 Antonio Corsello
Antonio Corsello Giulia C. I. Spolidoro1†
Giulia C. I. Spolidoro1† Gregorio P. Milani
Gregorio P. Milani Carlo Agostoni
Carlo Agostoni
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
OPINION article
Front. Med., 16 March 2023
Sec. Family Medicine and Primary Care
Volume 10 - 2023 | https://doi.org/10.3389/fmed.2023.1107855
This article is part of the Research TopicCare During Pregnancy and Early Childhood for Growth and Development in Low- and Middle- Income CountriesView all 20 articles
In recent years vitamin D has been in the spotlight of many researchers for its possible role in various disorders, including autoimmune and infectious diseases. Even if vitamin D deficiency remains a major public health problem, its symptomatic manifestations are less and less common in clinical practice, and pediatric age represents a “gray area” where vitamin D supplementation is often administered in the absence of an effective evaluation of its status. Moreover, a poor knowledge about different definitions of “deficiency,” “insufficiency,” and similar terms is spread among clinicians, while guidelines are not univocal, especially after the first year of life. The aim of this brief opinion paper is to sum up recent evidence about vitamin D status and its supplementation in pediatrics, in order to better clarify a common definition of its deficiency. The aim of this opinion article is to raise awareness on this topic among clinicians and encourage a discussion on the real need for routine 25-hydroxycholecalciferol serum evaluation and its supplementation.
The role of vitamin D for calcium metabolism and, especially, for the treatment of rickets was first identified in 1922 by the American biochemist Elmer McCollum (1879–1967) (1). After his observations, thousands of papers have shed light on its important and multifaceted function for human health, not only regarding the musculoskeletal system (2, 3). At the same time, several investigators have observed that a surprising number of patients may present deficient levels of this micronutrient, regardless of their age and origin (4–6). Vitamin D deficiency remains a major public health problem, even after a century since its discovery (7).
At least two under-rated factors might contribute to the persistence of this issue: the lack of a common definition of vitamin D deficiency and the existence of partially contrasting recommendations on vitamin D prophylaxis.
The aim of this opinion article is to highlight recent evidence about vitamin D status and its supplementation in pediatrics, to better clarify a common definition of its deficiency. Our goal is to raise awareness among clinicians of this topic and encourage a discussion on the real need for routine 25-hydroxycholecalciferol serum evaluation and supplementation.
Vitamin D plays an important role in bone growth and remodeling by osteoblasts and osteoclasts and is essential to maintain calcium, phosphate, and magnesium body homeostasis by regulating intestinal absorption, and renal absorption/excretion, alongside the parathyroid hormone (PTH). Plasma calcium and phosphate are mainly influenced by the active form of vitamin D (1α,25-dihydroxyvitamin D) and PTH, while a minor role is also attained by other humoral factors (8).
Magnesium is influenced, though to a lesser degree, by the same factors that control calcium, and it indirectly influences calcium by altering PTH synthesis and secretion in response to hypocalcemia and by assisting in the activation of vitamin D (9). Indeed, magnesium functions as a cofactor in many kidneys and liver enzymatic reactions and it is required by all the enzymes that intervene in vitamin D metabolization (10). Consequently, a lack of magnesium may result in disruption to the calcium/phosphate homestays regulated by active vitamin D/PTH and may cause vitamin D–resistant hypocalcemia (9, 10). On the other hand, vitamin D deficiency or overload may result in hypermagnesemia (magnesium not utilized) or hypomagnesemia (excessive consumption of magnesium).
In the early stages, vitamin D deficiency results in impaired calcium intestinal absorption and consequent low serum calcium levels (hypocalcemia). In turn, hypocalcemia stimulates PTH secretion which acts to normalize serum calcium by reducing renal calcium excretion, increasing renal phosphate excretion, and stimulating renal production of active vitamin D. High levels of PTH (hyperparathyroidism) also boost osteoclast activity which determines bone calcium release. The combination of low serum phosphate levels (hypophosphatasemia) and increased osteoclast activity results in bone demineralization (11).
In children, severe vitamin D deficiency may cause rickets, a childhood metabolic bone disease caused by under-mineralization of the growing bone. Following the growth plate closure, in older children and adults, the term “osteomalacia” is used to describe the demineralization of bone at sites of bone remodeling (12).
Vitamin D positive effects on the innate immune system are well known since the discovery of its historical beneficial effects on mycobacterium tuberculosis infection (13, 14). Vitamin D modulates monocytes, macrophages, dendritic cell responses, and the production of interleukins (15). Autoimmune diseases (ADs) are caused by an erroneous activation of the immune system, with subsequent destruction of tissues by autoreactive immune cells, which can react against self-antigens (16). Among the causes contributing to the development of ADs, an insufficient vitamin D serum concentration might play a significant role, as proven by epidemiologic findings of higher incidences of ADs among countries with lower sun exposures and high prevalence of vitamin D insufficiency (17, 18).
Recent studies found the vitamin D’s involvement in the suppression of T lymphocyte proliferation and adaptive immune system, causing a shift from a Th1 to a Th2 phenotype and a subsequent alteration in the differentiation and maturation of T cells, inducing T regulatory cells function and immune self-tolerance (19, 20). Moreover, B lymphocytes have been found to express vitamin D receptors, which, when activated, can inhibit the differentiation into plasma cells and modulate immunoglobulin production (21). All these effects could explain the possible connection between variable vitamin D serum levels and the probability to develop an AD (22).
Studies conducted among children with type 1 diabetes (T1D) found a significant difference in the incidence of disease according to the gradient of sun exposure in different countries and the seasonal variability (23, 24). Conflicting evidence has been found about the hypothesis that vitamin D supplementation could reduce the probability to develop T1D in early life, even if a protective correlation between minor incidence and higher serum levels has been found in some studies (25–27). Other studies observed a delay in the progression of beta-cells destruction when vitamin D is administered in an early stage of onset and diagnosis (28–30). Two meta-analyses found that the risk of developing T1D was significantly reduced in children supplemented with vitamin D (27, 31). For these reasons, avoiding a vitamin D insufficiency in patients at high risk for developing T1D is suggested, even if evidence for a specific supplementation in these subjects is lacking (17). Concerning other ADs, low 25(OH)D sera levels have been associated with the development of autoimmune thyroiditis, such as Hashimoto’s disease and Grave’s disease, both in children and adults (32–34).
Vitamin D also acts as an enhancement of the intestinal defense mechanisms, locally regulating the mucosal immune system and preventing harmful microbial proliferation (35, 36). For instance, an association between lower vitamin D concentrations and an increased risk of developing IBD has been suggested (37–40). This evidence can be strengthened by the reduced vitamin receptors expression found in the colon mucosa of mice affected by IBD when compared to healthy controls, with an increased production of Th1 and Th17 lymphocytes and inflammatory cytokines in the gastrointestinal tract (41, 42). For these reasons, according to recent interventional studies, a vitamin D supplementation can be considered a potential effective and safe therapeutic choice in patients with IBD (43–46).
Emerging evidence from various meta-analyses supposes a plausible role of low vitamin D levels in many other ADs, such as rheumatoid arthritis, systemic lupus erythematosus, and multiple sclerosis, and vitamin D receptors polymorphisms have been associated with higher incidences of several ADs (47–51). However, optimal vitamin D concentrations that could reduce the possible occurrence of ADs are not clear yet, even if levels higher than 20 ng/mL (about 50 nmol/L) should be considered sufficient to maintain the physiologic calcemic and non-calcemic functions of vitamin D (52).
Vitamin D deficiency has been recognized in a wide range of pathological conditions, from allergic to immune-mediated diseases such as diabetes or chronic inflammatory bowel diseases (25, 27, 53–55). More recently, vitamin D deficiency and its eventual supplementation have been even considered linked with COVID-19 symptoms and prevention, generally without any proof of a cause-and-effect relationship, including reverse causality (56–59).
