 Thais Montezuma1Sebastian Vernal2Elaine Nascimento Andrade3Jurema Guerrieri Brandão3,4
Thais Montezuma1Sebastian Vernal2Elaine Nascimento Andrade3Jurema Guerrieri Brandão3,4 Gustavo Laine Araújo de Oliveira3
Gustavo Laine Araújo de Oliveira3 Ciro Martins Gomes4,5*
Ciro Martins Gomes4,5*- 1Health Technology Assessment Unit, Hospital Alemão Oswaldo Cruz, São Paulo, Brazil
- 2LIM-49, Instituto de Medicina Tropical de São Paulo, Universidade de São Paulo, São Paulo, Brazil
- 3Coordenação-Geral de Vigilância das Doenças em Eliminação, Ministério da Saúde do Brasil, Brasília, Brazil
- 4Programa de Pós-Graduação em Ciências Médicas, Universidade de Brasília, Brasília, Brazil
- 5Programa de Pós-Graduação em Patologia Molecular, Universidade de Brasília, Brasília, Brazil
Introduction: The present study aimed to evaluate leprosy cure and relapse rates as primary outcomes related to two additional strategies for leprosy treatment: clofazimine for paucibacillary (PB) leprosy patients and clarithromycin for patients with rifampicin-resistant leprosy.
Methods: We conducted two systematic reviews (protocols CRD42022308272 and CRD42022308260). We searched the PubMed, EMBASE, Web of Science, Scopus, LILACS, Virtual Health Library and Cochrane Library databases, registers of clinical trial databases and gray literature. We included clinical trials evaluating the addition of clofazimine to PB leprosy treatment and the use of clarithromycin for treating patients with rifampicin-resistant leprosy. Risk of bias (RoB) in randomized clinical trials was assessed by the RoB 2 tool and that in non-randomized clinical trials was assessed by the ROBINS-I tool; and the certainty of the evidence was assessed by the Grading of Recommendations Assessment, Development and Evaluation (GRADE) system. A meta-analysis of dichotomous outcomes was performed.
Results: For clofazimine, four studies were included. Cure and relapse rates were not different with the addition of clofazimine to PB leprosy treatment and demonstrated very low certainty of evidence. For clarithromycin, six studies were included. Considerable heterogeneity resulted from the difference between comparators, and studies showed no difference in the assessed outcomes with the addition of clarithromycin to rifampicin-resistant leprosy treatment. Mild adverse events were reported for both drugs but did not significantly impact treatment.
Discussion: The effectiveness of both drugs still needs to be determined. Adding clofazimine to PB leprosy treatment may reduce the repercussions of an incorrect operational classification with no apparent relevant side effects.
Systematic review registration: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42022308272; https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42022308260, identifier: CRD42022308272; CRD42022308260.
1. Introduction
Leprosy is a chronic infectious granulomatous disease caused by Mycobacterium leprae and Mycobacterium lepromatosis that predominantly affects the skin and peripheral nerves (1). Regrettably, leprosy is still one of the most neglected diseases worldwide, impacting more than 120 countries, mainly in underdeveloped settings; more than 200 thousand new cases were reported in 2019 (2). Early diagnosis and treatment are crucial for reducing the burden of this disease and avoiding long-term irreversible consequences such as deformities and mutilations (3, 4).
Although leprosy is one of the oldest known diseases of humankind, effective leprosy treatment only began in 1941 with the discovery of sulfone (5, 6). The historical management of leprosy involved compulsory isolation, leading to permanent social stigma (7). Dapsone toxicity has always been a concern, joined by reports of resistance (8, 9). In this scenario, the World Health Organization (WHO) (5) recruited a group of specialists, called “THELEP.” Despite the lack of proper evidence in those days, the problem was too urgent for a solution to be delayed; thus, in 1981, THELEP recommended multidrug therapy (MDT) (5) to solve the dapsone resistance problem and to make shorter treatment periods possible.
Although new cases are registered annually, the incidence of leprosy has dramatically reduced since the introduction of MDT; however, leprosy persists in some countries with endemic pockets such as Brazil, India and Indonesia. Despite the success of MDT, new challenges still arise (2, 10). Recent reports of rifampicin-resistant M. leprae (11, 12) and the inherent difficulty in properly classifying patients as having the multibacillary (MB) or paucibacillary (PB) forms are also threats to leprosy control (13, 14). Considering the significant gap in the literature, the WHO relies on expert opinions. In 2018, the “Guidelines for the Diagnosis, Treatment and Prevention of Leprosy” (15) recommended the use of clofazimine for patients with PB leprosy and clarithromycin for leprosy cases resistant to rifampicin (Figure 1).
