 Antonella Adinolfi1*
Antonella Adinolfi1* Silvia Sirotti2
Silvia Sirotti2 Garifallia Sakellariou3,4
Garifallia Sakellariou3,4 Edoardo Cipolletta5
Edoardo Cipolletta5 Emilio Filippucci5
Emilio Filippucci5 Francesco Porta6
Francesco Porta6 Anna Zanetti7
Anna Zanetti7 Nicola Ughi1,7
Nicola Ughi1,7 Piercarlo Sarzi-Puttini2,8
Piercarlo Sarzi-Puttini2,8 Carlo Alberto Scirè7,9
Carlo Alberto Scirè7,9 Helen Keen10
Helen Keen10 Carlos Pineda11
Carlos Pineda11 Lene Terslev12Maria Antonietta D’Agostino13
Lene Terslev12Maria Antonietta D’Agostino13 Georgios Filippou2
Georgios Filippou2- 1Rheumatology Division, Multispecialist Medical Department, ASST Grande Ospedale Metropolitano Niguarda, Milan, Italy
- 2IRCCS Ospedale Galeazzi – Sant’Ambrogio, Rheumatology Department, Milan, Italy
- 3Department of Internal Medicine and Therapeutics, Università di Pavia, Pavia, Italy
- 4Istituti Clinici Scientifici Maugeri IRCCS, Pavia, Italy
- 5Rheumatology Unit, Department of Clinical and Molecular Sciences, Polytechnic University of Marche, Ancona, Italy
- 6Interdisciplinary Pain Medicine Unit, Rheumatology Section, Santa Maria Maddalena Hospital, Rovigo, Italy
- 7SIR Epidemiology, Research Unit, Milan, Italy
- 8Department of Biomedical and Clinical Sciences, Università degli studi di Milano, Milan, Italy
- 9School of Medicine, University of Milano Bicocca, Milan, Italy
- 10Medicine and Pharmacology Department, The University of Western Australia, Murdoch, Perth, WA, Australia
- 11Rheumatology Department, Instituto Nacional de Rehabilitacion, Mexico, Mexico
- 12Center for Rheumatology and Spine Diseases, Rigshospitalet, Copenhagen University, Copenhagen, Denmark
- 13Rheumatology, Fondazione Policlinico Universitario “Gemelli”, IRCCS, Rome, Italy
Objectives: To identify the prevalence of calcium pyrophosphate crystal deposition (CPPD) using ultrasound and conventional radiology at peripheral joints in patients with suspected or definite CPPD.
Methods: A systematic literature search was performed in PubMed and Embase using pre-defined search strategies from inception to April 2021 to identify studies that evaluated conventional radiology and ultrasound in detecting CPPD at peripheral joints, including definite or suspected CPPD [Research question 1 (RQ1) and Research Question 2 (RQ2), respectively]. For the meta-analysis, the first, second, and third sub-analysis included studies with the knee, and knee or wrist as the index joint for CPPD (without restrictions on the reference standard) and synovial fluid analysis or histology as a reference standard (without restrictions on the index joint), respectively.
Results: One-thousand eight hundred and twenty-seven manuscripts were identified, of which 94 articles were finally included. Twenty-two and seventy-two papers were included in RQ1 and RQ2, respectively. The knee had the highest prevalence for RQ1 and RQ2 by both conventional radiology and ultrasound, followed by the wrist with the highest prevalence for RQ1. The hand had the lowest CPPD prevalence. The third sub-analysis showed a higher CPPD prevalence on ultrasound than conventional radiology at the knee (only data available).
Conclusion: Among all peripheral joints, the knees and wrists could be regarded as the target joints for CPPD detection by imaging. Furthermore, ultrasound seems to detect a higher number of calcium pyrophosphate deposits than conventional radiology, even when using a more restrictive reference standard.
Introduction
Calcium pyrophosphate deposition (CPPD) is a chronic arthropathy caused by the presence of calcium pyrophosphate (CPP) deposits in articular and periarticular tissues (1). Although the exact incidence and prevalence of CPPD are still unknown, it is considered one of the most common chronic arthropathies (2), characterized by a prevalence that increases with age (3) and can reach up to 13% in the elderly, depending on the assessed joints and the tool used (4). In fact, one of the main issues for epidemiological studies on CPPD is related to the challenges regarding diagnosis.
For a long time, CPPD diagnosis was based on McCarty Criteria, which required both the identification of CPP crystals in synovial fluid analysis (SFA) and the presence of typical calcifications in conventional radiography (CR) for a “definite” diagnosis, while a “probable” diagnosis was defined by SFA or CR positive findings (5). In 2011, a panel of experts from the European League against Rheumatism (EULAR) changed this status. Experts stated that the presence of CPP crystals in the SFA was sufficient for a definite diagnosis. Furthermore, ultrasonography (US) has been endorsed for the first time as a promising tool for CPPD diagnosis (6).
Since then, growing interest in the use of imaging in CPPD has led to an improved definition of the framework for CPPD diagnosis. In particular, US application in CPPD management has been highly improved since its development by the CPPD subgroup of the OMERACT US Working group of a new set of US definitions for CPPD identification (7, 8), which demonstrated the reliability and accuracy of CPPD diagnosis (8–10). A recent systematic literature review (SLR) evaluated the diagnostic performance of CR and US in CPPD diagnosis, showing that both obtained good results with better sensitivity for US and slightly greater specificity for CR (11). Furthermore, an international working group composed of rheumatologists and musculoskeletal radiologist experts in microcrystalline arthritis has recently developed definitions for CPPD identification by CR, which were also assessed for reliability and accuracy, confirming the high specificity of CR for CPPD identification (12, 13).
Accounting for all, the use of imaging is gaining a leading role in CPPD diagnosis and potentially for follow-up in daily practice. However, given the wide range of CPPD joint involvement, it is particularly important to adopt a time-saving approach for US examination by assessing only the most frequently affected peripheral joints, thus increasing the effectiveness and feasibility. The identification of a minimum set of joints could also promote the application of a scoring system, which could be very useful in monitoring the evolution of CPPD.
Thus, the objective of this study was to perform a SLR to estimate the prevalence of CPPD, identified using CR, US or both at the peripheral joints of patients with a suspected or definite CPPD diagnosis, and to establish the most relevant joints for CPPD diagnosis and monitoring.
Methods
The Preferred Reporting Items for Systematic Reviews and Meta-analyzes (PRISMA 2020) guidelines for reporting systematic reviews and meta-analyzes were followed for this review (14).
A protocol defining all phases of this SLR (research questions, search strategy, and inclusion/exclusion criteria for the articles and methods for the analysis) was developed before the beginning of the study and was registered on the PROSPERO platform (Registration Number: CRD42020218155).
Structured search strategy
Two research questions were developed; the first aimed to assess the CPPD prevalence in peripheral joints based on imaging of patients with a definite, crystal proven, CPPD diagnosis [Research Question 1 (RQ1)], and the second one aimed to assess the prevalence of CPP deposits, based on imaging, in patients with suspicion of CPPD diagnosis according to clinical picture [Research Question 2 (RQ2)].
After defining the research questions, the patient, intervention, comparator, outcome (PICO) framework was used to develop the search strategy (15).
PubMed and Embase databases were searched from inception until April 2021. An additional hand search of articles’ references was performed to include as many eligible articles as possible. The search strategy was based on both MeSH terms and free text and is illustrated in the Supplementary material S1 (SP1).
Study selection and data extraction
The search included all the studies that evaluated the use of CR and/or US for detecting calcifications at the level of at least one peripheral joint [hand, wrist, elbow, shoulder, acromioclavicular (AC), hip, knee, ankle, foot] in adult patients with suspected or definite CPPD, without any restrictions on the reference test used for diagnosis.
The following study types were eligible for inclusion: cross-sectional case–control, cross-sectional cohort, longitudinal case–control, longitudinal cohort, retrospective cohort, and retrospective case–control. Case reports, case series, congress abstracts, and studies written in languages other than English were excluded.
The titles and abstracts of the retrieved references were screened by six reviewers (AA, EC, EF, GF, FP, and SS) according to pre-defined inclusion and exclusion criteria based on the PICOs. The reviewers worked in pairs to assess the abstracts, and discordant assessments were resolved by consensus.
Relevant full-text articles were evaluated by the same reviewers, and data were extracted using a standardized extraction form. Discordant assessments between the authors were resolved by consensus. Data were extracted using a standardized form, including author, publication year, study type, index test, reference test, inclusion criteria, and number of patients (cases and controls). The data on the frequency of calcifications are summarized in ad hoc tables.
For each article, data on the prevalence of calcifications were collected separately for every peripheral joint, according to the imaging technique applied. If available, data on the involvement of single joint structures (fibrocartilage, hyaline cartilage, tendons) were also retrieved. The frequency of involvement was assessed separately for every joint and according to the imaging techniques used. For each joint and structure, data of monolateral or bilateral involvement of calcifications were collected, divided according to the imaging tool. In case of missing laterality data, they were categorized as unknown.
Assessment of the risk of bias
The risk of bias of the selected studies was assessed using ad hoc instruments applied according to the type of article evaluated. For the diagnostic study, we used the modified version of the Quality Assessment of Diagnostic Accuracy Studies (QUADAS-2) tool (16), while and the Newcastle Ottawa Scale (NOS) was used for the assessment of case–control and cohort studies (17). Data extraction and quality assessment were performed by a single reviewer (EC) and checked by a second reviewer (SS). Any disagreements were resolved by consensus.
Data analysis
Descriptive analyzes and meta-analyzes were performed on the included studies. The descriptive analysis aimed to capture the global prevalence of CPPD in different joints. Except for a relevant degree of variability in the included studies regarding the index joints, reference standards, and imaging techniques, specific meta-analyzes were scheduled to collect as much data as possible from homogenous studies. Thus, the following analyzes were performed:
• Descriptive analysis including all studies: Evaluation of CPP deposit prevalence for each joint assessed. All analyzes were divided according to the research question and the imaging method used. If available in the text, the frequency of bilateral involvement at each anatomical site was also provided.
• Descriptive analysis including all studies: evaluation of CPP deposit prevalence at the level of the anatomical structures of a single joint. All analyzes were divided according to the research question and the imaging method used. If available, the frequency of bilateral involvement was also provided.
• Sub-analysis 1 (SB_1) included only studies that used the knee as the index joint for CPPD diagnosis, independent of the reference standard used. All analyzes were divided according to the research question and the imaging method used.
• Sub-analysis 2 (SB_2) included studies that used the knee or wrist as the index joint for CPPD diagnosis, independent of the reference standard used. All analyzes were divided according to the research question and the imaging method used.
• Sub-analysis 3 (SB_3) included only studies that used SFA alone (not the McCarty criteria) or histology as a reference standard for the diagnosis of CPPD independently from the index joint and imaging method used. All analyzes were divided according to the research question and the imaging method used.