Although cases of rickets and clinical manifestations of symptomatic vitamin D deficiency are actually rare, many studies worldwide have shown high rates of vitamin D deficiency and insufficiency (measured as the serum concentration of 25-hydroxycholecalciferol, 25(OH)D) in the pediatric population, with rates ranging on average between 40 and 75%, even in developed countries (60–63). The low rates of sunlight exposure in Nordic countries and the limited production in Southern ones, related to the natural protection of dark skin phenotypes toward light together with a diffused poor nutritional status, may represent possible cofactors of this evidence (64–66). Variable percentages of insufficiency/deficiency reported in the literature may be linked also to the variability of the screening methods, which often use improper terminologies and cut-offs. The universal application of unnecessary (and expensive) routine supplementations in a healthy population does not have a scientific rationale. Moreover, there is currently no scientific evidence to recommend vitamin D supplementation in the treatment and prevention of diseases like asthma, allergic, or immune disorders (67).
Consequently, it might be considered if and how a vitamin D deficiency may be responsible for so many different diseases. A meaningful point is represented by the lack of knowledge among clinicians about the current reference values of hypovitaminosis, probably related to the frequent and ambiguous use of terms such as “deficiency,” “sufficiency,” “adequacy,” or “insufficiency” (68, 69). As a consequence, surveys conducted on the general population and based on inappropriate cut-off values have sometimes led to unnecessary supplementations in healthy populations (52, 70, 71).
The threshold value about hypovitaminosis (and therefore “deficiency,” and not “insufficiency”) is debated (72–74), but according to some authorities we suggest considering adequate levels above 30 ng/mL (75 nmol/L). Values included in the range of 20–29 ng/mL (50–74 nmol/L) are then to be considered “insufficient” (Table 1) (75, 76). Furthermore, with the exception of subjects at risk of hypovitaminosis or those who may require supplementation (e.g., inadequate dietary intake), no screening of serum 25(OH)D dosages is recommended, nor an arbitrary or medically unjustified exogenous administration should be generally performed before verifying an effective deficiency/insufficiency (77, 78).

Table 1. Suggested cut-off values for the definition of vitamin D status based on circulating levels of 25(OH)D (74).
Several risk factors are associated with vitamin D deficiency in children and may be considered by clinicians upon deciding whether blood serum screening and/or vitamin D supplementation should be started.
The levels of vitamin D may also be influenced by ethnicity, genetic predispositions, and skin types, with darker skin types requiring more sunlight exposure to absorb vitamin D (72, 79–81). Lastly, there is a risk for vitamin D deficiency also for pediatric and adult subjects who are treated with certain medications (e.g., anti-epileptics, and glucocorticoids) and for patients with chronic diseases which prevent vitamin D intestinal absorption, such as celiac disease or cystic fibrosis, but also diseases which impact the liver, or the kidneys, preventing physiologic vitamin D metabolism (72, 82–85).
Another major risk factor of vitamin D deficiency is the insufficient sunlight exposure, which affects the body’s capacity to produce vitamin D (86, 87). Therefore, spending most of the time indoors or living in regions where the weather is mostly cloudy, and cold represents a risk for vitamin D deficiency. Accordingly, other factors such as latitude, and altitude, which directly impact the sun angle and ultraviolet radiations may impact vitamin D status (72).
Another known risk factor for vitamin D deficiency is related to age, with infants being more at risk of developing hypovitaminosis. Under 12 months of age, the risk is even higher for premature babies, who have less vitamin D deposits, and in children who are breastfed (88). Indeed, human breast milk is almost lacking in proper amounts of vitamin D, with concentrations that range from 10 to 80 IU/L in healthy lactating women, depending on the method of measurement (88, 89).
Considering the first 6 months of age, mothers who are lacking in vitamin D, supply even fewer amounts to their infants, while, higher breast milk quantities of vitamin D positively correlate with higher mother 25(OH)D serum levels (90–92). The rapid conversion of cholecalciferol to 25(OH)D in the mother’s liver represents another obstacle to a high passage of vitamin D, and it is maybe one of the main reasons for the 0.2 ratio between maternal and breast milk 25(OH)D (93).
The main problem of infants exclusively breastfed by mothers supplemented with 400 IU/day, the typical amount assumed during pregnancy, is the typical deficiency reported in this population (94, 95). Moreover, breastfed infants typically lack in adequate sunlight exposure and the administration could be affected by poor parental compliance (96, 97).
When exclusive breastfeeding is no longer sufficient to meet all the nutritional needs, it is, therefore, necessary to introduce other foods and liquids. This period is known as “complementary feeding” or “weaning,” and should generally be started after 6 months of life, with partial breastfeeding that may continue approximately up to 2 years of age (98).
Low dietary intake of vitamin D remains a common reason for vitamin D deficiency even in older children/adolescents, especially in overweight and obese individuals. Moreover, overweight and obese subjects are more at risk of low blood levels of vitamin D, as adiposity may prevent vitamin D release from the deposits in the fatty tissue and therefore its bioavailability (66, 99).
For all the mentioned reasons, most international and national guidelines actually recommend vitamin D prophylaxis to all infants during the first year of life, in order to prevent possible deficiency conditions and in consideration of the frequent, unpredictable, and often insufficient supply typical of the early infancy (73, 74). It has been estimated that infant formulas are able to provide appropriate amounts of vitamin D (400 IU/day) only once an average intake of at least 1 l of milk per day has been reached, which generally takes place when the baby’s body weight is more than 6 kg (100). Moreover, even if cholecalciferol (vitamin D3) seems to be more effective in raising 25(OH)D levels, there is no proven difference between the administration of ergocalciferol (D2) or D3 formulation in preventing possible deficiencies (101, 102). Dosages above 400 IU/day did not show significant differences in vitamin D sufficiency rates and bone health during the first year of life (94). Higher intakes have been suggested only in preterm births; in fact, the European Society of Pediatric Gastroenterology, Nutrition, and Hepatology (ESPGHAN) recommends prophylaxis with 800–1,000 IU/day (avoiding a pro kg dosage) during the first months of the preterm, in order to quickly correct the reduced infants’ levels of 25(OH)D, thus reducing the risk of symptomatic deficiencies (103). As for breastfeeding, although some recommendations advise for maternal supplementation of 600 IU per day, some data suggest that this practice does not significantly change the concentration of 25(OH)D in breast milk, which is generally poor in vitamin D (93). For this reason, the American Academy of Pediatrics recommends supplementing all breastfed and partially breastfed infants, regardless of maternal supplementation (88). However, adherence to these recommendations is low (104). Furthermore, due to the poor evidence to assess the benefits of supplementation for improving maternal and infant health outcomes, the World Health Organization (WHO) does not recommend routine vitamin D supplementation in pregnant women (105).
In consideration of the low levels of adherence to a daily administration of vitamin D found in many populations that differed for geographic and socioeconomic conditions, alternative approaches to a daily supplementation based on high doses (up to 6,400 IU/day) given directly to fully breastfeeding mothers have been found to be safe and equally effective in maintaining adequate levels of 25(OH)D, as well as monthly administrations of 50,000 IU given directly to infants (94, 104, 106–110).
After 12 months of life, evidence about pediatric vitamin D supplementation needs is less clear and univocal (111–114). A case-by-case evaluation of the toddler, child, and young adult lifestyle has then been recommended, to correct possible modifiable risk factors when present, particularly in adolescents, by virtue of their increased needs related to major skeletal growth and also the pubertal spurt (99). Any supplementation is therefore only indicated in cases of poor sun exposure or in specific conditions (111). This approach is also supported by WHO, which focuses the indication on vitamin D supplementation more on geographical location and sun exposure than on child age (115). As for the administration of fortified foods in early childhood, the consumption of vitamin D-fortified milk between 2 and 6 years may represent a safe and significantly effective nutritional measure in preventing 25(OH)D insufficiency during periods of reduced sunlight exposure (116–119). On the other hand, other societies, such as the Endocrine Society and the Institute of Medicine, recommend an average vitamin D intake of 600–1,000 IU/d between 1 and 18 years of age (120, 121).