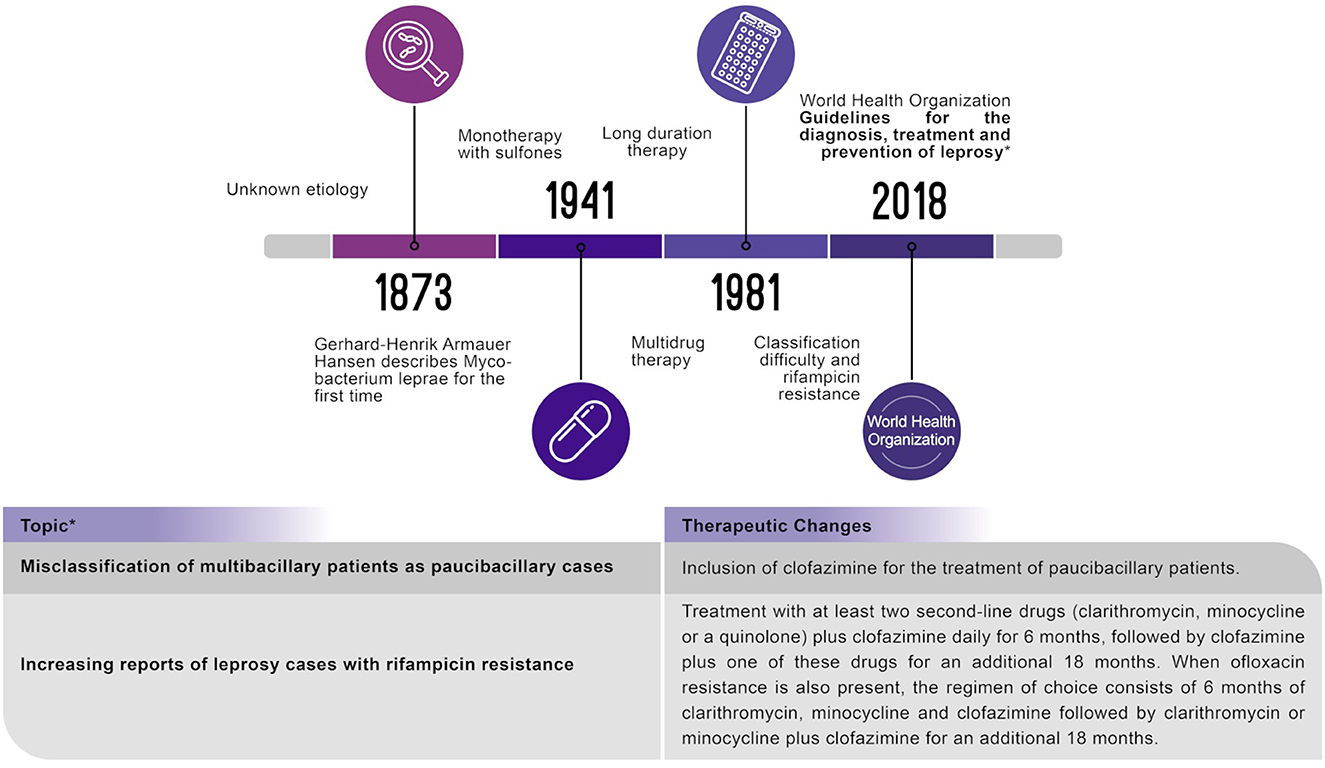
Figure 1. This systematic literature review evaluated clinical pathways and the World Health Organization recommendations.
The present study aimed to evaluate leprosy cure and relapse rates as primary outcomes related to two additional strategies for leprosy treatment: (I) clofazimine for PB leprosy patients and (II) clarithromycin for patients with rifampicin-resistant leprosy. In addition, as secondary outcomes, adverse events bacteriological and morphological index reductions, quality of life and treatment adherence were also assessed.
2. Methods
2.1. Protocol and registration
Two separate review protocols were recorded to analyse the two recent WHO therapeutic recommendations for leprosy treatment. The protocols were registered in the International Prospective Register of Systematic Reviews (PROSPERO): CRD42022308272 (clofazimine review) and CRD42022308260 (clarithromycin review). The reviews strictly followed the recommendations of the Cochrane Handbook for Systematic Reviews of Interventions (16) and were reported following the Reporting Items for Systematic Review and Meta-Analyses (PRISMA) statement (17).
2.2. Eligibility criteria
2.2.1. Population, intervention and comparator studies eligible for the clofazimine review
For the clofazimine review, studies targeting individuals of any age diagnosed with PB leprosy that addressed leprosy treatment using clofazimine in combination with dapsone and rifampicin for 6 months (WHO-PB-MDT) were eligible. For eligibility, dapsone and rifampicin must have been used for 6 months in a comparator group.
2.2.2. Population, intervention and comparator studies eligible for the clarithromycin review
For the clarithromycin review, studies targeting individuals of any age diagnosed with PB or MB leprosy that addressed leprosy treatment with the use of clarithromycin alone or in combination with another drug were eligible. One of the following drug combinations must have been used in a comparator group: dapsone, rifampicin, quinolone, minocycline, clofazimine, ofloxacin and/or sparfloxacin. The presence of rifampicin resistance was assessed by subgroup analysis.
2.2.3. Outcomes and study designs eligible for the clofazimine and clarithromycin reviews
Regarding eligibility, all studies must have evaluated at least one of the following outcomes: efficacy/effectiveness (cure and relapse rates and bacteriological and morphological index reductions), safety (any adverse event or serious adverse event), quality of life or treatment adherence. Eligible study designs included randomized clinical trials (RCTs), non-randomized clinical trials, and observational studies with comparator groups (cohort or case–control studies). Systematic reviews, narrative reviews, experimental animal studies, cross-sectional studies, or case reports were excluded. There were no restrictions regarding the study follow-up time, language or year of publication.
2.3. Sources of information and search strategy
For both reviews, literature searches were conducted on April 1, 2022, in the PubMed, EMBASE, Web of Science, Scopus, LILACS, Virtual Health Library (BVS) and Cochrane Library databases. PubMed, EMBASE and Cochrane Library alerts were set up to provide a weekly update of new literature until August 13, 2022. A search was performed for ongoing studies in clinicaltrials.gov and the International Clinical Trials Registry Platform (ICTRP). The thesis and dissertation databases were manually checked, and gray literature was accessed in the Opengrey.eu database. The reference lists of the relevant studies were searched by the “backwards snowballing” method (Supplementary Tables 1A, 2A, respectively).
2.4. Selection of studies
In both reviews, the references were exported to EPPI-4 (EPPI Centre, London, UK), and duplicates were removed using the automatic tool. The titles and abstracts were screened by two independent reviewers: CG and SV for the clofazimine review and CG and TM for the clarithromycin review. Disagreements were evaluated by a third reviewer: TM or SV. The full texts of the selected studies were evaluated in the same way.