SB_1 and SB_2 aimed to assess the impact of the index joint, and SB_3 aimed to assess the impact of the reference test on CPP deposit prevalence.
Statistical analysis
The descriptive analyzes were provided as the ratio between the imaging-positive cases and all the cases evaluated (either for the joint or the single articular structure). The results were also presented as percentages. About the bilateral assessment, the results were obtained evaluating all the imaging cases bilaterally positive and the cases evaluated bilaterally (shown in the text as ratios and percentages).
For the sub-analysis, 162 meta-analyzes were performed, one referring to each research question, sub-analysis, and joint analysis. Only meta-analyzes that included at least three studies were considered and presented in this paper. Information on the proportion of participants with CPP deposits in different joints was extrapolated from each study. Pooled estimates [with related 95% confidence intervals (CI)] were calculated using both fixed- and random-effects models. Heterogeneity was calculated using the I2 index and was high in all analyzes. For this reason, only pooled estimates from random-effects models were reported in the results section. The results were graphically presented using forest plots. All analyzes were performed using the R statistical software (Foundation for Statistical Computing, Vienna, Austria).
Results
Description of the studies
The search strategy identified 1827 records, 1822 from the databases, and five manually searched records (329 duplicates). Of the remaining 1,498 records, 954 were excluded based on their titles and abstracts, and 544 articles entered the full-text evaluation. Considering that 49 full texts were not retrievable (all articles were published before the 1970s), the detailed review included 494 articles. A total of 400 studies were excluded after reviewing the full text, most of which were rejected due to the study type, mainly case reports and case series, followed by outcome. Finally, 94 studies were included in the analysis.
All phases of the selection process are summarized in the Prisma Flow Chart (Figure 1).
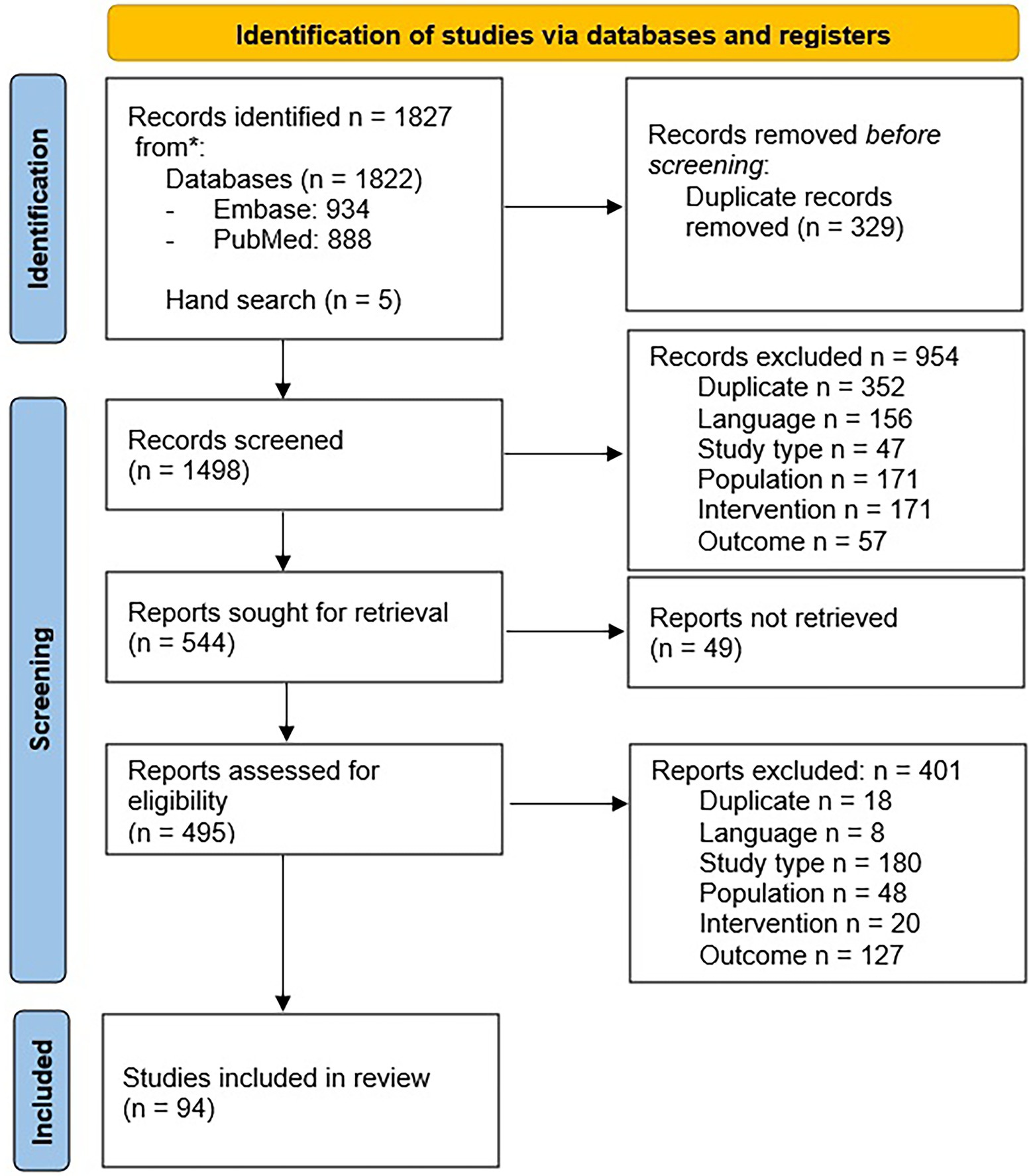
Figure 1. PRISMA 2020 flow diagram for systematic reviews.
For RQ1, 22 papers (18–39) were included, with a total population of 1,425 patients, 876 cases, and 549 controls. One study satisfied both research questions (34), including 16 patients with a definite CPPD diagnosis and 27 with a suspected diagnosis, using CR as either an index or a reference test.
The imaging technique used to detect the calcific deposits was CR alone in 10 articles (19, 29, 31–38) and US in four articles (23, 25–27), while eight papers evaluated both CR and US (18, 20–22, 24, 28, 30, 39). The reference standards were the McCarty Criteria in 12 articles (19–26, 29, 35, 36, 39), and SFA and CR alone in two (30, 38) and six (27, 31–34, 37)papers, respectively.
In RQ2, 72 articles were included (34, 40–110) with a total population of 30,480 patients, 3,027 cases, and 27,453 controls.
The imaging technique applied for the calcifications was CR in 61 papers (2, 38–53, 55–57, 59–63, 68–78, 80–88, 91–96, 98–107) and US alone in six studies (56, 60, 66, 68, 92, 110), while in four articles both imaging techniques (67, 69, 81, 99) were used. The reference standard applied for CPPD diagnosis was CR in 53 articles (34, 40, 41, 43, 45, 47–51, 53–55, 57–59, 61–65, 70–78, 80, 82–85, 87–90, 93, 94, 96–98, 100–105, 107–109), the McCarty criteria were used in five papers (42, 44, 46, 60, 95), US in four (56, 66, 69, 92) and SFA in eight studies (52, 68, 79, 81, 91, 99, 106, 110). Finally, only two articles used histology as reference standard (67, 86).
Considering both RQ1 and RQ2, the most assessed joint was the knee included in 74 papers (18, 19, 25–27, 29, 30, 33–35, 37–40, 42–51, 54–56, 58–76, 78, 80–85, 87–91, 93–102, 105–110), mainly as a single joint examined (39/72 papers), followed by the wrist included in 43 papers (19–21, 25, 32–37, 40, 42, 44–47, 51, 53, 56, 57, 59, 61, 69–73, 82, 83, 85, 87, 93, 95–97, 100, 102–105, 107, 108, 110) and the hip in 18 studies (22, 35, 37, 40–42, 45, 46, 59, 73, 77, 78, 85–87, 97, 102, 107), while the less included was the AC, evaluated only in four articles (31, 35, 92, 94). The characteristics of all included studies are summarized in Table 1, and all the data of each article assessed are summarized in SP2.

Table 1. Characteristics of the articles entered in the SLR.
Frequency of involvement of peripheral joints
Calcifications at imaging-descriptive results
Regarding RQ1, the wrist showed the highest CPP deposit prevalence, i.e., 92% (158/171) at US and 70% (240/343) at CR. A slightly lower prevalence was reported for the knee, i.e., 88% (146/166) at US and 62% (211/388) at CR. Regarding the other joints, the hip had the 65% (84/130) of deposit prevalence at CR and 90% (45/50) at US, while the prevalence at CR was 44% (34/77) and 31% (34/111) for elbow and shoulder, respectively. The lowest values were reported for the hand, with 19% (23/123) at CR and 9% (4/42) at US. Data on the laterality of joint involvement are not available for all the joints. The highest bilateral involvement was observed in the knee and wrist, with values of 86% (83/96) and 73% (49/67), respectively.
For RQ2, the knee was the joint with the highest CPPD prevalence, i.e., 85% (2,342/2770) and 93% (235/254) on CR and US, respectively, followed by the wrist with values that vary from 51% (492/955) at CR to 38% (27/80) at US. Considering only the sites assessed on a larger number of patients (>100), the hip and shoulder had a prevalence of CPP deposits equalling 36% (312/873) and 47% (68/143) on CR, respectively, while the hand showed the lowest prevalence, i.e., 14% (90/591) at CR. Bilateral involvement, mainly evaluable on CR, was higher in the wrist, knee, and hip, with values of 66% (203/309), 65% (641/985), and 50% (97/194), respectively.
All the descriptive results regarding joint involvement are summarized in Table 2.
