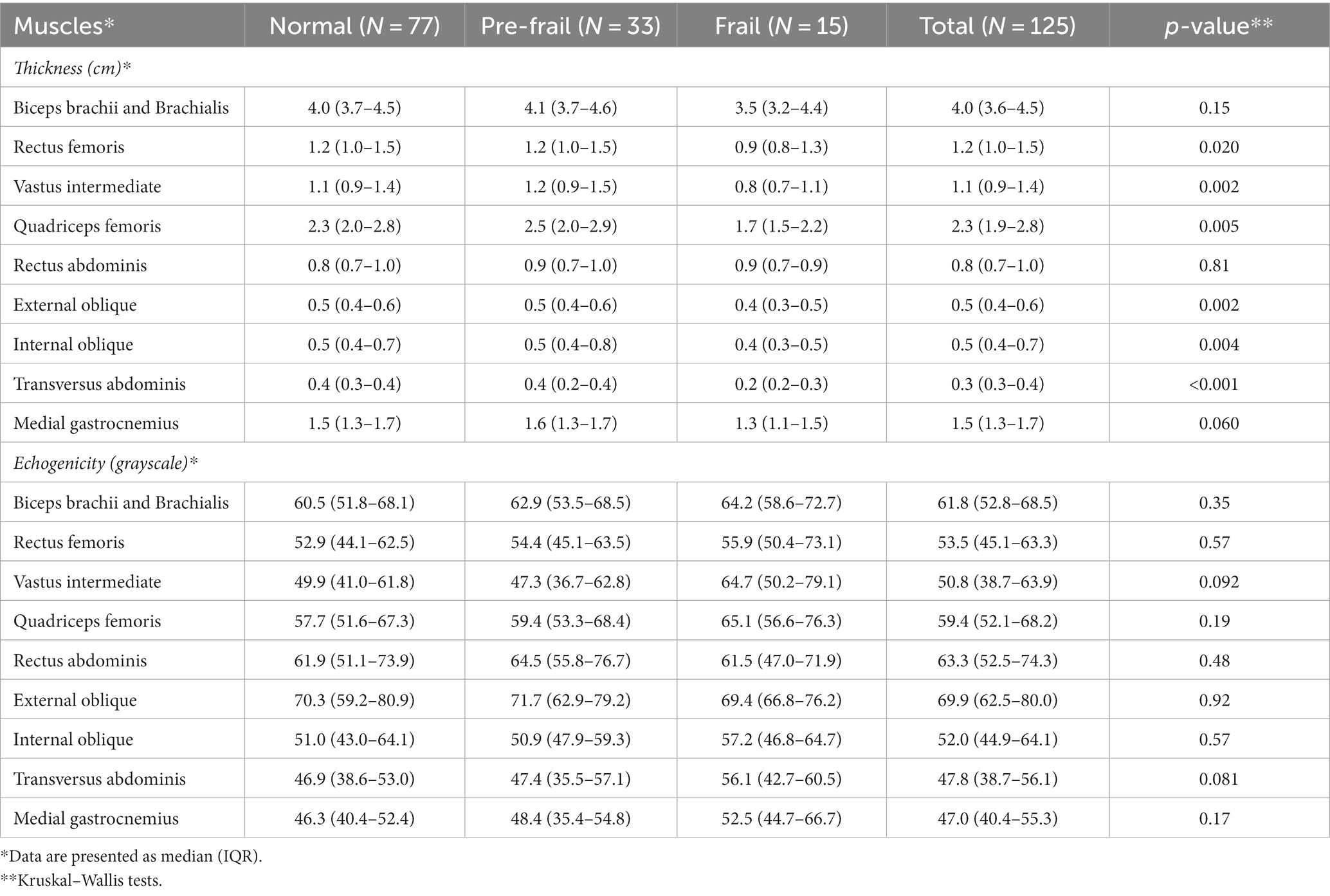
Table 2. Distribution of measurements of each muscle thickness and echogenicity, by degrees of frailty.
In Table 3, we describe the relationship between frailty and unfavorable outcomes. There was a significant correlation between frailty and length of stay, and, also, postoperative complications. The most frequent types of complications, considering the Clavien-Dindo Classification, were grades I (20.8%) and II (11.2%). There was no correlation between frailty and readmissions or death, considering the one-year follow-up period.
