 Eder Caceres1,2
Eder Caceres1,2 Juan C. Olivella1
Juan C. Olivella1 Miguel Yanez1
Miguel Yanez1 Emilio Viñan1
Emilio Viñan1 Laura Estupiñan1
Laura Estupiñan1 Natalia Boada1
Natalia Boada1 Ignacio Martin-Loeches3,4,5,6
Ignacio Martin-Loeches3,4,5,6 Luis Felipe Reyes1,7,8*
Luis Felipe Reyes1,7,8*- 1Unisabana Center for Translational Science, Universidad de La Sabana, Chía, Colombia
- 2Neurocritical Care Division, Critical Care Department, Clínica Universidad de La Sabana, Chía, Colombia
- 3Centro de Investigación Biomédica en Red de Enfermedades Respiratorias (CIBERES), Instituto de Salud Carlos III, Madrid, Spain
- 4Multidisciplinary Intensive Care Research Organization (MICRO), Department of Intensive Care Medicine, St. James's University Hospital, Dublin, Ireland
- 5Critical Care Department, Trinity Centre for Health Sciences, Dublin, Ireland
- 6Hospital Clínic, IDIBAPS, Universidad de Barcelona, Barcelona, Spain
- 7Facultad de Medicina, Universidad de La Sabana, Chía, Colombia
- 8Pandemic Science Institute, University of Oxford, Oxford, United Kingdom
Background: Traumatic brain injury (TBI) is a public health problem with a high burden in terms of disability and death. Infections are a common complication, with respiratory infections being the most frequent. Most available studies have addressed the impact of ventilator-associated pneumonia (VAP) after TBI; therefore, we aim to characterize the hospital impact of a broader entity, lower respiratory tract infections (LRTIs).
Methods: This observational, retrospective, single-center cohort study describes the clinical features and risk factors associated with LRTIs in patients with TBI admitted to an intensive care unit (ICU). We used bivariate and multivariate logistic regressions to identify the risk factors associated with developing LRTI and determine its impact on hospital mortality.
Results: We included 291 patients, of whom 77% (225/291) were men. The median (IQR) age was 38 years (28–52 years). The most common cause of injury was road traffic accidents 72% (210/291), followed by falls 18% (52/291) and assault at 3% (9/291). The median (IQR) Glasgow Coma Scale (GCS) score on admission was 9 (6–14), and 47% (136/291) were classified as severe TBI, 13% (37/291) as moderate TBI, and 40% (114/291) as mild TBI. The median (IQR) injury severity score (ISS) was 24 (16–30). Nearly 48% (141/291) of patients presented at least one infection during hospitalization, and from those, 77% (109/141) were classified as LRTIs, which included tracheitis 55% (61/109), ventilator-associated pneumonia (VAP) 34% (37/109), and hospital-acquired pneumoniae (HAP) 19% (21/109). After multivariable analysis, the following variables were significantly associated with LRTIs: age (OR 1.1, 95% CI 1.01–1.2), severe TBI (OR 2.7, 95% CI 1.1–6.9), AIS thorax (OR 1.4, 95 CI 1.1–1.8), and mechanical ventilation on admission (OR 3.7, 95% CI 1.1–13.5). At the same time, hospital mortality did not differ between groups (LRTI 18.6% vs. No LRTI 20.1%, p = 0.7), and ICU and hospital length of stay (LOS) were longer in the LRTI group (median [IQR] 12 [9–17] vs. 5 [3–9], p < 0.01) and (median [IQR] 21 [13–33] vs. 10 [5–18], p = 0.01), respectively. Time on the ventilator was longer for those with LRTIs.
Conclusion: The most common site/location of infection in patients with TBI admitted to ICU is respiratory. Age, severe TBI, thoracic trauma, and mechanical ventilation were identified as potential risk factors. LRTI was associated with prolonged ICU, hospital stay, and more days on a ventilator, but not with mortality.
Background
Traumatic brain injury (TBI) is a public health issue and a leading cause of mortality and disability in the younger population. Additionally, TBI impacts the quality of life of older adults, who usually have a reduced capacity to recover after these events (1, 2). TBI is associated with changes in the immune system mediated through inflammatory and autonomic pathways (3, 4) that seem to increase the susceptibility to infections during and after hospitalization (3–5). Among individuals with TBI who suffer nosocomial infections, a frequent source is the respiratory system or what we will denominate lower respiratory tract infections (LRTIs), including ventilator-associated pneumoniae (VAP), ventilator-associated tracheitis (VAT), and healthcare-associated pneumonia (HAP) (3, 6).
The most frequent sources of infection in previous cohorts of TBI have been respiratory and urinary, followed by surgical site infections. Regarding respiratory infections, a greater proportion of studies have focused on VAP. The frequency of VAP in these studies ranges from 31 to 47%, and some of them have found a positive correlation between VAP and several outcomes, including longer hospital stays and higher rates of mortality and disability. The severity of TBI, chest trauma, smoking history, drug abuse, and interventions, such as transfusions, sedation, and the need for a tracheostomy, are associated with VAP (7–11).