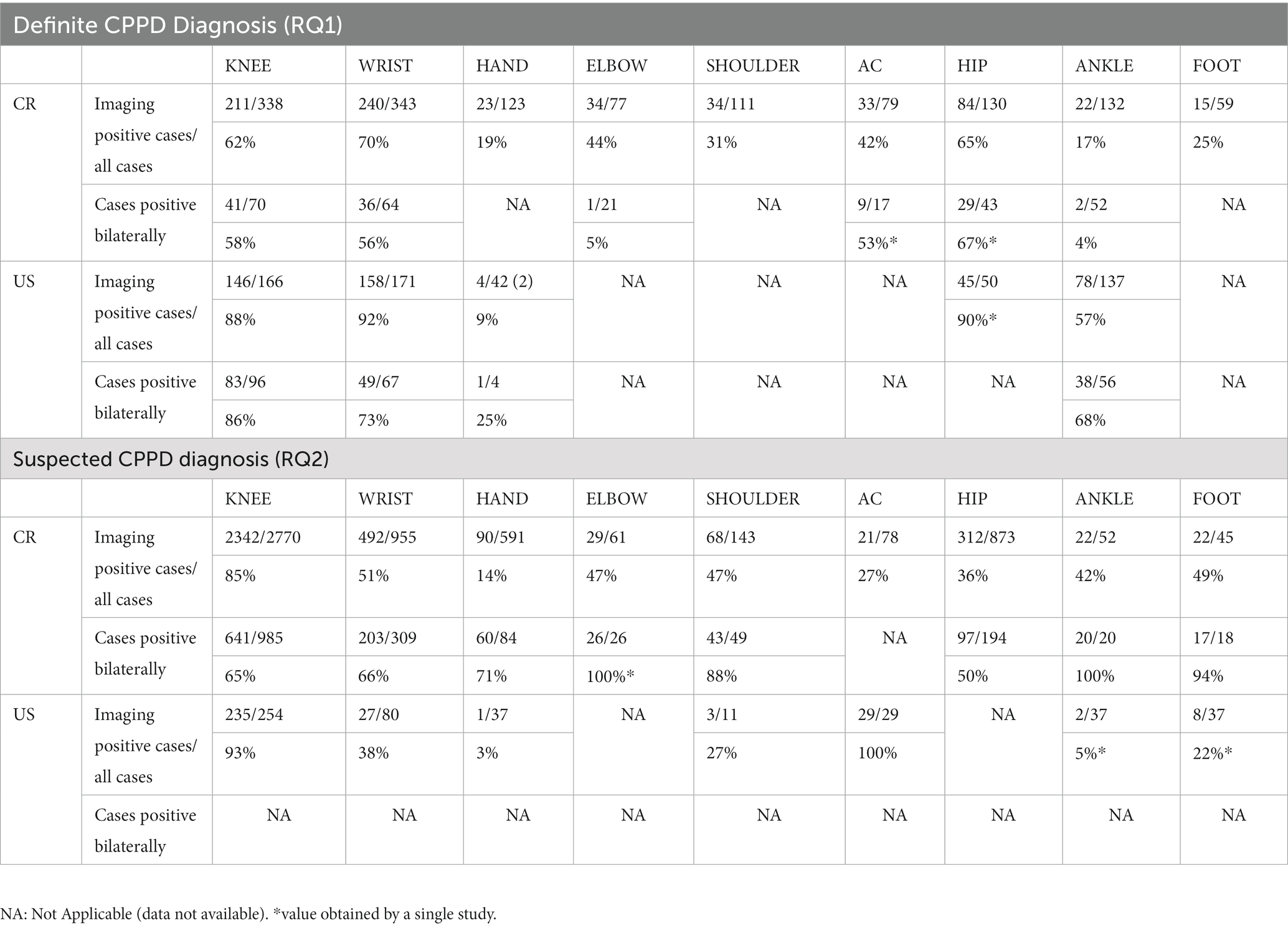
Table 2. Calcifications prevalence at level of each joint assessed: overall results.
Frequency of involvement of the joint structures
Among the studies of RQ1, the joint structures characterized by the highest prevalence of calcific deposits were the menisci, i.e., 90% (67/74) on US, and 59% (172/292) on CR, followed by the triangular fibrocartilage of the wrist (TFC), 56% (70/126) and 47% (139/293) at US and CR, respectively; the knee hyaline cartilage, 66% (94/143) and 33% (80/242)at US and CR, respectively; and the hip fibrocartilage, 50% (45/90) on US 38% (32/85) on CR. Regarding laterality, some results were available for TFC, characterized by bilateral involvement of up to 87% (27/31) on CR and 67% (47/70) on US.
For RQ2, the values were higher for the TFC, followed by the menisci and hyaline cartilage, but only on US (30, 24, and 15%, respectively), while the results were lower at CR (5, 9, and 6%, respectively). Regarding laterality, higher bilateral involvement was recorded for the menisci at CR (28%).
All results regarding CPPD prevalence of joint structures and laterality are shown in SP3.
Meta-analysis
In the SB_1, 73 articles (18, 19, 25–27, 29, 30, 33, 35, 37–40, 42–51, 54–56, 58–76, 78, 80–85, 87–91, 93–102, 105–110) (12 RQ1/61 RQ2) were included; 83 (18–21, 25–27, 29, 30, 32–40, 42–51, 54–56, 58–76, 78, 80–85, 87–91, 93–110) in the SB_2 (18 RQ1/65 RQ2); 14 papers (18, 28, 30, 38, 52, 67, 68, 79, 81, 86, 91, 99, 106, 110) (4 RQ1/10 RQ2) in the SB_3.
For RQ1, for both SB_1 and SB_2, the knee had an overall prevalence of 0.85 [0.62–0.95] with a higher value for US with respect to CR [0.93 (0.68–0.99) and 0.79 (0.44–0.95), respectively]. Regarding the wrist, the prevalence changed between SB_1 and SB_2. In fact, in SB_1, the overall CPP prevalence was 0.72 [0.47–0.88] with a lower value at CR 0.64 [0.39–0.83] and no data available in the US, while in SB_2 the overall prevalence was 0.87 [0.74–0.94], but the prevalence was higher for the US with respect to CR [0.92 (0.87–0.96) and 0.83 (0.61–0.94), respectively]. Decreasing overall prevalence values have been reported for the shoulders, ankles, and hands. The last was the joint characterized by the lowest result. Insufficient data were available for the other sites and SB_3.
With respect to RQ2, the knee had the highest prevalence without any differences between SB_1 and SB_2 and the imaging technique applied [overall value 0.98 (0.96–0.99), US 0.98 (0.88–1.00), CR 0.98 (0.96–0.99)]. Considering the wrist, the overall prevalence in SB_2 was 0.56 [0.45–0.66], with a greater prevalence on CR than on US [0.58 (048–0.68) and 0.33 (0.13–0.63) respectively]. For the other joints, the overall prevalence varied from 0.41 (0.10–0.81) for the elbow to 0.18 (0.11–0.29) for the hand. Considering SB_3, the data were available only for the knee, showing a higher prevalence when US was applied [overall value 0.87 (0.62–0.97), US 0.98 (0.75–1.00), CR 0.63 (0.35–0.84)].
The results of the meta-analysis are summarized in Table 3. Forest Plots of the knees are shown in Figures 2–5. Forest plots of the other joints are shown in SP4.
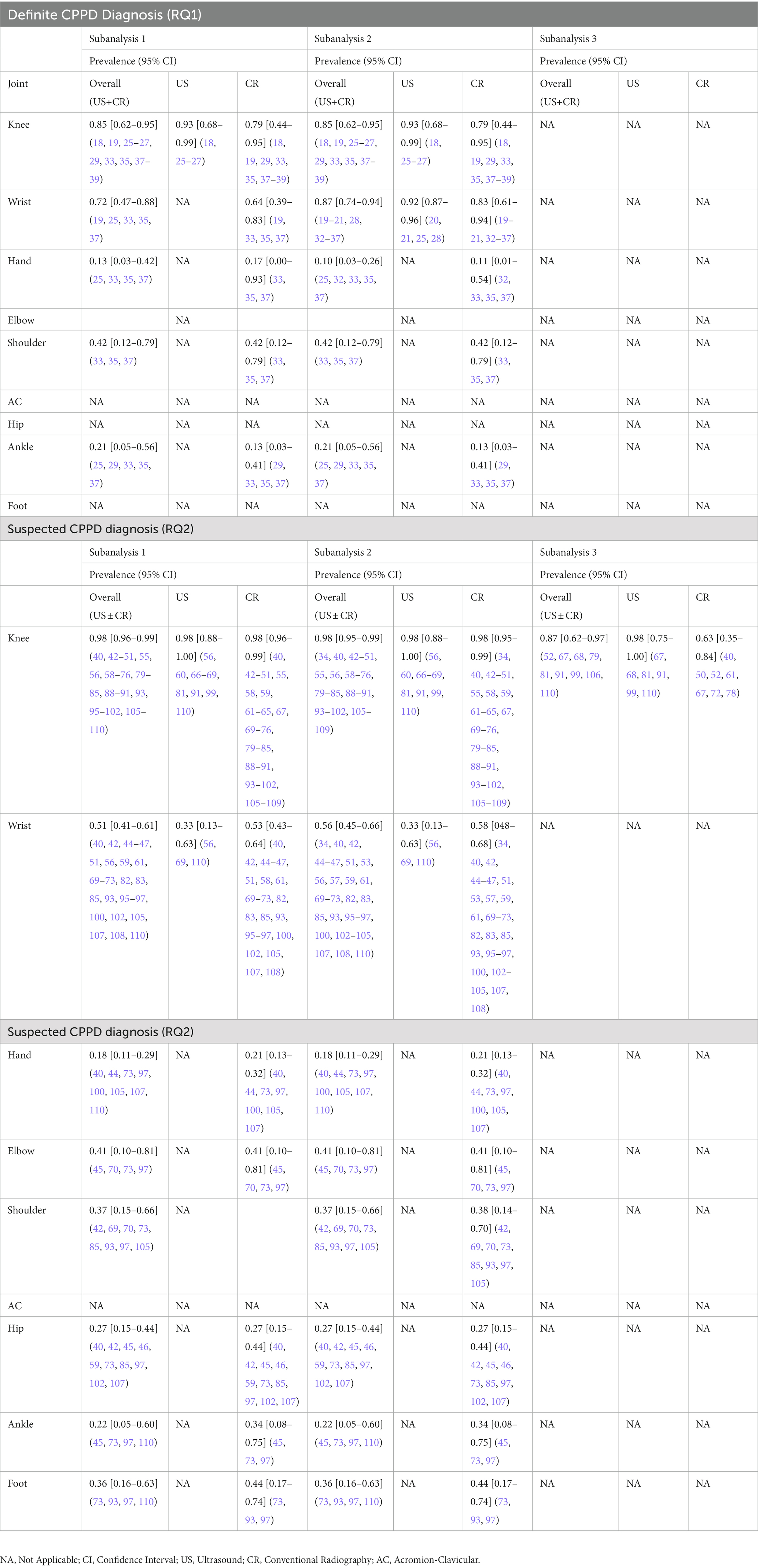
Table 3. Meta-analyzes results.