2.5. Data collection process
Data were extracted using a standardized form developed by a leprosy specialist (CG). Two reviewers extracted the data independently, and disagreements were resolved through consensus: GC + TM for the clofazimine review and CG + SV for the clarithromycin review. The extracted information is disclosed in Supplementary material B.
2.6. Risk of bias assessment of the included studies
The risk of bias of RCTs was assessed at the outcome level using the Cochrane 2.0 Risk of Bias tool (RoB 2), and that of non-randomized clinical trials was evaluated using the Risk of Bias In Non-randomized Studies of Interventions (ROBINS-I) tool by two independent evaluators with subsequent consensus (CG and TM).
2.7. Data analysis
Effect sizes are presented as relative risks (RR) for dichotomous outcomes and by the mean difference (MD) for continuous outcomes. Meta-analysis of the dichotomous outcomes was performed using a random-effects model with the Mantel–Haenszel method in Review Manager software version 5.4 (The Cochrane Collaboration, 2020) if at least two comparable studies were identified. Heterogeneity was verified by forest graphs, chi-squared values (p < 0.05) and I2 statistics (>50%). Regression models were used to assess publication bias if at least ten studies were included.
2.8. Analysis of certainty in the final set of evidence
The certainty in the set of evidence was analyzed using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) system (18).
3. Results
3.1. Results of the clofazimine review
3.1.1. Selected studies (clofazimine review)
The database search resulted in 8,841 references (11 RCT registers and 8,830 records identified in the databases, with 4,796 duplicate records removed), and 4,045 titles and abstracts were screened. Ultimately, 65 full texts were analyzed, and four studies were included in the review [eight publications (19–26), with four included in the main study by de Sá Gonçalves et al. (22) identified as a clinical trial for uniform multidrug therapy for leprosy patients in Brazil - U-MDT/CT-BR (21, 24–26)]. The flow chart of the selected studies (Supplementary Figure 1A) and the excluded studies, including the reasons for exclusion (Supplementary Table 3A), are shown in Supplementary material A.
3.1.2. Characteristics of the included studies (clofazimine review)
Three RCTs (19, 20, 22) and one non-RCT (23) were included; three were conducted in India, and one was conducted in Brazil. Four hundred sixty-four participants were included (the study sample size ranged from 40 to 300 patients with PB leprosy) (Table 1). In all studies, the diagnosis followed the criteria recommended by the WHO.
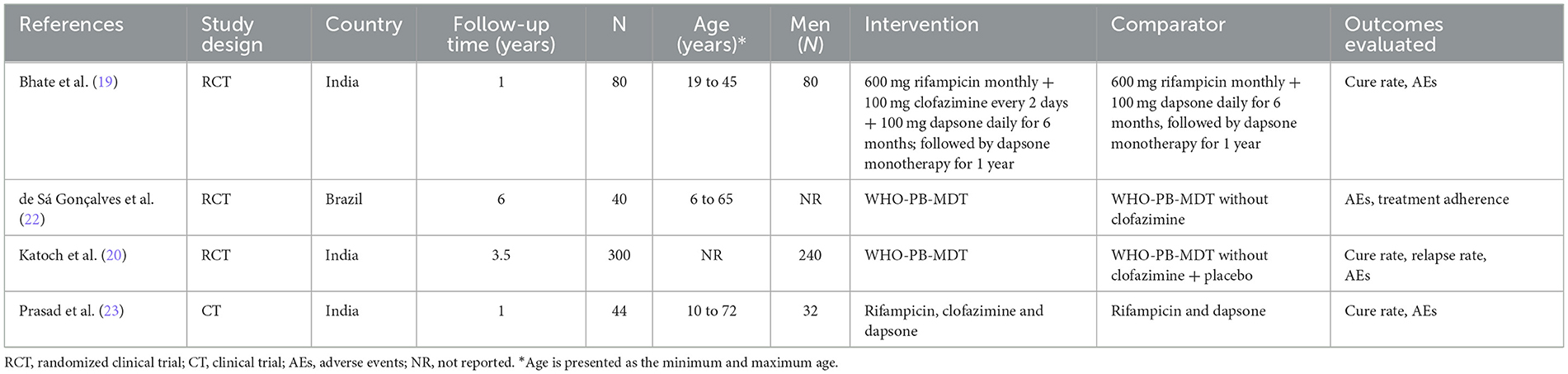
Table 1. Characteristics of the included studies evaluating the use of clofazimine in paucibacillary leprosy treatment.
3.1.3. Risk of bias (clofazimine review)
The studies by Bhate et al. (19) and Katoch et al. (20) were classified as having a high RoB for the cure outcome. The study by Katoch et al. (20) was classified as having a high RoB for the relapse outcome. These studies were evaluated by the RoB 2 tool. The study by Prasad et al. (23) was evaluated by the ROBINS-I tool and was classified as having a serious RoB for the cure outcome. The RoB analysis details are provided in Supplementary material B.
3.1.4. Primary outcomes (clofazimine review)
The cure outcome (clinical inactivity) was assessed in three studies (19, 20, 23) with a 6 month follow-up. The summary effect of the treatment using clofazimine for PB leprosy showed an RR of 1.09 (95% CI: 0.92 to 1.29) compared to that of the control treatment (dapsone and rifampicin). No significant heterogeneity was found. Two studies evaluated the cure outcome within a 12 month follow-up period (19, 23). The summary effect showed an RR of 1.05 (95% CI: 0.78 to 1.40). There was significant heterogeneity among the studies (P-value = 0.04; I2 = 75%) (Figure 2). Relapse was assessed in only one study (20) at a follow-up time between 2.5 and 3.5 years, with an RR of 0.20 (95% CI: 0.01 to 4.13).