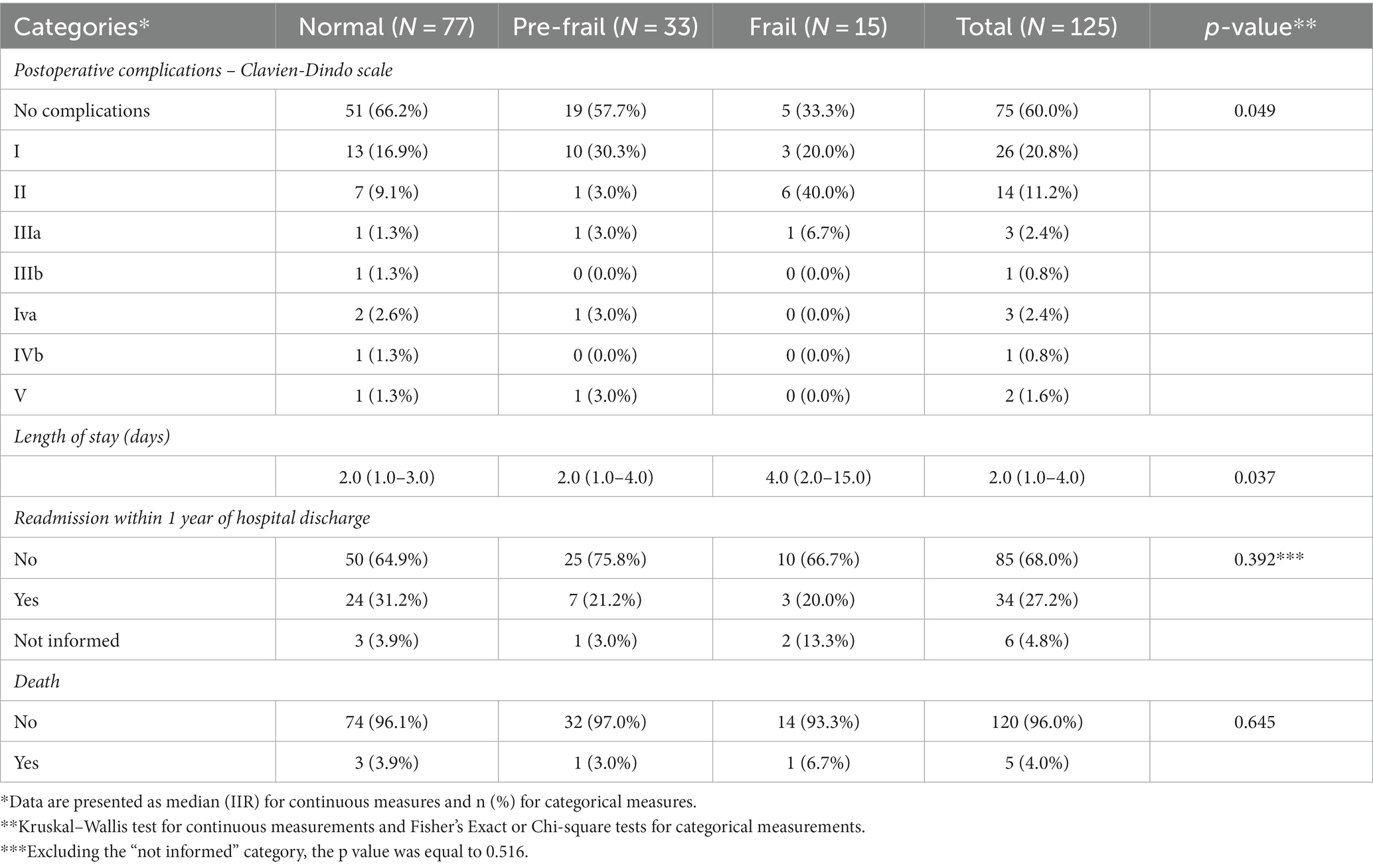
Table 3. Distribution of postoperative complications, length of stay, readmissions, and death up to 1 year of follow-up, separated by degrees of frailty.
Table 4 shows that lower gait speeds were associated with higher proportions of postoperative complications, longer length of stay, and higher occurrence of death. Similarly, Table 5 shows that lower handgrip strengths were associated with higher proportions of postoperative complications and longer length of stay, but there were no associations with readmission and death rates.
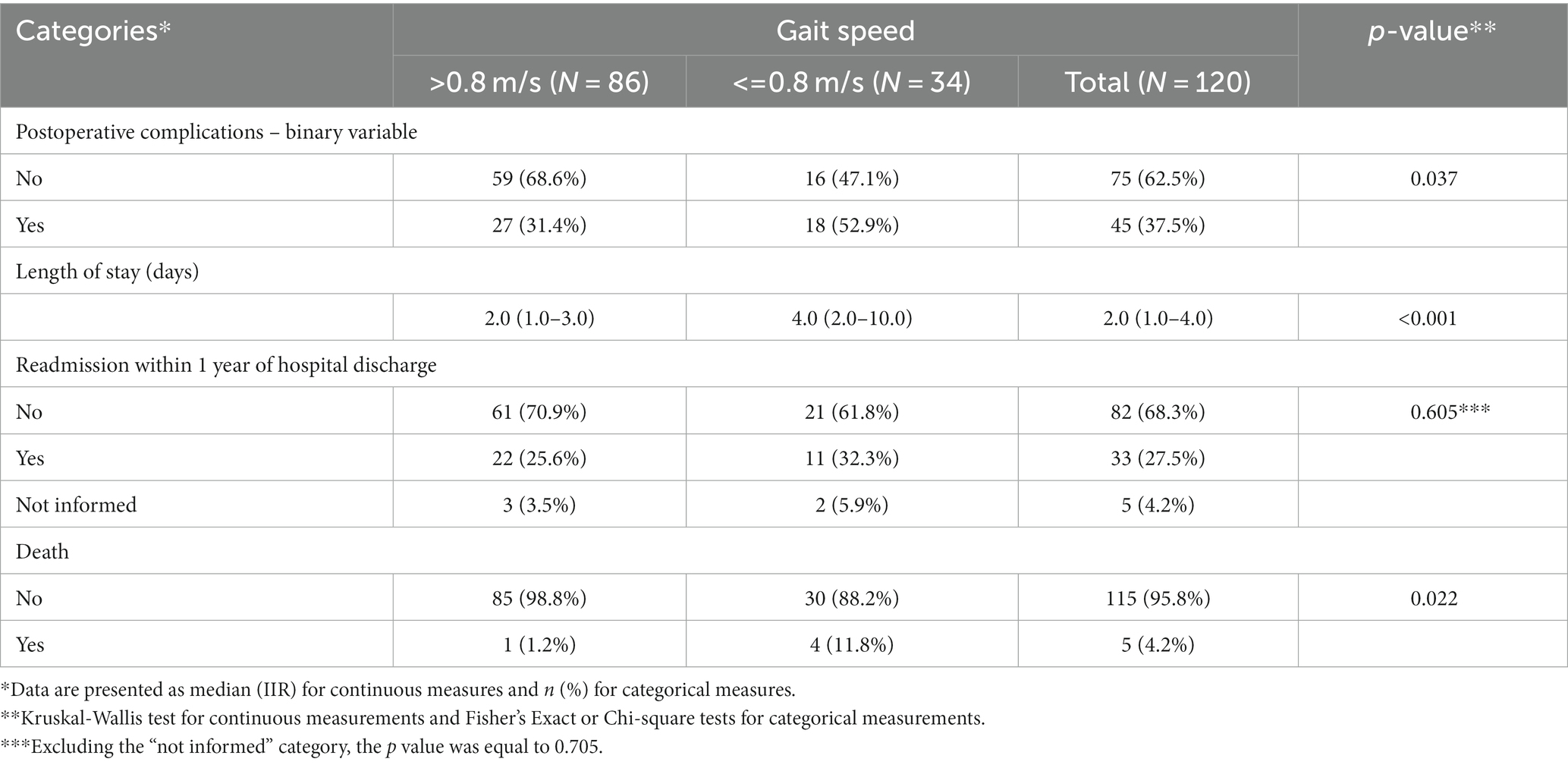
Table 4. Distribution of the studied outcomes: length of stay (days), readmission, and death due to any cause in up to 1 year of follow-up, separated into two categories of gait speed.