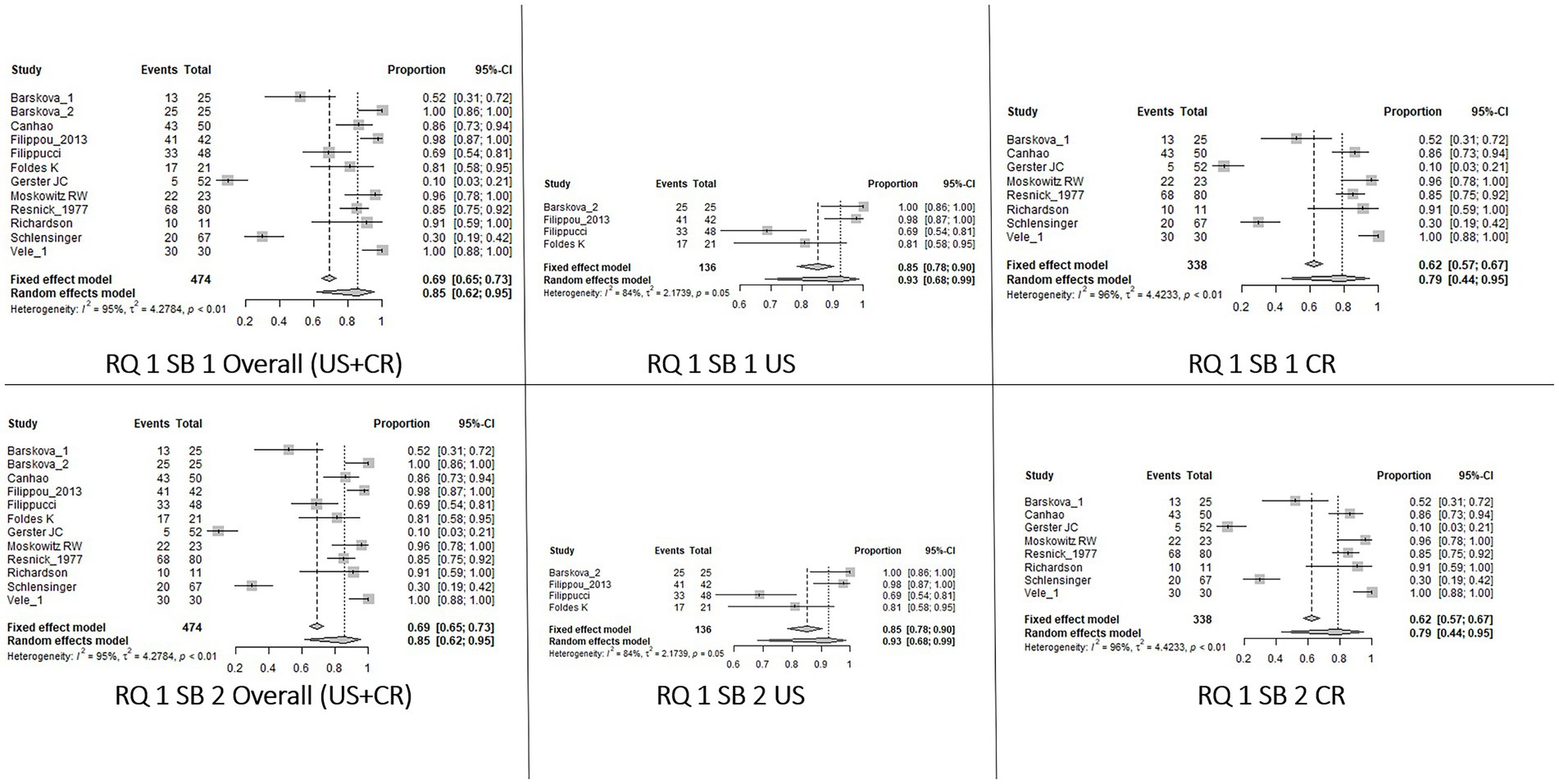
Figure 2. Forest Plot Knee, Research question 1 (RQ1), Sub_analysis 1 and 2: patients with definite diagnosis of CPPD and knee as index joint (SB_1) or knee and/or wrist (SB2) analyzed by imaging.
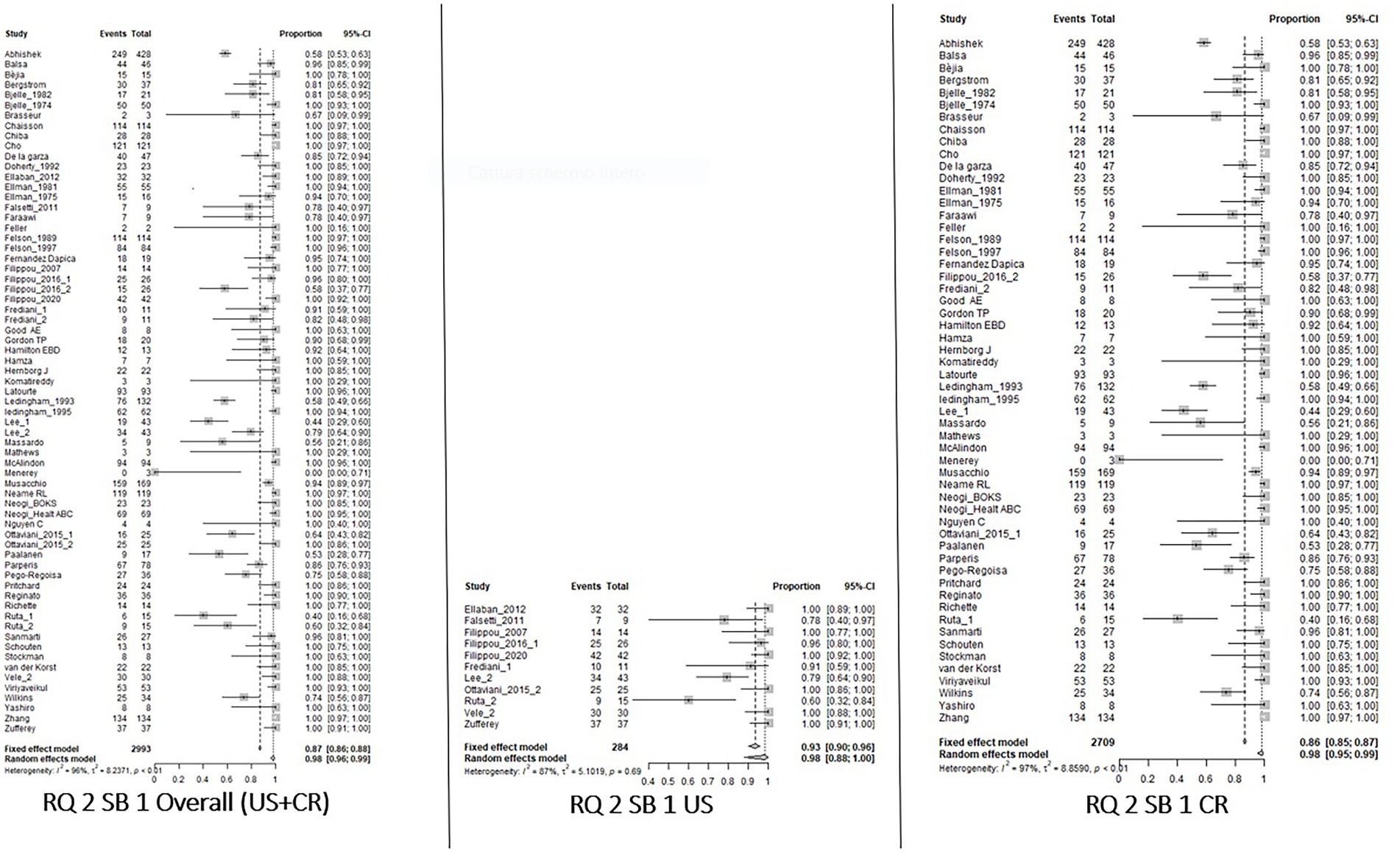
Figure 3. Forest Plot Knee, Research Question 2 (RQ 2), Sub_analysis 1: patients with suspected CPPD and the knee joint used as index joint, independently of the reference standard used for diagnosis, analyzed by imaging.
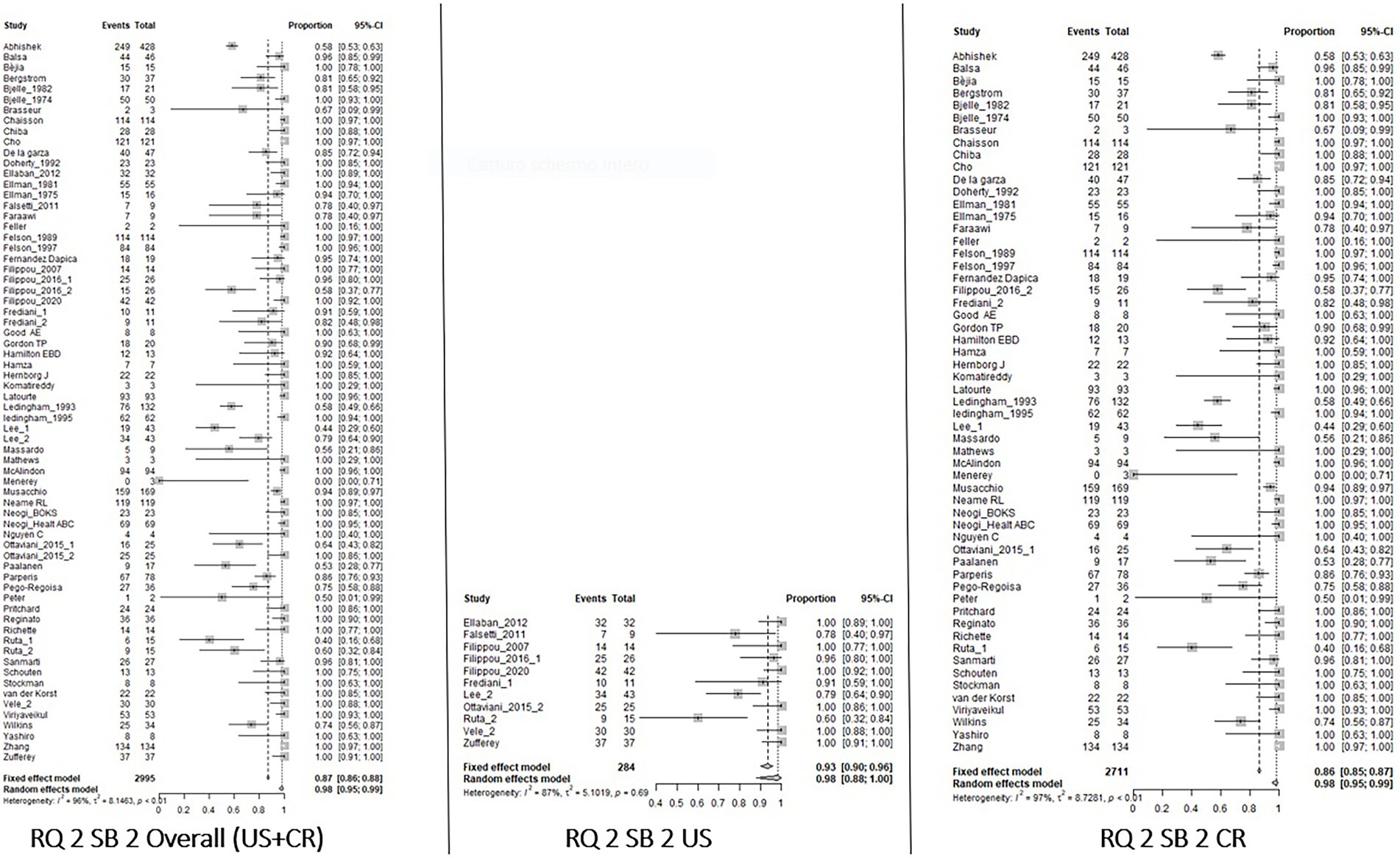
Figure 4. Forest Plot Knee, Research Question 2 (RQ 2), Sub_analysis 2: patients with suspected CPPD and knee/wrist used as index joint, independently of the reference standard used for diagnosis, analyzed by imaging.
