 Klara Martinsson1*
Klara Martinsson1* Andrea Di Matteo2
Andrea Di Matteo2 Carina Öhman3
Carina Öhman3 Anders Johansson3
Anders Johansson3 Anna Svärd1,4
Anna Svärd1,4 Kulveer Mankia2
Kulveer Mankia2 Paul Emery2
Paul Emery2 Alf Kastbom1,5
Alf Kastbom1,5- 1Division of Inflammation and Infection, Department of Biomedical and Clinical Sciences, Linköping University, Linköping, Sweden
- 2Leeds Musculoskeletal Biomedical Research Unit, LTHT and Leeds Institute of Rheumatic and Musculoskeletal Medicine, University of Leeds, Leeds, United Kingdom
- 3Department of Odontology, Umeå University, Umeå, Sweden
- 4Center for Clinical Research Dalarna, Uppsala University, Uppsala, Sweden
- 5Department of Rheumatology, Linköping University Hospital, Linköping, Sweden
Objectives: Periodontitis and underlying bacteria have been linked to the development of rheumatoid arthritis (RA). One suggested pathogen is Aggregatibacter actinomycetemcomitans (A.a.), which expresses leukotoxin A (LtxA) that can citrullinate human proteins, providing a possible trigger for the production of anti-citrullinated protein antibodies (ACPA). In this study, we seek to determine the presence of antibodies toward LtxA in patients at risk of developing RA.
Methods: Two prospective observational patient cohorts (one Swedish and one British) with symptomatic at-risk patients were studied. Anti-LtxA antibodies were analyzed by a cell-based neutralization assay in baseline serum and compared to 100 Swedish blood donors that served as controls.
Results: Serum anti-LtxA levels or positivity did not differ between patients and blood donors. In the British cohort, anti-LtxA was more prevalent among ACPA-positive arthralgia patients compared with ACPA-negative arthralgia cases (24% vs. 13%, p < 0.0001). In the Swedish at-risk cohort, anti-LtxA positive patients were at increased risk of progression to arthritis (hazard ratio (HR) 2.10, 95% CI 1.04–4.20), but this was not confirmed in the UK at-risk cohort (HR 0.99, CI 0.60–1.65).
Conclusion: Serum anti-LtxA is not elevated before RA diagnosis, and associations with disease progression and ACPA levels differ between populations. Other features of the oral microbiome should be explored in upcoming periodontitis-related RA research.
Introduction
Connections between mucosal tissues and rheumatoid arthritis (RA) development have been attracting increasing interest in recent years (1). In this context, the oral cavity is of particular interest due to the reported association between periodontitis and RA (2). Such a link was further substantiated by the identification of protein citrullination properties of bacteria underlying periodontitis, providing a possible trigger for the production of anti-citrullinated protein antibodies (ACPA) (2, 3). Aggregatibacter actinomycetemcomitans (A.a.) is a Gram-negative coccobacillus that is recognized as a pathogen in periodontitis. Recent findings indicate high systemic immunoreactivity against A.a. when compared with several other bacterial species that are commonly detected in the human commensal microflora (4). A.a. produces a toxin called leukotoxin A (LtxA), which is a major virulence factor in periodontitis in young individuals (5). Intriguingly, LtxA was shown to trigger protein hypercitrullination in interaction with neutrophils, and antibodies to LtxA were increased in RA and correlated with ACPA levels (3, 6). These features of A.a. are of great interest considering that ACPA occurrence is a strong predictor of arthritis development among individuals with arthralgia (7) and of joint erosions in patients with recent-onset RA (8). Despite this, the role of A.a. in RA development and progression has been sparsely investigated. Nevertheless, it was recently shown that anti-LtxA IgM levels associate with RA onset (9), and circulating A.a. antibodies were associated with subclinical atherosclerosis in RA (10).