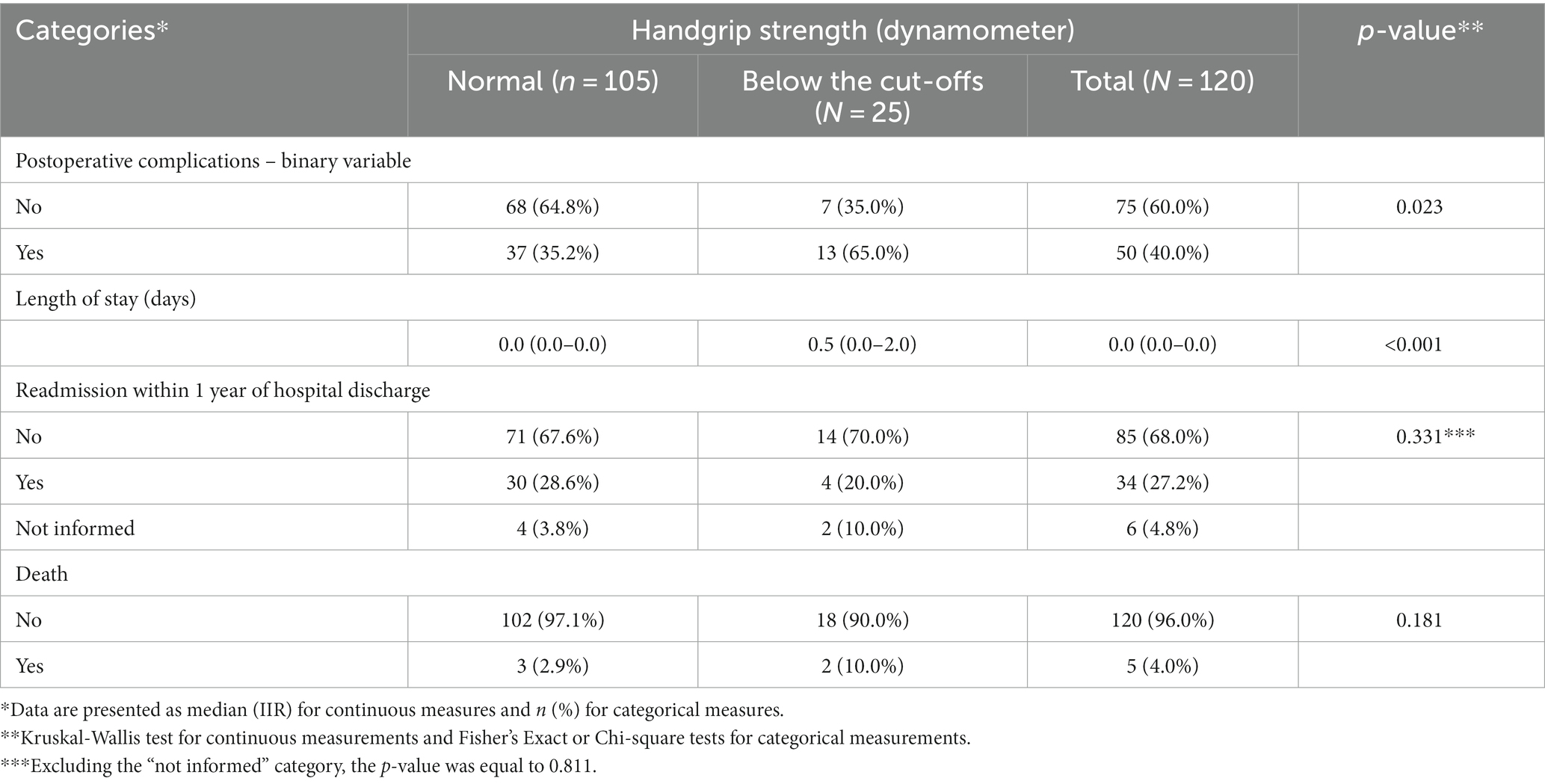
Table 5. Distribution of outcomes studied: length of stay (days), readmissions, and death due to any cause within up to 1 year of follow-up, separated into two categories of handgrip strength.
For the summary of the analysis of the eight muscle groups of the entire studied population, we used the statistical method Principal Component Analysis. Two principal components (or dimensions) were identified. The first principal component (PC1) assigned positive loadings for all thickness and echogenicity variables, i.e., all muscles were positively correlated with each other, that is, in an individual, if a muscle tended to be thinner or more echogenic, such characteristics tended to be replicated in other muscle groups. In other words, there is a congruence of measurements across the eight muscle groups. Vectors in Figure 1 (thickness and echogenicity) are all pointing toward the same direction in relation to the horizontal axis. The second principal component (PC2), on the other hand, assigned loadings with different sets of variables, and it can be interpreted as a contrast or divergence between the muscular behavior for appendicular and abdominal muscles. Component 2 is represented by the fact that the arrows for the appendicular muscles and those of the abdominal muscles are pointing toward opposite direction in relation to the vertical axis. The two principal components jointly explain 58.728 and 65.084% of the original variance for the thickness and echogenicity variables, respectively.