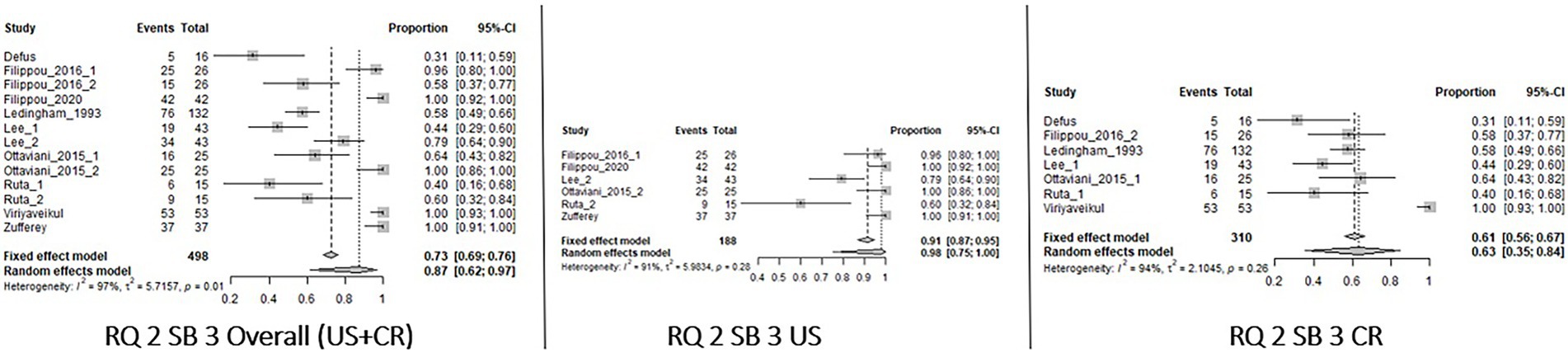
Figure 5. Forest Plot Knee, Research Question 2 (RQ 2), Sub-analysis 3: patients with suspected CPPD diagnosis and reference standard different than imaging, analyzed by imaging.
Assessment of the risk of bias
Most studies (88%, 83/94) showed a low risk of bias in many items, and the overall risk of bias was acceptable. Only a few studies had a high risk of bias (27, 53–55, 58, 65, 71, 90, 100, 104, 105).
Regarding the cohort study, the less fulfilled item was the comparability of the cohorts, which was related to the lack of matching of exposed and non-exposed patients or adjustment for confounders. Usually, the length of follow-up is not evaluable because most of the cohort studies included were mainly cross-sectional studies. For case–control studies, the main limitations were related to the representativeness of the cases and controls due to the lack of defined criteria for population selection. Finally, considering the diagnostic studies, the main source of bias was related to the reference standards used. In fact, in three studies, CR was applied as both index and reference standard (27, 53, 94), while in nine articles, the reference test was the McCarty criteria (20–24, 26, 29, 39, 60). All results of the NOS scale and QUADAS-2 are summarized in SP5.
Discussion
Currently, assessing the prevalence of CPPD remains challenging, mainly because of the heterogeneity of its clinical manifestations (6) and the lack of a non-invasive and accurate diagnostic technique. Furthermore, the natural history of CPPD is still unclear, and the patterns of involvement of the peripheral joints in terms of extent and chronological order have not been defined. In fact, despite being the most evaluated knee joint in the literature, previous studies have shown that radiographic chondrocalcinosis is common in wrists and hips, even in the absence of knee involvement (20, 40).
These aspects make imaging a potential cornerstone for CPPD diagnosis and monitoring. In this scenario, US presents several advantages as a noninvasive examination that can be applied to many joints in a short time. Moreover, US has been validated by the OMERACT validation process for diagnosis (10, 111). To further improve the application of imaging in CPPD, identifying the joints most frequently affected would improve feasibility and accuracy.
The OMERACT Ultrasound Working group in CPPD performed this SLR to collect the available data on the prevalence of CPPD in peripheral joints, assessed both by US and/or CR, to identify the most relevant joints to scan for CPPD diagnosis and monitoring. In fact, this SLR is the first multi-step approach that will lead to the creation of an US scoring system for CPPD.
Unfortunately, among the included studies, several sources of heterogeneity emerged, as the articles varied in terms of the type and number of joints evaluated, reference standard used, index joint, and CPPD clinical features. These differences made the articles less comparable and introduced biases in the descriptive analysis. Assessing the studies included in RQ1 and RQ2, some differences may be appreciated: for RQ1 (definite diagnosis), imaging was mainly applied on a larger number of joints or on sites different than the knee (only three of 22 articles evaluated the knee alone), using the knee as index joint for the diagnosis, while in the RQ2 (suspected CPPD) the knee was the only joint assessed for diagnosis in almost 50% of the articles, reducing the number of other joints available for analysis. Specific meta-analyzes were performed to address these issues. For each research question, studies were divided according to the index joint for CPPD (knee or wrist) and the reference standard used for diagnosis (selecting only studies that included SFA or histology). This selection led to the identification of the most homogenous study groups, comparable in meta-analyzes that assessed the prevalence of CPP deposits but, on the other hand, reduced the number of patients included in the analysis.
Considering the descriptive analysis, the knee and wrist resulted in the joints being mostly involved in CPPD at both CR and US, independent of the research question. The CPPD prevalence was higher with US at both sites for RQ1, while in RQ2 a higher CPPD prevalence in the knee was detected by US than by CR. In contrast, CR revealed more cases in the wrist than US. Meta-analyzes supported these findings. In fact, according to meta-analyzes, the knee is the joint characterized by the highest CPPD prevalence in RQ2, with values constantly equal to 0.98 in SB_1 and SB_2 (no differences according to the imaging technique used), whereas the prevalence decreased in RQ1 with a higher value in US than in CR [0.93 (0.68–0.99) and 0.79 (0.44–0.95), respectively]. The higher prevalence of CPPD among suspected patients was a surprising result, but is probably explained by the predominant assessment of the knee in RQ2, and by the simultaneous use of CR as an index and reference test in most of the studies included.
The higher CPPD prevalence at the level of the knee when US was applied was also shown in SB_3, which assessed only articles with a reference standard different from imaging [prevalence values: US 0.98 (0–75-1.00), CR 0.63 (0.35–0.84)]. The higher CPPD prevalence by US could be due to the higher sensitivity of this technique compared to CR in detecting CPP deposits at the knee level, as shown in previous studies (11, 67).
The results of this SLR also confirmed the common involvement of the wrist in CPPD, even higher than the knee in RQ1 according to the meta-analysis [US 0.92 (0.87–0.96), CR 0.83 (0.61–0.94)] but not in RQ2 [US 0.33 (0.13–0.63), CR 0.58 (0.48–0.68)]. Surprisingly, CPPD prevalence in the wrist was higher in US only in RQ1 and not in RQ2, but this is probably due to the widespread use of CR in RQ2 studies. In fact, the limited data available in the literature regarding a comparative assessment of the wrist showed a higher capability of US in detecting CPP deposits (11). For other joints, the hip showed a lower prevalence than the elbow or shoulder (0.27, 0.41 and 0.37 in the hip, elbow, and shoulder, respectively), but these results were obtained in a small number of patients and should be further addressed. Furthermore, all results were obtained only by CR and could be different if US was applied. Finally, the hand was the joint characterized by the lowest CPPD prevalence, from the 0.10 at the RQ1 to the 0.18 of the RQ2.
In addition, the descriptive results of the articular structures substantially confirmed the prevalence distribution of the whole joint, with higher values at the menisci, TFC, and knee hyaline cartilage. Again, these results were mainly obtained through CR, which could have some limitations.
The results of this SLR, although interesting, should be carefully evaluated. The included studies were heterogeneous in design, population, and reference standards. However, some degree of heterogeneity could be expected, as this is a frequent finding in meta-analysis (112). A common limitation of these studies was the use of CR as an index and reference test simultaneously, leading to a potential misidentification of the CPPD given the low sensitivity of CR, and mainly to an overestimation of the prevalence of deposition. Another issue regarding the joints assessed is that most of the articles evaluated only the knee and/or wrist, and very little data were available for other joints, making the results poorly reliable. Finally, other potentially very sensitive imaging techniques, such as computed tomography (CT) or dual-energy CT, were not included in this systematic review because very little data were available.
On the other hand, this SLR was the first attempt to collect literature data about the distribution of CPP deposits at peripheral joints using imaging techniques mainly applied in clinical practice. Furthermore, this SLR provided results regarding the single joint’s structure and bilateral involvement, and these data could be useful in clinical practice. The strengths of this SLR were the identification of sub-groups, ability to reduce the sources of heterogeneity, and the inclusion of meta-analysis aimed to assess the impact of the factors that mainly affected CPPD recognition by imaging: the index joint used to identify the deposits, and the reference standard used to confirm it. Finally, the overall quality of the studies included in the present SLR was acceptable, and the risk of bias was low to moderate.
Considering all the issues that have emerged, the future research agenda should include studies providing polyarticular assessment of CPPD patients, the definition of a tool for monitoring CPPD, and the planning of prospective studies.
In conclusion, the results of this SLR showed that the knee and wrist have the highest CPPD prevalence and should be incorporated into the set of joints for a CPPD follow-up. Furthermore, a higher prevalence of CPP deposits in the US was confirmed. Further, this SLR highlighted the widespread heterogeneity of the studies on CPPD, especially regarding the reference standard applied. This SLR will be the starting point for the development of a US scoring system by the OMERACT US working group for CPPD that could place US as the most validated tool for CPPD assessment both in clinical practice and for research.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
Author contributions
GF, GS, and CS contributed to the conception and design of the study. AA, EC, EF, FP, and SS collected the data. GS and AA organized the database. AZ and NU performed the statistical analysis. AA wrote the first draft of the manuscript. GS, GF, EF, and AZ wrote sections of the manuscript. All authors contributed to the manuscript revision, read, and approved the submitted version.