Considering these discrepant recommendations, the inconclusive data on this issue, and that universal screening of 25(OH)D serum levels cannot represent a feasible solution, new studies should assess if vitamin D evaluation in selected cases would be more appropriate and cost-effective than a routinary, continued, and widespread supplementation.
As was observed 10 years ago in the Consensus statement by the ESPGHAN Nutritional Committee, data on vitamin D concentration and vitamin D deficiency in healthy pediatric subjects are limited, with a lack of consistency in terms of study design and definition of vitamin D deficiency (72). From the studies examined in the statement, it appears that a considerable number of healthy European children and adolescents may be expected to be vitamin D deficient (122–134).
Besides, routine vitamin D screening in healthy children is currently not recommended by experts globally, which partially explains the lack of data and systematization of literature regarding vitamin D status in healthy subjects (73).
Finally, although there are few reports on possible damages from high levels of exogenous administration of vitamin D for example, in cases of mutation of the 24-hydroxylase gene or in sporadic cases of overdosages, possible conditions such as hypercalcemia and hypercalciuria might occur, leading up to acute symptoms such as pain, fever, chills, anorexia, and later to soft tissue calcification, and related chronic pathologies such as nephrocalcinosis in case of prolonged overdosages (135, 136). The issue is still discussed in the hypothesis of either a rare genetic predisposition, or real differences in comparison with the expected spontaneous epidemiological distribution of cases. Cases of vitamin D intoxication have been described only for serum levels above 150 ng/mL (137).
It should be once more stressed that vitamin D levels can significantly vary depending on the lifestyle and overall exposure to ultraviolet B rays, which is affected by factors such as geographic location, age, skin, and family habits (66, 138, 139). In newborns and infants, other factors may well affect vitamin D status such as season of birth, maternal prophylaxis in pregnancy, type of breastfeeding, human milk variable individual composition, and the family socioeconomic status (140, 141). Recently, the rising rate of obesity and the lipophilic nature of vitamin D have suggested the need for higher quantities of vitamin D for these subjects, up to at least 1,000–1,500 IU/day (99, 142).
The 25(OH)D serum dosage should be cautiously considered in clinical practice. The National Institute for Health and Care Excellence (NICE) guidelines recommend dosing 25(OH)D serum only in patients with signs of hypovitaminosis, or in the presence of documented risk factors that justifies their dosage (143). Instead, a 6-month 25(OH)D dosage may be appropriate in supplemented patients to evaluate its effectiveness or to consider whether to suspend it.
In Table 2, we summarize different guidelines and statements for supplementation.
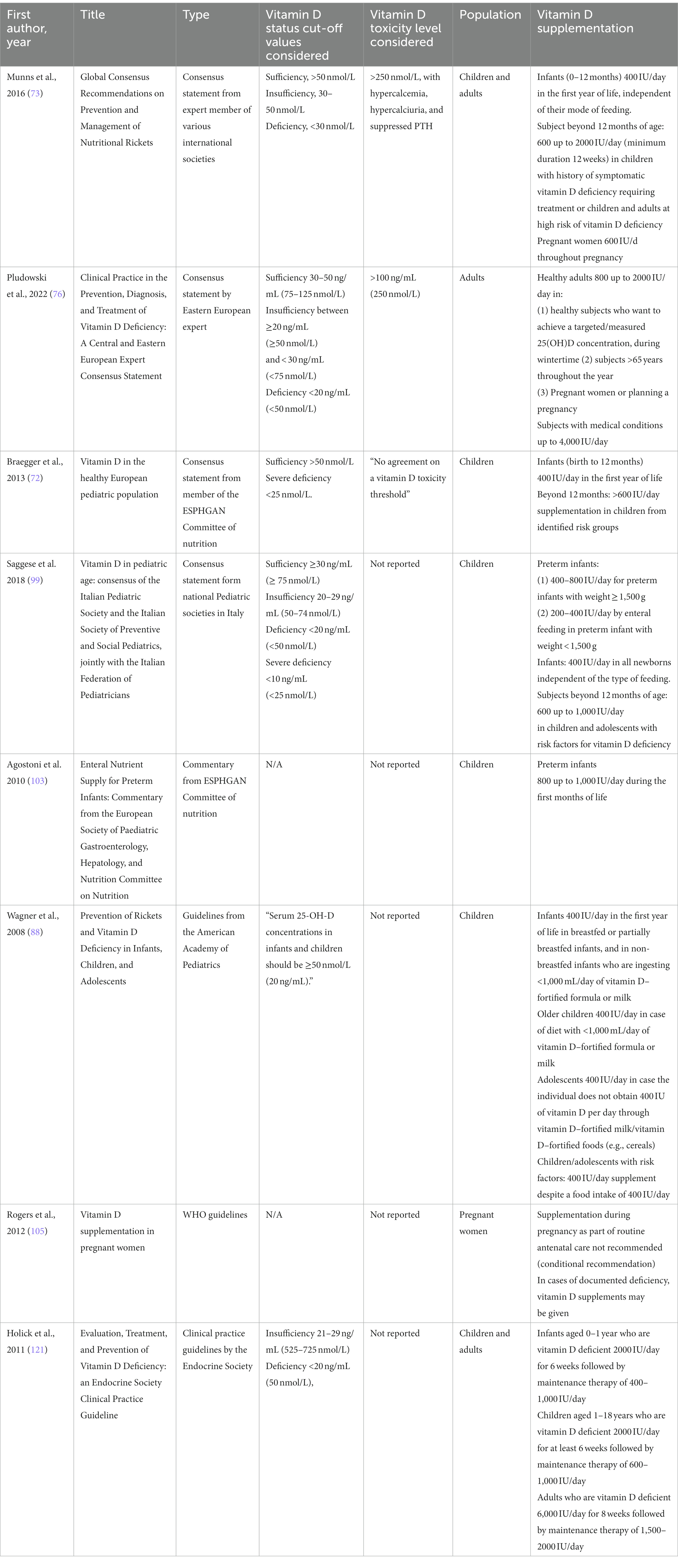
Table 2. Different guidelines for vitamin D supplementation.
All children during the first year of life should receive an oral supplementation of vitamin D. Beyond this age, geographic and cultural variability should always be considered by clinicians and scientific societies in recommending, or not, the need for supplementation. Vitamin D status may be closely connected to social inequities and related diseases. Moreover, constant and unjustified monitoring of vitamin D levels has then been considered unnecessary in the general population. Screening of serum 25(OH)D concentration should be carried out only in selected cases.
All authors listed have made a substantial, direct, and intellectual contribution to the work and approved it for publication.