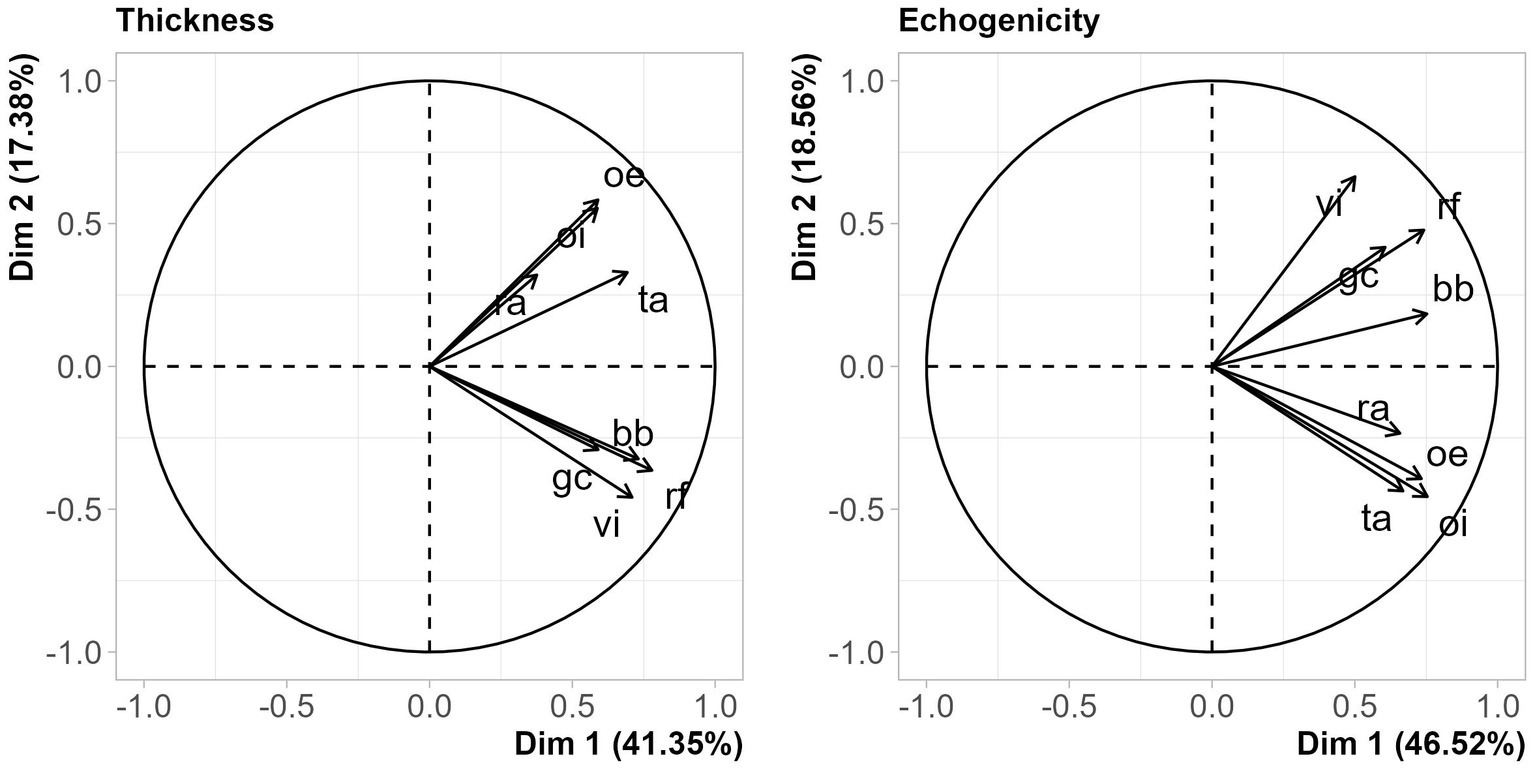
Figure 1. Principal component analysis of thickness and echogenicity measurements. The horizontal axis stands for the first principal component, the vertical, the second, whereas the arrows represents the original variables. Arrows with similar orientations show positively correlated variables.
The remaining results show the association of the principal components with the other study variables. For muscle thickness, higher values of component 1 were associated with male gender, younger age, lower degrees of frailty, higher gait speeds and normal handgrip strength measurements by dynamometry, absence of postoperative complications of grade II or higher on the Clavien-Dindo Classification, and not dying. There was no association of the component 1 with readmission for up to 1 year. There was a correlation of the component 2 with gender, that is, the thickness divergence between the appendicular and abdominal muscles occurred differently between the sexes: for men, the thickness of the appendicular muscles is greater than those presented by women. There were no other associations of the component 2 with other variables (Table 6).