Funding
This work was supported and funded by the Italian Ministry of Health: Ricerca Corrente.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at:
https://www.frontiersin.org/articles/10.3389/fmed.2023.1131362/full#supplementary-material
References
1.Rosenthal, AK. Articular cartilage vesicles and calcium crystal deposition diseases. Curr Opin Rheumatol. (2016) 28:127–32. doi: 10.1097/BOR.0000000000000244
2.Ciancio, G, Bortoluzzi, A, and Govoni, M. Epidemiology of gout and chondrocalcinosis. Reumatismo. (2012) 63:207–20. doi: 10.4081/reumatismo.2011.207
3.Ramonda, R, Musacchio, E, Perissinotto, E, Sartori, L, Punzi, L, Corti, MC, et al. Prevalence of chondrocalcinosis in Italian subjects from northeastern Italy. The pro.V.a. (PROgetto Veneto Anziani) study. Clin Exp Rheumatol. (2009) 27:981–4.
4.Abhishek, A. Calcium pyrophosphate deposition disease: a review of epidemiologic findings. Curr Opin Rheumatol. (2016) 28:133–9. doi: 10.1097/BOR.0000000000000246
5.Mccarty, DJ. Calcium pyrophosphate Dihydrate crystal deposition disease: nomenclature and diagnostic criteria. Ann Intern Med. (1977) 87:240–2. doi: 10.7326/0003-4819-87-2-240
6.Zhang, W, Doherty, M, Bardin, T, Barskova, V, Guerne, P-A, Jansen, TL, et al. European league against rheumatism recommendations for calcium pyrophosphate deposition. Part I: terminology and diagnosis. Ann Rheum Dis. (2011) 70:563–70. doi: 10.1136/ard.2010.139105
7.Filippou, G, Adinolfi, A, Iagnocco, A, Filippucci, E, Cimmino, MA, Bertoldi, I, et al. Ultrasound in the diagnosis of calcium pyrophosphate dihydrate deposition disease. A systematic literature review and a meta-analysis. Osteoarthr Cartil. (2016) 24:973–81. doi: 10.1016/j.joca.2016.01.136
8.Filippou, G, Scirè, CA, Damjanov, N, Adinolfi, A, Carrara, G, Picerno, V, et al. Definition and reliability assessment of elementary ultrasonographic findings in calcium pyrophosphate deposition disease: a study by the OMERACT calcium pyrophosphate deposition disease ultrasound subtask force. J Rheumatol. (2017) 44:1744–9. doi: 10.3899/jrheum.161057
9.Filippou, G, Scirè, CA, Adinolfi, A, Damjanov, NS, Carrara, G, Bruyn, GA, et al. Identification of calcium pyrophosphate deposition disease (CPPD) by ultrasound: reliability of the OMERACT definitions in an extended set of joints - an international multiobserver study by the OMERACT calcium pyrophosphate deposition disease ultrasound subtask force. Ann Rheum Dis. (2018) 77:1195–200. doi: 10.1136/annrheumdis-2017-212542
10.Filippou, G, Scanu, A, Adinolfi, A, Toscano, C, Gambera, D, Largo, R, et al. Criterion validity of ultrasound in the identification of calcium pyrophosphate crystal deposits at the knee: an OMERACT ultrasound study. Ann Rheum Dis. (2021) 80:261–7. doi: 10.1136/annrheumdis-2020-217998
11.Cipolletta, E, Filippou, G, Scirè, CA, di Matteo, A, di Battista, J, Salaffi, F, et al. The diagnostic value of conventional radiography and musculoskeletal ultrasonography in calcium pyrophosphate deposition disease: a systematic literature review and meta-analysis. Osteoarthr Cartil. (2021) 29:619–32. doi: 10.1016/j.joca.2021.01.007
12.Tedeschi, SK, Pascart, T, Latourte, A, Godsave, C, Kundakci, B, Naden, RP, et al. Identifying potential classification criteria for calcium pyrophosphate deposition disease: item generation and item reduction. Arthritis Care Res. (2022) 74:1649–58. doi: 10.1002/acr.24619
13.Sirotti, S, Becce, F, Sconfienza, LM, Terslev, L, Naredo, E, Zufferey, P, et al. Reliability and diagnostic accuracy of radiography for the diagnosis of calcium pyrophosphate deposition: performance of the novel definitions developed by an international multidisciplinary working group. Arthritis Rheumatol. (2022) 2022:42368. doi: 10.1002/art.42368
14.Page, MJ, McKenzie, JE, Bossuyt, PM, Boutron, I, Hoffmann, TC, Mulrow, CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. (2021) 372:n71. doi: 10.1136/bmj.n71
15.Aslam, S, and Emmanuel, P. Formulating a researchable question: a critical step for facilitating good clinical research. Indian J Sex Transm Dis AIDS. (2010) 31:47–50. doi: 10.4103/0253-7184.69003
16.Whiting, PF. QUADAS-2: a revised tool for the quality assessment of diagnostic accuracy studies. Ann Intern Med. (2011) 155:529. doi: 10.7326/0003-4819-155-8-201110180-00009
17.Gierisch, JM, Beadles, C, Shapiro, A, JR, MD, Cunningham, N, Bradford, D, et al. Health Disparities in Quality Indicators of Healthcare among Adults with Mental Illness. Washington, DC: Department of Veterans Affairs (US) (2014).
18.Barskova, VG, Kudaeva, FM, Bozhieva, LA, Smirnov, AV, Volkov, AV, and Nasonov, EL. Comparison of three imaging techniques in diagnosis of chondrocalcinosis of the knees in calcium pyrophosphate deposition disease. Rheumatology. (2013) 52:1090–4. doi: 10.1093/rheumatology/kes433
19.Canhão, H, Fonseca, JE, Leandro, MJ, Romeu, JC, Pimentão, JB, Teixeira Costa, J, et al. Cross-sectional study of 50 patients with calcium pyrophosphate dihydrate crystal arthropathy. Clin Rheumatol. (2001) 20:119–22. doi: 10.1007/s100670170081
20.Cipolletta, E, Smerilli, G, Mashadi Mirza, R, di Matteo, A, Carotti, M, Salaffi, F, et al. Sonographic assessment of calcium pyrophosphate deposition disease at wrist. A focus on the dorsal scapho-lunate ligament. Joint Bone Spine. (2020) 87:611–7. doi: 10.1016/j.jbspin.2020.04.012
21.Di Matteo, A, Filippucci, E, Salaffi, F, Carotti, M, Carboni, D, Di Donato, E, et al. Diagnostic accuracy of musculoskeletal ultrasound and conventional radiography in the assessment of the wrist triangular fibrocartilage complex in patients with definite diagnosis of calcium pyrophosphate dihydrate deposition disease. Clin Exp Rheumatol. (2017) 35:647–52.
22.Di Matteo, A, Filippucci, E, Cipolletta, E, Musca, A, Carotti, M, Mirza, RM, et al. Hip involvement in patients with calcium pyrophosphate deposition disease: potential and limits of musculoskeletal ultrasound. Arthritis Care Res. (2019) 71:1671–7. doi: 10.1002/acr.23814
23.Ellabban, AS, Kamel, SR, Omar, HASA, El-Sherif, AMH, and Abdel-Magied, RA. Ultrasonographic findings of Achilles tendon and plantar fascia in patients with calcium pyrophosphate deposition disease. Clin Rheumatol. (2012) 31:697–704. doi: 10.1007/s10067-011-1911-2
24.Falsetti, P, Frediani, B, Acciai, C, Baldi, F, Filippou, G, Prada, EP, et al. Ultrasonographic study of achilles tendon and plantar fascia in chondrocalcinosis. J Rheumatol. (2004) 31:2242–50.
25.Filippou, G, Filippucci, E, Tardella, M, Bertoldi, I, di Carlo, M, Adinolfi, A, et al. Extent and distribution of CPP deposits in patients affected by calcium pyrophosphate dihydrate deposition disease: an ultrasonographic study. Ann Rheum Dis. (2013) 72:1836–9. doi: 10.1136/annrheumdis-2012-202748
26.Filippucci, E, Gutierrez Riveros, M, Georgescu, D, Salaffi, F, and Grassi, W. Hyaline cartilage involvement in patients with gout and calcium pyrophosphate deposition disease. An ultrasound study. Osteoarthr Cartil. (2009) 17:178–81. doi: 10.1016/j.joca.2008.06.003
27.Foldes, K. Knee chondrocalcinosis: an ultrasonographic study of the hyalin cartilage. Clin Imaging. (2002) 26:194–6. doi: 10.1016/S0899-7071(01)00385-0
28.Forien, M, Combier, A, Gardette, A, Palazzo, E, Dieudé, P, and Ottaviani, S. Comparison of ultrasonography and radiography of the wrist for diagnosis of calcium pyrophosphate deposition. Joint Bone Spine. (2018) 85:615–8. doi: 10.1016/j.jbspin.2017.09.006
29.Gerster, JC, Baud, CA, Lagier, R, Boussina, I, and Fallet, GH. Tendon calcifications in chondrocalcinosis. A clinical, radiologic, histologic, and crystallographic study. Arthritis Rheum. (1977) 20:717–22. doi: 10.1002/art.1780200212
30.Gutierrez, M, di Geso, L, Salaffi, F, Carotti, M, Girolimetti, R, de Angelis, R, et al. Ultrasound detection of cartilage calcification at knee level in calcium pyrophosphate deposition disease. Arthritis Care Res. (2014) 66:69–73. doi: 10.1002/acr.22190
31.Huang, G-S, Bachmann, D, Taylor, JA, Marcelis, S, Haghighi, P, and Resnick, D. Calcium pyrophosphate dihydrate crystal deposition disease and pseudogout of the acromioclavicular joint: radiographic and pathologic features. J Rheumatol. (1993) 20:2077–82
32.Lindén, B. Symptomatic chondrocalcinosis at the wrist. Scand J Plast Reconstr Surg. (1977) 11:243–5. doi: 10.3109/02844317709025526
33.Moskowitz, RW, and Katz, D. Chondrocalcinosis and chondrocalsynovitis. (pseudogout syndrome). Analysis of twenty-four cases. Am J Med. (1967) 43:322–34. doi: 10.1016/0002-9343(67)90189-1
34.Peter, A, Simmen, BR, Brühlmann, P, Michel, BA, and Stucki, G. Osteoarthritis of the scaphoidtrapezium joint: an early sign of calcium pyrophosphate dihydrate disease. Clin Rheumatol. (2001) 20:20–4. doi: 10.1007/PL00011183
35.Resnick, D, Niwayama, G, Goergen, TG, Utsinger, PD, Shapiro, RF, Haselwood, DH, et al. Clinical, radiographic and pathologic abnormalities in calcium pyrophosphate dihydrate deposition disease (CPPD): pseudogout. Radiology. (1977) 122:1–15. doi: 10.1148/122.1.1
36.Resnick, D, and Utsinger, PD. The wrist arthropathy of ‘pseudogout’ occurring with and without chondrocalcinosis. Radiology. (1974) 113:633–41. doi: 10.1148/113.3.633
37.Richardson, BC, Chafetz, NI, Ferrell, LD, Zulman, JI, and Genant, HK. Hereditary chondrocalcinosis in a Mexican-American family. Arthritis Rheum. (1983) 26:1387–96. doi: 10.1002/art.1780261112
38.Schlesinger, N, Hassett, AL, Neustadter, L, and Schumacher, HRJ. Does acute synovitis (pseudogout) occur in patients with chronic pyrophosphate arthropathy (pseudo-osteoarthritis)? Clin Exp Rheumatol. (2009) 27:940–4.