This study was partially funded by Italian Ministry of Health—Current research IRCCS.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. McCollum, EV, Simmonds, N, Becker, JE, and Shipley, PG. Studies on experimental rickets: XXI an experimental demonstration of the existence of a vitamin which promotes calcium deposition. J Biol Chem. (1922) 53:293–312. doi: 10.1016/S0021-9258(18)85783-0
2. Zmijewski, MA. Vitamin D and human health. Int J Mol Sci. (2019) 20:145. doi: 10.3390/ijms20010145
3. Bendik, I, Friedel, A, Roos, FF, Weber, P, and Eggersdorfer, M. Vitamin D: a critical and essential micronutrient for human health. Front Physiol. (2014) 5:248. doi: 10.3389/fphys.2014.00248
4. Roth, DE, Abrams, SA, Aloia, J, Bergeron, G, Bourassa, MW, Brown, KH, et al. Global prevalence and disease burden of vitamin D deficiency: a roadmap for action in low- and middle-income countries. Ann N Y Acad Sci. (2018) 1430:44–79. doi: 10.1111/nyas.13968
5. Constantini, NW, Arieli, R, Chodick, G, and Dubnov-Raz, G. High prevalence of vitamin D insufficiency in athletes and dancers. Clin J Sport Med. (2010) 20:368–71. doi: 10.1097/JSM.0b013e3181f207f2
6. Holick, MF. High prevalence of Vitamin D inadequacy and implications for health. Mayo Clin Proc. (2006) 81:353–73. doi: 10.4065/81.3.353
7. Palacios, C, and Gonzalez, L. Is vitamin D deficiency a major global public health problem? J Steroid Biochem Mol Biol (2014) 144PA:138–145. doi: 10.1016/j.jsbmb.2013.11.003, 144
8. Allgrove, J. Physiology of calcium, phosphate and magnesium. Endocr Dev. (2009) 16:8–31. doi: 10.1159/000223685
9. Uwitonze, AM, and Razzaque, MS. Role of magnesium in Vitamin D activation and function. J Am Osteopath Assoc. (2018) 118:181–9. doi: 10.7556/jaoa.2018.037
10. Reddy, P, and Edwards, LR. Magnesium supplementation in Vitamin D deficiency. Am J Ther. (2019) 26:e124–32. doi: 10.1097/MJT.0000000000000538
11. Allgrove, J, and Shaw, NJ. A practical approach to Vitamin D deficiency and rickets. Endocr Dev. (2015) 28:119–33. doi: 10.1159/000381000
12. Uday, S, and Högler, W. Nutritional rickets and Osteomalacia in the twenty-first century: revised concepts, public health, and prevention strategies. Curr Osteoporos Rep. (2017) 15:293–302. doi: 10.1007/s11914-017-0383-y
13. Grad, R. Cod and the consumptive: a brief history of cod-liver oil in the treatment of pulmonary tuberculosis. Pharm Hist. (2004) 46:106–20.
14. Cervantes, JL, Oak, E, Garcia, J, Liu, H, Lorenzini, PA, Batra, D, et al. Vitamin D modulates human macrophage response to mycobacterium tuberculosis DNA. Tuberculosis (Edinb). (2019) 116:S131–7. doi: 10.1016/j.tube.2019.04.021
15. Dankers, W, Colin, EM, van Hamburg, JP, and Lubberts, E. Vitamin D in autoimmunity: molecular mechanisms and therapeutic potential. Front Immunol. (2016) 7:697. doi: 10.3389/fimmu.2016.00697
16. Kamen, DL, and Tangpricha, V. Vitamin D and molecular actions on the immune system: modulation of innate and autoimmunity. J Mol Med. (2010) 88:441–50. doi: 10.1007/s00109-010-0590-9
17. Altieri, B, Muscogiuri, G, Barrea, L, Mathieu, C, Vallone, CV, Mascitelli, L, et al. Does vitamin D play a role in autoimmune endocrine disorders? A proof of concept. Rev Endocr Metab Disord. (2017) 18:335–46. doi: 10.1007/s11154-016-9405-9
18. Prietl, B, Treiber, G, Pieber, TR, and Amrein, K. Vitamin D and immune function. Nutrients. (2013) 5:2502–21. doi: 10.3390/nu5072502
19. Bizzaro, G, and Shoenfeld, Y. Vitamin D and autoimmune thyroid diseases: facts and unresolved questions. Immunol Res. (2015) 61:46–52. doi: 10.1007/s12026-014-8579-z
20. Dimeloe, S, Nanzer, A, Ryanna, K, and Hawrylowicz, C. Regulatory T cells, inflammation and the allergic response—the role of glucocorticoids and Vitamin D. J Steroid Biochem Mol Biol (2010) 120:86–95. doi: 10.1016/j.jsbmb.2010.02.029
21. Chen, S, Sims, GP, Chen, XX, Gu, YY, Chen, S, and Lipsky, PE. Modulatory effects of 1,25-dihydroxyvitamin D3 on human B cell differentiation. J Immunol. (2007) 179:1634–47. doi: 10.4049/jimmunol.179.3.1634
22. Sassi, F, Tamone, C, and D’Amelio, P. Vitamin D: nutrient, hormone, and immunomodulator. Nutrients. (2018) 10:1656. doi: 10.3390/nu10111656
23. Maddaloni, E, Cavallari, I, Napoli, N, and Conte, C. Vitamin D and Diabetes Mellitus. Front Horm Res. (2018) 50:161–76. doi: 10.1159/000486083
24. Moltchanova, E V, Schreier, N, Lammi, N, and Karvonen, M. Seasonal variation of diagnosis of type1 diabetes mellitus in children worldwide. Diabet Med (2009) 26:673–678. doi: 10.1111/j.1464-5491.2009.02743.x
25. Stene, LC, and Joner, G. Use of cod liver oil during the first year of life is associated with lower risk of childhood-onset type 1 diabetes: a large, population-based, case-control study. Am J Clin Nutr. (2003) 78:1128–34. doi: 10.1093/ajcn/78.6.1128
26. Marjamäki, L, Niinistö, S, Kenward, MG, Uusitalo, L, Uusitalo, U, Ovaskainen, M-L, et al. Maternal intake of vitamin D during pregnancy and risk of advanced beta cell autoimmunity and type 1 diabetes in offspring. Diabetologia. (2010) 53:1599–607. doi: 10.1007/s00125-010-1734-8
27. Zipitis, CS, and Akobeng, AK. Vitamin D supplementation in early childhood and risk of type 1 diabetes: a systematic review and meta-analysis. Arch Dis Child. (2008) 93:512–7. doi: 10.1136/adc.2007.128579
28. Infante, M, Ricordi, C, Sanchez, J, Clare-Salzler, MJ, Padilla, N, Fuenmayor, V, et al. Influence of Vitamin D on islet autoimmunity and Beta-cell function in type 1 diabetes. Nutrients. (2019) 11:2185. doi: 10.3390/nu11092185
29. Li, X, Liao, L, Yan, X, Huang, G, Lin, J, Lei, M, et al.. Protective effects of 1-α-hydroxyvitamin D3 on residual β-cell function in patients with adult-onset latent autoimmune diabetes (LADA). Diabetes Metab Res Rev (2009) 25:411–416. doi: 10.1002/dmrr.977
30. Ataie-Jafari, A, Loke, S-C, Rahmat, AB, Larijani, B, Abbasi, F, Leow, MKS, et al. A randomized placebo-controlled trial of alphacalcidol on the preservation of beta cell function in children with recent onset type 1 diabetes. Clin Nutr. (2013) 32:911–7. doi: 10.1016/j.clnu.2013.01.012
31. Dong, J-Y, Zhang, W-G, Chen, JJ, Zhang, Z-L, Han, S-F, and Qin, L-Q. Vitamin D intake and risk of type 1 diabetes: a meta-analysis of observational studies. Nutrients. (2013) 5:3551–62. doi: 10.3390/nu5093551
32. Wang, J, Lv, S, Chen, G, Gao, C, He, J, Zhong, H, et al. Meta-analysis of the association between Vitamin D and autoimmune thyroid disease. Nutrients. (2015) 7:2485–98. doi: 10.3390/nu7042485