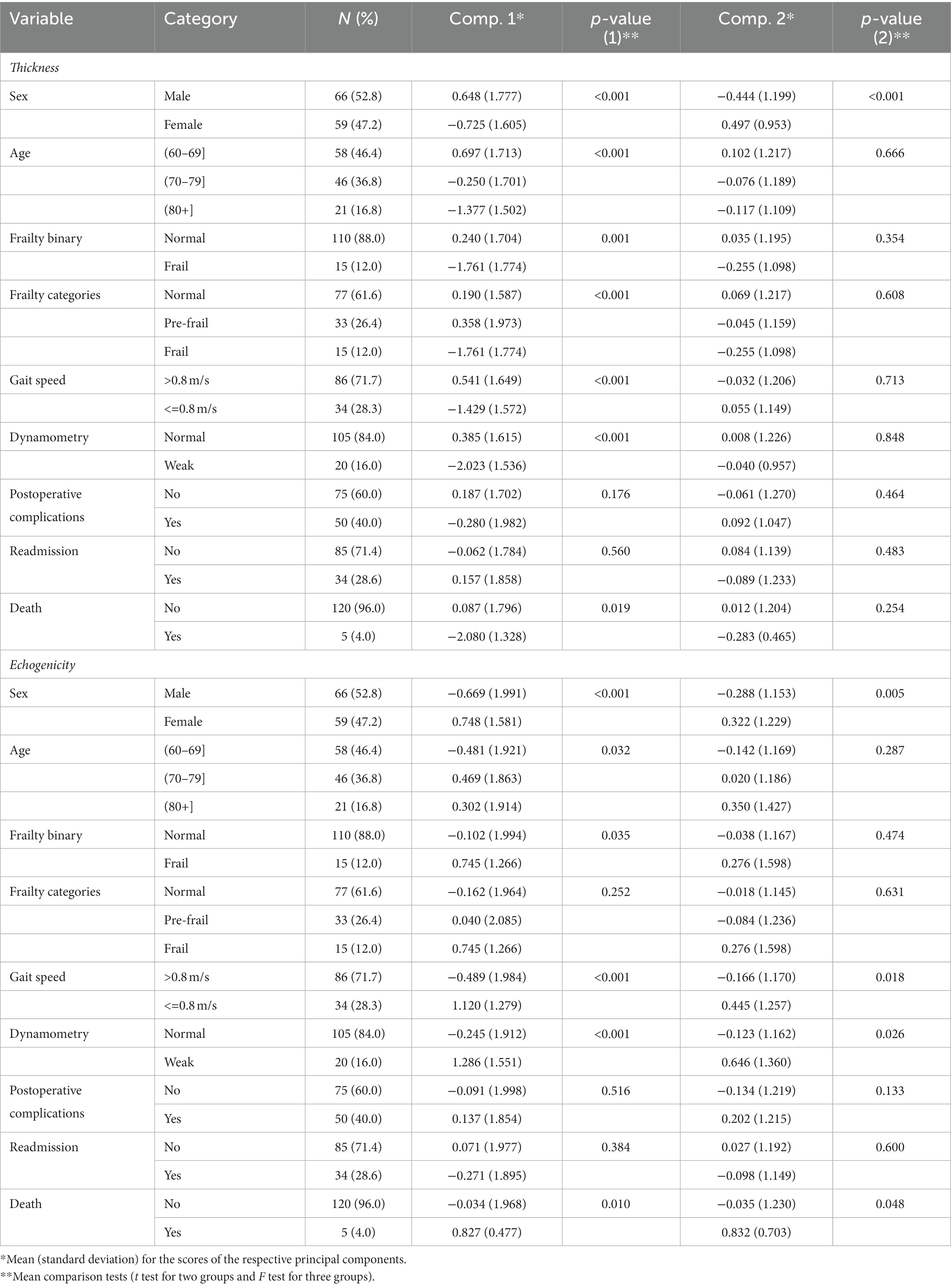
Table 6. Association between the principal components that summarize the thickness and echogenicity measurements and other categorical variables.
For echogenicity, higher values of component 1 were associated with female gender, older age, higher degrees of frailty (although only frailty categorized as a binary variable had a value of p <5%), lower gait speeds, lower handgrip strength measurements by dynamometry, and death (Table 6). There was an association of the component 2 with female gender, lower gait speeds and lower handgrip strength measurements by dynamometry, in addition to death - meaning that the echogenicity of the appendicular muscles, relative to those of the axial muscles, was higher for women, for people with low walking speed gait and low handgrip strength by dynamometry (Table 6).
4. Discussion
This study aimed to establish the association between frailty and sarcopenia in a series of 125 elderly subjects in the preoperative period of non-emergency surgery. As a secondary objective, we also sought to correlate sarcopenia and frailty with unfavorable outcomes, such as: longer hospital stays, readmissions, death, and postoperative complications.
Considering frailty, the prevalence found in our study was 12%, similar to other studies, which indicate the general prevalence of frailty from 10.7 to 13.6%. Interestingly enough, the prevalence of frailty in the elderly population varies from 4.0 to 59.1%, depending on the definition used and the population studied (16). The scale chosen to assess frailty in our study was the Modified Frailty Index 11 (mF11), which is already well established in the literature, and represents an accurate predictor of mortality and postoperative complications in surgery (30).
In our study, frailty was related to older age, but not to gender. This finding is coincident with the literature. Criteria for frailty were found in 16.7% of males and 6.8% of females (Appendix 1 in Supplementary material), differing from authors such as Collard and Fried, who found that the prevalence of frailty increases with age but is higher in women (16, 17, 31).
The prevalence of sarcopenia was 30.4% (Table 1), with no significant gender differences, when considering at least one criterion: gait speed below 0.8 m/s or handgrip strength below the expected limit for sex group. When considering at least two criteria, as recommended by the European consensus, the prevalence of sarcopenia in our study approaches the value of 14%, similar to that observed in the literature (32). The prevalence of sarcopenia varies enormously depending on the definition and instrument used to define it and the population studied. In studies carried out in the general population, the prevalence of sarcopenia in adults aged 60 to 70 years varies between 5 and 13%, increasing to 11 to 50% in those aged 80 years and over (33). In a meta-analysis that pooled studies with the definition of sarcopenia based on the European Working Group on Sarcopenia in Older People (EWGSOP) 2019 consensus, in healthy patients, aged 60 years and over, the overall estimates were 3.96% (32). In our study, the prevalence of sarcopenia, as defined by the European consensus, was slightly higher than that of frailty. It is important to keep in mind that frailty constitutes a broader functional spectrum compared to sarcopenia (34).