Other types of LRTIs might play a relevant role in the hospital course and outcomes of these patients (10). LRTIs could be considered a continuum spectrum of a single disease and, therefore, it might be valuable to describe its epidemiology and associated factors (12–14). This would allow a better understanding of this phenomenon and, accordingly, the development of measures to prevent and manage these complications. By identifying potential risk factors, we can highlight areas of care susceptible to improvement. In this study, our objectives are (a) to describe the epidemiology of lower respiratory tract infections (LRTIs) in our TBI cohort, (b) to determine factors associated with LRTI, and (c) to determine whether LRTI is associated with clinical outcomes (mortality, LOS).
Materials and methods
This is a retrospective, observational, single-center cohort of patients with traumatic brain injury (TBI) admitted to the intensive care unit (ICU). Using the electronic medical record, we searched for patients admitted to the ICU from August 2009 to December 2019 with the diagnosis of TBI. Once selected, the diagnosis was confirmed, and data were validated through a medical chart review. The Ethics Committee of Clínica Universidad de La Sabana approved this study and waived the need for informed consent as only routinely collected clinical data were recorded.
Data collection and storing
One or more dedicated and trained physicians collected clinical data through a medical chart review. These data included demographics, medical history, injury severity, and characteristics during the hospital stay. Data were collected using a Case report form (CRF) built on Research Electronic Data Capture (REDCap, version 8.11.11, Vanderbilt University, Nashville, Tenn.) hosted by the Universidad de Sabana. All study data were de-identified and stored securely by the Translational Science in Infectious Diseases and Critical Care Research Group at Universidad de La Sabana.
Definitions
Lower respiratory tract infection (LRTI) is used as a broad term that includes hospital-acquired pneumoniae (HAP), ventilator-associated pneumoniae (VAP), and ventilator-associated tracheobronchitis (VAT). These entities were diagnosed using the definition of IDSA/ATS guidelines (15). The IDSA guideline criteria were also followed to assess the diagnosis of other infectious complications, including catheter-associated urinary tract infection (CA-UTI), surgical site infection (SSI), and catheter-related bloodstream infection (CRBSI) (16–18). TBI severity was determined using the Glasgow Coma Scale (GCS). Subjects with mild head injury (GCS 13–15) were included in this cohort when they were admitted to ICU; usually, this occurs when there is a risk of clinical deterioration, other body part injuries, and/or comorbid conditions. The severity of trauma and body regions compromised was established using the Abbreviated Injury Score (AIS) and the Injury Severity Score (19). ISS is the sum of the squares of the highest AIS scores in the three most severely injured regions; it ranges from 1 to 75; the higher the score, the more severe the injury. Isolated TBI was defined as AIS head ≥3 and injury to any other region with AIS < 3. Patients with TBI and multiple traumas had AIS head ≥3 and trauma to any other body region with AIS ≥ 3.
Outcomes
The primary outcome was the diagnosis of LRTI during hospitalization. Clinical data were analyzed, and predictors of this primary outcome were identified. The secondary outcomes were hospital survival and the length of ICU and hospital stay.
Statistical analysis
We excluded patients for whom information on discharge or clinical severity was missing. The Shapiro–Wilk test was used to detect departures from normality, and numerical variables were reported as mean (DS) or median (IQR) according to distribution. Categorical data are reported as numbers and percentages. Logistic regression models were used to explore the predictor variables for the primary outcome. Potential predictors for the primary outcome were identified in a univariate analysis. Then, a multivariable model was constructed adjusting for TBI severity, the severity of the trauma, and illness severity scores (APACHE II, SOFA), with results reported as odds ratios (95% CI). For testing the goodness of fit, we used the Hosmer–Lemeshow test. In secondary outcomes analyses, differences in mortality and length of stay between subjects with and without LRTIs were analyzed using the chi-square test for differences in proportions and the Mann–Whitney U-test for non-parametric data. A two-tailed p-value of 0.05 or less was used to define statistical significance. Statistical analyses were performed using R (version 4.2.1) and Studio (version 2022.07.0) as the integrated development environment.
Results
From August 2009 to December 2019, 291 patients were enrolled. The baseline and clinical characteristics of the patients are presented in Table 1. The median (IQR) age was 38 (28–52) years, and men accounted for 77% (225/291) of the TBI admissions to the ICU. Road traffic accidents were the leading cause of TBI at 72% (210/291), followed by falls 18% (52/291) and assault at 3% (9/291). Median (IQR) GCS on admission was 9 (6–14), and 47% (136/291) were classified as severe TBI, 13% (37/291) as moderate TBI, and 40% (114/291) as mild TBI. Isolated TBI accounted for 21% (63/291), while the rest of the patients had associated injuries to at least one body region with AIS ≥ 3. In terms of lesions in other parts of the body, the more frequently compromised (AIS ≥ 3) were the thorax 29% (86/291), limbs 28% (84/291), and abdomen 14% (49/291). The median stay in the ICU was 7 (IQR, 4–13), and the median (IQR) hospital stay was 13 days (7–25 days). The frequency of patients requiring invasive ventilatory support was 83% (244/291), and the median (IQR) time on a ventilator was 5 days (3–9 days). Hospital mortality for this cohort was 19% (56/291), and survival time to death was 7 days (IQR, 4–13).