33. Muscogiuri, G, Mari, D, Prolo, S, Fatti, LM, Cantone, MC, Garagnani, P, et al. 25 Hydroxyvitamin D deficiency and its relationship to autoimmune thyroid disease in the elderly. Int J Environ Res Public Health. (2016) 13:850. doi: 10.3390/ijerph13090850
34. Sönmezgöz, E, Ozer, S, Yilmaz, R, Önder, Y, Bütün, I, and Bilge, S. Hypovitaminosis D in children with Hashimoto’s thyroiditis. Revista Medica de Chile. (2016) 144:611–6. doi: 10.4067/S0034-98872016000500009
35. Gubatan, J, and Moss, AC. Vitamin D in inflammatory bowel disease: more than just a supplement. Curr Opin Gastroenterol. (2018) 34:217–25. doi: 10.1097/MOG.0000000000000449
36. Corsello, A, Pugliese, D, Gasbarrini, A, and Armuzzi, A. Diet and nutrients in gastrointestinal chronic diseases. Nutrients. (2020) 12:2693. doi: 10.3390/nu12092693
37. Lim, W-C, Hanauer, SB, and Li, YC. Mechanisms of disease: vitamin D and inflammatory bowel disease. Nat Clin Pract Gastroenterol Hepatol. (2005) 2:308–15. doi: 10.1038/ncpgasthep0215
38. Limketkai, BN, Mullin, GE, Limsui, D, and Parian, AM. Role of Vitamin D in inflammatory bowel disease. Nutr Clin Pract. (2017) 32:337–45. doi: 10.1177/0884533616674492
39. Del Pinto, R, Pietropaoli, D, Chandar, AK, Ferri, C, and Cominelli, F. Association between inflammatory bowel disease and Vitamin D deficiency: a systematic review and meta-analysis. Inflamm Bowel Dis. (2015) 21:2708–17. doi: 10.1097/MIB.0000000000000546
40. Zhao, J, Wang, Y, Gu, Q, Du, Z, and Chen, W. The association between serum vitamin D and inflammatory bowel disease. Medicine. (2019) 98:e15233–3. doi: 10.1097/MD.0000000000015233
41. Liu, W, Chen, Y, Golan, MA, Annunziata, ML, du, J, Dougherty, U, et al. Intestinal epithelial vitamin D receptor signaling inhibits experimental colitis. J Clin Invest. (2013) 123:3983–96. doi: 10.1172/JCI65842
42. Illescas-Montes, R, Melguizo-Rodríguez, L, Ruiz, C, and Costela-Ruiz, VJ. Vitamin D and autoimmune diseases. Life Sci. (2019) 233:116744. doi: 10.1016/j.lfs.2019.116744
43. Fletcher, J, Cooper, SC, Ghosh, S, and Hewison, M. The role of Vitamin D in inflammatory bowel disease: mechanism to management. Nutrients. (2019) 11:1019. doi: 10.3390/nu11051019
44. Dipasquale, V, Lo Presti, G, Milani, GP, Corsello, A, Agostoni, C, and Romano, C. Vitamin D in prevention of autoimmune diseases. Front Biosci. (2022) 27:288. doi: 10.31083/j.fbl2710288
45. Reich, KM, Fedorak, RN, Madsen, K, and Kroeker, KI. Vitamin D improves inflammatory bowel disease outcomes: basic science and clinical review. World J Gastroenterol. (2014) 20:4934–47. doi: 10.3748/wjg.v20.i17.4934
46. Yang, L, Weaver, V, Smith, JP, Bingaman, S, Hartman, TJ, and Cantorna, MT. Therapeutic effect of vitamin d supplementation in a pilot study of Crohn’s patients. Clin Transl Gastroenterol. (2013) 4:e33–3. doi: 10.1038/ctg.2013.1
47. Wang, X-R, Xiao, J-P, Zhang, J-J, and Wu, Y-G. Decreased serum/plasma Vitamin D levels in SLE patients: a meta-analysis. Curr Pharm Des. (2018) 24:4466–73. doi: 10.2174/1381612825666190111145848
48. Zhang, J, Li, W, Liu, J, Wu, W, Ouyang, H, Zhang, Q, et al. Polymorphisms in the vitamin D receptor gene and type 1 diabetes mellitus risk: an update by meta-analysis. Mol Cell Endocrinol (2012) 355:135–142. doi: 10.1016/j.mce.2012.02.003
49. Feng, M, Li, H, Chen, S-F, Li, W-F, and Zhang, F-B. Polymorphisms in the vitamin D receptor gene and risk of autoimmune thyroid diseases: a meta-analysis. Endocrine. (2013) 43:318–26. doi: 10.1007/s12020-012-9812-y
50. Tizaoui, K, Kaabachi, W, Hamzaoui, A, and Hamzaoui, K. Association between vitamin D receptor polymorphisms and multiple sclerosis: systematic review and meta-analysis of case–control studies. Cell Mol Immunol. (2015) 12:243–52. doi: 10.1038/cmi.2014.47
51. Lee, YH, and Bae, S-C. Vitamin D level in rheumatoid arthritis and its correlation with the disease activity: a meta-analysis. Clin Exp Rheumatol. (2016) 34:827–33.
52. Amrein, K, Scherkl, M, Hoffmann, M, Neuwersch-Sommeregger, S, Köstenberger, M, Tmava Berisha, A, et al. Vitamin D deficiency 2.0: an update on the current status worldwide. Eur J Clin Nutr. (2020) 74:1498–513. doi: 10.1038/s41430-020-0558-y
53. Aranow, C. Vitamin D and the immune system. J Investig Med. (2011) 59:881–6. doi: 10.231/JIM.0b013e31821b8755
54. Cantorna, MT, and Vitamin, D. Multiple sclerosis and inflammatory bowel disease. Arch Biochem Biophys. (2012) 523:103–6. doi: 10.1016/j.abb.2011.11.001
55. Forno, E, Bacharier, LB, Phipatanakul, W, Guilbert, TW, Cabana, MD, Ross, K, et al. Effect of Vitamin D3 supplementation on severe asthma exacerbations in children with asthma and low Vitamin D levels: the VDKA randomized clinical trial. JAMA. (2020) 324:752–60. doi: 10.1001/jama.2020.12384
56. Brenner, H, and Vitamin, D. Supplementation to prevent COVID-19 infections and deaths-accumulating evidence from epidemiological and intervention studies calls for immediate action. Nutrients. (2021) 13:411. doi: 10.3390/nu13020411
57. Panfili, FM, Roversi, M, D’Argenio, P, Rossi, P, Cappa, M, and Fintini, D. Possible role of vitamin D in Covid-19 infection in pediatric population. J Endocrinol Investig. (2021) 44:27–35. doi: 10.1007/s40618-020-01327-0
58. Martineau, AR, and Forouhi, NG. Vitamin D for COVID-19: a case to answer? Lancet Diabetes Endocrinol. (2020) 8:735–6. doi: 10.1016/S2213-8587(20)30268-0
59. Yisak, H, Ewunetei, A, Kefale, B, Mamuye, M, Teshome, F, Ambaw, B, et al. Effects of Vitamin D on COVID-19 infection and prognosis: a systematic review. Risk Manag Healthc Policy. (2021) 14:31–8. doi: 10.2147/RMHP.S291584
60. Gordon, CM, Feldman, HA, Sinclair, L, Williams, AL, Kleinman, PK, Perez-Rossello, J, et al. Prevalence of Vitamin D deficiency among healthy infants and toddlers. Arch Pediatr Adolesc Med. (2008) 162:505–12. doi: 10.1001/archpedi.162.6.505
61. Zhu, Z, Zhan, J, Shao, J, Chen, W, Chen, L, Li, W, et al. High prevalence of vitamin D deficiency among children aged 1 month to 16 years in Hangzhou, China. BMC Public Health. (2012) 12:126. doi: 10.1186/1471-2458-12-126
62. Kumar, J, Muntner, P, Kaskel, FJ, Hailpern, SM, and Melamed, ML. Prevalence and associations of 25-Hydroxyvitamin D deficiency in US children: NHANES 2001–2004. Pediatrics. (2009) 124:e362–70. doi: 10.1542/peds.2009-0051