Frailty was correlated with sarcopenia, both in terms of loss of muscle strength and low gait speed, both conditions predefined by the EWGSOP consensus (32). Regarding the muscle mass criterion, frailty was correlated with smaller thicknesses of several muscles when evaluated separately, and there was also an association of frailty (binary variable) with component 1. It was previously seen that an increase in echogenicity of the quadriceps femoris is positively associated with age and negatively associated with muscle thickness and isometric knee extensor strength (35). In a big cohort of healthy men, the increase of echogenicity of the anterior thigh muscle compartment was related to diminished muscle strength (36). Nevertheless, in our study, no correlation was observed between echogenicity, and frailty. To justify our finding, it is important to point out that the most expressive gain in echogenicity already occurs in middle-aged individuals and may precede the loss of muscle mass (37).
Regarding the surgical outcomes associated with frailty, non-frail patients had fewer surgical complications, as assessed by the Clavien-Dindo Classification scale. There was a positive relationship between longer hospital stay and frailty. Readmissions within one year of follow-up were not correlated with frailty. No statistical correlation between death and frailty was observed. Studies indicate that the aging process varies between individuals depending on their overall functional reserves. This is reflected, for example, in a higher risk of poorer outcomes, given a surgical intervention, including greater chances of mortality (38).
Makary et al. studied patients undergoing elective surgery and demonstrated an increased risk of bad outcomes related to an increasing degree of frailty (39). McAdams-DeMarco et al. also demonstrated that frail patients undergoing kidney transplantation were significantly more likely to be readmitted earlier to the hospital, regardless of age (40). Frailty was directly related to an increase in the number of complications related to colorectal, cardiac and emergency surgery (41, 42).
In our study, considering the same outcomes, now faced with sarcopenia, lower gait speeds were associated with higher proportions of postoperative complications (Clavien-Dindo Classification equal to or above II), longer total hospital stay, and higher death rates. In the sarcopenia (loss of strength criterion), lower handgrip strengths were associated with higher incidence of post-surgical complications: Clavien-Dindo Classification equal to or above II and longer total hospital stay. No association with readmission or death was observed.
The mortality rate up to 1 year after surgery was 4% in our study group and it was especially related to sarcopenia (80% of these patients had severe sarcopenia). Of the 34 patients who underwent readmissions, 43.2% had at least 1 criterion to define sarcopenia or frailty.
5. Conclusion
In our study, sarcopenia, in all its domains, was associated with frailty. Unfavorable surgical outcomes were also associated with these two conditions.
Our findings also suggest that screening for sarcopenia and frailty in elderly patients who will undergo elective surgery is relevant, easy-to-perform and helps to access perioperative risk in this population.
We recognize, as limitations of this study, that this is a small sample in which the recruitment occurred in a single private hospital, that may cause restrictions to the generalization of our findings.
The present study is the first, to our knowledge, to assess sarcopenia in all its domains, with frailty, in a presurgical elderly population, with a 1 year follow up. The use of well-defined cutoff parameters, by the latest consensus of the EWGSOP 2019 contributes to create a more universal language for future studies in this area.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by Hospital Sirio Libanes. The patients/participants provided their written informed consent to participate in this study.
Author contributions
IS: conception and design of the work and acquisition of data for the work. CT and JS: substantial contributions to the analysis and interpretation of data for the work. CB: revising the article–intellectual content. AA: substantial contributions on acquisition of data for the work. RS: substantial contributions to the conception or design of the work. AB: substantial contributions to the conception or design of the work and accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. All authors contributed to the article and approved the submitted version.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2023.1185016/full#supplementary-material
References
1. Delmonico, MJ, Harris, TB, Lee, JS, Visser, M, Nevitt, M, Kritchevsky, SB, et al. Alternative definitions of sarcopenia, lower extremity performance, and functional impairment with aging in older men and women. J Am Geriatr Soc. (2007) 55:769–4. doi: 10.1111/j.1532-5415.2007.01140.x
2. Goodpaster, BH, Park, SW, Harris, TB, Kritchevsky, SB, Nevitt, M, Schwartz, AV, et al. The loss of skeletal muscle strength, mass, and quality in older adults: the health, aging and body composition study. J Gerontol A Biol Sci Med Sci. (2006) 61:1059–64. doi: 10.1093/gerona/61.10.1059