Previous studies on immune responses to A.a. have mostly used enzyme-linked immunoassays using A.a. LtxA as an antigen (3, 9). However, since the LtxA could be a starting point for the process leading to hypercitrullination and ACPA formation (3), it is of potential advantage to instead assess the functional (neutralizing) capacity of anti-LtxA in serum. The presence of systemic LtxA neutralizing activity has shown a strong correlation between systemic ab that binds LtxA (11) and the presence of A.a in the subgingival plaque (12). By using two cohorts of patients at risk of developing RA, we aimed to characterize the neutralizing anti-LtxA antibodies in relation to clinical course and autoantibody levels. This knowledge is of importance from an etiological perspective and to guide further work concerning dental interventions for the treatment of RA.
Materials and methods
Study populations
We included two independent at-risk cohorts, one Swedish with ACPA-positive patients only and one British with both ACPA-positive and ACPA-negative at-risk patients. Baseline characteristics are shown in Table 1. In addition, 100 Swedish healthy blood donors were included to serve as controls.
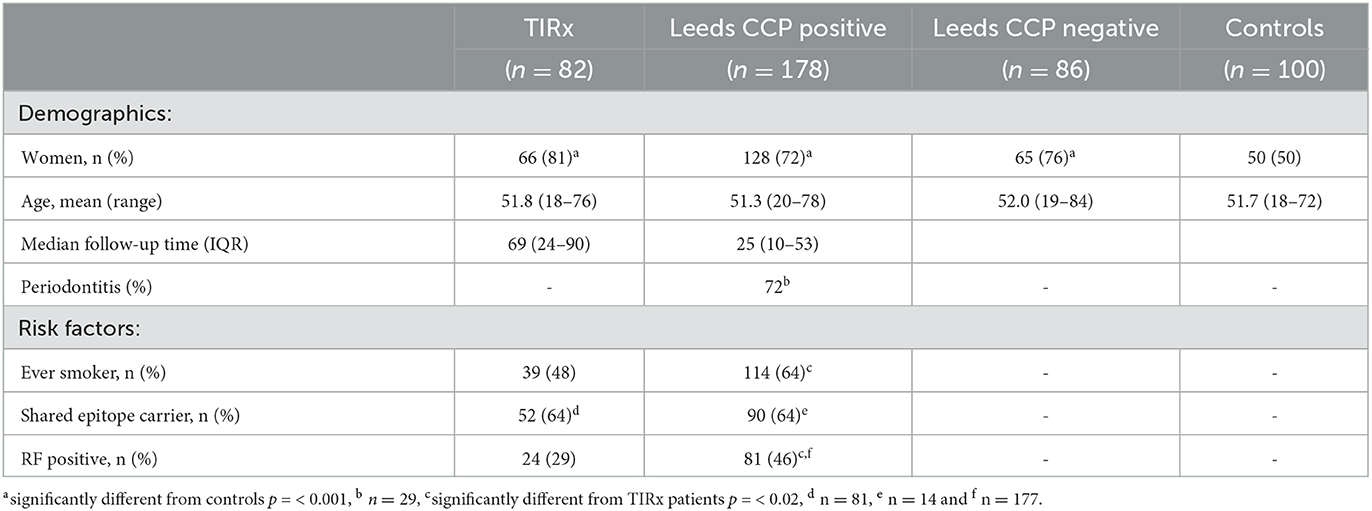
Table 1. Baseline characteristics of at-risk patients and controls.
At-risk patients
TIRx cohort
In the TIRx cohort (Swedish acronym for “xtra early rheumatology follow-up”), 82 patients with a positive IgG ACPA test in clinical routine and musculoskeletal pain of any sort and duration, but no baseline arthritis, were followed prospectively for the development of clinical arthritis (13). Patients were recruited between 2010 and 2013 at the rheumatology unit, Linköping University Hospital, Sweden. The exclusion criteria were previous rheumatic disease or treatment with oral corticosteroids within 6 weeks. Follow-up visits were scheduled regularly, and arthritis development was defined upon clinical examination by an experienced rheumatologist. The median follow-up time was 69 months [interquartile range (IQR) 24–90]. Progression to arthritis occurred in 39 out of 82 patients (48%) after the median 6 months (IQR: 1–71). A total of 15 patients (18%) had symptom duration up to 6 months, 27 (45%) patients had symptom duration between 6 and 18 months, and 30 (37%) patients had experienced symptoms >18 months prior to inclusion.