63. Haimi, M, and Kremer, R. Vitamin D deficiency/insufficiency from childhood to adulthood: insights from a sunny country. World J Clin Pediatr. (2017) 6:1–9. doi: 10.5409/wjcp.v6.i1.1
64. Engelsen, O. The relationship between ultraviolet radiation exposure and Vitamin D status. Nutrients. (2010) 2:482–95. doi: 10.3390/nu2050482
65. Dawodu, A, Davidson, B, Woo, JG, Peng, Y-M, Ruiz-Palacios, GM, de Lourdes Guerrero, M, et al. Sun exposure and Vitamin D supplementation in relation to Vitamin D status of Breastfeeding mothers and infants in the global exploration of human Milk study. Nutrients. (2015) 7:1081–93. doi: 10.3390/nu7021081
66. Tsiaras, WG, and Weinstock, MA. Factors influencing vitamin D status. Acta Derm Venereol. (2011) 91:115–24. doi: 10.2340/00015555-0980
67. Della Giustina, A, Landi, M, Bellini, F, Bosoni, M, Ferrante, G, Onorari, M, et al. Vitamin D, allergies and asthma: focus on pediatric patients. World Allergy Organ J. (2014) 7:27–6. doi: 10.1186/1939-4551-7-27
68. Sempos, CT, Heijboer, AC, Bikle, DD, Bollerslev, J, Bouillon, R, Brannon, PM, et al. Vitamin D assays and the definition of hypovitaminosis D: results from the first international conference on controversies in Vitamin D. Br J Clin Pharmacol. (2018) 84:2194–207. doi: 10.1111/bcp.13652
69. Kennel, KA, Drake, MT, and Hurley, DL. Vitamin D deficiency in adults: when to test and how to treat. Mayo Clin Proc. (2010) 85:752–8. doi: 10.4065/mcp.2010.0138
70. Manson, JE, Brannon, PM, Rosen, CJ, and Taylor, CL. Vitamin D deficiency — is there really a pandemic? N Engl J Med. (2016) 375:1817–20. doi: 10.1056/NEJMp1608005
71. Haines, ST, and Park, SK. Vitamin D supplementation: what’s known, what to do, and what’s needed. Pharmacotherapy. (2012) 32:354–82. doi: 10.1002/phar.1037
72. Braegger, C, Campoy, C, Colomb, V, Decsi, T, Domellof, M, Fewtrell, M, et al. Vitamin D in the healthy European paediatric population. J Pediatr Gastroenterol Nutr. (2013) 56:692–701. doi: 10.1097/MPG.0b013e31828f3c05
73. Munns, CF, Shaw, N, Kiely, M, Specker, BL, Thacher, TD, Ozono, K, et al. Global consensus recommendations on prevention and Management of Nutritional Rickets. J Clin Endocrinol Metab. (2016) 101:394–415. doi: 10.1210/jc.2015-2175
74. Saggese, G, Vierucci, F, Prodam, F, Cardinale, F, Cetin, I, Chiappini, E, et al. Vitamin D in pediatric age: consensus of the Italian pediatric society and the Italian Society of Preventive and Social Pediatrics, jointly with the Italian Federation of Pediatricians. Ital J Pediatr. (2018) 44:51. doi: 10.1186/s13052-018-0488-7
75. Holick, MF, and Vitamin, D. Deficiency. N Engl J Med. (2007) 357:266–81. doi: 10.1056/NEJMra070553
76. Kimball, SM, and Holick, MF. Official recommendations for vitamin D through the life stages in developed countries. Eur J Clin Nutr. (2020) 74:1514–8. doi: 10.1038/s41430-020-00706-3
77. Pludowski, P, Takacs, I, Boyanov, M, Belaya, Z, Diaconu, CC, Mokhort, T, et al. Clinical practice in the prevention, diagnosis and treatment of Vitamin D deficiency: a central and eastern European expert consensus statement. Nutrients. (2022) 14:1483. doi: 10.3390/nu14071483
78. Bleizgys, A, and Vitamin, D. Dosing: basic principles and a brief algorithm (2021 update). Nutrients. (2021) 13:4415. doi: 10.3390/nu13124415
79. Martin, CA, Gowda, U, and Renzaho, AMN. The prevalence of vitamin D deficiency among dark-skinned populations according to their stage of migration and region of birth: a meta-analysis. Nutrition. (2016) 32:21–32. doi: 10.1016/j.nut.2015.07.007
80. Akbari, AR, Khan, M, Adeboye, W, Hai Lee, LH, and Chowdhury, SI. Ethnicity as a risk factor for vitamin D deficiency and undesirable COVID-19 outcomes. Rev Med Virol. (2022) 32:e2291. doi: 10.1002/rmv.2291
81. Bahrami, A, Sadeghnia, HR, Tabatabaeizadeh, S-A, Bahrami-Taghanaki, H, Behboodi, N, Esmaeili, H, et al. Genetic and epigenetic factors influencing vitamin D status. J Cell Physiol. (2018) 233:4033–43. doi: 10.1002/jcp.26216
82. Cuppari, L, and Garcia-Lopes, MG. Hypovitaminosis D in chronic kidney disease patients: prevalence and treatment. J Ren Nutr. (2009) 19:38–43. doi: 10.1053/j.jrn.2008.10.005
83. Shaikh, AS, Guo, X, Li, Y, Cao, L, Liu, X, Li, P, et al. The impact of antiepileptic drugs on Vitamin levels in epileptic patients. Curr Pharm Biotechnol. (2018) 19:674–81. doi: 10.2174/1389201019666180816104716
84. Zhang, R, and Naughton, DP. Vitamin D in health and disease: current perspectives. Nutr J. (2010) 9:65. doi: 10.1186/1475-2891-9-65
85. Dominguez, LJ, Farruggia, M, Veronese, N, and Barbagallo, M. Vitamin D sources, metabolism, and deficiency: available compounds and guidelines for its treatment. Meta. (2021) 11:255. doi: 10.3390/metabo11040255
86. Holick, MF. The vitamin D deficiency pandemic: approaches for diagnosis, treatment and prevention. Rev Endocr Metab Disord. (2017) 18:153–65. doi: 10.1007/s11154-017-9424-1
87. Wacker, M, and Holick, MF. Sunlight and Vitamin D: a global perspective for health. Dermatoendocrinol. (2013) 5:51–108. doi: 10.4161/derm.24494
88. Chang, S-W, and Lee, H-C. Vitamin D and health - the missing vitamin in humans. Pediatr Neonatol. (2019) 60:237–44. doi: 10.1016/j.pedneo.2019.04.007
89. Wagner, CL, and Greer, FR, the Section on Breastfeeding and Committee on Nutrition. Prevention of rickets and Vitamin D deficiency in infants, children, and adolescents. Pediatrics. (2008) 122:1142–52. doi: 10.1542/peds.2008-1862
90. Tsugawa, N, Nishino, M, Kuwabara, A, Ogasawara, H, Kamao, M, Kobayashi, S, et al. Comparison of Vitamin D and 25-Hydroxyvitamin D concentrations in human breast Milk between 1989 and 2016-2017. Nutrients. (2021) 13:573. doi: 10.3390/nu13020573
91. Anusha, K, Hettiaratchi, U, Gunasekera, D, Prathapan, S, and Liyanage, G. Maternal Vitamin D status and its effect on Vitamin D levels in early infancy in a tertiary Care Centre in Sri Lanka. Int J Endocrinol. (2019) 2019:9017951–6. doi: 10.1155/2019/9017951
92. Jan Mohamed, HJ, Rowan, A, Fong, B, and Loy, S-L. Maternal serum and breast milk vitamin D levels: findings from the Universiti Sains Malaysia pregnancy cohort study. PLoS One. (2014) 9:e100705–5. doi: 10.1371/journal.pone.0100705
93. Wagner, CL, Taylor, SN, Johnson, DD, and Hollis, BW. The role of vitamin D in pregnancy and lactation: emerging concepts. Women's Health (Lond Engl). (2012) 8:323–40. doi: 10.2217/whe.12.17