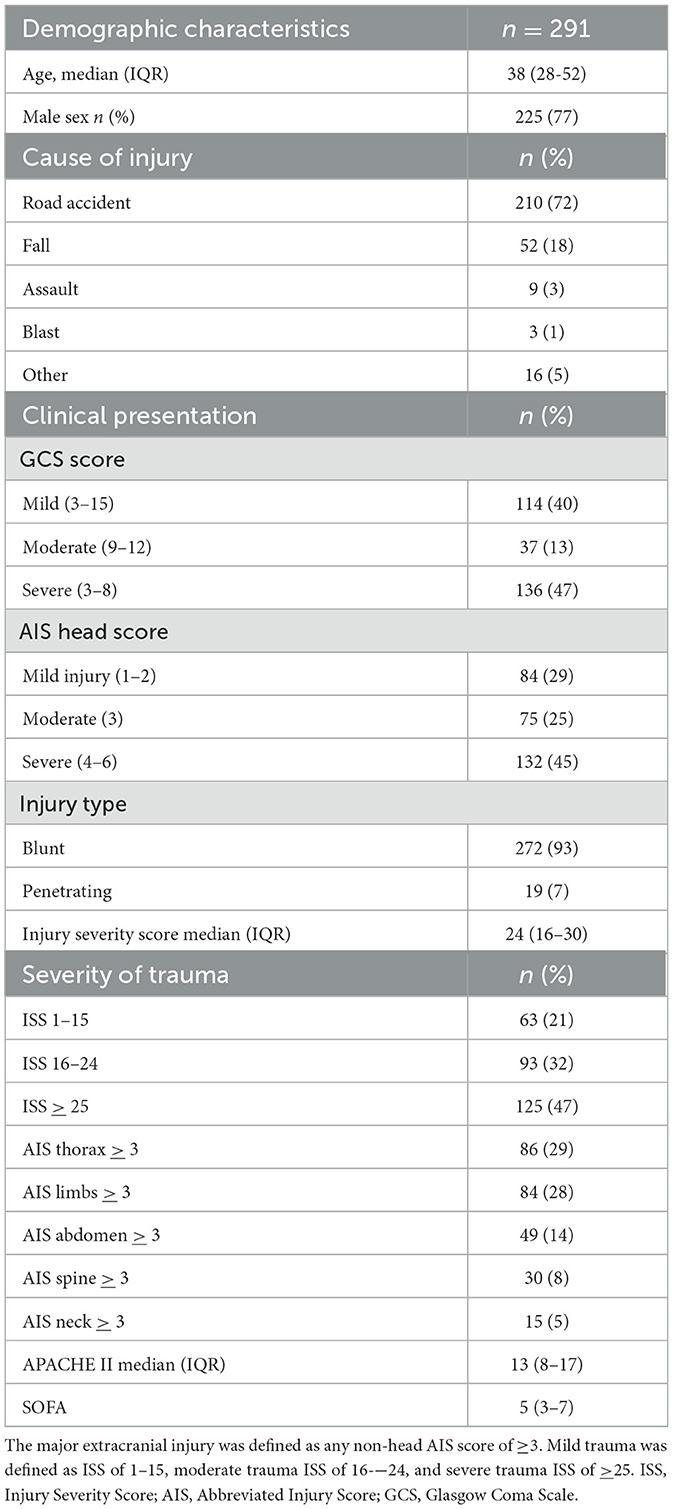
Table 1. Baseline and clinical characteristics of patients.
Infection complications were present in 48% (141/291) of patients, and from those, 77% (109/141) corresponded to LRTIs, 14% (20/141) to CA-UTI, 15% (22/141) to SSI, and 9% (14/141) to CRBSI. Regarding absolute frequency, 38% (109/291) had an LRTI, 7% (20/291) had a CA-UTI, 7% (22/291) had an SSI, and 5% (14/291) had a CRBSI. We obtained bacterial growth in 60% (62/109) of LRTI through bronchoalveolar lavage (BAL) of 16% (17/109) and tracheal aspirate of 32% (45/107). Most frequently, isolated bacteria were Staphylococcus aureus at 18% (20/109), Klebsiella pneumoniae at 10% (11/109), Enterobacter cloacae at 8% (9/109), Escherichia coli at 7% (8/109), Pseudomonas aeruginosa at 6% (7/109), and Serratia marcescens at 5% (6/109), among others with minor proportions. Among patients with LRTIs, 55% (61/109) were classified as TAV, 19% (21/109) as hospital-acquired pneumoniae (HAP), and 33% (37/109) as VAP. The median number of days in the hospital before presenting an LRTI was 5 (IQR, 3–9).