Leeds cohort
Anti-CCP positive at-risk individuals who took part in “The CCP Study: Coordinated Programme to Prevent Arthritis—Can We Identify Arthritis at a Pre-clinical Stage?” were enrolled from June 2008 to January 2019. A detailed description of the CCP study has been previously published (14, 15). In this national observational UK study, individuals who presented to their general practitioner (or other health professionals) with a new non-specific musculoskeletal symptom were tested for anti-CCP antibodies.
The individuals who have a positive anti-CCP2 test were then invited to Chapel Allerton Hospital, Leeds, UK, for further assessments at a dedicated research clinic as part of an observational longitudinal study until the development of inflammatory arthritis. Individuals with a negative anti-CCP antibody test were sent a postal questionnaire 12 months after enrollment, asking about their disease status (i.e., progression to inflammatory arthritis) (16).
For this study, we reviewed 178 anti-CCP positive individuals without baseline arthritis from the Leeds CCP cohort. Out of these subjects, 81 (46%) developed clinical arthritis during a median follow-up period of 25 months.
Control groups
A total of 100 healthy blood donors recruited from Linköping University Hospital served as controls for the at-risk patient cohorts. These controls were age-matched to the TIRx cohort. In the UK, 86 anti-CCP negative subjects with arthralgia were selected as controls.
Ethics
The ethical review board in Linköping, Sweden, approved the study protocol (Decision No. M220-09, 2015/236-32 and 2017/260-32). The Leeds CCP Study was approved by the NHS Health Research Authority National Research Ethics Service Committee Yorkshire and the Humber-Leeds West (REC reference: 06/Q1205/169). All participants signed written informed consent.
LtxA antibody assay
Anti-LtxA antibodies were analyzed for their LtxA neutralizing capacity. This was detected as reduction in cell damage, assessed by neutral red leakage, following exposure to purified LtxA (17). THP-1 cells in RPMI-10% fetal bovine serum (FBS)-50 nM phorbol myristate acetate were seeded at 1 x 106 cells/ml in flat 96 well plates and incubated at 37°C 5% CO2 overnight. The cells were washed with RPMI, and then patient serum and LtxA were added to the wells in triplicates. The plates were incubated for 2 h at 37°C with 5% CO2. The medium was removed, and 0.04 mg/ml neutral red diluted in RPMI-10% FBS was added to the wells and incubated for 90 min at 37°C with 5% CO2. The wells were washed with PBS (pH 7.4), and then 50% EtOH-1% acetic acid was added to lyse the cells. Following 10 min of incubation, the optical density (OD) was read at 650 nm (TECAN Sunrise, CA, USA). Anti-LtxA antibody neutralization capacity in percent was calculated by dividing serum sample OD with maximum cell viability OD (FBS) x 100. Serum samples inhibiting LtxA cell lysis >30% were classified as positive and <30% were classified as negative regarding anti-LtxA presence (11).
Autoantibody analyses
Serum secretory component-containing (SC) ACPA and IgM ACPA were measured by modifying commercially available anti-CCP ELISA kits (Euro-Diagnostica, Malmö, Sweden) as described earlier (18). Serum IgA and IgG ACPA were analyzed by a fluoroenzyme immunoassay (EliATM Phadia AB, Thermo Fisher Scientific, Uppsala, Sweden) as described previously (18). RF tests were performed in a clinical routine setting at each local laboratory associated with the participating rheumatology unit. Free SC in serum was analyzed using an in-house sandwich ELISA as previously described (19).
Statistics
Mann–Whitney U-test or Fisher's exact test was used to analyze differences between groups. The prognostic value of anti-LtxA antibodies was studied using Cox regression analysis and, when statistically significant in univariable analysis, adjusted in multivariable analysis for age, sex, smoking, RF status, ACPA levels, and symptom duration.
Results
The baseline characteristics of patients and controls are shown in Table 1.
There were no significant differences in anti-LtxA levels or percentage-positive individuals between the two at-risk cohorts and the controls (Figure 1).