94. Hollis, BW, Wagner, CL, Howard, CR, Ebeling, M, Shary, JR, Smith, PG, et al. Maternal versus infant Vitamin D supplementation during lactation: a randomized controlled trial. Pediatrics. (2015) 136:625–34. doi: 10.1542/peds.2015-1669
95. Corsello, A, Milani, GP, Giannì, ML, Dipasquale, V, Romano, C, and Agostoni, C. Different Vitamin D supplementation strategies in the first years of life: a systematic review. Healthcare. (2022) 10:1023. doi: 10.3390/healthcare10061023
96. Meena, P, Dabas, A, Shah, D, Malhotra, RK, Madhu, SV, and Gupta, P. Sunlight exposure and Vitamin D status in breastfed infants. Indian Pediatr. (2017) 54:105–11. doi: 10.1007/s13312-017-1010-9
97. Bae, YJ, and Kratzsch, J. Vitamin D and calcium in the human breast milk. Best Pract Res Clin Endocrinol Metab. (2018) 32:39–45. doi: 10.1016/j.beem.2018.01.007
98. Fewtrell, M, Bronsky, J, Campoy, C, Domellöf, M, Embleton, N, Fidler Mis, N, et al. Complementary feeding: a position paper by the European Society for Paediatric Gastroenterology, hepatology, and Nutrition (ESPGHAN) Committee on Nutrition. J Pediatr Gastroenterol Nutr. (2017) 64:119–32. doi: 10.1097/MPG.0000000000001454
99. Zakharova, I, Klimov, L, Kuryaninova, V, Nikitina, I, Malyavskaya, S, Dolbnya, S, et al. Vitamin D insufficiency in overweight and obese children and adolescents. Front Endocrinol (Lausanne). (2019) 10:103. doi: 10.3389/fendo.2019.00103
100. Dalle Carbonare, L, Valenti, MT, Del Forno, F, Caneva, E, and Pietrobelli, A. Vitamin D: Daily vs. Monthly use in children and elderly-what is going on? Nutrients. (2017) 9:E652. doi: 10.3390/nu9070652
101. Tripkovic, L, Lambert, H, Hart, K, Smith, CP, Bucca, G, Penson, S, et al. Comparison of vitamin D2 and vitamin D3 supplementation in raising serum 25-hydroxyvitamin D status: a systematic review and meta-analysis. Am J Clin Nutr. (2012) 95:1357–64. doi: 10.3945/ajcn.111.031070
102. Bilezikian, JP, Formenti, AM, Adler, RA, Binkley, N, Bouillon, R, Lazaretti-Castro, M, et al. Vitamin D: dosing, levels, form, and route of administration: does one approach fit all? Rev Endocr Metab Disord. (2021) 22:1201–18. doi: 10.1007/s11154-021-09693-7
103. Agostoni, C, Buonocore, G, Carnielli, VP, De Curtis, M, Darmaun, D, Decsi, T, et al. Enteral nutrient supply for preterm infants: commentary from the European Society of Paediatric Gastroenterology, hepatology and Nutrition Committee on Nutrition. J Pediatr Gastroenterol Nutr. (2010) 50:85–91. doi: 10.1097/MPG.0b013e3181adaee0
104. Perrine, CG, Sharma, AJ, Jefferds, MED, Serdula, MK, and Scanlon, KS. Adherence to vitamin D recommendations among US infants. Pediatrics. (2010) 125:627–32. doi: 10.1542/peds.2009-2571
105. World Health Organization. Guideline: vitamin D supplementation in pregnant women. Geneva: World Health Organization (2012).
106. Wheeler, BJ, Taylor, BJ, Herbison, P, Haszard, JJ, Mikhail, A, Jones, S, et al. High-dose monthly maternal cholecalciferol supplementation during Breastfeeding affects maternal and infant Vitamin D status at 5 months postpartum: a randomized controlled trial. J Nutr. (2016) 146:1999–2006. doi: 10.3945/jn.116.236679
107. Ahrens, KA, Rossen, LM, and Simon, AE. Adherence to Vitamin D recommendations among US infants aged 0 to 11 months, NHANES, 2009 to 2012. Clin Pediatr (Phila). (2016) 55:555–6. doi: 10.1177/0009922815589916
108. Hemmingway, A, Fisher, D, Berkery, T, Murray, DM, and Kiely, ME. Adherence to the infant vitamin D supplementation policy in Ireland. Eur J Nutr. (2021) 60:1337–45. doi: 10.1007/s00394-020-02334-w
109. O’Callaghan, KM, Taghivand, M, Zuchniak, A, Onoyovwi, A, Korsiak, J, Leung, M, et al. Vitamin D in breastfed infants: systematic review of alternatives to Daily supplementation. Adv Nutr. (2020) 11:144–59. doi: 10.1093/advances/nmz098
110. Tan, ML, Abrams, SA, and Osborn, DA. Vitamin D supplementation for term breastfed infants to prevent vitamin D deficiency and improve bone health. Cochrane Database Syst Rev (2018) 2018:CD013046. doi: 10.1002/14651858.CD013046
111. Day, RE, Krishnarao, R, Sahota, P, and Christian, MS. We still don’t know that our children need vitamin D daily: a study of parents’ understanding of vitamin D requirements in children aged 0-2 years. BMC Public Health. (2019) 19:1119. doi: 10.1186/s12889-019-7340-x
112. Martini, L, Pecoraro, L, Salvottini, C, Piacentini, G, Atkinson, R, and Pietrobelli, A. Appropriate and inappropriate vitamin supplementation in children. J Nutr Sci. (2020) 9:e20. doi: 10.1017/jns.2020.12
113. Taylor, SN. Vitamin D in toddlers, preschool children, and adolescents. Ann Nutr Metab. (2020) 76:30–41. doi: 10.1159/000505635
114. Patseadou, M, and Haller, DM. Vitamin D in adolescents: a systematic review and narrative synthesis of available recommendations. J Adolesc Health. (2020) 66:388–407. doi: 10.1016/j.jadohealth.2019.08.025
115. World Health Organization (2005). Vitamin and mineral requirements in human nutrition. Available at: https://apps.who.int/iris/handle/10665/42716
116. Akkermans, MD, Eussen, SR, van der Horst-Graat, JM, van Elburg, RM, van Goudoever, JB, and Brus, F. A micronutrient-fortified young-child formula improves the iron and vitamin D status of healthy young European children: a randomized, double-blind controlled trial. Am J Clin Nutr. (2017) 105:391–9. doi: 10.3945/ajcn.116.136143
117. Verduci, E, Di Profio, E, Corsello, A, Scatigno, L, Fiore, G, Bosetti, A, et al. Which Milk during the second year of life: a personalized choice for a healthy future? Nutrients. (2021) 13:3412. doi: 10.3390/nu13103412
118. Houghton, LA, Gray, AR, SzymLek-Gay, EA, Heath, A-LM, and Ferguson, EL. Vitamin D-fortified milk achieves the targeted serum 25-hydroxyvitamin D concentration without affecting that of parathyroid hormone in New Zealand toddlers. J Nutr. (2011) 141:1840–6. doi: 10.3945/jn.111.145052
119. Hower, J, Knoll, A, Ritzenthaler, KL, Steiner, C, and Berwind, R. Vitamin D fortification of growing up milk prevents decrease of serum 25-hydroxyvitamin D concentrations during winter: a clinical intervention study in Germany. Eur J Pediatr. (2013) 172:1597–605. doi: 10.1007/s00431-013-2092-6
120. Institute of Medicine (US) (2011). Committee to review dietary reference intakes for Vitamin D and calcium. Dietary reference intakes for calcium and Vitamin D. AC Ross, CL Taylor, AL Yaktine, and HB ValleDel, Washington (DC): National Academies Press (US).