39.Vele, P, Simon, SP, Damian, L, Felea, I, Muntean, L, Filipescu, I, et al. Clinical and ultrasound findings in patients with calcium pyrophosphate dihydrate deposition disease. Med Ultrason. (2018) 20:159–63. doi: 10.11152/mu-1193
40.Abhishek, A, Doherty, S, Maciewicz, R, Muir, K, Zhang, W, and Doherty, M. Chondrocalcinosis is common in the absence of knee involvement. Arthritis Res Ther. (2012) 14:R205. doi: 10.1186/ar4043
41.Axford, JS, Revell, P, Watt, I, Bomford, A, Williams, R, and Hamilton, EBD. Hip arthropathy in genetic hemochromatosis: radiographic and histologic features. Arthritis Rheum. (1991) 34:357–61. doi: 10.1002/art.1780340314
42.Balsa, A, Martin-Mola, E, Gonzalez, T, Cruz, A, Ojeda, S, and Gijon-Banos, J. Familial articular chondrocalcinosis in Spain. Ann Rheum Dis. (1990) 49:531–5. doi: 10.1136/ard.49.7.531
43.Béjia, I, Rtibi, I, Touzi, M, Zrour, S, Younes, M, and Naceur, B. Familial calcium pyrophosphate dihydrate deposition disease. Joint Bone Spine. (2004) 71:401–8. doi: 10.1016/j.jbspin.2003.10.012
44.Bergstrom, G, Bjelle, A, Sundh, V, and Svanborg, A. Joint disorders at ages 70, 75 and 79 years - a cross-sectional comparison. Br J Rheumatol. 25:333–41. doi: 10.1093/rheumatology/25.4.333
45.Bjelle, A, Edvinsson, U, and Hagstam, A. Pyrophosphate arthropathy in two Swedish families. Arthritis Rheum. (1982) 25:66–74. doi: 10.1002/art.1780250111
46.Bjelle, A, and Sundén, G. Pyrophosphate arthropathy: a clinical study of fifty cases. J Bone Joint Surg Br. (1974) 56-B:246–55. doi: 10.1302/0301-620X.56B2.246
47.Brasseur, J-P, Huaux, J-P, Devogelaer, J-P, and De Deuxchaisnes, CN. Articular chondrocalcinosis in seropositive rheumatoid arthritis. Comparison with a control group. J Rheumatol. (1987) 14:40–1.
48.Chaisson, CE, McAlindon, T, Felson, DT, Naimark, A, Wilson, PW, and Sawin, CT. Lack of association between thyroid status and chondrocalcinosis or osteoarthritis: the Framingham osteoarthritis study. J Rheumatol. (1996) 23:711–5.
49.Chiba, D, Tsuda, E, Sasaki, E, Takahashi, I, Nakaji, S, and Ishibashi, Y. Low prevalence of knee chondrocalcinosis and its catabolic association with serum matrix metalloproteinase 3: a rural Japanese population study. Int J Rheum Dis. (2018) 21:2011–8. doi: 10.1111/1756-185X.13067
50.Cho, NH, Song, Y, Lee, S, Sung, Y-K, and Jun, J-B. Incidence of knee chondrocalcinosis and its risk factors in a community-based cohort. Int J Rheum Dis. (2018) 21:1391–7. doi: 10.1111/1756-185X.13317
51.De la Garza-Montaño, P, Pineda, C, Lozada-Pérez, CA, Camargo-Ibarias, K, González-Hernández, MF, Avila-Luna, A, et al. Prevalence of chondrocalcinosis in a Mexican tertiary care institution of musculoskeletal disorders. Clin Rheumatol. (2019) 38:2595–602. doi: 10.1007/s10067-019-04614-1
52.Derfus, BA, Kurian, JB, Butler, JJ, Daft, LJ, Carrera, GF, Ryan, LM, et al. The high prevalence of pathologic calcium crystals in pre-operative knees. J Rheumatol. (2002) 29:570–4.
53.Devauchelle-Pensec, V, Berthelot, JM, Jousse, S, Samjee, I, Josseaume, T, Colin, D, et al. Performance of hand radiographs in predicting the diagnosis in patients with early arthritis. J Rheumatol. (2006) 33:1511–5.
54.Doherty, M, Belcher, C, Regan, M, Jones, A, and Ledingham, J. Association between synovial fluid levels of inorganic pyrophosphate and short term radiographic outcome of knee osteoarthritis. Ann Rheum Dis. (1996) 55:432–6. doi: 10.1136/ard.55.7.432
55.Doherty, M, Watt, I, and Dieppe, PA. Localised chondrocalcinosis in post-meniscectomy knees. Lancet. (1982) 319:1207–10. doi: 10.1016/S0140-6736(82)92336-4
56.Ellabban, AS, Kamel, SR, Abo Omar, HAS, El-Sherif, AMH, and Abdel-Magied, RA. Ultrasonographic diagnosis of articular chondrocalcinosis. Rheumatol Int. (2012) 32:3863–8. doi: 10.1007/s00296-011-2320-1
57.Ellman, MH, Brown, NL, and Katzenberg, CA. Acute pseudogout in chronic renal failure. Arch Intern Med. (1979) 139:795–6. doi: 10.1001/archinte.1979.03630440057019
58.Ellman, MH, Brown, NL, and Levin, B. Prevalence of knee chondrocalcinosis in hospital and clinic patients aged 50 or older. J Am Geriatr Soc. (1981) 29:189–92. doi: 10.1111/j.1532-5415.1981.tb01764.x
59.Ellman, MH, and Levin, B. Chondrocalcinosis in elderly persons. Arthritis Rheum. (1975) 18:43–7. doi: 10.1002/art.1780180109
60.Falsetti, P, Acciai, C, Volpe, A, and Lenzi, L. Ultrasonography in early assessment of elderly patients with polymyalgic symptoms: a role in predicting diagnostic outcome? Scand J Rheumatol. (2011) 40:57–63. doi: 10.3109/03009742.2010.486766
61.Faraawi, R, Harth, M, Kertesz, A, and Bell, D. Arthritis in hemochromatosis. J Rheumatol. (1993) 20:448–52.
62.Feller, ER, and Schumacher, HR. Osteoarticular changes in Wilson’s disease. Arthritis Rheum. (1972) 15:259–66. doi: 10.1002/art.1780150307
63.Felson, DT, Anderson, JJ, Naimark, A, Kannel, W, and Meenan, RF. The prevalence of chondrocalcinosis in the elderly and its association with knee osteoarthritis: the Framingham study. J Rheumatol. (1989) 16:1241–5.
64.Felson, DT, Zhang, Y, Hannan, MT, Naimark, A, Weissman, B, Aliabadi, P, et al. Risk factors for incident radiographic knee osteoarthritis in the elderly. Arthritis Rheum. (1997) 40:728–33. doi: 10.1002/art.1780400420
65.Fernandez Dapica, MP, and Gómez-Reino, JJ. Familial chondrocalcinosis in the Spanish population. J Rheumatol. (1986) 13:631–3.
66.Filippou, G, Frediani, B, Gallo, A, Menza, L, Falsetti, P, Baldi, F, et al. A ‘new’ technique for the diagnosis of chondrocalcinosis of the knee: sensitivity and specificity of high-frequency ultrasonography [5]. Ann Rheum Dis. (2007) 66:1126–8. doi: 10.1136/ard.2007.069344
67.Filippou, G, Adinolfi, A, Cimmino, MA, Scirè, CA, Carta, S, Lorenzini, S, et al. Diagnostic accuracy of ultrasound, conventional radiography and synovial fluid analysis in the diagnosis of calcium pyrophosphate dihydrate crystal deposition disease. Clin Exp Rheumatol. (2016) 34:254–60.
68.Filippou, G, Scanu, A, Adinolfi, A, Picerno, V, Toscano, C, Bortoluzzi, A, et al. The two faces of the same medal… or maybe not? Comparing osteoarthritis and calcium pyrophosphate deposition disease: a laboratory and ultrasonographic study. Clin Exp Rheumatol. (2020) 39:66–72. doi: 10.55563/clinexprheumatol/gu9j0q
69.Frediani, B, Filippou, G, Falsetti, P, Lorenzini, S, Baldi, F, Acciai, C, et al. Diagnosis of calcium pyrophosphate dihydrate crystal deposition disease: ultrasonographic criteria proposed. Ann Rheum Dis. (2005) 64:638–40. doi: 10.1136/ard.2004.024109
70.Good, AE, and Rapp, R. Chondrocalcinosis of the knee with gout and rheumatoid arthritis. N Engl J Med. (1967) 277:286–90. doi: 10.1056/NEJM196708102770603
71.Gordon, TP, Smith, M, and Ebert, B. Articular chondrocalcinosis in a hospital population: an Australian experience. Aust NZ J Med. (1984) 14:655–9. doi: 10.1111/j.1445-5994.1984.tb05019.x
72.Hamilton, EB, Bomford, AB, Laws, JW, and Williams, R. The natural history of arthritis in idiopathic haemochromatosis: progression of the clinical and radiological features over ten years. Q J Med. (1981) 50:321–9.
73.Hamza, M, Meddeb, N, and Bardin, T. Hereditary chondrocalcinosis in a Tunisian family. Clin Exp Rheumatol. (1992) 10:43–9.
74.Hernborg, J, Linden, B, and Nilsson, BE. Chondrocalcinosis: a secondary finding in osteoarthritis of the knee. Geriatrics. (1977) 32:123–124, 126.
75.Komatireddy, GR, Ellman, MH, and Brown, NL. Lack of association between hypothyroidism and chondrocalcinosis. J Rheumatol. (1989) 16:807–8.