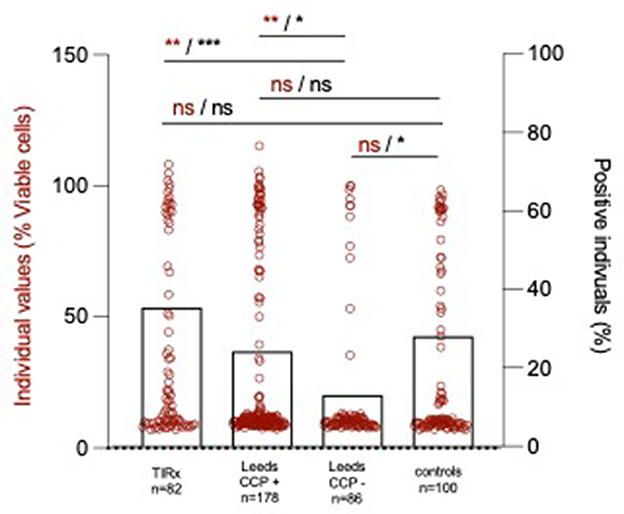
Figure 1. Individual anti-LtxA levels (red circles and statistical notations in red) and percentage positive individuals (black bars, mean ± SD and statistical notations in black). *p < 0.05, **p < 0.01, and ***p < 0.001.
Serum anti- LtxA and arthritis development
In the TIRx at-risk cohort, a larger proportion of patients progressing to arthritis was anti-LtxA antibody positive compared to those who did not progress (49% vs. 23 %, p = 0.021). This difference remained significant in univariable Cox regression analysis (HR 2.25, 95% CI 1.20–4.25 p = 0.012) and in multivariable Cox regression adjusted for possible confounders (HR 2.10, 95% CI 1.04–4.20, p = 0.037, Figure 2A). In the Leeds at-risk cohort, anti-LtxA seropositivity was not significantly different between progressors and non-progressors (25% vs. 24%, p = 1.0), and did not associate with arthritis development in Cox regression analysis (HR 0.99, CI 0.60–1.65, p = 0.973, Figure 2B).
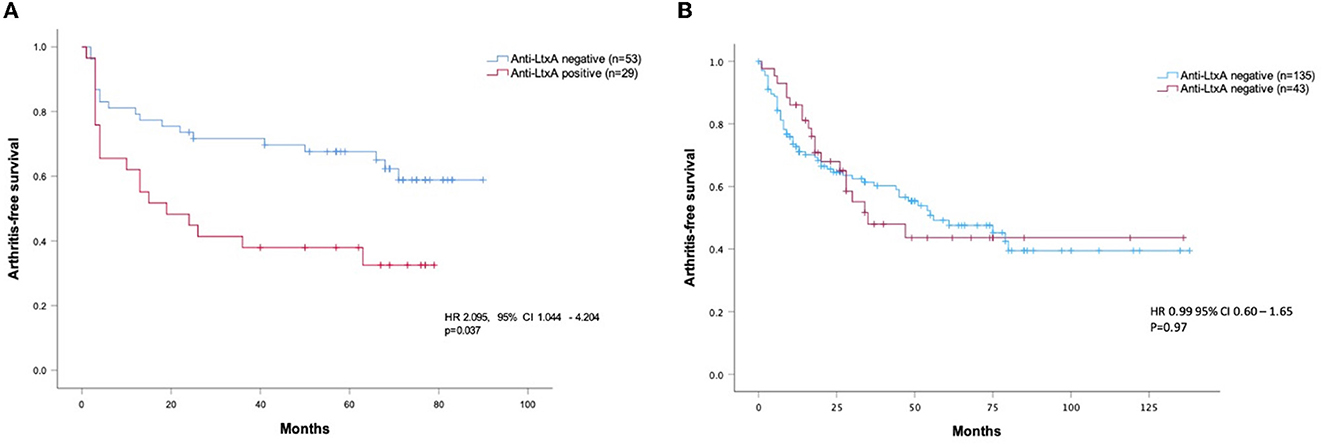
Figure 2. Baseline anti-LtxA levels vs. progression to arthritis in the TIRx cohort [(A) multivariable analysis] and the Leeds cohort [(B) univariable analysis]. Hazard ratio (HR) with 95% confidence interval (CI) in Cox regression adjusted for age, sex, smoking, RF status, ACPA levels, and symptom duration (TIRx only).