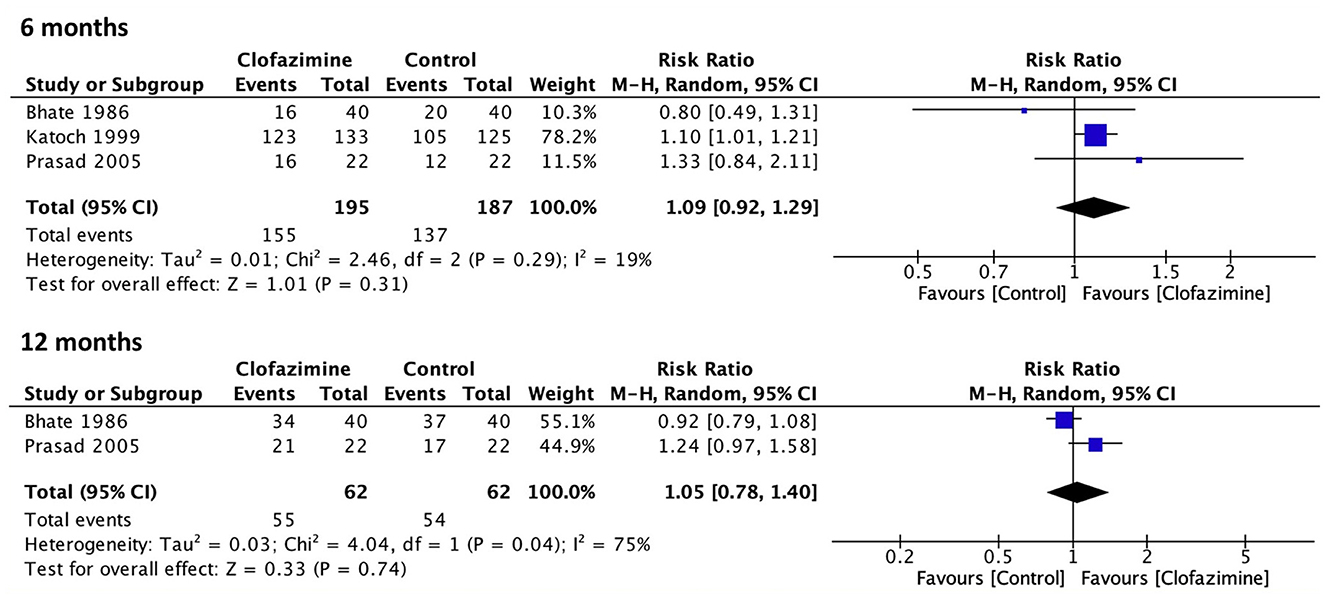
Figure 2. Meta-analysis of the studies evaluating clinical cure events comparing World Health Organization paucibacillary multidrug therapy for leprosy with (clofazimine) or without clofazimine (control) at the 6 and 12 month follow-ups.
3.1.5. GRADE approach (clofazimine review)
The certainty of the body of evidence was evaluated for the cure outcome and classified as having very low certainty. It was impossible to assess publication bias due to the small number of studies. In the same way, for the relapse outcome, it was impossible to assess inconsistency because only one study was included (Supplementary material B).
3.2. Results of the clarithromycin review
3.2.1. Selected studies (clarithromycin review)
The initial screening resulted in 2,133 references (two RCT registers and 2,131 records identified in databases, with 632 duplicate records removed), and 1,501 titles and abstracts were screened. Eleven full texts were evaluated, and six studies were included (27–32). The flow chart of the selected studies (Supplementary Figure 2A) and the excluded studies, including the reasons for exclusion (Supplementary Table 4A), are shown in Supplementary material A.
3.2.2. Characteristics of the included studies (clarithromycin review)
A total of 456 participants were included in six RCTs (27–32), and the sample size ranged from 14 to 300 individuals with MB leprosy. In the study by Ji et al. (29, 30), leprosy was diagnosed through skin smears, and in the other four included studies, the diagnosis was defined following the WHO's recommendations [included individuals with positive acid-fast bacilli and more than ten skin lesions (31)].
3.2.3. Risk of bias (clarithromycin review)
The study by Girdhar et al. (27) was classified as having a high risk of general bias, and the study by Ji et al. (29, 30) was assessed as having some concerns for the “cure” outcome. The study by Girdhar et al. (27) was also classified as having a high RoB for the relapse outcome. The RoB analysis details are provided in Supplementary material B.
3.2.4. Primary outcomes (clarithromycin review)
It was impossible to perform a meta-analysis of any of the outcomes due to the heterogeneity of the intervention arms and follow-up times of the included studies. The characteristics of the individual studies are presented in Table 2. The difference between comparators and the variety of associations made this a complex analysis. Only one study compared a modified MB-MDT substituting 600 mg of rifampicin per month with 2 g of clarithromycin per month vs. a classic WHO MB-MDT at 3 months after the start of therapy (28). Analyses of the cure and relapse outcomes of the included studies are presented in Tables 3, 4, respectively. Data on the cure and relapse outcomes at later times were not available.