Univariate comparison between cohorts with and without LRTIs (Table 2) revealed that patients who had an LRTI were significantly older (median [IQR] 43 years [32–55] vs. 37 years [IQR 25–50], p = 0.016) and had more severe head injuries according to GCS (median [IQR], 7 [5–13] vs. 12 [7–14], p < 0.01) and AIS head (median [IQR], 4 [3–4] vs. 3 [2–4], p < 0.01). APACHE II and SOFA scores were also higher for those patients with LRTIs (median [IQR], 14 [11–18] vs. 12 [6–17], p = 0.017) and 5 [4–7] vs. 4 [3–6], p < 0.01). In terms of the overall severity of the injury, including other body regions, severity by ISS was worse for the LRTI cohort (median [IQR], 26 [18–33] vs. 22 [14–29], p = 0.014). While hospital mortality did not differ between groups (LRTI 18.6% vs. No LRTI 20.1%, p = 0.7), ICU LOS was longer in the LRTI group (median [IQR] 12 [9–17] vs. 5 [3–9], p < 0.01). Furthermore, hospital LOS was also longer for those with LRTIs when compared to patients without LRTIs (median [IQR] 21 [13–33] vs. 10 [5–18], p = 0.01). Time on the ventilator was significantly longer for those with LRTIs (median [IQR] 9 [5–12] vs. 4 [3–7], p < 0.01).
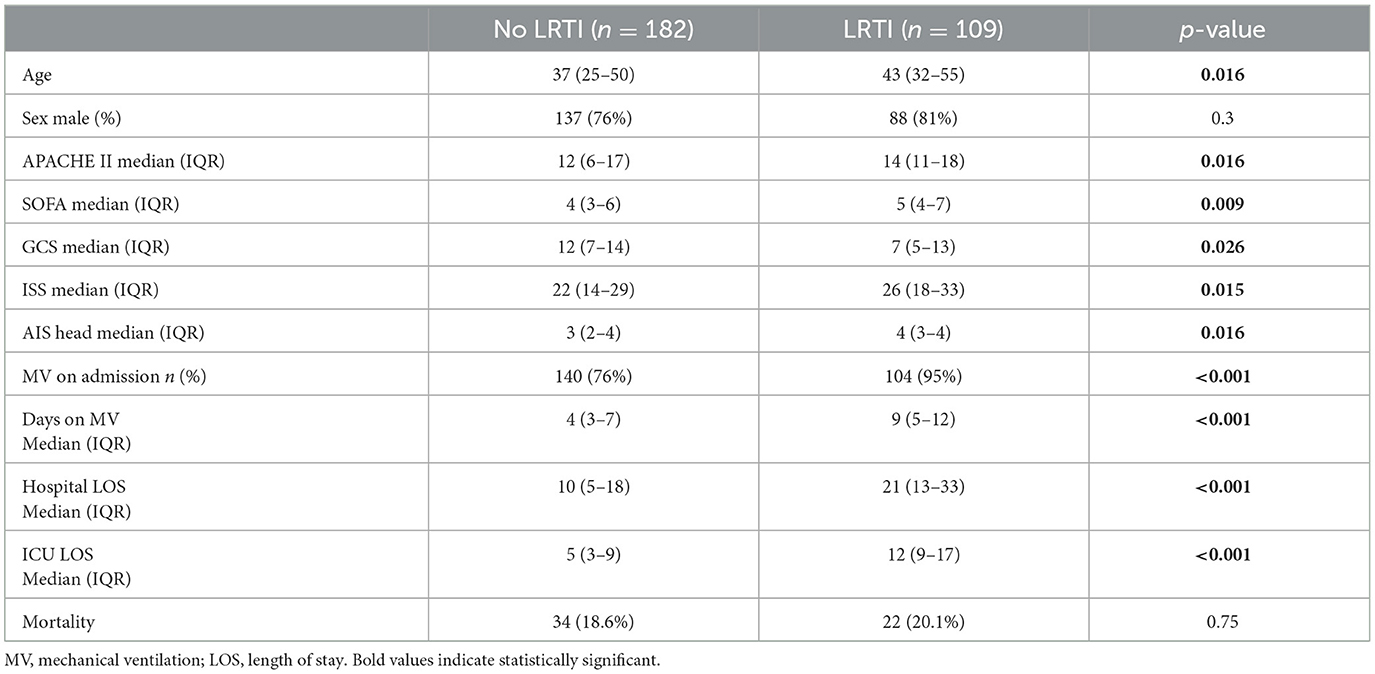
Table 2. Univariate comparison of baseline characteristics of TBI patients with and without LRTIs.