Serum anti-LtxA- and RA-related autoantibodies
Both the TIRx cohort and the ACPA-positive Leeds patients were more often anti-LtxA positive compared to the Leeds APCA-negative patients (35% vs. 13%, p = 0.001 and 24% vs. 13%, p = 0.035, respectively, Figure 1). Swedish blood donors (controls) were more often anti-LtxA positive than Leeds ACPA-negative at-risk patients (28% vs. 13%, p = 0.012, Figure 1). In TIRx, where all patients were IgG ACPA-positive, the levels were higher among patients positive for anti-LtxA compared with anti-LtxA negatives, with borderline statistical significance (mean 658 ± 1,007 vs. 334 ± 655 AU/mL; p = 0.073). A borderline significance was also seen in the Leeds cohort, where anti-LtxA positive showed higher IgG ACPA levels compared to anti-LtxA negative (mean 174 ± 149 vs. 133 ± 147 AU/mL, p = 0.068). Serum LtxA did not associate with IgA, IgM, SC ACPA, free SC, or RF status in the TIRx cohort (data not shown).
Serum anti-LtxA and periodontitis
Data on periodontitis were present for a subgroup of the Leeds at-risk cohort, but anti-LtxA positive at-risk patients did not more often suffer from periodontitis compared to anti-LtxA negative at-risk patients (73% vs. 72%, p > 0.9).
Discussion
To reach a better understanding of the possible role of A.a. in RA development and progression, we investigated toxin-neutralizing antibody responses in patients at risk of developing RA. The overall conclusion, from the present and previous studies (3, 9), is that A.a.-related antibody responses, as well as possible links to RA, appear to be substantially influenced by cohort characteristics and/or the context from which they have been recruited. In the Swedish at-risk cohort, we found neutralizing antibodies to A.a. LtxA prognostic for arthritis development among symptomatic ACPA-positive patients also after adjustments for smoking and other possible confounders. However, this association could not be replicated in the UK at-risk cohort despite inclusion criteria and baseline characteristics being very similar. In both at-risk cohorts, there were indications that a humoral response to LtxA associates with ACPA production, which is in agreement with the seminal study in established RA by Konig et al. (3). However, at-risk patients (ACPA-positive) did not have elevated anti-LtxA compared to (ACPA-negative) blood donors, possibly implying that A.a. enhances rather than initiates an ACPA response.
A major strength of this study is the inclusion of patients prior to arthritis onset, which enables proper determination of whether A.a. immunity precedes RA development or not. The use of two independent and geographically distinct cohorts, which resulted in discordant results, highlights that anti-LtxA results cannot readily be extrapolated across populations. There was a slightly lower occurrence of anti-LtxA in the British population compared to the Swedish, but whether or not that reflected a lower prevalence of A.a. or periodontitis could not be investigated in this study. Nevertheless, previous studies show a prevalence of periodontitis of 38% in the UK (20) and 40% in Sweden (21) suggesting that the prevalence of periodontitis does not stand for the slight differences in anti-LtxA ab occurrence between the two at-risk cohorts. Another possible drawback is that we did not specifically address antibody isotypes but instead applied a functional assay to detect anti-LtxA. We believe, however, that given the prevailing hypothesis of LtxA-induced hypercitrullination as a mechanistic link to RA, the total neutralizing capacity of the anti-LtxA antibody response is a relevant readout. We did not examine A.a. presence in the oral cavity, but it was previously reported from the UK at-risk cohort that A.a. DNA abundance was neither increased nor prognostic for arthritis development (20).
To conclude, we found some associations between A.a. and different aspects of RA development and progression. However, the results are not consistent across populations, implying that other features of the oral microbiome should be explored in upcoming periodontitis-related RA research.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by the ethical review board in Linköping, Sweden (Decision No. M220-09, 2017/260-32) and NHS Health Research Authority National Research Ethics Service Committee Yorkshire and the Humber—Leeds West, UK (REC reference: 06/Q1205/169). The patients/participants provided their written informed consent to participate in this study.
Author contributions
AK and AJ conceived and planned the experiments. KMar, CÖ, and AD carried out the experiments. AK and KMar took the lead in writing the manuscript. All authors contributed to the interpretation of the results, provided critical feedback, helped shape the research, analysis, and manuscript.