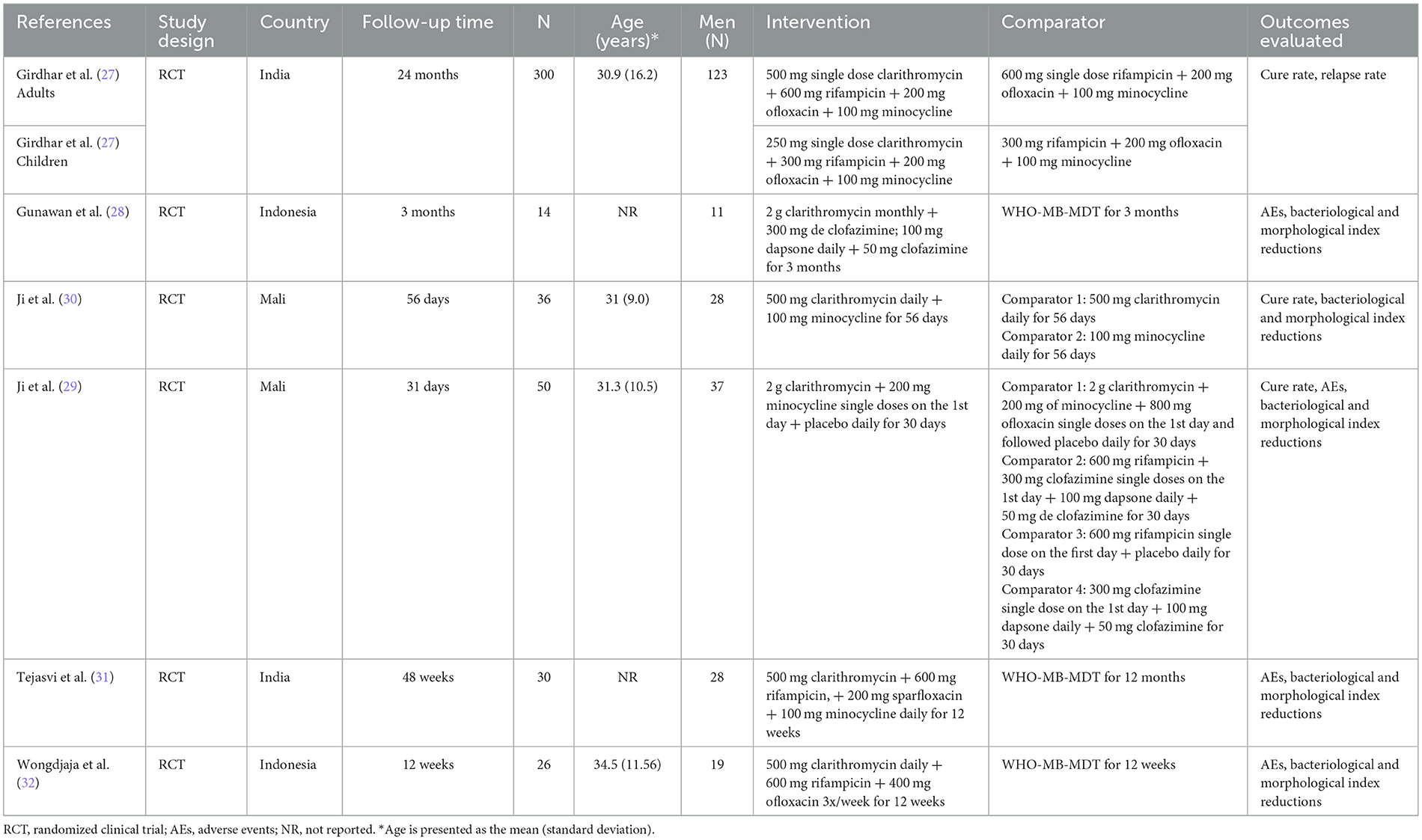
Table 2. Characteristics of the included studies evaluating the use of clarithromycin in leprosy treatment.
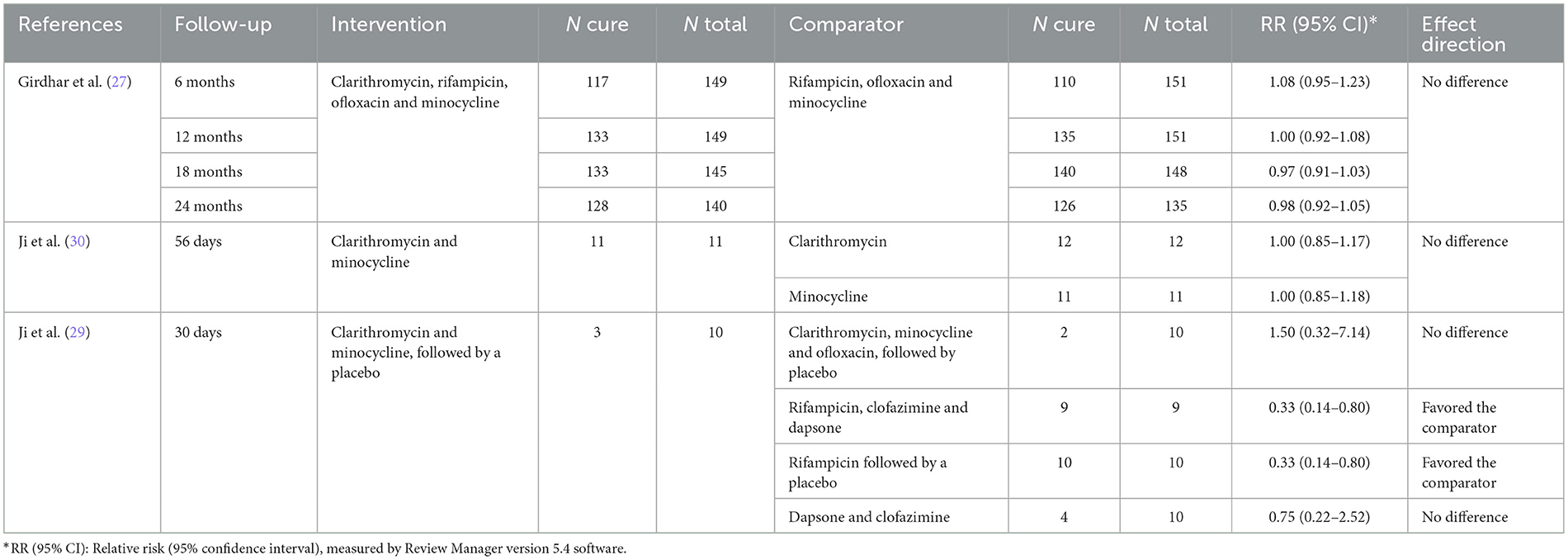
Table 3. Outcome analysis of the inclusion of clarithromycin in multibacillary leprosy treatment in the included studies.