Potential predictors for the primary outcome (LRTIs) were identified in the bivariate analysis (p < 0.1) and included age, ISS, mean blood pressure on admission, GCS, AIS of the head and the thorax, hemoglobin on admission, serum glucose on admission, SOFA, APACHE II, and invasive mechanical ventilation on admission. After multivariable analysis, the following variables remained significantly associated with LRTI (p < 0.05): age (OR 1.1, 95% CI, 1.01–1.2), severe TBI (OR 2.7, 95% CI, 1.1–6.9), AIS thorax (OR 1.4, 95% CI, 1.1–1.8), and mechanical ventilation on admission (OR 3.7, 95% CI, 1.1–13.5) (Table 3).
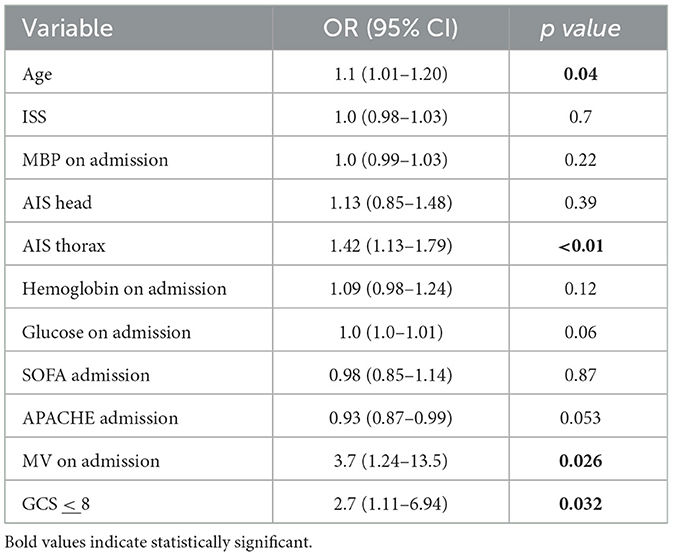
Table 3. Multivariate logistic regression analysis for LRTI in TBI patients admitted to ICU.
In univariate analysis, LRTI was not significantly associated with mortality (OR 1.01, 95% CI 0.88–1.18, p = 0.7). Variables associated with mortality (p < 0.1) in the univariate analysis included AIS head (OR 1.1, 95% CI 1.07–1.13, p < 0.01), ISS (OR 1.01, 95% CI 1.001–1.1, p < 0.01), oxygen saturation on admission (OR 0.5, 95% CI, 0.3–0.9, p = 0.03), severe TBI (CGS ≤ 8) (OR 1.2, 95% CI 1.08–1.31, p ≤ 0.01), SOFA score (OR 1.03, 95% CI 1.01–1.05, p < 0.001), APACHE II score (OR 1.02, 95% CI 1.01–1.03, p < 0.001), and blood transfusions (OR 1.1, 95% CI 1.01–1.22, p = 0.02).
Variables associated with mortality in the multivariable analysis included AIS head, APACHE II score, and transfusion of blood components (Table 4). Multivariate logistic regression also failed to demonstrate a significant association between LRTIs and mortality.
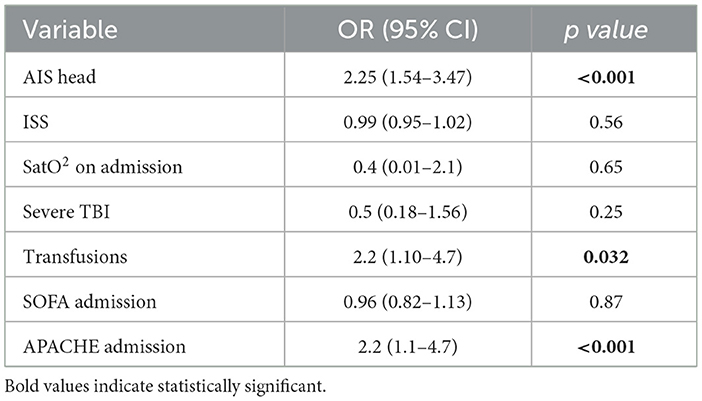
Table 4. Multivariate logistic regression analysis for mortality in TBI patients admitted to ICU.
Discussion
In this study, we found that a diagnosis of infection was made in almost half of the patients, with the respiratory system being the prevailing source. Among the different types of LRTIs, the most frequent was VAT. Patients who presented an LRTI had a more severe injury to the head and other body regions, had greater disease severity scores, and were older. We identified the following potential predictors for developing LRTIs after TBI in the ICU: age, severe TBI, trauma to the thorax, and being on mechanical ventilation. When comparing outcomes, those who presented with an LRTI stayed longer in the ICU and the hospital and spent more days on mechanical ventilation. However, mortality was not different even after adjusting for age and severity of trauma. This is consistent with a recent large prospective multicenter study that focused on VAP (10).