Funding
This study was supported by the Swedish Society of Medicine, the Swedish Research Council, the Medical Research Council of Southeast Sweden, King Gustaf V's 80-year foundation, the Swedish Rheumatism Association, and the Östergötland County Council. The Leeds CCP study was supported by the National Institute for Health Research (NIHR) Leeds Biomedical Research Centre (grant number: IS-BRC-1215-20015).
Acknowledgments
The authors would like to thank the TIRx patients and controls for their participation and are also grateful to all TIRx colleagues.
Conflict of interest
KMan reports personal fees from AbbVie, Lilly, and UCB AbbVie, outside the submitted work and research grants from Gilead and Lilly. PE reports consultant fees from BMS, AbbVie, MSD, Pfizer, Novartis, and Roche and personal fees from Abbvie, Gilead, Lilly, and Novartis, outside the submitted work and also reports research grants from AbbVie, BMS, Lilly, and Samsung.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Rooney CM, Mankia K, Emery P. The role of the microbiome in driving RA-related autoimmunity. Front Cell Dev Biol. (2020) 8:538130. doi: 10.3389/fcell.2020.538130
2. Eriksson K, Fei G, Lundmark A, Benchimol D, Lee L, Hu YOO, et al. Periodontal health and oral microbiota in patients with rheumatoid arthritis. J Clin Med. (2019) 8:jcm8050630. doi: 10.3390/jcm8050630
3. Konig MF, Abusleme L, Reinholdt J, Palmer RJ, Teles RP, Sampson K, et al. Aggregatibacter actinomycetemcomitans-induced hypercitrullination links periodontal infection to autoimmunity in rheumatoid arthritis. Sci Transl Med. (2016) 8:369ra176. doi: 10.1126/scitranslmed.aaj1921
4. Esberg A, Johansson A, Claesson R, Johansson I. 43-year temporal trends in immune response to oral bacteria in a Swedish population. Pathogens. (2020) 9:544. doi: 10.3390/pathogens9070544
5. Johansson A. Aggregatibacter actinomycetemcomitans leukotoxin: a powerful tool with capacity to cause imbalance in the host inflammatory response. Toxins (Basel). (2011) 3:242–59. doi: 10.3390/toxins3030242
6. Reichert S, Jurianz E, Natalie P, Schlumberger W, Dahnrich C, Johannsen N, et al. Is periodontitis a prognostic factor in order to indicate antibodies against citrullinated peptides in patients with rheumatoid arthritis? Clin Exp Rheumatol. (2020) 38:227–38. doi: 10.55563/clinexprheumatol/9p1bcm
7. Ten Brinck RM, van Steenbergen HW, van Delft MAM, Verheul MK, Toes REM, Trouw LA, et al. The risk of individual autoantibodies, autoantibody combinations and levels for arthritis development in clinically suspect arthralgia. Rheumatology (Oxford). (2017) 56:2145–53. doi: 10.1093/rheumatology/kex340
8. Ziegelasch M, Boman A, Martinsson K, Thyberg I, Jacobs C, Nyhall-Wahlin BM, et al. Anti-cyclic citrullinated peptide antibodies are associated with radiographic damage but not disease activity in early rheumatoid arthritis diagnosed in 2006-2011. Scand J Rheumatol. (2020) 49:434–42. doi: 10.1080/03009742.2020.1771761
9. Gomez-Banuelos E, Johansson L, Konig MF, Lundquist A, Paz M, Buhlin K, et al. Exposure to Aggregatibacter actinomycetemcomitans before Symptom Onset and the Risk of Evolving to Rheumatoid Arthritis. J Clin Med. (2020) 9:jcm9061906. doi: 10.3390/jcm9061906
10. Giles JT, Reinholdt J, Andrade F, Konig MF. Associations of antibodies targeting periodontal pathogens with subclinical coronary, carotid, and peripheral arterial atherosclerosis in rheumatoid arthritis. Arthritis Rheumatol. (2021) 73:568–75. doi: 10.1002/art.41572