Table 4. Relapse outcome analysis of the inclusion of clarithromycin in multibacillary leprosy treatment in the Girdhar et al. (27) study.
3.2.5. Analysis of certainty in the final set of evidence (clarithromycin review)
Regarding the heterogeneity of the studies, an analysis of the certainty of the evidence was performed, including the individual outcomes of each study, and the set was classified as having very low or low certainty of evidence (Supplementary material B). Downgraded domains of inconsistency and publication bias could not be evaluated.
3.3. Additional outcomes (clofazimine review and clarithromycin review)
Other outcomes, including bacteriological and morphological index reductions, were appraised for both reviews. Various adverse events were reported; nevertheless, these incidents were usually mild and did not significantly impact treatment feasibility. A detailed description of the other secondary outcomes is provided in Supplementary material B.
4. Discussion
The clofazimine and clarithromycin reviews showed no difference in the outcomes with the addition of clofazimine in PB leprosy treatment and the addition of clarithromycin in rifampicin-resistant leprosy treatment. The studies had methodological limitations, and the certainty of the evidence was very low. Thus, there is uncertainty about the new WHO recommendations for leprosy treatment.
Early diagnosis and treatment are among the most critical actions for leprosy control (8, 33). Treatment success depends on proper prescription of PB- or MB-MDT for 6 or 12 months, respectively, with a further distinction between adults and children. In addition, promoting, supervising and guaranteeing treatment adherence and preventing further reinfection, especially through the systematic assessment and follow-up of household contacts, are also crucial for leprosy control. At the end of MDT, clinical and bacilloscopic results are difficult to interpret since patients' reactional states can clinically worsen and bacillus depuration can be slow. Facing these difficulties, the determination of disease persistence or relapse becomes a challenging task for general physicians, making it impossible to rule out treatment failure and making further investigation of antimicrobial resistance mandatory (34).
The long-term MDT duration and the absence of precise criteria for cure evaluation reinforce that the treatment and follow-up of leprosy patients cannot be separated. Owing to the urgency to provide more effective and accessible therapies, in 2018, the WHO recommended the inclusion of clofazimine for PB patients and the inclusion of clarithromycin for patients with rifampicin resistance.
Considering the addition of clofazimine in PB leprosy treatment, the meta-analysis showed no significant difference in the clinical cure rates compared to the control treatment (dapsone and rifampicin) at the 6 and 12 month follow-ups. However, studies were considerably heterogeneous at the second time point. Only one study evaluated relapse (20) rates and showed that after 3.5 years of treatment, the inclusion of clofazimine in MDT for PB leprosy treatment was not different. Other outcomes, including adverse events, treatment adherence and patient satisfaction, were not different between the two types of PB-MDTs (Supplementary material B), and concerns regarding skin discolouration with clofazimine were discarded.
The inclusion of clofazimine has raised controversies and increased the costs of PB leprosy treatment (35). Although different treatment types for PB and MB leprosy still exist, the more similar the drugs are, the smaller the chance of relapse in MB leprosy patients wrongly identified as having PB leprosy. Moreover, the treatment scheme simplification facilitated the logistic distribution since only two types of blister drug packs (adults and children) were needed. Studies that tested a 6 month MB-MDT showed that the cure rate is still relevant in some cases (36), although these results should be interpreted carefully. Indeed, it seems that the incorporation of clofazimine into PB-MDT is safe and may mitigate possible relapses resulting from the sometimes tricky differentiation between PB and MB leprosy (37).
The inclusion of clarithromycin in the leprosy treatment arsenal is an interesting option once this drug is proven to be effective against mycobacteria (29, 38, 39). Even though this alternative focuses on antimicrobial resistance to rifampicin, it can also be an option for WHO-MDT in terms of adverse reactions and drug interactions. Unfortunately, most studies have associated this macrolide with rifampicin, meaning that the role of clarithromycin as a possible replacement for rifampicin still needs to be determined. No differences in the assessed outcomes were observed in the various types of multidrug combinations with clarithromycin. The only study that compared clarithromycin with clofazimine and dapsone vs. WHO-MB-MDT showed no difference in the reduction in the bacteriological index after 3 months of therapy (28). However, only a few patients (seven in each group) were included. No safety or adherence issues were detected in the evaluation of the secondary outcomes.
The RoB evaluation is shown in detail in Supplementary material B. Considerable methodological limitations were found in the studies that evaluated the effectiveness and safety outcomes. These biases can lead to overestimation or underestimation of the effect of the intervention. Although an extensive search of the literature was performed, it was impossible to assess publication bias due to the limited number of studies. The strengths of this review, in addition to the careful literature search, were the rigorous process and the full compliance with a previously registered protocol. Finally, the assessment of the certainty of the body of evidence was performed judiciously using the GRADE approach.
The assessment of the certainty of the evidence for the primary outcomes considering the use of clofazimine in PB leprosy treatment was judged to be very low. A similar judgement was made considering the use of clarithromycin in leprosy patients, with the certainty of evidence classified as very low or low. Given this finding, it is possible to determine that there is little confidence in the effect estimate obtained and that the true effect is probably substantially different from the estimated effect. The results also point to the imprecision of studies available in the literature. Thus, new studies with a good methodological quality and an adequate sample size must be carried out to investigate the effect of the inclusion of clofazimine and clarithromycin in leprosy treatment, as recently recommended by the WHO.