Previous cohorts had characterized the epidemiology of infections in TBI and found a respiratory source in frequencies as high as 94% of cases (20, 21). We assessed the diagnosis of LRTI through the ATS/IDS guidelines, which include clinical, radiological, and microbiologic criteria. Interestingly in our cohort, the most common type of LRTI was VAT, diagnosed in patients with fever, new or increased sputum production, microbial isolation in tracheal aspirate, and no radiographic evidence of pneumonia (15). Diagnosis and treatment of VAT are controversial and not readily recognized by some, partly due to the difficulty in evaluating infiltrates in a portable X-ray in the ICU. Moreover, severely traumatized patients might have potential confounders like lung contusion and aspiration. However, in the available literature, VAT has been associated with worse clinical outcomes, including progression to VAP, more extended ICU stay, and time on mechanical ventilation (13, 14). Our results underline the importance of a continuous and individualized evaluation of cases at a higher risk of LRTI, always considering differential diagnoses and context when suspecting a respiratory infection. This approach might lead to an earlier and more precise antibiotic prescription for those with a straightforward diagnosis and to avoid the widespread use of antibiotics when not readily indicated. Furthermore, we must strengthen our bundles of care in mechanical ventilation for this population to prevent and decrease LRTIs.
Patients with LRTI in our cohort were older and more severely traumatized. However, after multivariate analysis, the potential risk factors that remained were age, the severity of TBI, thoracic trauma, and being on mechanical ventilation. Other studies have found different variables associated with LRTIs, including blood transfusions, barbiturates infusion, spinal trauma, and ISS (11, 12, 14). Thoracic trauma represents a structural lung disruption that leads to inflammatory changes but does not necessarily end in a respiratory infection (22–24). As differentials, lung contusion, or aspiration warrants a thorough evaluation before diagnosing LRTI and prescribing antibiotics.
We found the severity of TBI as a potential risk factor for LRTIs. Patients with worse TBI might need higher and longer doses of sedation and are more frequently on advanced respiratory support (25, 26). These variables (sedation and mechanical ventilation) have been identified as predictors of LRTI (11). Additionally, we want to highlight that some clinical and preclinical evidence has highlighted that TBI might induce a state of immune depression through inflammatory and autonomic pathways (27, 28). This might facilitate the occurrence of sepsis, not only in the acute phase but also afterward (4). Several animal models have shown evidence that TBI induces cell death mechanisms, including apoptosis, programmed necrosis, or necroptosis (29, 30). Defects in membrane integrity and the release of intracellular components that act like damage-associate molecular patterns (DAMP) induce the further release of cytokines and assembling inflammasomes (8).
The IMPACT study demonstrated that plasma cytokine concentrations are associated with organ dysfunction, mortality, and poor outcomes in TBI [32]. Further research is needed on how this state of immune depression affects outcomes in the TBI population.
Regarding outcomes, patients who suffered from LRTIs had longer ICU and hospital stays and spent longer on respiratory support than those without LRTIs. However, mortality was not significantly different between those cohorts. Previous studies found that LRTI was associated with longer hospital stays, mechanical ventilation, and healthcare costs, coinciding with our results. On the contrary, the results regarding mortality might differ among cohorts (7, 13, 14). One meta-analysis included 15 studies of VAP in TBI and found longer hospitalization but no significant difference in mortality (11). These findings could be related to the awareness of the risk of infection and early antibiotic prescription in cases suspected to have LRTI, which avoids the progression of sepsis and death. However, antibiotics are sometimes not indicated, leading to overuse and increased bacterial resistance. Another explanation for no difference in mortality could be the heterogeneity in the type and severity of TBI, associated injuries, and criteria used for diagnosis of LRTI. These variables might be a difficulty when comparing cohorts and analyzing outcomes.
The main limitation of this study is that patient enrollment was retrospective using electronic medical records. Data collection relied on previous registries, which makes some information challenging to confirm. However, we used standardized definitions and scores to address this limitation and to confirm admission and hospital diagnoses. Outcomes and complications were also evaluated using a thorough medical chart review. Another limitation we acknowledge is that it was a single-center study, which means the generalizability of results can be compromised.