11. Brage M, Holmlund A, Johansson A. Humoral immune response to Aggregatibacter actinomycetemcomitans leukotoxin. J Periodontal Res. (2011) 46:170–5. doi: 10.1111/j.1600-0765.2010.01325.x
12. Sjodin B, Arnrup K, Matsson L, Wranne L, Carlsson J, Hanstrom L. Periodontal and systemic findings in children with marginal bone loss in the primary dentition. J Clin Periodontol. (1995) 22:214–24. doi: 10.1111/j.1600-051X.1995.tb00137.x
13. Eloff E, Martinsson K, Ziegelasch M, Cedergren J, Reckner A, Skogh T, et al. Autoantibodies are major predictors of arthritis development in patients with anti-citrullinated protein antibodies and musculoskeletal pain. Scand J Rheumatol. (2020) 2020:1–9. doi: 10.1136/annrheumdis-2019-eular.1644
14. Di Matteo A, Mankia K, Duquenne L, Mahler M, Corscadden D, Mbara K, et al. Third-generation anti-cyclic citrullinated peptide antibodies improve prediction of clinical arthritis in individuals at risk of rheumatoid arthritis. Arthritis Rheumatol. (2020) 72:1820–28. doi: 10.1002/art.41402
15. Rakieh C, Nam JL, Hunt L, Hensor EM, Das S, Bissell LA, et al. Predicting the development of clinical arthritis in anti-CCP positive individuals with non-specific musculoskeletal symptoms: a prospective observational cohort study. Ann Rheum Dis. (2015) 74:1659–66. doi: 10.1136/annrheumdis-2014-205227
16. Garcia-Montoya L, Nam JL, Duquenne L, Villota-Eraso C, Di Matteo A, Hartley C, et al. Prioritising referrals of individuals at-risk of RA: guidance based on results of a 10-year national primary care observational study. Arthritis Res Ther. (2022) 24:26. doi: 10.1186/s13075-022-02717-w
17. Repetto G. del Peso A, Zurita JL. Neutral red uptake assay for the estimation of cell viability/cytotoxicity. Nat Protoc. (2008) 3:1125–31. doi: 10.1038/nprot.2008.75
18. Kastbom A, Roos Ljungberg K, Ziegelasch M, Wetterö J, Skogh T, Martinsson K. Changes in anti-citrullinated protein antibody isotype levels in relation to disease activity and response to treatment in early rheumatoid arthritis. Clin Exp Immunol. (2018) 194:391–99. doi: 10.1111/cei.13206
19. Martinsson K, Roos Ljungberg K, Ziegelasch M, Cedergren J, Eriksson P, Klimovich V, et al. Elevated free secretory component in early rheumatoid arthritis and prior to arthritis development in patients at increased risk. Rheumatology (Oxford). (2020) 59:979–87. doi: 10.1093/rheumatology/kez348
20. Mankia K, Cheng Z, Do T, Hunt L, Meade J, Kang J, et al. Prevalence of periodontal disease and periodontopathic bacteria in anti-cyclic citrullinated protein antibody-positive at-risk adults without arthritis. JAMA Netw Open. (2019) 2:e195394. doi: 10.1001/jamanetworkopen.2019.5394
Keywords: ACPA, Aggregatibacter actinomycetemcomitans, rheumatoid arthritis, progression, periodontitis
Citation: Martinsson K, Di Matteo A, Öhman C, Johansson A, Svärd A, Mankia K, Emery P and Kastbom A (2023) Antibodies to leukotoxin A from the periodontal pathogen Aggregatibacter actinomycetemcomitans in patients at an increased risk of rheumatoid arthritis. Front. Med. 10:1176165. doi: 10.3389/fmed.2023.1176165
Received: 28 February 2023; Accepted: 10 July 2023;
Published: 03 August 2023.
Edited by:
Ioannis Parodis, Karolinska Institutet (KI), SwedenReviewed by:
Johanna Westra, University of Groningen, NetherlandsRyu Watanabe, Osaka Metropolitan University, Japan
Copyright © 2023 Martinsson, Di Matteo, Öhman, Johansson, Svärd, Mankia, Emery and Kastbom. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Klara Martinsson, a2xhcmEubWFydGluc3NvbkBsaXUuc2U=