5. Conclusion
The addition of clofazimine to PB leprosy treatment helps reduce the negative impact of misclassification with no additional apparent relevant side effects. Although new articles were published after the 2018 WHO recommendations, the effectiveness of this intervention and the inclusion of clarithromycin to substitute for rifampicin in the WHO-MDT still need to be determined. New clinical trials and investment in pharmacovigilance are essential for elucidating these topics.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Author contributions
TM, SV, and CG: formal analysis, investigation, resources, supervision, validation, visualization, writing—original draft, and writing—review and editing. EA, JB, and GO: formal analysis, investigation, and resources. All authors contributed to the article and approved the submitted version.
Funding
Conselho Nacional de Desenvolvimento Científico e Tecnológico e Ministério da Saúde do Brasil, No. 423596/2021-7, Brazil.
Acknowledgments
We thank all the professionals at the Hospital Universitário de Brasília, Brazil, who are involved in the support of leprosy patients.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2023.1139304/full#supplementary-material
Supplementary material A. Complete search strategy, the flow charts of study selection, and the tables of excluded studies, including the reasons for exclusion for both reviews.
Supplementary material B. Detailed evaluation of all secondary outcomes included in the clofazimine review, clarithromycin review, and certainty of evidence analysis using the GRADE approach.
References
1. Han XY, Sizer KC, Velarde-Félix JS, Frias-Castro LO, Vargas-Ocampo F. The leprosy agents Mycobacterium lepromatosis and Mycobacterium leprae in Mexico. Int J Dermatol. (2012) 51:952–9. doi: 10.1111/j.1365-4632.2011.05414.x
3. Smith CS, Noordeen SK, Richardus JH, Sansarricq H, Cole ST, Soares RC, et al. strategy to halt leprosy transmission. Lancet Infect Dis. (2014) 14:96–8. doi: 10.1016/S1473-3099(13)70365-7
4. Smith WCS, Aerts A. Role of contact tracing and prevention strategies in the interruption of leprosy transmission. Lepr Rev. (2014) 85:2–17. doi: 10.47276/lr.85.1.2
5. World Health Organization. Multidrug Therapy Against Leprosy : Development and Implementation Over the Past 25 Years (2004). p. 179.
6. Faget GH, Pogge RC, Johansen FA, Dinan JF, Prejean BM, Eccles CG. The promin treatment of leprosy. a progress report. Int J Lepr Other Mycobact Dis. (1966) 34:298–310.
7. Sermrittirong S, van Brakel WH. Stigma in leprosy: concepts, causes and determinants. Lepr Rev. (2014) 85:36–47. doi: 10.47276/lr.85.1.36
8. Andrade ESN, Brandão JG, da Silva JS, Kurizky PS, Rosa PS, Araújo WN, et al. A systematic review and meta-analysis of studies on the diagnostic accuracy and screening of tests to detect antimicrobial resistance in leprosy. Diagn Microbiol Infect Dis. (2021) 100:15325. doi: 10.1016/j.diagmicrobio.2021.115325
10. World Health Organization. Weekly Epidemiological Record: Leprosy (2021). p. 421–44. Available online at: https://www.who.int/publications/i/item/who-wer9636-421-444
11. Avanzi C, Maia RC, Benjak A, Nery JA, Sales AM, Miranda A, et al. Emergence of mycobacterium leprae rifampin resistance evaluated by whole-genome sequencing after 48 years of irregular treatment. Antimicrob Agents Chemother. (2020) 64:e00330-20. doi: 10.1128/AAC.00330-20
12. Cambau E, Saunderson P, Matsuoka M, Cole ST, Kai M, Suffys P, et al. Antimicrobial resistance in leprosy: results of the first prospective open survey conducted by a WHO surveillance network for the period 2009-15. Clin Microbiol Infect. (2018) 24:1305–10. doi: 10.1016/j.cmi.2019.01.004
13. Parkash O. Classification of leprosy into multibacillary and paucibacillary groups: an analysis. FEMS Immunol Med Microbiol. (2009) 55:1–5. doi: 10.1111/j.1574-695X.2008.00491.x
14. Pardillo FEF, Fajardo TT, Abalos RM, Scollard D, Gelber RH. Methods for the classification of leprosy for treatment purposes. Clin Infect Dis. (2007) 44:1096–9. doi: 10.1086/512809
15. World Health Organization. Guidelines for the Diagnosis, Treatment and Prevention of Leprosy (2018). p. 87.
16. Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, et al. Cochrane Handbook for Systematic Reviews of Interventions version 6.3 (updated February 2022) (2022).
17. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. (2021) 372:n71. doi: 10.1136/bmj.n71
18. Schünemann H, Brozek J, Guyatt G, Oxman A. GRADE handbook for grading quality of evidence and strength of recommendations. Updated October 2013. The GRADE Working Group (2013).
19. Bhate R, Gupta C, Chattopadhyay S, Singh I. Experience with multidrug therapy in paucibacillary leprosy. Indian J Dermatol. (1986) 58:244–50.
20. Katoch K, Natarajan M, Katoch VM, Singh HB, Bhatia AS. Chemotherapy trial in paucibacillary leprosy using clofazimine. Indian J Lepr. (1999) 71:311–24.
21. da Silva Cruz RC, Bührer-Sékula S, Penna GO, de Moraes MEA, de Sá Gonçalves H, de Araújo Stefani MM, et al. Clinical trial for uniform multidrug therapy for leprosy patients in Brazil (U-MDT/CT-BR): adverse effects approach. An Bras Dermatol. (2018) 93:377–84. doi: 10.1590/abd1806-4841.20186709
22. de Sá Gonçalves H, de Andrade Pontes MA, Bührer-Sékula S, Cruz R, Almeida PC, de Moraes MEA, et al. Brazilian clinical trial of uniform multidrug therapy for leprosy patients: the correlation between clinical disease types and adverse effects. Mem Inst Oswaldo Cruz. (2012) 107:74–8. doi: 10.1590/S0074-02762012000900013
23. Prasad PVS, Babu A, Kaviarasan PK, Viswanathan P, Tippoo R, MDT-MB. therapy in paucibacillary leprosy: a clinicopathological assessment. Indian J Dermatol Venereol Leprol. (2005) 71:242–5. doi: 10.4103/0378-6323.16614
24. de Andrade Pontes MA. Estudo Clínico De Multidrogaterapia Uniforme Para O Tratamento Da Hanseníase No Brasil (U-Mdt/Ct-Br): Estudo Comparativo Dos Efeitos Adversos (2015). p. 104.