3. Abellan van Kan, G. Epidemiology and consequences of sarcopenia. J Nutr Health Aging. (2009) 13:708–2. doi: 10.1007/s12603-009-0201-z
4. Janssen, I, Heymsfield, SB, and Ross, R. Low relative skeletal muscle mass (sarcopenia) in older persons is associated with functional impairment and physical disability. J Am Geriatr Soc. (2002) 50:889–6. doi: 10.1046/j.1532-5415.2002.50216.x
5. Baumgartner, RN, Koehler, KM, Gallagher, D, Romero, L, Heymsfield, SB, Ross, RR, et al. Epidemiology of sarcopenia among the elderly in New Mexico. Am J Epidemiol. (1998) 147:755–3. doi: 10.1093/oxfordjournals.aje.a009520
6. Roubenoff, R, and Kehayias, JJ. The meaning and measurement of lean body mass. Nutr Rev. (1991) 49:163–5. doi: 10.1111/j.1753-4887.1991.tb03013.x
7. Pichard, C, Kyle, UG, Morabia, A, Perrier, A, Vermeulen, B, and Unger, P. Nutritional assessment: lean body mass depletion at hospital admission is associated with an increased length of stay. Am J Clin Nutr. (2004) 79:613–8. doi: 10.1093/ajcn/79.4.613
8. Newman, AB, Kupelian, V, Visser, M, Simonsick, EM, Goodpaster, BH, Kritchevsky, SB, et al. Strength, but not muscle mass, is associated with mortality in the health, aging and body composition study cohort. J Gerontol A Biol Sci Med Sci. (2006) 61:72–7. doi: 10.1093/gerona/61.1.72
9. Buigues, C, Juarros-Folgado, P, Fernández-Garrido, J, Navarro-Martínez, R, and Cauli, O. Frailty syndrome and pre-operative risk evaluation: a systematic review. Arch Gerontol Geriatr. (2015) 61:309–1. doi: 10.1016/j.archger.2015.08.002
10. Robinson, TN, Walston, JD, Brummel, NE, Deiner, S, Brown, CH, Kennedy, M, et al. Frailty for surgeons: review of a National Institute on Aging conference on frailty for specialists. J Am Coll Surg. (2015) 221:1083–92. doi: 10.1016/j.jamcollsurg.2015.08.428
11. Morley, JE, Vellas, B, Abellan van Kan, G, Anker, SD, Bauer, JM, Bernabei, R, et al. Frailty consensus: a call to action. J Am Med Dir Assoc. (2013) 14:392–7. doi: 10.1016/j.jamda.2013.03.022
12. Revenig, LM, Canter, DJ, Taylor, MD, Tai, C, Sweeney, JF, Sarmiento, JM, et al. Too frail for surgery? Initial results of a large multidisciplinary prospective study examining preoperative variables predictive of poor surgical outcomes. J Am Coll Surg. (2013) 217:665–670e1. doi: 10.1016/j.jamcollsurg.2013.06.012
13. Fagard, K, Leonard, S, Deschodt, M, Devriendt, E, Wolthuis, A, Prenen, H, et al. The impact of frailty on postoperative outcomes in individuals aged 65 and over undergoing elective surgery for colorectal cancer: a systematic review. J Geriatr Oncol. (2016) 7:479–1. doi: 10.1016/j.jgo.2016.06.001
14. Chen, X, Mao, G, and Leng, SX. Frailty syndrome: an overview. Clin Interv Aging. (2014) 9:433–1. doi: 10.2147/CIA.S45300
15. Walston, J, Hadley, EC, Ferrucci, L, Guralnik, JM, Newman, AB, Studenski, SA, et al. Research agenda for frailty in older adults: toward a better understanding of physiology and etiology: summary from the American Geriatrics Society/National Institute on Aging research conference on frailty in older adults. J Am Geriatr Soc. (2006) 54:991–01. doi: 10.1111/j.1532-5415.2006.00745.x
16. Collard, RM, Boter, H, Schoevers, RA, and Oude Voshaar, RC. Prevalence of frailty in community-dwelling older persons: a systematic review. J Am Geriatr Soc. (2012) 60:1487–92. doi: 10.1111/j.1532-5415.2012.04054.x
17. Sternberg, SA, Schwartz, AW, Karunananthan, S, Bergman, H, and Mark Clarfield, A. The identification of frailty: a systematic literature review. J Am Geriatr Soc. (2011) 59:2129–38. doi: 10.1111/j.1532-5415.2011.03597.x
18. Polanczyk, CA, Marcantonio, E, Goldman, L, Rohde, LEP, Orav, J, Mangione, CM, et al. Impact of age on perioperative complications and length of stay in patients undergoing noncardiac surgery. Ann Intern Med. (2001) 134:637–3. doi: 10.7326/0003-4819-134-8-200104170-00008
19. Hamel, MB, Henderson, WG, Khuri, SF, and Daley, J. Surgical outcomes for patients aged 80 and older: morbidity and mortality from major noncardiac surgery. J Am Geriatr Soc. (2005) 53:424–9. doi: 10.1111/j.1532-5415.2005.53159.x
20. Cohen, R-R, Lagoo-Deenadayalan, SA, Heflin, MT, Sloane, R, Eisen, I, Thacker, JM, et al. Exploring predictors of complication in older surgical patients: a deficit accumulation index and the Braden scale. J Am Geriatr Soc. (2012) 60:1609–15. doi: 10.1111/j.1532-5415.2012.04109.x
21. Adams, P, Ghanem, T, Stachler, R, Hall, F, Velanovich, V, and Rubinfeld, I. Frailty as a predictor of morbidity and mortality in inpatient head and neck surgery. JAMA Otolaryngol Head Neck Surg. (2013) 139:783–9. doi: 10.1001/jamaoto.2013.3969
22. Zampini, JM. CORR insights®: association of a modified frailty index with mortality after femoral neck fracture in patients aged 60 years and older. Clin Orthop Relat Res. (2014) 472:1018–9. doi: 10.1007/s11999-013-3387-7
23. Álvarez-Bustos, A, Carnicero-Carreño, JA, Davies, B, Garcia-Garcia, FJ, Rodríguez-Artalejo, F, Rodríguez-Mañas, L, et al. Role of sarcopenia in the frailty transitions in older adults: a population-based cohort study. J Cachexia Sarcopenia Muscle. (2022) 13:2352–60. doi: 10.1002/jcsm.13055