76.Latourte, A, Rat, AC, Ngueyon Sime, W, Ea, HK, Bardin, T, Mazières, B, et al. Chondrocalcinosis of the knee and the risk of osteoarthritis progression: data from the knee and hip osteoarthritis long-term assessment cohort. Arthritis Rheumatol. (2020) 72:726–32. doi: 10.1002/art.41186
77.Ledingham, J, Dawson, S, Preston, B, Milligan, G, and Doherty, M. Radiographic patterns and associations of osteoarthritis of the hip. Ann Rheum Dis. (1992) 51:1111–6. doi: 10.1136/ard.51.10.1111
78.Ledingham, J, Dawson, S, Preston, B, Milligan, G, and Doherty, M. Radiographic progression of hospital referred osteoarthritis of the hip. Ann Rheum Dis. (1993) 52:263–7. doi: 10.1136/ard.52.4.263
79.Ledingham, J, Regan, M, Jones, A, and Doherty, M. Radiographic patterns and associations of osteoarthritis of the knee in patients referred to hospital. Ann Rheum Dis. (1993) 52:520–6. doi: 10.1136/ard.52.7.520
80.Ledingham, J, Regan, M, Jones, A, and Doherty, M. Factors affecting radiographic progression of knee osteoarthritis. Ann Rheum Dis. (1995) 54:53–8. doi: 10.1136/ard.54.1.53
81.Lee, KA, Lee, S-H, and Kim, H-R. Diagnostic value of ultrasound in calcium pyrophosphate deposition disease of the knee joint. Ann Rheum Dis. (2019) 27:781–7. doi: 10.1016/j.joca.2018.11.013
82.Massardo, L, Watt, I, Cushnaghan, J, and Dieppe, P. Osteoarthritis of the knee joint: an eight year prospective study. Ann Rheum Dis. (1989) 48:893–7. doi: 10.1136/ard.48.11.893
83.Mathews, JL, and Williams, HJ. Arthritis in hereditary hemochromatosis. Arthritis Rheum. (1987) 30:1137–41. doi: 10.1002/art.1780301008
84.McAlindon, T, Zhang, Y, Hannan, M, Naimark, A, Weissman, B, Castelli, W, et al. Are risk factors for patellofemoral and tibiofemoral knee osteoarthritis different? J Rheumatol. (1996) 23:332–7.
85.Menerey, KA, Eider, W, Brewer, GJ, Braunstein, EM, Schumacher, HR, and Fox, IH. The arthropathy of Wilson’s disease: clinical and pathologic features. J Rheumatol. (1988) 15:331–7.
86.Montgomery, KD, Williams, JR, Sculco, TR, and Dicarlo, E. Clinical and pathologic findings in hemochromatosis hip arthropathy. Clin Orthop. (1998) 347:179–87. doi: 10.1097/00003086-199802000-00020
87.Musacchio, E, Ramonda, R, Perissinotto, E, Sartori, L, Hirsch, R, Punzi, L, et al. The impact of knee and hip chondrocalcinosis on disability in older people: the ProVA study from northeastern Italy. Ann Rheum Dis. (2011) 70:1937–43. doi: 10.1136/ard.2011.150508
88.Neame, RL, Carr, AJ, Muir, K, and Doherty, M. UK community prevalence of knee chondrocalcinosis: evidence that correlation with osteoarthritis is through a shared association with osteophyte. Ann Rheum Dis. (2003) 62:513–8. doi: 10.1136/ard.62.6.513
89.Neogi, T, Nevitt, M, Niu, J, LaValley, MP, Hunter, DJ, Terkeltaub, R, et al. Lack of association between chondrocalcinosis and increased risk of cartilage loss in knees with osteoarthritis: results of two prospective longitudinal magnetic resonance imaging studies. Arthritis Rheum. (2006) 54:1822–8. doi: 10.1002/art.21903
90.Nguyen, C, Bazin, D, Daudon, M, Chatron-Colliet, A, Hannouche, D, Bianchi, A, et al. Revisiting spatial distribution and biochemical composition of calcium-containing crystals in human osteoarthritic articular cartilage. Arthritis Res Ther. (2013) 15:R103. doi: 10.1186/ar4283
91.Ottaviani, S, Juge, P-A, Aubrun, A, Palazzo, E, and Dieudé, P. Sensitivity and reproducibility of ultrasonography in calcium pyrophosphate crystal deposition in knee cartilage: a cross-sectional study. J Rheumatol. (2015) 42:1511–3. doi: 10.3899/jrheum.141067
92.Ottaviani, S, Goossens, J, Demaria, L, Forien, M, Palazzo, E, and Dieudé, P. Ultrasound shoulder assessment of calcium pyrophosphate disease with suspected polymyalgia rheumatic. Clin Exp Rheumatol. (2020) 38:1170–5.
93.Paalanen, K, Rannio, K, Rannio, T, Asikainen, J, Hannonen, P, and Sokka, T. Prevalence of calcium pyrophosphate deposition disease in a cohort of patients diagnosed with seronegative rheumatoid arthritis. Clin Exp Rheumatol. (2020) 38:99–106.
94.Parperis, K, Carrera, G, Baynes, K, Mautz, A, DuBois, M, Cerniglia, R, et al. The prevalence of chondrocalcinosis (CC) of the acromioclavicular (AC) joint on chest radiographs and correlation with calcium pyrophosphate dihydrate (CPPD) crystal deposition disease. Clin Rheumatol. (2013) 32:1383–6. doi: 10.1007/s10067-013-2255-x
95.Pego-Reigosa, JM, Rodriguez-Rodriguez, M, Hurtado-Hernandez, Z, Gromaz-Martin, J, Taboas-Rodriguez, D, Millan-Cachinero, C, et al. Calcium pyrophosphate deposition disease mimicking polymyalgia rheumatica: a prospective followup study of predictive factors for this condition in patients presenting with polymyalgia symptoms. Arthritis Care Res. (2005) 53:931–8. doi: 10.1002/art.21585
96.Pritchard, MH, and Jessop, JD. Chondrocalcinosis in primary hyperparathyroidism. Influence of age, metabolic bone disease, and parathyroidectomy. Ann Rheum Dis. (1977) 36:146–51. doi: 10.1136/ard.36.2.146
97.Reginato, AJ. Articular chondrocalcinosis in the Chiloe islanders. Arthritis Rheum. (1976) 19:395–404. doi: 10.1002/1529-0131(197605/06)19:3+<395::AID-ART1780190712>3.0.CO;2-T
98.Richette, P, Ayoub, G, Lahalle, S, Vicaut, E, Badran, AM, Joly, F, et al. Hypomagnesemia associated with chondrocalcinosis: a cross-sectional study. Arthritis Care Res. (2007) 57:1496–501. doi: 10.1002/art.23106
99.Ruta, S, Catay, E, Marin, J, Rosa, J, García-Monaco, R, and Soriano, ER. Knee effusion: ultrasound as a useful tool for the detection of calcium pyrophosphate crystals. Clin Rheumatol. (2016) 35:1087–91. doi: 10.1007/s10067-015-3100-1
100.Sanmarti, R, Panella, D, Brancos, MA, Canela, J, Collado, A, and Brugues, J. Prevalence of articular chondrocalcinosis in elderly subjects in a rural area of Catalonia. Ann Rheum Dis. (1993) 52:418–22. doi: 10.1136/ard.52.6.418
101.Schouten, JSAG, Van den Ouweland, FA, and Valkenburg, HA. A 12 year follow up study in the general population on prognostic factors of cartilage loss in osteoarthritis of the knee. Ann Rheum Dis. (1992) 51:932–7. doi: 10.1136/ard.51.8.932
102.Stockman, A, Darlington, LG, and Scott, JT. Frequency of chondrocalcinosis of the knees and avascular necrosis of the femoral heads in gout: a controlled study. Ann Rheum Dis. (1980) 39:7–11. doi: 10.1136/ard.39.1.7
103.Trentham, DE, Masi, AT, and Hamm, RL. Letter: Roentgenographic prevalence of chondrocalcinosis. Arthritis Rheum. (1975) 18:627–8. doi: 10.1002/art.1780180617
104.Utsinger, PD, Zvaifler, NJ, and Resnick, D. Calcium pyrophosphate dihydrate deposition disease without chondrocalcinosis. J Rheumatol. (1975) 2:258–64.
105.van der Korst, JK, Geerards, J, and Driessens, FC. A hereditary type of idiopathic articular chondrocalcinosis. Survey of a pedigree. Am J Med. (1974) 56:307–14. doi: 10.1016/0002-9343(74)90612-3
106.Viriyavejkul, P, Wilairatana, V, Tanavalee, A, and Jaovisidha, K. Comparison of characteristics of patients with and without calcium pyrophosphate dihydrate crystal deposition disease who underwent total knee replacement surgery for osteoarthritis. Osteoarthr Cartil. (2007) 15:232–5. doi: 10.1016/j.joca.2006.08.012
107.Wilkins, E, Dieppe, P, Maddison, P, and Evison, G. Osteoarthritis and articular chondrocalcinosis in the elderly. Ann Rheum Dis. (1983) 42:280–4. doi: 10.1136/ard.42.3.280
108.Yashiro, T, Okamoto, T, Tanaka, R, Ito, K, Hara, H, Yamashita, T, et al. Prevalence of chondrocalcinosis in patients with primary hyperparathyroidism in Japan. Endocrinol Jpn. (1991) 38:457–64. doi: 10.1507/endocrj1954.38.457
109.Zhang, W, Neame, R, Doherty, S, and Doherty, M. Relative risk of knee chondrocalcinosis in siblings of index cases with pyrophosphate arthropathy. Ann Rheum Dis. (2004) 63:969–73. doi: 10.1136/ard.2003.015206
110.Zufferey, P, Valcov, R, Fabreguet, I, Dumusc, A, Omoumi, P, and So, A. A prospective evaluation of ultrasound as a diagnostic tool in acute microcrystalline arthritis. Arthritis Res Ther. (2015) 17:188. doi: 10.1186/s13075-015-0701-7
111.Filippou, G, Scanu, A, Adinolfi, A, Toscano, C, Largo-Carazo, R, Naredo, E, et al. Diagnostic accuracy of ultrasound in calcium pyrophosphate deposition disease: preliminary results of the omeract US in CPPD sub-group. Ann Rheum Dis. (2019) 78:242. doi: 10.1136/annrheumdis-2019-eular.3460
Keywords: ultrasound, calcium pyrophosphate crystal deposition, conventional radiography, systematic review, CPPD, chondrocalcinosis
Citation: Adinolfi A, Sirotti S, Sakellariou G, Cipolletta E, Filippucci E, Porta F, Zanetti A, Ughi N, Sarzi-Puttini P, Scirè CA, Keen H, Pineda C, Terslev L, D’Agostino MA and Filippou G (2023) Which are the most frequently involved peripheral joints in calcium pyrophosphate crystal deposition at imaging? A systematic literature review and meta-analysis by the OMERACT ultrasound – CPPD subgroup. Front. Med. 10:1131362. doi: 10.3389/fmed.2023.1131362
Edited by:
Lucía Silva-Fernández, Hospital Universitario Son Espases, SpainReviewed by:
Abdallah El-Sayed Allam, Tanta University, EgyptCristina Hernández-Díaz, Hospital Juárez de México, Mexico
Copyright © 2023 Adinolfi, Sirotti, Sakellariou, Cipolletta, Filippucci, Porta, Zanetti, Ughi, Sarzi-Puttini, Scirè, Keen, Pineda, Terslev, D’Agostino and Filippou. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Antonella Adinolfi, YW50b25lbGxhLmFkaW5vbGZpQG9zcGVkYWxlbmlndWFyZGEuaXQ=