25. Ferreira IPS, Buhrer-Sékula S, de Oliveira MRF, Gonçalves H, Pontes MA, Penna MLF, et al. Patient profile and treatment satisfaction of Brazilian leprosy patients in a clinical trial of uniform six-month multidrug therapy (U-MDT/CT-BR). Lepr Rev. (2014) 85:267–74. doi: 10.47276/lr.85.4.267
26. de Sá Gonçalves H. Esquema Único De Tratamento Da Hanseníase: Influências Das Formas Clínicas Nos Efeitos Indesejáveis Dos Fármacos (2010). p. 144.
27. Girdhar A, Kumar A, Girdhar BK. A randomized controlled trial assessing the effect of adding clarithromycin to rifampicin, ofloxacin and minocycline in the treatment of single lesion paucibacillary leprosy in Agra District, India. Lepr Rev. (2011) 82:46–54. doi: 10.47276/lr.82.1.46
28. Gunawan H, Sasmojo M, Putri HE, Avriyanti E, Hindritiani R, Suwarsa O. Clinical pilot study: clarithromycin efficacy in multibacillary leprosy therapy. Int J Mycobacteriol. (2018) 7:152–5. doi: 10.4103/ijmy.ijmy_58_18
29. Ji B, Jamet P, Perani EG, Sow S, Lienhardt C, Petinon C, et al. Bactericidal activity of single dose of clarithromycin plus minocycline, with or without ofloxacin, against mycobacterium leprae in patients. Antimicrob Agents Chemother. (1996) 40:2137–41. doi: 10.1128/AAC.40.9.2137
30. Ji B, Jamet P, Perani EG, Bobin P, Grosset JH. Powerful bactericidal activities of clarithromycin and minocycline against mycobacterium leprae in lepromatous leprosy. J Infect Dis. (1993) 168:188–90. doi: 10.1093/infdis/168.1.188
31. Tejasvi T, Khaitan BK, Khanna N, Pandhi RK, Singh MK. Evaluation of a new fixed duration (12 weeks) multidrug regimen of bactericidal drugs in multibacillary leprosy. Indian J Lepr. (2006) 78:329–37.
32. Wongdjaja H, Junawanto I, Adam HAM, Tabri F, Muhlis. The effectiveness of rifampicin, ofloxacin, and clarithromycin combination therapy in multibacillary leprosy patients. In: The 23rd Regional Conference of Dermatology 2018 SCITEPRESS (2021). (Indonesia). p. 209–13. doi: 10.5220/0008154102090213
33. Frade MAC, de Paula NA, Gomes CM, Vernal S, Bernardes Filho F, Lugão HB, et al. Unexpectedly high leprosy seroprevalence detected using a random surveillance strategy in midwestern Brazil: a comparison of ELISA and a rapid diagnostic test. PLoS Negl Trop Dis. (2017) 11:e0005375. doi: 10.1371/journal.pntd.0005375
34. Andrade ESN, Brandão JG, da Silva JS, Coriolano CRF, Rosa PS, Moraes MO, et al. Antimicrobial resistance among leprosy patients in brazil: real-world data based on the national surveillance plan. Antimicrob Agents Chemother. (2022) 66:e0217021. doi: 10.1128/aac.02170-21
35. Lockwood DNJ, Lambert S, Srikantam A, Darlong J, Pai VV, Butlin CR, et al. Three drugs are unnecessary for treating paucibacillary leprosy—a critique of the WHO guidelines. PLoS Negl Trop Dis. (2019) 13:2–5. doi: 10.1371/journal.pntd.0007671
36. Penna GO, Bührer-Sékula S, Kerr LRS, de Araújo Stefani MM, Rodrigues LC, de Araújo MG, et al. Uniform multidrug therapy for leprosy patients in Brazil (U-MDT/CT-BR): results of an open label, randomized and controlled clinical trial, among multibacillary patients. PLoS Negl Trop Dis. (2017) 11:1–19. doi: 10.1371/journal.pntd.0005725
37. Rodrigues Júnior IA, Gresta LT, de Lourdes Meirelles Noviello M, Cartelle CT, Lyon S, Arantes RME. Leprosy classification methods: a comparative study in a referral center in Brazil. Int J Infect Dis. (2016) 45:118–22. doi: 10.1016/j.ijid.2016.02.018
Keywords: leprosy, meta-analysis, drug resistance, microbial, GRADE approach, systematic review
Citation: Montezuma T, Vernal S, Andrade EN, Brandão JG, de Oliveira GLA and Gomes CM (2023) Effectiveness and safety of multidrug therapy containing clofazimine for paucibacillary leprosy and clarithromycin for rifampicin-resistant leprosy: a systematic review and meta-analysis. Front. Med. 10:1139304. doi: 10.3389/fmed.2023.1139304
Received: 06 January 2023; Accepted: 11 April 2023;
Published: 10 May 2023.
Edited by:
Veronica Schmitz, Oswaldo Cruz Foundation (Fiocruz), BrazilReviewed by:
Pugazhenthan Thangaraju, All India Institute of Medical Sciences Raipur, IndiaHanlin Zhang, Peking Union Medical College Hospital (CAMS), China
Copyright © 2023 Montezuma, Vernal, Andrade, Brandão, de Oliveira and Gomes. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ciro Martins Gomes, Y2lyb2dvbWVzQHVuYi5icg==