121. Holick, MF, Binkley, NC, Bischoff-Ferrari, HA, Gordon, CM, Hanley, DA, Heaney, RP, et al. Evaluation, treatment, and prevention of vitamin D deficiency: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. (2011) 96:1911–30. doi: 10.1210/jc.2011-0385
122. Akman, AO, Tumer, L, Hasanoglu, A, Ilhan, M, and Caycı, B. Frequency of vitamin D insufficiency in healthy children between 1 and 16 years of age in Turkey. Pediatr Int. (2011) 53:968–73. doi: 10.1111/j.1442-200X.2011.03486.x
123. Andersen, R, Mølgaard, C, Skovgaard, LT, Brot, C, Cashman, KD, Chabros, E, et al. Teenage girls and elderly women living in northern Europe have low winter vitamin D status. Eur J Clin Nutr. (2005) 59:533–41. doi: 10.1038/sj.ejcn.1602108
124. Andersen, R, Mølgaard, C, Skovgaard, LT, Brot, C, Cashman, KD, Jakobsen, J, et al. Pakistani immigrant children and adults in Denmark have severely low vitamin D status. Eur J Clin Nutr. (2008) 62:625–34. doi: 10.1038/sj.ejcn.1602753
125. Das, G, Crocombe, S, McGrath, M, Berry, JL, and Mughal, MZ. Hypovitaminosis D among healthy adolescent girls attending an inner city school. Arch Dis Child. (2006) 91:569–72. doi: 10.1136/adc.2005.077974
126. Ginty, F, Cavadini, C, Michaud, P-A, Burckhardt, P, Baumgartner, M, Mishra, G-D, et al. Effects of usual nutrient intake and vitamin D status on markers of bone turnover in Swiss adolescents. Eur J Clin Nutr. (2004) 58:1257–65. doi: 10.1038/sj.ejcn.1601959
127. Grindulis, H, Scott, PH, Belton, NR, and Wharton, BA. Combined deficiency of iron and vitamin D in Asian toddlers. Arch Dis Child. (1986) 61:843–8. doi: 10.1136/adc.61.9.843
128. Guillemant, J, Le, HT, Maria, A, Allemandou, A, Pérès, G, and Guillemant, S. Wintertime vitamin D deficiency in male adolescents: effect on parathyroid function and response to vitamin D3 supplements. Osteoporos Int. (2001) 12:875–9. doi: 10.1007/s001980170040
129. Lapatsanis, D, Moulas, A, Cholevas, V, Soukakos, P, Papadopoulou, ZL, and Challa, A. Vitamin D: a necessity for children and adolescents in Greece. Calcif Tissue Int. (2005) 77:348–55. doi: 10.1007/s00223-004-0096-y
130. Lawson, M, and Thomas, M. Vitamin D concentrations in Asian children aged 2 years living in England: population survey. BMJ. (1999) 318:28. doi: 10.1136/bmj.318.7175.28
131. Lehtonen-Veromaa, MKM, Möttönen, TT, Nuotio, IO, Irjala, KMA, Leino, AE, and Viikari, JSA. Vitamin D and attainment of peak bone mass among peripubertal Finnish girls: a 3-y prospective study. Am J Clin Nutr. (2002) 76:1446–53. doi: 10.1093/ajcn/76.6.1446
132. Lippi, G, Montagnana, M, and Targher, G. Vitamin D deficiency among Italian children. CMAJ. (2007) 177:1529–30; author reply 1530. doi: 10.1503/cmaj.1070102
133. Østergård, M, Arnberg, K, Michaelsen, KF, Madsen, AL, Krarup, H, Trolle, E, et al. Vitamin D status in infants: relation to nutrition and season. Eur J Clin Nutr. (2011) 65:657–60. doi: 10.1038/ejcn.2010.285
134. Stellinga-Boelen, AAM, Wiegersma, PA, Storm, H, Bijleveld, CMA, and Verkade, HJ. Vitamin D levels in children of asylum seekers in the Netherlands in relation to season and dietary intake. Eur J Pediatr. (2007) 166:201–6. doi: 10.1007/s00431-006-0221-1
135. Marcinowska-Suchowierska, E, Kupisz-Urbańska, M, Łukaszkiewicz, J, Płudowski, P, and Jones, G. Vitamin D toxicity-a clinical perspective. Front Endocrinol (Lausanne). (2018) 9:550. doi: 10.3389/fendo.2018.00550
136. Dinour, D, Beckerman, P, Ganon, L, Tordjman, K, Eisenstein, Z, and Holtzman, EJ. Loss-of-function mutations of CYP24A1, the vitamin D 24-hydroxylase gene, cause long-standing hypercalciuric nephrolithiasis and nephrocalcinosis. J Urol. (2013) 190:552–7. doi: 10.1016/j.juro.2013.02.3188
137. Muneer, S, Siddiqui, I, Majid, H, Zehra, N, Jafri, L, and Khan, AH. Practices of vitamin D supplementation leading to vitamin D toxicity: experience from a low-middle income country. Ann Med Surg. (2022) 73:103227. doi: 10.1016/j.amsu.2021.103227
138. Rabufetti, A, Milani, GP, Lava, SAG, Edefonti, V, Bianchetti, MG, Stettbacher, A, et al. Vitamin D status among male late adolescents living in Southern Switzerland: Role of body composition and lifestyle. Nutrients. (2019) 11:2727. doi: 10.3390/nu11112727
139. Milani, GP, Simonetti, GD, Edefonti, V, Lava, SAG, Agostoni, C, Curti, M, et al. Seasonal variability of the vitamin D effect on physical fitness in adolescents. Scientific reports. (2021) 11:182. doi: 10.1038/s41598-020-80511-x
140. Fink, C, Peters, RL, Koplin, JJ, Brown, J, and Allen, KJ. Factors affecting Vitamin D status in infants. Children (Basel). (2019) 6:7. doi: 10.3390/children6010007
141. Viljakainen, HT, Saarnio, E, Hytinantti, T, Miettinen, M, Surcel, H, Mäkitie, O, et al. Maternal vitamin D status determines bone variables in the newborn. J Clin Endocrinol Metab. (2010) 95:1749–57. doi: 10.1210/jc.2009-1391
142. Castaneda, RA, Nader, N, Weaver, A, Singh, R, and Kumar, S. Response to Vitamin D3 supplementation in obese and non-obese Caucasian adolescents. Horm Res Paediatr. (2012) 78:226–31. doi: 10.1159/000343446
143. NICEOverview | Vitamin D: Supplement use in specific population groups | guidance. Avilable at: https://www.nice.org.uk/guidance/ph56 (Accessed September 20, 2022).
Keywords: vitamin D, micronutrients, vitamin supplementation, pediatric screening, child public health, dietary supplements, infant nutrition, rickets
Citation: Corsello A, Spolidoro GCI, Milani GP and Agostoni C (2023) Vitamin D in pediatric age: Current evidence, recommendations, and misunderstandings. Front. Med. 10:1107855. doi: 10.3389/fmed.2023.1107855
Edited by:
Sunita Taneja, Society for Applied Studies, IndiaReviewed by:
Pratibha Dwarkanath, St. John's Research Institute, IndiaCopyright © 2023 Corsello, Spolidoro, Milani and Agostoni. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Gregorio P. Milani, bWlsYW5pLmdyZWdvcmlvcEBnbWFpbC5jb20=
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.