24. Shen, Y, Hao, Q, Zhou, J, and Dong, B. The impact of frailty and sarcopenia on postoperative outcomes in older patients undergoing gastrectomy surgery: a systematic review and meta-analysis. BMC Geriatr. (2017) 17:188. doi: 10.1186/s12877-017-0569-2
25. Rubbieri, G, Mossello, E, and Di Bari, M. Techniques for the diagnosis of sarcopenia. Off J Ital Soc Osteoporosis Miner Metab Skelet Dis. (2014) 11:181–4. doi: 10.11138/ccmbm/2014.11.3.181
26. Arts, IMP, Pillen, S, Schelhaas, HJ, Overeem, S, and Zwarts, MJ. Normal values for quantitative muscle ultrasonography in adults. Muscle Nerve. (2010) 41:32–41. doi: 10.1002/mus.21458
27. Clavien, PA, Barkun, J, de Oliveira, ML, Vauthey, JN, Dindo, D, Schulick, RD, et al. The Clavien-Dindo classification of surgical complications: five-year experience. Ann Surg. (2009) 250:187–6. doi: 10.1097/SLA.0b013e3181b13ca2
28. For the SPRINTT ConsortiumCalvani, R, Marini, F, Cesari, M, Tosato, M, Picca, A, et al. Biomarkers for physical frailty and sarcopenia. Aging Clin Exp Res. (2017) 29:29–34. doi: 10.1007/s40520-016-0708-1,
29. Malmstrom, TK, Miller, DK, Simonsick, EM, Ferrucci, L, and Morley, JE. SARC-F: a symptom score to predict persons with sarcopenia at risk for poor functional outcomes. J Cachexia Sarcopenia Muscle. (2016) 7:28–36. doi: 10.1002/jcsm.12048
30. Subramaniam, S, Aalberg, JJ, Soriano, RP, and Divino, CM. New 5-factor modified frailty index using American College of Surgeons NSQIP data. J Am Coll Surg. (2018) 226:173–181e8. doi: 10.1016/j.jamcollsurg.2017.11.005
31. Fried, LP, Tangen, CM, Walston, J, Newman, AB, Hirsch, C, Gottdiener, J, et al. Frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci Med Sci. (2001) 56:M146–57. doi: 10.1093/gerona/56.3.M146
32. Cruz-Jentoft, AJ, Bahat, G, Bauer, J, Boirie, Y, Bruyère, O, Cederholm, T, et al. Sarcopenia: revised European consensus on definition and diagnosis. Age Ageing. (2019) 48:16–31. doi: 10.1093/ageing/afy169
33. von Haehling, S, Morley, JE, and Anker, SD. From muscle wasting to sarcopenia and myopenia: update 2012. J Cachexia Sarcopenia Muscle. (2012) 3:213–7. doi: 10.1007/s13539-012-0089-z
34. Rockwood, K, and Mitnitski, A. Frailty in relation to the accumulation of deficits. J Gerontol A Biol Sci Med Sci. (2007) 62:722–7. doi: 10.1093/gerona/62.7.722
35. Fukumoto, Y, Ikezoe, T, Yamada, Y, Tsukagoshi, R, Nakamura, M, Mori, N, et al. Skeletal muscle quality assessed from echo intensity is associated with muscle strength of middle-aged and elderly persons. Eur J Appl Physiol. (2012) 112:1519–25. doi: 10.1007/s00421-011-2099-5
36. Watanabe, Y, Yamada, Y, Fukumoto, Y, Ishihara, T, Yokoyama, K, Yoshida, T, et al. Echo intensity obtained from ultrasonography images reflecting muscle strength in elderly men. Clin Interv Aging. (2013) 8:993–8. doi: 10.2147/CIA.S47263
37. Fukumoto, Y, Ikezoe, T, Yamada, Y, Tsukagoshi, R, Nakamura, M, Takagi, Y, et al. Age-related ultrasound changes in muscle quantity and quality in women. Ultrasound Med Biol. (2015) 41:3013–7. doi: 10.1016/j.ultrasmedbio.2015.06.017
38. Chow, WB, Rosenthal, RA, Merkow, RP, Ko, CY, Esnaola, NF, American College of Surgeons National Surgical Quality Improvement Program, et al. Optimal preoperative assessment of the geriatric surgical patient: a best practices guideline from the American College of Surgeons National Surgical Quality Improvement Program and the American Geriatrics Society. J Am Coll Surg. (2012) 215:453–6. doi: 10.1016/j.jamcollsurg.2012.06.017
39. Makary, MA, Segev, DL, Pronovost, PJ, Syin, D, Bandeen-Roche, K, Patel, P, et al. Frailty as a predictor of surgical outcomes in older patients. J Am Coll Surg. (2010) 210:901–8. doi: 10.1016/j.jamcollsurg.2010.01.028
40. McAdams-DeMarco, MA, Law, A, Salter, ML, Chow, E, Grams, M, Walston, J, et al. Frailty and early hospital readmission after kidney transplantation. Am J Transplant. (2013) 13:2091–5. doi: 10.1111/ajt.12300
41. Robinson, TN, Wu, DS, Pointer, L, Dunn, CL, Cleveland, JC, and Moss, M. Simple frailty score predicts postoperative complications across surgical specialties. Am J Surg. (2013) 206:544–09. doi: 10.1016/j.amjsurg.2013.03.012
Keywords: sarcopenia, frailty, ultrasonography, aged, postoperative complications
Citation: de Salles ICD, Sernik R, da Silva JLP, Taconeli C, Amaral AA, de Brito CMM and Bierrenbach AL (2023) Sarcopenia, frailty, and elective surgery outcomes in the elderly: an observational study with 125 patients (the SAFESOE study). Front. Med. 10:1185016. doi: 10.3389/fmed.2023.1185016
Edited by:
Ozra Tabatabaei-Malazy, Tehran University of Medical Sciences, IranReviewed by:
Francesco Corica, University of Messina, ItalyFrancesco Cacciatore, University of Naples Federico II, Italy
Shirin Djalalinia, Ministry of Health and Medical Education, Iran
Nekoo Panahi, Tehran University of Medical Sciences, Iran
Copyright © 2023 de Salles, Sernik, da Silva, Taconeli, Amaral, de Brito and Bierrenbach. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Isabel Chateaubriand Diniz de Salles, aXNhYmVsLnNhbGxlc0Boc2wub3JnLmJy