In conclusion, LRTI is a frequent complication in patients with TBI and impacts clinical outcomes. Potential predictors of LRTI were identified; however, these findings are meant to be translated in the future into new hypotheses that deepen our understanding of the immune response in patients with TBI and ultimately lead to the design of novel prognostic and therapeutic tools.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by Universidad de La Sabana. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
Author contributions
EC: data analysis, statistical analysis, writing, and edition. MY, EV, and JO: data gathering, review, and edition. LE: data gathering, writing, and edition. NB: data gathering and edition. IM-L: writing, review, and edition. LR: data analysis, writing, review, and edition. All authors contributed to the article and approved the submitted version.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Gao G, Wu X, Feng J, Hui J, Mao Q, Jiang J, et al. Clinical characteristics and outcomes in patients with traumatic brain injury in China: a prospective, multicentre, longitudinal, observational study. Lancet Neurol. (2020) 19:670–7. doi: 10.1016/S1474-4422(20)30182-4
2. James SL, Bannick MS, Montjoy-Venning WC, Lucchesi LR, Dandona L, Dandona R, et al. Global, regional, and national burden of traumatic brain injury and spinal cord injury, 1990-2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. (2019) 18:56–87. doi: 10.1016/S1474-4422(18)30415-0
3. Meisel C, Schwab JM, Prass K, Meisel A, Dirnagl U. Central nervous system injury-induced immune deficiency syndrome. Nat Rev Neurosci. (2005) 6:775–86. doi: 10.1038/nrn1765
4. Sharma R, Shultz SR, Robinson MJ, Belli A, Hibbs ML, O'Brien TJ, et al. Infections after a traumatic brain injury: The complex interplay between the immune and neurological systems. Brain Behav Immun. (2019) 79:63–74. doi: 10.1016/j.bbi.2019.04.034
5. Kourbeti IS, Vakis AF, Papadakis JA, Karabetsos DA, Bertsias G, Filippou M, et al. Infections in traumatic brain injury patients. Clin Microbiol Infect. (2012) 18:359–64. doi: 10.1111/j.1469-0691.2011.03625.x
6. Harrison-Felix C, Whiteneck G, Devivo MJ, Flora D, Hammond M, Jha A. Causes of death following 1 year postinjury among individuals with traumatic brain injury. J Head Trauma Rehabil. (2006) 21:22–33. doi: 10.1097/00001199-200601000-00003
7. Hazeldine J, Lord JM, Belli A. Traumatic brain injury and peripheral immune suppression: primer and prospectus. Front Neurol. (2015) 6:235. doi: 10.3389/fneur.2015.00235
8. Zyung D, Zuege D, Boiteau P, Laupland K, Henderson E, Kortbeek J, et al. Ventilator-associated pneumonia in severe traumatic brain injury. Neurocrit Care. (2006) 5:108–14. doi: 10.1385/NCC:5:2:108
9. Bartolo M, Zucchella C, Aabid H, Valoriani B, Copetti M, Fontana A, et al. Impact of healthcare-associated infections on functional outcome of severe acquired brain injury during inpatient rehabilitation. Sci Rep. (2022) 12:5245. doi: 10.1038/s41598-022-09351-1
10. Glance LG, Stone PW, Mukamel DB, Dick AW. Increases in mortality, length of stay, and cost associated with hospital-acquired infections in trauma patients. Arch Surg. (2011) 146:794–801. doi: 10.1001/archsurg.2011.41
11. Kalil AC, Metersky ML, Klompas M, Muscedere J, Sweeney DA, Palmer LB, et al. Management of adults with hospital-acquired and ventilator-associated pneumonia: 2016 clinical practice guidelines by the infectious diseases society of america and the american thoracic society. Clin Infect Dis. (2016) 63:e61–111. doi: 10.1093/cid/ciw353
12. Greenspan L, McLellan BA, Greig H. Abbreviated injury scale and injury severity score: a scoring chart. J Trauma. (1985) 25:60–4. doi: 10.1097/00005373-198501000-00010
13. Anderson D, Kutsogiannis DJ, Sligl WI. Sepsis in Traumatic Brain Injury: Epidemiology and Outcomes. Canadian J Neurol Sci. (2020) 47:197–201. doi: 10.1017/cjn.2019.320
14. Cardozo LCM, da Silva RR. Sepse em pacientes com traumatismo craniencefálico em unidade de terapia intensiva: fatores relacionados à maior mortalidade. Rev Bras Ter Intensiva. (2014) 26:148–54. doi: 10.5935/0103-507X.20140022
15. Craven DE, Lei Y, Ruthazer R, Sarwar A, Hudcova J. Incidence and outcomes of ventilator-associated tracheobronchitis and pneumonia. Am J Med. (2013) 126:542–9. doi: 10.1016/j.amjmed.2012.12.012
16. Martin-Loeches I, Póvoa P, Rodríguez A, Curcio D, Suarez D, Mira JP, et al. Incidence and prognosis of ventilator-associated tracheobronchitis (TAVeM): A multicentre, prospective, observational study. Lancet Respir Med. (2015) 3:859–68. doi: 10.1016/S2213-2600(15)00326-4
17. Li Y, Liu C, Xiao W, Song T, Wang S. Incidence, risk factors, and outcomes of ventilator-associated pneumonia in traumatic brain injury: a meta-analysis. Neurocrit Care. (2020) 32:272–85. doi: 10.1007/s12028-019-00773-w
18. Salluh JIF, de Souza-Dantas VC, Martin-Loeches I, Lisboa TC, Rabello LSCF, Saad N, et al. Ventilator-associated tracheobronchitis: An update. Rev Bras Ter Intensiva. (2019) 31:541–7. doi: 10.5935/0103-507X.20190079
19. Wutzler S, Bläsius FM, Störmann P, Lustenberger T, Frink M, Maegele M, et al. Pneumonia in severely injured patients with thoracic trauma: Results of a retrospective observational multicentre study. Scand J Trauma Resusc Emerg Med. (2019) 27:1–10. doi: 10.1186/s13049-019-0608-4
20. Michelet P, Couret D, Brégeon F, Perrin G, D'Journo XB, Pequignot V, et al. Early onset pneumonia in severe chest trauma: A risk factor analysis. J Trauma - Injury, Infect Crit Care. (2010) 68:395–400. doi: 10.1097/TA.0b013e3181a601cb
21. Plurad DS, Kim D, Bricker S, Lemesurier L, Neville A, Bongard F, et al. Ventilator-associated pneumonia in severe traumatic brain injury: The clinical significance of admission chest computed tomography findings. J Surg Res. (2013) 183:371–6. doi: 10.1016/j.jss.2013.01.036
22. Hawryluk GWJ, Aguilera S, Buki A, Bulger E, Citerio G, Cooper DJ, et al. A management algorithm for patients with intracranial pressure monitoring: the Seattle International Severe Traumatic Brain Injury Consensus Conference (SIBICC). Inten Care Med. (2019) 45:1783–94. doi: 10.1007/s00134-019-05805-9
23. Nilsson P, Enblad P, Chambers I, Citerio G, Fiddes H, Howells T, et al. Survey of traumatic brain injury mangement in European Brain IT centers year 2001. Acta Neurochir. (2005) 95:51–3. doi: 10.1007/3-211-32318-X_11
24. Doran SJ, Henry RJ, Shirey KA, Barrett JP, Ritzel RM, Lai W, et al. Early or Late Bacterial Lung Infection Increases Mortality after Traumatic Brain Injury in Male Mice and Chronically Impairs Monocyte Innate Immune Function. Crit Care Med. (2020) 48:E418–28. doi: 10.1097/CCM.0000000000004273
25. Liu ZM, Chen QX, Chen ZB, Tian DF Li MC, Wang JM, et al. RIP3 deficiency protects against traumatic brain injury (TBI) by suppressing oxidative stress, inflammation, and inflammation apoptosis: Dependent on AMPK pathway. Biochem Biophys Res Commun. (2018) 499:112–9. doi: 10.1016/j.bbrc.2018.02.150
26. Yang XS Yi TL, Zhang S, Xu ZW Yu ZQ, Sun HT, et al. Hypoxia-inducible factor-1 alpha is involved in RIP-induced necroptosis caused by in vitro and in vivo ischemic brain injury. Sci Rep. (2017) 7:1–11. doi: 10.1038/s41598-017-06088-0
27. Liesz A, Dalpke A, Mracsko E, Antoine DJ, Roth S, Zhou W, et al. DAMP signaling is a key pathway inducing immune modulation after brain injury. J Neuroscience. (2015) 35:583–98. doi: 10.1523/JNEUROSCI.2439-14.2015
28. Kuwar R, Rolfe A, Di L, Xu H, He L, Jiang Y, et al. A novel small molecular NLRP3 inflammasome inhibitor alleviates neuroinflammatory response following traumatic brain injury. J Neuroinflammation. (2019) 16:1–14. doi: 10.1186/s12974-019-1471-y
29. Irrera N, Russo M, Pallio G, Bitto A, Mannino F, Minutoli L, et al. The role of NLRP3 inflammasome in the pathogenesis of traumatic brain injury. Int J Mol Sci. (2020) 21:1–18. doi: 10.3390/ijms21176204
Keywords: traumatic brain injury, hospital-acquired pneumonia, ventilator-associated tracheitis, ventilator-associated pneumonia, multiple trauma, acute brain injury
Citation: Caceres E, Olivella JC, Yanez M, Viñan E, Estupiñan L, Boada N, Martin-Loeches I and Reyes LF (2023) Risk factors and outcomes of lower respiratory tract infections after traumatic brain injury: a retrospective observational study. Front. Med. 10:1077371. doi: 10.3389/fmed.2023.1077371
Received: 22 October 2022; Accepted: 22 March 2023;
Published: 17 April 2023.
Edited by:
Marcos Ferreira Minicucci, São Paulo State University, BrazilReviewed by:
Marco Carbonara, IRCCS Ca' Granda Foundation Maggiore Policlinico Hospital, ItalyBrenda M. Morrow, University of Cape Town, South Africa
Copyright © 2023 Caceres, Olivella, Yanez, Viñan, Estupiñan, Boada, Martin-Loeches and Reyes. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Luis Felipe Reyes, bHVpcy5yZXllczVAdW5pc2FiYW5hLmVkdS5jbw==